Embed Size (px)
DESCRIPTION
Our mission is to enhance your ability to practice equine medicine by providing the latest info you need.
Citation preview

Vol 5 Issue 4 2015www.modernequinevet.comEquine Vet
The Modern
Managing keratopathyColic, Lameness, New NSAID and More
qPCR good tool foR EHV-1 managEmEnt

2 Issue 4/2015 | ModernEquineVet.com
TAbLe of CoNTeNTS
OPHTHALMOLOGY Goals for treating equine keratopathies .........................................................................8
TecHnIcIAn UPdATecolic associated with Salmonella ....................................................................................13
OrTHOPedIcSSubjective methods for identifying lameness ....................................................16rater agreement in visual lameness assessment during the lunge ........17
newSnew strain of canine influenza ..........................................................................3Aspen Veterinary resources launches new equine nSAId paste ..15Zoetis extends its immunization support guarantee ........................15comparative efficacy of intra-articular medications .............................17
LEGAL DISCLAIMER: The content in this digital issue is for general informational purposes only. PercyBo Publishing Media LLC makes no representations or warranties of any kind about the completeness, accuracy, timeliness, reliability or suitability of any of the information, including content or advertisements, contained in any of its digital content and expressly disclaims liability of any errors or omissions that may be presented within its content. PercyBo Publishing Media LLC reserves the right to alter or correct any content without any obligations. Furthermore, PercyBo disclaims any and all liability for any direct, indirect, or other damages arising from the use or misuse of the information presented in its digital content. The views expressed in its digital content are those of sources and authors and do not necessarily reflect the opinion or policy of PercyBo. The content is for veterinary professionals. ALL RIGHTS RESERVED. Reproduction in whole or in part without permission is prohibited.
qPcr useful tool for managing eHV-1
cOVer STOrY: 4
Cover Photo Courtesy of Dr. Pusterla
SaleS: robin Geller • [email protected]
editor: Marie rosenthal • [email protected]
art director: Jennifer Barlow • [email protected]
contributing writerS: Paul Basillo • Kathleen Ogle
coPY editor: Patty wall
Published by
p E r c y b omedia publishing
Equine VetThe Modern
advertiSerSShanks Veterinary equipment ................................. 3Avalon Medical ............................................................ 6
AAeVT ...........................................................................12
PO Box 935 • Morrisville, PA 19067Marie Rosenthal and Jennifer Barlow, Publishers

ModernEquineVet.com | Issue 4/2015 3
www.shanksvet.com • [email protected]
Lifting Large Animals Since 1957
FYI for those in a mixed animal practice
The canine influenza outbreak afflicting more than 1,000 dogs in chicago and other parts of the Midwest is caused by a different strain of the virus than was ear-lier assumed, according to laboratory scientists at cor-nell University and the University of Wisconsin.
researchers at cornell said results from additional testing indicate that the outbreak is being caused by a virus closely related to Asian strains of influenza A H3N2 viruses, which have been in wide circulation in southern chinese and South Korean dog populations since being identified in 2006. There is no evidence that it can be transmitted to humans.
The outbreak in the Midwest had been attributed to the H3N8 strain of virus, which has been circulating in US dog populations since it was identified in 2004. because the H3N2 virus had not been previously de-tected in North America, this outbreak suggests a re-cent introduction of the H3N2 virus from Asia.
After testing clinical samples from the outbreak, the New york State Animal Diagnostic Laboratory at cornell indicated that the virus was a new strain of influenza A. Subsequent testing, carried out with the assistance of the Wisconsin Veterinary Diagnostic Laboratory, identified the new subtype as H3N2. The National Veterinary Services Laboratories in Ames, Iowa, is sequencing two isolates from this outbreak, which were isolated at cornell, to facilitate rapid com-plete characterization of the viruses.
both Influenza strains can cause high fever, loss of appetite, coughing, nasal discharge and lethargy. Symptoms may be more severe in cases caused by the H3N2 virus. Some infected dogs may not show symp-toms at all. The H3N2 also has caused infection and respiratory illness in cats.
NewS
The canine-specific influenza A H3N8 reverse transciptase polymerase chain reaction (rt-pcr) in use in several laboratories will not detect this virus. Serology is also currently not available as the H3N2 virus is different enough from H3N8 that antibodies may not cross react. Veterinarians are advised that di-agnostic testing of samples from sick pets can be done using a broadly targeted Influenza A matrix rt-pcr assay. An H3N2-specific serologic assay is under de-velopment and will be available soon.
It is unknown if the current vaccine will provide any protection from this new virus. It does protect against H3N8, which is in circulation in some areas.
other preventive advice remains the same: Tell owners that in areas where the viruses are active, avoid places where dogs congregate, such as dog parks and grooming salons. MeV
influenza a: this digitally colorized negative-stained transmission electron micograph (teM) depicted a number of influenza a virions.
Midwest canine influenza outbreak caused by new virus strain
Cynt
hia G
oldsm
ith, C
DC

