Embed Size (px)
Citation preview
The Journal of Pain, Vol 13, No 2 (February), 2012: pp 131-138Available online at www.sciencedirect.com
The Interruptive Effect of Pain in a Multitask Environment: An
Experimental Investigation
Dimitri M. L. Van Ryckeghem,* Geert Crombez,* Christopher Eccleston,y
Baptist Liefooghe,* and Stefaan Van Damme**Department of Experimental-Clinical and Health Psychology, Ghent University, Ghent, Belgium.yCentre for Pain Research, The University of Bath, Bath, United Kingdom.
Received2011.Preparat001 of GThere areAddressExperimeDunantlaugent.be
1526-590
ª 2012 b
doi:10.10
Abstract: Daily life is characterized by the need to stop, start, repeat, and switch between multiple
tasks. Here, we experimentally investigate the effects of pain, and its anticipation, in a multitask en-
vironment. Using a task-switching paradigm, participants repeated and switched between 3 tasks, of
which 1 predicted the possible occurrence of pain. Half of the participants received low intensity pain
(N = 30), and half high intensity pain (N = 30). Results showed that pain interferes with the perfor-
mance of a simultaneous task, independent of the pain intensity. Furthermore, pain interferes with
the performance on a subsequent task. These effects are stronger with high intensity pain than
with low intensity pain. Finally, and of particular importance in this study, interference of pain on
a subsequent task was larger when participants switched to another task than when participants re-
peated the same task.
Perspective: This article is concerned with the interruptive effect of pain on people’s task perfor-
mance by using an adapted task-switching paradigm. This adapted paradigm may offer unique pos-
sibilities to investigate how pain interferes with task performance while people repeat and switch
between multiple tasks in a multitask environment.
ª 2012 by the American Pain Society
Key words: Pain, task switching, task interference, attention, pain anticipation.
Akey component of successful goal-directed
behavior in natural environments is the abilityto switch attention flexibly between multiple de-
mands, by preparing and protecting relevant actionsfrom irrelevant actions. While we usually experiencesuch switches as relatively effortless,42 a different pictureemerges in the context of pain. Most often, attention isprioritized towards pain, which interrupts the smoothrunning of goal-directed behavior.19,28
Performance on a cognitive task is known to be hinderedby the simultaneous presence of pain2,8,12-15,18,25,33,43
but also see32,37,45 or pain-related information (eg,pain words).31,34 This interference effect is especiallypronounced when pain is intense, novel, unpredictable,
May 29, 2011; Revised August 22, 2011; Accepted September 15,
ion of this paper was partly supported by Grant BOF/GOA2006/hent University and FWO project G.017807.no conflicts of interest thatmay arise as a result of this research.
reprint requests to Dimitri M. L. Van Ryckeghem, Department ofntal-Clinical and Health Psychology, Ghent University, Henrian 2, B-9000 Ghent, Belgium. E-mail: Dimitri.VanRyckeghem@
0/$36.00
y the American Pain Society
16/j.jpain.2011.09.003
or threatening.11,19,24,27 To date, the interference effectof pain has only been investigated in a unitary taskenvironment in which attention is directed toward oraway from a primary task. Largely unexplored is theeffect of pain in a multitask environment. Oneexception is the study of Eccleston17 in which chronicpain patients were required to switch attention betweendifferent tasks. Results of this study show that patientswith pain of high intensity were particularly impairedwhen they were instructed to switch between 2 tasks. Itremainsunclearhowexactlypain interfereswith taskper-formance in such a multitask environment. More system-atic research about the effects of pain on behavior ina multitask environment is necessary insofar as it offersunique possibilities to investigate how people performmultiple tasks despite pain.26 This line of research mayfurther help identify the cognitive processes underlyingmemory and attentional problems often reported bypatients with chronic pain.16,21
Here, we adapted a standard task-switching procedurein which healthy volunteers are cued to repeat or toswitch between 3 randomly presented tasks (see Kieselet al25 and Vandierendonck et al42 for a review). Oneof the tasks sometimes co-occurred with pain and thusbecame a signal for possible pain. Half of the participants
131

132 The Journal of Pain Pain in a Multitask Environment
experienced high intensity pain, the other half lowintensity pain. This study investigates 2 main questions.First, we ask whether pain, or its anticipation, immedi-ately interfere with task performance (immediate inter-ference effect). This is in line with previous literatureon task interruption by pain.5,38 However, thus farunexplored is the role of pain intensity on thisinterruptive effect. A second question is whether pain,or its anticipation during a task, also interferes withperformance on a subsequent task (prolongedinterference effect). Because switching requires greatercognitive effort in order to prepare the relevant task,42
and pain is especially known to interfere with high cog-nitive demand,40 a larger prolonged interference effectis predicted when switching between tasks than whenrepeating the same task. The prolonged interference ef-fect is also expected to be larger in a context of highcompared with low pain intensity.
Methods
ParticipantsSixty undergraduate students (48 females, Mage
= 18.95 years, SD = 2.63; 59 Caucasian) from Ghent Uni-versity participated for course credits. The majority re-ported good medical and psychological health(96.67%). Exclusion criteria included a self-reported cur-rent pain condition (eg, dental pain, fibromyalgia, backpain) or a self-reported current psychiatric condition,(eg, psychoses, anxiety disorders). We decided that par-ticipants would also be excluded from further analysesif they made errors on more than 20% of the trials.14
However, no participants were excluded for these rea-sons. The experiment, including all instructions and stim-ulus materials, was undertaken in Dutch, and allparticipants were therefore required to have Dutch asa first language. All participants provided written in-formed consent andwere fully debriefed after the exper-iment. The experiment was approved by the ethicalcommittee of the Faculty of Psychology and EducationalSciences of Ghent University.
ApparatusThe experiment was programmed and presented by
the INQUISITMillisecond (Seattle,WA) software package(Inquisit v.2.06, 2008) on an Excel computer (Pentium 4,2.8 GHz, 512 MB) with a 60-Hz, 17-inch color monitor.The viewing distance was approximately 60 cm.Pain stimuli were delivered by a constant current stim-
ulator (Digitimer DS7A: Digitimer Ltd, Hertfordshire, UK)with an internal frequency of 50 Hz for duration of 300ms. A train of square wave asymmetric 2-ms pulses (36pulses; 6 ms interpulse interval) was used. Pain stimuliwere delivered at the median nerve on the wrist of theright arm. The skin area of the electrode sites was firstrubbed with peeling gel (Nihon Kohden) to reduce skinresistance (similar as Van Ryckeghem et al44).
