Embed Size (px)
Citation preview

R
C
Tr
JFa
b
c
d
a
ARRAA
KACC
1
tlfs
H
h0
ARTICLE IN PRESSG ModelESUS-5901; No. of Pages 7
Resuscitation xxx (2014) xxx–xxx
Contents lists available at ScienceDirect
Resuscitation
j ourna l h o me pa g e : www.elsev ier .com/ locate / resusc i ta t ion
linical Paper
he impact of airway management on quality of cardiopulmonaryesuscitation: An observational study in patients during cardiac arrest
oyce Yeunga,b, Mehboob Chilwana,c, Richard Fieldd, Robin Daviesa,ang Gaoa,b, Gavin D. Perkinsa,c,∗
Heart of England NHS Foundation Trust, Birmingham Heartlands Hospital, Birmingham B9 5SS, United KingdomUniversity of Birmingham, School of Clinical and Experimental Medicine, Birmingham B15 2TT, United KingdomUniversity of Warwick, Warwick Medical School, Coventry CV4 7AL, United KingdomUniversity of Southampton, Faculty of Medicine, SO16 6YD, United Kingdom
r t i c l e i n f o
rticle history:eceived 4 September 2013eceived in revised form 7 February 2014ccepted 24 February 2014vailable online xxx
eywords:irway managementardiac arrestardiopulmonary resuscitation
a b s t r a c t
Background: Minimising interruptions in chest compressions is associated with improved survival fromcardiac arrest. Current in-hospital guidelines recommend continuous chest compressions after the airwayis secured on the premise that this will reduce no flow time. The aim of this study was to determine theeffect of advanced airway use on the no flow ratio and other measures of CPR quality.Methods: Consecutive adult patients who sustained an in-hospital cardiac arrest were enrolled in thisprospective observational study. The quality of CPR was measured using the Q-CPR device (Phillips, UK)before and after an advanced airway device (endotracheal tube [ET] or laryngeal mask airway [LMA])was inserted. Patients receiving only bag-mask ventilation were used as the control cohort. The primaryoutcome was no flow ratio (NFR). Secondary outcomes were chest compression rate, depth, compressionstoo shallow, compressions with leaning, ventilation rate, inflation time, change in impedance and timerequired to successfully insert airway device.Results: One hundred patients were enrolled in the study (2008–2011). Endotracheal tube and LMA place-ment took similar durations (median 15.8 s (IQR 6.8–19.4) vs LMA median 8.0 s (IQR 5.5–15.9), p = 0.1). Theuse of an advanced airway was associated with improved no flow ratios (endotracheal tube placement(n = 50) improved NFR from baseline median 0.24 IQR 0.17–0.40) to 0.15 to (IQR 0.09–0.28), p = 0.012;LMA (n = 25) from median 0.28 (IQR 0.23–0.40) to 0.13 (IQR 0.11– 0.19), p = 0.0001). There was no changein NFR in patients managed solely with bag valve mask (BVM) (n = 25) (median 0.29 (IQR 0.18–0.59) vs
median 0.26 (IQR 0.12–0.37), p = 0.888). There was no significant difference in time taken to successfullyinsert the airway device between the two groups.Conclusion: The use of an advanced airway (ETT or LMA) during in-hospital cardiac arrest was associatedwith improved no flow ratio. Further studies are required to determine the effect of airway devices onoverall patient outcomes.© 2014 Elsevier Ireland Ltd. All rights reserved.
. Introduction
Good quality CPR is paramount to patient survival.1,2 Observa-ional studies have shown that the quality of CPR is poor in realife.3,4 Interruptions in chest compressions decrease coronary per-
Please cite this article in press as: Yeung J, et al. The impact of airwaobservational study in patients during cardiac arrest. Resuscitation (2
usion pressure5 and are associated with decreased defibrillationuccess and poor outcome.4,6–9
∗ Corresponding author at: Heart of England NHS Foundation Trust, Birminghameartlands Hospital, Birmingham B9 5SS, United Kingdom.
E-mail address: [email protected] (G.D. Perkins).
ttp://dx.doi.org/10.1016/j.resuscitation.2014.02.018300-9572/© 2014 Elsevier Ireland Ltd. All rights reserved.
Although endotracheal intubation allows continuous chestcompressions,10 prolonged interruptions associated with intuba-tion may negate this benefit. Wang et al. observed a median timeto intubation of 46.5 s (IQR 23.5, 73) and substantial pauses in com-pressions 109.5 s (IQR 54–198). Overall intubation contributed to22.8% of all CPR interruptions in their study.11,12 The same studydemonstrated how serious complications could result from endo-tracheal intubation by inexperienced healthcare professionals withintubation errors found in 22.7% episodes. Of these, 3% had mis-
y management on quality of cardiopulmonary resuscitation: An014), http://dx.doi.org/10.1016/j.resuscitation.2014.02.018
placed or dislodged endotracheal tubes, 3% had multiple attemptsand 15% had failed intubations.