4 Issue 4/2015 | ModernEquineVet.com
adult QH mare with hindlimb weakness and incoordination kept in a homemade sling.

ModernEquineVet.com | Issue 4/2015 5
Phot
o cou
rtesy
of D
r. Pus
terla
Quantitative testing with polymerase chain reaction (qpcr) might provide better information for a veterinarian trying to de-cide how to manage a particular outbreak of equine herpes virus 1 (EHV-1), according to nicola Pusterla, DrMedVet, phD, profes-sor of equine medicine at the Uni-versity of california at Davis col-lege of Veterinary Medicine.
“There is a need to refine EHV-1 diagnostics to better de-termine and better assess the stage of the virus and disease form, but also to help the practi-tioner better interpret the results when making biosecurity deci-sions,” Dr. pusterla said.
Although every diagnostic laboratory does not offer qpcr, it can be useful for characterizing the stage and viral load of the virus and for monitoring the response to treatment, he explained. And
the results would not only apply to clinically infected animals, but also the asymptomatic shedder, which is a real cause for concern, he said at the 60th annual meeting of the American Association of Equine practitioners in Salt Lake city, Utah.
In studies done by Dr. pusterla and his colleagues, they found that the viral load in the nasal se-cretions of asymptomatic horses could range from very low to very high, meaning that some of them could shed virus at the same level of a clinically affected animal.
“Truly these are the horses that make me nervous,” Dr. pusterla said. “This is the everyday horse that comes into the clinic; the one that looks healthy. It is very diffi-cult to determine how much virus these horses shed, and these are the horses that will contaminate the environment and get other
horses infected.”During outbreaks, veterinar-
ians and horse owners take bio-security precautions for the sick animals, but the healthy-looking asymptomatic shedders often slip under the radar.
“We recognize the sick horses, we isolate them and take all the necessary precautions to prevent disease spread. but when it comes to asymptomatic horses, other than washing our hands between horses, we don’t do much. but these horses can actually shed very high virus in the nasal secretion. And definitely a contaminated environment can be a source of infection to other horses,” he said.
There was a brief discussion af-ter his presentation at the meeting about the asymptomatic shedders after one veterinarian asked if they should be swabbing every horse during an EHV-1 outbreak. Dr.
B y M a r i e r o s e n t h a l , M S
Better diagnostics for equine herpesvirus 1 are needed to determine the stage of the virus and to help practitioners make good biosecurity decisions.
for Managing eHV-1qPcr useful tool
CoVer STory

CoVer STory
pusterla acknowledged that might not be financially feasible, but it was probably a good idea to quar-antine everyone in the barn until you were sure what was going on.
“I don’t think there is a right or wrong answer,” he said. “It is depen-dent on finances. There have been many instances where we have been able to clear a quarantine situation based on qpcr testing only.”
The laboratory at Davis receives many clinical samples of not only clinically infected horses, but also from owners of horses that were in the same barn and might have been exposed, he explained. “It is mind-boggling how many asymp-tomatic horses are shedding very high numbers of virus. Quarantin-ing both is a good idea.
“We need to alter the percep-
tion that if the horse is not display-ing clinical signs, there is probably nothing wrong with this horse. The reality is that we rarely sample these horses, but there are horses that represent the same risk of dis-ease transmission as clinically in-fected animals,” Dr. pusterla said.
right now, qpcr is primarily used in the research setting instead of viral culture, but it can be a use-ful tool for the clinician, he said.
“EHV-1 comes in different shapes and colors, which means the virus can be present in various stages. It can be lytic or replica-tive, which is a stage of virus that is assumed to be infectious. The virus can also be non-lytic or non-replicating. It can also be present in a latent form, although that is usu-ally restricted to specific anatomi-cal sites, such as lymph nodes and trigeminal ganglia.”
The virus generates transcript messenger rNA that uses the host cell machinery to produce its own protein. Quantitation can take ad-vantage of this cell action by de-tecting the messenger rNA tran-
6 Issue 4/2015 | ModernEquineVet.com
Many asymptomatic
horses are actually shedding very high numbers
of eHV-1.

