Embed Size (px)
DESCRIPTION
Our mission is to enhance your ability to practice equine medicine by providing the latest info you need.
Citation preview

Vol 5 Issue 12 2015www.modernequinevet.comEquine Vet
The Modern
AAEP Meeting: Wound care without the traumaSuspensory ligament branch injury riskTechnician Update: Removal of a sequestrum on the proximal tibia
Not a diagnosis you want to make
Headshaker

2 Issue 12/2015 | ModernEquineVet.com
Table of ConTenTs
DerMaTologyWound care without the trauma .......................................................................................8
SporTS MeDIcInerisk factors for injury in Swiss horse racing ................................................................13
TechnIcIan upDaTeSurgical removal of a sequestrum on the proximal tibia ..................................17
neWSSuspensory ligament branch injury risk in Thoroughbreds .........................................................................3uc Davis integrates sports medicine for horses ...................14aaep honors Dr. nathaniel a. White, others .........................15
LEGAL DISCLAIMER: The content in this digital issue is for general informational purposes only. PercyBo Publishing Media LLC makes no representations or warranties of any kind about the completeness, accuracy, timeliness, reliability or suitability of any of the information, including content or advertisements, contained in any of its digital content and expressly disclaims liability of any errors or omissions that may be presented within its content. PercyBo Publishing Media LLC reserves the right to alter or correct any content without any obligations. Furthermore, PercyBo disclaims any and all liability for any direct, indirect, or other damages arising from the use or misuse of the information presented in its digital content. The views expressed in its digital content are those of sources and authors and do not necessarily reflect the opinion or policy of PercyBo. The content is for veterinary professionals. ALL RIGHTS RESERVED. Reproduction in whole or in part without permission is prohibited.
headshaking: not a diagnosis you want to make
coVer STory:
4
Cover photo Shutterstock/ Lenkadan
SAlES: Matthew Todd • [email protected]
EdiToR: Marie rosenthal • [email protected]
ART diREcToR: Jennifer Barlow • [email protected]
conTRibUTing WRiTERS: paul Basillo • Kathleen ogle
coPY EdiToR: patty Wall
Published by
p E r c y b omedia publishing
Equine VetThe Modern
AdvERTiSERSShanks Veterinary equipment ................................. 3ceVa animal health ................................................... 5avalon Medical ............................................................ 7
Merck animal health ................................................. 9universal Imaging ....................................................11aaeVT ...........................................................................16
PO Box 935 • Morrisville, PA 19067Marie Rosenthal and Jennifer Barlow, Publishers

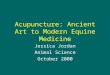
prevalence of Grade 2–3 suspensory ligament branch change was 18.5% (observer 1) and 23% (observer 2). once adjustments were made for interobserver dif-ferences, there was a significant association between Grade 2–5 sesamoiditis and Grade 2–3 suspensory ligament branch injury: 28% of sesamoids with Grade 2–5 sesamoiditis also had Grade 2–3 suspensory liga-ment branch change of Grade 2–3, compared with 4% of sesamoids considered to be normal. Eight horses de-veloped clinical SLbI, of which 5 had Grade 2-5 sesa-moiditis and Grade 2–3 suspensory ligament branch change at initial imaging assessment. When considered separately, both Grade 2–5 sesamoiditis and Grade 2–3 suspensory ligament branch change were significant risk factors for subsequent SLbI. When these hap-pened concurrently, there was a significantly increased risk of clinical SLbI. MeV
ModernEquineVet.com | Issue 12/2015 3
There is an association between sesmoiditis and sus-pensory ligament branch changes, and these changes can be found on ultrasound, according to a recent study. There is also a relationship between these con-ditions and subsequent clinical suspensory ligament branch injury (SLbI), especially when these findings transpire concurrently.
This prospective study aimed to investigate the associations among radiographic signs of sesamoid-itis, ultrasonographic signs of suspensory ligament branch desmitis and subsequent clinical SLbI.
before commencing training, 50 yearling Thor-oughbreds from a single training facility were evalu-ated. radiographic changes in sesamoid bones were graded on a scale of 0 to 5: changes of Grades 2–5 were considered as possibly significant sesamoiditis. Ultrasonographic changes in the forelimb suspenso-ry ligament branches were graded from 0 to 3, with Grades 2–3 considered as possibly significant. Further imaging was performed only if clinical SLbI occurred over the course of the subsequent nine months.
The prevalence of Grade 2–5 sesamoiditis in ini-tial radiographs was 20.5% (observer 1) and 23% (observer 2) of all 200 sesamoid bones assessed. The
Suspensory ligament branch injury risk in Thoroughbreds
news noTes
For more information:
Plevin S, McLellan J, O’Keeffe T. Association between sesamoiditis, subclinical ultrasonographic suspensory ligament branch change and subsequent clinical injury in yearly Thoroughbreds. Equine Vet J. 2015. [Epub ahead of print Oct. 29] )
http://onlinelibrary.wiley.com/doi/10.1111/evj.12497/abstract www.shanksvet.com • [email protected]
Lifting Large Animals Since 1957
Phot
o cou
rtesy
of th
e Equ
ine Ve
terina
ry Jo
urna
l
Transverse image of subsequent injury of the suspensory ligamentbranch.

4 Issue 12/2015 | ModernEquineVet.com
CoVer sTory
Phot
o cou
rtesy
of w
ww.b
oblan
grish
.com
B y M a r i e r o s e n t h a l , M S
One of the last labels that Peter R. Morresey, bVSc, MAcVSc, DAcT, DAcVIM, wants to put on a horse that “shakes” its head is headshaker, he said at the Northeast Association of Equine practitioners annual meeting in pittsburgh.
“Headshaking is a really difficult problem to deal with,” he said. The true etiology is unknown; it is difficult to diagnose; and good treatments are lack-ing, explained Dr. Morresey, an internal medicine specialist at rood and riddle Equine Hospital in Lexington, Ky.
In addition, there are many reasons why a horse could be moving its head. Therefore, a horse should not be diagnosed and labeled as a headshaker until all other differentials have been eliminated. precipitating causes can be as simple as ill-fitting tack or a more-complicated disease process, he said.
classic characteristics of the clinical syndrome of headshaking are intermit-tent and violent swinging of the head up and down and side to side. The onset is typically early middle age—about 8 to 9 years old—and geldings are overrep-resented. In addition, there appears to be a predilection among certain breeds, especially Quarter horses, paints and Appaloosas. The problem tends to occur in late spring and summer, and exercise can exacerbate the condition.
Headshaking is not normally associated with the horse looking behind, he said. It is associated with snorting and rubbing the nose. Some horses will strike their noses on surfaces and can actually do some serious damage. These actions imply some sort of irritation to the nasal cavity, he said.
HEAdSHAkingnot a diagnosis you want to make

