Embed Size (px)
Citation preview

www.elsevier.com/locate/schres
Schizophrenia Research
The prodromal questionnaire (PQ): Preliminary validation
of a self-report screening measure for prodromal
and psychotic syndromes
Rachel L. Loewya,T, Carrie E. Beardenb, Jennifer K. Johnsonb,
Adrian Rainec, Tyrone D. Cannona,b
aDepartment of Psychology, University of California, Los Angeles, 1285 Franz Hall, Box 951563, Los Angeles, CA 90095-1563, United StatesbDepartment of Psychiatry and Biobehavioral Sciences, University of California, Los Angeles, Box 956968, Rm 2265, 300 Medical Plaza,
Los Angeles, CA 90095-6968, United StatescDepartment of Psychology, University of Southern California, S.G.M. Building, Los Angeles, CA 90089-1061, United States
Received 30 September 2004; received in revised form 2 March 2005; accepted 14 March 2005
Available online 17 May 2005
Abstract
This study aims to establish preliminary validity of the Prodromal Questionnaire (PQ), a 92-item self-report screening
measure for prodromal and psychotic symptoms. Adolescents and young adults (N =113) referred to a prodromal psychosis
research clinic completed the PQ and the Structured Interview for Prodromal Syndromes (SIPS [Miller, T.J., McGlashan, T.H.,
Woods, S.W., Stein, K., Driesen, N., Corcoran, C.M., Hoffman, R., Davidson, L., 1999. Symptom assessment in schizophrenic
prodromal states. Psychiatric Quarterly 70(4), 273–287]), an interview with established validity for predicting future psychosis.
When maximizing selection of true positive cases, scores on a subset of PQ items that assess positive symptoms predicted a
concurrent prodromal or psychotic SIPS diagnosis with 90% sensitivity and 49% specificity. The PQ shows good preliminary
validity in detecting individuals with an interview-diagnosed prodromal or psychotic syndrome, but it is less sensitive to the
threshold between prodromal and full-blown psychosis.
D 2005 Elsevier B.V. All rights reserved.
Keywords: Assessment; Prodrome; Psychosis; Schizophrenia; Screening
0920-9964/$ - see front matter D 2005 Elsevier B.V. All rights reserved.
doi:10.1016/j.schres.2005.03.007
T Corresponding author. Tel.: +1 310 794 9673; fax: +1 310 794
9740.
E-mail addresses: [email protected] (R.L. Loewy),
[email protected] (C.E. Bearden),
[email protected] (J.K. Johnson), [email protected]
(A. Raine), [email protected] (T.D. Cannon).
1. Introduction
During the past decade, over a dozen research
clinics have been established to investigate the onset,
pathophysiology, and treatment of the prodromal
phase of schizophrenia by assessing symptomatic
79 (2005) 117–125

R.L. Loewy et al. / Schizophrenia Research 79 (2005) 117–125118
individuals who may be at risk for psychosis.
However, the difficulty of participant ascertainment
has limited the ability of these clinics to produce
empirical results in a timely manner (Heinssen et al.,
2003). Where such data have been reported, approx-
imately one-third of referrals meet criteria for inter-
view-based diagnoses of high-risk status (Yung et al.,
2003).
While clinicians and researchers have long noted
the signs that appear in patients just prior to a
psychotic break, the first set of prodromal criteria
with empirical validity in predicting future psychosis
were recently developed by Yung and McGorry
(1996). Based on descriptions of the prodrome
compiled from retrospective accounts of first-episode
or remitted schizophrenia patients and their relatives,
case studies, high-risk studies, and studies of the
prodrome to psychotic relapse, researchers developed
a set of prodromal criteria that define three bat-riskQsyndromes, which have been incorporated into a semi-
structured interview, the Comprehensive Assessment
of at Risk Mental States (CAARMS; Yung et al.,
2003). These criteria were modified slightly to form
the basis of a similar interview, the Structured
Interview for Prodromal Syndromes (SIPS), along
with the Scale of Prodromal Symptoms (SOPS),
which were used in the current study (Miller et al.
2002, 1999). The syndromes refer specifically to the
blate prodrome,Q a period of illness just prior to full
psychosis (Addington, 2004; Yung et al., 1998).
