Embed Size (px)
Citation preview
The Hand
Bucky Boaz, ARNP-C
Examination of the Upper Extremity
A detailed history should include:Patient’s ageHandednessOccupationHobbiesChief complaintDescription of how and when the problem startedDuration of symptomsAggravating and alleviating factors
Examination of the Upper Extremity
If an injury is involved:The environment in which the injury or insult occurred should be determined.
If crush injury, are heat or chemicals involved?Was the environment clean or dirty?
Past medical history is useful in the presence of systemic conditions that have manifestations in the hand.
Anatomy Review
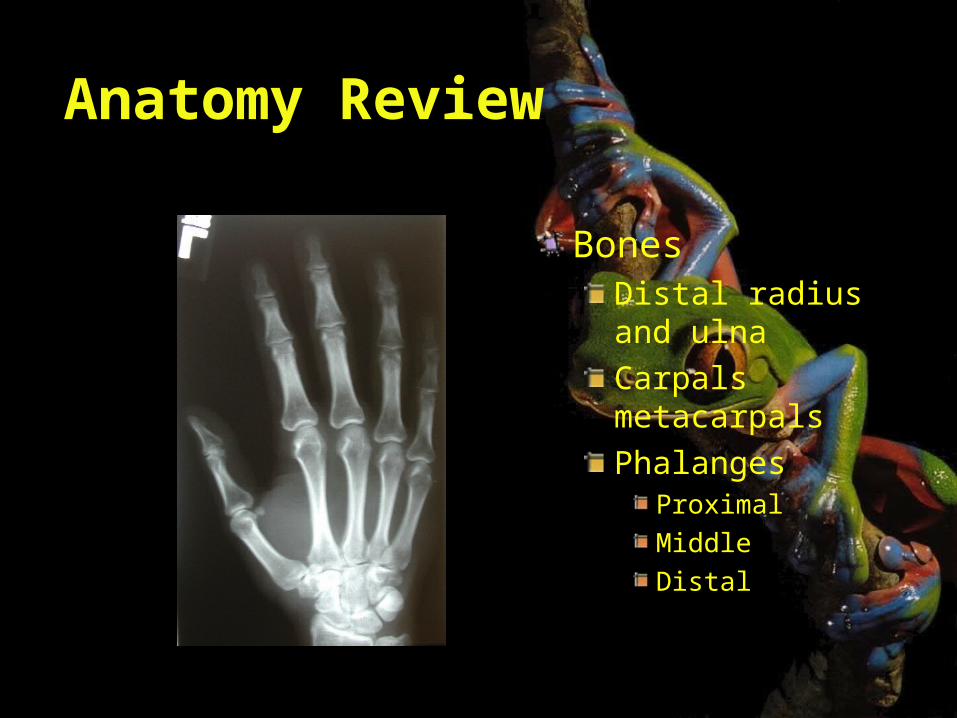
BonesDistal radius and ulnaCarpals metacarpalsPhalanges
ProximalMiddleDistal
Anatomy Review
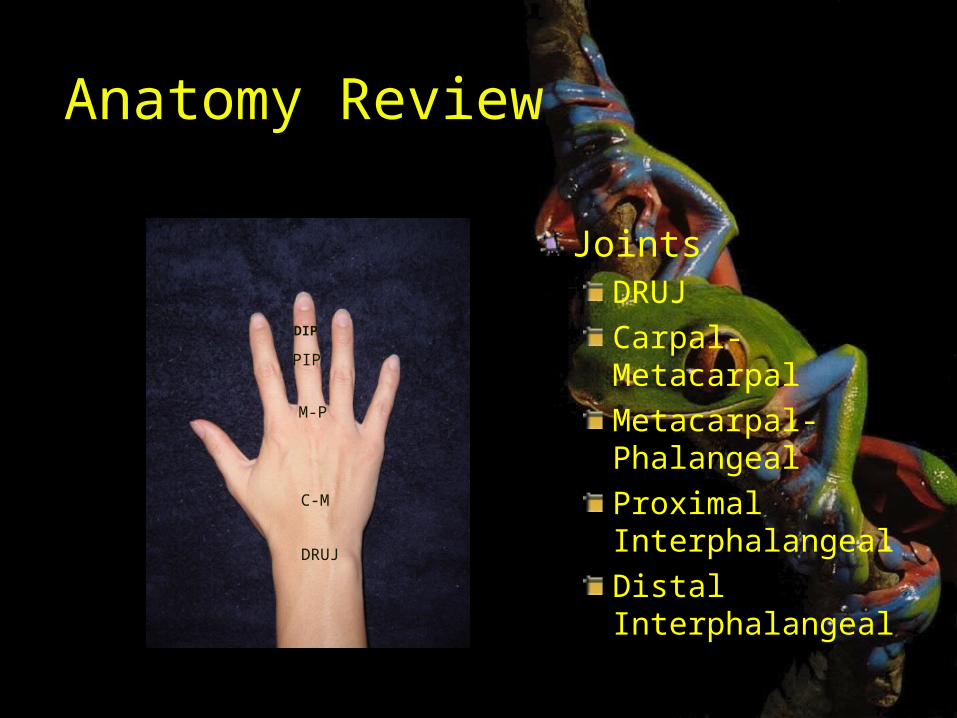
JointsDRUJCarpal-MetacarpalMetacarpal-PhalangealProximal InterphalangealDistal Interphalangeal
DRUJ
C-M
M-P
PIP
DIP
Anatomy Review
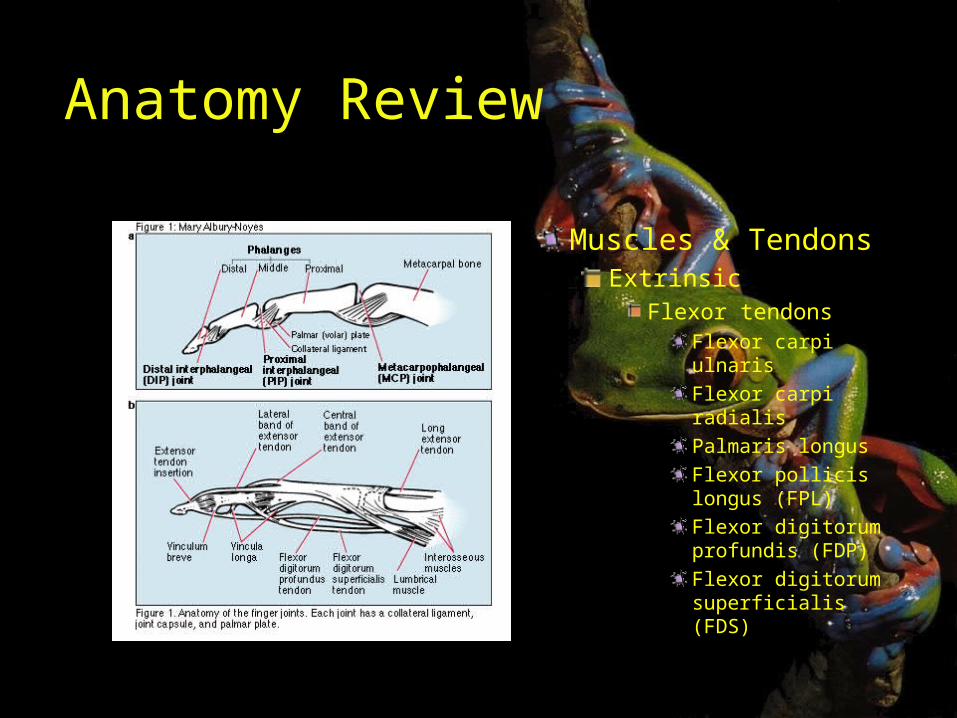
Muscles & TendonsExtrinsic
Flexor tendonsFlexor carpi ulnarisFlexor carpi radialisPalmaris longusFlexor pollicis longus (FPL)Flexor digitorum profundis (FDP)Flexor digitorum superficialis (FDS)
Anatomy Review
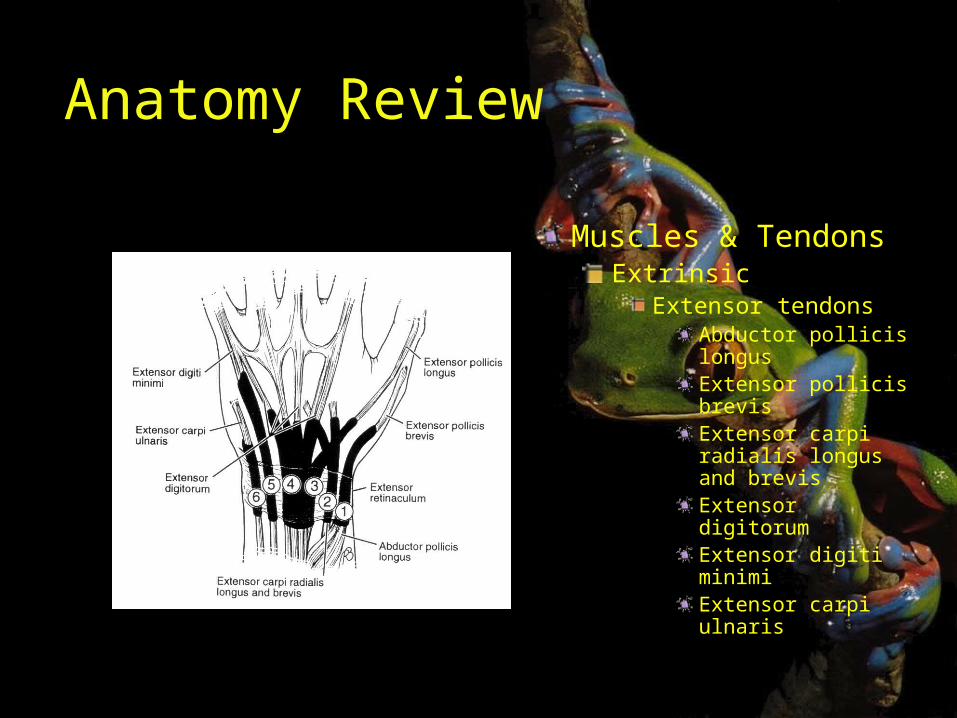
Muscles & TendonsExtrinsic
Extensor tendonsAbductor pollicis longusExtensor pollicis brevisExtensor carpi radialis longus and brevisExtensor digitorumExtensor digiti minimiExtensor carpi ulnaris
Anatomy Review
Muscles & Tendons
ExtrinsicExtension of MPFlex of IP
IntrinsicAbduct and adduct fingersFlexion of MPExtension of IP
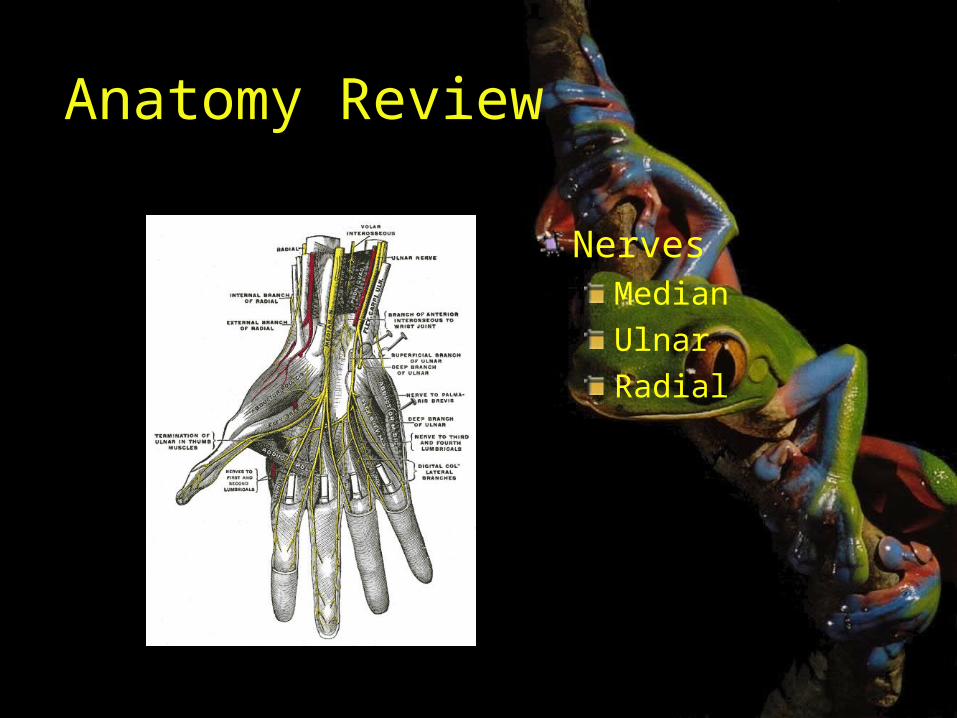
Anatomy Review
NervesMedianUlnarRadial
Examination of the Hand and Wrist
Complete exam:ObservationPalpationRange of motionNeurologic testingVascular assessmentStability testing
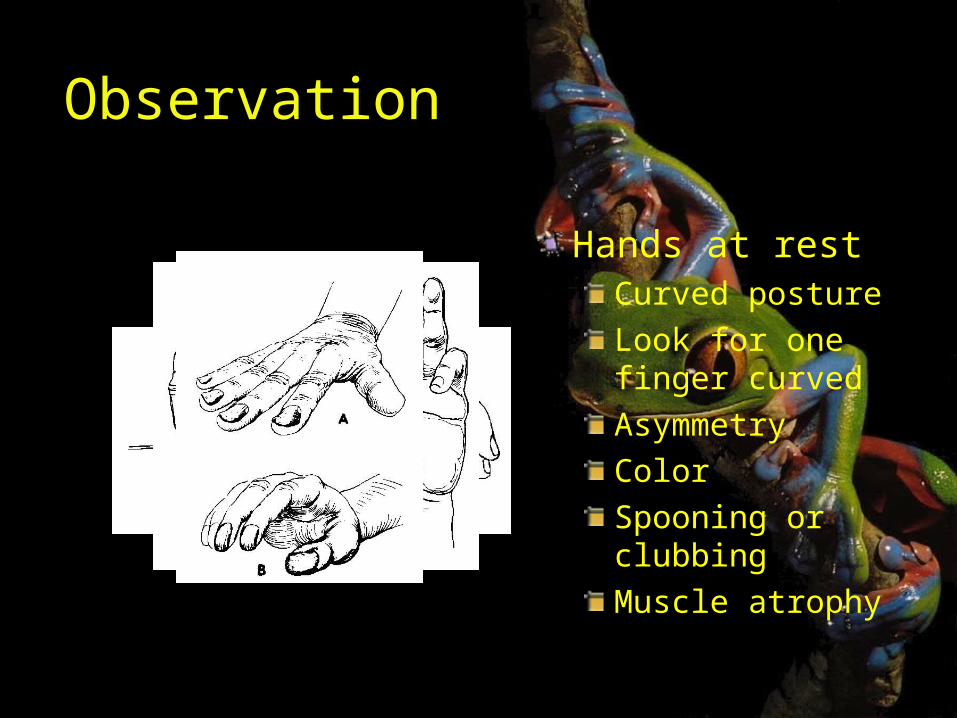
Observation
Hands at restCurved postureLook for one finger curvedAsymmetryColorSpooning or clubbingMuscle atrophy