In the pre-hospital setting, questions remain whether advancedairway management improves patient survival with at times

ING ModelR
2 itatio
ca6witmoaat1ar
uStTdTfe
2
2
Cnc&T
2
aiaae
2bhratte
2
F(i
2
dt
ARTICLEESUS-5901; No. of Pages 7
J. Yeung et al. / Resusc
ontrasting results reported by studies in both adult and paedi-tric cardiac arrests.13–16 A nationwide registry study in Japan of49,359 patients found no survival benefit from any advanced air-ay management compared with bag valve mask ventilation.17 The
mplementation of minimally interrupted/cardio-cerebral resusci-ation protocols in this setting has led to improved survival.18 The
ulti-centre Resuscitation Outcome Consortium (ROC) in the USbserved higher survival in patients who did not receive advancedirway management. However in those patients who receiveddvanced airway management, endotracheal intubation was betterhan using a supraglottic airway device (adjusted OR 1.40; 95% CI:.04, 1.89).19 To date, there is a lack of research to elucidate howirway management may impact on quality of cardiopulmonaryesuscitation.
Current resuscitation guidelines recommend intubation to bendertaken only by those trained in advanced airway management.upraglottic airway devices have been advocated as an alternativeo endotracheal tube and are now part of resuscitation guidelines.20
heir ease of insertion without interrupting CPR makes supraglotticevices such as laryngeal mask airway (LMA) an attractive option.21
o date, most research on airway management in cardiac arrest hasocused on quality of CPR in manikins. This study aims to assess theffect of airway device on quality of CPR in adult cardiac arrests.
. Methods
.1. Approvals
The study was approved by Birmingham and Black Country andoventry Research and Ethics Committees. Given the observationalature of the study, the committees declared that individual patientonsent was not required. The study was approved by Research
Development Department of Heart of England NHS Foundationrust.
.2. Setting
The study was conducted at Birmingham Heartlands hospital, large teaching hospital with approximately 800 in-patient bedsn Birmingham, United Kingdom. The Emergency Department seespproximately 100,000 new patients each year. The hospital man-ges approximately 350 in-hospital and 240 out-of-hospital arrestsach year.
Consecutive cardiac arrests which took place from November008 to May 2011 were included in the study. Episodes were eligi-le for this study if airway device was inserted by a member of theospital cardiac arrest team. All cardiac arrest team members haveeceived training in the insertion of laryngeal mask airway (LMA)nd are authorised to use them during cardiac arrest. It is the hospi-al policy that cardiac arrest team member must use a LMA unlesshey have been specifically trained and assessed as competent inndotracheal intubation.
.3. Airway management and devices
Available airway adjuncts and devices in Heart of England NHSoundation Trust were all disposable and included bag valve maskMarshall Products, UK), endotracheal tubes (Portex®, Smith Med-cal, UK) and laryngeal mask airways (Marshall Products, UK).
.4. Study design
Please cite this article in press as: Yeung J, et al. The impact of airwaobservational study in patients during cardiac arrest. Resuscitation (2
This was a prospective observational study. Cardiac arrests wereefined as loss of pulse that required chest compressions. Consecu-ive adult patients requiring cardiopulmonary resuscitation from in
PRESSn xxx (2014) xxx–xxx
and out-of-hospital cardiac arrests were eligible for inclusion. Vic-tims of traumatic cardiac arrest and those aged less than 18 yearswere excluded. Only data from the first arrest was collected if apatient suffered multiple arrests in order to avoid confounding fac-tors. Episodes were also excluded if there was no quality of CPR datarecorded or if the type of airway device used was not recorded.
2.5. Data collection
Background data about patients who suffered cardiac arrestsincluded age, gender, location of arrests, presenting rhythm wascollected from patient notes. Clinical data about the time of inser-tion of airway, any disruption to chest compressions, and the typeof airway device used was collected by direct observation at cardiacarrests.
Quality of CPR data were collected from Heartstart MRx with Q-CPR (Philips Medical System) Management and Feedback Tool andanalysed using QCPR Review software (Version 2.1.0, Laerdal Med-ical). The system consists of a small reusable compression sensorand a set of standard multifunction defibrillation electrode padsattached to a defibrillator. The Q-CPR compression sensor meas-ures compression force and acceleration from which compressiondepth, proportion of compressions with depth <38 mm, proportionof compressions with leaning, compression rate and no flow ratio(proportion of resuscitation attempt when compressions are notbeing performed) are recorded.22,23 Thus a lower no flow ratiois associated with less interruptions in CPR and represents bet-ter quality CPR than a high no flow ratio. The multifunction padsmeasure chest impedance from which ventilation rate, averageinflation time and average impedance change during inflation arecalculated.24
The time of airway insertion was determined for each individualepisode from the use of a stop watch during direct observations by amember of the research team, documentation from medical recordsand verified on the QCPR Review software. Time to insertion of air-way was calculated manually from episodes and measured as thetime from the beginning of episode until first recorded ventilationafter successful insertion of airway. The time taken to insert the air-way was recorded from by direct observations by a member of theresearch team and measured the time taken from starting to insertthe airway until airway was secured and confirmed as effective.
2.6. Statistical analysis
The primary outcome was no flow ratio. Based on data from aprevious in-hospital CPR study,25 (no flow ratio standard deviation0.13) we calculated that we would require 20 patients in each armto detect a 0.1 difference in no flow ratio with 90% power. To allowfor potential problems with data capture, we set out to recruit atleast 25 patients into each arm of the study.