Therefore, patients diagnosed with these syndromes
whose transition to psychosis would be expected to do
so quickly (i.e. within 1–2 years); initial validity data
for the two structured clinical interviews show that
approximately 40–54% of diagnosed patients’ tran-
sition to full psychosis within a year (Miller et al.,
2002; Yung et al., 2003).
While promising, the administration of these
interviews requires specific training and several
hours of clinicians’ time. In order to increase the
yield of participants within a clinic-referred sample,
we developed the Prodromal Questionnaire, a self-
report prodromal psychosis survey. The goal of this
study was to examine the preliminary psychometric
properties of the screening measure, primarily
through assessing concurrent validity with suspected
prodromal and psychotic syndrome diagnoses based
on structured clinical interview.
2. Methods
2.1. Materials
The PQ is a 92-item self-report questionnaire that
takes approximately 20 min to complete. Most items
were adapted from the Schizotypal Personality Ques-
tionnaire (Raine, 1991) and from probe questions in
the SIPS (Miller et al., 2002); some original items
were also added. The items are answered true/false
and sum to form four major subscales: 1) Positive
symptoms (e.g. unusual thinking and perceptual
abnormalities), 2) Negative symptoms (e.g. flat affect
and social isolation), 3) Disorganized symptoms (e.g.
odd behavior) and 4) General symptoms (e.g. depres-
sion and role functioning). Sample items include
bSometimes I think that people can read my mind,Qand bI tend to avoid social activities with other
people.QPresence of a bprodromal syndromeQ was diag-
nosed using the Criteria for Prodromal Syndromes
(COPS), as assessed by the SIPS. The COPS
identifies three bprodromal syndromesQ defined by:
1) Attenuated positive symptoms (APPS), 2) Brief
intermittent psychotic symptoms (BIPS) and 3)
Decline in role functioning and either a diagnosis of
schizotypal personality disorder or a first-degree
relative with psychotic disorder (Genetic Risk and
Deterioration Prodromal Syndrome, GRDPS). The
SIPS assesses for a psychotic syndrome using the
criteria defining the Presence of Psychotic Syndromes
(POPS). Diagnosis of a bpsychotic syndromeQ may
not correspond precisely to a DSM-IV psychotic
disorder diagnosis but, rather, refers to psychotic
symptoms of particular duration and intensity (Miller
et al., 2002). Interviewers also rate the same four
symptom domains assessed by the PQ on the Scale of
Prodromal Symptoms (SOPS).
2.2. Participants and assessments
Study participants were 158 individuals, aged 12–
35, who were referred to the Staglin Music Festival
Center for Assessment and Prevention of Prodromal
States (CAPPS) at UCLA because of suspected
prodromal psychotic symptoms. Participants were
referred to CAPPS from the following sources: the
UCLA NPI’s Division of Child and Adolescent

R.L. Loewy et al. / Schizophrenia Research 79 (2005) 117–125 119
Psychiatry (approximately 36% of referrals), school
counselors (28%), outpatient mental health clinicians
(27%), self-referral in response to advertisements
placed in local newspapers and newsletters at local
universities, community colleges and local chapters of
the National Alliance for the Mentally Ill (6%), or
another source, such as a current patient or person
familiar with CAPPS (3%). The majority of referrals
were made by mental health clinicians who had
previously seen a presentation from CAPPS staff that
described the Center and inclusion/exclusion criteria
for our study.
Participants referred to the CAPPS program con-
tacted the intake coordinator, who conducted a short
phone screen. The coordinator briefly described the
program and the types of qualifying symptoms, as
well as exclusion criteria (diagnoses of schizophrenia
or schizoaffective disorder, neurological disorder, IQ
less than 70, substance dependence or abuse related to
onset of symptoms). Callers were encouraged to
consider the relevance of these criteria to their case
and discuss any questions with the coordinator but
were not required to provide any information over the
phone. Callers were then offered the opportunity to
schedule an assessment. Once they arrived at CAPPS,
93% of patients completed the study procedures. For
the 7% (N =9) who were unable to complete study
procedures, this was most often due to the patient
being considered an acute danger to self or others,
and/or too disorganized to complete the interview,
leading to an inpatient hospitalization. A few cases
were deemed incapable of giving informed consent
due to the severity of symptoms at the time of
interview.
