Embed Size (px)
DESCRIPTION
Serious Mental Illness module Lecture I Chris Gale Department of Psychological Medicine, Dunedin School of Medicine. University of Otago. The NZ mental health plan and serious mental illness. New Zealand Mental Health Plan. Official documents: Te Tahuhu - PowerPoint PPT Presentation
Citation preview
The NZ mental health plan and serious mental illness.
Serious Mental Illness module
Lecture I
Chris Gale
Department of Psychological Medicine,Dunedin School of Medicine.
University of Otago
New Zealand Mental Health Plan.
Official documents: Te Tahuhu Te Tahuhu is the ridgepole that provides essential
support. Full document emphasisies that all these issues need to
be implemented by the collective of people. Language remains politically correct, without good
definitions (particularly of recovery), and does not consider evidence base around treatment.
Services are left with multiple goals, at times conflicted. This has led to this document being of limited utility to clinicians.
The following text is taken from the website.
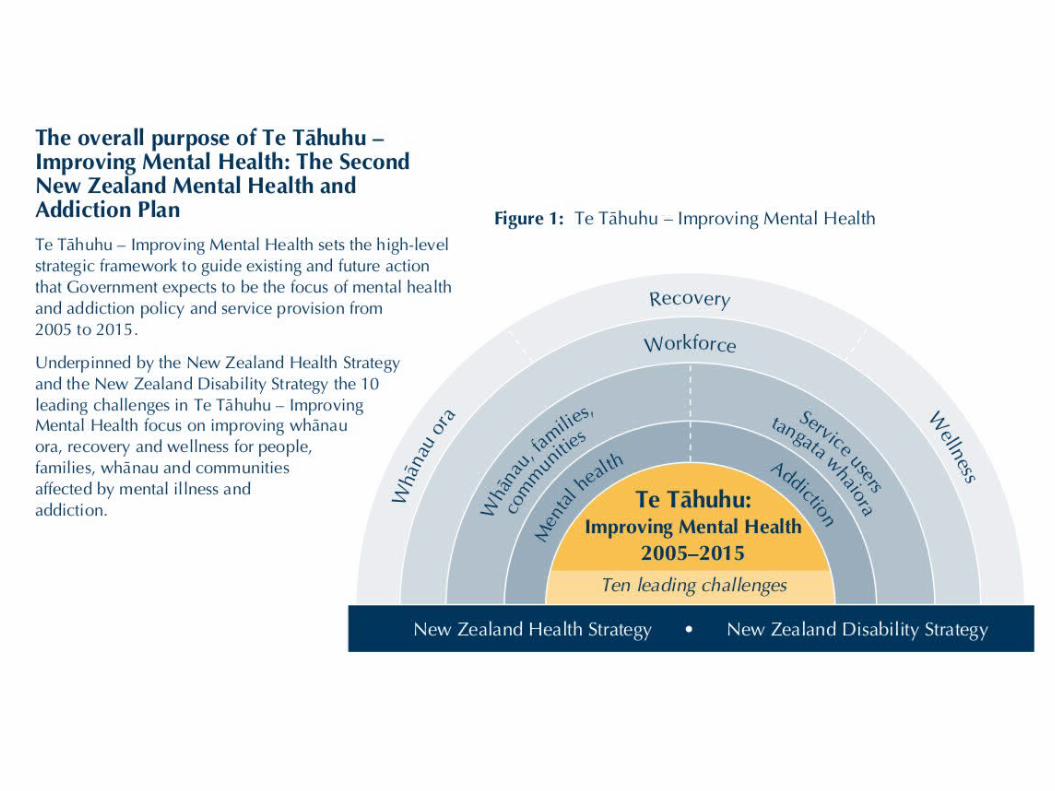
Te Tāhuhu – Improving Mental health 2005-2015
Te Tāhuhu: Improving Mental Health outlines Government policy and priorities for mental health and addiction for the 10 years between 2005 and 2015, and provides an overall direction for investment in mental health and addiction. It builds on the current Mental Health Strategy contained in Looking Forward (1994) and Moving Forward (1997), and the Mental Health Commission’s Blueprint for Mental Health Services (1998).