Quality of CPR data were analysed for the whole episode beforeand after airway insertion to investigate the impact of airwaydevice. Data were assessed for normality using Sharpiro–Wilk test.For before and after effects, normally distributed data were com-pared by paired t-tests, non-parametric data were analysed bypaired Mann–Whitney U-test. To compare airway groups, datawere analysed using ANOVA with Bonferroni correction. Betweensubject factor was type of airway used and within subject factorwas episode. A p value of <0.05 was considered signficant for alltests.
3. Results
y management on quality of cardiopulmonary resuscitation: An014), http://dx.doi.org/10.1016/j.resuscitation.2014.02.018
During the study period, the majority of out of hospital cardiacarrests had airway device inserted prior to arriving into the hospital,leaving 33 (28.7%) episodes that fulfilled study criteria. During the

ARTICLE IN PRESSG ModelRESUS-5901; No. of Pages 7
J. Yeung et al. / Resuscitation xxx (2014) xxx–xxx 3
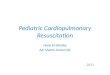
Number of cardiac arrests = 307
OHCA, n=194 IHCA, n=113
Documented airway device, n=33
QCPR data, n=115
Excluded: no documented airway, n=14
Excluded: QCPR not used, n=32
Documented airway device, n=67
QCPR data, n=81
Excluded: QCPR not used, n=79
Excluded: airway inserted prior to arrival in hospital, n=82
Included in study, n=67
Included in study, n=33
is out
ssec
mvsptr
3a
aLt
w
TC
Fig. 1. Diagram of cardiac arrests included in the study (OHCA
ame time period, 67 (82.7%) of in hospital cardiac arrests fulfilledtudy criteria and were included in the study (Fig. 1). A total of 100pisodes were included providing 1108 min of CPR data and 79,283hest compressions for analyses.
Endotracheal tube (ETT) was inserted in 50 episodes, laryngealask airway (LMA) was used in 25 episodes and bag valve mask
entilation was used (BVM) in the 25 episodes. There were noignificant differences in age, gender, presenting rhythm betweenatients in all three airway groups (Table 1). There were also no sta-istically significant differences in ROSC and survival to dischargeates.
.1. Quality of chest compressions before and after insertion ofirway device
All episodes in the study achieved continuous compressionsnd asynchronous ventilations after insertion of either ETT or
Please cite this article in press as: Yeung J, et al. The impact of airwaobservational study in patients during cardiac arrest. Resuscitation (2
MA. Compressions to ventilations ratio of 30:2 were maintainedhroughout episodes in BVM groups.
To differentiate temporal differences in CPR quality over time,e included a ‘before and after insertion’ effects for BVM group.
able 1haracteristics of three airway groups. Data given as number (%) except for mean age ± S
ETT (n = 50) LM
OHCA 18 (36)
Mean age ± SD 71.7 ± 13.3
Male 31 (62%) 16Shockable rhythm 8 (16%) 3ROSC 24 (48%) 6Survival to discharge 6 (12%)
of hospital cardiac arrests, IHCA is in hospital cardiac arrests).
The median time of insertion of both ETT and LMA (140 s) was usedas the cut point for before and after insertion in BVM group.
Comparing before and after insertion of an airway device, bothETT and LMA led to significant reduction in NFR (ETT p = 0.012, LMAp = 0.0001) (Table 2). There was no significant changes in NFR BVMgroup (p = 0.888). The insertion of airway did not affect other qualityof chest compression parameters.
3.2. Ventilation before and after insertion of device
There were 14 episodes (3 in ETT group, 2 in LMA group, 9 inBVM group) where no change in impedance tracing attributed toventilations could be found. It was unclear whether this was dueto misplacement of airway device leading to inability to achieveeffective ventilation or overall poor quality of impedance recording.These episodes were therefore excluded in further analyses.
Average inflation time was calculated as average time betweenstart and top of ventilation and was measured in seconds. In BVM
y management on quality of cardiopulmonary resuscitation: An014), http://dx.doi.org/10.1016/j.resuscitation.2014.02.018
group, the average inflation time increased in time from 0.81 s to0.92 s suggesting that time needed to inflate the chest increasedwith the duration of arrest but this was not found to be statisticallysignificant (p = 0.076) (Table 3). There were also non-significant
D.
A (n = 25) BVM (n = 25) p value
4 (16) 11 (44) 0.75172.4 ± 11.2 73.1 ± 15.3 0.802
(64%) 19 (76%) 0.488 (12%) 2 (8%) 0.121 (25%) 8 (32%) 0.0791 (4%) 2 (8%) 0.514

Please cite this article in press as: Yeung J, et al. The impact of airwaobservational study in patients during cardiac arrest. Resuscitation (2
ARTICLE ING ModelRESUS-5901; No. of Pages 7
4 J. Yeung et al. / Resuscitatio
Tab
le
2Q
ual
ity
of
CPR
befo
re
and
afte
r
inse
rtio
n
of
airw
ay
dev
ice.
