Embed Size (px)
Citation preview
The MCA Dopplerand its Role in theEvaluation of FetalAnemia and FetalGrowth Restriction
Mauro H. Schenone, MD, Giancarlo Mari, MD*
KEYWORDS
� MCA � Doppler � IUGR � Fetal anemia
DIAGNOSIS OF FETAL ANEMIA BEFORE THE USE OF THE MIDDLE CEREBRAL ARTERYPEAK SYSTOLIC VELOCITY
Before the widespread use of the middle cerebral artery (MCA) peak systolic velocity(PSV), the management of maternal red cell alloimmunization was based on an indirectmeasurement of fetal hemolysis using spectrophotometric analysis of the amnioticfluid (optical density [OD] at 450 nm).1 The method to predict the severity of the hemo-lytic disease of the fetus and neonate was introduced by Liley in 1961.2 The only optionin the diagnosis of anemia from causes other than red cell alloimmunization was thepercutaneous umbilical cord sampling that was initially performed with fetoscopyand, since 1983, under ultrasound guidance.3
FETAL MCA: 23 YEARS OF LITERATURE
Woo and colleagues4 reported serial Doppler flow velocity-time waveforms of theMCA at its origin from the internal carotid arteries in 14 patients with normal singletonpregnancies. The A/B ratio showed a progressive decrease with advancing gesta-tional age. Kirkinen and colleagues5 recorded blood flow velocity waveforms fromintracranial arteries in 83 normal and 84 high-risk pregnancies. They concluded thatthere was a decrease in the resistance index (RI) toward the end of the pregnancyand that continuous forward flow during diastole was always present in normal cases.Furthermore, they stated that an RI below the tenth percentile was associated with
The authors have nothing to disclose.Department of Obstetrics and Gynecology, University of Tennessee Health Science Center, 853Jefferson Avenue, Room E102, Memphis, TN 38103, USA* Corresponding author.E-mail address: [email protected]
Clin Perinatol 38 (2011) 83–102doi:10.1016/j.clp.2010.12.003 perinatology.theclinics.com0095-5108/11/$ – see front matter � 2011 Elsevier Inc. All rights reserved.
Schenone & Mari84
newborns that were small for gestational age (SGA) and/or the appearance of subse-quent cardiotocographic abnormalities.By 1990, there were 9 published studies in the literature focused on characterizing
the fetal MCA Doppler flow velocity waveform in normal pregnancies, abnormal preg-nancies (primarily intrauterine growth-restricted [IUGR] fetuses), and pregnancies inwhich fetal distress was present.6–13 In 1989, Mari and colleagues10 determined thepulsatility index (PI) in the middle cerebral, anterior cerebral, and internal carotidarteries in 30 fetuses (12 normal, 14 IUGR, and 4 post–in utero blood transfusion aspart of the treatment of Rh isoimmunization) between 23 and 37 weeks of gestation.Their work demonstrated the importance of knowing which cerebral vessel is beinginsonated, because the PI was significantly different in the middle cerebral and internalcarotid arteries when compared with the anterior cerebral artery. Since the introduc-tion of the MCA Doppler to fetal medicine, more than 600 studies have been pub-lished, covering divergent topics from better known areas (eg, IUGR and fetalanemia) to less-explored areas, such as the effects of medications on the MCA14–21
and fetal intracranial hemorrhage.22–24
MCA-PSV FOR THE DIAGNOSIS OF FETAL ANEMIA: A BRIEF HISTORY OF ITSCONCEPTION
The use of the MCA-PSV for the diagnosis of fetal anemia is considered one of the fewpractice-changing discoveries in fetal medicine. One of the most important contribu-tions of the MCA-PSV to clinical practice has been the dramatic reduction in thenumber of invasive procedures performed in the management of red cell alloimmu-nized pregnancies.25
Mari and colleagues26 reported that the PI of the MCA decreases within 2 hoursafter intrauterine blood transfusion and that the MCA-PSV was a better parameterthan the PI in the assessment of pregnancies complicated by fetal anemia.27 Vyasand colleagues28 studied 24 Rh-isoimmunized pregnancies and noted an increasein the MCA mean blood velocity, hypothesizing that the increase of blood flow couldbe attributed to a decrease in blood viscosity, as previously suggested by experimen-tation in dogs.29 A few years later, the same group reported that the MCA mean bloodvelocity was not an optimal parameter to assess fetal anemia.30
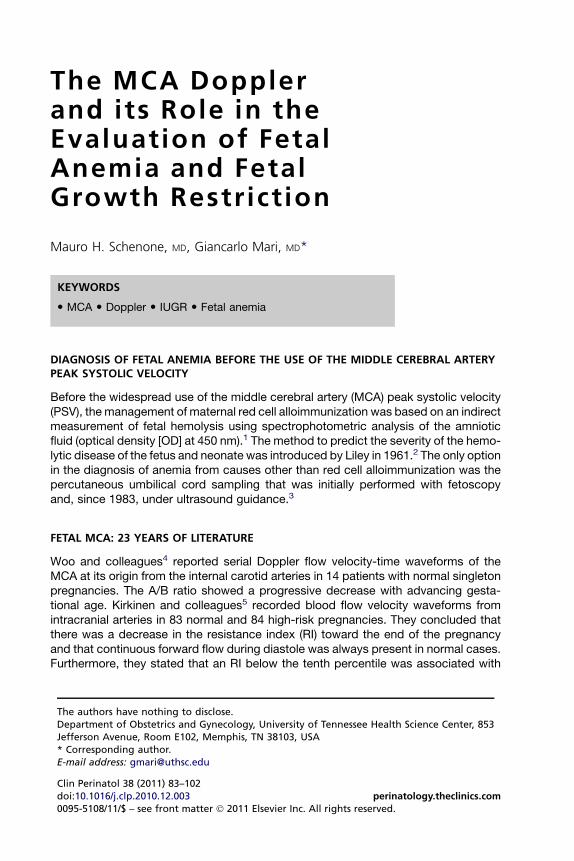
The reference range for the MCA-PSV was reported in 1995 (Fig. 1).31 In the samestudy, it was reported that all the anemic fetuses had an MCA-PSV greater than themean of the range of normal values. The false-positive rate was 50%; althoughhigh, had this rate been applied in clinical practice at that time, it would have elimi-nated 50% of the invasive procedures.In 1997, MCA Doppler waveforms were examined before and after intrauterine
blood transfusion. It was noted that the increase of the fetal hematocrit was associ-ated with a decrease in the MCA-PSV, and the results were later reproduced.32,33
A study of 111 fetuses at risk for anemia because of red cell alloimmunization and265 normal fetuses later changed the practice of how the former were evaluated.25
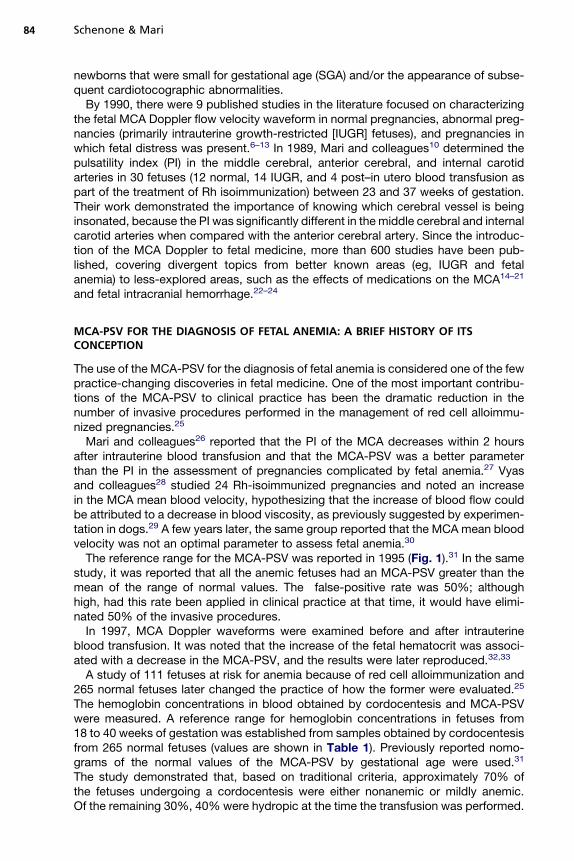
The hemoglobin concentrations in blood obtained by cordocentesis and MCA-PSVwere measured. A reference range for hemoglobin concentrations in fetuses from18 to 40 weeks of gestation was established from samples obtained by cordocentesisfrom 265 normal fetuses (values are shown in Table 1). Previously reported nomo-grams of the normal values of the MCA-PSV by gestational age were used.31
The study demonstrated that, based on traditional criteria, approximately 70% ofthe fetuses undergoing a cordocentesis were either nonanemic or mildly anemic.Of the remaining 30%, 40% were hydropic at the time the transfusion was performed.