Now FDA approved for use in the U.S. and available from your veterinary distributor, Tildren® (tiludronate disodium) controls clinical signs associated with navicular syndrome in horses. Tildren works at the areas of active bone resorption, restoring balance to the process of bone remodeling.
NOW AVAILABLE IN THE U.S. Over 250,000 doses administered worldwide in the last 12 years.
©2015 Ceva Animal Health, LLC. Lenexa, KS 66215 TILDREN is a registered trademark of Ceva Santé Animale, France.
Do not use in horses with impaired renal function or with a history of renal disease. NSAIDs should not be used concurrently with TILDREN. Concurrent use of NSAIDs with TILDREN may increase the risk of renal toxicity and acute renal failure. Horses should be observed closely for 4 hours post-infusion for the development of clinical signs consistent with colic or other adverse reactions. Caution should be used when administering TILDREN to horses with conditions affecting mineral or electrolyte homeostasis (e.g. HYPP, hypocalcemia) and conditions which may be exacerbated by hypocalcemia (e.g. cardiac disease). The safe use of TILDREN has not been evaluated in horses less than 4 years of age, in pregnant or lactating mares, or in breeding horses.
Contact your local distributor or Ceva Animal Health representative for more information.
TILDREN.COM/US
12963_cev_Tildren_PrintAds_Vet_ModernEquine_1502_FullPage_vFA.indd 1 1/28/15 11:21 AM

6 Issue 12/2015 | ModernEquineVet.com
Bisphosphonate drug for intravenous infusion. For use in horses only.
Brief Summary: See package insert for full prescribing information.
Caution: Federal law restricts this drug to use by or on the order of a licensed veterinarian.
Description
TILDREN is a sterile powder. Each vial of TILDREN contains 500 mg of tiludronic acid (as tiludronate disodium) and 250 mg mannitol USP (excipient).
IndicationTILDREN is indicated for the control of clinical signs associated with navicular syndrome in horses.
Contraindications
Do not use in horses with known hypersensitivity to tiludronate disodium or to mannitol. Do not use in horses with impaired renal function or with a history of renal disease. Bisphosphonates are excreted by the kidney; therefore, conditions causing renal impairment may increase plasma bisphosphonate concentrations resulting in an increased risk for adverse reactions.
Warnings
Do not use in horses intended for human consumption. NSAIDs should not be used concurrently with TILDREN. Concurrent use of NSAIDs with TILDREN may increase the risk of renal toxicity and acute renal failure. Appropriate wash-out periods should be observed between NSAID and TILDREN administration, and BUN and creatinine should be monitored. If treatment for discomfort is required after TILDREN administration, a non-NSAID treatment should be used.
Human Warnings
Not for human use. Keep this and all drugs out of the reach of children. Consult a physician in case of accidental human exposure.
Precautions
Approximately 30-45% of horses administered TILDREN will demonstrate transient signs consistent with abdominal pain (colic). Hand-walking the horse may improve or resolve the colic signs in many cases. If a horse requires medical therapy, non-NSAID treatments should be administered due to the risk for renal toxicity. Avoid NSAID use.
TILDREN should be administered slowly and evenly over 90 minutes to minimize the risk of adverse reactions.
Horses should be well hydrated prior to administration of TILDREN due to the potential nephrotoxic effects of TILDREN.
Concurrent administration of other potentially nephrotoxic drugs should be approached with caution, and if administered, renal function should be monitored.
Caution should be used when administering TILDREN to horses with conditions affecting mineral or electrolyte homeostasis (e.g. hyperkalemic periodic paralysis (HYPP), hypocalcemia, etc.) and conditions which may be exacerbated by hypocalcemia (e.g. cardiac disease). TILDREN should be used with caution in horses receiving concurrent administration of other drugs that may reduce serum calcium (such as tetracyclines) or whose toxicity may exacerbate a reduction in serum calcium (such as aminoglycosides).
Horses with HYPP (heterozygous or homozygous) may be at an increased risk for adverse reactions, including colic signs, hyperkalemic episodes, and death.
The safe use of TILDREN has not been evaluated in horses less than 4 years of age. The effect of bisphosphonates on the skeleton of growing horses has not been studied; however, bisphosphonates inhibit osteoclast activity which impacts bone turnover and may affect bone growth.
Bisphosphonates should not be used in pregnant or lactating mares, or mares intended for breeding. The safe use of TILDREN has not been evaluated in pregnant or lactating mares, or in breeding horses.
Increased bone fragility has been observed in laboratory animals treated with bisphosphonates at high doses or for long periods of time. Bisphosphonates inhibit bone resorption and decrease bone turnover which may lead to an inability to repair microdamage within the bone. In humans, atypical femur fractures have been reported in patients on long term bisphosphonate therapy; however, a causal relationship has not been established.
Adverse Reactions: The most common adverse reactions reported in the field efficacy and safety studies were clinical signs consistent with abdominal discomfort or colic. Other reported signs were frequent urination, muscle fasciculations, polyuria with or without polydipsia, and inappetance/anorexia.
For technical assistance or to report suspected adverse reactions, call 1-800-999-0297.
Marketed by: Ceva Animal Health, LLC Lenexa, KS 66215
Tildren® is a registered trademark of Ceva Santé Animale, France
NADA 141-420, approved by the FDA
Headshakers will have an unremark-able physical and neurological examina-tion. If the veterinarian sees dental dis-ease, oral mucosal ulcerations, pain in the neck or upper spine—those issues should be dealt with first to see if the headshaking is eliminated.
There are several ideas about its cause. one is that it is a photosensitivity, equiv-alent to the human photic sneeze, which makes sense given its seasonal onset, he said. researchers are starting to think that light stimulates the trigeminal nerve in the horse’s face and causes it to tingle, itch or burn, and the horse reacts by shaking its head or snorting, rubbing and banging its nose to stop the sensation.
“In horses, headshaking can be tied to the daylight period, and headshaking is treated with melatonin,” he said. “So, it’s not a leap.”
A similar syndrome is seen in humans who suffer photic sneeze or trigeminal neuralgia. In some individuals, bright light kicks the trigeminal nerve into ac-tion. They will get nasal engorgement, their eyes will run and they sneeze. It al-most looks like an allergic reaction, but there is no allergic component to this, so that is what makes it so difficult to under-stand, according to Dr. Morresey.
other people will experience a pro-found, acute onset of burning and itch-ing that shoots across the face and feels like an electric shock. There are no other pathological signs.
If horses suffer conditions similar to the human photic sneeze and trigeminal neuralgia, it’s easy to see where it might start violently shaking its head, he said.
Another contributor may be a hor-monal imbalance (which is why geld-ings might be overrepresented), vascular changes, or temporohyoid osteoarthrop-athy, according to Dr. Morresey. Some reports have linked it to an infection, but other studies have not borne that out.
Seasonal allergy could also be a cause, especially in a horse that has a good bit of skin irritation, he explained. “Nasal irrita-tion may be giving us a syndrome that is similar to the classic headshaker in horses. Like us, some of these horses suffer from al-lergies and these allergies are often going to be seasonal. you might see other things on this horse. perhaps you will have urticaria and the horse is moving its head around in a noxious fashion, and the client will say, ‘My horse is a headshaker,’” Dr. Morresey said.
Diagnosis“Headshaking is a diagnosis of exclusion.
HEAdSHAkER TREATMEnT
Treatment Dose/frequency comments
cyproheptadine 0.3mg/kg PO q12h Moderate improvement. Lethargy
carbamazepine 2–8mg/kg PO q6h-q12h Moderate improvement. (May be combined with cyproheptadine) Unpredictable efficacy
hydroxyzine 1mg/kg PO q12h Moderate improvement.
Fluphenazine 50 mg IM Repeat 1–4 monthly. Neurological dysfunction.
phenobarbital 3–6 mg/kg PO q12h Calmative. Sedation.
gabapentin 5–20 mg/kg PO q12h–q24h Anecdotal reports, variable.
corticosteroids Standard dosage Also variable success pulse therapy reported.
Magnesium Variable Calmative.
Melatonin 15–18 mg PO q24h Altered hair shedding.
Sodium cromoglycate eye drops Apply OU q6h Seasonal head shakers.
CoVer sTory