Te Tāhuhu – Improving Mental Health has been informed by extensive public consultation and consultation with the health sector over the past 18 months and responds, in particular to the calls from the sector for a more strategic and over-arching plan. It is based on an outcomes framework and describes ten leading challenges that need to be addressed in order for government outcomes for mental health and addiction to be achieved.
All New Zealanders in their communities
People make informed decisions to promote their mental health
and wellbeing value diversity and support and enable people with
experience of mental illness and addiction to fully participate in society and in the everyday life of their communities and whānau
Service see a trusted and high-performing mental health and
addiction sector, and have confidence that if they need them, they can access high-quality mental health and addiction services
People with experience of mental illness and addiction
Person have the same opportunities as everyone else to fully
participate in society and in the everyday life of their communities and whānau
Service experience trustworthy agencies that work across
boundaries and enable service users to lead their own recovery
experience recovery-focused mental health services that provide choice, promote independence, and are effective, efficient, responsive and timely
Whānau and friends who support and who are affected by people with experience of mental
illness and addiction Person
maintain their own wellbeing and participate in society and in the everyday life of their communities and whānau
Service experience agencies that operate in a way which
enables them to support their family members’ recovery and maintain their own wellbeing
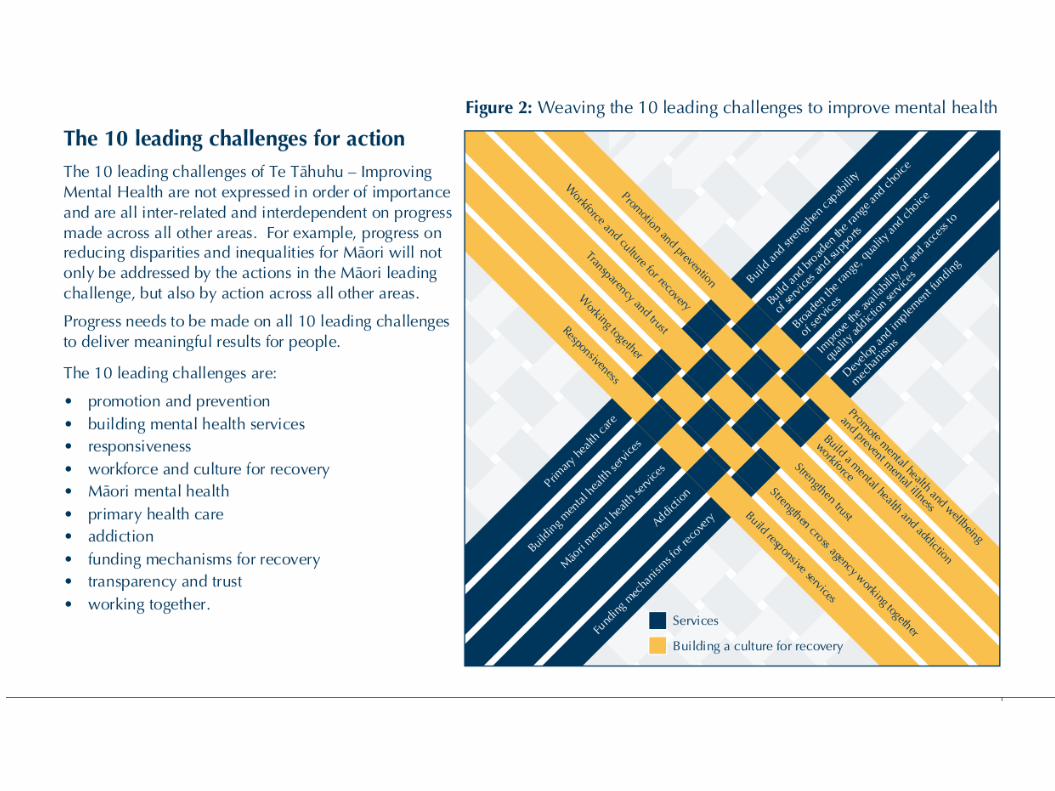
Leading Challenges. Promotion and prevention
Promote mental health and wellbeing and prevent mental illness and addiction Building mental health services
Build and broaden the range and choice of services and supports, which are funded for people who are severely affected by mental illness Responsiveness
Build responsive services for people who are severely affected by mental illness and/or addiction Workforce and culture for recovery
Build a mental health and addiction workforce -- and foster a culture amongst providers -- that supports recovery, is person centred, culturally capable, and delivers an ongoing commitment to assure and improve the quality of services for people
Māori mental health
Continue to broaden the range, quality and choice of mental health and addiction services for Māori Primary health care
Build and strengthen the capability of the primary health care sector to promote mental health and wellbeing and to respond to the needs of people with mental illness and addiction
Addiction
Improve the availability of and access to quality addiction services, and strengthen the alignment between addiction services and services for people with mental illness
Funding mechanisms for recovery
Develop and implement funding mechanisms for mental health and addiction that support recovery, advance best practice and enable collaboration
Transparency and trust
Strengthen trust in services and accountability and information systems Working together
Strengthen cross-agency working together
Te Kōkiri: The Mental Health and Addiction Action Plan 2006-2015