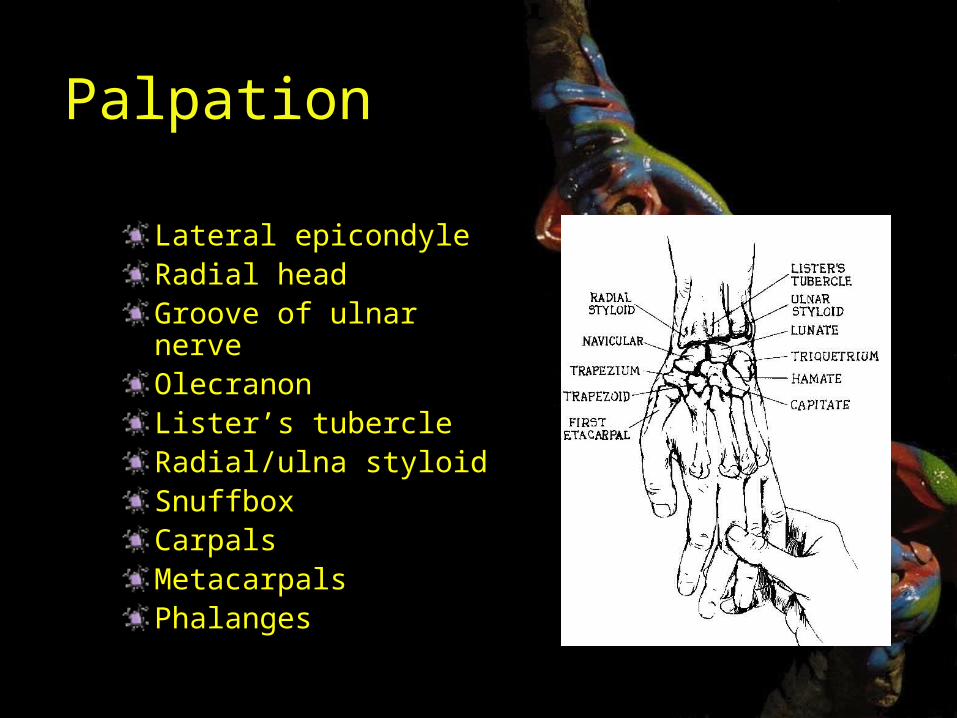
Palpation
Lateral epicondyleRadial headGroove of ulnar nerveOlecranonLister’s tubercleRadial/ulna styloidSnuffboxCarpalsMetacarpalsPhalanges
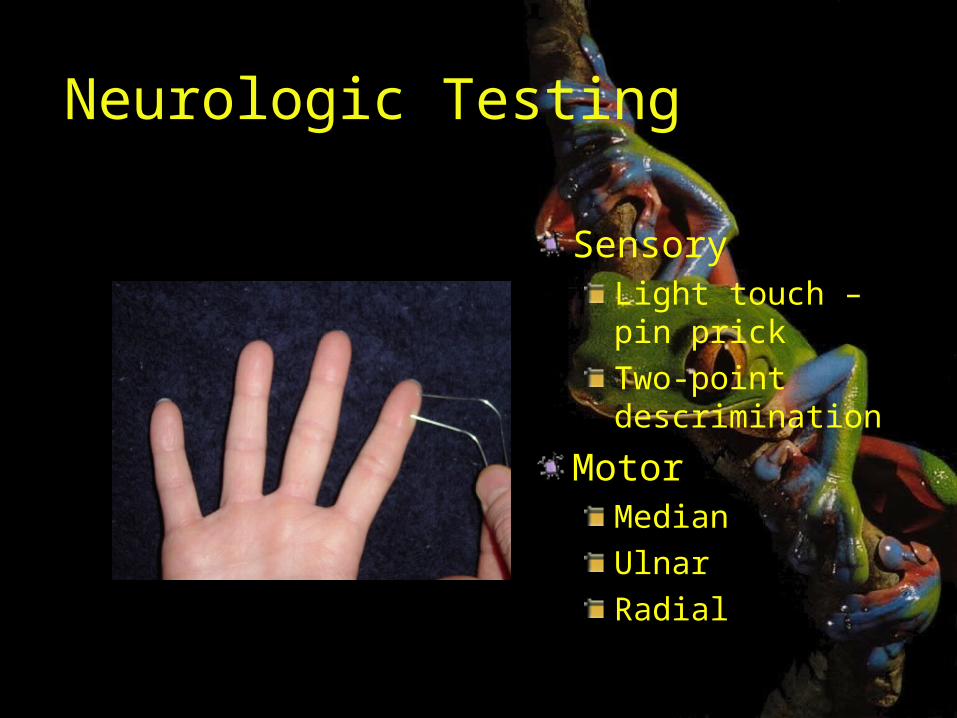
Neurologic Testing
SensoryLight touch – pin prickTwo-point descrimination
MotorMedianUlnarRadial
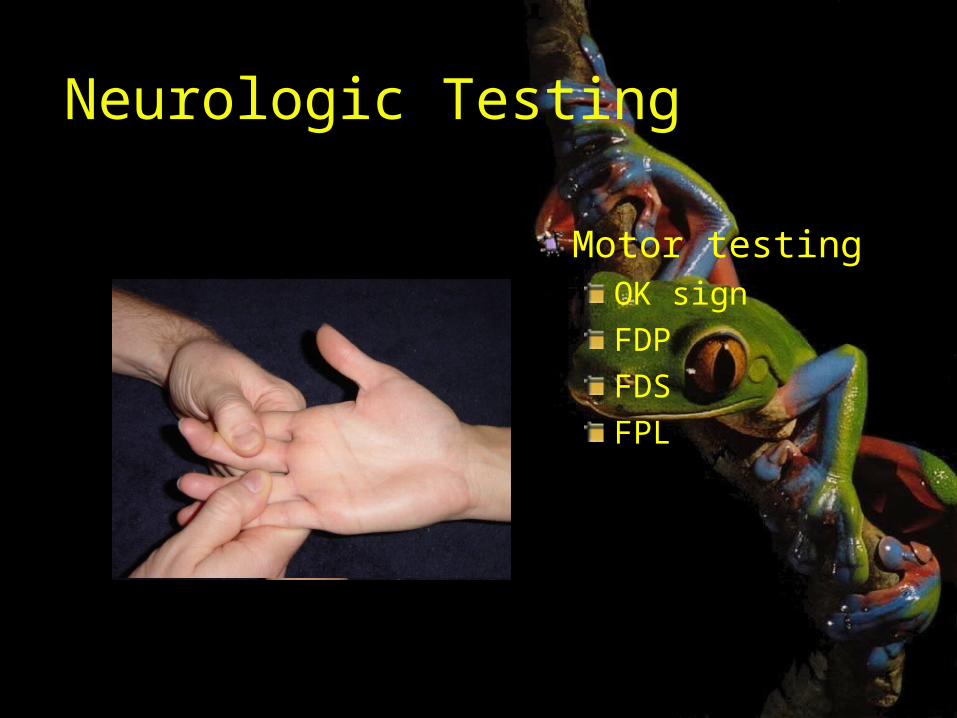
Neurologic Testing
Motor testingOK signFDPFDSFPL
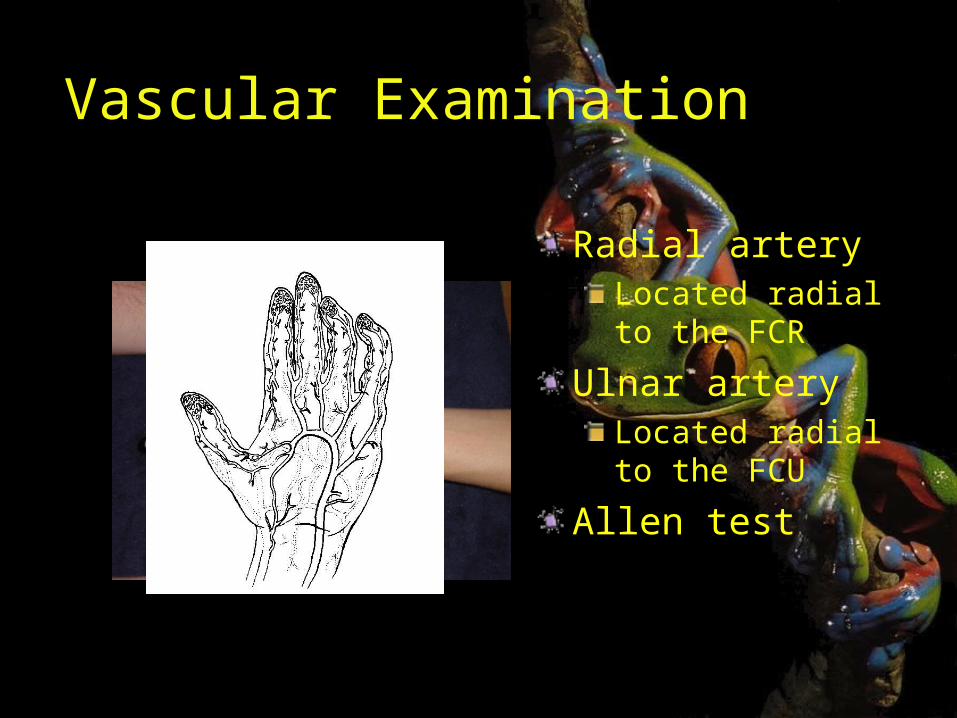
Vascular Examination
Radial arteryLocated radial to the FCR
Ulnar arteryLocated radial to the FCU
Allen test
Stability Testing
Ulnar collateral ligamentsRadial collateral ligamentsGamekeeper’s/ skier’s thumb
Special Tests
Finklestein’s testFroment’s signWatson testShuck testBasal joint grindCompression testPhalen’s testTinel’s sign
TAP
Common Traumatic Injuriesof the Hand
Bone and Soft Tissue

Considerations on Treating Hand Injuries
Type of injuryThe patient
Associated diseasesSocioeconomic factorsAbility to cooperate with treatment planMotivation to get well
Managing the patientRecognizing the injuryMaking the proper diagnosisInitiating the appropriate care plan
Referrals
Emergent referralsOpen fracturesFractures with neurovascular compromiseSignificant soft tissue injuryIrreducible dislocations or fractures with significant deformity
Referrals
Urgent referrals (next day or two)Closed flexor or extensor tendon injuriesDisplaced, angulated, or malrotated closed fracturesCarpal bone and distal radius fractures
History
Complete historyHand dominanceOccupationAvocationsCircumstances surrounding the injury
When and whereMechanism of injury
Location and character of painNumbness or tingling
Radiographs
Examine prior to ordering filmsStress views are useful in demonstrating injuries not present on plain viewsOccasionally CT scan or MRI are needed to evaluate an injury
Description of Fractures
Be able to accurately describe a radiograph to a colleague