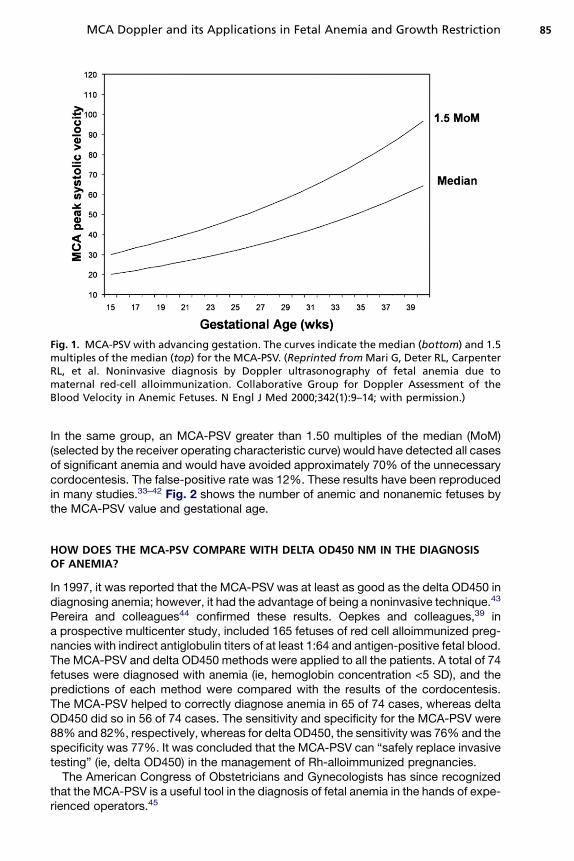
Fig. 1. MCA-PSV with advancing gestation. The curves indicate the median (bottom) and 1.5multiples of the median (top) for the MCA-PSV. (Reprinted fromMari G, Deter RL, CarpenterRL, et al. Noninvasive diagnosis by Doppler ultrasonography of fetal anemia due tomaternal red-cell alloimmunization. Collaborative Group for Doppler Assessment of theBlood Velocity in Anemic Fetuses. N Engl J Med 2000;342(1):9–14; with permission.)
MCA Doppler and its Applications in Fetal Anemia and Growth Restriction 85
In the same group, an MCA-PSV greater than 1.50 multiples of the median (MoM)(selected by the receiver operating characteristic curve) would have detected all casesof significant anemia and would have avoided approximately 70% of the unnecessarycordocentesis. The false-positive rate was 12%. These results have been reproducedin many studies.33–42 Fig. 2 shows the number of anemic and nonanemic fetuses bythe MCA-PSV value and gestational age.
HOW DOES THE MCA-PSV COMPARE WITH DELTA OD450 NM IN THE DIAGNOSISOF ANEMIA?
In 1997, it was reported that the MCA-PSV was at least as good as the delta OD450 indiagnosing anemia; however, it had the advantage of being a noninvasive technique.43
Pereira and colleagues44 confirmed these results. Oepkes and colleagues,39 ina prospective multicenter study, included 165 fetuses of red cell alloimmunized preg-nancies with indirect antiglobulin titers of at least 1:64 and antigen-positive fetal blood.The MCA-PSV and delta OD450 methods were applied to all the patients. A total of 74fetuses were diagnosed with anemia (ie, hemoglobin concentration <5 SD), and thepredictions of each method were compared with the results of the cordocentesis.The MCA-PSV helped to correctly diagnose anemia in 65 of 74 cases, whereas deltaOD450 did so in 56 of 74 cases. The sensitivity and specificity for the MCA-PSV were88% and 82%, respectively, whereas for delta OD450, the sensitivity was 76% and thespecificity was 77%. It was concluded that the MCA-PSV can “safely replace invasivetesting” (ie, delta OD450) in the management of Rh-alloimmunized pregnancies.The American Congress of Obstetricians and Gynecologists has since recognized
that the MCA-PSV is a useful tool in the diagnosis of fetal anemia in the hands of expe-rienced operators.45
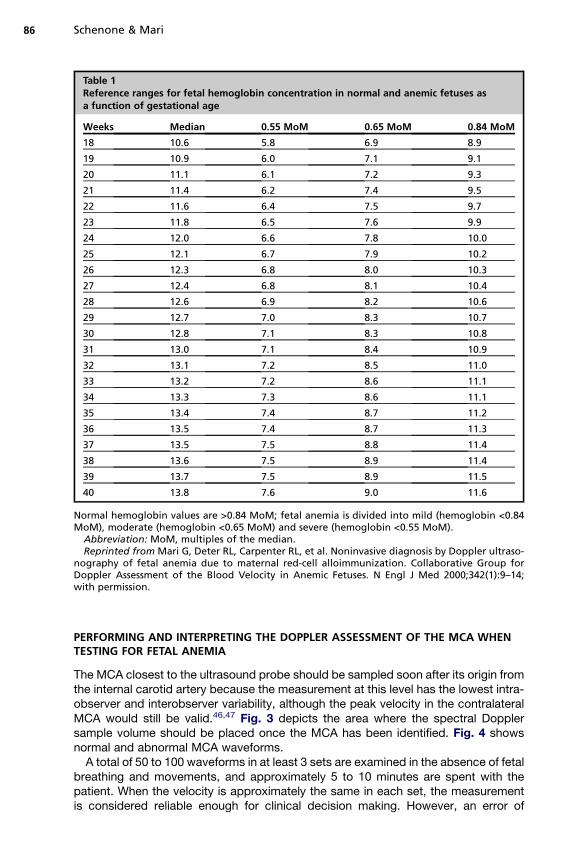
Table 1Reference ranges for fetal hemoglobin concentration in normal and anemic fetuses asa function of gestational age
Weeks Median 0.55 MoM 0.65 MoM 0.84 MoM
18 10.6 5.8 6.9 8.9
19 10.9 6.0 7.1 9.1
20 11.1 6.1 7.2 9.3
21 11.4 6.2 7.4 9.5
22 11.6 6.4 7.5 9.7
23 11.8 6.5 7.6 9.9
24 12.0 6.6 7.8 10.0
25 12.1 6.7 7.9 10.2
26 12.3 6.8 8.0 10.3
27 12.4 6.8 8.1 10.4
28 12.6 6.9 8.2 10.6
29 12.7 7.0 8.3 10.7
30 12.8 7.1 8.3 10.8
31 13.0 7.1 8.4 10.9
32 13.1 7.2 8.5 11.0
33 13.2 7.2 8.6 11.1
34 13.3 7.3 8.6 11.1
35 13.4 7.4 8.7 11.2
36 13.5 7.4 8.7 11.3
37 13.5 7.5 8.8 11.4
38 13.6 7.5 8.9 11.4
39 13.7 7.5 8.9 11.5
40 13.8 7.6 9.0 11.6
Normal hemoglobin values are >0.84 MoM; fetal anemia is divided into mild (hemoglobin <0.84MoM), moderate (hemoglobin <0.65 MoM) and severe (hemoglobin <0.55 MoM).
Abbreviation: MoM, multiples of the median.Reprinted from Mari G, Deter RL, Carpenter RL, et al. Noninvasive diagnosis by Doppler ultraso-
nography of fetal anemia due to maternal red-cell alloimmunization. Collaborative Group forDoppler Assessment of the Blood Velocity in Anemic Fetuses. N Engl J Med 2000;342(1):9–14;with permission.
Schenone & Mari86
PERFORMING AND INTERPRETING THE DOPPLER ASSESSMENT OF THE MCA WHENTESTING FOR FETAL ANEMIA
The MCA closest to the ultrasound probe should be sampled soon after its origin fromthe internal carotid artery because the measurement at this level has the lowest intra-observer and interobserver variability, although the peak velocity in the contralateralMCA would still be valid.46,47 Fig. 3 depicts the area where the spectral Dopplersample volume should be placed once the MCA has been identified. Fig. 4 showsnormal and abnormal MCA waveforms.A total of 50 to 100 waveforms in at least 3 sets are examined in the absence of fetal
breathing and movements, and approximately 5 to 10 minutes are spent with thepatient. When the velocity is approximately the same in each set, the measurementis considered reliable enough for clinical decision making. However, an error of
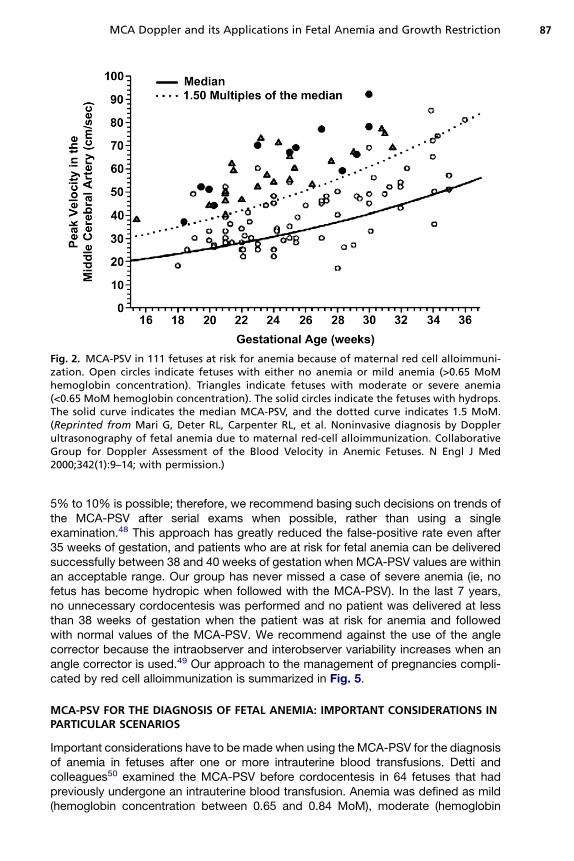
Fig. 2. MCA-PSV in 111 fetuses at risk for anemia because of maternal red cell alloimmuni-zation. Open circles indicate fetuses with either no anemia or mild anemia (>0.65 MoMhemoglobin concentration). Triangles indicate fetuses with moderate or severe anemia(<0.65 MoM hemoglobin concentration). The solid circles indicate the fetuses with hydrops.The solid curve indicates the median MCA-PSV, and the dotted curve indicates 1.5 MoM.(Reprinted from Mari G, Deter RL, Carpenter RL, et al. Noninvasive diagnosis by Dopplerultrasonography of fetal anemia due to maternal red-cell alloimmunization. CollaborativeGroup for Doppler Assessment of the Blood Velocity in Anemic Fetuses. N Engl J Med2000;342(1):9–14; with permission.)
