Embed Size (px)
Citation preview

The Impact of Physician and ICD-10
Terminology On ObamaCare Initiatives
July, 2015
James S. Kennedy, MD, CCS
1

Disclaimer The materials utilized in this presentation are intended solely for use in
conjunction with today’s seminar. Although great efforts have been taken in the preparation of today’s
material, the speaker and his employer does not assume responsibility for errors or omissions or for damages resulting from the use of the information contained therein.
Advice is general, thus participants should consult professional counsel for specific legal, ethical, technical and clinical questions prior to claim submission.
This lecture was prepared with information that was publicly available on April 1, 2015
ICD-9-CM, ICD-10 and MS-DRGs are constantly evolving. Please consult official guidance prior to code preparation or submission.
2

Speaker Information
• James S. Kennedy MD CCS President, CDIMD Engaged in Clinical Documentation and Coding Integrity (CDCI)
physician/CDS/coder education, training, and process development • Education and Certifications Medical School – UT Memphis, 1979 Board Certified – Internal Medicine, 1983 AHIMA CCS Certification – 2001 • Publications
– 2007 – AHIMA – Severity Adjusted DRGs, an MS-DRG Primer – 2009 – ACDIS – Physician Query Handbook – Ongoing – “Minute for the Medical Staff” in HcPRO’s Medical Records Briefings – Ongoing – “Coding Clinic Update” – HcPRO’s CDI Journal (ACDIS)
• Contact (615) 479-7021 – Cellular [email protected]
3

Objectives • Have a firm understanding of how CMS and the state of
California evaluate physician/hospital quality
• Know the differences between the CDC’s ICD-9-CM and ICD-10-CM/PCS terminology
• Master challenging definitions impacting severity and risk adjustment
• Devise a plan to assure the integrity of their ICD-10-CM/PCS data measuring patient outcomes
4

Like the Phone Book Interesting Characters – Terrible Plot
Dictionary without
Definitions

Dictionary w/o Definitions
Note that clinical terms are assigned numbers which, if submitted, labels the patient with that condition

ICD-10 Implementation Date October 1, 2015 - Tentative
7
Diagnoses Procedures
ICD-10-CM (Clinical Modification)
All entities - providers and facilities for diagnoses in all settings: – Hospital inpatients – Hospital outpatients – Physicians offices – Emergency department – Home health – Long-term care – Rehabilitation facilities
ICD-10-PCS (Procedure Coding System)
Used by inpatient facilities ONLY • Includes outpatient facility services
rendered within the prior 72 hours of writing the inpatient order
• Very different than ICD-9-CM or CPT
CPT • Physician and outpatient/observation
facility services still utilize CPT • CPT does not change!!

Morbidity Uses Varying Implementation Throughout the World
The US is one of the last industrialized country to
adopt ICD-10 for clinical use

US Modifications – ICD-10-CM and PCS The Cooperating Parties
• CDC • Responsible for diagnoses
• CMS • Responsible for inpatient
procedures
• American Hospital Assn. • Responsible for interpreting
ICD-9 or ICD-10 (Coding Clinic)
• American HIM Assn. • Provides input from coding
community
9

ICD-10-CM/PCS Basics
• ICD-10-CM/PCS (and ICD-9-CM) are NOT clinical languages (like SNOMED) – ICD-9-CM and ICD-10-CM/PCS are useful for classifying
healthcare data for administrative purposes, including reimbursement claims, health statistics, and other uses where data aggregation is advantageous
• ICD-10-CM/PCS is based ONLY on provider documentation of clinical language, not on a patient’s clinical characteristics that are abstracted by a data analyst (e.g. like STS, NCDR, or ATS databases) – The provider must use the magic words that drive ICD-10-
CM/PCS code assignment based upon patient circumstances
10

ICD-10 Physician Revenue Cycle Impact
• Ancillary claim payment
– “Medical necessity” is currently based on an ICD-9-CM
• ICD-10 codes after October 1, 2014
– Payers typically release diagnosis codes supporting “medical necessity” through provider bulletins
• ICD-10 Payer Transition
– Starts with the CMS General Equivalence Mappings
– Additional modifications added according to their policies
– Results often published on the web or in their bulletins
• Hard to find

CMS National Coverage Determinations Home PT Monitoring
• Note that codes for secondary hypercoagulable states are not included.
http://tinyurl.com/CMSICD10LCDs

http://www.cms.gov/Medicare/Coding/ICD10/Downloads/ICD-10-guidance.pdf

“Family of Codes”
• “Family of codes” is the same as the ICD-10 three-character category. – Codes within a category are clinically related and provide
differences in capturing specific information on the type of condition.
– For instance, category H25 (Age-related cataract) contains a number of specific codes that capture information on the type of cataract as well as information on the eye involved.
• Examples include: H25.031 (Anterior subcapsular polar age-related cataract, right eye), which has six characters; H25.22 (Age-related cataract, morgagnian type, left eye), which has five characters; and H25.9 (Unspecified age-related cataract), which has four characters.
• One must report a valid code and not a category number. In many instances, the code will require more than 3 characters in order to be valid.