Correct name of bone or joint involvedOpen or closed fractureIntraarticular or extraarticularWhether the fracture is shortened, displaced, malrotated, or angulatedFracture pattern
Description of Dislocations
Be able to accurately describe a dislocation
Described with the position of the distal bone relative to the proximal bone
Dorsal vs volar dislocationRadial vs ulnar dislocationCan have a combination of two

Complications
By far, the largest potential problem with any hand or wrist injury is stiffness.Soft tissue complications:
Tendon adhesionsCapsular contractures
Fracture healing timeHand: 3-4 weeksDistal radius: 5-7 weeks
Complications
Bony complications:MalunionAngulationMalrotationShorteningIntra-articular step-offNonunion is uncommon in hand or wrist
Fractures of the Distal Phalanx
The distal phalanx is the most common fracture in the hand, accounting for approximately 50% of hand fractures
Fractures of the Distal Phalanx
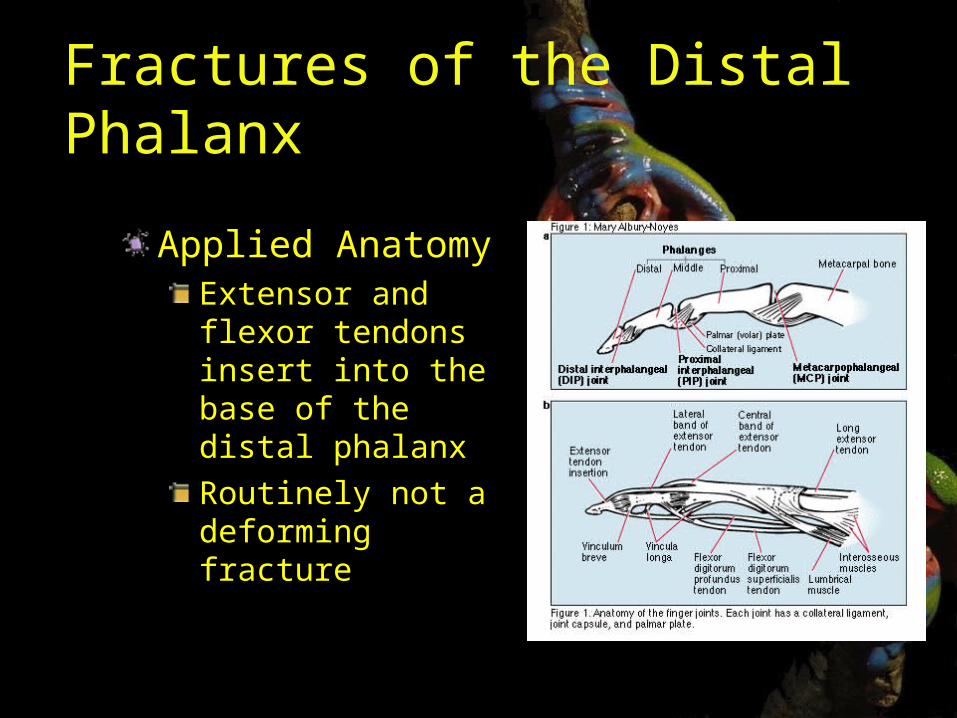
Applied AnatomyExtensor and flexor tendons insert into the base of the distal phalanxRoutinely not a deforming fracture
Fractures of the Distal Phalanx
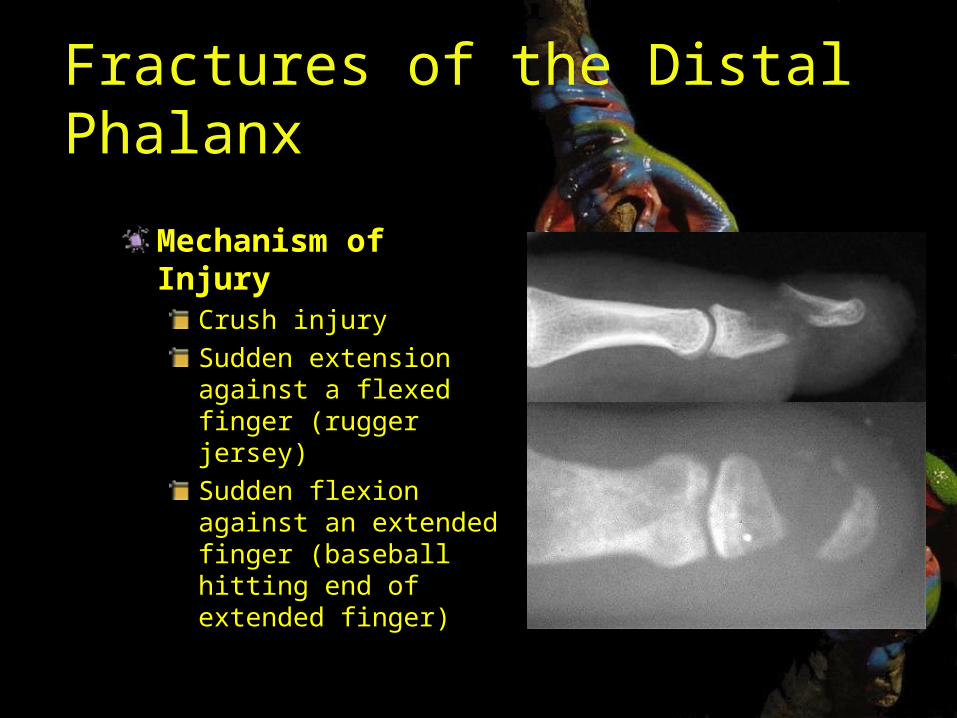
Mechanism of Injury
Crush injurySudden extension against a flexed finger (rugger jersey)Sudden flexion against an extended finger (baseball hitting end of extended finger)
Fractures of the Distal Phalanx
Associated Injuries
Nailbed lacerationsNail plate avulsionSkin lacerationsSubungal hematoma
History and Physical Exam
Check both flexor and extensor functionDocument sensory exam
Fractures of the Distal Phalanx
Radiographs2 – 3 views to look for fractureUse hot light if needed
ClassificationLongitudinalTransversecomminuted
TreatmentNon-displaced or minimally displaced can use variety of splints
Immobilize the DIP only
Reduce displaced fracturesOpen wounds may need more definitive treatment
Fractures of the Distal Phalanx
OutcomesCold intoleranceTip sensitivityStiffnessNailplate irregularities