Task-Switching ParadigmWeemployed a task-cuing procedure, inwhich trials of
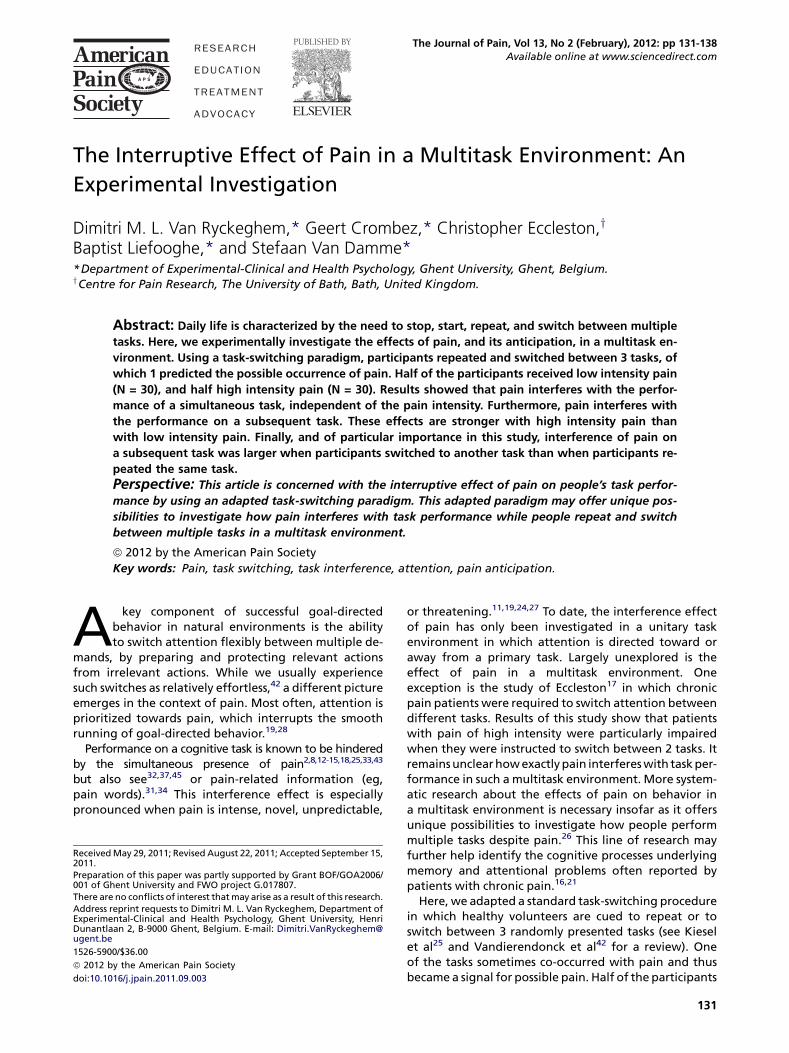
3 randomly presented reaction-time tasks are performed.In a first ‘‘shape’’ task, participants were instructed to de-cide whether a target stimulus was a square or triangle.In a second ‘‘color’’ task, participants were instructed todecide whether the target stimulus consisted of a palegrey or dark grey color. In a third ‘‘orientation’’ task, par-ticipants were instructed to decide whether the targetstimulus was vertically or diagonally oriented.Fig 1 depicts an example of a trial. Each trial started
with a cue indicating the task to be performed. Thecues were the words ‘‘shape,’’ ‘‘color,’’ or ‘‘orientation’’presented in white courier-new font size 19. After 500ms, the task cue was replaced by a black screen for 500ms, afterwhich the target stimuluswas presented. Targetstimuli varied across 3 features: color (pale grey or darkgrey), shape (triangle or square), and orientation (verti-cal or diagonal), resulting in 8 different target stimuli.Each target stimulus was 34 � 34 mm in size. The targetstimulus remained on the screen until participantsmade a response or 7,000 ms elapsed.Participants responded to the target stimulus by
speaking aloud the particular shape (‘‘square’’ or ‘‘trian-gle’’), color (‘‘pale’’ or ‘‘dark’’), or orientation (‘‘vertical’’or ‘‘diagonal’’). Response latencies were recorded bya voice key (REACSYS R-51). Response errors were en-coded by the experimenter on a trial-to-trial basis. Fivehundred milliseconds after the response, a new trialstarted. For 1 of 3 tasks—the pain-related task—the tar-get onset sometimes co-occurred with an electrocutane-ous stimulus (ECS). The task associated with the ECS wascounterbalanced over participants.