Medi-Cal ICD-10 Medical Necessity - Crosswalk
• Medi-Cal implementation of ICD-10 – Medi-Cal will be using a crosswalk solution in the legacy
California Medicaid Management Information System (CA-MMIS).
• Medi-Cal has mapped all ICD-10 codes to corresponding ICD-9 codes by starting with the General Equivalence Mappings (GEMs) provided by the Centers for Medicare & Medicaid Services (CMS) and modifying the mappings to align with existing Medi-Cal policy.
• Claims will be run against the crosswalk to determine the ICD-9 value to process through the system.
• Will an ICD-10 to ICD-9 crosswalk be published? – Medi-Cal will not publish the crosswalk. – However, the provider manuals will be updated with the
ICD-10 codes as appropriate.

Mapping Tool http://tinyurl.com/I9toI10crosswalk
Note how ICD-10-CM combined benign, malignant, and unspecified HTN into one code, I10 - HTN

Potential Problems with GEMS:
• A single ICD-9-CM code may now be represented by multiple ICD-10-CM codes • One to many
• Multiple ICD-9-CM codes may map to only one ICD-10 code • Many to one
• An ICD-10 code cannot be arbitrarily chosen from the GEM • A code may not represent the complexity of the illness (e.g. unspecified
code) – this could result in underpayments • A code may overstate the complexity of the illness – this could result in
audits and retrospective recovery of payments
ALWAYS VERIFY CODES IN THE ICD-10-CM BOOK PRIOR TO CLAIM SUBMISSION. DO NOT RELY ON ANY GEM TOOL ALONE
17

StJHS’s ICD-10 Strategy - CDI
Physician
CDI Team
ICD-10 Coder

What’s Old? ICD-9-CM
19

What’s New ICD-10-CM
20

ICD-9-CM and ICD-10-CM/PCS
Diagnoses and Procedures
Code Type ICD-9-CM ICD-10-CM ICD-10 PCS
Diagnosis 14,567 codes 69,832 codes
Inpatient Procedures
3,878 codes 71,920 codes
21

Overall Changes
• 34,250 (50%) are related to the musculoskeletal system
• 17,045 (25%) are related to fractures
• 10,582 (62%) of fracture codes to distinguish ‘right’ vs. ‘left’
• ~25,000 (36%) of all ICD-10 codes to distinguish ‘right’ vs. ‘left’

Differences from ICD-9-CM to ICD-10-CM
ICD-9-CM
Diagnosis Codes ICD-10-CM
Diagnosis Codes
Laterality No Laterality
Laterality –
Right or Left account for 35-40% of codes
Code Construction
3-5 digits 7 digits
First digit is alpha (E or V) or numeric
Digit 1 is alpha; Digit 2 is numeric
Digits 2-5 are numeric Digits 3–7 are alpha or numeric
Decimal is placed after the third character
Decimal is placed after the third character
Placeholders No placeholder characters “X” placeholders
# of Codes 14,000 codes 69,000 codes
Severity Limited Severity Parameters Extensive Severity Parameters
Combination Limited Combination Codes Extensive Combination Codes
Excludes Notes
1 type of Excludes Notes 2 types of Excludes Notes

Clinical Changes Expansions and Deletions
• Marked expansion of codes – Trauma, overdoses, or complications
treatment phases – Office encounters – Asthma – Diabetes mellitus – Obstetrics (trimesters) – Non-pressure ulcer staging – Myocardial infarction timing and vessel
involvement – Open fractures staging – Cerebral hemorrhage location – Ischemic stroke vessel involvement – Coma (Glasgow Coma Scale) – Atrial flutter and fibrillation – Drug underdosing
• Deletion of MD language, such as: – Urosepsis
• Must say “sepsis due to UTI”
– SIRS due to infection • Must say “sepsis” or
“severe sepsis”
– Accelerated or malignant hypertension
• Must describe the organ dysfunction caused by hypertension to measure severity
MD progress notes and DC summaries must use ICD-10-CM’s language (Index or Table) as to defend the assigned code

General Equivalence Mapping
This exercise will NOT capture new ICD-10 specificities Validate all mappings using ICD-10 Index, Table, and Guidelines