All clinical evaluations were completed by MA,
PhD, or MD level mental health specialists or by
other trained staff members with commensurate
extensive prior training in clinical interviewing. The
original CAPPS clinical interviewer team was trained
on the SIPS by Dr. Tandy Miller (Miller et al., 2003,
1999), one of the developers of the instrument.
During this training, raters completed a didactic
component followed by independently rating six
videotaped SIPS interviews. Certification requires
that interviewers achieve good to excellent reliability
(ICCs N .75 for all SOPS symptom ratings, and
kappas z .80 for prodromal syndrome diagnoses) on
SIPS training videotapes as compared with bgold
standardQ ratings developed by Dr. Miller and her
clinical team at Yale, as well as achieve this reliability
standard on three live interview cases, as compared to
ratings by experienced assessment supervisors. For
further quality assurance, members of a clinical
consensus team, which includes the Director of
Clinical Assessment (CEB) and other authors (RLL,
JKJ), independently completed SIPS ratings for the
first 12 CAPPS cases. Reliability analyses indicated
good to excellent inter-rater reliability regarding
individual symptoms (ICCsN .75), prodromal syn-
dromes (kappasz .90), and GAF scores (ICCsz .80).
.80). Any cases with diagnostic discrepancies were
brought to regular meetings of the clinical consensus
team or the Director of Clinical Assessment for
resolution. The study protocol and informed consent
procedures were approved by the UCLA Institutional
Review Board.
Participants (N =149) completed the PQ and at
least the positive symptom scale of the SIPS. Because
positive symptoms provide the basis for inclusion
diagnoses, the additional SIPS sections were not
administered to individuals who clearly did not meet
criteria for a prodromal syndrome when time was
limited. Interviews were conducted at the intake
assessment with the participant and a parent or other
informant, when available. Written informed consent
and/or child assent with parent consent was obtained
after the procedures had been fully explained.
Participants with an estimated IQ less than 70, a
neurological disorder, or serious substance use that
was temporally related to the onset of prodromal
symptoms were not included in the current analyses
(N =12). Of the remaining 113 subjects with complete
data, 37 met criteria for a present psychotic syndrome,
39 participants met criteria for a prodromal syndrome
(5 BIPS, 31 APPS, 1 GRDPS, 2 APPS and GRDPS),
and 37 did not meet criteria for either a prodromal or
psychotic syndrome as assessed by the SIPS.
Demographic characteristics of the sample are
presented in Table 1. As can be seen in the table,
the overall sample is predominantly (65%) male and
ethnically diverse. Age, gender, ethnicity, and parental
education did not differ significantly between diag-
nostic groups, although there was a trend toward
fewer males in the prodromal group, as compared to
both the psychotic group and cases who were neither
prodromal nor psychotic ( p =.06). PQ scores were not

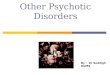
0
0.2
0.4
0.6
0.8
1
0 0.2 0.4 0.6 0.8 1
False Positive Rate (1- Specificity)
Fig. 1. ROC curve: PQ positive symptoms predicting no SIPS
diagnosis vs. prodromal/psychotic diagnoses.
Table 1
Demographic characteristics
SIPS diagnosis F or v2 p
Psychotic
(N =37)
Prodromal
(N =39)
Neither
(N =37)
Age (years) 19.3F5.3 17.3F3.8 17.6F5.0 0.63 0.19
Male 76% 51% 72% 5.6 0.06
Caucasian 41% 46% 33% 1.3 0.52
Parental
education
(years)
15.4F2.6 15.9F3.9 14.3F3.7 1.83 0.17
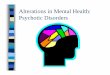
0
0.2
0.4
0.6
0.8
1
0 0.2 0.4 0.6 0.8 1
False Positive Rate (1 - Specificity)
Fig. 2. ROC curve: PQ total symptoms predicting no SIPS diagnosis
vs. prodromal/psychotic diagnoses.
R.L. Loewy et al. / Schizophrenia Research 79 (2005) 117–125120
statistically related to age (r =.06, p =.53) or parental
education (r=� .10, p= .30).