Procedure
Preparation Phase
Participants were individually tested in a dimly litroom. Half of the participants were randomly assignedto a low pain intensity group (N = 30; 29 females; Mage
= 18.77; SD = 1.96), the other half to a high pain intensitygroup (N = 30; 19 females; Mage = 19.13; SD = 3.18). Aftergiving informed consent, participants were familiarizedwith the ECS. In the low pain intensity group, partici-pants were given 3 ECS (same stimulus parameters, ex-cept for its intensity: .5, .75, and 1 mA). Participantswere then informed that the last stimulus of 1 mAwouldbe used in the experiment proper. In previous researchthis stimulus has been shown to be slightly painful.44 Inthe high pain intensity group, a series of ECS (same stim-ulus parameters, except for its intensity) was assessed, inwhich the intensity increased stepwise until participant’stolerance levelwas reached (.5, 0.75, 1, 1.25, 1.50mA,.).Participants were asked to proceed with the toleranceprocedure until they found that the pain level reachedthe maximum they could tolerate. Mean stimulus inten-sity of the ECS in the high pain intensity group was 3.98mA. Participants were informed that the stimulus at tol-erance level would be used in the experiment proper. Inboth the low and high pain intensity group, the last pain
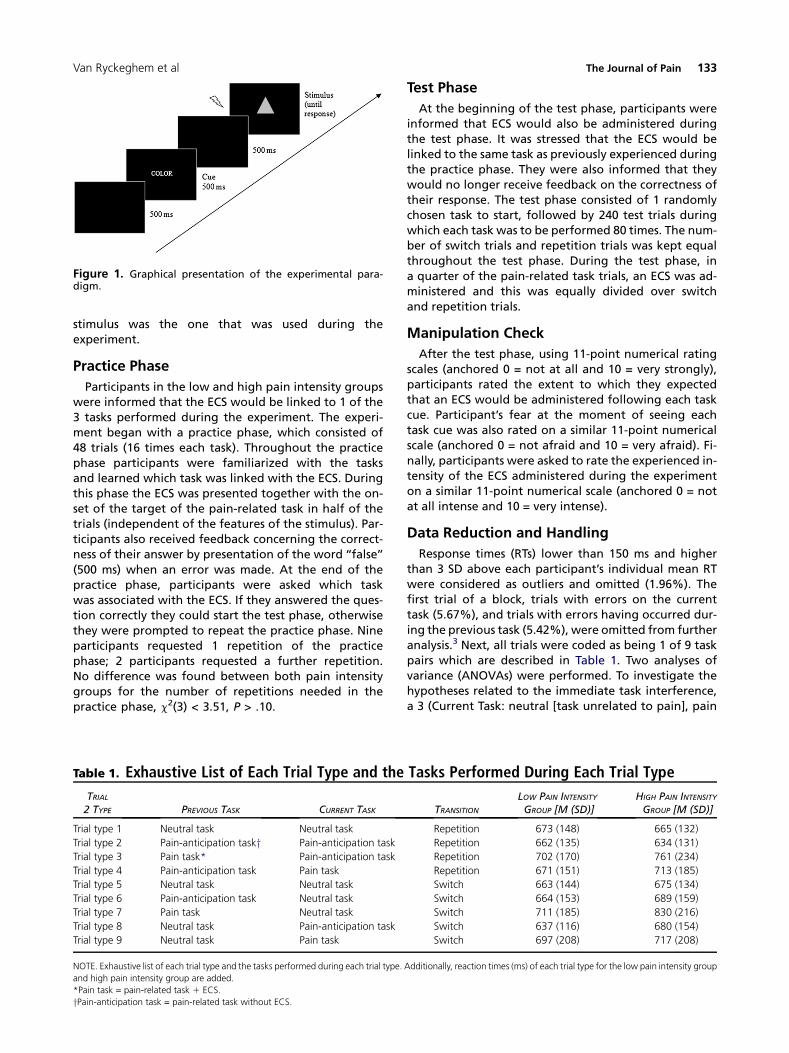
Figure 1. Graphical presentation of the experimental para-digm.
Van Ryckeghem et al The Journal of Pain 133
stimulus was the one that was used during theexperiment.
Practice Phase
Participants in the low and high pain intensity groupswere informed that the ECS would be linked to 1 of the3 tasks performed during the experiment. The experi-ment began with a practice phase, which consisted of48 trials (16 times each task). Throughout the practicephase participants were familiarized with the tasksand learned which task was linked with the ECS. Duringthis phase the ECS was presented together with the on-set of the target of the pain-related task in half of thetrials (independent of the features of the stimulus). Par-ticipants also received feedback concerning the correct-ness of their answer by presentation of the word ‘‘false’’(500 ms) when an error was made. At the end of thepractice phase, participants were asked which taskwas associated with the ECS. If they answered the ques-tion correctly they could start the test phase, otherwisethey were prompted to repeat the practice phase. Nineparticipants requested 1 repetition of the practicephase; 2 participants requested a further repetition.No difference was found between both pain intensitygroups for the number of repetitions needed in thepractice phase, c2(3) < 3.51, P > .10.
Table 1. Exhaustive List of Each Trial Type and the
TRIAL2 TYPE PREVIOUS TASK CURRENT TASK
Trial type 1 Neutral task Neutral task
Trial type 2 Pain-anticipation tasky Pain-anticipation task
Trial type 3 Pain task* Pain-anticipation task
Trial type 4 Pain-anticipation task Pain task
Trial type 5 Neutral task Neutral task
Trial type 6 Pain-anticipation task Neutral task
Trial type 7 Pain task Neutral task
Trial type 8 Neutral task Pain-anticipation task
Trial type 9 Neutral task Pain task
NOTE. Exhaustive list of each trial type and the tasks performed during each trial type.
and high pain intensity group are added.
*Pain task = pain-related task 1 ECS.
yPain-anticipation task = pain-related task without ECS.
Test Phase
At the beginning of the test phase, participants wereinformed that ECS would also be administered duringthe test phase. It was stressed that the ECS would belinked to the same task as previously experienced duringthe practice phase. They were also informed that theywould no longer receive feedback on the correctness oftheir response. The test phase consisted of 1 randomlychosen task to start, followed by 240 test trials duringwhich each task was to be performed 80 times. The num-ber of switch trials and repetition trials was kept equalthroughout the test phase. During the test phase, ina quarter of the pain-related task trials, an ECS was ad-ministered and this was equally divided over switchand repetition trials.
Manipulation Check
After the test phase, using 11-point numerical ratingscales (anchored 0 = not at all and 10 = very strongly),participants rated the extent to which they expectedthat an ECS would be administered following each taskcue. Participant’s fear at the moment of seeing eachtask cue was also rated on a similar 11-point numericalscale (anchored 0 = not afraid and 10 = very afraid). Fi-nally, participants were asked to rate the experienced in-tensity of the ECS administered during the experimenton a similar 11-point numerical scale (anchored 0 = notat all intense and 10 = very intense).