ModernEquineVet.com | Issue 12/2015 7
We need to get rid of all the organic causes of disease,” he said.
Take a detailed history, includ-ing management procedures, diet, exercise and environmental chang-es. When investigating idiopathic headshaking following exclusion of other diseases, the horse should ex-hibit characteristic head motion of rapid downward motion of the nose followed by upward flinging of the head. The physical should include oral cavity, ophthalmic and oto-scopic examinations. Endoscopy of the upper airway, including the gut-tural pouches, and radiography of the head and throatlatch region are indicated. computed tomography and magnetic resonance imaging may help visualization bone and soft tissue. In some cases there is thick-ening around the trigeminal nerve.
Local anesthesia of the infra-
orbital nerve has been used as an aid to diagnosis but reported suc-cess is low. In a study by Mair, et al., infraorbital anesthesia with 2% mepivacaine improved three out of 19 horses, had no effect on eight horses and worsened symptoms in another eight horses.
In another study by Newton, et al, only one in eight horses im-proved and only by 50%, however, a lower dose of mepivacaine was given. Using more local anesthet-ic infiltration may affect adjacent nerves, he said.
bilateral anesthesia of the pos-terior ethmoidal nerve (maxillary nerve) improved 13 of 17 horses in one study and 23 of 27 horses in another. However, the location of the nerve requires an extended period for diffusion of the anes-thetic to achieve a full effect, Dr.
Morresey cautioned. Management of the condition involves changes in the environment to minimize stimluli such as light and airborne irritants, and various medications that show some efficacy in some cases. Surgical approaches have been reported, however compli-cation and reoccurrence rates are high, and improvements slight in most cases, meaning this ap-proach is at best an attempt at sal-vaging the horse
“It is quite interesting to talk to clients [about headshaking]; it al-most seems like they tend to want their horse to be a headshaker so they can blame the behavior on something,” he said. “but I really, re-ally don’t want them to have a head-shaker. The owners just want some-thing to fix it. And as we know, that is very difficult to do.” MeV

8 Issue 12/2015 | ModernEquineVet.com
B y p a u l B a s i l i o
derMaTology
There’s an old adage in the wound healing field that says, “Never put something on a wound that you would be unwilling to put in your eye.” It’s a simple premise, but it’s one that can be overlooked in general practice.
“In the veterinary field, it’s a bit horrifying to consider all the things we put in horse wounds,” said Dean A. Hendrickson, DVM, DAcVS, professor of clini-
cal sciences at colorado State Uc University. “Think about someone coming by and squirting these things into your eye one week apart just to see how you would re-spond to it. Except for a hyperton-ic saline dressing, I don’t put any-thing in a wound that I wouldn’t put in my eye, and I’ve seen much better healing responses. Some-times the animal heals in spite of us, not because of us.”
Wound preparationIt is crucial to truly evaluate the wound, and Dr. Hendrickson rec-ommended clipping the area first.
“I had a horse that came in caked with dirt, blood and debris,” he explained at the 61st Annual AAEp convention here in Las Vegas. “The skin edges had been carefully opposed with horizon-tal mattress sutures, but the horse became sorer as time went on. I
Wound carewithout the trauma
Phot
o cou
rtesy
of D
r. Dea
n A. H
endr
ickso
n
A dry wound with crusting after tumor removal