2.3. Statistical analyses
Concurrent validity of the PQ against the SIPS
was examined in several ways. First, stepwise
logistic regression analyses were performed with
PQ scales as the independent variables and SIPS
diagnosis as the dependent variable, dichotomized
first as no SIPS diagnosis versus prodromal/psychotic
SIPS diagnoses, and then classified as no SIPS
diagnosis/prodromal versus psychotic syndrome SIPS
diagnosis. Next, receiver operating characteristic
(ROC) analyses were used to assess the accuracy of
the PQ against the SIPS. ROC curves plot the true
positive rate against the false positive rate for the
different possible cutpoints of a test, showing the
tradeoff between sensitivity and specificity (any
increase in sensitivity will be accompanied by a
decrease in specificity). The closer the curve follows
the left-hand border and then the top border of the
ROC space, the more accurate the test, while the
closer the curve comes to the 458 diagonal of the
ROC space, the less accurate the test. Test accuracy
is considered statistically significant when the con-
fidence interval for the area under the curve (AUC) is
greater than .50, indicating that the test predicts
diagnosis better than chance (Zweig and Campbell,
1993). Correlations of PQ scale scores with SOPS
scale scores also examined agreement between the
measures. Internal consistency of the PQ subscales
was measured using Cronbach’s alpha statistic.
Statistical analyses were performed using SAS
version 8.2 (SAS, 1999) and MedCalc for Windows,
version 7.4.1.0 (Medcalc, 2005).
3. Results
Stepwise logistic regression analysis with PQ
subscale scores as independent variables and SIPS
diagnosis as the dependent variable revealed a
significant effect of total PQ score on diagnosis for
prodromal/psychotic syndrome versus no SIPS diag-
nosis (v2=25.6, df =1, p b .0001). Positive symptom
score also significantly predicted SIPS diagnostic
status by logistic regression (v2 = 27.4, df = 1,
p b .0001; positive symptoms b =.14, p =.002). How-
ever, the other individual PQ subscale scores did not

Table 2
SIPS diagnostic classification accuracy by PQ scores
PQ score cutoff Sensitivity Specificity PPVa (%) NPVa (%) Positive LRa
Value (%) 95% CI Value (%) 95% CI
Outcome classification: SIPS diagnosis of prodromal/psychotic versus neither
PQ positive symptomsb z8 90 80–95 49 32–66 78 69 1.74
PQ positive symptomsc z14 71 60–81 81 65–92 89 58 3.76
PQ total symptomsb z19 91 82–96 38 23–55 75 67 1.5
PQ total symptomsc z36 70 58–80 84 68–94 90 57 4.3
Outcome classification: SIPS diagnosis of psychotic versus prodromal/neither
PQ positive symptomsc z17 68 50–82 63 51–74 47 80 1.83
PQ positive symptomsb z26 35 20–52 90 80–95 62 74 3.34
PQ total symptomsc z36 76 59–88 60 47–70 48 83 1.86
PQ total symptomsb z59 27 14–44 90 82–96 50 70 2.05
a PPV=positive predicative value, NPV=negative predictive value, LR=likelihood ratio.b PQ cutoff values chosen to result in 90% correct classification of SIPS prodromal cases.c PQ cutoff values at point that maximizes overall accuracy.
R.L. Loewy et al. / Schizophrenia Research 79 (2005) 117–125 121
significantly predict SIPS-based prodromal status
(negative symptoms b = .09, p = .21; disorganized
symptoms b =� .11, p =.36; general/affective symp-
toms b =� .02, p =.77).
Receiver operating characteristic (ROC) curves
were plotted for PQ positive symptom items to predict
no SIPS diagnosis versus SIPS prodromal/psychotic
syndrome diagnoses. The area under the curve was
significant for positive symptom score (See Fig. 1,
AUC=.79, SE= .042, 95% CI= .699–.857) and total
score (See Fig. 2, AUC= .77, SE= .044, 95%
CI= .685–.847). For use as a screening measure, PQ
prediction thresholds (8 or more positive symptom
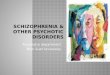
0
0.2
0.4
0.6
0.8
1
0 0.2 0.4 0.6 0.8 1
False Positive Rate (1 - Specificity)
Fig. 3. ROC curve: PQ positive symptoms predicting no SIPS
diagnosis/prodromal vs. psychotic diagnosis.
items) were set to achieve 90% sensitivity, resulting in
49% specificity and good overall classification accu-
racy. Alternatively, a cutoff score (14 or more positive
symptom items) can be selected to balance sensitivity
(71%) and specificity (81%). Table 2 shows further
details of these analyses. The PQ was less sensitive to
the distinction between prodromal and psychotic
syndrome diagnoses. When assessing PQ classifica-
tion accuracy of SIPS psychotic syndrome diagnoses
versus prodromal/no SIPS diagnosis, the area under
the ROC curve (see Fig. 3) was significant for positive
symptom score (AUC=.67, SE= .056, 95% CI= .573–
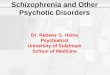
0
0.2
0.4
0.6
0.8
1
0 0.2 0.4 0.6 0.8 1False positive rate (1 - Specificity)
Fig. 4. ROC curve: PQ total symptoms predicting no SIPS
diagnosis/prodromal vs. psychotic diagnosis.