Data Reduction and Handling
Response times (RTs) lower than 150 ms and higherthan 3 SD above each participant’s individual mean RTwere considered as outliers and omitted (1.96%). Thefirst trial of a block, trials with errors on the currenttask (5.67%), and trials with errors having occurred dur-ing the previous task (5.42%), were omitted from furtheranalysis.3 Next, all trials were coded as being 1 of 9 taskpairs which are described in Table 1. Two analyses ofvariance (ANOVAs) were performed. To investigate thehypotheses related to the immediate task interference,a 3 (Current Task: neutral [task unrelated to pain], pain
Tasks Performed During Each Trial Type
TRANSITION
LOW PAIN INTENSITYGROUP [M (SD)]
HIGH PAIN INTENSITYGROUP [M (SD)]
Repetition 673 (148) 665 (132)
Repetition 662 (135) 634 (131)
Repetition 702 (170) 761 (234)
Repetition 671 (151) 713 (185)
Switch 663 (144) 675 (134)
Switch 664 (153) 689 (159)
Switch 711 (185) 830 (216)
Switch 637 (116) 680 (154)
Switch 697 (208) 717 (208)
Additionally, reaction times (ms) of each trial type for the low pain intensity group

134 The Journal of Pain Pain in a Multitask Environment
anticipation [Task in which the ECS is expected but notdelivered], pain [Task in which the ECS is expected anddelivered]) � 2 (Pain Intensity Group: high, low) ANOVAwith repeated measures on the first factor was per-formed. For this ANOVA we selected only trials in whichthe preceding trial was neutral and in which the currenttask differed from the task on the preceding trial. In do-ing so, our results cannot be confounded by a possibleprolonged interference effect stemming from the dis-ruptive effects of pain or its anticipation on the preced-ing trial, or effects related to the difference betweenrepeating and switching tasks (see Vandierendoncket al42 for a review). Contrast analyses were planned tocompare trials in which the current task was neutralwith both other conditions separately. To investigatethe hypotheses related to the prolonged task interfer-ence effect, a 2 (Transition: repetition, switch)� 3 (Previ-ous Task: neutral, pain anticipation, pain) � 2 (PainIntensity Group: low, high) ANOVA with repeated mea-sures on the first 2 factors was performed. In this ANOVAwe selected both repetition and switch trials. Again,planned contrasts were conducted to compare trials inwhich the previous task was neutral with both other con-ditions separately. Effect sizes were measured with par-tial Eta-squared or, wherever possible, we calculatedeffect sizes for independent samples using the formulaproposed by Borenstein et al,6 and the 95% ConfidenceInterval (95% CI). We determined whether Cohen’sd was small (.20), medium (.50), or large (.80).10
Results
Participants’ CharacteristicsThere were no age differences between the low pain
intensity group and high pain intensity group (t(59) <1, P > .10). A c2-test showed no differences betweenboth groups as a function of health status (c2(3) < 1,P > .10) and socioeconomic status (c2(3) = 5.12, P > .10).A difference was found as a function of participants’gender (c2(1) = 10.41, P < .01). No differences howeverwere observed on the pain intensity rating and reactiontimes as a function of gender (All t’s < 1.63).
Manipulation CheckResults of the postexperimental numerical rating
scales indicated that the experimental manipulationwas successful. First, participants reported more fear ofthe cue of the pain-related task (M= 5.77, SD = 2.41) com-pared with the cues of both neutral tasks (M = 2.06, SD =2.17), t(59) = 10.55, P < .001, d = 1.61; 95% CI = 1.16: 2.09.Second, they expected to receive an ECS after a pain-related task cue (M = 7.08, SD = 2.13) more often than af-ter a neutral task cue (M= 1.78, SD = 1.89), t(59) = 13.56, P< .001, d = 2.63; 95% CI = 2.00: 3.26. Third, participants ofthe high pain intensity group (M = 6.50, SD = 2.01) ratedthe ECS they received during the experimental phase asmore intense than the participants allocated to the lowpain intensity group (M = 3.23, SD = 2.14), t(58) = 6.08, P <.001, d = 1.58; 95% CI = 1.00: 2.15.
Reaction Time Data
Immediate Task Interference
We hypothesized that pain or the anticipation of painwould immediately impair task performance, especiallywhen pain was highly intense. To test our hypothesesa 3 (Current Task: neutral, pain anticipation, pain) � 2(Pain Intensity Group: high, low) ANOVAwas performed.As predicted, the main effect of Current Task was signif-icant, F(2, 57) = 3.65, P < .05, hp
2 = .11. The main effect ofPain Intensity Group was not significant, F(1,58) < 1, d =.17; 95% CI = �.34: .68. The interaction between TrialType and Pain Intensity Group failed to reach signifi-cance, F(2, 57) < 1.17, hp
2 = .04. With regard to the signif-icant main effect of Current Task, planned contrastanalyses indicated that anticipation of pain during a cur-rent task did not hamper task performance comparedwith performance on a neutral task, F(1,58) < 1.01, d =.08; 95% CI = �.07: .23. But participants’ performancewas slower on a task when pain was experienced (M =707, SD = 207), compared with performance on a neutraltask (M = 669, SD = 138; F(1, 58) = 3.76, P = .06, d = .20;95% CI = .00: .40).