ModernEquineVet.com | Issue 4/2015 7
scripts to determine the presence of a replicating lytic virus.
This was the approach Dr. pusterla took with 130 naturally infected animals. Using blood and nasal secretions, the researchers de-termined the presence or absence of the rNA transcripts and then correlated the absolute quantita-tion with the presence or absence of these transcripts. They found a significant difference among the samples from blood and nasal se-cretions and from symptomatic and asymptomatic horses. There was a 170-fold higher viral load in the nasal secretions than in the blood. “The more virus there is, the more likely that one of these will be actively replicating,” he said.
Quantitation can also be used to look at viral signature for different disease forms. He looked at sam-ples from 27 horses with EHV-1 myeloencephalopathy (EHM) and 27 horses with active EHV-1 infec-tion, fever and nasal discharge—but without neurological deficits, and 52 asymptomatic horses.
Sixty-four percent of the of EHM horses tested positive in blood, with what Dr. pusterla termed a low viral load, but he found a very high viral load in nasal secretions. The viral loads were so high in several horses, he called them Typhoid Marys.
“They are not good for your practice and they are not good for your neighboring horse. These are highly contagious horses,” he said, adding that the results ended the event the horses were attending.
The horses with EHV-1 infec-tion but without neurological defi-cit had similar viral loads in blood and nasal secretions.
Genotyping can allow veteri-narians to characterize the viruses as either neuropathogenic or non-neuropathogenic. Horses infected with a neuropathogenic EHV-1 strain often have higher viral loads in the blood compared with
horses infected with a non-neuro-pathogenic EHV-1 strains, while the viral load in nasal secretions is often similar between horses in-fected with the two different EHV-1 genotypes, he said.
Finally, pcr can help veterinar-ians monitor treatment and quar-antine. They followed 12 horses with EHM from the time they pre-sented at the hospital in the acute stage, collected daily blood and na-sal secretions for the entire hospital stay and saw a steady decline in the amount of virus detected in nasal secretions and blood.
The virus declined steadily with the total number of positive days in nasal secretions ranging from five to nine with a median of 6.5 days.
When the blood samples were reviewed, only 10 out of 12 horses with EHM tested pcr positive. There was a steady decline over time with days of detection ranging from 2-5 with a median of five days.
They also looked at overall sur-vival based on qpcr load in blood
and nasal secretions of horses with EHM. Among 22 horses that presented because of acute onset of neurological signs, 14 of them were hospitalized and discharged. Eight died or were humanely de-stroyed because they were not re-sponsive to treatment. Looking at the viral load in nasal secretions between survivor and non survi-vor, there is an average of 300-fold higher viral load in non-survivors versus survivors. The difference in blood was 10-fold higher between the two horse groups.
The quantitation of viruses can help determine disease form, its vi-ral stage, whether virus is actively replicating, as well as the response to treatment, making it a valuable tool for the clinician, according to Dr. pusterla. At the present time, EHV-1 viral quantitation is only offered at the Uc Davis real-time pcr research and Diagnostics core Facility at Davis for diagnostic purposes (www.vetmed.ucdavis.edu/vme/taqmanservice). MeV
adult thoroughbred with hindlimb weakness and incoordination (horse is in the sling for support).
Phot
o cou
rtesy
of D
r. Pus
terla

8 Issue 4/2015 | ModernEquineVet.com
Corneal disease is common in equine practice, and the standards of care keep changing, which can make it challenging for field vet-erinarians, explained dennis E. Brooks, DVM, phD, DAcVo, at the 60th Annual American As-sociation of Equine practitioners convention in Salt Lake city.
The current medical standards of care for treating ulcers in horses consists of three things, according to Dr. brooks of the University of Florida college of Veterinary Medicine. “you have to sterilize the ulcer, suppress the uveitis and reduce the enzyme activity in the tear film,” he explained. “At some point soon, we’re going to have a fourth component of the medical standard of care for corneal ulcers, which is to use available drugs to minimize scarring.”
Epithelial cells of the cor-nea migrate at a rate of
approximately 1 mm daily, so clini-cians should expect treatment for a 5-mm ulcer to last about 5 days in the horse. Healing is fast in the beginning and then slows down, so the response is not linear. If an ulcer does not respond within this general time frame, then culture or cytology are indicated to docu-ment the reason.
“The growth of blood vessels in the eye can be effected by systemic flunixin,” Dr. brooks explained. “If you use too high of a dose of flu-nixin, or use it too often, that can slow vascularization in the cornea. The horse will feel better with a lot of flunixin, but you’re delaying the corneal healing.”
Most clinicians were taught that if a horse has a bad cor-neal ulcer, then
marked uveitis will also be present. However, Dr. brooks said that this is not necessarily true.
“They will have some degree of uveitis,” he explained. “The horse eye is good at compartmentaliz-ing the inflammation inside the eye. If the eye has some corneal ulceration, you will see uveitis in the front of the eye. you may see flare, a small pupil and maybe hypopyon or hyphema, but you can’t see what’s going on behind the iris. The vast majority of the time when the horse has a bad corneal ulcer, the vitreous and retina will be fine. The uveitis should resolve as the ulcer heals.”
Goals for treating
opHTHALMoLogy
B y P a u l B a s i l i o
equine Keratopathies
Shut
terst
ock/
Anas
tasij
a Pop
ova