ModernEquineVet.com | Issue 12/2015 9
1 UC Davis (Nicola Pusterla) & Merck Animal Health. Infectious Upper Respiratory Surveillance Program. Ongoing Research 2008-present.
2 Townsend HGG. Onset of protection against live-virus equine influenza challenge following vaccination naive horses with a modified-live vaccine. Unpublished data.
Visit us online to learn more about Merck Animal Health and the equine products and programs that help you keep horses healthy.
The Science of Exceptional
Stop flu where it starts.
Trust Flu Avert® I.N. for superior protection against relevant flu strains threatening the U.S. horse population.1
• Just ONE dose required - An ideal first flu vaccine for young horses - Provides protection at the site of infection
and long-lasting immunity
• Proven safe and effective - Intranasal application leaves no risk for
injection site reactions to interfere with training or competing
• Rapid onset of protection - Onset of flu protection within five to
seven days following one dose – no matter when your horse was last vaccinated for flu.2
Now that’s exceptional.
The Science of Healthier Animals
2 Giralda Farms • Madison, NJ 07940 • merck-animal-health-usa.com • 800-521-5767Copyright © 2015 Intervet Inc., d/b/a/ Merck Animal Health, a subsidiary of Merck & Co., Inc.All Rights reserved. 51358 2/14/ EQ-1244
Science_Ad-FluAvertIN_825x10875.indd 1 12/28/15 10:16 AM

10 Issue 12/2015 | ModernEquineVet.com
wound Care
cleaned the wound and clipped the area, and two puncture wounds could be seen going into the car-pus with synovial fluid leaking out. you can’t see what’s there until you get the hair out of the way.”
After the hair is removed, clean-ing the wound may be the most im-portant step. Dr. Hendrickson not-ed that clinicians probably do more accidental harm to the wound at this stage. Gloves are necessary. If the wound is over an area of bone or a synovial membrane, then asep-tic technique is indicated.
organisms are not picky. Wheth-er it’s a stick, a rock, suture material or a $200 titanium screw, foreign material in a wound can affect heal-ing and increase the infective dose of some organisms. “In some cases, wounds are
dirty and need to be cleaned, but if you stop for a minute and are honest about the situation, then we have to admit that everything we do to a wound causes some trauma to the wound bed,” Dr. Hendrickson explained.
In 1919, Dr. Alexander Flem-ing said that it was impossible to sterilize a wound using an anti-septic. Almost a full century later, there has not been a controlled clinical study that refutes that as-sertion. The best case scenario for antiseptics is to reduce the bacteri-al burden, but standard antiseptic therapy tends not to do that as well as is commonly thought.
povidone iodine, the unofficial gold standard in veterinary and hu-man medicine for wound care, has been used in countless wounds, but the controls in the published clini-cal studies were fairly suspect, Dr. Hendrickson said.
In fact, studies have repeatedly failed to show that povidone iodine promotes healing, and it can actu-ally impair wound healing, reduce wound strength and can lead to infection. The povidone iodine ef-fectively causes necrosis of the tis-
sue that functions as foreign mate-rial leading to increased bacterial counts.
“I come from a ‘big hammer’ family in northern Montana,” Dr. Hendrickson joked. “If I did some-thing with a small hammer that didn’t work, then I just got a bigger hammer. We do a lot of that when we scrub. If a little bit of scrubbing doesn’t clean the wound, then we scrub harder. I would ask that cli-nicians ignore that second step. If the wound isn’t cleaned with gentle scrubbing or lavage with a moist sponge using a physiologic agent such as saline or lactated ringer so-lution, then try something else.”
antibioticsDr. Hendrickson tends to shy away from continued use of systemic antibiotics following an initial “blast” dose, but topical antibiotics can be highly valuable for equine wound care.
Silver sulfadiazine (SSD) cream is a common choice in wounds in both equine and human medicine. Silver impregnated dressings elute silver into the wound to kill the bacteria and can be easily removed following use. This can offer a re-spite from having to apply SSD cream to a wound and then having to use lavage or scrub the wound to remove the cream.
Nitrofurazone is another com-monly used topical antibiotic in horses, but Dr. Hendrickson is not sold. “As much as we use nitrofu-razone in horses, there is not one positive study for its use in wound healing,” he explained. “I some-times joke that if you’re going to investigate a new topical agent then you should use povidone io-dine and nitrofurazone as control agents, because almost everything looks better than these two.”
Triple antibiotic ointment (bac-itracin, neomycin and polymyxin b) has shown some great effective-
Evaluating the AntisepticsThere are many antiseptic options, but all are not equal. Dr. Dean A. Hendrickson offered his thoughts on the available options.
chlorhexidine — This has a longer residual effect than povidone iodine, but the label says that we shouldn’t put around the cornea, in the ear, or in synovial structures. Any time we see that, we should probably look a little more carefully at what we’re doing. A study in 2012 in The Journal of Orthopaedic Trauma showed no statistical difference in the presence or quantity of bacteria with saline vs chlorhexidine.
Hydrogen peroxide — The old argument for hydrogen peroxide was that if it was bubbling, that meant it was working. Its antimicrobial effect is overstated. A recent study in PLOS One showed that there is some benefit in low concentrations for enhancing angiogenesis in wound closure, but the process is slowed at high concentrations.
vinegar — Studies have shown that using vinegar on the right wounds and with the right bacteria can have great results. A solution of 0.25% or 0.5% has shown to have bactericidal effect against gram-positive and gram-negative organisms, with particular effectiveness against Pseudomonas species.
Moist wounds are happy wounds. The balance between dry and wet can make the difference in helping the wound heal.