MCA Doppler and its Applications in Fetal Anemia and Growth Restriction 87
5% to 10% is possible; therefore, we recommend basing such decisions on trends ofthe MCA-PSV after serial exams when possible, rather than using a singleexamination.48 This approach has greatly reduced the false-positive rate even after35 weeks of gestation, and patients who are at risk for fetal anemia can be deliveredsuccessfully between 38 and 40 weeks of gestation when MCA-PSV values are withinan acceptable range. Our group has never missed a case of severe anemia (ie, nofetus has become hydropic when followed with the MCA-PSV). In the last 7 years,no unnecessary cordocentesis was performed and no patient was delivered at lessthan 38 weeks of gestation when the patient was at risk for anemia and followedwith normal values of the MCA-PSV. We recommend against the use of the anglecorrector because the intraobserver and interobserver variability increases when anangle corrector is used.49 Our approach to the management of pregnancies compli-cated by red cell alloimmunization is summarized in Fig. 5.
MCA-PSV FOR THE DIAGNOSIS OF FETAL ANEMIA: IMPORTANT CONSIDERATIONS INPARTICULAR SCENARIOS
Important considerations have to be made when using the MCA-PSV for the diagnosisof anemia in fetuses after one or more intrauterine blood transfusions. Detti andcolleagues50 examined the MCA-PSV before cordocentesis in 64 fetuses that hadpreviously undergone an intrauterine blood transfusion. Anemia was defined as mild(hemoglobin concentration between 0.65 and 0.84 MoM), moderate (hemoglobin
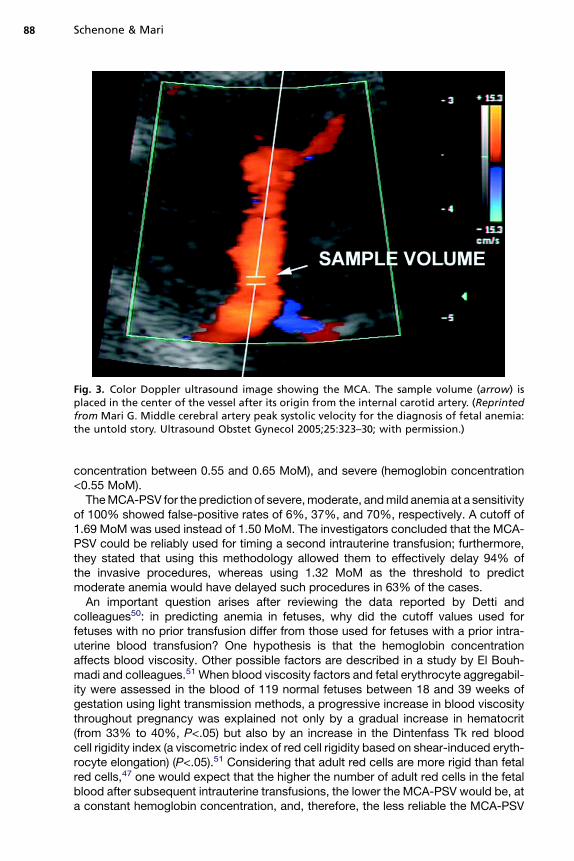
Fig. 3. Color Doppler ultrasound image showing the MCA. The sample volume (arrow) isplaced in the center of the vessel after its origin from the internal carotid artery. (Reprintedfrom Mari G. Middle cerebral artery peak systolic velocity for the diagnosis of fetal anemia:the untold story. Ultrasound Obstet Gynecol 2005;25:323–30; with permission.)
Schenone & Mari88
concentration between 0.55 and 0.65 MoM), and severe (hemoglobin concentration<0.55 MoM).TheMCA-PSV for the prediction of severe,moderate, andmild anemia at a sensitivity
of 100% showed false-positive rates of 6%, 37%, and 70%, respectively. A cutoff of1.69 MoM was used instead of 1.50 MoM. The investigators concluded that the MCA-PSV could be reliably used for timing a second intrauterine transfusion; furthermore,they stated that using this methodology allowed them to effectively delay 94% ofthe invasive procedures, whereas using 1.32 MoM as the threshold to predictmoderate anemia would have delayed such procedures in 63% of the cases.An important question arises after reviewing the data reported by Detti and
colleagues50: in predicting anemia in fetuses, why did the cutoff values used forfetuses with no prior transfusion differ from those used for fetuses with a prior intra-uterine blood transfusion? One hypothesis is that the hemoglobin concentrationaffects blood viscosity. Other possible factors are described in a study by El Bouh-madi and colleagues.51 When blood viscosity factors and fetal erythrocyte aggregabil-ity were assessed in the blood of 119 normal fetuses between 18 and 39 weeks ofgestation using light transmission methods, a progressive increase in blood viscositythroughout pregnancy was explained not only by a gradual increase in hematocrit(from 33% to 40%, P<.05) but also by an increase in the Dintenfass Tk red bloodcell rigidity index (a viscometric index of red cell rigidity based on shear-induced eryth-rocyte elongation) (P<.05).51 Considering that adult red cells are more rigid than fetalred cells,47 one would expect that the higher the number of adult red cells in the fetalblood after subsequent intrauterine transfusions, the lower the MCA-PSV would be, ata constant hemoglobin concentration, and, therefore, the less reliable the MCA-PSV
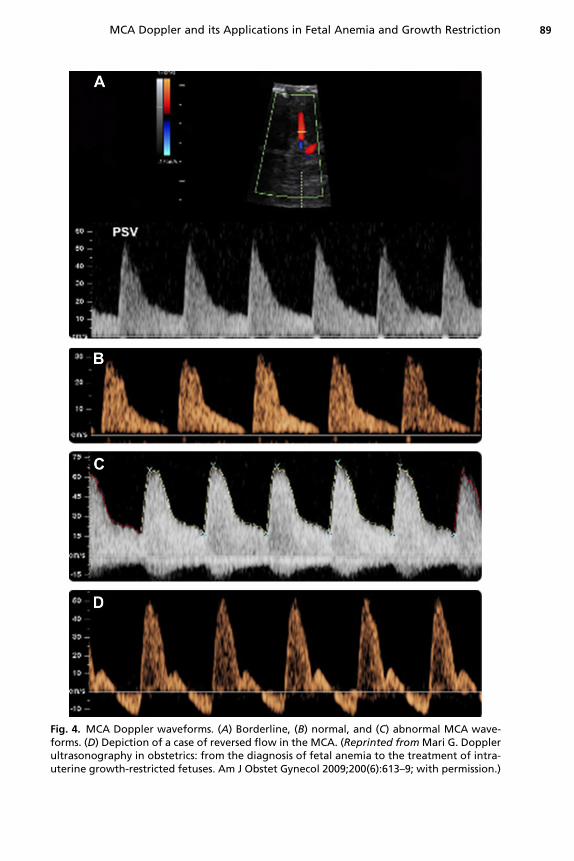
Fig. 4. MCA Doppler waveforms. (A) Borderline, (B) normal, and (C) abnormal MCA wave-forms. (D) Depiction of a case of reversed flow in the MCA. (Reprinted fromMari G. Dopplerultrasonography in obstetrics: from the diagnosis of fetal anemia to the treatment of intra-uterine growth-restricted fetuses. Am J Obstet Gynecol 2009;200(6):613–9; with permission.)
