Embed Size (px)
Citation preview
AMERICAN JOURNAL OF INDUSTRIAL MEDICINE 49:780–790 (2006)
The Impact of Work-RelatedMusculoskeletal Disorders onWorkers’ Caregiving Activities
Renee-Louise Franche, PhD,� Jason D. Pole, MSc, Sheilah Hogg-Johnson, PhD,Marjan Vidmar, MD, MSc, and Curtis Breslin, PhD
Background The purpose of the study was to describe and quantify the impact of work-related musculoskeletal disorders on workers’ caregiving activities.Methods A cross-sectional study was conducted in which a telephone survey wasadministered to 187 lost-time workers’ compensation claimants from Ontario, of whom49.2% were women. Forty-eight percent of the injured workers were providing unpaid careprior to the injury.Results Injured workers providing caregiving reported an average reduction in time spentin caregiving activities of 5.5 hr/week, 8 months post-injury. A Sex X Return-to-work statusANCOVA was conducted with difference in caregiving hours as the dependent variable,and with the following covariates: Mean number of caregiving hours, comorbidities, siteof injury, and education. Independent of weekly hours of caregiving, decreases incaregiving hours were significantly higher if the worker was a woman or had not returnedto work.Conclusions Work-related musculoskeletal disorders have a significant impact onworkers’ time spent in unpaid caregiving activities, an example of the social consequencesof occupational injuries. Occupational and caregiving roles are limited by work-related disorders in a parallel fashion. Am. J. Ind. Med. 49:780–790, 2006.� 2006 Wiley-Liss, Inc.
KEY WORDS: workers’ compensation; caregiving; return-to-work; musculoskeletaldisorders; occupational injury; gender
INTRODUCTION
Work-related injuries resulting in lost time at work affect
close to 400,000 Canadians [Association of Workers’
Compensation of Canada, 2002] and 1.5 million Americans
every year [Bureau of Labor Statistics, 2003]1. The vast
majority of the research conducted on the consequences of
work-related injuries has focused on economic outcomes and
duration of the disability, the latter being most commonly
defined by duration on compensation. While the literature on
other physical and medical conditions has addressed the
impact of disease on quality of life and family life, very little
attention has been devoted to this issue with regards to work-
related injuries.
Only recently has the importance of the social
consequences of work-related injuries been recognized.
Both the National Institute for Occupational Safety & Health
and the Robert Wood Johnson Foundation have supported
� 2006Wiley-Liss, Inc.
1 These statistics are from the Survey of Occupational Injuries and Illnesseswhich are based on employer-generated workplace incident logs.
Institute for Work & Health and University of Toronto,Toronto, CanadaFinancial sponsor: Institute for Work & Health.*Correspondence to: Rene¤ e-Louise Franche, Institute for Work & Health, 481University
ave., Suite 800,Toronto, Ontario M5G 2E9, Canada. E-mail: [email protected]
Accepted14 May 2006DOI10.1002/ajim.20352. Published online inWiley InterScience
(www.interscience.wiley.com)
research on a wider scope of outcomes, including social
impact of work-related injury [Pransky et al., 1997; Morse
et al., 1998]. In a conceptual framework developed by Dembe
[2001], three main arenas are outlined in which occupational
injuries have consequences for workers’ social roles: The
work environment, family and friends, and the community.
The current article addresses the impact of work-related
musculoskeletal (MSK) injuries on the role of the worker as a
provider of care to family and friends.
THE WORKER AS A CAREGIVER
Many workers combine the roles associated with paid
work and unpaid caregiving work. In Canada, 15% of
employed women and 10% of employed men are caregivers,
when caregiving is defined as ‘‘providing care to maintain or
enhance people’s independence’’ [Cranswick, 1997]. In the
United States, 25% of workers provide unpaid caregiving to
an elderly person [Bond et al., 1998]. Regarding providing
care to their children, 45% of Canadian workers have
children at home [Duxbury and Higgins, 2001] and 46% of
American workers have children under 18 who livewith them
at least half-time [Bond et al., 1998]. It is estimated that over
the next 10 years, as the demographic trend towards an aging
population continues, the total number of employed
caregivers will increase from 11.0 to 15.6 million working
Americans [Wagner, 1997].
Caregiving activities provided to individuals with long-
term illnesses have been categorized into (1) Care provision
involving tasks inside the home such as personal care,
mobility, and household chores and (2) Care management
tasks, such as management of money, transportation,
management of appointments. This categorization has been
supported by factor analysis [Kramer and Kipnis, 1995]. For
caregivers, participation in these activities involves varying
levels of sense of choice and of obligation. In addition, a third
dimension of caregiving which is not consistently addressed
in studies of caregiving activities is the offer of emotional
support to the recipient [Cranswick, 1997].
What happens when a caregiver is injured at work? What
are the consequences for caregivers and their caregiving
recipients? Very few studies have addressed these questions,
and only indirectly, by providing information on activity
limitations reported by injured workers. Workers with upper
extremity cumulative trauma disorders have reported inter-
ference with activities which would typically be involved in
caregiving such as performing household activities [Keogh
et al., 2000], gripping, carrying bags, and bathing [Morse
et al., 1998]. These limitations are present in 40% of injured
workers with upper extremity disorders even 28 months after
registering their compensation claim [Keogh et al., 2000].
Regarding child care, injured workers with upper extremity
disorders are 8.2 times (CI 4.9–13.8) more likely than
controls (without any work-related musculoskeletal pain) to
report ‘‘a lot of’’ or ‘‘some’’ difficulty in child care activities
[Morse et al., 1998]. Of most relevance is the finding that, as
long as 28 months after their initial claim, workers with
work-related cumulative trauma disorders report a higher
percentage of interference in their home activities (63.9%) as
compared to both work (53.3%) and sleep (44.1%) [Keogh
et al., 2000]. The latter finding points to a disparity between
workers’ experience and the research community’s alloca-
tion of resources to specific research topics: While workers
report more disruption in their home lives as a result of work-
related injuries, research activities have been focused on the
cost and duration of work disability, defined as compensation
costs and time on benefits, as primary outcomes.
The current study seeks to fill a gap in the information
available on injured workers’ caregiving activities. We were
specifically interested in investigating how caregiving hours
are affected by a work-related injury. The study’s main
objectives were the following:
Objective 1: Provide descriptive information about
characteristics of workers with work-related MSK
disorders who are also providing care to children or
family or friends, about who their caregiving recipients
are, and about time spent in caregiving activities before
and after injury.