Te Kōkiri: The Mental Health and Addiction Action Plan has been developed to directly implement Te Tāhuhu – Improving Mental Health 2005-2015: The Second New Zealand Mental Health and Addiction Plan.
Te Kōkiri is the result of extensive consultation with the mental health and addiction sector over the past two years.
The Ministry of Health and District Health Boards jointly developed the action plan and undertook a comprehensive approach to its development.
An Advisory Group was established in August 2005 made up of representatives of the Mental Health Commission and District Health Boards, along with individuals selected on the basis of their expertise, skills and knowledge. A process of pre-consultation on a draft to elicit broader sector feedback included: senior peer reviewers feedback on a draft from key stakeholders presentations to key groups.
This was followed by a formal consultation period and analysis of submissions, in March/April 2006. Te Kōkiri is a high-level document that takes a comprehensive approach, and like Te Tāhuhu –
Improving Mental Health includes a mix of both high-level initiatives and specific operational actions. In relation to specific actions, key stakeholders and milestones/measures are identified. Timeframes are set and clustered around three time periods, 1-3 years, 3-5 years and 5-10 years.
The action plan also clearly defines the responsibilities of the Ministry of Health and District Health Boards, the two agencies with stewardship responsibilities for implementing the action plan.
Te Kokori as a centrally directed document..
Long. Detailed, but without hard outcomes. Over emphasis political needs not research base:
Sense that the government can manage research and determine outcomes.
Directions towards recovery, inclusiveness. Lack of ethical considerations (lost in postmodern sense of
silence). Driven by ministry and managerial clinicians. Important for DHBs as the government is the monopoly
funder.
Consequences of the national guidelines.
One size fits all outcomes. Denigration of professional skills. Elevation of central planners and managers.
Paradoxically, a loss of political power by consumers who are now subsumed into the ministerial discourse.
Use of terms without clear definitions or not needed: Tanagata Whaiora. Recovery.
Problems with definitions.
What is the purpose of mental health? What is “Serious Mental Illness”? Who is a mental health user? What is recovery?
Psychiatry vs mental health.
Psychiatry is part of medicine. We treat diseases: cure, control, comfort. We deal with people who have illnesses, within the ethical bases
and boundaries of medicine. We use a clinical and scientific evidence base to do this.
Mental Health is wholistic. Not just the absence of disease, but wellbeing. Based on populations Paradoxically, easy to measure, and general approach is taken
from a political or public health paradigm. This can and has been subverted during the neoliberal (Thatcherite
in UK) move to all aspects of government being run by technocratic managers, as if in a market.
What is “Serious Mental Illness”
USA The definition of SMI stipulated in PL 102-321 requires the person to
have at least one 12-month DSM disorder, other than a substance use disorder, and to have "serious impairment." Subsequently, SAMHSA decided that "serious impairment" should be defined as a Global Assessment of Functioning (GAF) score of less than 60.
