Embed Size (px)
Citation preview
THE PRIMARY HEALTH CARE PROVIDER’S COMPUTER AS A PARTNER IN TEACHING
Larry A. Green, M.D.
he primary care provider has unique op- T portunities and unique problems. As an entry point into the entire health care system, he or she may function as the observer of early manifestations of sickness and distress that may defy diagnosis; as a gatekeeper to the remainder of the health care delivery system; and in a setting of relative isolation from major medical center resources. In addition, the primary care provider, similar to most American physicians, is often a business per- son concerned with effectiveness, efficiency, overhead, and profit.
Only during the past 12 years have adequate and effective postdoctoral training programs existed to assist the explicit preparation of primary care providers. These programs ini- tially developed curricula based largely on the anecdotal experience of existing providers and now continue to pursue program refine- ments based upon the needs of served popu- lations and struggling providers. Among the impediments encountered by primary care providers seeking to meet the needs of the population under their care are: inadequate understanding of early disease and the process of primary care; coping with the knowledge explosion without the luxury of subspeciali- zation; having real information at the right time, i.e., when a particular patient’s manage- ment is in question. Effective information management in the office setting of the
primary care provider is a necessary step in overcoming these impediments.
Health care providers have always used information systems. Some use their memory and a 3 x 5 card, while others use peg boards and problem-oriented charts. Many are now turning to computers-first for financial man- agement and then, perhaps, for patient and practice management. Computers, used wisely in the primary care provider’s office, offer the opportunity to manage information and 1) help describe primary care without disrupting prac- tice; 2) cope with information overload asso- ciated with expanding medical knowledge; 3) access current knowledge quickly and con- veniently. The ingredients for data systems that can provide these descriptive, organiza- tional and accessing functions exist. The problems now are integration of components and use by providers. The experiences of the Family Medicine Information System (FMIS) developed by the Mountain Plains Outreach Program, Inc., Denver, offer some valuable lessons to those seeking further developments in office-based information systems.
The information required to do billing functions provides important descriptors of primary care. Encounter data must answer “who did what for whom, when, where, at what price.” Registration data must answer “who is in my practice, where do they live, and what payment mechanisms do they use.”
MOBIUS Volume 3, Number 2 00 0 1983 by The Regents of the University of California
26 MOBIUS
FMIS was designed to inextricably link data collection to billing.The result was a complete financial management package and a 98 per- cent or better collection rate of a data base that also reported age and sex distributions, morbidity patterns, service consumption, geographic distributions, family structures, charging patterns, and cohorts of patients with similar problems or characteristics. By standardizing the data collection forms and coding schemes for services and problems, information from over twenty practices in- volving some 60,000 patients could be com- bined to allow comparisons and contrasts among providers, practices and regions. Dedi- cated phone lines from each practice to a central computer in Denver allowed prac- tices 23 hours per day on-line interaction with their computer, and month-end closing assured timely reporting.
After five years of operation it is apparent that: health care providers will use computers in their offices; health care providers will share data from and about their practices when confidentiality is assured; fiscal man- agement can be enhanced with computer applications in billing; data from practices can be successfully used to affect undergraduate, graduate and continuing medical education curricula; the full capacity of computer appli- cations in the medical office is far from realized.
In summary, we now know that data sys- tems can be constructed that assist the primary care provider even in settings of relative isola- tion (e.g., communities as small as 900 people), and simultaneously provide information about early disease and gatekeeping. For example, in FMIS the most common type of headache is not tension or migraine, but headache not otherwise specified; and one of the providers using FMIS spent 4 percent of his patients’ dollar on thyroid function tests, but changed his behavior to reflect the remainder of the system once this overuse was identified.
The fundamental problems now are inte- gration and use. These problems are multi-
factorial and remain unsolved because of con- ceptual and technical limitations.
The conceptual limitations include: confu- sion about what constitutes relevant and ade- quate denominators for the numerators pour- ing out of office computers; uncertainty about how, if at all, the computer should impact directly upon the provider-patient encounter; conflict about who should define and pay for these emerging data management capabilities; confusion about the limits of the responsibili- ties assumed by providers, vendors, designers, and dreamers; lack of wisdom about which data are important; lack of creativity required to convert mere data to information; and lack of commitment to use this information to teach and practice better.
The technical limitations include: measur- ing the accuracy, reliability, and validity of practice-based data; selecting the best of com- peting taxonomies for services, diagnoses, race, geo-codes; selecting hardware with the right capacities at the right time; inadequate archiving strategies, coping with the bias asso- ciated with reimbursement incentives and disincentives; organizing practices into net- works; and rising communication costs.