Objective 2: Examine the relationship between gender and
changes in time spent in caregiving activities after a
work-related MSK injury.
Objective 3: Examine the relationship between return-
to-work status and potential changes in time spent in
caregiving activities after a work-related MSK injury.
METHODS
Participants
This cross-sectional study included a group of lost-time
claimants with a work-related back, upper extremity or neck
MSK disorder who reported caregiving activities prior to
injury. The eligible population for this study were workers
employed by firms with workers’ compensation coverage in
the province of Ontario, Canada. In Ontario, approximately
65% of the workforce is covered by the Workplace Safety &
Insurance Board (WSIB) [Workplace Safety & Insurance
Board, 2002]. Participants in the study all had accepted lost-
time claims for back, neck, or upper extremity MSK
injuries. Only claimants reporting caregiving activities prior
to being injured are the focus of this article. Potential
participants were identified through the WSIB claim
database. They were interviewed by telephone approxi-
mately 8 months after the date of their injury, as recorded in
the WSIB database.
Eligible participants had to have filed a new lost-time
claim for temporary total disability, with no previous claim
Work-Related MSK Disorders and Caregiving 781

made in the previous 3 months. Temporary total disability
refers to a situation in which the worker is completely off
work for a period of time which is assumed to be temporary,
and during which the worker receives compensation for lost
income. In contrast, temporary partial disability refers to a
situation where a worker is continuing to work at reduced
hours for a period of time which is assumed to be temporary,
during which the worker receives compensation for the
partially lost income. Other inclusion criteria were: Lost-
time absence of a minimum of 7 days duration during the first
14 days following the injury date and a minimum age of
15 years. Participants considered ‘‘caregivers’’ were provid-
ing caregiving prior to their injury to their own children of
16 years or less, grandchildren of 16 years old or less, a family
member, or a friend.
Respondents reporting a fracture, amputation, burn,
hernia, head injury, concussion, electrocution, or who
experienced difficulty speaking or understanding English
were not eligible to participate. In addition, participants with
a security concern as identified in WSIB database (indivi-
duals with previous violent or harassing behavior) were also
not eligible to participate.
Procedure
To comply with privacy protection standards, potential
study participants were initially contacted by WSIB staff
who outlined the main objectives of the study and asked
permission to provide contact information to the research
team. Participants were then contacted and interviewed by
phone by interviewers from a survey unit which was
administratively and geographically separate from WSIB.
The questionnaire included questions about their injury, pain,
employer, workplace, and healthcare provider. All partici-
pants gave verbal consent over the telephone to complete the
questionnaire and were also asked to return a signed consent
form. Participants were also asked for consent to link the
questionnaire data to WSIB administrative data. All
extracted information from the WSIB database was de-
identified. The process of extraction is governed by a
special agreement between the investigators’ main research
institute and WSIB. The agreement protects the confidenti-
ality of the information and limits access to the information.
The study was approved by the University of Toronto Ethics
Review Board.
Instrumentation
Sociodemographic information
The following information was collected by self-
report and coded using categorical variables: Sex, marital
status, personal income, family income, education, number
of employees working at worksite, and full-time/part-
time status. Age and number of dependent children
were also reported. In addition, information on age and sex
of the target study population was extracted from WSIB
database.
Work status
The working status was assessed with the following two
questions: ‘‘Have you gone back to work at any point since
your injury?’’ followed by ‘‘Are you still at work?’’
Individuals reporting that they had gone back to work and
who were still at work were considered as working, even if
they returned to a different job, or at different hours. All other
individuals, who were not working at the time of the
interview, including those who had made an earlier attempt to
return to work, were considered as not working. In addition,
information on time on benefits was extracted from the WSIB
database, 8 months post-injury. It is now recognized that
compensation status can not be considered as an index of
whether the individual has returned to work, in that many
individuals who are no longer receiving benefits are never-
theless not back at work [Dasinger et al., 1999]. However, it
remains a variable which is closely related to work status.
Injury and workplace information
Site of injury and firm size were extracted from WSIB
database and coded using categorical variables. Site of injury
was confirmed verbally during the initial phone call.
Occupational classification
Data was extracted from the WSIB database and coded
as white collar, pink collar, or blue collar, using the system
devised by Gaudette et al. [2003].
Comorbidity
The Saskatchewan Comorbidity Scale was used to assess
comorbidities [Cote, 1996; Jaroszynski et al., 1996]. This 15-
item self-report scale assesses the presence of 15 types of
comorbidities. For each item, participants are asked if they
experienced the condition and then how much it affected their
health, rating it on a scale from 0 to 4. The total score consists
of a summative score of all items. Reliability and validity
have been established [Cote, 1996; Jaroszynski et al., 1996].
One item was added to the version used in the current study
for female participants to assess whether they had been
pregnant in the last 6 months.
Caregiving hours
Two questions assessed participants’ caregiving activ-
ities associated with childcare and/or with care of a relative or
782 Franche et al.

friend, both before the injury and at time of interview (see
Table I for questions).
Analytical Approach
Participation rates and sample characteristics were first
examined. Generalizability of findings was assessed by
comparing study participants to study population on WSIB
sociodemographic and work characteristics.
In order to assess the impact of injury on caregiving
activities, the primary outcome variable of the study was the
change score between reported pre-injury and post-injury
hours per week spent in caregiving activities provided to
child/family/friend combined. Pre-injury hours of providing
childcare and pre-injury hours providing care to a relative or
friend were summed to provide the sum of all pre-injury
caregiving hours. The same approach was used for post-
injury caregiving hours.
An analysis of covariance (ANCOVA ) was conducted in
which the impact of sex, return-to-work (RTW) status, and
Sex X RTW status interaction was assessed on the difference
between caregiving hours before and after injury. It has been
demonstrated that the difference between two measurements
is related to the magnitude of the measurement [Bland and
Altman, 1995]. Therefore, in this analysis, we controlled for
the confounding effect of the pre-injury and post-injury
means of weekly hours of caregiving by using the mean of the
pre-injury and post-injury caregiving hours as a covariate.
This strategy allowed us to limit the impact of possible
ceiling and floor effects and of regression to the mean.
The potential confounding effect of the following
variables was investigated: Age, personal income, family
income, site of injury, marital status, education, comorbidity,
part-time/full-time status, and type of caregiving recipients.