Prolonged Task Interference
We hypothesized that pain or the anticipation of painduring 1 taskwould interferewith performanceon a sub-sequent task, in particular when participants were re-quired to switch to another task and when pain was ofhigh intensity. In order to avoid confounding effects ofimmediate interference, trials in which pain was deliv-ered in the current task were excluded (trials in whichpain was merely anticipated in the current task werenot excluded, as previous analyses showed no immediateinterference effect in these trials). To test our hypothesesa 2 (Transition: repetition, switch) � 3 (Previous Task:neutral, pain anticipation, pain) � 2 (Pain IntensityGroup: low, high) ANOVA was performed. There wasa main effect of Previous Task, F(2,57) = 21.63, P < .001,hp
2 = .43. With regard to the significant main effect ofPrevious Task, planned contrast analyses indicated thatparticipants were significantly slower when the previoustask was painful (M = 751, SD = 194), than when the pre-vious task was neutral (M = 669, SD = 134; F(1,58) = 35.14,P < .001, d = .43; 95% CI = .27: .59). Participants’ perfor-mance however did not differ between when the previ-ous task was pain anticipating (M = 662, SD = 137) andwhen the previous task was neutral (M = 669, SD = 134;F(1,58) = 1.24, P > .10, d = .05; 95% CI = �.04: .14). Therewas also amain effect of Transition, F(1,58) = 5.88, P< .05,d = .14; 95% CI = .02: .27, showing that participants wereslower on switch trials (M = 705, SD = 156) than on repe-tition trials (M = 683, SD = 148). Next, the interaction be-tween Pain Intensity Group and Transition wassignificant, F(1,58) = 5.69, P < .05, d = .62; 95% CI = .10:1.13, indicating that the difference in RTs betweenswitch trials and repetition trials was significantly largerfor the high pain intensity group (M = 45, SD = 62) thanfor low pain intensity Group (M = 0, SD = 81). Further-more the interaction between Previous Task and Pain In-tensity Group, F(2,57) = 5.67, P < .01, hp
2 = .17, as well as
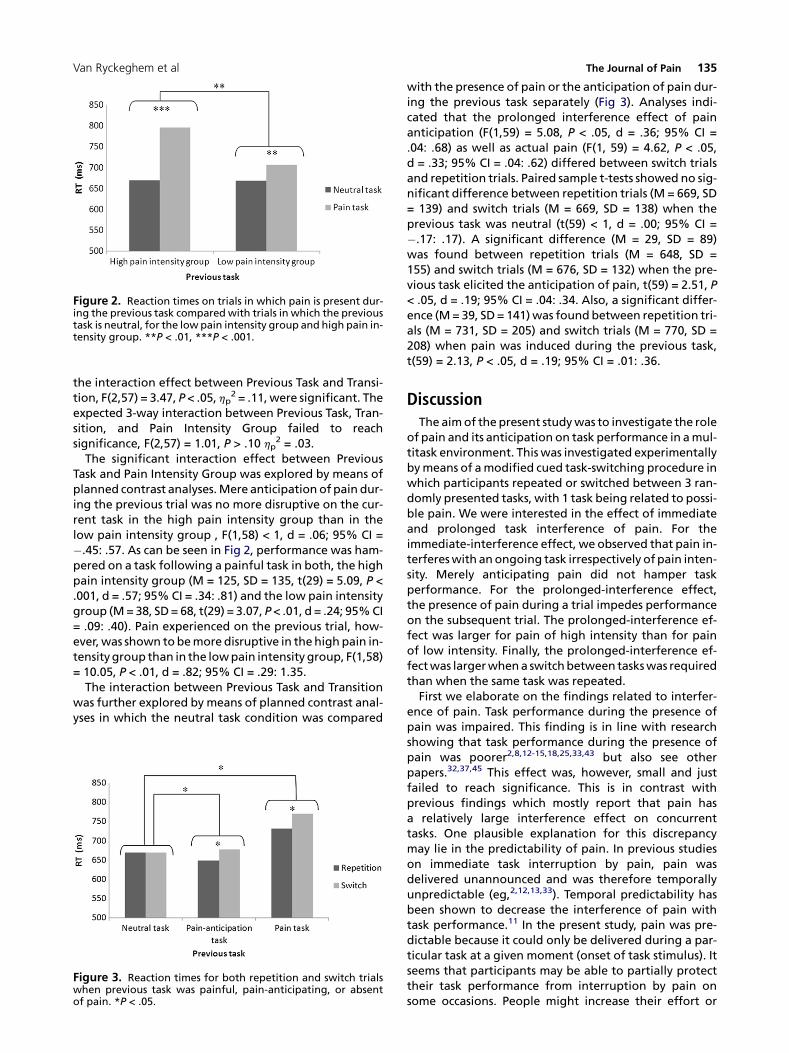
Figure 2. Reaction times on trials in which pain is present dur-ing the previous task comparedwith trials in which the previoustask is neutral, for the lowpain intensity group and high pain in-tensity group. **P < .01, ***P < .001.
Van Ryckeghem et al The Journal of Pain 135
the interaction effect between Previous Task and Transi-tion, F(2,57) = 3.47, P < .05, hp
2 = .11,were significant. Theexpected 3-way interaction between Previous Task, Tran-sition, and Pain Intensity Group failed to reachsignificance, F(2,57) = 1.01, P > .10 hp
2 = .03.The significant interaction effect between Previous
Task and Pain Intensity Group was explored by means ofplanned contrast analyses.Mere anticipation of pain dur-ing the previous trial was no more disruptive on the cur-rent task in the high pain intensity group than in thelow pain intensity group , F(1,58) < 1, d = .06; 95% CI =�.45: .57. As can be seen in Fig 2, performance was ham-pered on a task following a painful task in both, the highpain intensity group (M = 125, SD = 135, t(29) = 5.09, P <.001, d = .57; 95% CI = .34: .81) and the low pain intensitygroup (M=38, SD= 68, t(29) = 3.07, P< .01, d = .24; 95%CI= .09: .40). Pain experienced on the previous trial, how-ever,was shown tobemore disruptive in thehigh pain in-tensitygroup than in the lowpain intensity group, F(1,58)= 10.05, P < .01, d = .82; 95% CI = .29: 1.35.The interaction between Previous Task and Transition
was further explored by means of planned contrast anal-yses in which the neutral task condition was compared
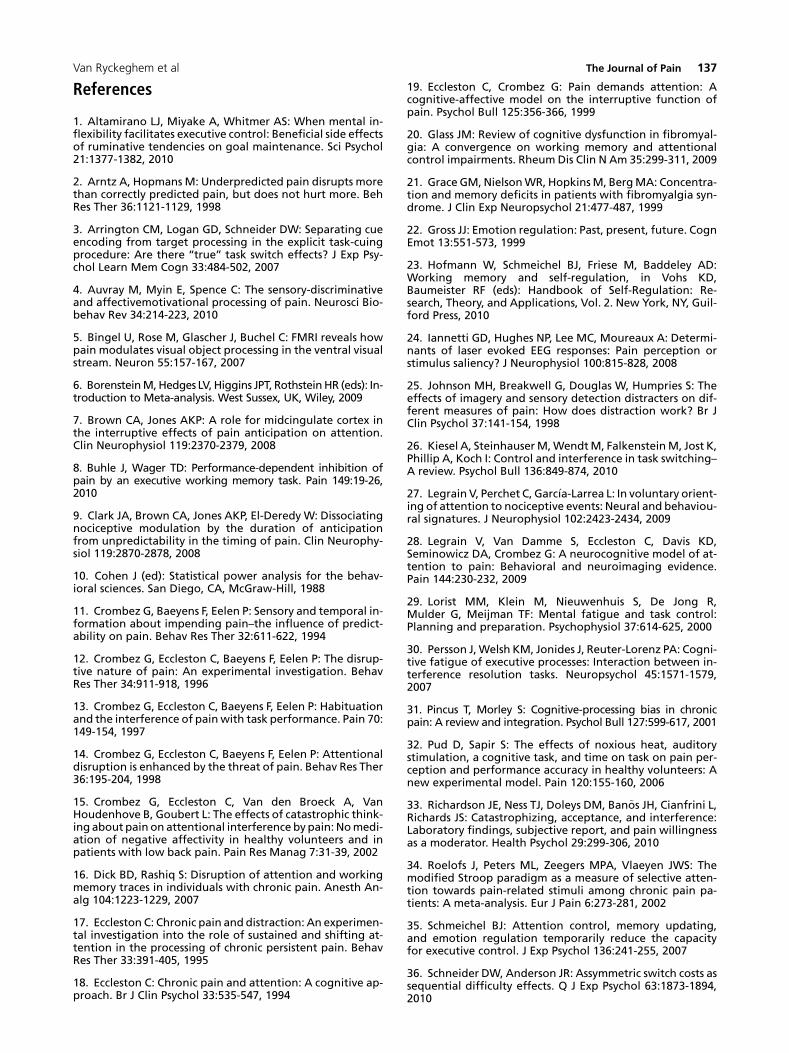
Figure 3. Reaction times for both repetition and switch trialswhen previous task was painful, pain-anticipating, or absentof pain. *P < .05.
