Embed Size (px)
Citation preview

Arncncafl /ouma/ o /Or lhop~yc / t lahy , 77(4), Cktober 2001 0 2001 American Orthopsychiatnc Associahon, Inc.
The Mental Health and Biosocial Context of Help- Seeking in Longitudinal Perspective: The Midtown Longitudinal Study, 1954 to 1974
Ernest Joel Millman, Ph.D., M.P.H.
This study o f a representative community suwirior sample of 695 respondents from the 1954 Midtoilin Manhattan Study found that parental socioeconomic status unequiz)ocalli/ predicted help-seeking. Age, gender, adult S E S , and impaired mental Iwalth in 1954 predicted help-seeking interactively. The mental health of help-seekers continued to be unfaziorable, or was worsening, from 1954 to 1974.
-
ommunity studies of psychiatric disorder in the general population have long been a ba- C sis for the planning of mental health ser-
vices (Weissman, Myers, & Ross, 1986). The Epi- demiological Catchment Area study (Robins & Regier, 1991) and the National Comorbidity Study (Kessler et al., 1994) broadened the scope of such research to the United States, which had already been designated as a community for health studies (Sagen, 1970). The findings of these two studies have been contrasted (Blazer (e Kaplan, 2000; Millman, 1998; Regier et al., 1984, 1998) to those of such community studies as the Midtown Man- hattan Study (Srole, Langner, Opler, & Rennie, 1962).
The citation of the Midtown study by such emi- nent scholars as Regier and colleagues over a 14- year period ( 1 984-1 998) indicates the continued applicability of its data to this issue. The Midtown study assessed mental health in a manner compara- ble to Axis V of the DSM-IV (American Psychi- atric Association [APA], 1994; Srole, 1975). It es- timated that, in 1954, 23% of the adult residents in one area of Manhattan had an “impaired” level of mental health. defined as corresponding to a clini- cally significant need for treatment (Millman, 1998; Srole et al., 1978). This prevalence level has
been evaluated as too high to estimate medically necessary treatment need in the general population (Regier. 1998; Regier el al., 1998).
Help-seeking is the response of persons, as- sessed by themselves or significant others as need- ing help, who accept the assessment and have the means to seek help. One way to attempt to strengthen the plausibility of the Midtown mea- surement of impaired mental health as an indicator of treatment need is to determine if help-seeking by the study sample was associated with impaired mental health. An associated concern is whether predictions of help-seeking by impaired mental health are qualified by the biosocial context of help-seeking, defined by age, gender, and socio- economic status (SES), alone or in combination.
Data to address these questions are available from the Midtown Longitudinal Study (MLS), 1954-1974, which interviewed 695 of the original 1,660 Midtown respondents 20 years later (Srole & Fischer, 1980; Srole & Millman, 1998).* The MLS was unprecedented in following up a representa- tive community sample of adults who had partici- pated in a landmark sociopsychiatric epidemiologi-
*These data are available in the 1x0 Srole Archive. llobart and William Smith Colleges. Geneva. N Y 14456: courfesy ot‘ Mrs. Leo Srole
Ernest Joel Millrnm 451
cal study. No statistical study of these data has ex- amined all of the possible predictions of help- seeking that might be made by impaired mental health and the associated biosocial characteristics of age, gender, and SES.
The first goal of the present study is to deter- mine if help-seeking was associated with impaired mental health. Subsidiary to this goal is to deter- mine if 1954 mental health status predicted help- seeking between 1954 and 1974. Another sub- sidiary goal is to elucidate the relationship of help- seeking between 1954 and 1974 to the sample’s mental health status at the beginning and end of this period. The null hypothesis implied by the first goal is that the mental health status of help-seekers was not different from that of non-help-seekers in either I954 or 1974.
The second study goal is to determine if the as- sociation of mental health status and help-seeking varies when the biosocial context of help-seeking varies. Variations in biosocial context are defined as combinations of levels of age, gender, and SES, both parental and own as an adult. The implied nul l hypothesis is that neither 1954 mental health status nor biosocial characteristics, alone or in combination, predicted help-seeking.
METHOD Snniyliizg yrocediires. The MLS was not a
planned follow-up study (Srole & Fischer, 1980; Srole R Millman, 1998). A research team directed by the late Leo Srole, MLS principal investigator, established that an adequate representative sur- vivor sample of the 1,660 respondents could be re- located (Srole R Millman, 1998). Of 858 living re- located respondents, 695 ( 8 1 %) were reinter- viewed and form the MLS sample.