To identify covariates, we ran the original ANCOVA
described above with each potential confounding variable
as a covariate. If the change in the beta estimates for sex,
RTW status, or Sex X RTW interaction between the original
ANCOVA and the ANCOVAwith a potential confounder was
greater than 10%, the given variable was considered to be a
confounding variable. The ANCOVA was then re-run with
the covariates identified using this method.
RESULTS
Study Participation Flow andParticipation Rates
Over the course of 12 weeks, 1,890 potential participants
were identified from WSIB claim records. Due to time
constraints, WSIB staff recruiters attempted contact by
telephone with 1,719 potential participants and successfully
reached 873 individuals. Of those, 110 were ineligible due to
injury site or type, language problems, or temporary partial
disability status, and 193 refused to be contacted by the
research team. A group of 570 agreed to be contacted by the
research team, which was administratively and geographi-
cally separate from the WSIB. It should be noted that a sub-
component of the study involved sending a paper and pencil
questionnaire to 104 participants to examine the suitability of
this methodology. Their data is not included in this article.
Of the 466 participants who were called by the research
team for a telephone interview, 47 were unreachable, 18 were
found to be ineligible due to injury criteria, language criteria,
or other ineligibility, and 214 refused to participate. Of
the 401 contacted and eligible participants, 187 individuals
agreed to participate, yielding a participation rate of 47%.
This participation rate is comparable to a study using
TABLE I. Questions Assessing Caregiving Status and Activities
(1) For thosewith children or grandchildren under the age of16Thequestions in this section are about activities directly related to takingcare of yourchildrensuchasplaying,bringing themtoschool ordaycare, organizingactivities,helpingwith homework
(a) Prior to your injury, about howmuch time did you spend on child related activities per week?________ Hours
(b) Howmuch time do you spend on child related activities per weeknow?________ Hours
(2)Thequestions inthissectionareaboutactivitiesdirectly relatedtotakingcareofa relativeor friend,suchaspersonal care,helpingwithdailyactivities,givingmedication,arranging for home care, etc.
(a) Are you involved in the care of an elderly or ill familymember or friend?ONo:OYes:
(b) Prior to your injury, about howmuch time did you spend taking care of an elderly or ill familymemberor friendper week?________ Hours
(c) Howmuch time do you spend on this type of care now?________ Hours
Work-Related MSK Disorders and Caregiving 783

a similar recruitment procedure [Cote et al., 2003]. All
187 participants completed the interview. Of the 187
participants, 90 reported providing caregiving activities at
the time of their injury. Ten participants did not consent to
linkage and consequently, their WSIB data is not reported in
the results of this study.
Study Sample Characteristics andGeneralizability of Findings
The average time between injury and interview time was
of 233.05 days (SD¼ 19.12). Of the 187 participants, 90