General Equivalence Mapping Combination Codes with Hematuria

General Equivalence Mapping Priapism and Impotence
This exercise will NOT capture all new ICD-10 specificities Validate all mappings using ICD-10 Index, Table, and Guidelines

General Equivalence Mapping Other Specified Disorders

Clinical Changes Expansions and Deletions
• Marked expansion of codes – Trauma, overdoses, or complications
treatment phases – Office encounters – Asthma – Diabetes mellitus – Obstetrics (trimesters) – Non-pressure ulcer staging – Myocardial infarction timing and vessel
involvement – Open fractures staging – Cerebral hemorrhage location – Ischemic stroke vessel involvement – Coma (Glasgow Coma Scale) – Atrial flutter and fibrillation – Drug underdosing
• Deletion of MD language, such as: – Urosepsis
• Must say “sepsis due to UTI”
– SIRS due to infection • Must say “sepsis” or
“severe sepsis”
– Accelerated or malignant hypertension
• Must describe the organ dysfunction caused by hypertension to measure severity
MD progress notes and DC summaries must use ICD-10-CM’s language (Index or Table) as to defend the assigned code

New Specificity in ICD-10-CM ICD9 ICD9 Title ICD10 ICD-10 Title Mapping Theory
0723 Mumps pancreatitis B263 Mumps pancreatitis Exact match
5770 Acute pancreatitis B252 Cytomegaloviral pancreatitis I10 combines 2 or more I9 codes
5770 Acute pancreatitis K850 Idiopathic acute pancreatitis Approximate match
5770 Acute pancreatitis K851 Biliary acute pancreatitis Approximate match
5770 Acute pancreatitis K852 Alcohol induced acute pancreatitis
Approximate match
5770 Acute pancreatitis K853 Drug induced acute pancreatitis
Approximate match
5770 Acute pancreatitis K858 Other acute pancreatitis Approximate match
5770 Acute pancreatitis K859 Acute pancreatitis, unspecified
Approximate match
5771 Chronic pancreatitis K860 Alcohol-induced chronic pancreatitis
Approximate match
5771 Chronic pancreatitis K861 Other chronic pancreatitis Approximate match
30
ICD-10-CM, the term “hyperbilirubinemia” does not code to jaundice
The physician must say “jaundice”

Meditech 5.67

Code for Acute Pancreatitis Does Not Account for Necrosis
• SIRS with or without organ dysfunction due to pancreatitis does

« Note the SIRS criteria

1992 Definition of SIRS 2 out of 4
1. Body temperature >38°C or <36°C
2. Heart rate >90/minute
3. Respiratory rate >20/minute or PaCO2 lower than 32 mmHg
4. White blood cell count >12,000 /μL or <4,000/μL

Sepsis vs. SIRS ICD-9-CM vs. ICD-10-CM Table of Diseases
ICD-9-CM SIRS (systemic inflammatory response syndrome) 995.90
due to infectious process 995.91
with acute organ dysfunction 995.92
non-infectious process 995.93
with acute organ dysfunction 995.94
ICD-10-CM Syndrome, systemic inflammatory response
NO CODE FOR SIRS DUE TO INFECTION (aka sepsis) or SEPSIS SYNDROME
of non-infectious origin (without organ dysfunction) R65.10
-- with acute organ dysfunction R65.11
PHYSICIAN MUST SAY “SEPSIS”, NOT “SIRS due to INFECTION”,
TO GET “SEPSIS” IN ICD-10
X

Sepsis in Meditech 5.67

ICD-9-CM vs. ICD-10-CM Appendicitis with peritonitis
ICD-9-CM • 540.0 With generalized peritonitis
– Appendicitis (acute) with: perforation, peritonitis (generalized), rupture:
• fulminating • gangrenous • obstructive • Cecitis (acute) with: perforation, peritonitis
(generalized), rupture • Rupture of appendix
– Excludes: acute appendicitis with peritoneal abscess (540.1)
• 540.1 With peritoneal abscess – Abscess of appendix
• With generalized peritonitis
• 540.9 Without mention of peritonitis – Acute:
• appendicitis without mention of perforation, peritonitis, or rupture:
• Fulminating • gangrenous • inflamed • obstructive
– cecitis without mention of perforation, peritonitis, or rupture
ICD-10-CM • K35.2 Acute appendicitis with generalized
peritonitis – Appendicitis (acute) with generalized (diffuse)
peritonitis following rupture or perforation of appenix
– Perforated appendix NOS – Ruptured appendix NOS
• K35.3 Acute appendicitis with localized peritonitis
– Acute appendicitis with or without perforation or rupture NOS
– Acute appendicitis with or without perforation or rupture with localized peritonitis
– Acute appendicitis with peritoneal abscess
• K35.8 Other and unspecified acute appendicitis
– K35.80 Unspecified acute appendicitis • Acute appendicitis NOS • Acute appendicitis without (localized)
(generalized) peritonitis
– K35.89 Other acute appendicitis