Mrnsiirerireiit procediires. Although the 1954 in- terview had been comprehensive in its coverage of the respondents’ biopsychosocial characteristics and personal history, taking on average 90 minutes (Srole c ~ t a1.- lY62). the 1974 interview was even more extensive. requiring on average I80 minutes. MLS measures were based both on the 1954 and 1974 interviews.
Mc’ritnl Iicnltli. In 1954. two psychiatrists re- viewed data summary sheets for each of the 1,660 respondents and. on that basis, rated the global mental health of each respondent. defined as the level of strain in adult role functioning. This rating coincided with the psychiatrists’ rating of need for mental health treatment. The rating included six
levels: well, mild, moderate, marked, severe, and incapacitated. The marked through incapacitated levels were often combined to form an impaired level, which was the benchmark of clinically sig- nificant need for mental health treatment (Millman, 1998; Srole et al., 1962, 1978). The 1954 interview had included 83 adult symptom and interviewer observation items. These were also included in the 1974 interview. Multiple regression analysis was used to reproduce the psychiatrists’ ratings (Singer, Cohen, Garfinkel, & Srole, 1976; Srole & Millman, 1998). The psychiatrists’ ratings were satisfactorily reproduced (Pearson zero-order cor- relation r=0.78, p<.OOOOO5; Spearman correla- tion=0.75, p<.000005; Kappa=0.40). The regres- sion-based measure of mental health status is re- ferred to as MH54.
The regression findings were then applied to the 1974 data to yield the 1974 measure, referred to as MH74, commensurate with MH54.
Socioecoiiomic status. The rationale for these SES measures has been described in detail (Lang- ner & Michael, 1963; Srole et al., 1962, 1978; Srole & Millman, 1998). Parental socioeconomic status (SESPAR) was a composite of the father’s level of occupation and the father’s level of education, col- lapsed into three approximately equal levels.
The measure of the Midtown respondents’ own level of SES in 1954 (SES54) was a composite pri- marily of their levels of occupation, education, in- come, and rent, collapsed into three approximately equal levels.
Help-seeking. MLS participants were coded as “ I ” if they responded affirmatively (or “0” other- wise) to any of the following three items in the 1974 interview: I . People sometimes go to a hospital or nursing home for an cmotional or nervous condition. Of course, these too are medi- cal problems treated by doctors and nurses. Have you ever been in a hospital or nursing home for such an emotional or nervous condition’? 2 . Have you ever gone to a hospital clinic or non-hospital clinic for an emotional or nervous condition? How old were you when you went to such a clinic for the first time‘? 3 . To get help for an emotional problem or nervous condition people also go to other kinds of professionals outside ofa hos- pital or clinic. For such personal problems have you ever gone to a private psychiatrist, psychologist. counselor. clergyman, social worker, group therapist. or other similar kind of profes- sional?
Class$cation procedures. All variables are cate- gorical. The dependent measure is help-seeking. The independent biosocial measures are: level of age, 1=20-39 in 1954, 2=40-59 in 1954; gender,
452
1 =males, 2=females; and SESPAR and SES54, 1 =lower, 2=middle, 3=higher. The six-point men- tal health ratings (MH54 and MH74) were some- times collapsed into three levels: I=well, 2=mild- to-moderate; 3=impaired (comprising marked, severe, and incapacitated). To indicate clinically significant need for mental health treatment in 1954, MH54 was sometimes coded I =impaired mental health in 1954,O=not impaired.
Statistical procedures. Standard statistical pro- cedures are used, primarily crosstabulation and multiple logistic regression (Bishop, Fienberg, & Holland, 1975). The criterion for statistical signifi- cance is 0.05, two-tailed if possible. Cross-tabula- tions are statistically assessed using Pearson’s Chi- Square, with Yates’s correction for attenuation when df-1; McNemar’s Chi-square for Symmetry (X2McN), with correction for attenyation; and the McNemar Odds Ratio (ORMcN). x McN provides an overall test of the null hypothesis that the probabil- ity that respondents had more favorable levels of mental health in 1974 than in 1954 was equal to the probability that respondents had less favorable levels of MH74 than MH54. ORMcN measures the relative likelihood that respondents would have fa- vorable (versus unfavorable) changes in mental health from 1954 to 1974. Findings from multiple logistic regression analyses were assessed using the model chi-square. Using the sheltering strat- egy, individual coefficients were interpreted only if the model chi-square was statistically significant (Cohen & Cohen, 1983; Millman, 1997).