with the presence of pain or the anticipation of pain dur-ing the previous task separately (Fig 3). Analyses indi-cated that the prolonged interference effect of painanticipation (F(1,59) = 5.08, P < .05, d = .36; 95% CI =.04: .68) as well as actual pain (F(1, 59) = 4.62, P < .05,d = .33; 95% CI = .04: .62) differed between switch trialsand repetition trials. Paired sample t-tests showed no sig-nificant difference between repetition trials (M = 669, SD= 139) and switch trials (M = 669, SD = 138) when theprevious task was neutral (t(59) < 1, d = .00; 95% CI =�.17: .17). A significant difference (M = 29, SD = 89)was found between repetition trials (M = 648, SD =155) and switch trials (M = 676, SD = 132) when the pre-vious task elicited the anticipation of pain, t(59) = 2.51, P< .05, d = .19; 95% CI = .04: .34. Also, a significant differ-ence (M= 39, SD= 141)was foundbetween repetition tri-als (M = 731, SD = 205) and switch trials (M = 770, SD =208) when pain was induced during the previous task,t(59) = 2.13, P < .05, d = .19; 95% CI = .01: .36.
DiscussionThe aimof the present studywas to investigate the role
of pain and its anticipation on task performance in amul-titask environment. This was investigated experimentallybymeans of amodified cued task-switching procedure inwhich participants repeated or switched between 3 ran-domly presented tasks, with 1 task being related to possi-ble pain. We were interested in the effect of immediateand prolonged task interference of pain. For theimmediate-interference effect, we observed that pain in-terfereswith anongoing task irrespectively of pain inten-sity. Merely anticipating pain did not hamper taskperformance. For the prolonged-interference effect,the presence of pain during a trial impedes performanceon the subsequent trial. The prolonged-interference ef-fect was larger for pain of high intensity than for painof low intensity. Finally, the prolonged-interference ef-fectwas largerwhena switchbetween taskswas requiredthan when the same task was repeated.First we elaborate on the findings related to interfer-
ence of pain. Task performance during the presence ofpain was impaired. This finding is in line with researchshowing that task performance during the presence ofpain was poorer2,8,12-15,18,25,33,43 but also see otherpapers.32,37,45 This effect was, however, small and justfailed to reach significance. This is in contrast withprevious findings which mostly report that pain hasa relatively large interference effect on concurrenttasks. One plausible explanation for this discrepancymay lie in the predictability of pain. In previous studieson immediate task interruption by pain, pain wasdelivered unannounced and was therefore temporallyunpredictable (eg,2,12,13,33). Temporal predictability hasbeen shown to decrease the interference of pain withtask performance.11 In the present study, pain was pre-dictable because it could only be delivered during a par-ticular task at a given moment (onset of task stimulus). Itseems that participants may be able to partially protecttheir task performance from interruption by pain onsome occasions. People might increase their effort or

136 The Journal of Pain Pain in a Multitask Environment
prioritize nonpain tasks when they expect that pain willinterfere.11,14 However, it may be the case that theshielding of attention from pain may have somenegative effects later on as was found in this study.To our knowledge, our results are the first of their kind
to reveal that pain can have a prolonged interference ef-fect. Indeed, the disruptive effect of pain on task perfor-mance may not be limited to the pain experience itself,but may extend even when pain has already dissipated.In our study, this prolonged effect variedwith pain inten-sity. High intense pain resulted in a stronger prolongedinterference effect than low intense pain. Several expla-nations are possible. First, the increase of effort to shieldattention from immediate pain (see above) may tempo-rarily deplete effort leading to a worse performance onthe following trial.23,35 Second, it is possible thatparticipants ruminate about pain immediately aftercompletion of a trial with pain. Because rumination isknown to be cognitively demanding,22 it may interferewith the preparation of the subsequent task, resultingin a decreased performance on the following task.1 Offurther interest is the finding that the prolonged-interference effect of pain was more pronounced whenparticipants switched between tasks. Because switchingbetween tasks is more demanding than repeatingtasks,42 we may indeed expect that switching betweentasks will detrimentally affect task performance whencognitive resources are depleted or when task load isheightened (eg, during rumination).29,30,33,36,41 Toconclude, we can state that although the ability of painto disrupt current performance is already frequentlyresearched, and its function has been variouslydescribed as an evolved interrupt forming part ofa general defensive system,4,20,40 further research toclarify under which conditions pain interferes with taskperformance is still necessary.A further aspect of these results relates to the influ-
ence of pain anticipation. Based on previous studies indi-cating that pain anticipation increases attention for painand results in task interference,7,14 we expected thatanticipation of pain would interfere with taskperformance in the present study. This prediction wasnot supported. It may well be that the interference bypain anticipation is more subtle than the interferencerelated to pain. The fact that the pain was temporallypredictable might even have further reduced theinterference effect of pain anticipation. Furthermore,interference by pain anticipation may also be morelimited in time than interference related to pain. In linewith this, Van Damme et al39 found interference effectsfor pain cues that were very close in time to the onsetof the next experimental event (100ms). Effects were ab-sent for large intervals (eg, 500 and 900ms).39 In the pres-ent study, the interval between the task cue—whichindicates if pain is impending—and the stimulus onsetwas 1,000 ms, which may have been too long to observean immediate-interference effect for pain anticipation.The absence of an overall prolonged-interference effecton the basis of pain anticipation may be explained in