Dat
a
give
n
as
mea
n
±
SD, e
xcep
t
for
pro
por
tion
s
wh
ich
are
give
n
as
med
ian
(IQ
R).
Qu
alit
y
par
amet
er
ETT
(n
=
50)
LMA
(n
=
25)
BV
M
(n
=
25)
Bef
ore
Aft
er
p
valu
e
Bef
ore
Aft
er
p
valu
e
Bef
ore
Aft
er
p
valu
e
No
flow
rati
o
0.24
(0.1
7,
0.40
)
0.15
(0.0
9,
0.28
)
0.01
2*0.
28
(0.2
3,
0.40
)
0.13
(0.1
1,
0.19
)
0.00
01*
0.29
(0.1
8,
0.59
)
0.26
(0.1
2,
0.37
)
0.88
8C
onti
nu
ous
com
pre
ssio
ns,
n
(%)
0
(0%
)
50
(100
%)
0
(0%
)
25
(100
%)
0
(0%
)
0
(0%
)C
omp
ress
ion
dep
th
(mm
)
44.3
9
±
13.3
44.4
2
±
13.1
0.97
8
44.2
4
±
13.7
45.5
2
±
13.1
0.56
5
48.5
3
±
14.9
53.2
0
±
17.3
0.10
3C
omp
ress
ion
rate
113.
6
±
16.3
115.
0
±
12.8
0.54
4
116.
9
±
18.8
118.
9
±
13.0
0.57
6
118.
3
±
13.3
118.
1
±
13.0
0.92
3Pr
op
com
p
dep
th
<
38
mm
0.08
(0.0
2,
0.37
)
0.09
(0.0
1,
0.55
)
0.67
4
0.05
(0.0
1,
0.70
)
0.21
(0.0
1,
0.43
)
0.75
8
0.05
(0.0
1,
0.11
) 0.
02
(0.0
1,
0.07
)
0.64
2Pr
op
com
p
wit
h
lean
ing
0.03
(0.0
, 0.1
8)
0.11
(0.0
1,
0.32
)
0.06
9
0.09
(0.0
2,
0.27
)
0.05
(0.0
, 0.2
3)
0.24
4
0.05
(0.0
1,
0.37
)
0.02
(0.0
0,
0.17
)
0.77
8
*Si
gnifi
can
t
at
p
<
0.05
.
PRESSn xxx (2014) xxx–xxx
increases in average inflation time after airway insertion in bothLMA (p = 0.888) and ETT group (p = 0.787). These trends may reflectdeteriorating pulmonary compliance which is seen when the dura-tion of the resuscitation attempt increases.26,27
Average change in impedance between start and top of ven-tilation and was measured in ohms. There was no statisticallysignificant difference found between before and after insertion inall 3 airway group (Table 3).
Insertion of ETT led to a significant increase in ventilationrate from 6.9 ± 4.9 min–1 to 10.6 ± 4.3 min−1 (p = 0.0001). Similarincrease in ventilation rate was not seen in LMA and BVM group(Table 3).
3.3. Airway device and time to insertion
There was no significant difference in median time to insert ETTand LMA (Table 4). There was no difference found in median timetaken to successfully insert the airway between the two groups (ETT15.8 s IQR 6.8, 19.4 vs LMA 8.0 s IQR 5.5, 15.9, p = 0.109) (Table 4).Of note, there were three episodes where LMA was used to provideairway management but was then deemed unsatisfactory by theoperator. On all three occasions, LMAs were changed into ETTs byanaesthetists. In ETT group, all patients were successfully intubatedon first attempt and there were no recorded failed intubations inour sample. No regurgitation after airway insertion was reportedin the study.
4. Discussion
This is the first clinical study to demonstrate that the use ofETT or LMA significantly improved the quality of cardiopulmonaryresuscitation by reducing overall no flow ratio. This occurred pri-marily due to switching from a compression to ventilation ratio of30:2 to continuous chest compression and asynchronous ventila-tion. Airway devices were inserted with minimal interruptions inCPR (ETT 15 s, LMA 8 s) and the quality of CPR (compression rate,depth, leaning) was maintained after device insertion.
There are limited published data on the impact of airway deviceon quality of CPR in the clinical setting. In a simulation study, Aboand colleagues compared insertion of oesophageal combitube (ETC)vs endotracheal intubation (ETT) by paramedics.28 Time to success-ful airway insertion was measured and combitube was found to besignificantly faster than ETC (ETC 75.5 s (IQR 66, 99.5) vs ETT 110.5 s(IQR 87.5, 125.5), p = 0.002). Once inserted, ETC was associated withreduced no flow time (ETC 66.5 s IQR 60–74, ETT 73.5 IQR 68.5, 95,p = 0.005). An observational study by Wiese et al. compared the useof the disposable airway device – laryngeal tube suction (LTS-D)with bag mask ventilation (BMV) during simulated resuscitationon a manikin. Their results suggested that NFT could be reducedsignificantly with the use of LTS-D compared to BMV (105.2 svs 149.7 s respectively, p < 0.01) in a simulated setting.12 Thesefindings are consistent with an observational study by Kramer-Johansen et al. in humans which measured the quality of CPR beforeand after intubation. Mean no flow ratio decreased from 61% (SD20) before intubation to 41%(SD 18) after intubation.29 The numberof compressions delivered per minute was also significantly higher(47 min−1 (SD 25) before, 71 min−1 (SD 23) after). Ventilation ratealso increased after intubation (5.6 min−1 (SD 3.7) before, 14 min−1
(SD 5.0) after) reflecting the transition from ventilation betweencycles of compressions and continuous chest compression.