Appendicitis in Meditech 5.67

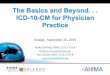
APR-DRG Relative Weights Appendicitis with Appendectomy
Appendicitis with Appendectomy
2.58
1.75
1.02
0.75
0
Appendicitis with focal peritonitis
Sepsis with focal or generalized peritonitis
Severe Sepsis with generalized peritonitis
Higher depending on the organ dysfunction

2012 Diagnostic Criteria for Sepsis Infection, documented or suspected & “some” of the following:
• General variables – Fever (> 38.3°C or 101°F) – Hypothermia (core temperature < 36°C) – Heart rate > 90/min or more than two SD
above the normal value for age – Tachypnea – Altered mental status – Significant edema or positive fluid balance
(> 20 mL/kg over 24 hr) – Hyperglycemia (plasma glucose > 140
mg/dL or 7.7 mmol/L) in the absence of diabetes
• Inflammatory variables – Leukocytosis (WBC count > 12,000/μL) – Leukopenia (WBC count < 4000/μL) – Normal WBC count with greater than 10%
immature forms – Plasma C-reactive protein > two or SD
above the normal value – Plasma procalcitonin > two or SD above
the normal value
• Hemodynamic variables – Arterial hypotension (SBP < 90 mm Hg,
MAP < 70 mm Hg, or an SBP decrease >40 mm Hg in adults or less than two SD below normal for age)
• Organ dysfunction variables – Arterial hypoxemia (Pao2/Fio2 < 300) – Acute oliguria (urine output < 0.5
mL/kg/hr for at least 2 hrs despite adequate fluid resuscitation)
– Creatinine increase > 0.5 mg/dL or 44.2 μmol/L
– Coagulation abnormalities (INR > 1.5 or aPTT > 60 s)
– Ileus (absent bowel sounds) – Thrombocytopenia (platelet count <
100,000/μL) – Hyperbilirubinemia (plasma total bilirubin
> 4 mg/dL or 70 μmol/L) – Tissue perfusion variables – Hyperlactatemia (> 1 mmol/L) – Decreased capillary refill or mottling
Source: http://www.sccm.org/Documents/SSC-Guidelines.pdf

2005 Clinical Indicators of Sepsis in Pediatrics

Sepsis vs. SIRS ICD-9-CM vs. ICD-10-CM Table of Diseases
ICD-9-CM SIRS (systemic inflammatory response syndrome) 995.90
due to infectious process 995.91
with acute organ dysfunction 995.92
non-infectious process 995.93
with acute organ dysfunction 995.94
ICD-10-CM Syndrome, systemic inflammatory response
NO CODE FOR SIRS DUE TO INFECTION (aka sepsis) or SEPSIS SYNDROME
of non-infectious origin (without organ dysfunction) R65.10
-- with acute organ dysfunction R65.11
PHYSICIAN MUST SAY “SEPSIS”, NOT “SIRS due to INFECTION”,
TO GET “SEPSIS” IN ICD-10
X

New in ICD-10-CM Chronic Non-Pressure Ulcer Codes
• Requires dynamic staging much like pressure ulcers – Different methodology – Note if present on admission
L97111 Non-pressure chronic ulcer of right thigh limited to breakdown of skin
L97112 Non-pressure chronic ulcer of right thigh with fat layer exposed
L97113 Non-pressure chronic ulcer of right thigh with necrosis of muscle
L97114 Non-pressure chronic ulcer of right thigh with necrosis of bone
L97119 Non-pressure chronic ulcer of right thigh with unspecified severity

ICD-10-PCS Debridement

DRG Impact Wound Debridement
Documentation DRG DRG Name RW Reimbursement
Pressure ulcer with excision or debridement
592 (w/MCC) Skin Ulcers
1.4249 $11,399
593 (w/CC) 1.0196 $8,156
Pressure ulcer with excisional skin debridement
570 (w/MCC) Skin Debridement
2.3952 $19,162
571 (w/CC) 1.4664 $11,731
Excisional debridement of subcutaneous tissue or fascia, or muscle
579 (w/MCC) Other Subcutaneous Procedures
2.7263 $21,810
580 (w/CC) 1.5727 $12,582
Excisional debridement of (not to) bone
981 (w/MCC) Procedure unrelated to PDx
4.9968 $39,974
982 (w/CC) 2.8150 $22,520
Surgeons must document BOTH the words “excisional”
and “debridement” to get the higher weighted DRGs