a similar way. Although we did not find an overallprolonged-interference effect of pain anticipation dur-ing the previous task, results did show that switching be-tween tasks compared with repeating tasks was moreimpaired when the previous task involved pain anticipa-tion than when the previous task was neutral. This find-ing may be explained by the fact that the task which isassociated with pain anticipation (and also pain) be-comes more arousing and more active than the othertasks.46 It may then be more difficult to switch froma dominant task towards another task, whereas repeat-ing the dominant task may become easier. Further inves-tigation is warranted on exactly when anticipation ofpain interferes with task performance.7,9,47
Several theoretical implications emerge from the pres-ent study. First, pain not only decreases performance onsingle tasks, but also when multiple tasks are presented.This interruption extends beyond current tasks to theperformance of subsequent tasks. Effect size indices indi-cate that this prolonged-interference effect may be im-portant to take into account, especially when pain isintense (d = .57; moderate effect size). Although thishas been suggested for a number of years,19 a suitableparadigmhas only nowbeen created to allow for the dis-aggregation of these effects. Task environments ofgreater complexity are needed in order to observe the in-terruptive function of pain. Not only will complex envi-ronments improve the validity of findings, they willalso enable the observation of attentional strategies cre-ated in response to multiple demands. Finally, it is worthnoting that the prolonged-interference effect observedin complex environments was sensitive to alterations inthe characteristics of the pain stimulus, specifically hereits intensity. Further investigation is warranted on the ef-fects of other characteristics of pain, both bottomup (eg,novelty) and top down (eg, motivational significance).28
This study has some limitations. First, the use of thistask-switching paradigm in a pain context is novel, soreplication is necessary. Second, different calibration cri-teria were applied for the low- and high-level pain stim-ulus for practical reasons. The low-level pain stimuluswas stimulus-locked for all participants, whereas thehigh-level pain stimulus was individually determined asa stimulus at tolerance level. Future research may optto use a more sophisticated calibration procedure (eg,Zeidan et al48). Third, the present study was conductedwith students using experimental pain stimuli. There-fore, one should be cautious in generalizing these re-sults to other nonclinical populations and clinicalpopulations in a daily life context. Fourth, post hocpower analyses indicated that small effects may havebeen missed due to a lack of statistical power, in partic-ular interaction effects related to the between-groupmanipulation of pain intensity.Despite these considerations, the present investigation
expands our understanding of the influence of pain ontask performance in a multitask environment and pro-vides methods for the further investigation of attentiontoward and away from pain in complex environments.
Van Ryckeghem et al The Journal of Pain 137
References
1. Altamirano LJ, Miyake A, Whitmer AS: When mental in-flexibility facilitates executive control: Beneficial side effectsof ruminative tendencies on goal maintenance. Sci Psychol21:1377-1382, 2010
2. Arntz A, Hopmans M: Underpredicted pain disrupts morethan correctly predicted pain, but does not hurt more. BehRes Ther 36:1121-1129, 1998
3. Arrington CM, Logan GD, Schneider DW: Separating cueencoding from target processing in the explicit task-cuingprocedure: Are there ‘‘true’’ task switch effects? J Exp Psy-chol Learn Mem Cogn 33:484-502, 2007
4. Auvray M, Myin E, Spence C: The sensory-discriminativeand affectivemotivational processing of pain. Neurosci Bio-behav Rev 34:214-223, 2010
5. Bingel U, Rose M, Glascher J, Buchel C: FMRI reveals howpain modulates visual object processing in the ventral visualstream. Neuron 55:157-167, 2007
6. BorensteinM,Hedges LV,Higgins JPT, RothsteinHR (eds): In-troduction to Meta-analysis. West Sussex, UK, Wiley, 2009
7. Brown CA, Jones AKP: A role for midcingulate cortex inthe interruptive effects of pain anticipation on attention.Clin Neurophysiol 119:2370-2379, 2008
8. Buhle J, Wager TD: Performance-dependent inhibition ofpain by an executive working memory task. Pain 149:19-26,2010
9. Clark JA, Brown CA, Jones AKP, El-Deredy W: Dissociatingnociceptive modulation by the duration of anticipationfrom unpredictability in the timing of pain. Clin Neurophy-siol 119:2870-2878, 2008
10. Cohen J (ed): Statistical power analysis for the behav-ioral sciences. San Diego, CA, McGraw-Hill, 1988
11. Crombez G, Baeyens F, Eelen P: Sensory and temporal in-formation about impending pain–the influence of predict-ability on pain. Behav Res Ther 32:611-622, 1994
12. Crombez G, Eccleston C, Baeyens F, Eelen P: The disrup-tive nature of pain: An experimental investigation. BehavRes Ther 34:911-918, 1996
13. Crombez G, Eccleston C, Baeyens F, Eelen P: Habituationand the interference of painwith task performance. Pain 70:149-154, 1997
14. Crombez G, Eccleston C, Baeyens F, Eelen P: Attentionaldisruption is enhanced by the threat of pain. Behav Res Ther36:195-204, 1998