ModernEquineVet.com | Issue 4/2015 9
equine Keratopathies

10 Issue 4/2015 | ModernEquineVet.com
opHTHALMoLogy
Stromal abscessesStromal abscesses are a lit-
tle more difficult to treat, Dr. brooks noted. The deeper the abscess, the more likely it is to be fungal; the trick lies in the choice of antifungal.
“In Florida, we’re using a lot
of voriconazole, but it’s not work-ing as well as it used to,” he said. “I’m terrified. I don’t know when we’re going to see a new antifungal drug.”
For deep stromal abscesses, standard of care consists of topi-cal therapy with antimicrobials,
in defense of atropineAtropine does three things, but most people can only name two, according to Dr. Brooks.
The common uses are for dilation of the pupil to reduce the chance of synechiae and to help with eye pain. In humans, atropine can have a profound effect on pain associated with corneal ulcers and uveitis, because the drug relieves spasm of the ciliary muscle.
In horses, that muscle is smaller, so the effect is muted, yet still useful.
The third “little known” use of atropine is that atropine makes the blood vessels in the iris stronger.
“It minimizes aqueous flare,” Dr. Brooks explained. “Flare can cause a lot of damage in uveitis. If you don’t control flare, then that can encourage synechiae formation and can potentially encourage development of glaucoma. The first clinical sign is flare, and the last sign to resolve is flare. If they have flare, then the disease is still active. They need atropine, but at a reduced dose.”
If Dr. Brooks places a horse on atropine, he will warn the owner to call him if the horse stops eating or if it has symptoms of colic.
“Atropine is not that dangerous, “he said. "But we should be careful. We have no choice but to use it."
atropine, flunixin and a systemic antimicrobial.
“Some of the medical treat-ments go on for weeks to months,” he said. “over the years, I have learned that when I think that things are okay, they’re not. The horses can be slow to vascularize an abscess. I may reduce the ther-apy, but it’s difficult to tell when to stop the therapy. part of me is re-lieved when a client comes in and says that they ran out of voricon-azole, but the eye looks good. It can be helpful when they run out of medication.”
Dr. brooks no longer recom-mends using the gynecologic or dermatologic formulations for miconazole due to the number of irritation issues associated with them. If the horse can be referred, he believes surgery may be more beneficial for more severe stromal abscesses.
corneal squamous cell carcinomaFor horses with squamous cell
carcinoma around the eye, Dr. brooks said that treatment results are drastically better if you debulk the tumor and do some other type of therapy.
“If client finances are an is-sue regarding keratectomy, then I think corneal squamous cell is the best kind of squamous cell carci-noma,” he said. “It’s the only one where you have a chance of cur-ing it. If the tumor spreads into the conjunctivae or the eyelid, then there are blood vessels there. In the cornea, there are none—at least initially.”
If the clients do not elect a keratectomy for the horse, then chemotherapy or radiation can be initiated. Dr. brooks recom-mends 5-fluorouracil 1%. It is relatively inexpensive and can be used two or three times daily. He has recently noticed a de-cline in effectiveness, however, and is eager to start using mito-mycin-c.Sh
utte
rstoc
k/m
oleku
ul.be
a stromal abscess (above) can be difficult to treat.
Imag
e cou
rtesy
o Dr
. Bro
oks

ModernEquineVet.com | Issue 4/2015 11
Imag
es co
urte
sy of
Dr. B
rook
s
eosinophilic keratitisEosinophilic keratitis mass le-
sions look remarkably like squa-mous cell carcinoma, but they can be distinguished by the presence of small yellow sulfur granules on the surface of the mass.
“There is a big difference, though,” he said. “cancer is bad. Eosinophilic keratitis is immune-mediated.”
cytology is invaluable in these cases, and Dr. brooks recom-mended keeping the slide exami-nation in-house. Allow the slide to air dry, and examine it for eosino-phils. If the area is ulcerated, then topical steroids should be avoided.
“We didn’t see eosinophilic
keratitis for a long time,” he said. “Habronema spp was known for having a role in this, and we had the idea that ivermectin was getting rid of the parasite and eosinophilic keratitis was disappearing. Now that it is coming back, we’re seeing Habronema spp in the skin as well.”
Subepithelial keratomycosis“Subepithelial keratomycosis
is a disease that scared me,” Dr. brooks said. “I didn’t know where it came from and I had never seen it before. I had a horse with a painful eye, and I found faint retention of fluorescein that I couldn’t explain.”
cytologic examination of a scraping showed Aspergillus spp. “I no longer believe that fungal ulcers just 'happen’ in horses,” he said. “There is a whole series of events. First, the tear film gets screwed up, and then they get abrasions, and then they get an ulcer.”
The problem is that this condi-tion initially looks like immune-mediated keratitis. Dr. brooks typically uses response to anti-fungal treatment to help with the differential. If the horse does not respond to a three-week course of antifungals, then a fungus can likely be ruled out. MeV
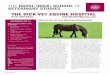
examples of several equine corneal diseases (from left): Squamous cell carcinoma; eosinophilic keratitis; subepithelial keratomycosis.
Four steps should be taken for corneal ulcers (above): sterilize, suppress uveitis, reduce enzyme activity and minimize scarring.
gynocologic or dermatologic
formulations of miconazole can
irritate the equine eye.

AAEVT MembershipBi-Annual NewsletterWeekly “HoofBeats” Email NewsblastFull access to www.aaevt.org, including the Career Center and the LibraryUp-to-date information on the AAEVTDiscounted registration for AAEVT Regional Meetings and the annual AAEP/AAEVT ConventionNTRA, Working Advantage and Platinum Performance BenefitsThe opportunity to participate in the AAEVT Online Certification Program or to become a member of the AEVNT Academy-Specialty in Equine Veterinary Nursing Scholarship opportunities. AAEVT’s Equine Manual for Veterinary Technicians (Blackwell Publishing 20% discount on purchase price)Opportunity to attend Purina’s Annual Equine Veterinary Technician Conference - All Expenses paid!
•••••
•••
••
•
AAEVT ObjectivesProvide opportunities for CE, training, communication, and networkingEducate the equine veterinary community and the public about our professionInform Members of issues affecting our professionAssist in providing the best medical care to improve the health and welfare of the horse
••••
AAEVT Online Equine Certification ProgramA three course, 10 module, equine-only online program offered through ACTGeared toward Credentialed Veterinary Technicians, Assistants, Support staff, & StudentsAreas of study include: equine medical terminology, anatomy and physiology, parasitology, laboratory, diagnostics, equine basics (breeds, wellness, husbandry,) diagnostic procedures, emergency medicine, restraint, pharmacology, surgical assistance and anesthesia, equine office proceduresA certificate of completion is awarded to those who: Successfully complete required courses Complete the list of required skills (per a supervising DVM who is an AAEP member) Attend an AAEVT regional CE symposium and participate in the we labsThose individuals who successfully complete the programs will be recognized as AAEVT Certified Equine Veterinary Technicians / AAEVT Certified Equine Veterinary Assistants depending on their current designation. The certificate is recognized by the AAEVT and the AAEP but does not grant the credentialed status by the AVMAFor more information go to www.aaevt.4act.com or call 800-357-3182
•••
•
•
•
For mo re in f o r mat i on vi st www.aae vt.org*American Association of Equine Veterinary Technicians and Assistants
AAEVT Mission Statement: To promote the health and welfare of the horse through the education and professional enrichment of the equine veterinary technician and assistant.
AAEV T M E M b E r s h i pMembership in the AAEVT is open to all veterinary technicians, assistants, support staff and those employed in the veterinary health care industry worldwide. Student membership is open to those currently enrolled in an AVMA/CVMA accredited veterinary technology program.