Wound Debridement ICD-10 Requirements
• If the word “debridement” is used, indicate – If it is excisional, non-excisional, or
the removal of a foreign body
– The instrument used • Scissors, scalpel, VersaJet, cautery, wire,
curette, irrigation, whirlpool, etc.
– The type of tissue excised • Skin, subcutaneous area, fascia, tendon,
muscle, bone, joint
– The anatomic location
46

Breast Surgery
• A 40 yo lady with a proportionally large left breast “mass” with calcifications on mammography presents for surgery. – An open biopsy indicates high-grade carcinoma
without clear margins, thus a complete mastectomy with a “sentinel node” biopsy was performed.
– Frozen section of the lymph node shows cancer, thus further axillary lymph node “dissection” was carried out.
47

Need for Nature and Anatomic Location of the Breast Tumor
• “Mass” is NOT a neoplasm or tumor – Physician must say
“tumor” or “neoplasm” – For inpatients, cannot
take information from the pathology reports
• Need the anatomic location of the tumor – Often, the location is on
an outpatient document that is not available to the hospital
48
Must code the
laterality or
else the claim
can be denied

Lymph Node Biopsy & “Dissection”
• No code in ICD-10 for “dissection”
• Was the lymph node biopsy diagnostic or therapeutic?
• Excision or resection? – All of the axillary lymph
nodes - resection? • Radical = resection
– Some of the axillary lymph nodes - excision?
• Sampling = excision
49

Axillary Lymph Nodes
50
Source: Public Domain
http://tinyurl.com/86ndkex
• Vary from 20-30 – Brachial (or "lateral") – Pectoral (or "anterior") – Subscapular (or
"posterior") – Central – Apical (or "medial" or
"subclavicular")
• Was it the provider’s intent to remove some or all of the lymph nodes? – ICD-10-CM coding rules
allow for the word “radical” to mean “all of the tissue” within a certain area

Amputations Need for Exact Operative Anatomy • Lower Body (include laterality)
– Hindquarter – Femoral Region – Knee Region – Upper/Lower Leg
• High (proximal) • Mid (mid portion) • Low (distal)
– Foot • Complete or partial
ray(s)/metatarsal(s)
– Toe • High (proximal phalanx) • Mid (PIP joint or middle phalanx) • Low (DIP joint or distal phalanx)
• Upper Body (include laterality) – Forequarter – Shoulder Region – Elbow Region – Upper/Lower Arm
• High (proximal) • Mid (mid portion) • Low (distal)
– Hand • Complete or partial
ray(s)/metacarpal(s)
– Thumb/Finger • High (proximal phalanx) • Mid (PIP joint or middle phalanx) • Low (DIP joint or distal phalanx)
51

Cleft Palate Repair
• Palate description
– Hard/Soft/Both
• Bilateral/Unilateral
• Complete/Incomplete
• With/without Cleft Lip Involvement
– If Cleft Lip involvement—Bilateral/Unilateral
52

Omentum
• Any operation on the omentum requires that the physician document “greater omentum” or “lesser omentum” – ICD-10 does not
allow for “omentum” alone
53

Need for Exact Operative Anatomy
Coders need to know what biliary, GI,
circulatory, or other anatomy is partially
or completely removed, divided,
transferred, or inspected

ICD-10-PCS Lysis of Postoperative Adhesions
• 15-20% of open heart procedures commonly have adhesions – Almost 100% of
reoperations
• Requires a tedious lysis of adhesions, typically lasting around an hour, to reach the operative site
• Incidental injuries are common
• How do we handle this in ICD-10-PCS?

Coding Clinic (ICD-10), 1st Q, 2014, p.4 Lysis of Adhesions
• Carefully review the entire operative report (and not just the title) to determine the clinical significance of the adhesions and the complexity of the lysis of adhesions. – Coders should not code adhesions and lysis thereof, based solely on mention
of adhesions or lysis in an operative report. – Determination as to whether the adhesions and the lysis are significant
enough to code and report must be made by the surgeon.
• If obstruction is not present but a strong band prevents the surgeon from access to the organ (being removed), requiring lysis before the operation can proceed, then – Both the diagnosis of adhesions and the lysis procedure should be coded,
unless instructional notes in the Alphabetical Index, Tabular List, or guidelines preclude the separate coding.
• If adhesions exist without causing any symptoms in the patient or increasing the difficulty of performing the operative procedure. then – Coding a diagnosis of adhesions and the procedure of lysis of adhesions is
inappropriate.