(Kessler, Arch Gen Psych, 2003)
UKFor 25 years the care of serious mental illness (SMI; which usually
denotes schizophrenia, severe depression, and mania)...
(Marks, Brit J Psych, 1994)
What is recovery?
Abscence of disease – equivelant to remission (which we can measure eg. HAM-A less than seven for GAD).
Living well with a disability (or by extension, a disease).
Taking the symptoms of mental illness and turning remission into a form of spiritual growth.
A form of political empowerment for people who have been in the psychiatric system. (Often associated with antipsychiatry)
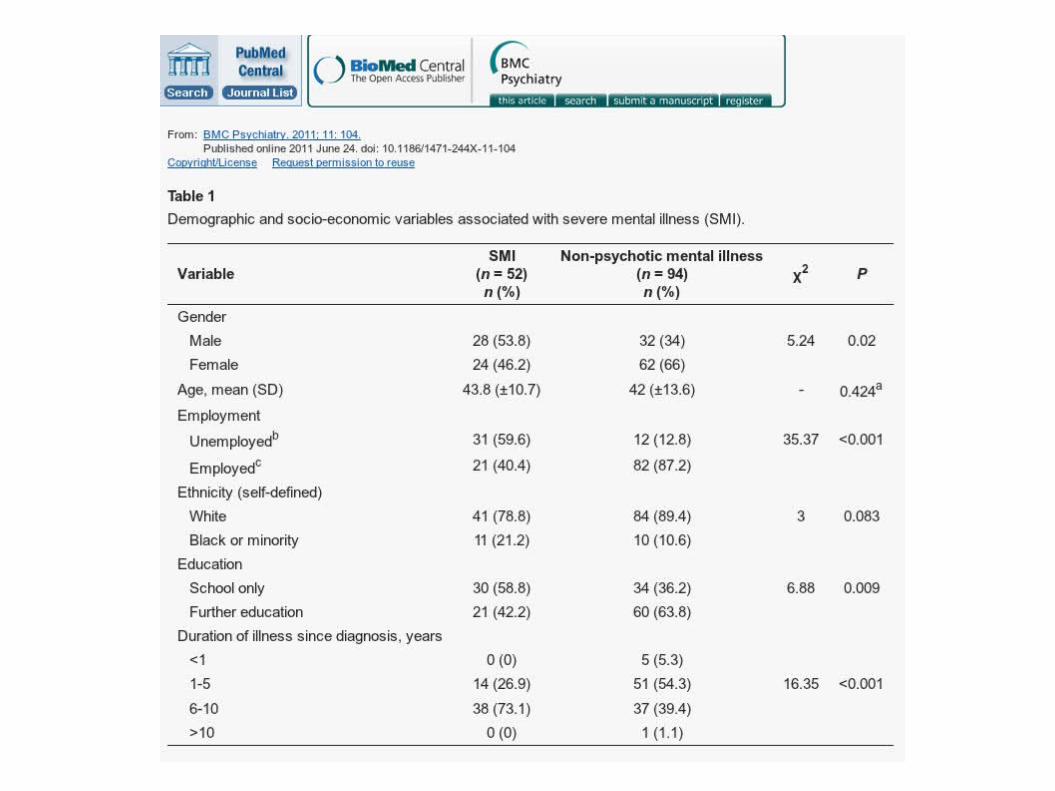
Who has SMI? Buhagiar K, Parsonage L, Osborn DP. BMC Psychiatry 2011 Jun 24
People with SMI and non-psychotic mental illness were recruited from an out-patient adult mental health service in London.
Cross-sectional comparison between the two groups was conducted by means of a self-completed questionnaire.
A total of 146 people participated in the study, 52 with SMI and 94 with non-psychotic mental illness. There was no statistical difference between the two groups with respect to the perception of global physical health.
However, physical health was considered to be a less important priority in life by people with SMI (OR 0.5, 95% CI 0.2-0.9, p = 0.029). There was no difference between the two groups in their desire to change high risk behaviours.
People with SMI are more likely to have a health locus of control determined by powerful others (p < 0.001) and chance (p = 0.006).