Of course there are other limitations, and perhaps one or more will prove insurmount- able. Despite these limitations, however, the future of the computer in the health provider’s office appears bright. When any one use of the computer justifies its expense, the poten- tial for revolution in continuing medical edu- cation exists. The office-based computer pro- vides the opportunity to bring absolutely current knowledge to the provider-patient encounter as it occurs-not in Hawaii next March. The future does not lie in mere storage of information, however. It lies in: superb and constant editing of information, not just data, about patient management; presentation of the information that answers the practitioner’s question about the patient she or he is seeing now; presentation of new knowledge that should change the way a practitioner manages

GREEN 27
patients when that new knowledge becomes available without regard to whether or not the practitioner asks for that information.
The structure is simple. Central computers can be the library; wire, plastic and waves can be the means of distribution; and office com- puters can be the means of presentation. The right information can be taught at the right time.
Obviously, all health care providers could use such a system for continuing medical edu- cation, but the primary care provider would be especially benefited. Having rejected sub- specialization as a primary means of coping with information overload, the primary care provider could use such an information sys- tem to find and use information needed, rather than simply the information available. The same system can be used to collect informa- tion about primary care in the office setting and begin to develop new knowledge about this poorly understood area of medicine. The office computer as a partner in teaching can also offer personalized instruction. These efforts center around the provider’s question, “How am I doing?” Examples of computer audit accompanied by relevant instruction already exist. Computerized interpretation of electrocardiograms have evolved to include instruction in EKG interpretation, and not just course work via cathode ray tube. Systems, such as the Community Electrocardiographic Interpretative Service’s system in Denver, audit individual interpretors and provide feedback about interpretation style and over- sights. An interpretor who misreads a finding can be informed of his departure from peer- established criteria and simultaneously in- formed of standards, definitions and criteria.
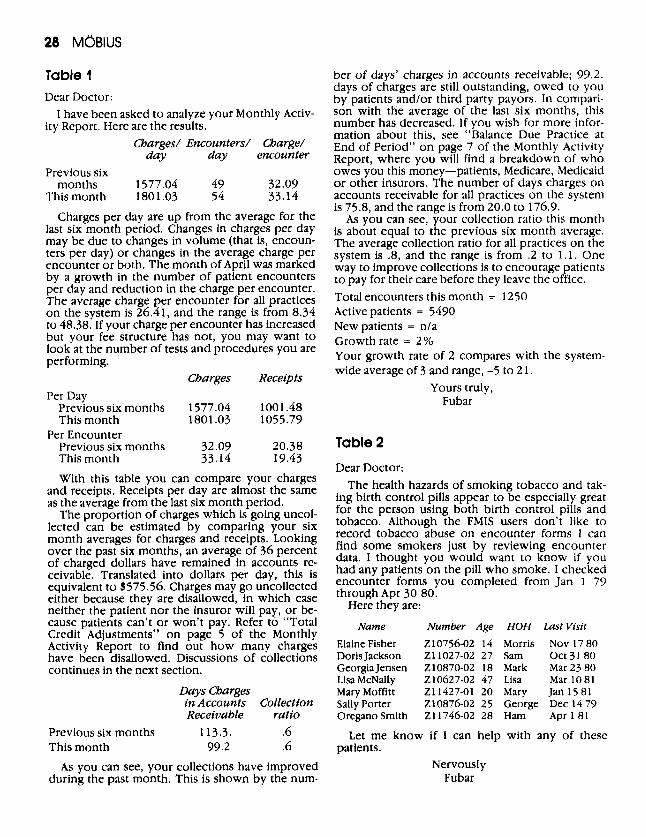
Table 1 presents a computer-generated and computer-written analysis of the financial status of one practice, including comparisons to other practices and suggestions for improve- ment. Table 2 presents a similarly prepared report concerning the interaction of two patient characteristics that, when coexistent, should
prompt specific action by the patient’s health care provider. The report takes the additional step of identifying for the provider which of hidher own patients are at risk and can even address reminder letters to these patients.
Conclusion Financial management applications of com- puters now justify for many providers the expense of owning and operating an office computer. Once available in the office, further applications are feasible, including new ap- proaches to research and continuing medical education. A system integrating registration and encounter data with educational resources is now possible and can offer personalized education conveniently and at the most im- portant time: when the provider and the pa- tient need it. 00
REFERENCESlFOOTNOTES
1. For information about FMIS and an example of its use:
Green LA, Simmons RL, Reed FM, et al: A family medi- cine information system: The beginning of a network for practicing and resident family physicians J Fam Pract 1978; 7:567. Green, LA, Reed MF, Martini C, et al: Differences in morbidity patterns among rural, urban, and teaching family practices: A one-year study of twelve Colorado family practices. J Fam Pract 1979; 9:1075.
2. For information about Dartmouth’s Cooperative In- formation Project and its use:
Nelson EC, Kirk JW, Bise BW, et al: The Cooperative Information Project: Part 2: Some initial clinical, quality assurance, and practice management studies. J Fam Pract 1981; 13:867.