(48%) injured workers were involved in caregiving activities
prior to their injury.
Using the boxplot procedure separately for each sex, we
identified outliers who had extreme scores on caregiving
hours before or after injury and these cases were deleted from
our analyses. Outliers were defined as individuals whose
hours of pre- or post-caregiving were two standard deviations
above the pre and post means, respectively. Four outliers (one
female, three males) were identified. Their responses
suggested that the respondents had not understood the survey
questions: For instance, they reported zero pre-injury hours
of caregiving after declaring themselves caregivers, or stated
that they were working full-time and providing 80 hr of
unpaid caregiving. Of the remaining 86 participants, 64
(74.4%) provided care to their children or grandchildren, 14
(16.3%) to a family member or friend, and 8 (9.3%) to both
children/grandchildren and family member or friend.
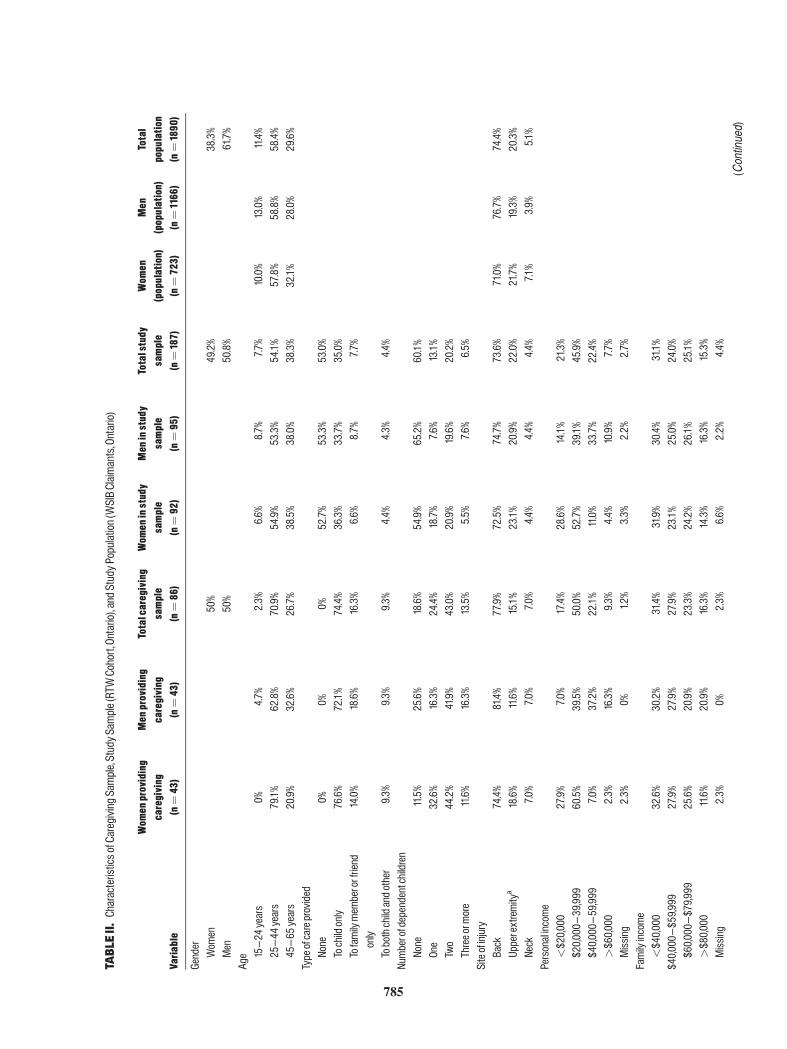
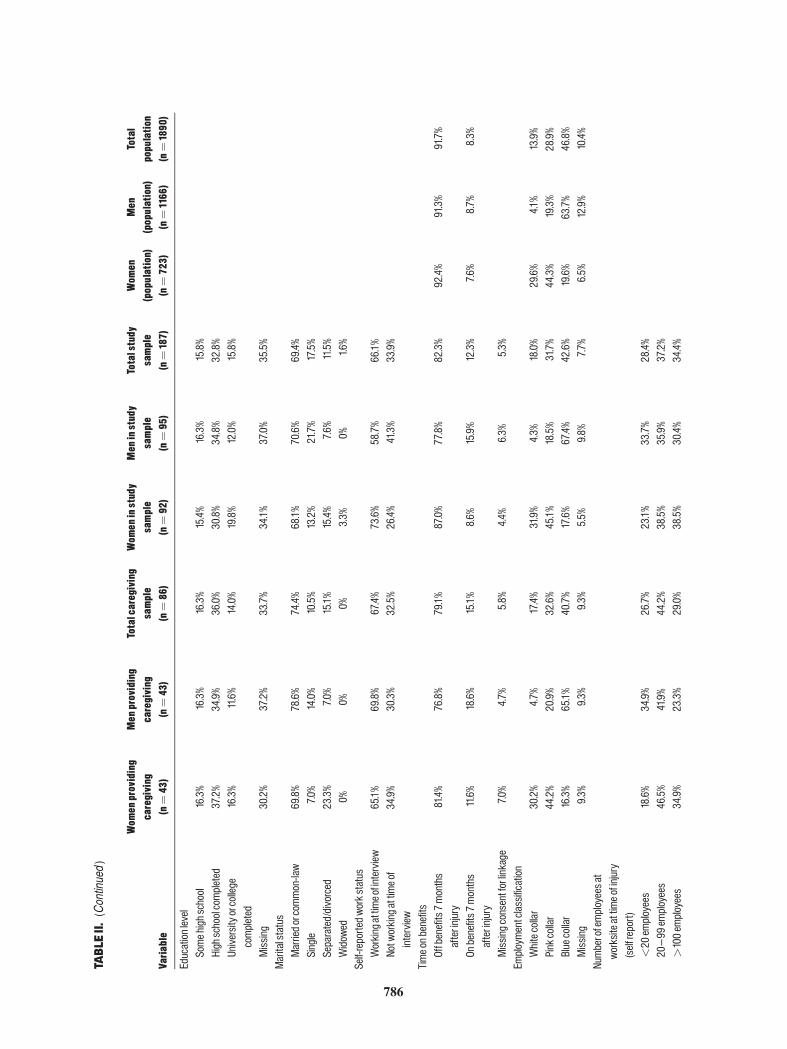
Sociodemographic and workplace characteristics are
reported in Table II for the caregiving sample (n¼ 86), the
complete study sample (n¼ 187), as well as for the study
population (n¼ 1890) (when available from WSIB records).
This allows to address the issue of the generalizability of our
findings by examining the comparability of the study sample
and study population. No statistical testing was conducted to
address these differences in view of the very large number of
potential participants in the study population, which would
lead to detecting negligible differences which are still
statistically significant. In the study sample, participants
were more likely to be women and to be older than in
the study population. Regarding whether they were receiving
compensation 8 months after injury, men in the study
sample were more likely to be on benefits than the study
population. Site of injury, employment classification, and
firm size were all comparable across study sample and study
population.
Main Analyses
The following variables were found to be significant
confounders: Site of injury, comorbidity, and education. For
site of injury, given the low number of neck injuries in our
sample, the neck and upper extremity sites of injury were
collapsed into one category. For comorbidities, given the
skewed distribution of that variable, it was recoded into a
dichotomous variable: Having no comorbidity versus having
at least one comorbidity.
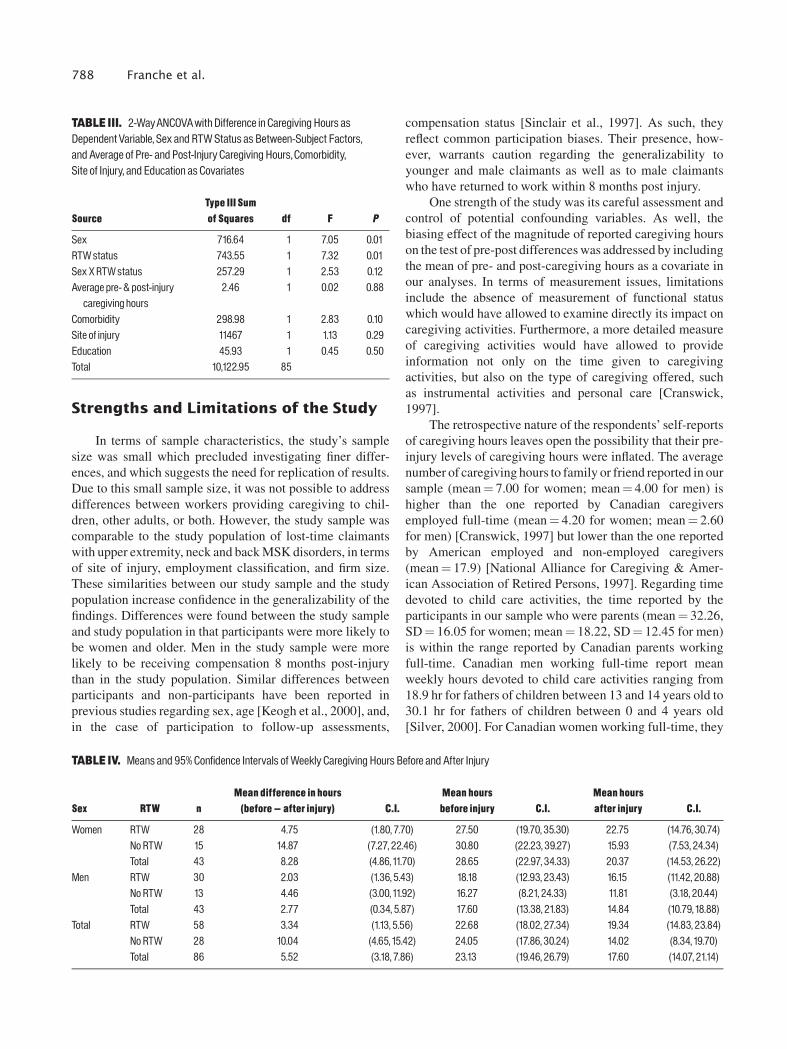
The final Sex X RTW status ANCOVA was conducted,
with change score in pre- and post-injury caregiving hours as
the dependent variable, and with the following variables as
covariates: Mean pre- and post-injury caregiving hours, site
of injury, comorbidity, and education (Table III). Main
effects for sex and RTW status were significant, and the Sex X
RTW status interaction was not. Women had larger decreases
in caregiving hours after injury than men. Individuals who
were not back at work had larger decreases in caregiving
hours. Residual plots for the dependent variable were visually
examined and did not indicate departure from model
assumptions.