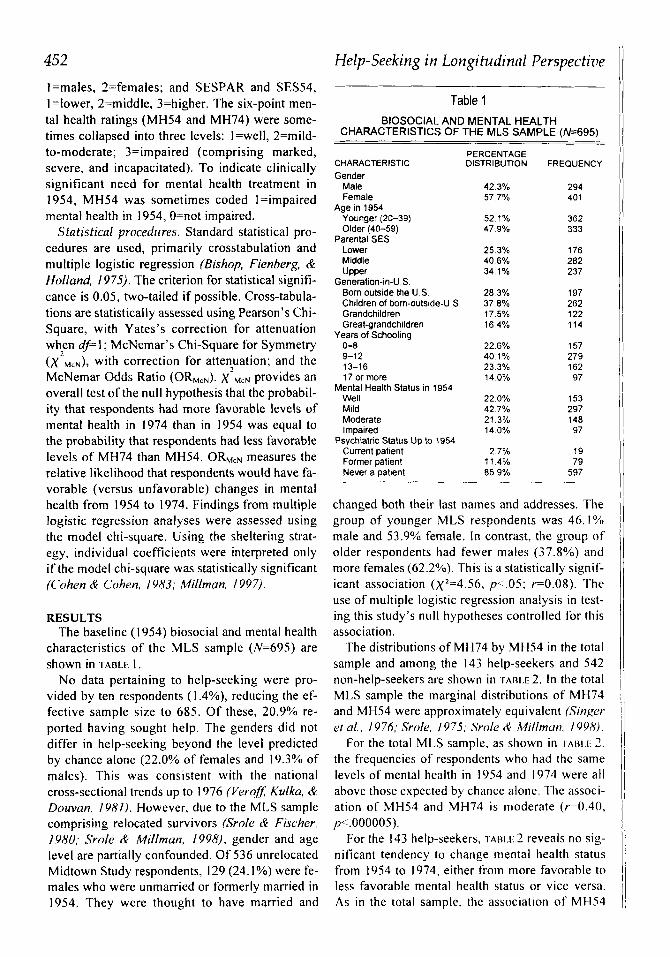
RESULTS The baseline ( 1 954) biosocial and mental health
characteristics of the MLS sample (N=695) are shown in TADLE 1.
No data pertaining to help-seeking were pro- vided by ten respondents (1.4%), reducing the ef- fective sample size to 685. Of these, 20.9% re- ported having sought help. The genders did not differ in help-seeking beyond the level predicted by chance alone (22.0% of females and 19.3% of males). This was consistent with the national cross-sectional trends up to I976 (Verqf, Kulka, & Douvan. I Y N I ) . However, due to the MLS sample comprising relocated survivors (Srofe (e Fischer, 1980; Srole & Millman. 1998), gender and age level are partially confounded. Of 536 unrelocated Midtown Study respondents, 129 (24.1 YO) were fe- males who were unmarried or formerly married in 1954. They were thought to have married and
Help-Seeking in Longitudinnl Perspective
Table 1 BlOSOClAL AND MENTAL HEALTH
CHARACTERISTICS OF THE MLS SAMPLE (N=695)
PERCENTAGE CHARACTERISTIC DISTRIBUTION FREQUENCY Gender
Male Female
Age in 1954 Younger (20-39) Older (40-59)
Parental SES Lower Middle Upper
Generation-in-U S Born outside the U S Children of born-outside-U S Grandchildren Great-grandchildren
Years of Schooling 0-8 9-1 2 13-16 17 or more
Well Mild Moderate Impaired
Current patient Former patient Never a patient
Mental Health Status in 1954
Psychiatric Status Up to 1954
42 3% 294 57 7% 401
52 1% 362 47 9% 333
25 3% 176 40 6% 282 34 1% 237
28 3% 197 37 8% 262 17 5% 122 16 4% 114
22 6% 157 40 1% 279 23 3% 162 14 0% 97
22 0% 153 42 7% 297 21 3% 148 14 0% 97
2 7% 19 11 4% 79 85 9% 597
changed both their last names and addresses. The group of younger MLS respondents was 46.1% male and 53.9% female. In contrast, the group of older respondents had fewer males (37.8%) and more females (62.2%). This is a statistically signif- icant association (x2=4.56, p<.05; r=0.08). The use of multiple logistic regression analysis in test- ing this study’s nul l hypotheses controlled for this association.