There are a number of uncertainties about the role of advanced
y management on quality of cardiopulmonary resuscitation: An014), http://dx.doi.org/10.1016/j.resuscitation.2014.02.018
airways in cardiac arrest. Firstly there is uncertainty about whetherventilation is required at all in the early stages of cardiac arrest. Aseries of recent studies from the Arizona and other groups sup-port the value of prioritising cardio-cerebral resuscitation over

ARTICLE IN PRESSG ModelRESUS-5901; No. of Pages 7
J. Yeung et al. / Resuscitation xxx (2014) xxx–xxx 5
Table 3Ventilation characteristics before and after airway insertion. Data given as median (IQR) and mean ± SD.
Ventilation ratea Average inflation time (s) Average change in impedance (�)
Before insertion After insertion p value Before insertion After insertion p value Before insertion After insertion p value
BVM (n = 16) 9.1 ± 4.6 6.9 ± 4.1 0.104 0.81 (0.71, 1.00) 0.92 (0.84, 1.02) 0.076 0.73 (0.49, 0.91) 0.84 (0.70, 1.06) 0.131LMA (n = 23) 6.6 ± 4.0 7.9 ± 4.7 0.129 0.94 (0.83, 1.03) 0.96 (0.84, 1.09) 0.888 0.81 (0.66, 1.15) 0.80 (0.68, 1.07) 0.692ETT (n = 47) 6.9 ± 4.9 10.6 ± 4.3 0.0001* 0.97 (0.80, 1.05) 0.98 (0.84, 1.09) 0.787 0.86 (0.65, 1.18) 0.93 (0.68, 1.08) 0.507
vThplfRdiao
riliap(ccdeR
aIltttfiltEv2acc
eaen
TT
a Excluding episodes with no ventilation detected.* Significant at p = 0.05.
entilation in the early stages of out-of-hospital cardiac arrest.30–32
he present study examined patients in the later stage of out-of-ospital cardiac arrest or in-hospital arrest (higher percentage ofatients with secondary cardiac arrest) where some form of venti-
ation is required. Our study was not powered to examine patientocused outcomes. Thus our finding of no statistical difference inOSC rates (ETT 48%, LMA 25%, BVM 32%, p = 0.078) or survival toischarge rates (ETT 12%, LMA 4%, BVM 8%, p = 0.519) needs to be
nterpreted with caution. In other studies advanced airway man-gement (ETT/Combitube,13 ETT14,16) was associated with worseutcomes.
The timing of airway intervention and any impact on inter-uptions in chest compression are likely to be important. Theres evidence supporting avoidance of interruptions in CPR particu-arly during the early phases of resuscitation.6,7,33,34 Interruptionsn CPR are linked to reductions in coronary perfusion pressure35
nd development of ventricular fibrillation.36 Clinical studies haveroduced conflicting results with Shy identifying early intubationwithin 12 min) as linked to improved survival in out-of-hospitalardiac arrest (RR late intubation 0.42, 95% CI 0.26, 0.69).37 Byontrast, the American Heart Association’s National Registry of Car-iopulmonary Resuscitation failed to find any association betweenarly advanced airway intervention (<5 min) vs late (>5 min) forOSC or survival to discharge rates.38
Given these uncertainties it is essential that if an advancedirway is planned, interruptions in CPR are kept to a minimum.n this study, the median recorded time taken to insert ETT wasonger and took 15.8 s (IQR 6.8, 19.4). In comparison, median timeaken to insert LMA was shorter (8.0 s IQR 5.5, 15.9) and withinhe recommended time. Although the difference was not foundo be statistically significant, LMA was quicker to insert. Similarndings were reported in a manikin study by Gatward and col-
eagues who compared the time taken to intubate with time neededo insert other supraglottic devices during chest compressions.39
ndotracheal intubation was found to be the slowest amongst theolunteers (19.0 s IQR 15.9, 24.0), followed by LMA (14.6 s IQR 12.8,0.0) and iGel (7.8 s IQR 7.2, 9.0). The shorter time taken to insertirway in this study could be explained by hospital policy and resus-itation guidelines that intubation was only undertaken by thoseompetent at intubation.20
One major advantage of using LMA is the ease of insertion
Please cite this article in press as: Yeung J, et al. The impact of airwaobservational study in patients during cardiac arrest. Resuscitation (2
ven by non-experts but research has shown that airway man-gement training on the ALS course on its own could not providenough practical airway management and ventilation skills foron-anaesthetic trainees to become competent in managing an
able 4ime to insertion and time taken to insert device of the two groups.