Exact Body Part Being Released
57
While there are options for
unspecified parts of the
esophagus, stomach, small
intestine and large intestine…
ICD-10-PCS does have
specificity for which part of
these organs is being released
Other structures
can be freed as
well, including:
• Gallbladder
• Peritoneum
• Kidney
• Ureter
• Uterus
• Fallopian Tube
• Others

Lysis of Cardiac Adhesions Anatomy Requirements in the Table
Unlike the gut, there
is no option for lysis
of adhesions
surrounding the
heart

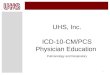
DRG Consequences Lysis of Cardiac Adhesions w/CABG
CABG with no documentation of extensive lysis of adhesions • PDX - I25.110 - ASHD of
native coronary artery with unstable angina pectoris
• PProc – 021009W – for the CABG
MS-DRG 236 – Coronary Bypass w/o Cardiac Cath w/o MCC – 3.7777 NOTE: Also the resultant MS-DRG if only the pericardium is being released
CABG with documentation of extensive lysis of adhesions adherent to the heart
• PDX - I25.110 - Atherosclerotic heart disease of native coronary artery with unstable angina pectoris
• SDx – I31.0 – Chronic adhesive pericarditis
• PProc – 021009W for the CABG
• SProc – Adhesiolysis
– 4 code options - 02N(6,7,K,L)0ZZ
– Codeable only if the surgeon describes the exact HEART anatomy being released
MS-DRG 229 – Other Cardiothoracic Procedures with CC – 4.4606

Expected costs CV Surgery
60
MS-DRG MDC MS-DRG Title Weights Payment
216 05 CARDIAC VALVE & OTH MAJ CARDIOTHORACIC PROC W CARD CATH W MCC 9.5238 $76,190
217 05 CARDIAC VALVE & OTH MAJ CARDIOTHORACIC PROC W CARD CATH W CC 6.3291 $50,633
218 05 CARDIAC VALVE & OTH MAJ CARDIOTHORACIC PROC W CARD CATH W/O CC/MCC 5.5693 $44,554
219 05 CARDIAC VALVE & OTH MAJ CARDIOTHORACIC PROC W/O CARD CATH W MCC 7.7067 $61,654
220 05 CARDIAC VALVE & OTH MAJ CARDIOTHORACIC PROC W/O CARD CATH W CC 5.2056 $41,645
221 05 CARDIAC VALVE & OTH MAJ CARDIOTHORACIC PROC W/O CARD CATH W/O CC/MCC 4.6347 $37,078
231 05 CORONARY BYPASS W PTCA W MCC 7.7247 $61,798
232 05 CORONARY BYPASS W PTCA W/O MCC 5.5976 $44,781 233 05 CORONARY BYPASS W CARDIAC CATH W MCC 7.3493 $58,794
234 05 CORONARY BYPASS W CARDIAC CATH W/O MCC 4.8816 $39,053 235 05 CORONARY BYPASS W/O CARDIAC CATH W MCC 5.7089 $45,671
236 05 CORONARY BYPASS W/O CARDIAC CATH W/O MCC 3.7952 $30,362 237 05 MAJOR CARDIOVASC PROCEDURES W MCC 5.0843 $40,674 238 05 MAJOR CARDIOVASC PROCEDURES W/O MCC 3.4241 $27,393

Medicare-Severity DRGs PDx, CCs and MCCs
• CC = Complications and comorbidities – Moderate resource
consumption increase, averaging • Medicine – $2,400 • Surgery – $6,000
• MCC = Major CCs – Major resource consumption
increase, averaging • Medicine – $4,800 • Surgery – $13,000
CC and MCC definers
√ Significant acute disease (e.g., AMI, stroke, acute respiratory
failure, acute renal failure, pneumonia, septicemia)
√ Acute exacerbations of significant chronic diseases
(e.g., acute systolic heart failure) √ Advanced or end-stage chronic
diseases (e.g., AIDS (not positive HIV), stage IV,
V chronic kidney disease or end-stage renal disease)
√ Chronic diseases associated with extensive debility
(e.g., functional quadriplegia)
http://www.cms.gov/Medicare/Coding/ICD10/ICD-10-MS-DRG-Conversion-Project.html

MS-DRG CC/MCC Table
Not a CC CC MCC
AMS or acute delirium
Unresponsive
Delirium due to a
“medical condition” or
postprocedural state
Toxic or metabolic
encephalopathy
Unconscious or coma
Oxygen dependency
Chronic
respiratory failure
Acute on chronic
respiratory failure
Cystitis
Urosepsis (no code)
UTI or acute cystitis
Bacteremia Sepsis due to UTI
CAD
Stable angina
Demand ischemia
AS of CABG graft
NSTEMI
STEMI
HFpEF
HFrEF
Systolic CHF
Diastolic CHF
Acute systolic CHF
Acute diastolic CHF