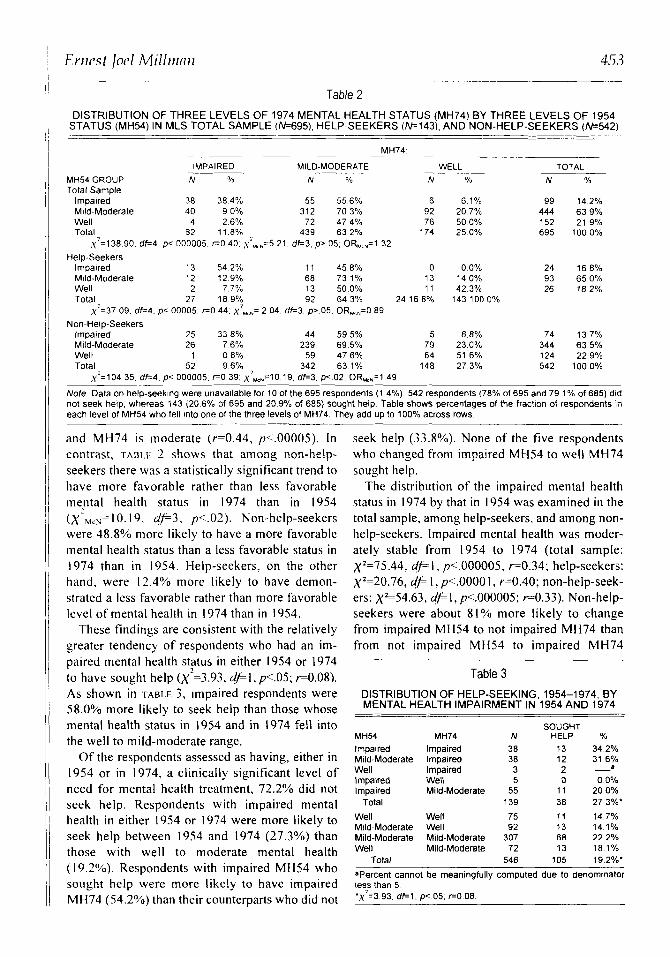
The distributions of MH74 by MH54 in the total sample and among the 143 help-seekers and 542 non-help-seekers are shown in ‘rA1u.E 2. In the total MLS sample the marginal distributions of MH74 and MH54 were approximately equivalent (Singer ei al.. 1976; Srole. 1975; Srole & Millmun. 1998).
For the total MLS sample, as shown in IAIH.I. 7 . the frequencies of respondents who had the same levels of mental health in 1954 and 1974 were all above those expected by chance alone. The associ- ation of MH54 and MH74 i s moderate (r=0.40, p<.000005).
For the 143 help-seekers, i-AB1.f; 2 reveals no sig- nificant tendency to change mental health status from 1954 to 1974. either from more favorable to less favorable mental health status or vice versa. As in the total sample, the association of MHS4
Errirst locl Milliiinri 453 ~ -
Table 2 DISTRIBUTION OF THREE LEVELS OF 1974 MENTAL HEALTH STATUS (MH74) BY THREE LEVELS OF 1954
STATUS (MH54) IN MLS TOTAL SAMPLE (1\1=695), HELP-SEEKERS (M143). AND NON-HELP-SEEKERS (W542) -
MH74
MILD-MODERATE WELL ____ IMPAIRED MH54 GROUP N Oh N Y o N % Total Sample
Impaired 38 384% 55 556% 6 6 1 % Mild-Moderate 40 9 0 % 312 703% 92 207% Well 4 2 6 % 72 474% 76 500% Total. 82 118% 439 63 2% 174 25 0%
,y'=138 90 df=4 p< 000005 G O 40 ~ ' ~ , , = 5 21 df=3 p> 05 OR,,,=l 32 Help-Seekers
Impaired 13 54 2% 1 1 458% 0 0 0 % 13 14 0% Mild-Moderate 12 129% 68 73 1%
Well 2 7 7 % 13 500% 11 42 3% Total 27 189% 92 64 3% 24 16 8% 143 100 0%
,y'=37 09 d k 4 p< 00005 r=O 44 x UrN= 2 04 d e 3 p> 05 OR,,,=O 89 Non-Help-Seekers
Impaired 25 358% 44 595% 5 6 8 % Mdd-Moderate 26 7 6% 239 69 5% 79 230% Well 1 0 8 % 59 476% 64 51 6% Total 52 9 6 % 342 63 1% 148 27 3%
u2=104 35 df=4 D< 000005 F O 39 ~~.,,=10 19 df=3 D< 02 OR.,,=l 49
TOTAL N %
99 14 2% 444 63 9% 152 21 9% 695 1000%
24 168% 93 650% 26 182%
74 13 7% 344 63 5% 124 22 9% 542 100 0%
~ ~ ~
Note Data on help-seeking were unavailable for 10 of the 695 respondents (1 4%) 542 respondents (78% of 695 and 79 1% of 685) did not seek help, whereas 143 (20 6% of 695 and 20 9% of 685) sought help Table shows percentages of the fraction of respondents in each level of MH54 who fell into one of the three levels of MH74 They add up to 100% across rows
and MH74 is moderate (r=0.44, p<.00005). In contrast, TAIXE 2 shows that among non-help- seekers there was a statistically significant trend to have more favorable rather than less favorable mental health status in 1974 than in 1954 ( x - ~ ~ ~ = 10.19, 4 p 3 , pc.02). Non-help-seekers were 48.8% more likely to have a more favorable mental health status than a less favorable status in 1974 than in 1954. Help-seekers, on the other hand, were 12.4% more likely to have demon- strated a less favorable rather than more favorable level of mental health in 1974 than in 1954.