When to referOpen fractures in need of nail bed repairLarge skin lossSuspected flexor or extensor tendon involvement
Nailbed Injury
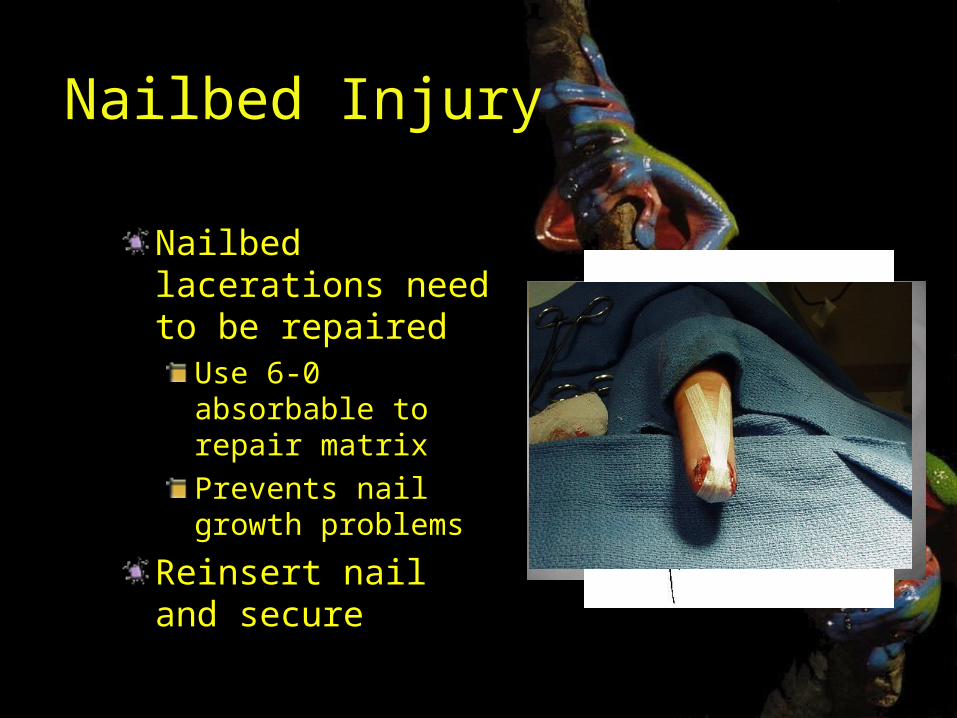
Nailbed lacerations need to be repaired
Use 6-0 absorbable to repair matrixPrevents nail growth problems
Reinsert nail and secure
Subungual Hematoma
Results from blunt trauma to nailVery painfulRelieved by
CauteryHeated paperclip18g needle
Subungual Hematoma
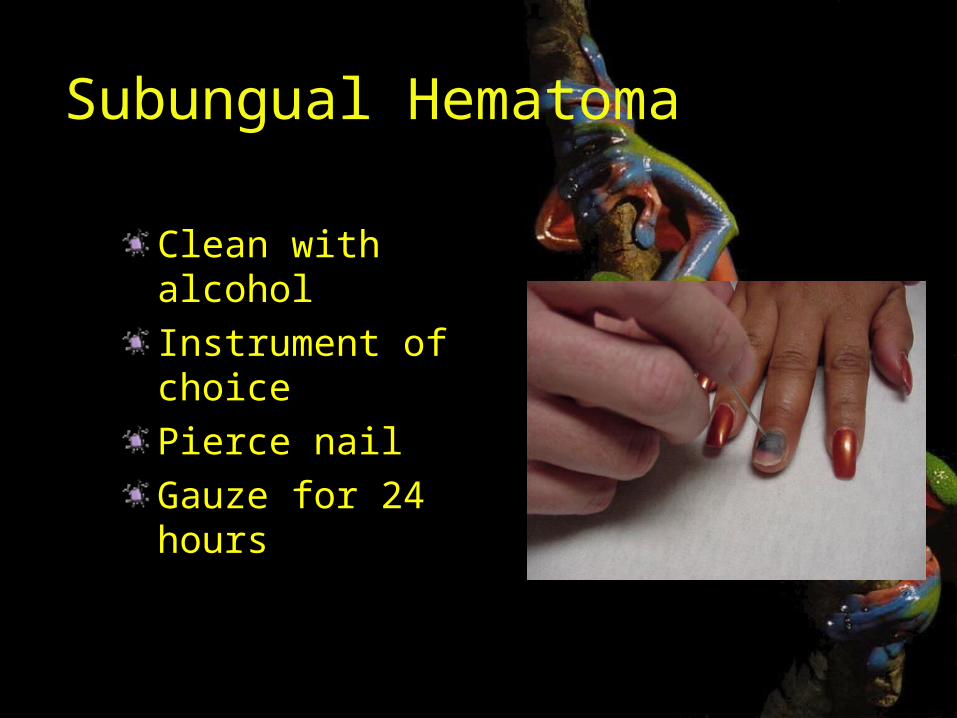
Clean with alcoholInstrument of choicePierce nailGauze for 24 hours
Mallet Fingers(soft tissue and bony)
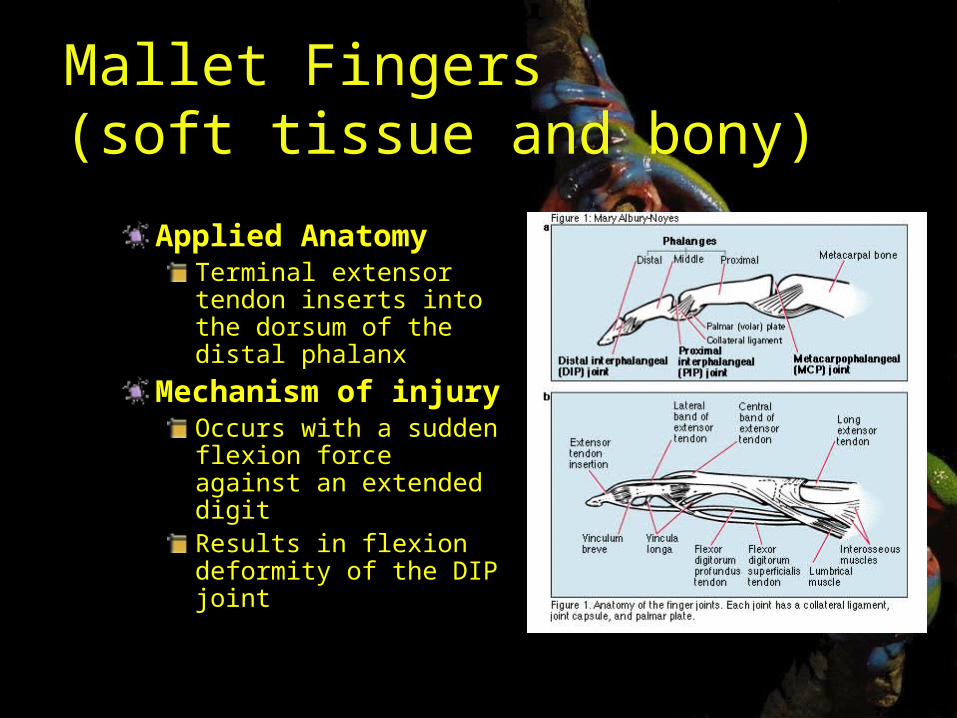
Applied AnatomyTerminal extensor tendon inserts into the dorsum of the distal phalanx
Mechanism of injury
Occurs with a sudden flexion force against an extended digitResults in flexion deformity of the DIP joint
Mallet Fingers(soft tissue and bony)
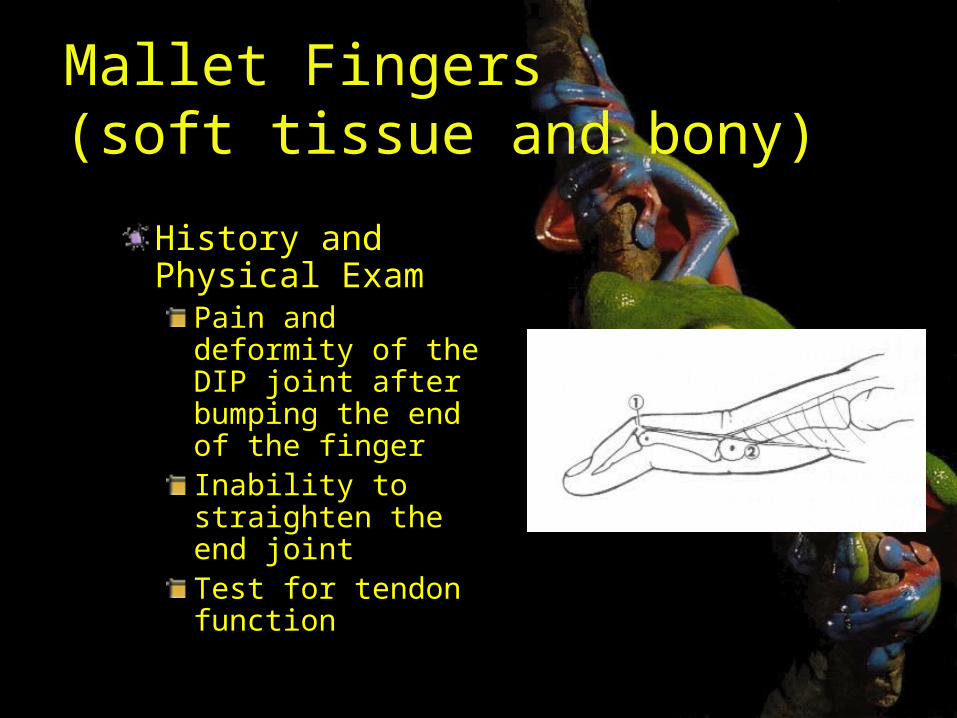
History and Physical Exam
Pain and deformity of the DIP joint after bumping the end of the fingerInability to straighten the end jointTest for tendon function
Mallet Fingers(soft tissue and bony)
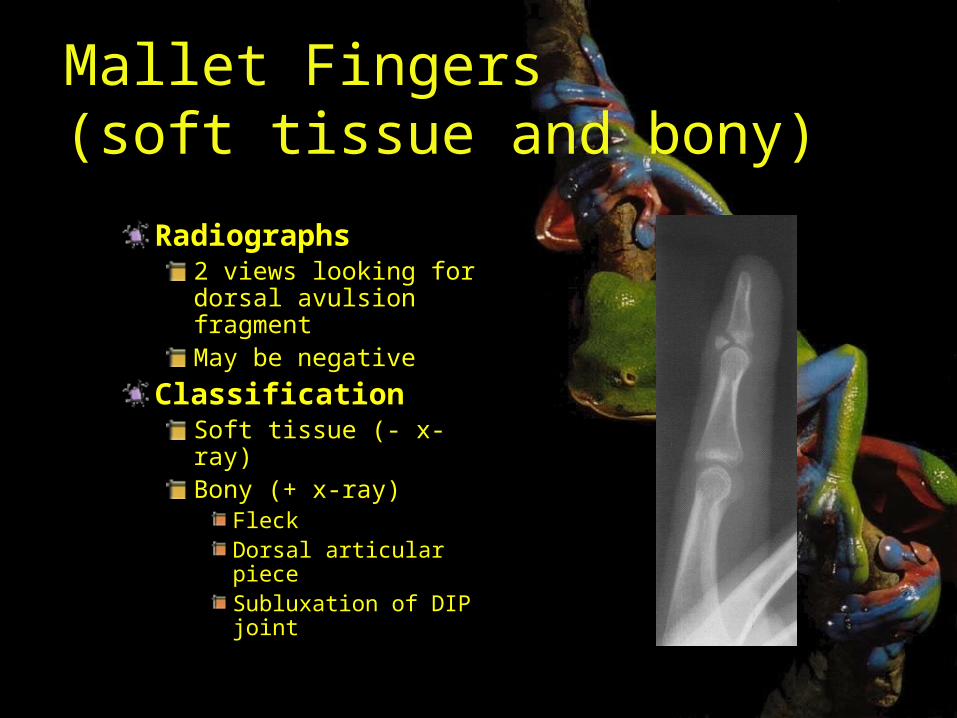
Radiographs2 views looking for dorsal avulsion fragmentMay be negative
ClassificationSoft tissue (- x-ray)Bony (+ x-ray)
FleckDorsal articular pieceSubluxation of DIP joint
Mallet Fingers(soft tissue and bony)
TreatmentClosed reductionContinuously splint DIP in full extension for 6 to 10 weeks
Only immobilize the DIP
Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
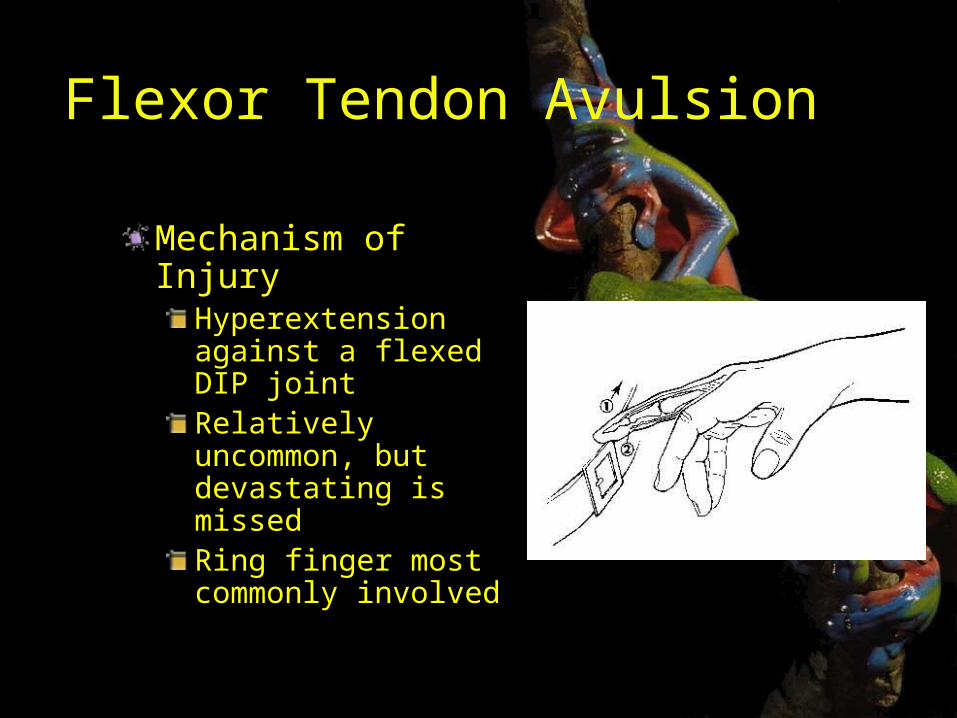
Flexor Tendon Avulsion
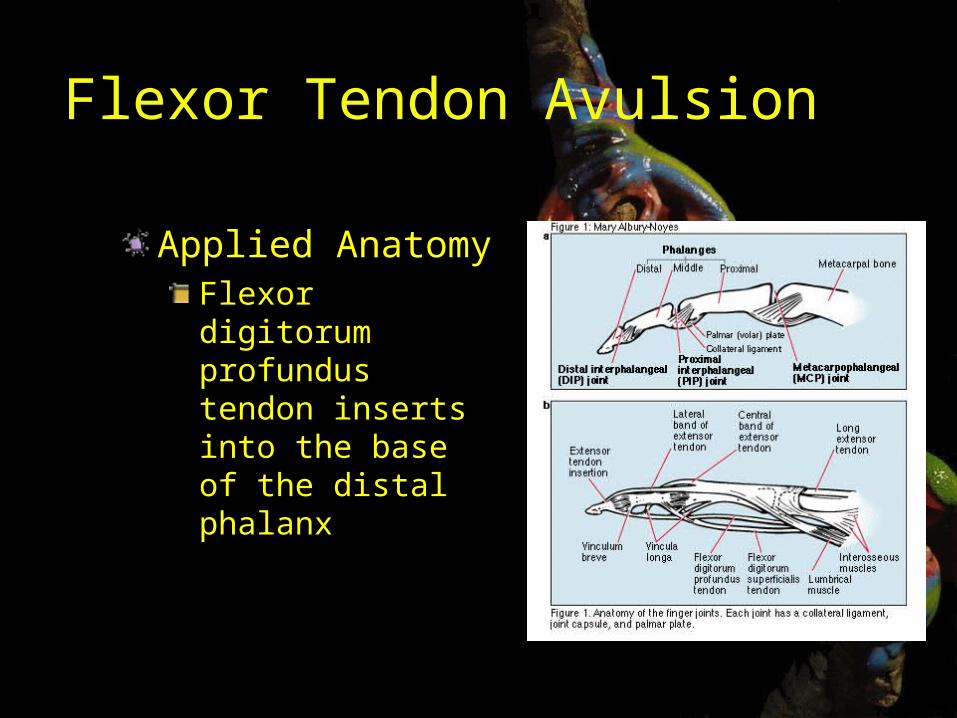
Applied AnatomyFlexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion
Mechanism of Injury
Hyperextension against a flexed DIP jointRelatively uncommon, but devastating is missedRing finger most commonly involved
Flexor Tendon Avulsion
Associated injuriesNone