EndotrachealtubeN = 50
Laryngeal maskairwayN = 25
p value
Time to insertion (s) 145.5 (86.8,305.3)
126.0 (40.0,306.0)
0.132
Time taken to insert airway (s) 15.8 (6.8, 19.4) 8.0 (5.5, 15.9) 0.109Failed insertion (%) 0 (0%) 3 (12%) 0.012
airway. A study by Deakin reported 37.5% of ALS trained non-anaesthetic trainees failing to insert LMA in anaesthetised patients,11% resulting in airway complications compared to none in anaes-thetic trainees.40 Interestingly, this study reported three episodeswhere effective ventilation was not achieved with LMA and this waslater changed to ETT. In contrast to some published studies,11,41,42
the results did not reveal a high complication rate from endotra-cheal intubation and no failed intubation was reported.
The use of LMAs can be problematic in the emergency setting.The pressure seal formed by LMA is relatively low which can pre-vent effective ventilation when there is high airway pressure or lowpulmonary compliance as seen in cardiac arrest.43 A recent study bySegal and colleagues elicited impact of supraglottic devices (SAD)on cardiovascular haemodynamics in pigs.44 In the swine model,three different SADs designed for human use (King tube, LMA andCombitube) all caused significant reduction in carotid bloodflow.The authors suggested that the increase in supraglottic pressure ledto potential compression of carotid arteries which was also demon-strated in carotid angiography post mortem. Due to the obviouslimitation of the animal model, the authors urged more researchinto this important area. In clinical use, LMAs can also be easily dis-lodged, requiring care with their use and frequent repositioning.Compared to ETT, the use of LMAs cannot isolate the airway andaspiration risk is high due to reduced oesophageal sphincter pres-sure during cardiac arrest.45 Although a Japanese study on out ofhospital cardiac arrests reported a higher arterial pH with patientsventilated through LMA than BVM (pH 7.117 vs 7.075, p = 0.02).46
The group did not report any difference in gaseous exchange (PO2or PaCO2) or survival benefit. A recent propensity matched observa-tional study in out-of-hospital cardiac arrest which included 5278patients treated with BVM, intubation or LMA. This study foundlower survival to discharge amongst patients receiving LMA com-pared to BVM (OR 0.45 (0.25–0.82)).47
4.1. Limitations
This study has several limitations. The sample size was smalland there were more episodes in the ETT group than LMA and BVMgroups. The study sample included both out-of-hospital and in-hospital cardiac arrests therefore it was not possible to evaluateany impact on ROSC or patient survival. The study only comparedtwo commonly available types of airway devices: ETT and LMA andtheir effects on quality of CPR. Other supraglottic airway devices arealso suitable to be used in cardiac arrests such as iGel39,48, laryngealtube,49 and combitube.50
Data collection was via defibrillator pads and measurements ofthoracic impedance. Once robust review of our collected data wasundertaken, we could not eliminate the artefacts imposed on seg-ments of data during ongoing chest compressions. This effect mayhave most impact on ventilation parameters. Another measure of
y management on quality of cardiopulmonary resuscitation: An014), http://dx.doi.org/10.1016/j.resuscitation.2014.02.018
ventilation was capnography which we were unable to collect dueto limited availability of equipment. A study by Edelson exam-ined the use of capnography and thoracic impedance found thatboth tend to underestimate ventilation rate.51 As yet there is no

ING ModelR
6 itatio
ro
5
sercaac
C
fii
A
bH
R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
3
4
4
4
4
4
4
4
ARTICLEESUS-5901; No. of Pages 7
J. Yeung et al. / Resusc
eliable method of assessing delivered tidal volumes and efficiencyf ventilation during cardiac arrest.
. Conclusions
This is the first study to demonstrate that the use of ETT or LMAignificantly improves overall no flow ratio during resuscitationpisodes when compared with using BVM in the in hospital envi-onment. There was also no significant difference in quality of chestompressions between three airway groups. Time taken to insertirway devices was within recommended limits. Further studiesre needed to examine the effectiveness of different airways duringardiac arrests.
onflict of interest statement
Dr Yeung received a Resuscitation Council UK PhD fellowshiprom 2008 to 2011 which covered her PhD fees. No other fund-ng was received for this study. The authors declared no conflict ofnterest.
cknowledgements
The authors would like to thank the cardiac arrest team mem-ers and the Resuscitation Department at Birmingham Heartlandsospital.
eferences
1. Wik L. Rediscovering the importance of chest compressions to improve theoutcome from cardiac arrest. Resuscitation 2003;58:267–9.
2. Wik L, Steen PA, Bircher NG. Quality of bystander cardiopulmonary resus-citation influences outcome after prehospital cardiac arrest. Resuscitation1994;28:195–203.
3. Abella BS, Sandbo N, Vassilatos P, et al. Chest compression rates duringcardiopulmonary resuscitation are suboptimal: a prospective study during in-hospital cardiac arrest. Circulation 2005;111:428–34.
4. Abella B, Alvarado J, Myklebust H, et al. Quality of cardiopulmonary resuscitationduring in-hospital cardiac arrest. JAMA 2005;293:305–10.
5. Steen S, Liao Q, Pierre L, Paskevicius A, Sjöberg T. The critical importance ofminimal delay between chest compressions and subsequent defibrillation: ahaemodynamic explanation. Resuscitation 2003;58:249–58.