Systolic and Diastolic Heart Failure
• As above, not codeable in ICD-9-CM as diastolic or systolic HF • Physician must state “diastolic” or “systolic” or both to get CC or
MCC
63

Heart Failure in Meditech 5.67

Hypoxemia and Hypercapnia Respiratory Insufficiency/Failure
Always list the underlying cause, such as
status asthmaticus, drug overdose, CHF
Entity MS-DRG
Hypoxemia No CC
Hypercapnia No CC
Respiratory insufficiency or distress
No CC
Acute respiratory insufficiency or distress
Not a CC
Acute resp. failure MCC
Chronic resp. failure CC

Respiratory Failure in Meditech 5.67

MS-DRG CC/MCC Table
Not a CC CC MCC
Diabetes Mellitus
Uncontrolled -
Hyperosmolar state
DKA
Blood loss anemia
Acute blood loss
anemia
Toxic anemia
(x chemotherapy)
+ HIV AIDS or +HIV with
previous Hx of AIDS
Ranson’s criteria
(w/pancreatitis)
SIRS
(due to pancreatitis)
SIRS w/organ
dysfunction
Stool with
+ occult blood GI bleeding
GI bleeding from
defined site
(e.g., PUD)

68
Acute Blood Loss Anemia (not ↓ Hct)
• “Acute blood loss anemia” - CC • Major Bleeding Definition
– Clinically overt – Associated with a fall of the hemoglobin level of 2.0 g/dL (e.g. Hct
drop of 6) or required transfusion of at least 2 units of red cells, or involved a critical organ or was fatal
MS-DRG MS-DRG Title Weights Payment 377 G.I. HEMORRHAGE W MCC 1.7775 $14,220 378 G.I. HEMORRHAGE W CC (e.g. acute blood loss anemia) 1.0021 $8,017
379 G.I. HEMORRHAGE W/O CC/MCC 0.6776 $5,421

+HIV (not reportable in CA) vs. HIV Disease (MCC)
• +HIV (no code)
– Includes HIV-infected individual who never had exhibited symptoms
– Based on documentation of +HIV only
• HIV-disease (MCC)
– Currently having acute HIV symptoms
– + HIV with previous HIV-related symptoms
– + HIV with current or previous HIV-related disease
– Current AIDS or previous history of AIDS
69
Must Be Documented on Each Admission

MS-DRG CC/MCC Table
Not a CC CC MCC
Acute renal
insufficiency
Toxic nephropathy
Acute renal failure
Acute kidney injury
Acute tubular necrosis
Acute cortical necrosis
CRI or CKD CKD Stage 4 or 5 ESRD
Chronic/persistent
atrial fibrillation
Persistent
atrial fibrillation
Acute systolic/diastolic
HF due to rapid afib
Past Hx of multiple
DVT on warfarin
Hypercoagulable
state -
Peripheral neuropathy Autonomic peripheral
neuropathy -
Underweight with
anorexia
Cachexia
Malnutrition Severe malnutrition

MDC 5 – DVTs With Hypercoagulable State
MS-DRG MS-DRG title Weights
294 DEEP VEIN THROMBOPHLEBITIS W CC/MCC 1.0373
295 DEEP VEIN THROMBOPHLEBITIS W/O CC/MCC 0.6403
• Primary hypercoagulable states (CC) Initial Recurrent
– Factor V Leiden – 12%–20% / 40%–50%
– Protein C def – 2%–5% / 5%–10%
– Protein S def – 1%–3% / 5%–10%
– AT3 deficiency – 1%–2% / 2%– 5%
• Secondary hypercoagulable states (CC) – Active cancer, chemotherapy (L-asparaginase, thalidomide,
anti-angiogenesis therapy), myeloproliferative disorders, HIT, nephrotic syndrome, intravascular coagulation and fibrinolysis/DIC, TTP, sickle cell disease, oral contraceptives or estrogen, pregnancy/postpartum state, selective estrogen receptor modulator therapy (tamoxifen and raloxifene), antiphospholipid antibodies, PNH, Wegener granulomatosis
Thrombophilia now
has a code
“Still to be ruled out”