MCA Doppler and its Applications in Fetal Anemia and Growth Restriction 89
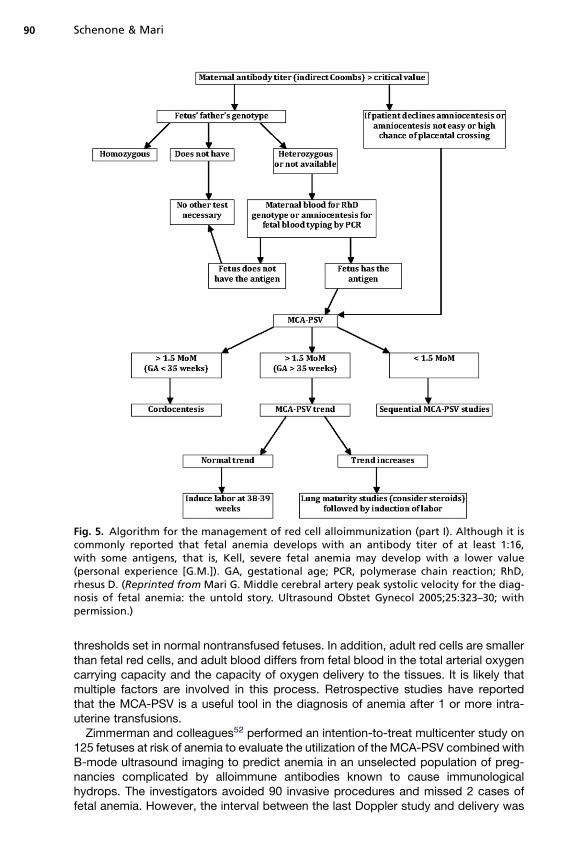
Fig. 5. Algorithm for the management of red cell alloimmunization (part I). Although it iscommonly reported that fetal anemia develops with an antibody titer of at least 1:16,with some antigens, that is, Kell, severe fetal anemia may develop with a lower value(personal experience [G.M.]). GA, gestational age; PCR, polymerase chain reaction; RhD,rhesus D. (Reprinted from Mari G. Middle cerebral artery peak systolic velocity for the diag-nosis of fetal anemia: the untold story. Ultrasound Obstet Gynecol 2005;25:323–30; withpermission.)
Schenone & Mari90
thresholds set in normal nontransfused fetuses. In addition, adult red cells are smallerthan fetal red cells, and adult blood differs from fetal blood in the total arterial oxygencarrying capacity and the capacity of oxygen delivery to the tissues. It is likely thatmultiple factors are involved in this process. Retrospective studies have reportedthat the MCA-PSV is a useful tool in the diagnosis of anemia after 1 or more intra-uterine transfusions.Zimmerman and colleagues52 performed an intention-to-treat multicenter study on
125 fetuses at risk of anemia to evaluate the utilization of the MCA-PSV combined withB-mode ultrasound imaging to predict anemia in an unselected population of preg-nancies complicated by alloimmune antibodies known to cause immunologicalhydrops. The investigators avoided 90 invasive procedures and missed 2 cases offetal anemia. However, the interval between the last Doppler study and delivery was
MCA Doppler and its Applications in Fetal Anemia and Growth Restriction 91
approximately 3 weeks. In the same study, labor was induced in 6 pregnancies after35 weeks. The neonates were not anemic. The conclusions of this study were (1) theMCA-PSV may be used to diagnose anemia, (2) the interval between subsequentstudies after 30 weeks of gestation should be less than 3 weeks, and (3) after 34 weeksof gestation, the trend of the MCA-PSV may decrease the number of cases with false-positive results. The increase in the false-positive rate after 35 weeks of gestationcould be because of different fetal behavioral states. The MCA-PSV could be falselyincreased when the measurement is performed during a period of rest immediatelyafter a period of fetal activity.The MCA-PSV is useful in cases of Kell isoimmunization,25,53 particularly because
the delta OD450 has been proved not to be of help in such cases.54 This is thoughtto be related to the pathophysiology of this disease, in which the predominant mech-anism of anemia is not hemolysis but rather bone marrow suppression oferythropoiesis.55
The MCA-PSV is also of use in diagnosing anemia secondary to parvovirusinfection,56,57 fetomaternal hemorrhage,58 and a-thalassemia-1.59
TheMCA-PSV has been studied in twin pregnancies. In a study of 16monochorionicand 32 dichorionic pregnancies, Dashe and colleagues60 concluded that MCA-PSVvalues in uncomplicated twin pregnancies are comparable with previously publishedsingleton norms. Klaritsch and colleagues61 examined 50 uncomplicated monochor-ionic diamniotic (MCDA) pregnancies for a total of 100 examinations of theMCA-PSV, assessed biweekly from 15 weeks of gestation, to create normative rangesfrom 15 to 37 weeks of gestation. Measurements between 18 and 37 weeks of gesta-tion were comparable to those in singletons; however, before 18 weeks of gestation,the MCA-PSV values were higher in MCDA twin pregnancies compared with singletonreferences. It would be reasonable to assume that the MCA-PSV, using previouslyestablished reference and cutoff values, could be used for the prediction of anemiain twin pregnancies between 18 and 35 weeks of gestation, but there exists a lackof evidence in this area. Evidence is also needed in cases of twin-to-twin transfusionsyndrome (TTTS). In this pathologic condition of twin gestations, the correlation of theMCA-PSV and hemoglobin concentration has only been tested in pregnancy 24 hoursafter the death of 1 monochorionic twin.62 To hypothesize the utility of the MCA-PSV incases of TTTS, several researchers have studied these cases to confirm physiologicprinciples of the sequential laser technique for TTTS treatment and to create a toolfor post–laser treatment prognosis.63,64
FETAL MCA DOPPLER AND IUGR: TRACING THE CONCEPT OF IUGR BACKTO ITS ORIGIN
Traditionally, babies born with a low birth weight were likely considered preterm. Theconcept of IUGR in the literature dates back to the 1960s, when Battaglia andLubchenco65 and Lubchenco and colleagues66 published their work in whichoutcomes were recorded based on birth weight adjusted for gestational age. Oncesuch reference values for birth weight by gestational age became available, newbornscould be differentiated as small, adequate, or large for gestational age,67 and theconcept of intrauterine malnourishment affecting birth weight independent of gesta-tional age gained acceptance. The introduction of ultrasonography in obstetricsallowed the assessment of fetal biometry.68 There exist numerous publications andseveral methods to estimate the fetal weight to the point that it would be impracticalto quote every method in this article. Among the most popular are the methodsdescribed by Shepard and colleagues69 and Hadlock and colleagues.70 Using
Schenone & Mari92
formulas to assess fetal weight allowed one to establish whether a fetus wasadequately grown for gestational age or not. Alexander and colleagues71 publishedan extensive profile of birth weight percentiles for gestational ages between 20 and44 weeks after analyzing data from more than 3 million live births.When using large cross-sectional population based growth curves, the reference
values perform best when managing patients from the same population included inthe study but not as well for individuals from other populations in which fetuses andnewborns can be constitutionally smaller or larger, potentially leading to diagnosesof abnormalities in normal cases. Therefore, attempts have been made to individualizethese curves and diagnose abnormalities only when an individual curve falls belowa projected trend. Deter and colleagues72 have been the first to individualize fetalgrowth parameters. Debate of this issue is ongoing, and the definition of IUGR basedon an estimated fetal weight (EFW) less than the tenth percentile for gestational agecontinues to be challenged.
DOPPLER ULTRASONOGRAPHY IN THE MANAGEMENT OF IUGR
IUGR represents a threat not only for the fetus but also for the individual as a child andadult. Barker and Osmond73 have described an association between birth weightbelow the tenth percentile and the later development of hypertension, hypercholester-olemia, coronary heart disease, impaired glucose tolerance, and diabetes mellitus. Inutero diagnosis and treatment becomes an appealing approach to reduce the burdenexerted by IUGR on society. There are more than 10,000 publications in the literaturerelated to the diagnosis and management of fetuses with IUGR, which is only the tip ofthe iceberg in the frenetic quest for a solution to this problem.Assuring fetal well being and adequately timing delivery of fetuses with IUGR is
paramount; however, the optimal methods are still the subject of much debate.Doppler ultrasonography for the assessment of fetal hemodynamics is one of themost important of these methods, considering that one of the principal pathophysio-logic explanations for IUGR is placental insufficiency, which directly translates intohemodynamic changes in the fetus. Doppler ultrasonography of the umbilical andmiddle cerebral arteries in combination with biometry has been quoted as the besttool to identify small fetuses at risk for an adverse outcome.74–76
Fitzgerald and Drumm77 pioneered the introduction of Doppler ultrasonography inobstetrics, specifically in the assessment of IUGR fetuses, when they reported thatumbilical artery (UA) waveforms are abnormal in fetuses with IUGR and that reversedblood flow of the UA is associated with a poor prognosis.77 Since then, there havebeen numerous publications on this topic.Doppler ultrasonography in the management of IUGR involves the study of multiple
vessels aside from those more commonly assessed (ie, the UA, MCA, and ductusvenosus), and a multitude of vessels have been proposed as part of such manage-ment. Because of the scope of the topic, discussion is limited to the role of theMCA in the management of IUGR.