Universal ImagingSee the difference
UNIVERSAL I M A G I N G TM
TRANSFORMTHE QUALITY OF CARE
Ultrasound Digital Radiography Cloud & PACS Continued EducationLeading-edge systems tailored to the equine
practitioner.
Ultra-light, fully wireless systems with auto X-ray detection technology.
Comprehensive cloud-based image storage
and management.
Focused on improving the quality of care that you offer your patients.
Innovative Mobile Solutions For Today’s Equine Practitioner
800.842.0607 | www.universalimaginginc.com
myRad D-EVODigital Radiography
ULTRA-LIGHT DIGITAL RADIOGRAPHY FOR TODAY’S EQUINE PRACTITIONER.
FujiFilm’s sophisticated imaging technologies and advanced processing bring the image quality of myRad D-EVO to the next level.
ISS Technology improves signal strength and dose efficiency, resulting in images with an unprecedented level of diagnostic content.
SmartSwitch (AED) Technology eliminates generator synchronization problems by automatically sensing x-ray photons to initiate image acquisition.
ULTRA-PORTABLE ULTRASOUND DESIGNED FOR VETERINARY MEDICINE
Compact, powerful and easily transportable, EXAGO offers veterinary practices exceptional image quality and unparalleled ease-of-use.
Best image quality of any 6-lb. system - B, B+B, B+M modes, Color Flow Mapping, Pulsed Wave-Power Doppler, Cardiac, Video Clips, MSK – All Standard
Industry leading battery run time of up to 6 hours enhances the portability by eliminating the need for a power source.
EQUINE PRO PACKAGE SPECIALPurchase a myRad-DEVO with a C24i (10x12) or P35i (14x17) detector before January 15, 2015 and get an EXAGO ultrasound with one probe for $10,000, PLUS a free one or two day VetPD Continued Educa-
tion course held anywhere in the world.
CLICK HERE TO LEARN MORE
BUY THIS GET THIS FOR $10,000
15 lbs. 6 lbs.

12 Issue 12/2015 | ModernEquineVet.com
ness. The product was launched in the 1950s as a prescription and in the 1970s as an over-the-counter agent, and the resistance pattern has had almost no change since its inception.
“SSD, triple antibiotics and surfactant-based cleansers are some of the things that we can put on a wound to minimize our nega-tive impact on the wounds them-selves,” Dr. Hendrickson said.
Wound dressingsMoist wounds are happy wounds. The balance between dry and wet can make the difference in wound healing.
“I believe that you must keep a wound moist if you want the most effective healing to take place,” Dr. Hendrickson said. “choose a dressing that helps to accomplish this.”
Debridement dressings (e.g., hypertonic saline) are simple, easy to use and essentially suck fluid out of the bacteria until they die.
Dr. Hendrickson prefers 20% sa-line dressings. Healthy cells can handle this solution of saline, but tenuous cells cannot.
“I change dressings based on the amount and character of the exudate, not by the calendar,” he said. “If a wound has a lot of exu-date, I will change dressing fre-quently because the exudate can dilute the hypertonic saline. For wounds with less exudate, I may cover the dressing with plastic to maintain moisture.”
It is important to never use hy-pertonic saline directly over bone. This may lead to bone sequestrum.
Dressings that are impregnated with polyhexamethylene biguanide (pHMb) are available in sponges, roll gauzes and other types. These dressings are designed to stop bac-terial penetration to wounds, but they can also kill the bacteria with-in the wounds themselves.
“other uses for pHMb include contact lens solutions, so this works out well for our goal,” he said.
pHMb works by disrupting the outer phospholipid membrane and allowing the cytoplasm to leak out. Dr. Hendrickson recom-mended moistening the dressing before placing it.
“I no longer believe that horses create more exuberant granula-tion tissue than other species,” he noted. “I think equine veterinar-ians create more exuberant granu-lation tissue than other species. For years we were always afraid to consider granulation tissue in horse wounds because the wounds we dealt with already had so much exuberant granulation tissue.”
In the right environment, how-ever, granulation tissue can be help-ful to cause wound contraction and help wounds heal faster. one of Dr. Hendrickson’s preferred dressings for this purpose involve alginate, a derivative of seaweed. The dress-ings come in a nonwoven pad and also include calcium to encourage wound contraction. Wound exu-date tends to be high in sodium; the dressing pulls in the sodium and donates calcium to the wound.
“one thing to note about these is that they are very absorptive,” he said. “If you have a wound on the edge of being dry and you put a calcium alginate dressing on it, it will desiccate the wound. I al-ways pre-moisten these with sa-line solution.”
Alginate dressings also stimu-late the granulation beds to come through bone. If a bone is exposed, Dr. Hendrickson recommended cu-retting and debridement followed by a moistened alginate dressing. The bone should be debrided until it is bleeding or glistening.
“I can cover an almost com-pletely denuded, dry, chalky cannon bone and have it covered in granu-lation within about seven days with calcium alginate,” he said. “I have not had a horse develop a bone se-questration as a result.” MeV
wound Care
Wound after it had healed using moist wound healing techniques.
Phot
o cou
rtesy
of D
r. Dea
n A. H
endr
ickso
n

ModernEquineVet.com | Issue 12/2015 13
Risk factors exist in horse racing in Switzerland, which are specific to each discipline (trot, flat and obstacle), according to a new study by researchers at the University of berne.
This retrospective study aimed to evaluate the risk factors related to clinical injury in various horse racing disciplines in Switzerland. The researchers analyzed all race starts in flat, obstacle and trot rac-ing over four years, including a total of 17,760 race starts in 1,738 races at 10 racecourses.
The age, sex, earnings, distance and time raced, place, jockey/driv-er, owner, trainer, track surface typeand (if grass) the surface con-ditions were recorded. racetrack veterinarians recorded clinical and non-clinical observations and recorded these with a standard-ized Veterinary code system.
At least one Veterinary code was
recorded for 525 horses: the most common was non-clinical one, i.e. Non-Starter. The highest incidence of Veterinary codes was associated with obstacle races (106/1000 starts), followed by flat races (27/1000) and then trot races (21/1000).
Multivariable logistic regres-sion models were used to analyze risk factors in each discipline. Horses were more often recorded as fallen or pulled up in obstacle races than in other disciplines. Horses finishing over eighth place had a higher risk of clinical events than those placed 1–3 in flat, ob-stacle and trotting races. In trot racing, gait abnormalities and lameness were the most common Veterinary codes recorded and there was a lower risk of clinical events for runners on porphyre sand than on grass. The risk was approximately doubled for those whose driver was also their train-
er. The researchers speculated that this may be due to trainers feeling more able to take risks when driv-ing their own horse.
In flat racing, one race course had a higher risk of clinical events than some of the others but no as-sociations were found relating to the race course surface. obstacle races of over 2,401 meters carried a lower risk of injury.
The researchers pointed out that some confounding factors may ac-count for some of the associations found in this study, and that there is a need to improve the standardiza-tion of event recording. However, the study represents a positive initial step in identifying risk factors for racing injury that may allow steps to be taken toward prevention.
Further study is required to determine how these factors influ-ence rates of injury and how they can be reduced. MeV
©
Schweizer C, Ramseyer A, Gerber V, et al. Retrospective evaluation of all recorded horse race starts in Switzerland during a four year period focusing on disciplinespecific risk factors for clinical events. Equine Vet J 2015 [Epub ahead of print Nov. 18, 2015] http://onlinelibrary.wiley.com/doi/10.1111/evj.12515/abstract
For more information:
Shut
terst
ock/
Vent
ura
Risk factorsfor injury in Swiss horse racing
sporTs MediCine