Adult Malnutrition New Definition
http://www.tinyurl.com/2012Malnutrition
72

Adult Malnutrition Meets 2 out of 6 Criteria
• Insufficient energy intake
• Weight loss
• Loss of muscle mass
• Loss of subcutaneous fat
• Localized or generalized fluid accumulation that may sometimes mask weight loss
• Diminished functional status as measured by handgrip strength
2 out of 6
criteria used
based on
inflammatory
status
Prealbumin
and albumin
are no
longer
criteria for
malnutrition
73

Adult Malnutrition Criteria
• Acute vs. chronic illness
• Severe vs. non-severe disease
• Albumin/prealbumin don’t matter
http://tinyurl.com/2012malnutrition

Dieticians Impact on Malnutrition Capture
75

CMS’s Emphasis Upon Complications
76

What are AHRQ PSIs?
• The Patient Safety Indicators (PSIs) are a set of indicators providing information on potential in hospital complications and adverse events following surgeries, procedures, and childbirth. – The PSIs were developed after a comprehensive
literature review, analysis of ICD-9-CM codes, review by a clinician panel, implementation of risk adjustment, and empirical analyses.
– Pediatric measures are also in place
http://www.qualityindicators.ahrq.gov/modules/psi_overview.aspx
77

NQF-approved PSI 90 – Composite
http://tinyurl.com/NQF-PSIs 78

NQF Individual Measures
http://tinyurl.com/NQF-PSIs
79

ICD-9-CM - http://www.cdc.gov/nchs/data/icd9/icd9cm_guidelines_2011.pdf
ICD-10-CM - http://www.cdc.gov/nchs/data/icd9/icd10cm_guidelines_2014.pdf
80

Definition of a Complication in Coding Clinic
• It is important to note that not all conditions that occur during or following surgery are classified as complications. – First, there must be more than a routinely expected condition or
occurrence, and – There must be a cause-and-effect relationship between the care
provided and the condition, and • Differentiation between surgical/pharmaceutical care and diseases
– There is indication in the documentation that it is a complication.
• The coder cannot make the determination whether something that occurred during surgery is a complication or an expected outcome. – Only a physician can diagnose a condition, and the physician must
explicitly document whether the condition is a complication. – If it is not clearly documented, the coder should query the physician
for clarification.
Source: Coding Clinic, First Quarter 2011 Pages: 13-14
81

Accidental Lacerations During Surgery Coding Clinic, 2nd Quarter 2007, pp. 11–12
• Question: During an procedure, the surgeon noted, “a small capsular injury of the spleen, which was hemostatic.” – This injury did not require repair.
• An esophagogastroduodenscopy (EGD) was then performed for evaluation of the distal esophagus since the mass had adhered at the gastroesophageal junction. – The EGD revealed a serosal injury to the stomach, which
was repaired with interrupted Lembert sutures. The surgeon did not include the intraoperative tears in the diagnostic statement. What are the appropriate code assignments?
82

Coding Clinic Answer
• Answer: Query the provider, and if the provider states the tear is not clinically significant, omit codes for both the diagnosis and procedure. – When a tear is documented in the operative report, such as a
small serosal tear of the stomach, the surgeon should be queried as to whether the small tear was an incidental occurrence inherent in the surgical procedure or whether the tear should be considered by the physician to be a complication of the procedure.
– If the provider documents that the seromuscular tear is a complication of the surgery, assign code 998.2, Accidental puncture or laceration during a procedure, as an additional diagnosis. This advice is consistent with that previously published in Coding Clinic, 3rd Quarter 1990, p. 18.
83

A Compliant Complications Query 2013 ACDIS-AHIMA Practice Brief
• Clinical scenario: During the removal of an abdominal mass, the surgeon documents, in the description of the operative procedure, a “serosal injury to the stomach was repaired with interrupted sutures.”
• Query: In the description of the operative procedure a serosal injury to the stomach was noted and repaired with interrupted sutures. Was this serosal injury and repair: – A complication of the procedure _____________ – Integral to the above procedure _____________ – Not clinically significant ____________________ – Other ___________ – Clinically Undetermined____________
Please document your response in the health record or below accompanied by clinical substantiation.
• Rationale: This is an example of a query necessary to determine the clinical significance of a condition resulting from a procedure. http://www.tinyurl.com/2013QueryPB
84

PSI 11 – Postoperative Respiratory Failure
85
Immediate Postoperative Progress Note
Discharge Summary

86

Bottom Line
• ICD-9-CM (and ICD-10) codes are crucial – Definitions are critical – Documentation infrastructure must support the
higher specificity
• Physicians are be incentivized to document and code completely in their offices – Especially important if they form Accountable Care
Organizations or participate in other entities emphasizing cost efficiency and outcomes.
• This lecture will orient the healthcare provider of what is needed now and what we can expect in the future
87