MCA DOPPLER IN THE ASSESSMENT OF IUGR FETUSES
The structure of the MCA makes it a convenient target for in utero flow velocimetrystudies and, at the same time, opens a window to observe the circulation within thecentral nervous system of the fetus, which is involved in many, if not all, pathologicprocesses in fetal medicine, including IUGR.One of the earliest reports on this subject was by Echizenya and colleagues.7 They
used pulsed Doppler ultrasonography to examine the significance of MCA flow
MCA Doppler and its Applications in Fetal Anemia and Growth Restriction 93
velocimetry as a fetal assessment tool and examined the association betweenabnormal blood flow values and perinatal morbidity in normal and abnormal pregnan-cies (including IUGR). They reported abnormal values in 71.7% of the abnormal preg-nancy group in contrast to a 23.7% rate in normal pregnancies. It was concluded thatvelocimetry of the MCA was the most reliable method to diagnose fetal distress. Thefollowing section addresses each of the MCA Doppler–derived parameters relevant tothe study of IUGR.
MCA PI AND RI
The RI and PI were used in most of the initial studies on MCA Doppler in IUGR fetuses,and they continue to represent the mainstay of the assessment in such cases. Ishi-matsu and colleagues8 reported lower values of the MCA RI in asymmetrical SGAfetuses when compared with normal and symmetric SGA fetuses. van den Wijngaardand colleagues11 demonstrated a reduced PI in IUGR fetuses when compared withnormal fetuses, and these findings were later reproduced.78,79
Chiba and Murakami80 performed Doppler studies of the MCA and cordocentesis todetermine the levels of venous cord blood gases in 17 fetuses with IUGR. Theyreported a significant positive correlation between the MCA RI and PO2 and pH,whereas a negative correlation was noted between the MCA RI and PCO2.The MCA Doppler has also been assessed as a predictor of perinatal outcomes.
Mari and Deter77 compared outcomes of SGA fetuses with a normal MCA PI withoutcomes of those with an abnormal value and concluded that SGA fetuses witha normal MCA PI are at a lower risk for adverse outcomes than those with an abnormalPI. In the same study, the investigators emphasized that the reference ranges of the PIin appropriate-for-gestational-age (AGA) fetuses have a parabolic shape withadvancing gestation. The lowest PI values were observed during the 2 periods of braingrowth spurt. In these 2 periods, the brain demands more nutrients because of theincreased metabolic requirement.Bahado-Singh and colleagues81 studied 203 IUGR fetuses and measured the MCA
PI and UA PI. Perinatal outcome was categorized as (1) birth weight less than the tenthpercentile, (2) birth weight less than the fifth percentile, (3) perinatal complications(meconium-stained fluid, cesarean delivery for fetal distress, 5-minute Apgar score<7, perinatal death, neonatal intensive care unit stay of more than 24 hours, hypogly-cemia, or polycythemia), (4) birth weight less than the tenth percentile with perinatalcomplications, or (5) birth weight less than the fifth percentile with perinatal complica-tions. They reported a statistically significant increase in adverse perinatal outcomesin cases with an abnormal cerebroplacental ratio (the MCA PI divided by the UA PI).In 2000, Baschat and colleagues82 studied Doppler velocimetry of the UA, MCA,
inferior vena cava, ductus venosus, and free umbilical vein in 121 IUGR fetuses. Peri-natal outcomes including mortality, respiratory distress, bronchopulmonary dysplasia,intraventricular hemorrhage, necrotizing enterocolitis, circulatory failure, and levels ofUA blood gases were recorded. The only statistically significant association noted wasthat between the abnormal ductus venosus flow and fetal death.Ulrich and colleagues83 reported that the brain sparing effect represented a risk
factor for early neurological morbidity in fetuses with absent or reverse end-diastolicflow of the UA.One study addresses the use of the MCA PI as a prognostic factor for long-term
outcomes. Roza and colleagues84 reported that a higher UA to MCA ratio (using theMCA PI) correlated with higher scores of internalizing and somatic complaints scalesin toddlers.
Schenone & Mari94
REVERSAL OF BRAIN SPARING EFFECT
An IUGR fetus with a previously low PI that suddenly presents with an elevatedMCA PIhas been linked to poor outcomes.74 Konje and colleagues85 reported reversal of thebrain sparing effect in 8 fetuses, 4 of which ended as stillbirths and the remainder diedduring the neonatal period.Rowlands and Vyas86 published a study that included 5 IUGR fetuses that were
longitudinally monitored until the time of fetal death. Of the 5 fetuses, 2 developedreversal of the brain sparing effect 48 hours before death. This finding has been repro-duced by others.87,88
REVERSE END-DIASTOLIC FLOW IN THE MCA: WHAT DOES IT MEAN?
Sepulveda and colleagues89 describe a case of IUGR with brain sparing effect, inwhich the MCA PI increased back to normal limits at 29 weeks of gestation. Oneweek later, reverse end-diastolic flow of the MCA was seen on the day of in utero fetaldeath. Caution must be exerted when interpreting these data because only 1 case isdescribed, and reverse end-diastolic flow of the MCA can be iatrogenically induced byapplying excessive pressure over the fetal cranium.
MCA-PSV: A NEW PARAMETER IN THE ASSESSMENT OF IUGR FETUSES
Mari and colleagues90 performed a longitudinal assessment of the MCA PI and MCA-PSV in 30 growth-restricted fetuses with an EFW less than the third percentile. Peri-natal mortality was recorded, and MCA PI and PSV values were classified as normalor abnormal. Forward stepwise logistic regression indicated that the MCA-PSV wasthe best parameter in the prediction of perinatal mortality (odds ratio, 14; 95% confi-dence interval, 1.4–130, P<.05; Nagerlke R[2] 5 31). This finding may be explained bythe fact that the MCA PI in IUGR fetuses can normalize in later stages after becomingabnormally low (ie, reversal of the brain sparing effect); conversely, once the MCA-PSV becomes abnormal, it remains as such.
WHY IS THE MCA-PSV INCREASED IN IUGR FETUSES?
Plausible mechanisms that explain the increase of the MCA-PSV in anemic fetuseshave been elucidated, but IUGR fetuses are not necessarily anemic. There must beanother reason for the increase in the MCA-PSV in this group of fetuses.Akalin-Sel and colleagues91 postulated that hypoxemia alone or with hypercapnia is
responsible for cerebral vascular responses as part of the complex group of regulatorymechanisms that play a role in the circulatory redistribution in human fetal growthrestriction.Hanif and colleagues92 performed a study demonstrating that the mechanisms that
determine increased MCA-PSV in anemic AGA fetuses are different from those in non-anemic IUGR fetuses. Two groups of fetuses were studied: one included 14 fetuses atrisk for anemia because of red cell alloimmunization and the other included 22 IUGRfetuses. The hemoglobin concentration and level of umbilical vein blood gases weredetermined in both groups. The relationship between the MCA-PSV and the hemo-globin concentration, PO2, PCO2, and pH values were assessed by regression analysisusing multiples of the mean in the 2 groups. In the group at risk for anemia, the fetalhemoglobin concentration was the only parameter related to the MCA-PSV (R2 50.34, P<.05). In fetuses with IUGR, the PCO2 (R
2 5 0.36, P<.01) and the PO2 (R2 5 0.30,
P<.01) correlated well with the MCA-PSV, but no relationship was found between theMCA-PSV and the hemoglobin concentration. In anemic fetuses, the high MCA-PSV is
MCA Doppler and its Applications in Fetal Anemia and Growth Restriction 95
related to a decreased fetal hemoglobin concentration that is thought to be respon-sible for the decrease in blood viscosity and consequently an increased cardiacoutput. In IUGR fetuses, the MCA-PSV increase is related to hypoxemia and hyper-capnia and thus to brain autoregulation.
WHERE DO THE MCA DOPPLER ABNORMALITIES FIT IN THE SEQUENCE OF ABNORMALFETAL TESTING IN IUGR?