These findings are consistent with the relatively greater tendency of respondents who had an im- paired mental health s t p s in either 1954 or 1974 to have sought help (~-=3.93, 4'1, p<.05; ~ 0 . 0 8 ) . As shown in 'TABLE 3. impaired respondents were 58.0% more likely to seek help than those whose mental health status in 1954 and in 1974 fell into the well to mild-moderate range.
Of the respondents assessed as having, either in 1954 or in 1974, a clinically significant level of need for mental health treatment, 72.2% did not seek help. Respondents with impaired mental health in either 1954 or 1974 were more likely to seek help between 1954 and 1974 (27.3%) than those with well to moderate mental health (19.29'0). Respondents with impaired MH54 who sought help were more likely to have impaired MH74 (54.2%) than their counterparts who did not
seek help (33.8%). None of the five respondents who changed from impaired MH54 to well MH74 sought help.
The distribution of the impaired mental health status in 1974 by that in 1954 was examined in the total sample, among help-seekers, and among non- help-seekers. Impaired mental health was moder- ately stable from 1954 to 1974 (total sample: x2=75.44, dp I , p<.000005, r=0.34; help-seekers: x2=20.76, d p I , p<.OOOO I , r=0.40; non-help-seek- ers: xL54.63, dpl, p<.000005; ~ 0 . 3 3 ) . Non-help- seekers were about 81% more likely to change from impaired MH54 to not impaired MH74 than from not impaired MH54 to impaired MH74
Table 3 DISTRIBUTION OF HELP-SEEKING, 1954-1 974, BY MENTAL HEALTH IMPAIRMENT IN 1954 AND 1974
SOUGHT MH54 MH74 N HELP %
Impaired Impaired 38 13 34 2% Mild-Moderate Impaired 38 12 316% Well Impaired 3 2 -a
lmpaired Well 5 0 0 0% Impaired Mild-Moderate 55 11 200%
Total 139 38 273%'
Well Well 75 11 14 7% Mild-Moderate Well 92 13 141% Mild-Moderate Mild-Moderate 307 68 22 2% Well Mild-Moderate 72 13 101%
Total 546 105 192%'
'Percent cannot be meaningfully computed due to denominator less than 5 ',y2=3 93. d e l , p< 05, r=O 08
454 Help-Secking in Longitrrdiiznl Persprc - t i~? was restricted in the 1954 study to exposure to psychotherapists in hospitals, clinics. and private offices. Among impaired respondents. the higher their level of SESS4. the higher was their probabil- ity of having ever been patients: lower, 71.0%: middle, 22.5%; and upper. S I .S?/O. tiowcver the higher their level of SESS4, the lower was their probability of having had impaired rather than well mental health, so that the lower SES group had the greatest probability of impaired mental health and the upper group the least probability. Younger re- spondents were more likely to ever have been pa- tients than older respondents (34.9% vs 12.3%). Finally, when mental health impairment was con- trolled, having ever been a patient was not related to either gender or marital status.