People with SMI appear to give less priority to their physical health needs. Health promotion for people with SMI should aim to raise awareness of modifiable high-risk lifestyle factors. Findings related to locus of control may provide a theoretical focus for clinical intervention in order to promote a much needed behavioural change in this marginalised group of people.
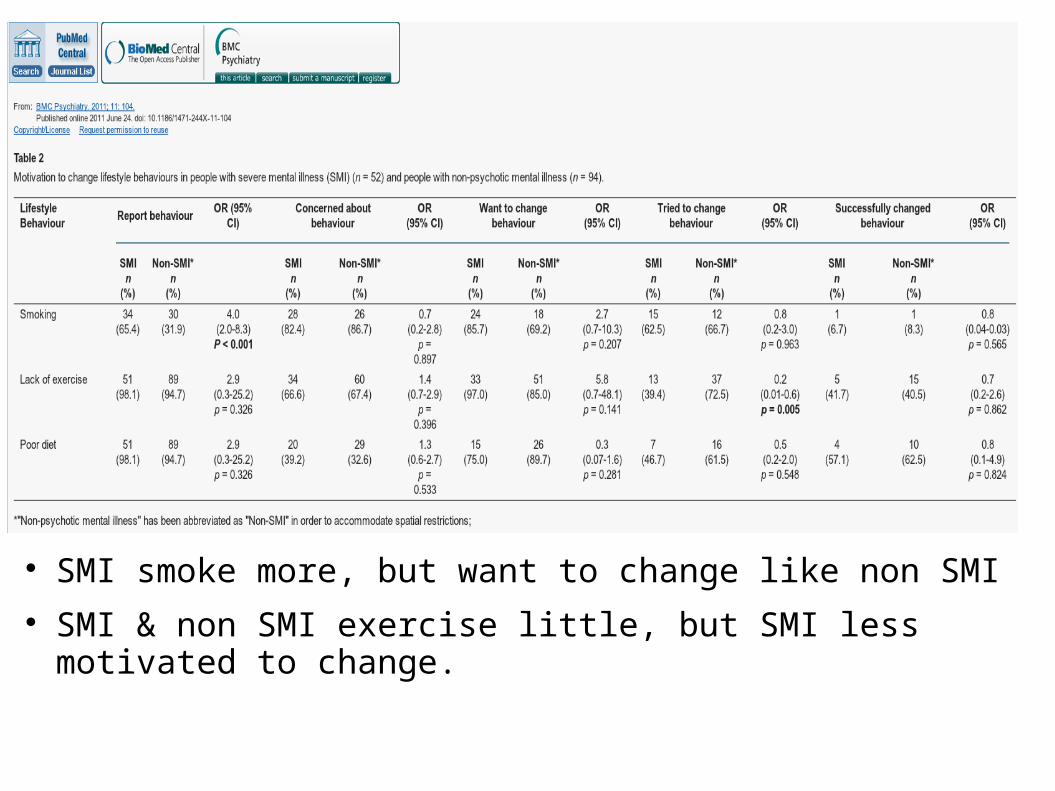
SMI smoke more, but want to change like non SMI SMI & non SMI exercise little, but SMI less motivated to
change.
Does SMI Matter. (Hayes, Cheung et al, J Psychom Res. Feb
2012) Aim to see if aggression, hallucinations, delusions or other factors
contribute to excess mortalility in SMI. SMI cases > 15 years in large mental healthcare case register (South
London and Maudsley Trust (SLaM), 2007 – 2010 6880 cases, 242 deaths Bipolar disorder was associated with reduced mortality risk compared to
schizophrenia (HR 0.7; 95% CI 0.4–0.96; p = 0.028). Mortality was not significantly associated with hallucinations and
delusions or overactive–aggressive behaviour, but was associated with physical illness/disability.
There was a positive association between mortality and subclinical depression among individuals with schizophrenia (HR 1.5; 1.1–2.2; p = 0.019) but a negative association with subclinical and more severe depression among those with schizoaffective disorder (HR 0.1; 0.02–0.4; p = 0.001 and 0.3; 0.1–0.8; p = 0.021, respectively).