The decreased MCA PI has been historically regarded as an early finding in thesequence of abnormal testing in IUGR, whereas its reversal and an abnormal increasehave been described as a late finding.86–88 Reverse end-diastolic flow in the MCA hasbeen anecdotally described in the literature as an agonal sign, although it is possible toiatrogenically create this when applying pressure over the fetal cranium with the ultra-sound probe.89 Hecher and colleagues93 serially assessed 93 IUGR fetuses andreported a sequence of appearance of abnormal findings in fetal testing. The firstparameter to become abnormal was the amniotic fluid index, followed by the PI inthe UA, MCA, and aorta, and lastly ductus venosus, inferior vena cava and fetal heartrate short term variability. Baschat and colleagues94 reported changes in fetal well-being testing related to the time of delivery or stillbirth. Doppler abnormalitiespreceded biophysical profile deterioration. The researchers noted 3 patterns ofDoppler deterioration. Most patients (72%) followed a particular sequence: abnormalUA PI and brain sparing effect followed by venous Doppler deterioration, which iscompatible with what Hecher and colleagues reported. Ferrazi and colleagues95
obtained similar results. Mari and colleagues96 reported that the above mentionedsequence in 10 fetuses with IUGR followed this order: abnormal UA PI, MCA PI,ductus venosus, and then MCA-PSV. Once again the pattern was reproduced.After following 104 fetuses with IUGR, Turan and colleagues97 reported that the
characteristics of the cardiovascular changes in IUGR depend on gestational age atonset and severity of the placental disease.There is an important limitation to the evidence available. IUGR cases are studied as
a single noxa, which may explain the conflicting areas in the literature. We believe thatIUGR fits better into the category of a syndrome, in which the restriction of growth isthe end point (something in common) for different pathologic entities. To better eluci-date the causes and consequences of IUGR, studies should discriminate among thedifferent causes that lead to the syndromic IUGR.74 Our group believes that IUGRfetuses should be divided into several categories, based on the specific maternal orfetal abnormality or the absence of any abnormality.74
PERFORMING AND INTERPRETING FETAL MCA DOPPLER WHEN IUGR IS SUSPECTED
The literature on Doppler is saturated with many studies that have performed Doppleranalysis on 3 continuous waveforms, selected more often from a group of 5 to 15waveforms. We believe this is insufficient, especially when basing clinical decisionson these results. This belief has been supported by the results of recent studies.98–100
Several vessels can have abnormal waveforms following maternal contractions orfollowing a fetal deceleration.101,102 Therefore, incorrect or unreliable data can beobtained if clinicians limit themselves to 3 waveforms.In our institution, a Doppler examination usually ranges between 20 and 60 minutes.
In severe IUGR fetuses, between 500 and 1000 waveforms are obtained for eachvessel at each exam. By studying somany waveforms, it is more likely to clearly under-stand the vascular changes occurring in IUGR fetuses, while being practical enoughfor sonographers to complete the studies even in a busy ultrasonography unit. The
Schenone & Mari96
best approach is one that includes the assessment of the UA and the MCA on 1 to 3different occasions and 5 to 10 minutes apart in the absence of fetal movements andbreathing. In each set, at least 10 to 15 waveforms should be obtained. If the quality ofthe waveforms is good, the analysis can be performed either on all the waveforms oron 3 waveforms from each set.There are 3 possible scenarios. First, the first set of waveforms has a normal PI. If
this is the case, then it is not necessary to obtain the next 2 sets and the PI value isconsidered normal. In such cases, the UA and the MCA Doppler are repeated in 2weeks if the gestational age is less than 30 weeks and in 1 week if the gestationalage is greater than 30 weeks. If the PI values remain normal at the following Dopplerexam, the fetus is considered to be a constitutionally small fetus and further Dopplerscans are not carried out.Second, if the UA or the MCA has an abnormal PI in the first set of waveforms, the
other 2 sets of waveforms are obtained. If the PI is abnormal in the following 2 setsalso, an average of the 3 sets is obtained, and the conclusion is that the overall valueis abnormal.Third, if the waveforms have different values, that is, an abnormal PI in the first set
and a normal PI in the second or third set, the conclusion is that the waveforms repre-sent a transitional phase. This transitional phase precedes the abnormal phase.98
In the presence of IUGR cases with an abnormal PI value, investigators and clini-cians use different protocols because there are no clear data on the subject to suggestthe use of one approach versus another. We have previously reported our method-ology when managing IUGR cases with an abnormal UA Doppler.25
SUMMARY
The MCA Doppler examination is a great resource in the diagnosis and managementof fetal anemia and IUGR. As a window into the hemodynamics of the fetal centralnervous system, its potential is clearly unlimited. In cases of IUGR, the MCA Dopplerflow velocimetry shows early and late changes. The PSV is proposed as a desirableparameter in every evaluation of IUGR fetuses, particularly because it has beendemonstrated to perform better than other parameters in the prediction of perinatalmortality. Further research is needed, especially studies that discriminate amongthe different types of IUGR. In cases of fetal anemia, it is widely accepted that theMCA-PSV should be used in the diagnosis and management of cases. Furtherresearch is suggested to address the utility of this method in the prediction of anemiain fetuses after 35 weeks of gestation.
REFERENCES
1. Bevis DC. The composition of liquor amnii in haemolytic disease of the newborn.J Obstet Gynaecol Br Emp 1953;60(2):244–51.
2. Liley AW. Liquor amnil analysis in the management of the pregnancy compli-cated by rhesus sensitization. Am J Obstet Gynecol 1961;82:1359–70.
3. Daffos F, Capella-Pavlovsky M, Forestier F. Direct collection of fetal blood fromthe umbilical vein under echography. First results, prospects. Presse Med1983;12(16):1017 [in French].
4. Woo JS, Liang ST, Lo RL, et al. Middle cerebral artery Doppler flow velocitywaveforms. Obstet Gynecol 1987;70(4):613–6.
5. Kirkinen P, Muller R, Huch R, et al. Blood flow velocity waveforms in human fetalintracranial arteries. Obstet Gynecol 1987;70(4):617–21.
MCA Doppler and its Applications in Fetal Anemia and Growth Restriction 97
6. Satoh S, Koyanagi T, Hara K, et al. Developmental characteristics of blood flowin the middle cerebral artery in the human fetus in utero, assessed using thelinear-array pulsed Doppler method. Early Hum Dev 1988;17(2-3):195–203.
7. Echizenya N, Kagiya A, Tachizaki T, et al. Significance of velocimetry asa monitor of fetal assessment and management. Fetal Ther 1989;4(4):188–94.
8. Ishimatsu J, Hotta M, Matsunaga T, et al. Cerebral artery blood flow velocitywaveforms in normal and small for dates fetuses. Kurume Med J 1989;36(4):181–4.
9. Arstrom K, Eliasson A, Hareide JH, et al. Fetal blood velocity waveforms innormal pregnancies. A longitudinal study. Acta Obstet Gynecol Scand 1989;68(2):171–8.
10. Mari G, Moise KJ Jr, Deter RL, et al. Doppler assessment of the pulsatility indexin the cerebral circulation of the human fetus. Am J Obstet Gynecol 1989;160(3):698–703.
11. van den Wijngaard JA, Groenenberg IA, Wladimiroff JW, et al. Cerebral Dopplerultrasound of the human fetus. Br J Obstet Gynaecol 1989;96(7):845–9.
12. Satoh S, Koyanagi T, Fukuhara M, et al. Changes in vascular resistance in theumbilical and middle cerebral arteries in the human intrauterine growth-retarded fetus, measured with pulsed Doppler ultrasound. Early Hum Dev1989;20(3–4):213–20.
13. Veille JC, Cohen I. Middle cerebral artery blood flow in normal and growth-retarded fetuses. Am J Obstet Gynecol 1990;162(2):391–6.
14. Mari G, Kirshon B, Moise KJ Jr, et al. Doppler assessment of the fetal and ute-roplacental circulation during nifedipine therapy for preterm labor. Am J ObstetGynecol 1989;161(6 Pt 1):1514–8.
15. Lima MM, Souza AS, Diniz C, et al. Doppler velocimetry of the uterine, umbilicaland fetal middle cerebral arteries in pregnant women undergoing tocolysis withoral nifedipine. Ultrasound Obstet Gynecol 2009;34(3):311–5.
16. Guclu S, Gol M, Saygili U, et al. Nifedipine therapy for preterm labor: effects onplacental, fetal cerebral and atrioventricular Doppler parameters in the first 48hours. Ultrasound Obstet Gynecol 2006;27(4):403–8.
17. Pirhonen JP, Erkkola RU, Ekblad UU. Uterine and fetal flow velocity waveforms inhypertensive pregnancy: the effect of a single dose of nifedipine. Obstet Gyne-col 1990;76(1):37–41.
18. Cobellis L, De Luca A, Pecori E, et al. Mid-trimester fetal-placental velocimetryresponse to nifedipine may predict early the onset of pre-eclampsia. In Vivo2006;20(1):183–6.
19. Hata T, Manabe A, Hata K, et al. Changes in blood velocities of fetal circulationin association with fetal heart rate abnormalities: effect of sublingual administra-tion of nifedipine. Am J Perinatol 1995;12(2):80–1.
20. Mari G, Moise KJ Jr, Deter RL, et al. Doppler assessment of the pulsatility indexof the middle cerebral artery during constriction of the fetal ductus arteriosusafter indomethacin therapy. Am J Obstet Gynecol 1989;161(6 Pt 1):1528–31.
21. Parilla BV, Tamura RK, Cohen LS, et al. Lack of effect of antenatal indomethacinon fetal cerebral blood flow. Am J Obstet Gynecol 1997;176(6):1166–9 [discus-sion: 1169–71].
22. Mari G, Abuhamad AZ, Keller M, et al. Is the fetal brain-sparing effect a riskfactor for the development of intraventricular hemorrhage in the preterm infant?Ultrasound Obstet Gynecol 1996;8(5):329–32.