History and Physical ExamPain on volar surface of digit
May extend into palm with eccymosis
Cannot flex tipResting hand has extension of DIP jointNo active flexion
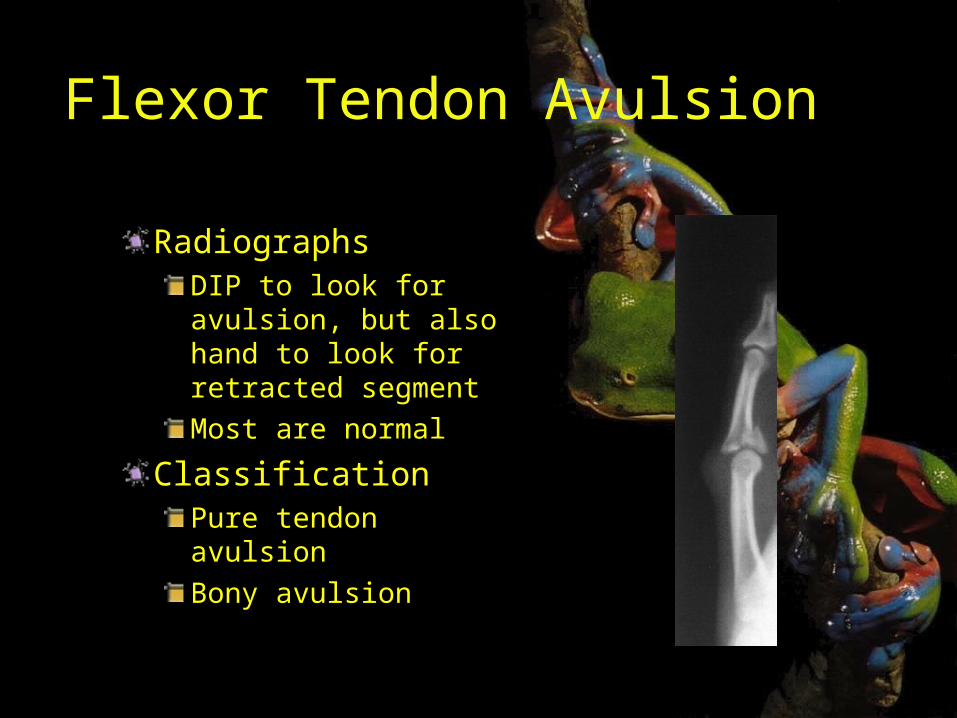
Flexor Tendon Avulsion
RadiographsDIP to look for avulsion, but also hand to look for retracted segmentMost are normal
ClassificationPure tendon avulsionBony avulsion
Flexor Tendon Avulsion
TreatmentShould be splinted and referred in a semi-urgent fashionSurgery is required
OutcomesResults correlate with delay in treatment
Early do wellPostoperative hand therapy is important
Middle and Proximal Phalangeal Fractures
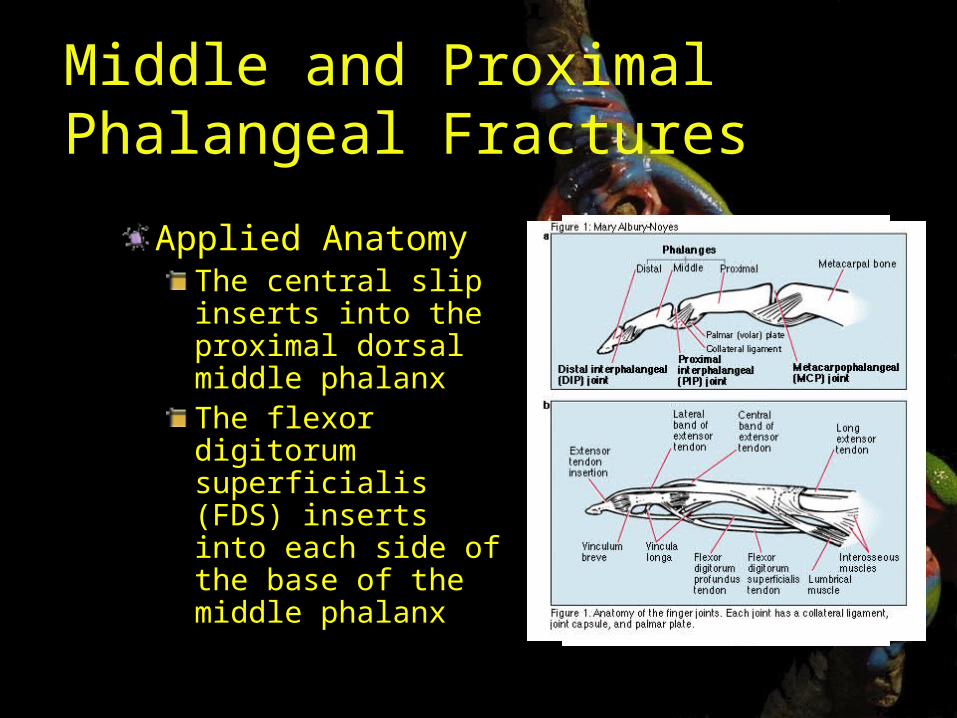
Applied AnatomyThe central slip inserts into the proximal dorsal middle phalanxThe flexor digitorum superficialis (FDS) inserts into each side of the base of the middle phalanx
Middle and Proximal Phalangeal Fractures
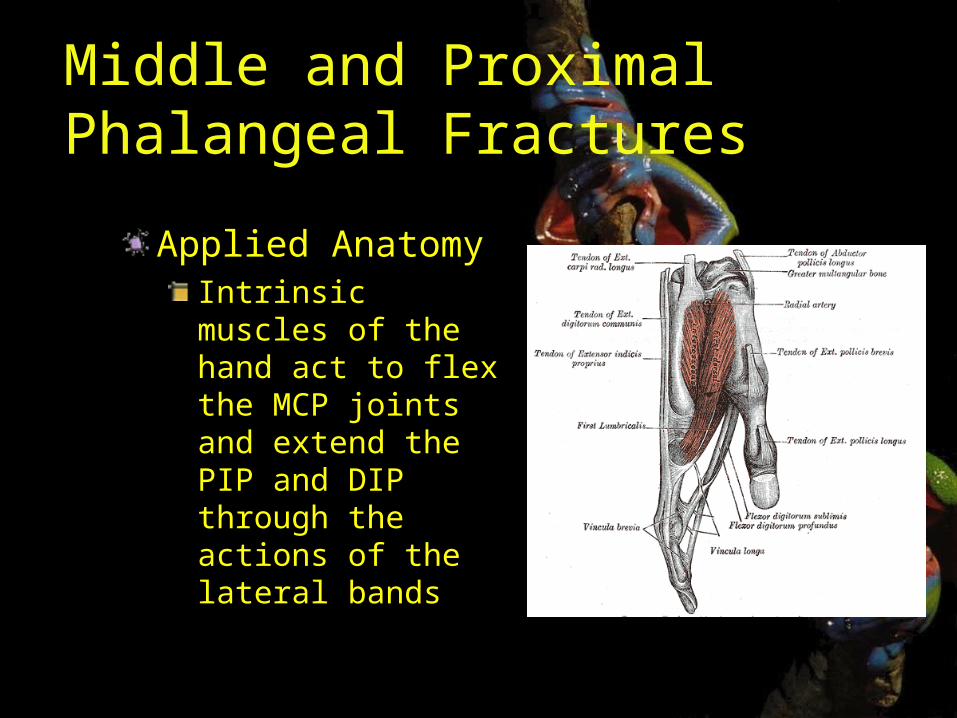
Applied AnatomyIntrinsic muscles of the hand act to flex the MCP joints and extend the PIP and DIP through the actions of the lateral bands
Middle and Proximal Phalangeal Fractures
Mechanism of Injury
Direct blow to the digit or a twisting injury
Associated InjuriesOpen injuriesLacerations to tendons or neurovascular bundlesImportant to evaluate for DIP injuries
History and Physical Exam
Evaluate for malrotation
Subtle fractures on x-ray can have significant malrotation when flexed
Middle and Proximal Phalangeal Fractures
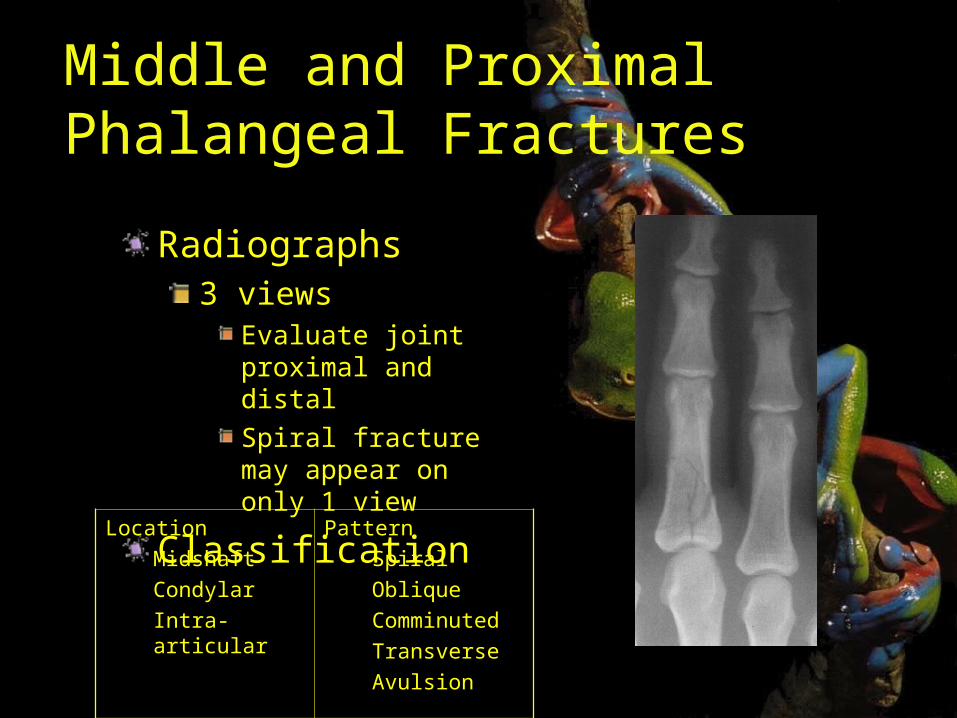
Radiographs3 views
Evaluate joint proximal and distalSpiral fracture may appear on only 1 view
ClassificationLocationMidshaftCondylarIntra-articular
PatternSpiralObliqueComminutedTransverseAvulsion
Middle and Proximal Phalangeal Fractures
TreatmentMost can be treated non-surgically
Protect range of motionBuddy tape
What to referDisplaced, malrotated, joint involvementComminuted, spiral, and oblique are unstable