14 Issue 12/2015 | ModernEquineVet.com
A burgeoning service at the Uc Davis veterinary hos-pital is its Equine Integrative Sports Medicine Service. consisting of an array of complementary medical and evaluative procedures, the service is attracting many clients looking to maximize the performance of their sport horses.
Led by Sarah le Jeune, cVA, cert, Vet. chiro, DVM, assistant professor of clinical surgical and radiological sciences, who is board certified in surgery and sports medicine/rehabilitation, as well as certified in acupunc-ture and chiropractic, the service offers treatments and
evaluations of the entire equine athlete.With the subtlest issues potentially affecting an ath-
lete, Dr. le Jeune said it is important to examine every aspect of a horse and its equipment, right down to a blanket or a small piece of tack. beyond physical limi-tations such as injuries, equipment can certainly play a role in determining the success of an athlete. one of the most important elements of peak performance can be proper saddle fit. Ill-fitting saddles can be a deter-mining factor in a horse with back pain. Many saddles are too narrow and can pinch a horse’s back, causing significant restrictions of back movement, which is critical to proper functionality of an athlete.
Many of Dr. le Jeune’s patients compete in dressage, where a horse’s performance is judged on its gaits and movements. Even the slightest ailment can cause a decrease in performance and ultimate score. So while Dr. le Jeune evaluates for limb lameness and other sig-nificant ailments, she also examines secondary factors like a horse’s hoofs, teeth, and diet. The benefit for her
clients of using Uc Davis is that if Dr. le Jeune discov-ers a dental or nutrition issue, she can consult with Uc Davis’ board-certified experts in those areas without having to refer the horse to another facility, saving her clients added trips to other locations.
Many of Dr. le Jeune’s appointments are not at the hospital. She prefers to see horses in their home en-vironment. Traveling to a hospital can cause a horse’s adrenaline to mask any mild or subtle issues it may have. by seeing them in their natural environment, however, horses remain calm and the evaluation will reveal their true state of health. Home visits also give Dr. le Jeune an opportunity to evaluate a training ses-sion with a horse’s rider and trainer, giving her a better understanding of that horse’s condition. often times, Dr. le Jeune will even ride a horse herself to get a feel for more subtle issues that can only be discovered by riding rather than by examining.
Working with trainers is important to gain insight into the full background of a horse and what may be affecting its optimal performance. Is the horse having behavioral issues or is it in pain?
“In my experience, most of those issues are pain related,” said Dr. le Jeune. “rarely are there truly pri-mary behavioral issues. Most horses want to do what we want them to do. The reason they’re not doing a particular task is because there’s pain.”
After discovering the cause of pain, there are sev-eral treatment options Dr. le Jeune can perform. Some major injuries will require surgery, and she will work with clients to rehabilitate the horse and hopefully re-turn it to competition. recovery for equine athletes is similar to that for human athletes, and Dr. le Jeune will team with trainers to determine the proper timing of recovery procedures and workouts.
Many times, an athlete’s back, neck or muscle pain can be treated with chiropractic and acupuncture treatments. These procedures are becoming increas-ingly popular, and can easily be integrated into con-ventional diagnostic and treatment modalities to opti-mize clinical outcome.
In addition to equine athletes, Dr. le Jeune also sees livestock athletes, such as bucking bulls. bulls with back pain simply won’t perform. Like other animals, many livestock also respond positively to acupuncture to alleviate their pain. previously, she has used acu-puncture to optimize the performance of a popular bull from the professional bull riders tour.
Not every patient of Dr. le Jeune’s is an athlete, though. Many non-athletes also benefit from her service, such as geriatric or arthritic horses that have trouble standing up and laying down. MeV
news noTes
Uc davis integrates Sports Medicine for Horses
dr. Sarah le Jeune applies a chiropractic treatment at the Equine integrative Sports Medicine Service at Uc davis veterinary hospital.
Phot
o cou
rtesy
of U
niver
sity o
f Cali
forn
ia Da
vis