Unadjusted means and standard deviations of differ-
ences in weekly caregiving hours before and after injury, as
well as weekly caregiving hours before and after injury, are
found in Table IV. It can be observed that overall, injured
workers reported an average decrease of 5.52 hr per week in
caregiving activities 8 months after injury. Of note are
continuing reductions even for those workers who have
returned to work.
DISCUSSION
The results of our study document the impact of work-
related MSK disorders on workers’ caregiving activities
provided to their children, relatives, and friends. Injured
workers, approximately 8 months post-injury, report an
average reduction in time spent in caregiving activities of
5.52 hr per week, the equivalent of two-thirds of a work day.
Reduction in caregiving time is more pronounced if the
worker is not working at the time of interview and if the
worker is a woman.
Close to half of injured workers with lost-time claims
were caregivers, equally divided between men and women,
which underscores the relevance of our study for many
injured workers. The gender distribution is similar to the one
found in Canadian workers who provide care to a person with
a long-term health problem—approximately 40% men and
60% women [Cranswick, 1997]. Our findings raise the
important issue of the indirect costs of work-related MSK
disorders for both the affected worker and their immediate
social environment, including the recipient of caregiving,
other family and friends who may need to take over
caregiving services, and social agencies such as schools
and homecare services.
Our results address the myth surrounding findings
regarding the slower or less frequent return to work of
women, findings which, it is important to note, remain
inconsistent [Krause et al., 2001]. When studies have found
women returning to work at a slower rate than men, it has
784 Franche et al.
TABLE
II.CharacteristicsofCaregivingSample,StudyS
ample(RTWCohort,Ontario),andStudyP
opulation(WSIBClaim
ants,Ontario)
Varia
ble
Wom
enproviding
caregiving
(n¼43)
Men
providing
caregiving
(n¼43)
Totalcaregiving
sample
(n¼86)
Wom
eninstudy
sample
(n¼92)
Men
instudy
sample
(n¼95)
Totalstudy
sample
(n¼187)
Wom
en(population)
(n¼723)
Men
(population)
(n¼1166)
Total
population
(n¼1890)
Gender
Wom
en50%
49.2%
38.3%
Men
50%
50.8%
61.7%
Age 15^24
years
0%4.7%
2.3%
6.6%
8.7%
7.7%
10.0%
13.0%
11.4%
25^44
years
79.1%
62.8%
70.9%
54.9%
53.3%
54.1%
57.8%
58.8%
58.4%
45^65
years
20.9%
32.6%
26.7%
38.5%
38.0%
38.3%
32.1%
28.0%
29.6%
Typeofcareprovided
None
0%0%
0%52.7%
53.3%
53.0%
Tochildonly
76.6%
72.1%
74.4%
36.3%
33.7%
35.0%
Tofamilymem
berorfriend
only
14.0%
18.6%
16.3%
6.6%
8.7%
7.7%
Tobothchildandother
9.3%
9.3%
9.3%
4.4%
4.3%
4.4%
Numberofdependentchildren
None
11.5%
25.6%
18.6%
54.9%
65.2%
60.1%
One
32.6%
16.3%
24.4%
18.7%
7.6%
13.1%
Two
44.2%
41.9%
43.0%
20.9%
19.6%
20.2%
Threeorm
ore
11.6%
16.3%
13.5%
5.5%
7.6%
6.5%
Siteofinjury
Back
74.4%
81.4%
77.9%
72.5%
74.7%
73.6%
71.0%
76.7%
74.4%
Upperextremity
a18.6%
11.6%
15.1%
23.1%
20.9%
22.0%
21.7%
19.3%
20.3%
Neck
7.0%
7.0%
7.0%
4.4%
4.4%
4.4%
7.1%
3.9%
5.1%
Personalincome
<$20,000
27.9%
7.0%
17.4%
28.6%
14.1%
21.3%
$20,000^
39,999
60.5%
39.5%
50.0%
52.7%
39.1%
45.9%
$40,000^
59,999
7.0%
37.2%
22.1%
11.0%
33.7%
22.4%
>$60,000
2.3%
16.3%
9.3%
4.4%
10.9%
7.7%
Missing
2.3%
0%1.2%
3.3%
2.2%
2.7%
Familyincome
<$40,000
32.6%
30.2%
31.4%
31.9%
30.4%
31.1%
$40,000^
$59,9
9927.9%
27.9%
27.9%
23.1%
25.0%
24.0%
$60,000^
$79,999
25.6%
20.9%
23.3%
24.2%
26.1%
25.1%
>$80,000
11.6%
20.9%
16.3%
14.3%
16.3%
15.3%
Missing
2.3%
0%2.3%
6.6%
2.2%
4.4%
785
(Continued)
786
TABLE
II.(Continued)
Varia
ble
Wom
enproviding
caregiving
(n¼43)
Men
providing
caregiving
(n¼43)
Totalcaregiving
sample
(n¼86)
Wom
eninstudy
sample
(n¼92)
Men
instudy
sample
(n¼95)
Totalstudy
sample
(n¼187)
Wom
en(population)
(n¼723)
Men
(population)
(n¼1166)
Total
population
(n¼1890)
Educationlevel
Somehighschool
16.3%
16.3%
16.3%
15.4%
16.3%
15.8%
Highschoolcompleted
37.2%
34.9%
36.0%
30.8%
34.8%
32.8%
Universityorcollege
completed
16.3%
11.6%
14.0%
19.8%
12.0%
15.8%
Missing
30.2%
37.2%
33.7%
34.1%
37.0%
35.5%
Maritalstatus
Marriedorcommon-law
69.8%
78.6%
74.4%
68.1%
70.6%
69.4%
Single
7.0%
14.0%
10.5%
13.2%
21.7%
17.5%
Separated/divorced
23.3%
7.0%
15.1%
15.4%
7.6%
11.5%
Widowed
0%0%
0%3.3%
0%1.6%
Self-reportedworkstatus
Workingattim
eofinterview
65.1%
69.8%
67.4%
73.6%
58.7%
66.1%
Notworkingattim
eof
interview
34.9%
30.3%
32.5%
26.4%
41.3%
33.9%
Timeonbenefits
Offbenefits7months
afterinjury
81.4%
76.8%
79.1%
87.0%
77.8%
82.3%
92.4%
91.3%
91.7%
Onbenefits7
months
afterinjury
11.6%
18.6%
15.1%
8.6%
15.9%
12.3%
7.6%
8.7%
8.3%
Missingconsentforlinkage
7.0%
4.7%
5.8%
4.4%
6.3%
5.3%
Employmentclassification
Whitecollar
30.2%
4.7%
17.4%
31.9%
4.3%
18.0%
29.6%
4.1%
13.9%
Pinkcollar
44.2%
20.9%
32.6%
45.1%
18.5%
31.7%
44.3%
19.3%
28.9%
Bluecollar
16.3%
65.1%
40.7%
17.6%
67.4%
42.6%
19.6%
63.7%
46.8%
Missing
9.3%
9.3%
9.3%
5.5%
9.8%
7.7%
6.5%
12.9%
10.4%
Numberofemployeesat
worksiteattim
eofinjury
(selfreport)
<20
employees
18.6%
34.9%
26.7%
23.1%
33.7%
28.4%
20^99
employees
46.5%
41.9%
44.2%
38.5%
35.9%
37.2%
>100em
ployees
34.9%
23.3%
29.0%
38.5%
30.4%
34.4%
been suggested that they may do so in order to attend to the
needs of their children, or to other family members requiring
their help [Clarke et al., 1999]. The results of our study
dispute such an interpretation for both sexes. Indeed, both
men and women who had not returned to work at the time of
the interview reported significantly greater decreases in
caregiving hours following their injury, as compared to
workers who had returned to work. Our findings suggest that
the injury experience of these individuals involves limita-
tions in both their occupational and caregiving roles, and
possibly in other areas.