6. Edelson DP, Abella BS, Kramer-Johansen J, et al. Effects of compression depthand pre-shock pauses predict defibrillation failure during cardiac arrest. Resus-citation 2006;71:137–45.
7. Wik L, Kramer-Johansen J, Myklebust H, et al. Quality of cardiopulmonary resus-citation during out-of-hospital cardiac arrest. JAMA 2005;293:299–304.
8. Studnek JR, Thestrup L, Vandeventer S, et al. The association between prehospitalendotracheal intubation attempts and survival to hospital discharge among out-of-hospital cardiac arrest patients. Acad Emerg Med 2010;17:918–25.
9. Shy BD, Rea TD, Becker LJ, Eisenberg MS. Time to intubation and survival inprehospital cardiac arrest. Prehosp Emerg Care 2004;8:394–9.
0. Nolan JP, Soar J. Airway techniques and ventilation strategies. Curr Opin CritCare 2008;14:279–86.
1. Wang HE, Simeone SJ, Weaver MD, Callaway CW. Interruptions in cardiopul-monary resuscitation from paramedic endotracheal intubation. Ann Emerg Med2009;54:645–52, e1.
2. Wiese CHR, Bartels U, Schultens A, et al. Influence of airway management strat-egy on “no-flow-time” during an “advanced life support course” for intensivecare nurses – a single rescuer resuscitation manikin study. BMC Emerg Med2008;8:4.
3. Hanif MK, Niemann AMJT. Advanced airway management does not improveoutcome of out-of-hospital cardiac arrest. Acad Emerg Med 2010;17:926–31.
4. Studnek JT, Vandeventer L, Ward S, Staley SR, Garvey K, Blackwell LT. The asso-ciation between prehospital endotracheal intubation attempts and survival tohospital discharge among out-of-hospital cardiac arrest patients. Acad EmergMed 2010;17:918–25.
5. Stiell IG, Wells GA, Field B, et al. Advanced cardiac life support in out-of-hospitalcardiac arrest. N Engl J Med 2004;351:647–56.
6. Gausche M, Lewis RJ, Stratton SJ, et al. Effect of out-of-hospital pediatric endo-
Please cite this article in press as: Yeung J, et al. The impact of airwaobservational study in patients during cardiac arrest. Resuscitation (2
tracheal intubation on survival and neurological outcome: a controlled clinicaltrial. JAMA 2000;283:783–90.
7. Hasegawa K, Hiraide A, Chang Y, Brown DF. Association of prehospital advancedairway management with neurologic outcome and survival in patients with out-of-hospital cardiac arrest. JAMA 2013;309:257–66.
4
4
PRESSn xxx (2014) xxx–xxx
8. Bobrow BJ, Clark LL, Ewy GA, et al. Minimally interrupted cardiac resuscita-tion by emergency medical services for out-of-hospital cardiac arrest. JAMA2008;299:1158–65.
9. Wang HE, Szydlo D, Stouffer JA, et al. Endotracheal intubation versussupraglottic airway insertion in out-of-hospital cardiac arrest. Resuscitation2012;83:1061–6.
0. Deakin CN, Soar JP, Sunde J, Koster K, Smith RW, Perkins GBGD. European Resus-citation Council Guidelines for Resuscitation 2010. Section 4. Adult advanced lifesupport. Resuscitation 2010;81:1305–52.
1. Soar J. The I-gel supraglottic airway and resuscitation – some initial thoughts.Resuscitation 2007;74:197.
2. Kramer-Johansen J, Edelson DP, Losert H, Köhler K, Abella BS. Uniform repor-ting of measured quality of cardiopulmonary resuscitation (CPR). Resuscitation2007;74:406–17.
3. Aase SMH. Compression depth estimation for CPR quality assessment using DSPon accelerometer signals. IEEE Trans Biomed Eng 2002;49:263–8.
4. Risdal M, Aase SO, Stavland M, Eftestøl T. Impedance-based ventilationdetection during cardiopulmonary resuscitation. IEEE Trans Biomed Eng2007;54:2237–45.
5. Edelson DP, Litzinger B, Arora V, et al. Improving in-hospital cardiacarrest process and outcomes with performance debriefing. Arch Intern Med2008;168:1063–9.
6. Paal P, Neurauter A, Loedl M, et al. Effects of stomach inflation on haemodynamicand pulmonary function during spontaneous circulation in pigs. Resuscitation2009;80:470–7.
7. Davis K, Johannigman JA, Johnson RC, Branson RD. Lung compliance followingcardiac arrest. Acad Emerg Med 1995;2:874–8.
8. Abo BN, Hostler D, Wang HE. Does the type of out-of-hospital airway interferewith other cardiopulmonary resuscitation tasks? Resuscitation 2007;72:234–9.
9. Kramer-Johansen J, Myklebust H, Wik L, et al. Quality of out-of-hospital car-diopulmonary resuscitation with real time automated feedback: a prospectiveinterventional study. Resuscitation 2006;71:283–92.