3. For information about COSTAR (an office computer system that includes the entire medical record) contact Mitre Corporation in McLean, Virginia. 4. For a discussion about information overload in medi- cal practice:
Dornhorst AC: Information overload: why medical education needsashakeup. Lancet Sept 5,1981; 513.
5. For information about progress toward organizing real information for distribution to health providers’ offices via computer contact:
Dr. David Steinman Associate Professor 1180 Clermont Street Department of Family Medicine Denver, CO 80220 University of Colorado (303) 394 5191
28 MOBIUS
Table 1 Dear Doctor:
ity Report. Here are the results. I have been asked to analyze your Monthly Activ-
Charges/ Encounters/ Charge/ day day encounter
Previous six months 1577.04 49 32.09
This month 1801.03 54 33.14 Charges per day are up from the average for the
last six month period. Changes in charges per day may be due to changes in volume (that is, encoun- ters per day) or changes in the average charge per encounter or both. The month of April was marked by a growth in the number of patient encounters per day and reduction in the charge per encounter. The average charge per encounter for all practices on the system is 26.41, and the range is from 8.34 to 48.38. If your charge per encounter has increased but your fee structure has not, you may want to look at the number of tests and procedures you are performing.
Per Day Charges Receipts
Previous six months 1577.04 1001.48 This month 1801.03 1055.79
Previous six months 32.09 20.38 This month 33.14 19.43 With this table you can compare your charges
and receipts. Receipts per day are almost the same as the average from the last six month period.
The proportion of charges which is going uncol- lected can be estimated by comparing your six month averages for charges and receipts. Looking over the past six months, an average of 36 percent of charged dollars have remained in accounts re- ceivable. Translated into dollars per day, this is equivalent to $575.56, Charges may go uncollected either because they are disallowed, in which case neither the patient nor the insuror will pay, or be- cause patients can’t o r won’t pay. Refer to “Total Credit Adjustments” on page 5 of the Monthly Activity Report to find out how many charges have been disallowed. Discussions of collections continues in the next section.
Days Charges
Per Encounter
in Accounts Collection Receivable ratio
Previous six months 113.3. .6 This month 99.2 .6
As you can see, your collections have improved during the past month. This is shown by the num-
ber of days’ charges in accounts receivable; 99.2. days of charges are still outstanding, owed t o you by patients and/or third party payors. In compari- son with the average of the last six months, this number has decreased. If you wish for more infor- mation about this, see “Balance Due Practice at End of Period” on page 7 of the Monthly Activity Report, where you will find a breakdown of who owes you this money-patients, Medicare, Medicaid or other insurors. The number of days charges on accounts receivable for all practices on the system is 75.8, and the range is from 20.0 to 176.9.
As you can see, your collection ratio this month is about equal to the previous six month average. The average collection ratio for all practices on the system is 3, and the range is from .2 to 1.1. One way to improve collections is to encourage patients to pay for their care before they leave the office. Total encounters this month = 1250 Active patients = 5490 Newpatients = nla Growth rate = 2% Your growth rate of 2 compares with the system- wide average of 3 and range, -5 to 2 1 .
Yours truly, Fubar
Table 2
Dear Doctor: The health hazards of smoking tobacco and tak-
ing birth control pills appear to be especially great for the person using both birth control pills and tobacco. Although the FMIS users don’t like to record tobacco abuse on encounter forms 1 can find some smokers just by reviewing encounter data. I thought you would want to know if you had any patients on the pill who smoke. I checked encounter forms you completed from Jan 1 79 through Apr 30 80.
Here they are:
Name Number Age HOH Last Visit
Elaine Fisher 210756-02 14 Morris Nov 17 80 Doris Jackson Z11027-02 27 Sam Oct 31 80 Georgia Jensen 210870-02 18 Mark Mar 23 80 Lisa McNally 210627-02 47 Lisa Mar 10 81 Mary Moffitt 211427-01 20 Mary Jan 15 81 Sally Porter 210876-02 25 George Dec 14 79 Oregano Smith Z11746-02 28 Ham Apr 1 81
patients. Let me know if I can help with any of these
Nervously Fubar

GREEN 29
Larry A. Green, M.D. Dr. Green is director of the Family Medicine Residency at Mercy Medical Center in Denver, Colorado. He is also associate professor of Family Medicine at the Uni- versity of Colorado School of Medicine. His major re- search interests are the development of the systems and
tools required to study Family Medicine from an office- based perspective. He is currently chairman of the steer- ing COmmifteK Of the Ambulatory Sentinel PrlCtiCe Pro- ject Of North America, a network of Primary Care prac- tices scattered across the United States and Canada.
Requests for reprints: Larry A. Green, M.D., Residency Director, Mercy Medical Center, 1619 Milwaukee Street, Denver. CO 80206