ModernEquineVet.com | Issue 12/2015 15
The American Association of Equine practitioners (AAEp) presented Nathaniel A. White II, DVM, MS, DAcVS, with the Distinguished Life Member Award for his leadership and substantial volunteerism within the as-sociation during his 43 years of membership.
The Distinguished Life Member Award honors an AAEp member who has made outstanding contribu-tions to the association throughout his or her career. Dr. White, professor emeritus of equine surgery at Virgin-ia-Maryland college of Veterinary Medicine’s Marion dupont Scott Equine Medical center and president of the AAEp in 2010, is chair of the AAEp’s National Equine Health plan Task Force, which is establishing an Equine Disease communication center to serve as a national hub for equine disease reporting. He serves on the management board and as co-U.S. editor of Equine Veterinary Education.
A 1971 graduate of cornell University, Dr. White was instrumental in the establishment and served as long-time chair of the AAEp Foundation, which has distrib-uted more than $3.3 million to improve the welfare of the horse. He served two terms on the AAEp board of direc-tors, volunteered with the AAEp on call program from 1994–2000, delivered the 2006 Frank J. Milne State-of-the-Art Lecture and received the AAEp’s Distinguished Service Award in 2004.
Since joining the AAEp in 1973, Dr. White has also volunteered his time and expertise through service on numerous committees and councils, including Abstract review, convention planning, Educational programs, Finance, Nominating, president’s Advisory, public poli-cy, research, Student relations, and Trail and Events.
Also honored were Virginia Reef, DVM, DAcVIM, DAcVSMr, DEcVDI, director of large animal cardiol-ogy and diagnostic ultrasonography at the University of pennsylvania School of Veterinary Medicine, who re-ceived the American Association of Equine practitioners 2015 Distinguished Educator—Academic Award and John W. Lee Jr., DVM, who received the 2015 Distin-guished Educator—Mentor Award.
The Distinguished Educator—Academic Award honors an individual who has demonstrated a sig-nificant impact on the development and training of equine practitioners.
A pioneer in the diagnostic use of ultrasonographic technology, Dr. reef perfected the technology in her clini-cal use and then taught it to students and practitioners alike. In the ensuing 30-plus years, ultrasonography has contributed to early diagnosis of musculoskeletal injury, significantly reducing catastrophic athletic tendon and ligament injuries.
Many practitioners who use ultrasound have been
AAEP Honors dr. nathaniel A. White ii, othersinfluenced by Dr. reef, whether in the classroom, in the lab or through her hundreds of publications that include more than 50 original re-search papers, over 50 case reports, about 130 abstracts in proceedings, 11 major review articles and 80 book chapters.
Dr. reef is an invited speaker at domestic and interna-tional meetings. Her dedication to expanding ultrasonog-raphy technique among her veterinary colleagues is fur-ther evident when conducting wet labs. Dr. reef seeks out local practitioners to procure live horses with the types of injuries she is teaching, arranges shipping of these horses to the wet lab and coordinates co-instructors and assistants to ensure a first-class learning experience for attendees.
Dr. reef earned her DVM in 1979 from The ohio State University. She completed her internship and resi-dency in large animal medicine in 1982 at penn Vet, where she has served on the faculty ever since. She is the Mark Whittier and Lila Griswold Allam professor of Medicine as well as section chief of sports medicine and imaging at penn Vet’s New bolton center. Among her honors and awards are the Michael Moxon Kate Memo-rial Distinguished Lecturer Award and The ohio State University Distinguished Alumnus Award.
recently retired, Dr. Lee's enthusiastic support and guidance of new veterinarians and students helped shape many successful careers. The Distinguished Educator—Mentor Award honors an individual who has demonstrated a significant impact on the develop-ment of equine practitioners through mentoring.
A 1974 graduate of cornell University, Dr. Lee founded Unionville Equine Associates in oxford, penn., where he practiced from 1983 until relocating to New Mexico in May. During this time, he nurtured the confidence and development of his young team members gradually by presenting challenges in a manner that encouraged in-dependent thinking while honing their craft. Dr. Lee also promoted a healthy growth trajectory by helping his team develop professional connections throughout the industry and by presenting opportunities for career advancement.
His influence also extended to students through insti-tution of a formal internship/externship program at the practice and his enthusiasm to share his joy of veterinary medicine and serve as a source of advice and support to the many high school, college and veterinary school stu-dents who shadowed Dr. Lee on ride-alongs. MeV
nathaniel A. White ii, dvM, MS, dAcvS
John W. lee Jr., dvMvirginia Reef, dvM, dAcviM, dAcvSMR, dEcvdi
Phot
os co
urte
sy of
AAEP

AAEVT MembershipBi-Annual NewsletterWeekly “HoofBeats” Email NewsblastFull access to www.aaevt.org, including the Career Center and the LibraryUp-to-date information on the AAEVTDiscounted registration for AAEVT Regional Meetings and the annual AAEP/AAEVT ConventionNTRA, Working Advantage and Platinum Performance BenefitsThe opportunity to participate in the AAEVT Online Certification Program or to become a member of the AEVNT Academy-Specialty in Equine Veterinary Nursing Scholarship opportunities. AAEVT’s Equine Manual for Veterinary Technicians (Blackwell Publishing 20% discount on purchase price)Opportunity to attend Purina’s Annual Equine Veterinary Technician Conference - All Expenses paid!
•••••
•••
••
•
AAEVT ObjectivesProvide opportunities for CE, training, communication, and networkingEducate the equine veterinary community and the public about our professionInform Members of issues affecting our professionAssist in providing the best medical care to improve the health and welfare of the horse
••••
AAEVT Online Equine Certification ProgramA three course, 10 module, equine-only online program offered through ACTGeared toward Credentialed Veterinary Technicians, Assistants, Support staff, & StudentsAreas of study include: equine medical terminology, anatomy and physiology, parasitology, laboratory, diagnostics, equine basics (breeds, wellness, husbandry,) diagnostic procedures, emergency medicine, restraint, pharmacology, surgical assistance and anesthesia, equine office proceduresA certificate of completion is awarded to those who: Successfully complete required courses Complete the list of required skills (per a supervising DVM who is an AAEP member) Attend an AAEVT regional CE symposium and participate in the we labsThose individuals who successfully complete the programs will be recognized as AAEVT Certified Equine Veterinary Technicians / AAEVT Certified Equine Veterinary Assistants depending on their current designation. The certificate is recognized by the AAEVT and the AAEP but does not grant the credentialed status by the AVMAFor more information go to www.aaevt.4act.com or call 800-357-3182
•••
•
•
•
For mo re in f o r mat i on vi st www.aae vt.org*American Association of Equine Veterinary Technicians and Assistants
AAEVT Mission Statement: To promote the health and welfare of the horse through the education and professional enrichment of the equine veterinary technician and assistant.
AAEV T M E M b E r s h i pMembership in the AAEVT is open to all veterinary technicians, assistants, support staff and those employed in the veterinary health care industry worldwide. Student membership is open to those currently enrolled in an AVMA/CVMA accredited veterinary technology program.