Variables Crude hazard ratio (95% CI)
Adjusted hazard ratio (95% CI)
Adjusted P value
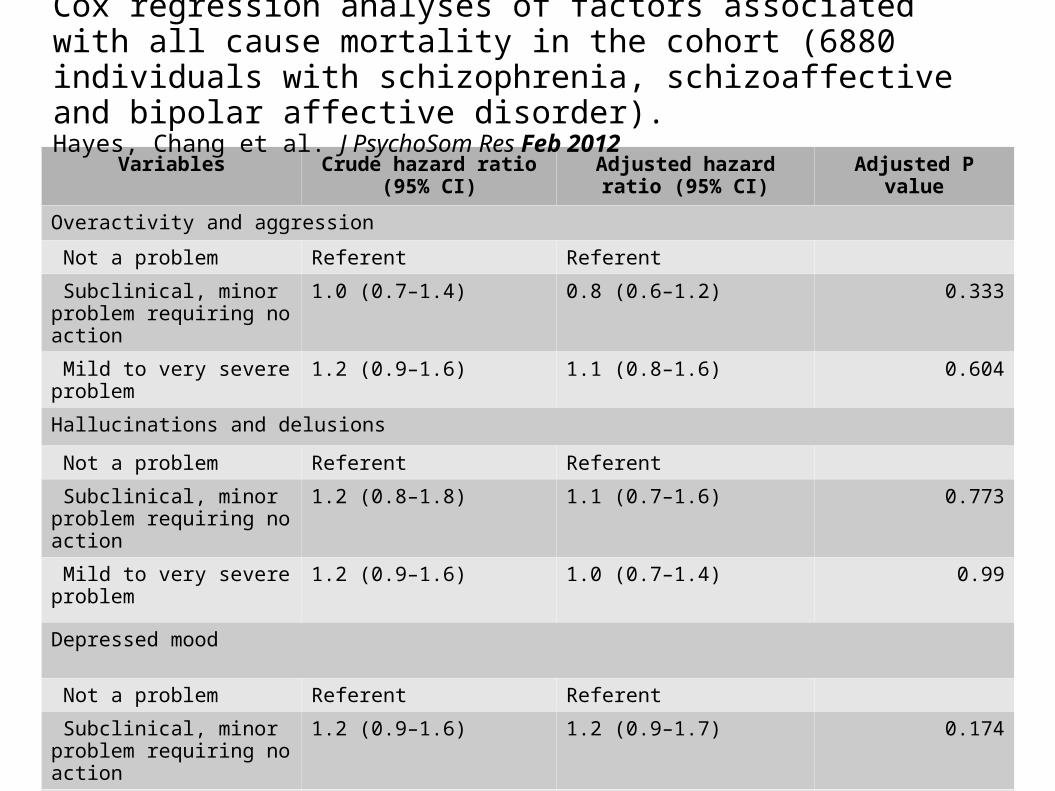
Overactivity and aggression
Not a problem Referent Referent
Subclinical, minor problem requiring no action
1.0 (0.7–1.4) 0.8 (0.6–1.2) 0.333
Mild to very severe problem
1.2 (0.9–1.6) 1.1 (0.8–1.6) 0.604
Hallucinations and delusions
Not a problem Referent Referent
Subclinical, minor problem requiring no action
1.2 (0.8–1.8) 1.1 (0.7–1.6) 0.773
Mild to very severe problem
1.2 (0.9–1.6) 1.0 (0.7–1.4) 0.99
Depressed mood
Not a problem Referent Referent
Subclinical, minor problem requiring no action
1.2 (0.9–1.6) 1.2 (0.9–1.7) 0.174
Mild to very severe problem
0.9 (0.6–1.2) 0.9 (0.6–1.3) 0.534
Cox regression analyses of factors associated with all cause mortality in the cohort (6880 individuals with schizophrenia, schizoaffective and bipolar affective disorder). Hayes, Chang et al. J PsychoSom Res Feb 2012
Variables Crude hazard ratio (95% CI)
Adjusted hazard ratio (95% CI)