This study of MLS data is limited by its sample size, which lacks the statistical power to sensi- tively evaluate three-way and four-way interaction predictions among biosocial and mental health predictors. Another limitation is the disproportion- ate loss to follow-up of female respondents in the 1954 Midtown Study who were younger (<40 years old) and single. However, the validity of the survivor sample for follow-up purposes was estab- lished by the MLS’s own design consultants.
The MLS is limited by the composition of its sample in other respects. Because the parent study was restricted to white residents of “midtown” Manhattan (Srole ct ul.. lY62) , the ethnicity of the follow-up sample is necessarily all white. Due to the follow-up design, no member of the MLS sam- ple was under 40 years of age in 1974.
MLS study findings are generalizable to the sur- vivors of the community sample in the Midtown Study in 1954. The percentage of respondents who reported having sought help by 1974 (2 I YO) ap- proaches the 26% reported in 1976 for the U.S. adult population, whereas the percentage of re- spondents who had ever been psychiatric patients equaled the 14% reported in 1957 for the U.S. adult population (Verofet a/.. 1981). A historical limitation is that the mental health service system has expanded since 1974, as it had in the years prior to 1954, and from 1954 to 1974 (Witkin cl al., 1998). Concomitantly. insurance coverage for mental health treatment had also expanded. How- ever income and insurance coverage are so closely associated (Alegria, Bij l , Lin, Wulters. & Kessler, 2000) that the SES54 measure can be considered to be a surrogate measure of insurance coverage.
The mental health measure may be viewed as a
(xZb,,..=5.8O, 4‘1, p<.OS). Thus, respondents who did not seek help were significantly more likely than those who did seek help to be on a 20-year course of improved mental health status.*
To assess the predictions by mental health and biosocial characteristics of help-seeking, a hierar- chical logistic multiple regression analysis was done in three stages. The first stage estimated the odds of seeking help as a function of I ) age level, 2) gender (sex), 3) the interaction of age and gen- der, 4) SESPAR, 5) SES54, and 6) impaired men- tal health status in 1954 (IMP54). The results were as follows: The model x’ was 44.17, 4 F 6 , p<.OOOOS. Statistically significant predictions not qualified by two-way interactions were as follows: The younger respondents were 65% more likely to seek help than the older respondents. With each level of increasingly favorable SESPAR. help- seeking was 37% more likely. Help was sought by 12.4% of the lower SESPAR respondents, 18.9% of the middle SESPAR respondents, and 29.5% of the upper SESPAR respondents.
The second stage estimated the odds of seeking help as a function of all pairs of predictors (i.e., all two-way interactions). The model x2 was 16.66, dp9, p<O.OS. A pair of two-way interactions were statistically significant: age X SES54 and sex X IMP54. Model X’S for all three-way and all four- way interactions were not statistically significant. The age X SES54 association was as follows: of the younger respondents, 34.0% with higher SES54, 20.5% with lower SES54, and 20.2% with middle SES54 sought help; of the older respon- dents, 22.8% with higher, 5.2% with lower, and 12.8% with middle SES54 sought help.
The sex x IMP54 association is statistically sig- nificant exclusively among the male respondents. Help was sought by 24.5% of respondents with im- paired MH54. Of those with impaired MH54, 17.0% of the females sought help versus 4 I .9% of the7 males, a statistically significant difference ( ~ - = 7 . 4 3 , + I , p<.Ol; ~ 0 . 2 8 ) .
DISCUSSION The 1954 Midtown Manhattan Study (Srole et
ul., 1962) found that, among respondents in clini- cally significant need of mental health treatment due to impaired mental health. 26.7% had ever been psychiatric patients, versus 9.3% of the oth- ers. The scope of questioning about help-seeking
*Tabular representations of these data and of findings reported in the balance ofthis section are available from the author.
Ernest loel Millmnn 455 limitation, since it does not establish criteria for psychiatric disorders as defined by the DSM (APA, 1994). However, this may not be a limitation but rather a characterization of the treatment need of community respondents in a manner analogous to Axis V of DSM-Ill (APA. 1980: Srole, 1975; Vail- lunt CY. Schnurr, 1988) I
The present study, although limited because it was done nearly 30 years after the data were col- lected, was conceived in response to a proposal by eminent mental health scholars to rethink ways of estimating the need of the general population for mental health treatment--e.g., in view of managed care considerations (Regier, 1998; Regier el al.. 1998). Part of the rethinking was to reassess such classic community studies as the Midtown Study, and explore the possibility of their having overesti- mated that need. By examining in detail the rela- tionship between mental health status at the begin- ning and end of the 1954 to 1974 MLS period to help-seeking from 1954 to 1974, the findings ofthis study have reinforced the estimate of need for men- tal health treatment made by the Midtown Study.