TeCHNICIAN upDATe
Kristina Perry, CVT
a 17-year-old Quarter Horse mare presented to cSU for colic of 24 hours duration. She was anorexic and lying down frequently and was exam-
ined by the referring veterinarian that evening. She had a temperature of 102°F, reduced borbor-
gymi in all four quadrants and a heart rate of 50 beats/min. We administered 1.1 mg/kg of IV flunixin meglu-mine and passed a nasogastric tube and obtained 6L of reflux. She was comfortable throughout the evening following initial treatment, but became mildly painful again the following morning.
Presentationon hospital admission she had a heart rate of 54
beats/min, reduced gut sounds, a temperature of 102°F and hyperemic mucous membranes. A naso-gastric tube was passed and 10L of reflux was ob-tained. An ultrasound showed a small intestine with
6–8 mm wall thickness and normal peritoneal fluid. The complete blood count (cDc) results showed leucopenia (leukocyte count 4.6 x 10^3/uL, rI: 5.5 – 10.5 x 10^3/uL), neutropenia with a left shift (seg-mented neutrophil count = 2.6 x 10^3/uL, rI: 3.0 – 7.0 x 10^3/uL; band neutrophil count = 0.2 x 10^3/uL, rI: 0.0-0.1 x 10^3/uL) and had hyperfibrinogen-emia (700.0 mg/dL, rI: 100.0 – 400.0 mg/dL). Neu-trophils were described as slightly toxic.
chemistry values showed low hypophosphatemia (1.1 mg/dL, rI: 1.7 – 4.5 mg/dL), hypocalcemia (10.9 mg/dL, rI: 11.5 – 14.0 mg/dL), and hypomagnesiu-memia (1.4 mg/dL, rI: 1.6 -2.2 mg/dL), an elevated total protein (8.0 GM/DL, rI: 5.8 – 7.4 GM/DL), hy-perglobulinemia (5.1 GM/DL, rI: 2.5 – 4.5 GM/DL), elevated cK (660 IU/L, rI: 100 – 470 IU/L), AST (397 IU/L, rI: 185 – 375 IU/L) and GGT (28 IU/L, rI: 10 – 25 IU/L).
An IV catheter was placed and a bolus of 10 L poly-ionic crystalloid fluids were administered and then a maintenance rate of 3L/hr was given with calcium gluconate and magnesium added. A lidocaine crI was started as well and polymixin b was administered ev-
Colic secondary to enteritis and nasogastric reflux associated with Salmonella hadar infection
AAEVT MembershipBi-Annual NewsletterWeekly “HoofBeats” Email NewsblastFull access to www.aaevt.org, including the Career Center and the LibraryUp-to-date information on the AAEVTDiscounted registration for AAEVT Regional Meetings and the annual AAEP/AAEVT ConventionNTRA, Working Advantage and Platinum Performance BenefitsThe opportunity to participate in the AAEVT Online Certification Program or to become a member of the AEVNT Academy-Specialty in Equine Veterinary Nursing Scholarship opportunities. AAEVT’s Equine Manual for Veterinary Technicians (Blackwell Publishing 20% discount on purchase price)Opportunity to attend Purina’s Annual Equine Veterinary Technician Conference - All Expenses paid!
•••••
•••
••
•
AAEVT ObjectivesProvide opportunities for CE, training, communication, and networkingEducate the equine veterinary community and the public about our professionInform Members of issues affecting our professionAssist in providing the best medical care to improve the health and welfare of the horse
••••
AAEVT Online Equine Certification ProgramA three course, 10 module, equine-only online program offered through ACTGeared toward Credentialed Veterinary Technicians, Assistants, Support staff, & StudentsAreas of study include: equine medical terminology, anatomy and physiology, parasitology, laboratory, diagnostics, equine basics (breeds, wellness, husbandry,) diagnostic procedures, emergency medicine, restraint, pharmacology, surgical assistance and anesthesia, equine office proceduresA certificate of completion is awarded to those who: Successfully complete required courses Complete the list of required skills (per a supervising DVM who is an AAEP member) Attend an AAEVT regional CE symposium and participate in the we labsThose individuals who successfully complete the programs will be recognized as AAEVT Certified Equine Veterinary Technicians / AAEVT Certified Equine Veterinary Assistants depending on their current designation. The certificate is recognized by the AAEVT and the AAEP but does not grant the credentialed status by the AVMAFor more information go to www.aaevt.4act.com or call 800-357-3182
•••
•
•
•
For m ore i nf or m at i on vi st www.aae v t.org*American Association of Equine Veterinary Technicians and Assistants
AAEVT Mission Statement: To promote the health and welfare of the horse through the education and professional enrichment of the equine veterinary technician and assistant.
AAEV T M E M b E r s h i pMembership in the AAEVT is open to all veterinary technicians, assistants, support staff and those employed in the veterinary health care industry worldwide. Student membership is open to those currently enrolled in an AVMA/CVMA accredited veterinary technology program.
Natio
nal In
stitu
te of
Aller
gy an
d Inf
ectio
us D
iseas
es (N
IAID
)
Produced by the national institute of allergy and infectious diseases (niaid), this digitally-colorized scanning electron micrograph (SeM) depicts a number of red-colored Salmonella sp. bacteria, as they were in the process of invading a mustard-colored, ruffled immune cell. Salmonella sp. bacteria are a common cause of foodborne disease.
ModernEquineVet.com | Issue 4/2015 13