Stable nondisplacedSplint 8-10 days followed by buddy tapeFollow-up x-ray 8-10 days to ensure no displacement
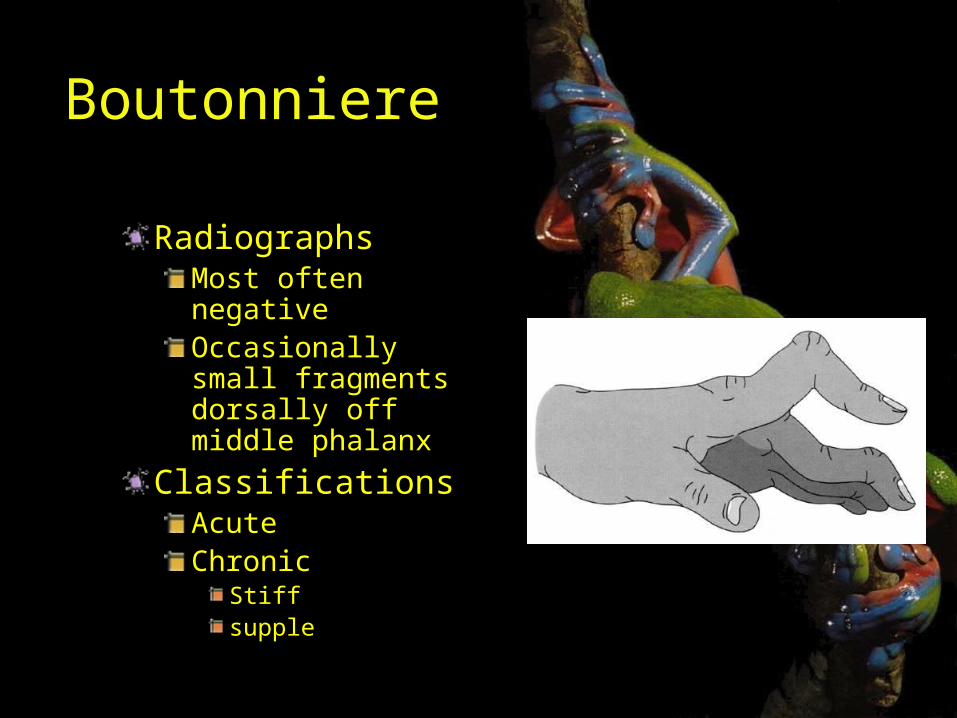
Boutonniere
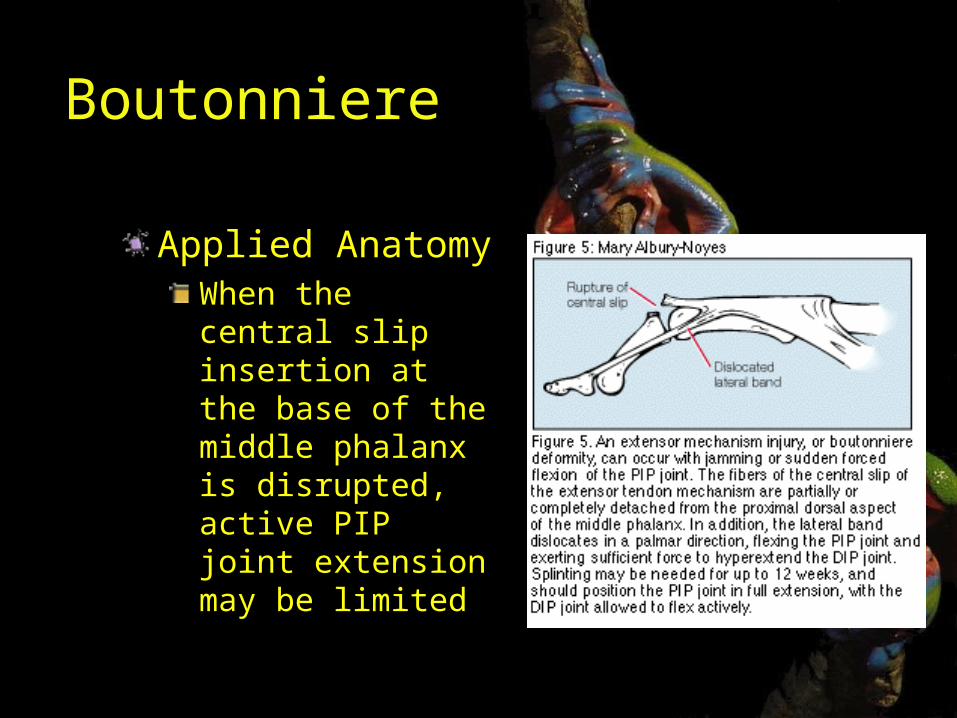
Applied AnatomyWhen the central slip insertion at the base of the middle phalanx is disrupted, active PIP joint extension may be limited
Boutonniere
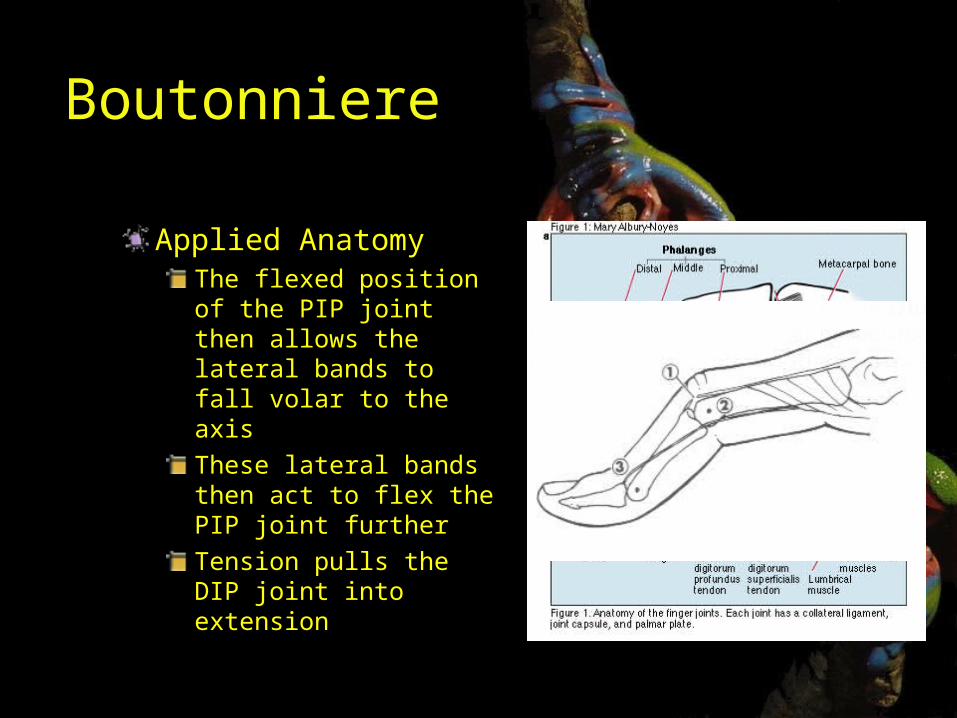
Applied AnatomyThe flexed position of the PIP joint then allows the lateral bands to fall volar to the axis These lateral bands then act to flex the PIP joint furtherTension pulls the DIP joint into extension
Boutonniere
Mechanism of InjuryAcute flexion force to PIP jointPIP does not immediately fall into a flexed positionSeveral weeks after the injury the digit assumes a buttonhole posture.Other mechanism include PIP dislocation and central slip lacerations
History and Physical Exam
Pain and swelling about PIPInability to fully extend PIPDIP flexion is limitedLongstanding cases
PIP flexionPassive extension not possible
Boutonniere
RadiographsMost often negativeOccasionally small fragments dorsally off middle phalanx
ClassificationsAcuteChronic
Stiffsupple
Boutonniere
TreatmentIf not sure of central slip, assume it is and splint the PIP in full extensionAcute boutonnieres
4 weeks of full extension splinting of PIP with active DIP flexion exercisesOccasionally need surgery
Chronic boutonnieresHand therapyPossible surgery
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
Most common orthopedic hand injury that can result in long-term digital stiffness and impairment
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
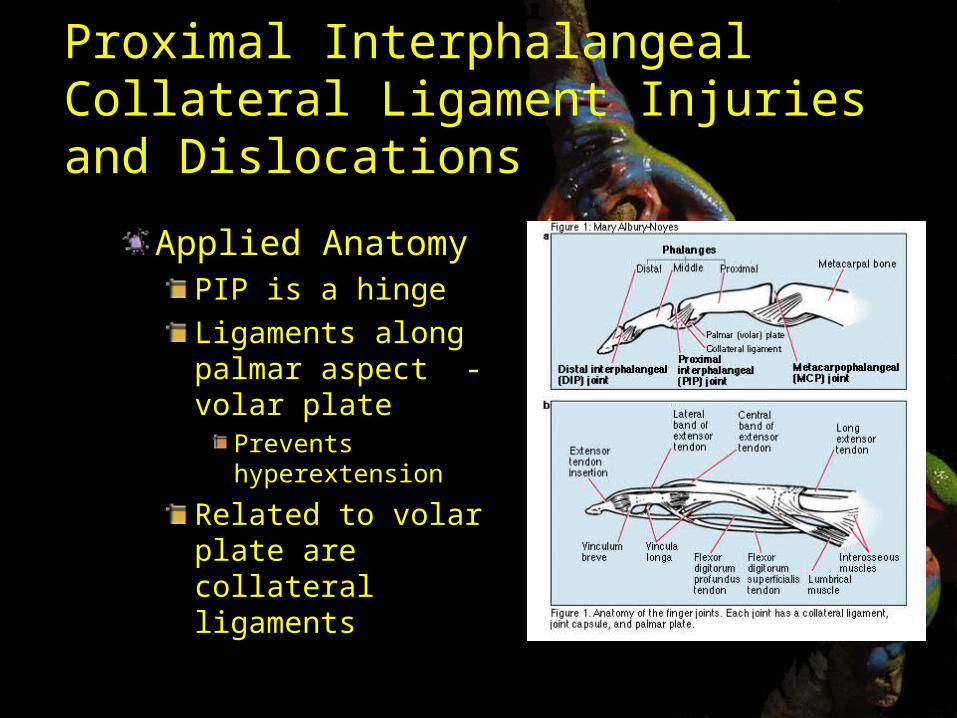
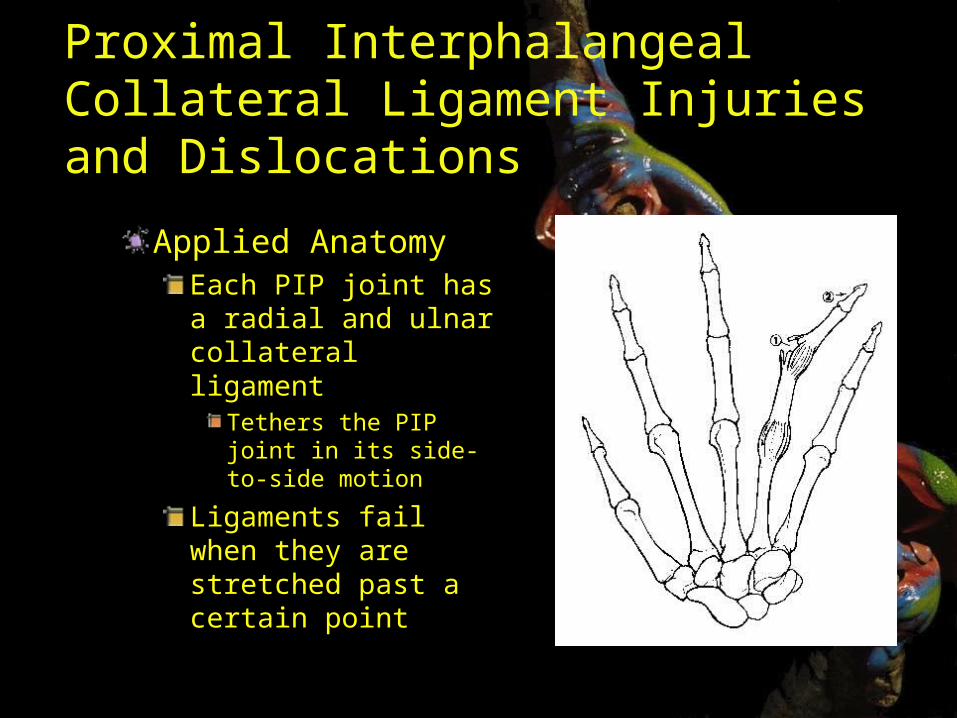
Applied AnatomyPIP is a hingeLigaments along palmar aspect - volar plate
Prevents hyperextension
Related to volar plate are collateral ligaments
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
Applied AnatomyEach PIP joint has a radial and ulnar collateral ligament