The two-way interaction predictions reported here could not have been anticipated from prior published reports (Holzer et al., 1986; Kadushin, 1968; Srnle et al., 1962, 1978; Veroffet al., 1981). An earlier analysis of MLS data on help-seeking had examined the predictions made by a compli- cated life-span model, including, among many predictors, age, MH54, SESPAR, and SES54, sep- arately for male and female respondents (Millman, IYOS; Srolr R Millman, 1998). This analysis had found that the prediction of help-seeking by im- paired MHS4 held for males only. The study re- ported here describes this phenomenon in one model that accounts for all possible two-way and three-way predictions made by age, gender, MHS4, SESPAR, and SES54.
It was quite expectable on the basis of published studies that the respondents from less socioeco- nomically favorable backgrounds, as measured by SESPAR, would be the least likely to seek help, and that those from the most favorable back- grounds would be most likely to seek help (Holzer crt ul.. 1986; Kudushin, 1968; Srole et al.s 1962, IV7X. Veroffet ul.. 1981). Although the general predictions made in this study by the biosocial pre- dictors are consistent with the time series of corre- lational findings reported on a national scale from 1957 to 1976 (Vrrqfet ul.. 1981), there are more complicated predictions as well.
CONCLUSION The need for help of MLS respondents who
sought treatment between 1954 and 1974 is demonstrated by their mental health status in I954 and 1974. Furthermore. the associations of help- seeking between 1954 and 1974 with impaired mental health in either 1954 or 1974 enhance the plausibility of impaired mental health as an indica- tor of the need for mental health treatment within the biosocial context of help-seeking. The practi- cal implication for current policy and programs lies in the present study’s reinforcement of the ear- lier finding that, up to 1974, there was a substantial portion of the general population that was in need of mental health treatment and that did not receive help (Millman, 1998; Srole & Millman. 1998).
References Alegria, M., Bi.il. R.V.. Lin, E., Walters. E W.. & kessler, R.C.
(2000). Income differences in persons seeking outpatient treatment for mental disorders. Archives of General I’sychi- atry. 57, 383-391.
American Psychiatric Association. ( I 980). Diugnostic andsta- tistical manual of mental disorders (3rd ed.). Washington. DC: Author.
American Psychiatric Association. ( 1994). Diagnostic andsta- tistical manual o/mental disorders (4th ed.). Washington. DC: Author.
Bishop,Y.M.M.. Fienherg, S.E., & Holland P.W. (1975). Dis- crete multivariate analysis: Theory and practice. Cam- bridge, MA: MIT Press.
Blazer, D.G., & Kaplan, B.H. (2000). Commentary: Contro- versies in community-based psychiatric epidemiology-let the data speak for themselves. Archives ofceneral Psychra- try, 57,221-228.
Cohen, J., & Cohen, P. (1983). Applied multiple regres- sion/correlation analysis ,for the hehavroral sciences (2nd ed.). Hillsdale, NJ: Erlhauni.
llolzer, C.E., Shea, B.M., Swanson, J.W., Leaf, P.J.. Meyers, J.K., George, L., Weissman, M.M.. & Bednarski. P.S. (1986). The increased risk for specific psychiatric disorders among persons o f low socioeconomic status. American Journal of Social Psychiatry. 6,259-27 I .
Kadushin, C. (1968). Why people go to psychiatrists. New York: Atherton.
Kessler. R.C., McGonagle. K.A.. Zhao. S.. Nelson. C.B., Hughes, M., Eshleman, S., Wittchen, H.U., & Kendler, K.S. (1994). Lifetime and 12-month prevalence o f DSM-Ill-R psychiatric disorders in the United States: Results from the National Comorhidity Survey. Archives of General Ps.vchi- atry, 51. 8-19.
Langner, T.S.. & Michael, S.T. (1963). Li/e stress and menial health: The Midtown Manhattan Study. New York: Free Press.
Millman. E.J. (1997). Statistical appendices. personal history and health: The Midtown Longitirdinal Study. 1954 to 1974. Ann Arbor, MI: UMI Microfilm LD03613.