14 Issue 4/2015 | ModernEquineVet.com
ery 12 hours. ranitidine was administered every eight hours, as well as a flunixin meglumine IV every 12 hours. Net volume of reflux obtained was 4L/hr which continued to be obtained over the course of 48 hours of hospitalization.
The following morning her temperature was 102.5°F, she had decreased gut sounds, and she re-mained hemiconcentrated despite fluid treatment with a pcV and Tp of 45 and 7.5 gm/dL, respectively.
no signs of improvementThroughout the day she continued to display signs
of colic, was pacing and had muscle fasciculations. Subsequent abdominal ultrasounds throughout the day showed a dilated fluid-filled stomach, 5–6 cm di-lated hypomotile loops of small intestine with 3 mm wall thickness. An abdominal tap was performed, and serosanguinous fluid was removed and submit-ted for chemistry and cytology. protein was 3.8 g/dL, nucleated cells were 1470/µL. cell type was 40% neu-trophils, 40% large mononuclear cells and 20% lym-phocytes. It was described as a modified transudate. A venous blood gas showed a low pH of 7.3 and a mildly low ionized calcium (1.2 mm/L, rI: 1.3 - 1.9 mm/L).
Her condition continued to deteriorate over the 48 hours she was hospitalized and endotoxemia per-sisted. based on her poor response to an aggressive medical therapy plan, she was humanely euthanized.
Necropsy was performed and jejunum and Il-eum had edema, thickening, and a dull reddish mu-cosal coloration from the end of the duodenum to
the cecum. Ileal mesenteric lymph nodes had acute hemorrhage and histopathology reflected paneth cell metaplasia in the jejunum. Aerobic culture on feces grew Salmonella, group c2, serotype Hadar. cultures of the small intestinal contents within the affected bowel were positive for Salmonella enteric, serovar Hadar, as well.
This case description outlines a clinically typical presentation of Duodenitis-proximal Jejunitis (DpJ) with uncharacteristic lesions of DpJ seen on necropsy that were later associated with Salmonella cultured from the affected intestine. Salmonella typically pres-ents clinically as enterocolitis with acute severe diar-rhea and a protein-losing enteropathy. This horse was protein-conserving and did not have diarrhea.
Atypical presentations of salmonellosis can include gastric reflux and ileus without diarrhea, and horses can be carriers shedding Salmonella without any clini-cal signs of disease. Since nosocomial infections are common in equine hospitals, precautions should be taken to limit exposure to other hospitalized patients. Salmonella has been cultured from gastric reflux and feces of horses post-operatively in colic patients, as well as in horses being treated medically for DpJ indicat-ing a need for biosecurity measures and the use of pcr and/or culture in sick horses presenting for DJp with or without diarrhea. MeV
About the authorKristina Perry, CVT, is an equine critical care nurse at Colorado State University.
TeCHNICIAN upDATe
Sellon, D., 2014, Equine Infectious Diseases, 2nd Edition, Saunders Elsevier, St. Louis, 615 p. Reed, S. et al, 2009, Equine Internal Medicine, 3rd Edition, Saunders Elsevier, St. Louis,1469 p.
For more information:
Sign up ToDAy * we promise not to bombard you with emails. Just a notice when new information is available. Send us your email address