Tethers the PIP joint in its side-to-side motion
Ligaments fail when they are stretched past a certain point
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
Mechanism of Injury
Sudden force directed to tip of digit results in hyperextension
Spectrum ranging from slight hyperextension grade I sprain to frank dislocation
Associated InjuryIf the skin tears open, it is an open dislocation
History and Physical Exam
Joint swollen and tenderTest collateral ligaments to ascertain partial vs complete
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
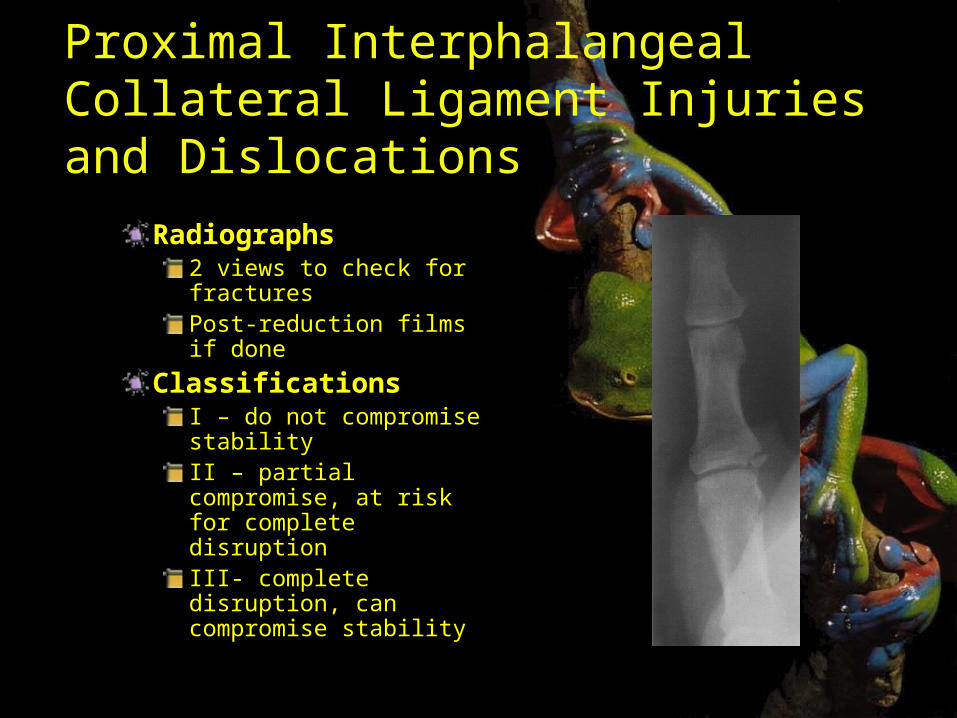
Radiographs2 views to check for fracturesPost-reduction films if done
ClassificationsI – do not compromise stabilityII – partial compromise, at risk for complete disruptionIII- complete disruption, can compromise stability
Proximal Interphalangeal Collateral Ligament Injuries and Dislocations
TreatmentEarly mobilization after a few days of splinting
Buddy tape for 4 weeks
A rare volar PIP joint dislocation requires 3-4 weeks of splinting in extension
OutcomesThese injuries can heal with some permanent fusiform swelling from scar tissue.Long term problem is not recurrent instability, but stiffness
For this reason, early range of motion program is most often recommended
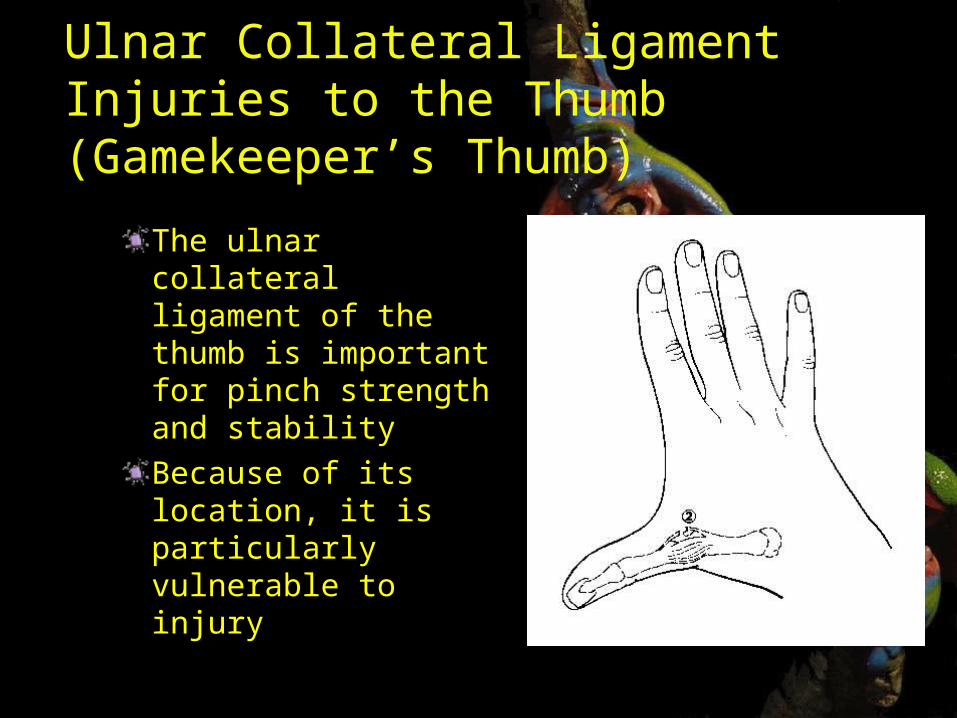
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeper’s Thumb)
The ulnar collateral ligament of the thumb is important for pinch strength and stabilityBecause of its location, it is particularly vulnerable to injury
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeper’s Thumb)
Mechanism of Injury
Combination of hyperextension and a radially directed force at the thumb MP joint (fall with a pole in the hand while skiing)
History and Physical Exam
Moderate swelling and eccymosis over ulnar side of MP jointIn complete tears stress testing of UCL shows a poor endpoint