ModernEquineVet.com | Issue 12/2015 17
AAEVT MembershipBi-Annual NewsletterWeekly “HoofBeats” Email NewsblastFull access to www.aaevt.org, including the Career Center and the LibraryUp-to-date information on the AAEVTDiscounted registration for AAEVT Regional Meetings and the annual AAEP/AAEVT ConventionNTRA, Working Advantage and Platinum Performance BenefitsThe opportunity to participate in the AAEVT Online Certification Program or to become a member of the AEVNT Academy-Specialty in Equine Veterinary Nursing Scholarship opportunities. AAEVT’s Equine Manual for Veterinary Technicians (Blackwell Publishing 20% discount on purchase price)Opportunity to attend Purina’s Annual Equine Veterinary Technician Conference - All Expenses paid!
•••••
•••
••
•
AAEVT ObjectivesProvide opportunities for CE, training, communication, and networkingEducate the equine veterinary community and the public about our professionInform Members of issues affecting our professionAssist in providing the best medical care to improve the health and welfare of the horse
••••
AAEVT Online Equine Certification ProgramA three course, 10 module, equine-only online program offered through ACTGeared toward Credentialed Veterinary Technicians, Assistants, Support staff, & StudentsAreas of study include: equine medical terminology, anatomy and physiology, parasitology, laboratory, diagnostics, equine basics (breeds, wellness, husbandry,) diagnostic procedures, emergency medicine, restraint, pharmacology, surgical assistance and anesthesia, equine office proceduresA certificate of completion is awarded to those who: Successfully complete required courses Complete the list of required skills (per a supervising DVM who is an AAEP member) Attend an AAEVT regional CE symposium and participate in the we labsThose individuals who successfully complete the programs will be recognized as AAEVT Certified Equine Veterinary Technicians / AAEVT Certified Equine Veterinary Assistants depending on their current designation. The certificate is recognized by the AAEVT and the AAEP but does not grant the credentialed status by the AVMAFor more information go to www.aaevt.4act.com or call 800-357-3182
•••
•
•
•
For m ore i nf or m at i on vi st www.aae v t.org*American Association of Equine Veterinary Technicians and Assistants
AAEVT Mission Statement: To promote the health and welfare of the horse through the education and professional enrichment of the equine veterinary technician and assistant.
AAEV T M E M b E r s h i pMembership in the AAEVT is open to all veterinary technicians, assistants, support staff and those employed in the veterinary health care industry worldwide. Student membership is open to those currently enrolled in an AVMA/CVMA accredited veterinary technology program.
TeChniCian updaTe
By Jenna Powell, BS, RVT of San Dieguito Equine Group
A 17-year-old mare, used for polo, was presented for treatment of a wound with a chronic draining tract.
The wound occurred approximately four weeks prior to presentation when the mare was kicked while in the pasture. The wound was located on the mare’s proximal left hind limb, corresponding with the cra-nial aspect of the proximal tibia. radiographs were taken one week prior to presentation and confirmed the presence of a sequestrum.
The wound was cleaned and aseptically probed. The wound tract extended to the surface of the proximal tibia. The bone surface was rough and irregular. An ul-trasonogram showed an irregular surface on both the proximal and cranial surfaces of the tibia. The irregular surfaces corresponded with the presence of the seques-trum. In the interest of proper healing and a return to work, the horse underwent surgery for debridement of the bone surface and removal of the sequestrum.
The mare was brought to the clinic five days later and surgery was scheduled for the next day. The pre-surgical bloodwork revealed that the mare was healthy and able to undergo the planned general anesthesia.
For the surgery, a 14-gauge, 5.25 inch IV catheter was placed in the left jugular vein, and 3 g of IV gen-tamicin and 2 g IV phenylbutazone were administered. Nine million units of IM procaine penicillin G and 5 mg of detomidine were administered, and the patient was walked to the surgery suite. The mare was tranquil-ized with 350 mg xylazine. Anesthesia was induced us-ing 30 mg of diazepam and 1.5 g of ketamine.
The induction went smoothly, and the patient was placed in right lateral recumbency on the surgery table. The surgical plane of anesthesia was maintained using inhaled isoflurane. The left hind leg was clipped from hock to stifle and then aseptically prepped and draped with an Ioban. An orthopedic surgical drape was then placed over the whole leg. An 8 cm incision was made over the cranial aspect of the proximal tibia and the ab-normal tissue of the draining tract was identified and resected. The cranial surface of the tibia and the seques-trum were debrided.
The bone surface was lavaged with saline and ami-kacin. Next, the subcutaneous tissue was closed over the bone surface using absorbable suture. The cuta-neous tissue was closed with non-absorbable suture.
surgical removal of a sequestrum on the proximal Tibia
The patient was taken off of isoflurane inhalation anesthesia as the closing of the surgical incision was started. A sterile bandage was placed over the surgi-cal site. The mare was moved to recovery and placed in right lateral recumbency.
The mare had a smooth recovery but spent a pro-longed period in lateral recumbency before standing. The mare was administered 5 g IV methocarbamol af-ter standing to help with residual muscle spasms and cramping. The day after surgery, the mare was sore and stiff on her left hind leg but began to ambulate more freely as she walked. The mare was released to her own-er with instructions to keep the mare on stall rest. The owner was given the following medications to admin-ister: 1.5 g doxycycline to be given orally twice a day for 14 days and 2 g phenylbutazone to be given orally once a day for five days. An appointment was made to recheck the mare three days postsurgery.
At her three day recheck, the mare was bright and eating, drinking, defecating, and urinating normally. She was ambulating well, the incision site was clean and the sutures were in place. There was no peri-incisional edema. At a recheck eight days after surgery, there was moderate swelling of the surgical incision and there was slight gaping at the proximal aspect of the incision.
Aspiration of the peri-incisional edema showed that a seroma had formed at the incision site. The se-roma was infused with 600 mg gentamicin, and the two distal sutures were removed from the incision site to facilitate draining.
Five days later (day 13 post-surgery), the surgical site was rechecked. The seroma was still present, and the incision site was sterilely prepped and drained again. Amikacin was infused into the seroma. At that time, the owner was advised to keep the mare on 1.5 g doxy-cycline orally twice a day for an additional seven days to help with any possible infection associated with the seroma. The mare was checked two more times in the following week, and made good progress. At the final recheck 23 days after surgery, the mare was given clear-ance to make a gradual return to work provided that she did not become lame with increased exercise.
Special thanks to Dr. Maureen Kelleher and Dr. Mi-chael Manno for their assistance. MeV
about the authorBy Jenna Powell, BS, RVT, is an equine technician at San Dieguito Equine Group in San Marcos, Calif.

reach your veterinarians wherever they are, whenever they want.
For aDVerTISIng raTeS anD InForMaTIon, eMaIlMatthew Todd
Equine VetThe Modern