ModernEquineVet.com | Issue 4/2015 15
NewS NoTeS
The combination treatment of triamcinolone ace-tonide and hyaluronate administered intra-articularly was less effective in the short term than intra-articular triamcinolone alone for the treatment of noninfec-tious synovitis or osteoarthritis, according to a recent study by researchers from The Netherlands.
The use of intra-articular corticosteroids in com-bination with hyaluronate was thought to be superior to intra-articular corticosteroids alone, although no study has supported this opinion.
In this multicenter, prospective, open-labeled, randomized clinical trial, horses with lameness lo-calized to a single joint received either triamcinolone acetonide or triamcinolone acetonide in combina-tion with hyaluronate, via the intra-articular route.
Eighty horses from 13 clinics were recruited; 39 received triamcinolone alone and 41 horses received the combined treatment. Lameness was assessed prior to treatment and three weeks afterward. A suc-cessful outcome was defined by a reduction in lame-ness by two or more grades. The proportion of horses returning to their previous level of performance at three months was also assessed.
After three weeks, 87.8% of horses receiving just tri-amcinolone had a successful outcome, compared with 64.1% receiving the combined treatment (p=0.01). both treatments were associated with a significant re-duction in lameness and joint effusion. Approximately
aspen veterinary resources launches vetameg equine Paste, new equine nSaid
Aspen Veterinary resources Ltd. recently intro-duced Vetameg Equine paste (flunixin meglumine), indicated for the alleviation of inflammation and pain associated with musculoskeletal disorders in the horse.
Each Aspen Veterinary resources’ Vetameg paste (flunixin meglumine) 30 mg syringe contains flu-nixin meglumine equivalent to 1,500 mg flunixin, which is therapeutically equivalent to the branded banamine paste (Merck).
Vetameg Equine paste adds to the ever-growing
Zoetis expands equine immunization Support guarantee to include eHv-1 and -4
Zoetis has expanded the Equine Immunization Support Guarantee (ISG) to include the respiratory forms of equine herpesvirus type 1 (EHV-1) and type 4 (EHV-4) viruses.
These respiratory viruses cause disease that varies in severity from subclinical to severe and are characterized by fever, lethargy, anorexia, nasal discharge and cough. Through the Equine ISG, Zoetis stands behind its line of vaccines, a program that provides horse owners up to $5,000 for reasonable diagnostic and treatment costs if a properly vaccinated horse contracts a corresponding equine disease.
“The program was expanded to offer the most comprehensive health care for horses,” said robert Holland, DVM, PhD, director of Outcomes Research, Zoetis. “It showcases our confidence in the safety and efficacy of our equine Fluvac Innovator line of vaccines with the MetaStim adjuvant.”
The average cost for diagnosis and treatment of EHV-4 ranges from $1,600 to $2,700 per horse, according to Dr. Holland.
To be eligible for the Equine ISG, vaccinations must be obtained and administered by a licensed veterinarian.
The ISG provides veterinarians an opportunity to discuss vaccination with horse owners and help them provide the best possible health care for their animals, explained Kevin Hankins, DVM, Equine Veterinary Services, Zoetis. “The Equine Immunization Support Guarantee offers additional peace-of-mind to horse owners looking to help provide the best possible disease protection for their horses.”
Other disease protection backed by the Equine ISG includes infection from West Nile, equine influenza, tetanus, Eastern equine encephalomyelitis, Western equine encephalomyelitis and Venezuelan equine encephalomyelitis. For full eligibility requirements and details on the Equine ISG visit www.zoetisus.com/isg. MeV
line of effective equine products offered by Aspen Veterinary resources, including Vetameg Injectable, Mineral Max, Equi-bute paste and Equi-bute Inject-able, among others. MeV
comparative efficacy of intra-articular medications
For more information:
de Grauw JC, Visser-Meijer MC, Lashley F, et al. Intra-articular treatment with triamcinolone compared with triamcinolone with hyaluronate: A randomised open-label multicentre clinical trial in 80 lame horses. Equine Vet J. 2015 [Epublished ahead of print February).
half the horses in each group had returned to their previous level of performance at three months.
older horses—those older than 13 years—had re-duced success rate of the combination treatment. MeV

Identifying subtle lameness is difficult because the evaluation is often subjective, so more objective mea-sures to identify lameness are always being sought.
There is often disagreement among clinicians, es-pecially when mild lameness exists, said Josh don-nell, DVM, of colorado State University, at the 60th annual meeting of the American Association of Equine practitioners held in Salt Lake city, Utah.
Dr. Donnell and his colleagues compared subjec-tive clinical evaluations, unblinded and blinded, with two objective methods: the force plate, which mea-sures ground reaction forces, and a body-mounted inertial sensor system, with accelerometers and gy-roscopes attached to the horse. The sensors quantify movement asymmetry of the torso resulting from significant differences in limb loading between the left and right halves of the stride.
His study included 16 horses that underwent a baseline evaluation to determine lameness. Each horse had surgically induced osteoarthritis (oA) in one carpal joint and sham surgery in the contralater-al joint as a control. Subsequent lameness evaluations were performed at days 15, 42 and 71.
First the investigators studied each method for its ability to identify lameness within the limb that had induced disease. Then the investigators looked for agreement in lameness detection among the methods.
The horses were outfitted with the inertial sensor
system and trotted across the force plate. A single strike on the force plate by a forelimb and 25 contin-uous strikes measured by the inertial sensor system constituted a trial. For each time point there were five valid trials performed.
Additionally, unblinded subjective evaluation was performed at each point by a single experienced cli-nician who also performed musculoskeletal exams on the horses. The horses were graded using the AAEp lameness scale while they were trotting over the force plate on the same runway.
Finally, the trails were videotaped, and four ex-perienced clinicians viewed the videos and made an evaluation. This was considered the blinded subjective evaluation. The clinicians, using the AAEp lameness scale, reached a consensus as to which limb was lame. blinded subjective evaluations were performed with-out the benefit of full musculoskeletal examinations.
Subjective evaluationsThe unblinded evaluations identified half the
horses lame at baseline. After the induction of osteo-arthritis all the horses were identified as lame within the oA limb, with the number of horses deemed lame slowly decreasing to about half the horses at the end of the study, Dr. Donnell reported.
The blind evaluators, who reviewed videos of the horses trotting, identified five horses as being lame at baseline with the number of horses deemed lame increasing to 13 at day 15 and then slowly declined declining to 10 at day 71.
“There was a significant difference between the AAEp lameness scores of the blinded and unblinded subjective evaluations with the blinded scores being 27% lower,” Dr. Donnell said.
Objective measuresboth the force plate (the mean peak vertical force
decreased 3.6% from baseline to post-disease in-duction) and the inertial sensor system showed an increase in the number of horses determined to be lame from baseline to the end of the study.
of the objective measures, the inertial sensor sys-tem’s results were most similar to the blinded subjec-tive evaluation, and the force plate identified the limb with induce oA the least often, Dr. Donnell reported.
The inertial sensor system identified the most num-ber of horses as being lame throughout the study start-ing at 12 at baseline and that increased to all horses at the end of the study. The force plate identified about half the horses as being lame at baseline. That number
16 Issue 4/2015 | ModernEquineVet.com
orTHopeDICS
Horses benefit from a combination of objective and subjective methods for evaluating lameness
checking for lameness in a circle.Photo courtesy of Dr. Josh Donnell.