0. Ewy GA. Cardiocerebral resuscitation: the new cardiopulmonary resuscitation.Circulation 2005;111:2134–42.
1. Ewy GA, Zuercher M, Hilwig RW, et al. Improved neurological outcome with con-tinuous chest compressions compared with 30:2 compressions-to-ventilationscardiopulmonary resuscitation in a realistic swine model of out-of-hospital car-diac arrest. Circulation 2007;116:2525–30.
2. Ewy GA, Kern KB. Recent advances in cardiopulmonary resuscitation: cardio-cerebral resuscitation. J Am Coll Cardiol 2009;53:149–57.
3. Hoyer CB, Christensen EF, Eika B. Increase in pre-shock pause caused by drugadministration before defibrillation: an observational, full-scale simulationstudy. Resuscitation 2010;81:343–7.
4. Kellum MJ, Kennedy KW, Ewy GA. Cardiocerebral resuscitation improves sur-vival of patients with out-of-hospital cardiac arrest. Am J Med 2006;119:335–40.
5. Berg RA, Sanders AB, Kern KB, et al. Adverse hemodynamic effects of interruptingchest compressions for rescue breathing during cardiopulmonary resuscitationfor ventricular fibrillation cardiac arrest. Circulation 2001;104:2465–70.
6. Chamberlain D, Frenneaux M, Steen S, Smith A. Why do chest compressions aiddelayed defibrillation? Resuscitation 2008;77:10–5.
7. Shy BD, Rea TD, Becker LJ, Eisenberg MS. Time to intubation and survival inprehospital cardiac arrest. Prehosp Emerg Care 2004;8:394–9.
8. Wong ML, Carey S, Mader TJ, Wang HE. American Heart Association NationalRegistry of Cardiopulmonary Resuscitation I. Time to invasive airway placementand resuscitation outcomes after inhospital cardiopulmonary arrest. Resuscita-tion 2010;81:182–6.
9. Gatward JJ, Thomas MJC, Nolan JP, Cook TM. Effect of chest compressions onthe time taken to insert airway devices in a manikin. Br J Anaesth 2008;100:351–6.
0. Deakin CD, Murphy D, Couzins M, Mason S. Does an advanced life supportcourse give non-anaesthetists adequate skills to manage an airway? Resusci-tation 2010;81:539–43.
1. Wang HE, Cook LJ, Chang C.-C.H., Yealy DM, Lave JR. Outcomes after out-of-hospital endotracheal intubation errors. Resuscitation 2009;80:50–5.
2. Nolan J. Strategies to prevent unrecognised oesophageal intubation during out-of-hospital cardiac arrest. Resuscitation 2008;76:1–2.
3. Wenzel V, Idris AH, Banner MJ, et al. Respiratory system compliance decreasesafter cardiopulmonary resuscitation and stomach inflation: impact of largeand small tidal volumes on calculated peak airway pressure. Resuscitation1998;38:113–8.
4. Segal N, Yannopoulos D, Mahoney BD, et al. Impairment of carotid artery bloodflow by supraglottic airway use in a swine model of cardiac arrest. Resuscitation2012;83:1025–30.
5. Gabrielli A, Wenzel V, Layon AJ, von Goedecke A, Verne NG, Idris AH. Loweresophageal sphincter pressure measurement during cardiac arrest in humans:potential implications for ventilation of the unprotected airway. Anesthesiology2005;103:897–9.
6. group S-Ks. Comparison of arterial blood gases of laryngeal mask airwayand bag-valve-mask ventilation in out-of-hospital cardiac arrests. Circ J2009;73:490–6.
y management on quality of cardiopulmonary resuscitation: An014), http://dx.doi.org/10.1016/j.resuscitation.2014.02.018
7. Shin SD, Ahn KO, Song KJ, Park CB, Lee EJ. Out-of-hospital airway managementand cardiac arrest outcomes: a propensity score matched analysis. Resuscitation2012;83:313–9.
8. Wharton NM, Gibbison B, Gabbott DA, Haslam GM, Muchatuta N, Cook TM. I-gelinsertion by novices in manikins and patients. Anaesthesia 2008;63:991–5.

ING ModelR
itation
4
5
ARTICLEESUS-5901; No. of Pages 7
J. Yeung et al. / Resusc
Please cite this article in press as: Yeung J, et al. The impact of airwaobservational study in patients during cardiac arrest. Resuscitation (2
9. Wiese CH, Bahr J, Popov AF, Hinz JM, Graf BM. Influence of airway managementstrategy on “no-flow-time” in a standardized single rescuer manikin scenario (acomparison between LTS-D and I-gel). Resuscitation 2009;80:100–3.
0. Doerges V, Sauer C, Ocker H, Wenzel V, Schmucker P. Airway management dur-ing cardiopulmonary resuscitation – a comparative study of bag-valve-mask,
5
PRESS xxx (2014) xxx–xxx 7
y management on quality of cardiopulmonary resuscitation: An014), http://dx.doi.org/10.1016/j.resuscitation.2014.02.018
laryngeal mask airway and combitube in a bench model. Resuscitation1999;41:63–9.
1. Edelson DP, Eilevstjonn J, Weidman EK, Retzer E, Hoek TLV, Abella BS. Capnog-raphy and chest-wall impedance algorithms for ventilation detection duringcardiopulmonary resuscitation. Resuscitation 2010;81:317–22.