Ulnar Collateral Ligament Injuries to the Thumb (Gamekeeper’s Thumb)
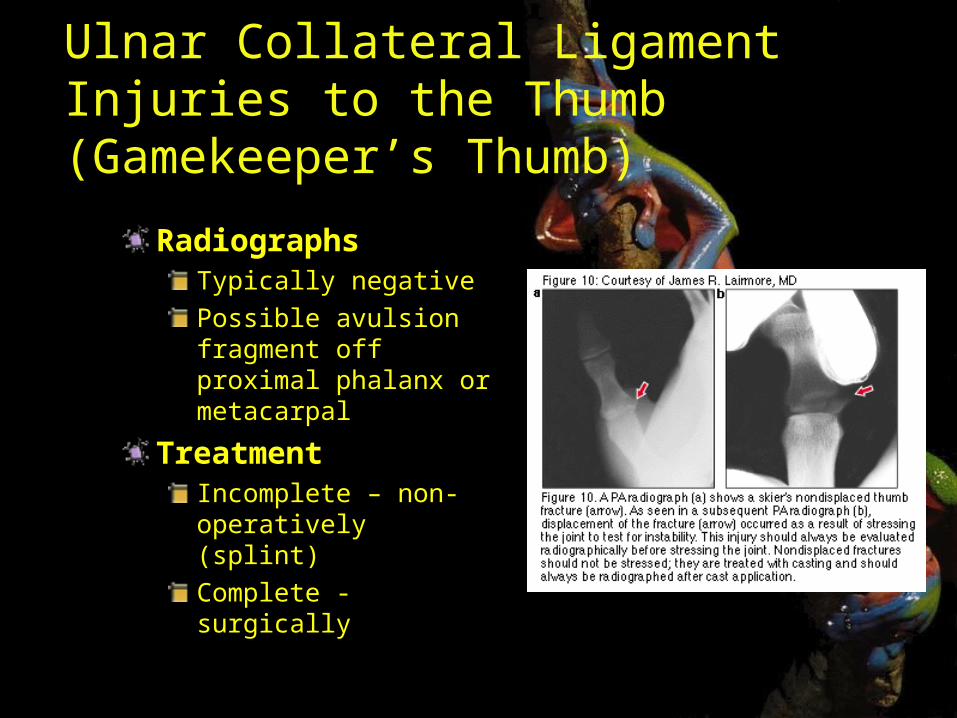
RadiographsTypically negativePossible avulsion fragment off proximal phalanx or metacarpal
TreatmentIncomplete – non-operatively (splint)Complete - surgically
Bennett's Fracture Dislocation
Most frequent of all thumb fractureDescribed in 1882 by Dr. Edward BennetIt is a fracture dislocation, intra-articular fracture at base of carpometacarpal (CMC) joint of the thumb
Bennett's Fracture Dislocation
Mechanism of Injury
Results from axial blow directed against the partially flexed metacarpal; (ie. from fist fights)
History and Physical Exam
Moderate swelling and eccymosis over the CMC jointPain with ROM or palpation
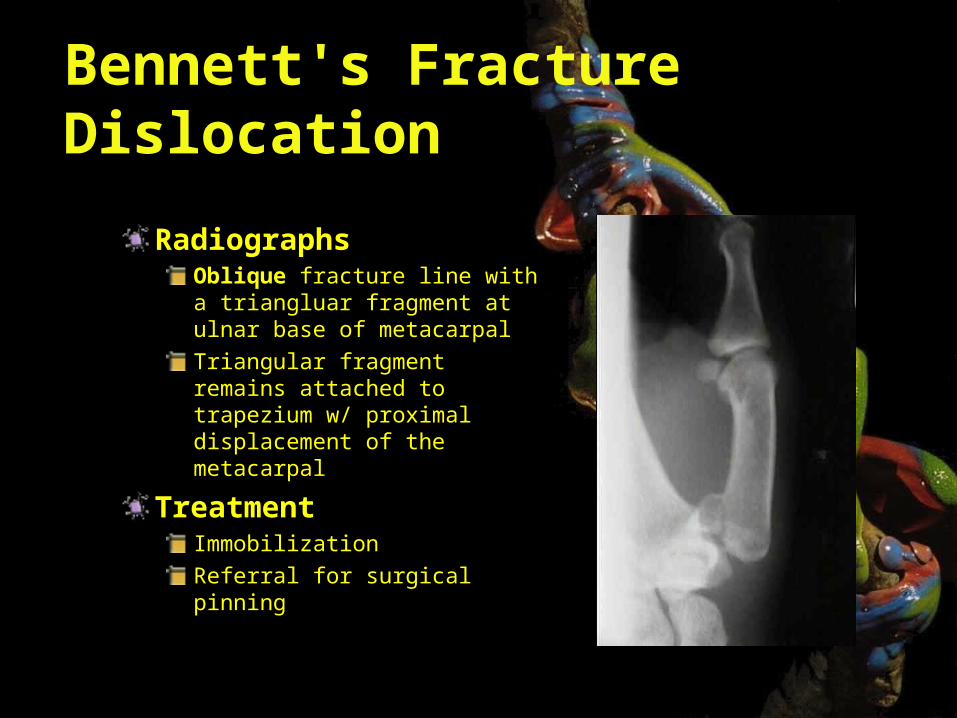
Bennett's Fracture Dislocation
RadiographsOblique fracture line with a triangluar fragment at ulnar base of metacarpalTriangular fragment remains attached to trapezium w/ proximal displacement of the metacarpal
TreatmentImmobilizationReferral for surgical pinning
Infections of the Hand
Conditions That Mimic Infection
GoutPyogenic granulomaAcute calcificationForeign body reactionHerpetic whitlowMetastatic lesions
PseudogoutRheumatoid arthritisGranuloma annulareLocal reactions
Paronychia
Infection localized to the proximal and lateral skin folds of fingers and toes
Staph aureus Group A or D StrepPseudomonasGram-negative bacteriaanerobes
Paronychia
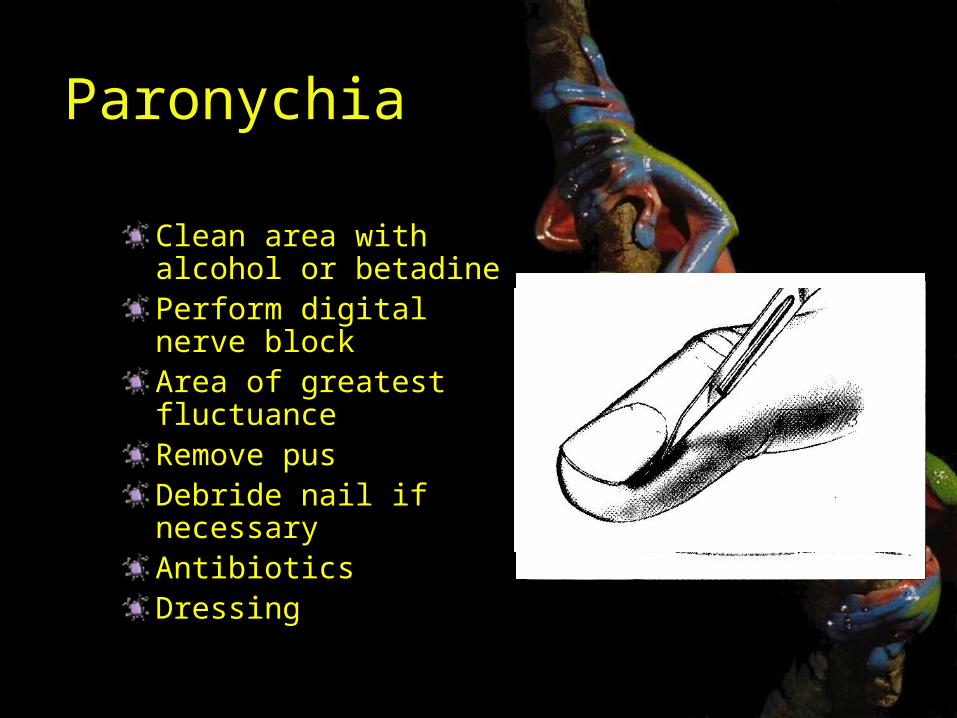
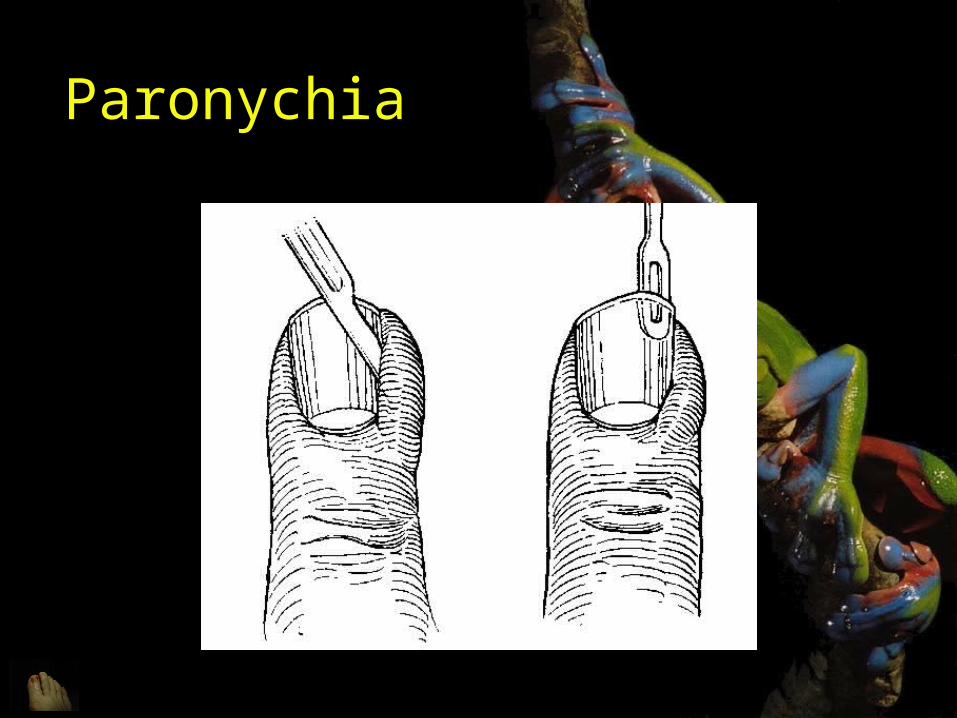
Clean area with alcohol or betadinePerform digital nerve blockArea of greatest fluctuanceRemove pusDebride nail if necessaryAntibioticsDressing
Paronychia
Felon
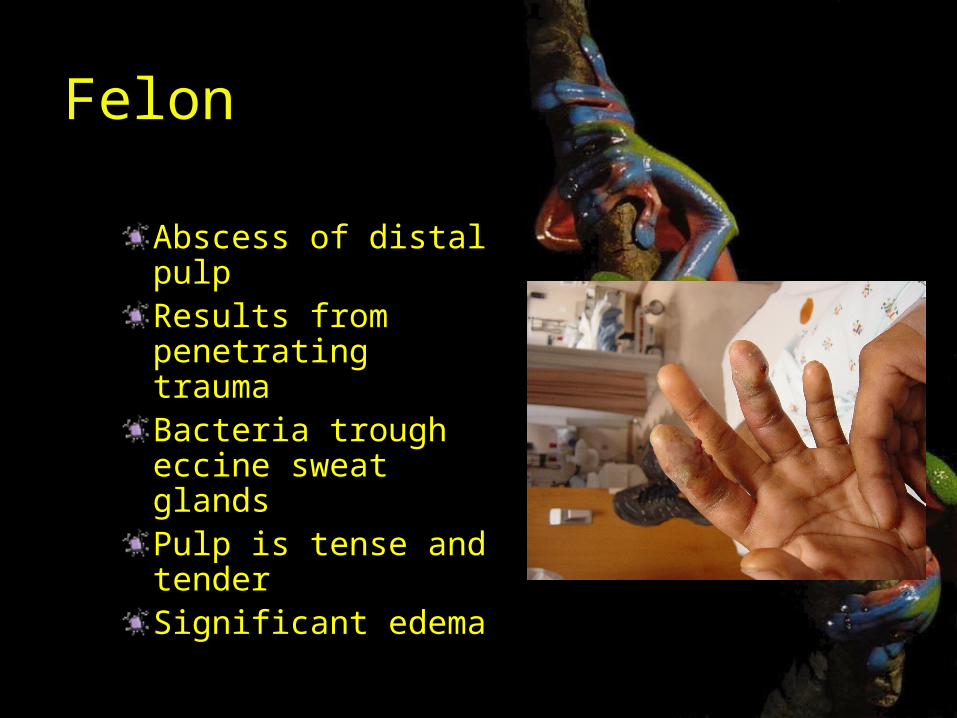
Abscess of distal pulpResults from penetrating traumaBacteria trough eccine sweat glandsPulp is tense and tenderSignificant edema
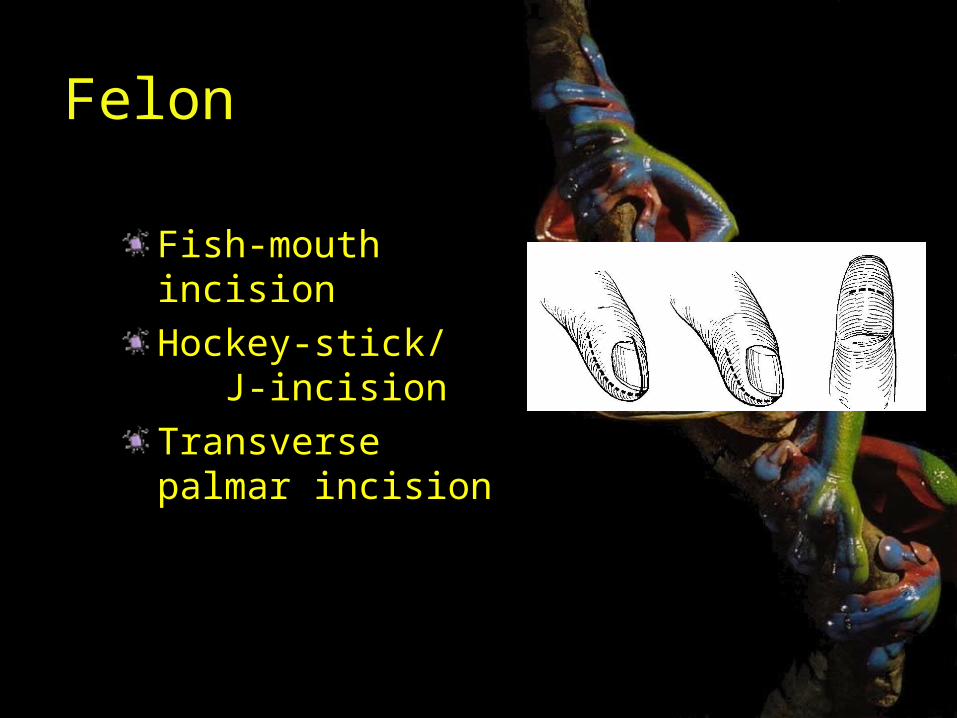
Felon
Fish-mouth incisionHockey-stick/ J-incisionTransverse palmar incision

Questions?