23. Kirkinen P, Orden MR, Partanen K. Cerebral blood flow changes associated withfetal intracranial hemorrhages. Acta Obstet Gynecol Scand 1997;76(4):308–12.
Schenone & Mari98
24. Kawamura A, Yamada H, Nagao T, et al. Posterior cerebral aneurysm associ-ated with complete occlusion of the middle cerebral artery caused subarach-noid hemorrhage: a case report. No Shinkei Geka 1996;24(12):1107–11 [inJapanese].
25. Mari G, Deter RL, Carpenter RL, et al. Noninvasive diagnosis by Doppler ultra-sonography of fetal anemia due to maternal red-cell alloimmunization. Collabo-rative Group for Doppler Assessment of the Blood Velocity in Anemic Fetuses.N Engl J Med 2000;342(1):9–14.
26. Mari G, Moise KJ Jr, Deter RL, et al. Flow velocity waveforms of the umbilical andcerebral arteries before and after intravascular transfusion. Obstet Gynecol1990;75(4):584–9.
27. Mari G, Moise KJ, Kirshon B, et al. Middle cerebral artery pulsatility index andmaximal velocity as indicators of fetal anemia. Paper presented at the Societyfor Gynecologic Investigation. St Louis (MO), March, 1990.
28. Vyas S, Nicolaides KH, Campbell S. Doppler examination of the middle cerebralartery in anemic fetuses. Am J Obstet Gynecol 1990;162(4):1066–8.
29. Fan FC, Chen RY, Schuessler GB, et al. Effects of hematocrit variations onregional hemodynamics and oxygen transport in the dog. Am J Physiol 1980;238(4):H545–52.
30. Hecher K, Snijders R, Campbell S, et al. Fetal venous, arterial, and intracardiacblood flows in red blood cell isoimmunization. Obstet Gynecol 1995;85(1):122–8.
31. Mari G, Adrignolo A, Abuhamad AZ, et al. Diagnosis of fetal anemia withDoppler ultrasound in the pregnancy complicated by maternal blood groupimmunization. Ultrasound Obstet Gynecol 1995;5(6):400–5.
32. Mari G, Rahman F, Olofsson P, et al. Increase of fetal hematocrit decreases themiddle cerebral artery peak systolic velocity in pregnancies complicated byrhesus alloimmunization. J Matern Fetal Med 1997;6(4):206–8.
33. Teixeira JM, Duncan K, Letsky E, et al. Middle cerebral artery peak systolicvelocity in the prediction of fetal anemia. Ultrasound Obstet Gynecol 2000;15(3):205–8.
34. Kowalczyk D, Guzikowski W, Kubicki J, et al. Doppler measurements of bloodflow in the middle cerebral artery for the diagnosis of fetal anemia. GinekolPol 2003;74(10):1160–5 [in Polish].
35. Ahmed B, Ghaffari Z, Ismail RS, et al. Non-invasive diagnosis of fetal anemiadue to maternal red-cell alloimmunization. Saudi Med J 2005;26(2):256–9.
36. L’Ubusky M, Prochazka M, Santavy J, et al. Contribution of Doppler examinationin pregnancy at risk of alloimune fetus anemia. Ceska Gynekol 2005;70(1):27–9[in Czech].
37. Bullock R, Martin WL, Coomarasamy A, et al. Prediction of fetal anemia in preg-nancies with red-cell alloimmunization: comparison of middle cerebral arterypeak systolic velocity and amniotic fluid OD450. Ultrasound Obstet Gynecol2005;25(4):331–4.
38. Collins CY, Ott WJ. Evaluating suspected fetal anemia with Doppler ultrasound.J Reprod Med 2005;50(6):379–82.
39. Oepkes D, Seaward PG, Vandenbussche FP, et al. Doppler ultrasonographyversus amniocentesis to predict fetal anemia. N Engl J Med 2006;355(2):156–64.
40. Nardozza LM, Moron AF, Araujo Junior E, et al. Rh alloimmunization: Doppler oramniotic fluid analysis in the prediction of fetal anemia? Arch Gynecol Obstet2007;275(2):107–11.
MCA Doppler and its Applications in Fetal Anemia and Growth Restriction 99
41. Ochoa-Torres MA, Hernandez-Herrera RJ, Luna-Garcia SA, et al. Usefulness ofDoppler ultrasonography to detect fetal anemia in Rh alloimmunized pregnan-cies. Rev Med Inst Mex Seguro Soc 2007;45(3):219–23 [in Spanish].
42. Maciuleviciene R, Gaurilcikas A, Simanaviciute D, et al. Fetal middle cerebralartery Doppler velocimetry in cases of rhesus alloimmunization. J Matern FetalNeonatal Med 2008;21(6):361–5.
43. Mari G, Penso C, Sbracia M, et al. Delta OD450 and doppler velocimetry of themiddle cerebral artery peak velocity in the evaluation for fetal alloimmune hemo-lytic disease: Which is best? Am J Obstet Gynecol 1997;180(Suppl):18.
44. Pereira L, Jenkins TM, Berghella V. Conventional management of maternal redcell alloimmunization compared with management by Doppler assessment ofmiddle cerebral artery peak systolic velocity. Am J Obstet Gynecol 2003;189(4):1002–6.
45. American College of Obstetricians and Gynecologists. ACOG Practice BulletinNo. 75: management of alloimmunization. Obstet Gynecol 2006;108(2):457–64.
46. Abel DE, Grambow SC, Brancazio LR, et al. Ultrasound assessment of the fetalmiddle cerebral artery peak systolic velocity: A comparison of the near-fieldversus far-field vessel. Am J Obstet Gynecol 2003;189(4):986–9.
47. Moise KJ Jr. The usefulness of middle cerebral artery Doppler assessment in thetreatment of the fetus at risk for anemia. Am J Obstet Gynecol 2008;198(2):161,e161–4.
48. Detti L, Mari G, Akiyama M, et al. Longitudinal assessment of the middle cere-bral artery peak systolic velocity in healthy fetuses and in fetuses at risk foranemia. Am J Obstet Gynecol 2002;187(4):937–9.
49. Mari G, Abuhamad AZ, Cosmi E, et al. Middle cerebral artery peak systolicvelocity: technique and variability. J Ultrasound Med 2005;24(4):425–30.
50. Detti L, Oz U, Guney I, et al. Doppler ultrasound velocimetry for timing thesecond intrauterine transfusion in fetuses with anemia from red cell alloimmuni-zation. Am J Obstet Gynecol 2001;185(5):1048–51.
51. El Bouhmadi A, Boulot P, Laffargue F, et al. Rheological properties of fetal redcells with special reference to aggregability and disaggregability analyzed bylight transmission and laser backscattering techniques. Clin Hemorheol Micro-circ 2000;22(2):79–90.
52. Zimmerman R, Carpenter RJ Jr, Durig P, et al. Longitudinal measurement ofpeak systolic velocity in the fetal middle cerebral artery for monitoring pregnan-cies complicated by red cell alloimmunisation: a prospective multicentre trialwith intention-to-treat. BJOG 2002;109(7):746–52.
53. van Dongen H, Klumper FJ, Sikkel E, et al. Non-invasive tests to predict fetalanemia in Kell-alloimmunized pregnancies. Ultrasound Obstet Gynecol 2005;25(4):341–5.
54. Vaughan JI, Warwick R, Letsky E, et al. Erythropoietic suppression in fetalanemia because of Kell alloimmunization. Am J Obstet Gynecol 1994;171(1):247–52.
55. Vaughan JI, Manning M, Warwick RM, et al. Inhibition of erythroid progenitorcells by anti-Kell antibodies in fetal alloimmune anemia. N Engl J Med 1998;338(12):798–803.
56. Delle Chiaie L, Buck G, Grab D, et al. Prediction of fetal anemia with Dopplermeasurement of the middle cerebral artery peak systolic velocity in pregnanciescomplicated by maternal blood group alloimmunization or parvovirus B19 infec-tion. Ultrasound Obstet Gynecol 2001;18(3):232–6.
Schenone & Mari100
57. Cosmi E, Mari G, Delle Chiaie L, et al. Noninvasive diagnosis by Doppler ultra-sonography of fetal anemia resulting from parvovirus infection. Am J ObstetGynecol 2002;187(5):1290–3.
58. Eichbaum M, Gast AS, Sohn C. Doppler sonography of the fetal middle cerebralartery in the management of massive fetomaternal hemorrhage. Fetal DiagnTher 2006;21(4):334–8.
59. Leung WC, Oepkes D, Seaward G, et al. Serial sonographic findings of fourfetuses with homozygous alpha-thalassemia-1 from 21 weeks onwards. Ultra-sound Obstet Gynecol 2002;19(1):56–9.
60. Dashe JS, Ramus RM, Santos-Ramos R, et al. Middle cerebral artery peaksystolic velocity in monochorionic and dichorionic twin pregnancies.J Ultrasound Med 2007;26(2):195–200.