Women reported significantly greater reductions in
caregiving hours than men, even after accounting for general
differences in the overall amount of time spent caregiving. A
recent review of gender differences in caregivers suggests
that female caregivers are more involved in care provision
tasks than male caregivers: Women engage in more
caregiving tasks involving hands-on, day-to-day activities
such as personal care and household tasks than men [Yee and
Schulz, 2000]. Given the more physical nature of care
provision tasks, as opposed to care management tasks, it is
possible that the greater decrease in caregiving hours
observed in female injured workers is related to the more
physically challenging nature of their caregiving activities.
In addition, it is also possible that the nature of women’s work
differs from men’s in our sample, and that they have
occupations to which it is more difficult to return to, due to
higher physical demands or to psychosocial factors.
It should be noted that among caregiving women, a
surprisingly high number of them (23.3%) were separated or
divorced, as compared to 7% of caregiving men. Although
statistically non-significant (w2¼ 5.02, P¼ 0.08), this
higher prevalence of separated or divorced women as
opposed to men in our sample is perplexing. It may reflect
a sampling bias which could not be directly assessed as
WSIB claim files do not capture marital status. It could also
reflect a naturally occurring higher likelihood for working
separated/divorced women to maintain caregiving responsi-
bilities, as opposed to men. Finally, it is also possible that
women who are separated or divorced and who also
provide caregiving are more likely than married caregiving
men to (1) become injured at work and/or (2) to make a lost-
time claim. The demands of caregiving, combined with a
lower level of social support and poorer health typically
associated with their marital status [Orth-Gomer and
Johnson, 1987; Kawachi et al., 1996], may render them
more vulnerable to work-related MSK disorders through a
variety of pathways such as the indirect physiological
mediation of the impact of increased psychological stress
[Cassel, 1976; Melzack, 1999]. The design of our study does
not permit to reach any conclusions regarding this point.
Only a prospective study of a working population, with the
time of inception prior to injury, could inform us regarding
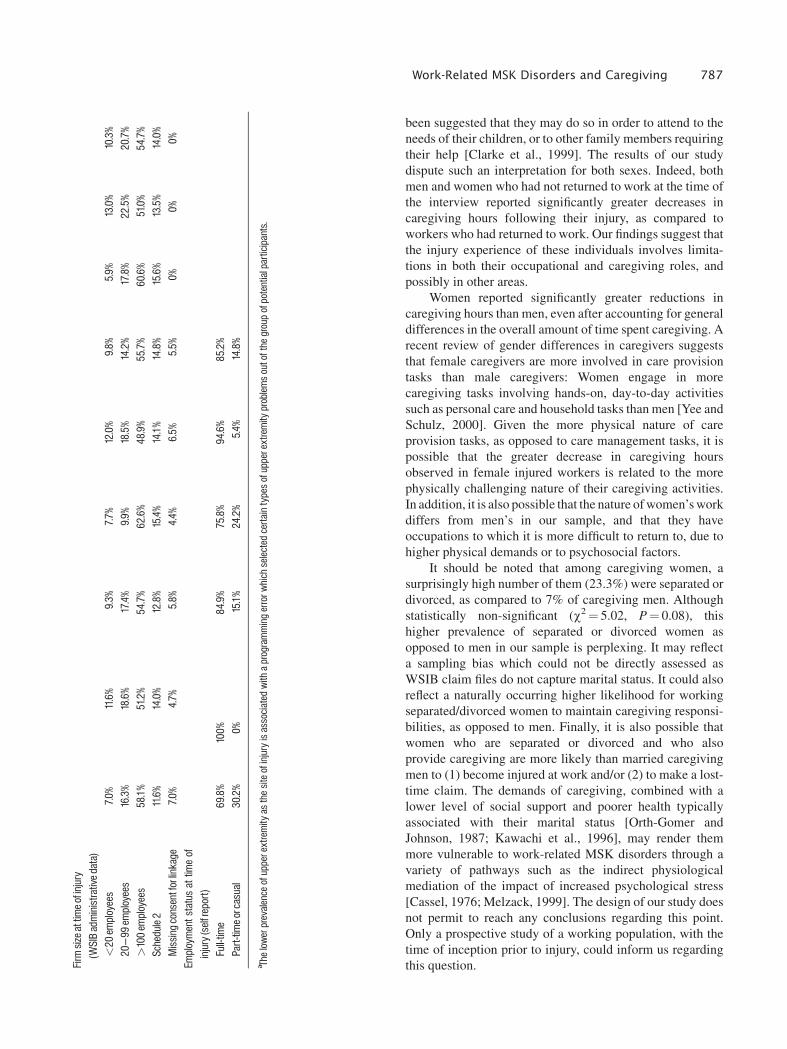
this question.Firm
sizeattimeofinjury
(WSIBadministrativedata)
<20
employees
7.0%
11.6%
9.3%
7.7%
12.0%
9.8%
5.9%
13.0%
10.3%
20^99
employees
16.3%
18.6%
17.4%
9.9%
18.5%
14.2%
17.8%
22.5%
20.7%
>100em
ployees
58.1%
51.2%
54.7%
62.6%
48.9%
55.7%
60.6%
51.0%
54.7%
Schedule2
11.6%
14.0%
12.8%
15.4%
14.1%
14.8%
15.6%
13.5%
14.0%
Missingconsentforlinkage
7.0%
4.7%
5.8%
4.4%
6.5%
5.5%
0%0%
0%Em
ploymentstatusattim
eof
injury(selfreport)
Full-tim
e69.8%
100%
84.9%
75.8%
94.6%
85.2%
Part-tim
eorcasual
30.2%
0%15.1%
24.2%
5.4%
14.8%
a Thelowerprevalenceofupperextremity
asthesiteofinjuryisassociated
with
aprogrammingerrorw
hichselectedcertaintypesofupperextremity
problem
soutofthe
groupofpotentialparticipants.