15. Crombez G, Eccleston C, Van den Broeck A, VanHoudenhove B, Goubert L: The effects of catastrophic think-ing about pain on attentional interference bypain: Nomedi-ation of negative affectivity in healthy volunteers and inpatients with low back pain. Pain Res Manag 7:31-39, 2002
16. Dick BD, Rashiq S: Disruption of attention and workingmemory traces in individuals with chronic pain. Anesth An-alg 104:1223-1229, 2007
17. Eccleston C: Chronic pain anddistraction: An experimen-tal investigation into the role of sustained and shifting at-tention in the processing of chronic persistent pain. BehavRes Ther 33:391-405, 1995
18. Eccleston C: Chronic pain and attention: A cognitive ap-proach. Br J Clin Psychol 33:535-547, 1994
19. Eccleston C, Crombez G: Pain demands attention: Acognitive-affective model on the interruptive function ofpain. Psychol Bull 125:356-366, 1999
20. Glass JM: Review of cognitive dysfunction in fibromyal-gia: A convergence on working memory and attentionalcontrol impairments. Rheum Dis Clin N Am 35:299-311, 2009
21. Grace GM, NielsonWR, HopkinsM, BergMA: Concentra-tion and memory deficits in patients with fibromyalgia syn-drome. J Clin Exp Neuropsychol 21:477-487, 1999
22. Gross JJ: Emotion regulation: Past, present, future. CognEmot 13:551-573, 1999
23. Hofmann W, Schmeichel BJ, Friese M, Baddeley AD:Working memory and self-regulation, in Vohs KD,Baumeister RF (eds): Handbook of Self-Regulation: Re-search, Theory, and Applications, Vol. 2. New York, NY, Guil-ford Press, 2010
24. Iannetti GD, Hughes NP, Lee MC, Moureaux A: Determi-nants of laser evoked EEG responses: Pain perception orstimulus saliency? J Neurophysiol 100:815-828, 2008
25. Johnson MH, Breakwell G, Douglas W, Humpries S: Theeffects of imagery and sensory detection distracters on dif-ferent measures of pain: How does distraction work? Br JClin Psychol 37:141-154, 1998
26. Kiesel A, SteinhauserM,WendtM, FalkensteinM, Jost K,Phillip A, Koch I: Control and interference in task switching–A review. Psychol Bull 136:849-874, 2010
27. Legrain V, Perchet C, Garc�ıa-Larrea L: In voluntary orient-ing of attention to nociceptive events: Neural and behaviou-ral signatures. J Neurophysiol 102:2423-2434, 2009
28. Legrain V, Van Damme S, Eccleston C, Davis KD,Seminowicz DA, Crombez G: A neurocognitive model of at-tention to pain: Behavioral and neuroimaging evidence.Pain 144:230-232, 2009
29. Lorist MM, Klein M, Nieuwenhuis S, De Jong R,Mulder G, Meijman TF: Mental fatigue and task control:Planning and preparation. Psychophysiol 37:614-625, 2000
30. Persson J,Welsh KM, Jonides J, Reuter-Lorenz PA: Cogni-tive fatigue of executive processes: Interaction between in-terference resolution tasks. Neuropsychol 45:1571-1579,2007
31. Pincus T, Morley S: Cognitive-processing bias in chronicpain: A review and integration. Psychol Bull 127:599-617, 2001
32. Pud D, Sapir S: The effects of noxious heat, auditorystimulation, a cognitive task, and time on task on pain per-ception and performance accuracy in healthy volunteers: Anew experimental model. Pain 120:155-160, 2006
33. Richardson JE, Ness TJ, Doleys DM, Ban~os JH, Cianfrini L,Richards JS: Catastrophizing, acceptance, and interference:Laboratory findings, subjective report, and pain willingnessas a moderator. Health Psychol 29:299-306, 2010
34. Roelofs J, Peters ML, Zeegers MPA, Vlaeyen JWS: Themodified Stroop paradigm as a measure of selective atten-tion towards pain-related stimuli among chronic pain pa-tients: A meta-analysis. Eur J Pain 6:273-281, 2002
35. Schmeichel BJ: Attention control, memory updating,and emotion regulation temporarily reduce the capacityfor executive control. J Exp Psychol 136:241-255, 2007
36. Schneider DW, Anderson JR: Assymmetric switch costs assequential difficulty effects. Q J Exp Psychol 63:1873-1894,2010

138 The Journal of Pain Pain in a Multitask Environment
37. SeminowiczDA,DavisKD:Are-examinationofcognitionin-teractions: Implications for neuroimaging. Pain 130:8-13, 2007
38. Vancleef L, Peters M: Pain catastrophizing, but not in-jury/illness sensitivity or anxiety sensitivity, enhances atten-tional interference by pain. J Pain 7:23-30, 2006
39. Van Damme S, Crombez G, Eccleston C: Retarded disen-gagement from pain cues: The effects of pain catastrophiz-ing and pain expectancy. Pain 100:111-118, 2002
40. Van Damme S, Legrain V, Vogt J, Crombez G: Keepingpain in mind: A motivational account of attention to pain.Neurosci Biobeh Rev 34:204-213, 2010
41. van der Linden D, Frese M, Meijman TF: Mental fatigueand the control of cognitive processes: Effects on persevera-tion and planning. Acta Psychol 113:45-65, 2003
42. Vandierendonck A, Liefooghe B, Verbruggen F: Taskswitching: Interplay of reconfiguration and interference.Psych Bull 136:601-626, 2010
43. Vangronsveld KLH, Van Damme S, Peters ML,Vlaeyen JWS, Goossens M, Crombez G: An experimental in-
vestigation on attentional interference by threatening fixa-tions of the neck in patients with chronic whiplashsyndrome. Pain 127:121-129, 2007
44. Van Ryckeghem DML, Van Damme S, Crombez G,Eccleston C, Verhoeven K, Legrain V: The role of spatial at-tention in attentional control over pain: An experimental in-vestigation. Exp Brain Res 208:269-275, 2011
45. Veldhuijzen DS, Kenemans JL, de Bruin CM, Olivier B,Volkerts ER: Pain and attention: Attentional disruption ordistraction. J Pain 7:11-20, 2006
46. Verguts T, NotebaertW: Adaptation by binding: A learn-ing account of cognitive control. Trends Cogn Sci 13:252-257, 2009
47. Wiech K, Lin C, Brodersen KH, Bingel U, Ploner M,Tracey I: Anterior insula integrates information about sa-lience into perceptual decisions about pain. J Neurosci 30:16324-16331, 2010
48. Zeidan F, Gordon NS, Merchant J, Goolkasian P: The ef-fects of brief mindfulness meditation training on experi-mentally induced pain. J Pain 11:199-209, 2010





