61. Klaritsch P, Deprest J, Van Mieghem T, et al. Reference ranges for middle cere-bral artery peak systolic velocity in monochorionic diamniotic twins: a longitu-dinal study. Ultrasound Obstet Gynecol 2009;34(2):149–54.
62. Senat MV, Loizeau S, Couderc S, et al. The value of middle cerebral artery peaksystolic velocity in the diagnosis of fetal anemia after intrauterine death of onemonochorionic twin. Am J Obstet Gynecol 2003;189(5):1320–4.
63. Kontopoulos EV, Quintero RA. Assessment of the peak systolic velocity of themiddle cerebral artery in twin-twin transfusion syndrome. Part I: preoperativeassessment. Am J Obstet Gynecol 2009;200(1):61, e61–5.
64. Pathak B, Quintero R, Kontopoulos E, et al. Postoperative middle cerebral arterypeak systolic velocity changes confirm physiological principles of the sequentiallaser technique for twin-twin transfusion syndrome. Fetal Diagn Ther 2010;28(3):140–4.
65. Battaglia FC, Lubchenco LO. A practical classification of newborn infants byweight and gestational age. J Pediatr 1967;71(2):159–63.
66. Lubchenco LO, Hansman C, Dressler M, et al. Intrauterine growth as estimatedfrom liveborn birth-weight data at 24 to 42 weeks of gestation. Pediatrics 1963;32:793–800.
67. Creasy RK, Resnik R, Iams JD, editors. Creasy and Resnik’s maternal-fetalmedicine: principles and practice. 6th edition. Philadelphia: Saunders/Elsevier;2009. p. 635.
68. Donald I, Macvicar J, Brown TG. Investigation of abdominal masses by pulsedultrasound. Lancet 1958;1(7032):1188–95.
69. Shepard MJ, Richards VA, Berkowitz RL, et al. An evaluation of two equations forpredicting fetal weight by ultrasound. Am J Obstet Gynecol 1982;142(1):47–54.
70. Hadlock FP, Harrist RB, Carpenter RJ, et al. Sonographic estimation of fetalweight. The value of femur length in addition to head and abdomen measure-ments. Radiology 1984;150(2):535–40.
71. Alexander GR, Himes JH, Kaufman RB, et al. A United States national referencefor fetal growth. Obstet Gynecol 1996;87(2):163–8.
72. Deter RL, Rossavik IK,Harrist RB, et al.Mathematicmodeling of fetal growth: devel-opment of individual growth curve standards. Obstet Gynecol 1986;68(2):156–61.
73. Barker DJ, Osmond C. Infant mortality, childhood nutrition, and ischaemic heartdisease in England and Wales. Lancet 1986;1(8489):1077–81.
74. Mari G, Picconi J. Doppler vascular changes in intrauterine growth restriction.Semin Perinatol 2008;32(3):182–9.
75. Mari G, Deter RL. Middle cerebral artery flow velocity waveforms in normal andsmall-for-gestational-age fetuses. Am J Obstet Gynecol 1992;166(4):1262–70.
MCA Doppler and its Applications in Fetal Anemia and Growth Restriction 101
76. Trudinger BJ, Giles WB, Cook CM, et al. Fetal umbilical artery flow velocitywaveforms and placental resistance: clinical significance. Br J Obstet Gynaecol1985;92(1):23–30.
77. FitzGerald DE, Drumm JE. Non-invasive measurement of human fetal circulationusing ultrasound: a new method. Br Med J 1977;2(6100):1450–1.
78. Rizzo G, Arduini D. Fetal cardiac function in intrauterine growth retardation. AmJ Obstet Gynecol 1991;165(4 Pt 1):876–82.
79. Locci M, Nazzaro G, De Placido G, et al. Fetal cerebral haemodynamic adapta-tion: a progressive mechanism? Pulsed and color Doppler evaluation. J PerinatMed 1992;20(5):337–43.
80. Chiba Y, Murakami M. Cerebral blood flow dynamics in fetus. No To Hattatsu1992;24(2):136–9 [in Japanese].
81. Bahado-Singh RO, Kovanci E, Jeffres A, et al. The Doppler cerebroplacentalratio and perinatal outcome in intrauterine growth restriction. Am J Obstet Gyne-col 1999;180(3 Pt 1):750–6.
82. Baschat AA, Gembruch U, Reiss I, et al. Relationship between arterial andvenous Doppler and perinatal outcome in fetal growth restriction. UltrasoundObstet Gynecol 2000;16(5):407–13.
83. Ulrich S, Kalder M, Hitschold T, et al. Prognostic value of Doppler flowmeasurement of the middle cerebral artery for morbidity of premature infantswith null or negative flow in umbilical arteries. Zentralbl Gynakol 1996;118(11):605–9 [in German].
84. Roza SJ, Steegers EA, Verburg BO, et al. What is spared by fetal brain-sparing?Fetal circulatory redistribution and behavioral problems in the general popula-tion. Am J Epidemiol 2008;168(10):1145–52.
85. Konje JC, Bell SC, Taylor DJ. Abnormal Doppler velocimetry and blood flowvolume in the middle cerebral artery in very severe intrauterine growth restric-tion: is the occurrence of reversal of compensatory flow too late? BJOG 2001;108(9):973–9.
86. Rowlands DJ, Vyas SK. Longitudinal study of fetal middle cerebral artery flowvelocity waveforms preceding fetal death. Br J Obstet Gynaecol 1995;102(11):888–90.
87. Erz W, Gonser M. Doppler ultrasound of the middle cerebral artery: pre-finalnormalization of cerebrovascular circulation? Geburtshilfe Frauenheilkd 1995;55(7):407–10 [in German].
88. Chitrit Y, Zorn B, Filidori M, et al. Ominous normalization of middle cerebralartery flow velocity waveforms preceding fetal death: case report. Fetal DiagnTher 1995;10(2):106–10.
89. Sepulveda W, Shennan AH, Peek MJ. Reverse end-diastolic flow in the middlecerebral artery: an agonal pattern in the human fetus. Am J Obstet Gynecol1996;174(5):1645–7.
90. Mari G, Hanif F, Kruger M, et al. Middle cerebral artery peak systolic velocity:a new Doppler parameter in the assessment of growth-restricted fetuses. Ultra-sound Obstet Gynecol 2007;29(3):310–6.
91. Akalin-Sel T, Nicolaides KH, Peacock J, et al. Doppler dynamics and theircomplex interrelation with fetal oxygen pressure, carbon dioxide pressure,and pH in growth-retarded fetuses. Obstet Gynecol 1994;84(3):439–44.
92. Hanif F, Drennan K, Mari G. Variables that affect the middle cerebral artery peaksystolic velocity in fetuses with anemia and intrauterine growth restriction. Am JPerinatol 2007;24(8):501–5.
Schenone & Mari102
93. Hecher K, Bilardo CM, Stigter RH, et al. Monitoring of fetuses with intrauterinegrowth restriction: a longitudinal study. Ultrasound Obstet Gynecol 2001;18(6):564–70.
94. Baschat AA, Gembruch U, Harman CR. The sequence of changes in Dopplerand biophysical parameters as severe fetal growth restriction worsens. Ultra-sound Obstet Gynecol 2001;18(6):571–7.
95. Ferrazzi E, Bozzo M, Rigano S, et al. Temporal sequence of abnormal Dopplerchanges in the peripheral and central circulatory systems of the severelygrowth-restricted fetus. Ultrasound Obstet Gynecol 2002;19(2):140–6.
96. Mari G, Deter R, Hanif F, et al. Sequence of cardiovascular changes occurring insevere IUGR fetuses – part II. Ultrasound Obstet Gynecol 2006;28:390.
97. Turan OM, Turan S, Gungor S, et al. Progression of Doppler abnormalities inintrauterine growth restriction. Ultrasound Obstet Gynecol 2008;32(2):160–7.
98. Picconi JL, Hanif F, Drennan K, et al. The transitional phase of ductus venosusreversed flow in severely premature IUGR fetuses. Am J Perinatol 2008;25(4):199–203.
99. Picconi JL, Kruger M, Mari G. Ductus venosus S-wave/isovolumetric A-wave(SIA) index and A-wave reversed flow in severely premature growth-restrictedfetuses. J Ultrasound Med 2008;27(9):1283–9.
100. Fu J, Olofsson P. Fetal ductus venosus, middle cerebral artery and umbilicalartery flow responses to uterine contractions in growth-restricted human preg-nancies. Ultrasound Obstet Gynecol 2007;30(6):867–73.
101. Devoe L, Golde S, Kilman Y, et al. A comparison of visual analyses of intrapar-tum fetal heart rate tracings according to the new National Institute of ChildHealth and Human Development guidelines with computer analyses by an auto-mated fetal heart rate monitoring system. Am J Obstet Gynecol 2000;183(2):361–6.
102. Dawes GS, Redman CW, Smith JH. Improvements in the registration and anal-ysis of fetal heart rate records at the bedside. Br J Obstet Gynaecol 1985;92(4):317–25.





