Work-Related MSK Disorders and Caregiving 787
Strengths and Limitations of the Study
In terms of sample characteristics, the study’s sample
size was small which precluded investigating finer differ-
ences, and which suggests the need for replication of results.
Due to this small sample size, it was not possible to address
differences between workers providing caregiving to chil-
dren, other adults, or both. However, the study sample was
comparable to the study population of lost-time claimants
with upper extremity, neck and back MSK disorders, in terms
of site of injury, employment classification, and firm size.
These similarities between our study sample and the study
population increase confidence in the generalizability of the
findings. Differences were found between the study sample
and study population in that participants were more likely to
be women and older. Men in the study sample were more
likely to be receiving compensation 8 months post-injury
than in the study population. Similar differences between
participants and non-participants have been reported in
previous studies regarding sex, age [Keogh et al., 2000], and,
in the case of participation to follow-up assessments,
compensation status [Sinclair et al., 1997]. As such, they
reflect common participation biases. Their presence, how-
ever, warrants caution regarding the generalizability to
younger and male claimants as well as to male claimants
who have returned to work within 8 months post injury.
One strength of the study was its careful assessment and
control of potential confounding variables. As well, the
biasing effect of the magnitude of reported caregiving hours
on the test of pre-post differences was addressed by including
the mean of pre- and post-caregiving hours as a covariate in
our analyses. In terms of measurement issues, limitations
include the absence of measurement of functional status
which would have allowed to examine directly its impact on
caregiving activities. Furthermore, a more detailed measure
of caregiving activities would have allowed to provide
information not only on the time given to caregiving
activities, but also on the type of caregiving offered, such
as instrumental activities and personal care [Cranswick,
1997].
The retrospective nature of the respondents’ self-reports
of caregiving hours leaves open the possibility that their pre-
injury levels of caregiving hours were inflated. The average
number of caregiving hours to family or friend reported in our
sample (mean¼ 7.00 for women; mean¼ 4.00 for men) is
higher than the one reported by Canadian caregivers
employed full-time (mean¼ 4.20 for women; mean¼ 2.60
for men) [Cranswick, 1997] but lower than the one reported
by American employed and non-employed caregivers
(mean¼ 17.9) [National Alliance for Caregiving & Amer-
ican Association of Retired Persons, 1997]. Regarding time
devoted to child care activities, the time reported by the
participants in our sample who were parents (mean¼ 32.26,
SD¼ 16.05 for women; mean¼ 18.22, SD¼ 12.45 for men)
is within the range reported by Canadian parents working
full-time. Canadian men working full-time report mean
weekly hours devoted to child care activities ranging from
18.9 hr for fathers of children between 13 and 14 years old to
30.1 hr for fathers of children between 0 and 4 years old
[Silver, 2000]. For Canadian women working full-time, they
TABLE III. 2-WayANCOVAwith Difference in Caregiving Hours asDependentVariable, Sex and RTWStatus as Between-Subject Factors,and Average of Pre- and Post-Injury Caregiving Hours,Comorbidity,Site of Injury, and Education as Covariates
SourceType IIISumof Squares df F P
Sex 716.64 1 7.05 0.01RTWstatus 743.55 1 7.32 0.01SexXRTWstatus 257.29 1 2.53 0.12Average pre- & post-injurycaregivinghours
2.46 1 0.02 0.88
Comorbidity 298.98 1 2.83 0.10Site of injury 11467 1 1.13 0.29Education 45.93 1 0.45 0.50Total 10,122.95 85
TABLE IV. Means and 95%Confidence Intervals ofWeekly Caregiving Hours Before and After Injury
Sex RTW nMean difference in hours(before ^ after injury) C.I.
Mean hoursbefore injury C.I.
Mean hoursafter injury C.I.
Women RTW 28 4.75 (1.80, 7.70) 27.50 (19.70, 35.30) 22.75 (14.76, 30.74)NoRTW 15 14.87 (7.27, 22.46) 30.80 (22.23, 39.27) 15.93 (7.53, 24.34)Total 43 8.28 (4.86,11.70) 28.65 (22.97, 34.33) 20.37 (14.53, 26.22)
Men RTW 30 2.03 (1.36, 5.43) 18.18 (12.93, 23.43) 16.15 (11.42, 20.88)NoRTW 13 4.46 (3.00,11.92) 16.27 (8.21, 24.33) 11.81 (3.18, 20.44)Total 43 2.77 (0.34, 5.87) 17.60 (13.38, 21.83) 14.84 (10.79,18.88)
Total RTW 58 3.34 (1.13, 5.56) 22.68 (18.02, 27.34) 19.34 (14.83, 23.84)NoRTW 28 10.04 (4.65,15.42) 24.05 (17.86, 30.24) 14.02 (8.34,19.70)Total 86 5.52 (3.18, 7.86) 23.13 (19.46, 26.79) 17.60 (14.07, 21.14)
788 Franche et al.

report mean weekly hours devoted to child care
activities ranging from 18.2 hr for mothers of children
between 13 and 14 years old to 44.8 hr for mothers of children
between 0 to 4 years old [Silver, 2000]. Taken together,
these comparisons suggest that the retrospective nature of the
respondent’s self-report of caregiving hours was within the
expected range.