Millman, E.J. (1998). Midtown Manhattan prevalence rates and the implied need for treatment: Meeting the challenge ofpublic mental health. Archives o/General Psychiatry, 55, 1146-1 147.
Regier, D.A. (1998). Response to letters to the editor. Archives ?/General Psychiatry. 55, 1147.

456 Help-Seeking in Longitudinal Perspectiae Regier. D.A.. Kaelber, C.T., Rae, D.S., Farmer, M.E., Knau-
per. B.. Kessler, R.C., & Norquist, G.S. (1998). Limitations ol'diagnostic criteria and assessment instruments for mental disorders: Implications for research and policy. Archives of (knrral Psychiatry. 55. 109-1 15.
Regier. D.A.. Meyers. J.K.. Kramer, M.. Robins, L.N.. Blazer. D.G.. tlorigh, R.L., Eaton. W.W., & Locke. B.Z. (1984). .The NlMH Epidemiological Catchment Area Program: Iiis- lorical context, ma.jor objectives, and study population char- acteristics. Archives ofGeneral Psychiatry. 41,933-941.
Robins, L.N., & Regier D.A. (Eds.). (1991). Psychiairicdisor- ders i n America: The Epidemiologic Catchmeni Area Study. New York: Free Press.
Sagen.0. (1970). The llnited States as an epidemiologic labora- lory: An overview. In 1.1. Kessler& M.L. Levin (Eds.), 7he com- munity as an epidemiologic laboratory: A casebook of cam- munity studies(pp.271-278). Baltimore: Johns Hopkins Press.
Singer. E.. C'ohen. S.M., Garfinkel, R., & Srole, L. ( 1 976). Replicating psychiatric ratings through multiple regression analysis: The Midtown Manhattan Restudy. Journal o/ Health Cti Social Behavior. I ? . 376-387.
Srole, 1. (1975). Measurement and classification in sociopsy- chiatric epidemiology: The Midtown Manhattan Study (1954) and Midtown Manhattan Restudy. Journal ofHealth R Social Behavior, 16,347-364.
Srole. L.. & Fischer, A.K. (1980). The Midtown Manhattan 1.ongitudinal Study vs. 'The Mental Paradise Lost' doc- trine: A controversy joined. Archives of General Psychiatry,
Srole, L., Langner, T.S., Michael, S.T., Kirkpatrick, P., Opler, 37.209-22 I .
M.K., & Rennie, T.A.C. (1978). Mental heal/h in the metropolis: The Midtown Manhatian Study. (Revised and enlarged edition.) I . . Srole & A.K. Fischer (Eds.) . New York: New York University Press.
Srole. L.. Langner, T.S., Opler. M.K.. & Rennie. ' I .A.C. (1962). Mental healih in the metropolis. Vol. 1 o f the Mid- town Manhattan Siudy. New York: Mcciraw-Hill
Srole, L., & Millman. E.J. ( 1998). Personal history and health: The Midioivn Longitudinal Siudy. I954 to 1974. New Brunswick, NJ: Transaction Publishers.
Vaillant, G., & Schnurr, P. (1988). What is a case? A 45-year study o f psychiatric impairment o f a college sample se- lected for mental health. Archives of General Psychia/ry.
Veroff, J., Kulka. R.A.,& Douvan, E. (1981). Mentalhealth in America: Parferns of help seekrqq,from 1957 10 1976. Ncw York: Basic Books.
Weissman, M.M., Myers. J.K.. & Ross, C.E. (1986). Commu- nity studies in psychiatric epidemiology: An introduction. In M.M. Weissman, J . K . Myers. & C.F. Ross (Eds.). ('om- munity surveys ofpsychiatric disorders ( p p . 1-19). New Brunswick. NJ: Rutgers llniversity Press.
Witkin, M.J., Atay, J.E., Manderscheid. R.W.. DeLozier. J.. Male, A., & Gillespie, R. (1998). Highlights o f organized mental health services in 1994 and inajor national and state trends. In R.W. Manderscheid & M.J. Henderson (Eds.), Mental health. United States. I998 ( p p . 143-1 69) . Center for Mental Health Services. DHHS Pub. No. (SMA) 99-3285, Washington. DC: U S , Government Printing Of- fice.
45,3 13-3 19.
For reprints Ernest Joel Millman, Ph.D., Harlem Hospital Center/Columbia University, Department of Psvchiatry, 506 I .enox Avenue, WP-5, New York, NY 10037





