Adjusted P value
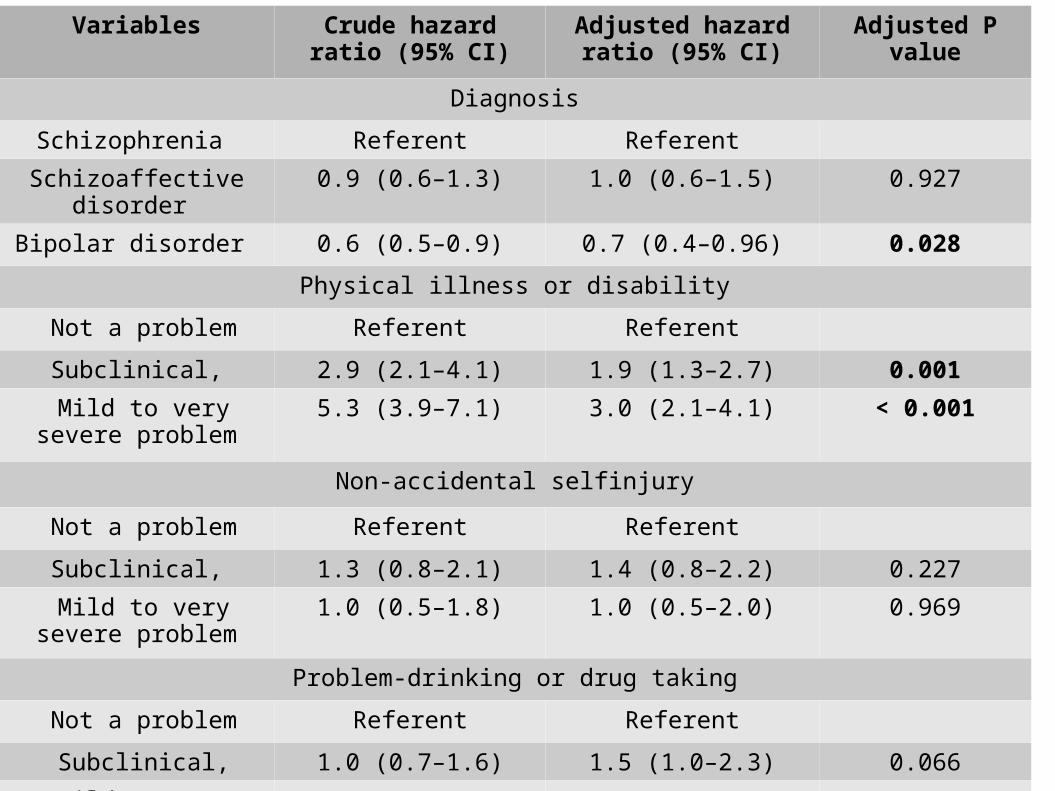
Diagnosis
Schizophrenia Referent Referent
Schizoaffective disorder 0.9 (0.6–1.3) 1.0 (0.6–1.5) 0.927
Bipolar disorder 0.6 (0.5–0.9) 0.7 (0.4–0.96) 0.028
Physical illness or disability
Not a problem Referent Referent
Subclinical, 2.9 (2.1–4.1) 1.9 (1.3–2.7) 0.001
Mild to very severe problem
5.3 (3.9–7.1) 3.0 (2.1–4.1) < 0.001
Non-accidental selfinjury
Not a problem Referent Referent
Subclinical, 1.3 (0.8–2.1) 1.4 (0.8–2.2) 0.227
Mild to very severe problem
1.0 (0.5–1.8) 1.0 (0.5–2.0) 0.969
Problem-drinking or drug taking
Not a problem Referent Referent
Subclinical, 1.0 (0.7–1.6) 1.5 (1.0–2.3) 0.066
Mild to very severe problem
0.9 (0.6–1.3) 1.2 (0.8–1.8) 0.444
Variables Crude hazard ratio (95% CI)
Adjusted hazard ratio (95% CI)
Adjusted P value
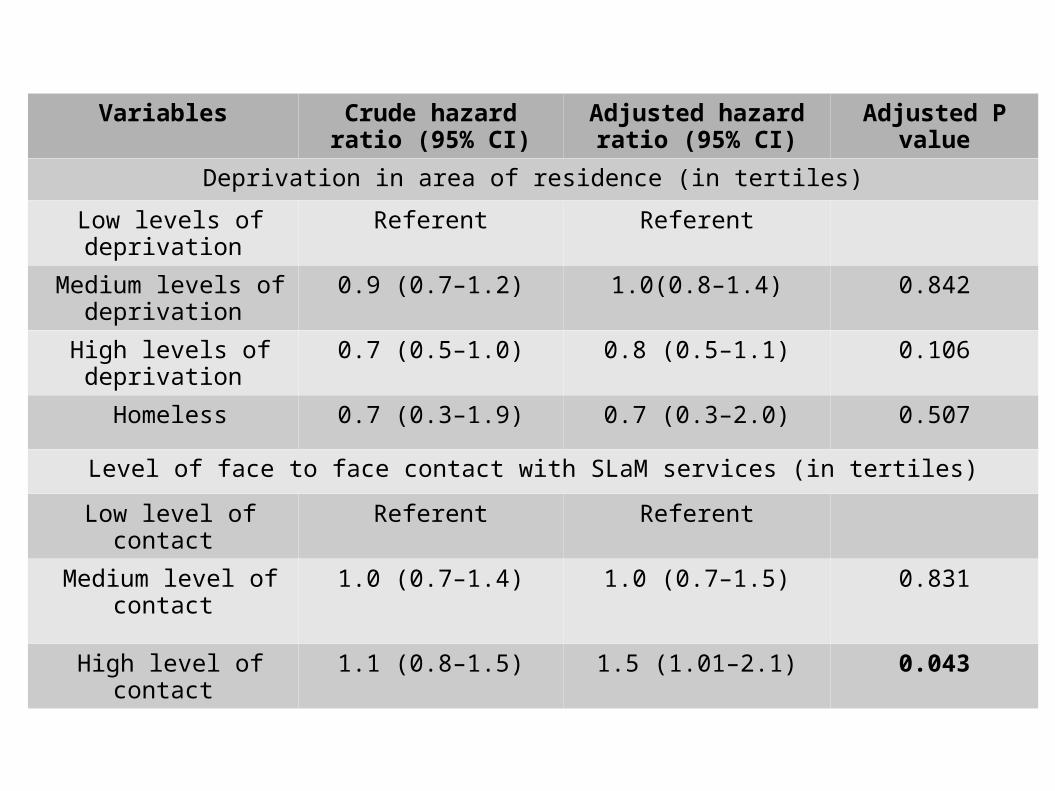
Deprivation in area of residence (in tertiles)
Low levels of deprivation
Referent Referent
Medium levels of deprivation
0.9 (0.7–1.2) 1.0(0.8–1.4) 0.842
High levels of deprivation
0.7 (0.5–1.0) 0.8 (0.5–1.1) 0.106
Homeless 0.7 (0.3–1.9) 0.7 (0.3–2.0) 0.507
Level of face to face contact with SLaM services (in tertiles)
Low level of contact Referent Referent
Medium level of contact
1.0 (0.7–1.4) 1.0 (0.7–1.5) 0.831
High level of contact 1.1 (0.8–1.5) 1.5 (1.01–2.1) 0.043
Comments SMI.
SMI is best seen as following diagnoses. Level of disability is high.
SMI are different from non SMI in clinical populations.
SMI may not predict premature death, but a diagnosis of schizophrenia does. Comorbid physical problems are highly significant. In South London, those in contact MHS were those
at highest risk.




![Penetti v. Quarterman: Mental Illness, the Death Penalty ... · Quarterman: Mental Illness, the Death ... defendants with mental disabilities, ... 2007] MENTAL ILLNESS, THE DEATH](https://img.pdfslide.net/doc/110x75/5b5ab3597f8b9ac7498c87d6/penetti-v-quarterman-mental-illness-the-death-penalty-quarterman-mental.jpg)