CONCLUSIONS
To our knowledge, our study represents the first one
addressing and quantifying the impact of work-related MSK
disorders on workers’ time spent in caregiving activities for
both children and family or friends. When considered in
conjunction with previous literature on work disability
following a work-related injury, our findings support the
view that such injuries impact on both occupational and
caregiving activities in a parallel fashion—activities in both
types of life domains are significantly limited by a work-
related injury. Future research should focus on understanding
the pathways of such limitations, as the contribution of
functional status, physical health, and mental health status
have not been investigated with regards to caregiving and
other non-occupational activities. Our findings suggest the
presence of sex differences in caregiving activities of injured
workers, which should be examined with studies of larger
sample sizes. Finally, differences between caregivers for
children and those offering care to adult family and friends
should be investigated.
Working men and women providing caregiving are a
growing proportion of the labor force. The current study
points to the necessity to address the needs of these workers
and of their immediate social environment, when they suffer
a work-related injury.
ACKNOWLEDGMENTS
We thank the staff at the Workplace Safety & Insurance
Board of Ontario for their assistance in the project, as well
as Ms. Alysha Williams for her assistance in providing
statistics regarding time use of Canadian and American
workers.
REFERENCES
Association of Workers’ Compensation of Canada. 2002. Workers’compensation occupational disease and occupational stress legislationand policies-2002. Mississauga: Association of Workers’ Compensa-tion Boards of Canada (AWCBC).
Bland JM, Altman DG. 1995. Comparing methods of measurement:Why plotting difference against standard method is misleading. Lancet346:1085–1087.
Bond JT, Galinsky E, Swanberg JE. 1998. The 1997 Nationalstudy of the Changing Workforce. U.S.: Families and Work Institute.
Bureau of Labor Statistics. 2003. Lost-worktime injuries and illnesses:Characteristics and resulting days away from work, 2001. Washington,DC: Bureau of Labor Statistics.
Cassel J. 1976. The contribution of the social environment to hostresistance. Am J Epidemiol 104:107–114.
Clarke J, Chung J, Cole DC, Hogg-Johnson S, Haidar H, ECC PrognosisModelling Group. 1999. Working Paper #85. Gender and benefitduration in lost time work-related soft tissue disorders: Relationshipswith work and social factors. Toronto, Canada: Institute for Work &Health.
Cranswick K. 1997. Canada’s Caregivers. Can Soc Trends 47:2–6.
Cote P. 1996. The prevalence and determinants of chronic neck pain inthe Saskatchewan adult population. Master of Science Dissertation,University of Saskatchewan.
Cote P, Baldwin ML, Johnson WG. 2003. Working Paper #205. Earlypatterns of care for occupational back pain. Toronto, Canada: Institutefor Work & Health.
Dasinger LK, Krause N, Deegan LJ, Brand RJ, Rudolph L. 1999.Duration of work disability after low back injury: A comparison ofadministrative and self-reported outcomes. Am J Ind Med 35:619–631.
Dembe AE. 2001. The social consequences of occupational injuries andillnesses. Am J Ind Med 40:403–417.
Duxbury L, Higgins C. 2001. Work-life balance in the new millenium:Where are we? Where do we need to go? Report No. W 12. Ottawa:Canadian Policy Research Networks.
Gaudette LA, Richardson A, Huang S. 2003. Which workers smoke?Health Rep 10:35–45.
Jaroszynski G, Cassidy JD, Cote P, Carroll L, Zeber J, Yong-Hing K.1996. Development, reliability and concurrent validity of a new self-assessed co-morbidity scale. Personal communication.
Kawachi I, Colditz GA, Ascherio A, Rimm EB, Giovannucci E,Stampfer MJ, Willett WC. 1996. A prospective study of social networksin relation to total mortality and cardiovascular disease in men in theUSA. J Epidemiol Community Health 50:245–251.
Keogh JP, Nuwayhid I, Gordon JL, Gucer P. 2000. The impact ofoccupational injury on injured worker and family: Outcomes of upperextremity cumulative trauma disorders in Maryland workers. Am J IndMed 38:498–506.
Kramer BJ, Kipnis S. 1995. Eldercare and work-role conflict: Toward anunderstanding of gender differences in caregiver burden. Gerontologist35:340–348.
Krause N, Frank JW, Dasinger LK, Sullivan T, Sinclair SJ. 2001.Determinants of duration of disability and return to work after work-related injury and illness: Challenges for future research. Am J Ind Med40:464–484.
Melzack R. 1999. Pain and Stress: A New Perspective. In: Gatchel RJ,Turk DC, editors. Psychological Factors in Pain. Critical Perspectives.New York: The Guilford Press, p 89–106.
Morse TF, Dillon C, Warren N, Levenstein C, Warren A. 1998. Theeconomic and social consequences of work-related musculoskeletaldisorders: The Connecticut upper-extremity surveillance project(CUSP). Int J Occup Environ Health 4:209–216.
National Alliance for Caregiving & American Association of RetiredPersons. 1997. Family caregiving in the U.S. - Findings from a NationalSurvey Report No. Final Report U.S.
Orth-Gomer K, Johnson JV. 1987. Social network interaction andmortality. A six year follow-up study of a random sample of the Swedishpopulation. J Chronic Dis 40:949–957.
Pransky G, Feuerstein M, Himmelstein J, Katz JN, Vickers-Lahti M.1997. Measuring functional outcomes in work-related upper extremity
Work-Related MSK Disorders and Caregiving 789

disorders. Development and validation of the Upper Extremity FunctionScale. J Occup Environ Med 39:1195– 1202.
Silver C. 2000. Being there: The time dual-earner couples spend withtheir children. Can Soc Trends 57:26–29.
Sinclair SJ, Hogg-Johnson SA, Mondloch MV, Shields SA. 1997. Theeffectiveness of an early active intervention program for workers withsoft tissue injuries: the Early Claimant Cohort study. Spine 22:2919–2931.
Wagner DL. 1997. Comparative analysis of caregiver data for caregiversto the elderly 1987 and 1997 U.S.
Workplace Safety & Insurance Board. 2002. Coverage under theOntario Workplace Safety and Insurance Act. 1–10. Toronto, Ontario,Canada.
Yee JL, Schulz R. 2000. Gender differences in psychiatric morbidityamong family caregivers: A review and analysis. Gerontologist 40:147–164.
790 Franche et al.