ModernEquineVet.com | Issue 4/2015 17
Shut
terst
ock/
Lilac
Mou
ntain
increased to about 10 at day 15, and then decreased to seven horses at the end of the study.
In comparing methods for identifying lameness independent on oA induction, Dr. Donnell found that the blinded subjective and the unblinded subjec-tive evaluations, which agreed 66% of the time.
The next two methods in agreement were the un-blinded subjective evaluation and the inertial sensor system, which were in agreement 53% of the time.
The inertial sensor system and the force plate were in agreement 36% of the time.
There was a large difference between the un-blinded and blinded subjective evaluation at iden-tifying the disease-induced limb on day 15: the un-blinded evaluators identified the disease-induced limb 87% of the time compared with 38% for the blinded evaluators.
“The difference between the subjective evalua-tions was potentially due to the blinded evaluator be-ing biased and having an expectation that the horses were going to be lame post-disease induction, and that unblinded evaluator was able to perform mus-culoskeletal exams,” Dr. Donnell explained, adding that lameness has been shown to be less recognizable on video exams, which would have been a clear dis-advantage to the blinded evaluators.
Inertial sensors don’t have an opinion; they only record the horse’s actual motion—but accurately and repeatably, explained Kevin Keegan, DVM, MS, DAcVS, a professor at the University of Missouri college of Veterinary Medicine and co-inventor of the Lameness Locator (Equinosis), an inertial sen-sor system to detect lameness. Dr. Keegan was not involved in the study.
“As long as the inertial sensors are used correctly, the sensors record what is happening. They record to a precision of less than 1 mm, and the system is designed to indicate differential loading between the limbs. pref-erentially loading of one limb over the one on the other side is the primary means a horse uses to reduce pain in an affected limb, and this is reflected as asymmetric movement of the head and torso,” he explained.
because of the difficulty in identifying pain caus-ing mild lameness, Dr. Donnell, said currently there is not a gold standard to identify mild lameness but combination of subjective and objective methods might be the best solution. “Horses can’t talk [and tell us about their pain]. A combination of subjective and objective methods could be helpful especially when identifying subtle lameness,” he said. MeV
Dr. Donnell’s study was funded by the Orthopaedic Re-search Center Foundation at Colorado State Univer-sity, Fort Collins, Colo. Instrumentation for use in the study was provided by Equinosis LLC, St. Louis, MO.
When assessing lame horses on the lunge, the agreement among raters was poor for hindlimb lameness and poor-to-moderate for forelimb lameness, according to a recent study in the Equine Veterinary Journal.
Consistent identification of lameness is important for diagnosis and reassessment of lame horses. Lunging during the lameness examination may accentuate low-grade lameness, European researchers said. However, visual assessment of lameness is inher-ently subjective.
In this cross-sectional, observational study, rater agreement during lunging exercise was assessed in 23 horses. Videos of these horses trotting on a straight line and during the lunge on hard and soft surfaces were evaluated by 86 equine veterinarians of variable expe-rience, with some videos reviewed more than once to assess intra-rater agreement.
Raters were asked to identify the lamest limb on each video. Less experienced equine practitioners (<5 years equine experience or doing <100% equine work) showed poor agreement in terms of selection of the lamest limb during trotting on a circle, agreement was moderate for experienced practitioners and found to be higher for forelimb lame-ness across all levels of experience. Intra-rater repeatability was moderate but varied between raters. MeV
rater agreement of visual lameness assessment in horses during lunging
NewS NoTeS
For more information: Hammarberg M, Egenvall A, Pfau T, Rhodin M. Rater agreement of visual lameness assessment in horses during lunging. Equine Vet J. 2015. [E pub ahead of print February 2015].
http://onlinelibrary.wiley.com/doi/10.1111/evj.12385/abstract

reach your veterinarians wherever they are, whenever they want.
FOr AdVerTISInG rATeS And InFOrMATIOn, eMAILrobin gellar
Equine VetThe Modern