R.L. Loewy et al. / Schizophrenia Research 79 (2005) 117–125122
.753) and total score (See Fig. 4, AUC= .64,
SE= .057, 95% CI= .546–.729). Although statistically
significant, the classification accuracy was substan-
tially lower than that for PQ score prediction of no
SIPS diagnosis versus prodromal/psychotic syndrome
diagnoses and would be less than adequate in practice,
as outlined in the bottom portion of Table 2.
PQ subscales were moderately correlated with
corresponding SIPS scales for positive symptoms
(r(102)= .60, p b .0001), negative symptoms (r(57)=
.53, p b .0001), general symptoms (r(54) = .49,
p =.0001) and for the total scales (r(53)= .49, p=
.0002), with a low correlation for disorganized
symptoms (r(55)= .27, p =.039). Cronbach’s alpha
was .92 for positive symptoms (45 items), .88 for
negative symptoms, (19 items), .79 for disorganized
symptoms (13 items), .85 for general symptoms (15
items), and .96 for the total scale (92 items).
4. Discussion
The concurrent validity data indicate that the PQ
can distinguish participants with prodromal/psy-
chotic-syndrome SIPS diagnoses from those with no
SIPS diagnosis. As expected, given that SIPS
diagnoses are primarily defined by positive symp-
toms, the PQ positive symptom subscale showed the
greatest association with SIPS diagnosis. For use as a
screening instrument, we chose to maximize sensi-
tivity when differentiating prodromal/psychotic cases
from those with no SIPS diagnosis, thereby lowering
the rate of rejected true prodromal/psychotic cases.
Thus, the PQ would correctly reject approximately 5
out of 10 non-prodromal/non-psychotic participants
(i.e., a 50% reduction in time and resources spent
interviewing SIPS-negative referrals), at the cost of
excluding approximately one out of ten actual
prodromal/psychotic cases. Of note, approximately
one-third of patients referred to our clinic for
screening were found to be experiencing fully
psychotic syndromes, suggesting that referring clini-
cians may be unaware of the presence or severity of
psychotic symptoms in some patients they are
treating. Therefore, the PQ may be useful in
identifying young people who may otherwise go
undetected and, therefore, untreated for their psy-
chotic illness.
Differentiating psychotic participants from prodro-
mal subjects using the PQ resulted in less than
adequate classification accuracy. These results are
consistent with our expectation that a simple true–
false self-report screening measure would not be
sensitive to the threshold between the late prodromal
stage and full-blown psychosis. The detailed diag-
nostic definitions of psychosis provided by the SIPS
are based on the severity, frequency and duration of
symptoms, dimensions that cannot be efficiently
assessed with a brief screen and, thus, are not assessed
by the PQ.
Most PQ scales showed moderate correlations with
the corresponding SIPS scales, also supporting con-
current validity. The disorganized scale showed only a
modest correlation, likely because many disorganized
symptoms on the SIPS (e.g., odd behavior) are rated
by observation, while the PQ is based exclusively on
self-report. Internal consistency of the PQ scales was
high.
Currently, we propose that the PQ be used only for
the purpose of screening in clinical high-risk and early
psychosis research clinics and not outside of mental
health settings for the following reasons. First, the
concurrent validity statistics presented in this paper
were based on an benrichedQ sample with a very high
base rate of the target syndrome. Sensitivity would be
much weaker in samples with low base rates of true
prodromal/psychotic cases (O’Toole, 2000). Second,
the PQ does not specifically assess distress or treat-
ment-seeking behavior related to prodromal symp-
toms, although these factors are integral to the
prodrome construct. Rather, we expect to use the
screen in settings where individuals present for
treatment due to distressing symptoms that they or
their mental health clinician suspect may represent the
psychosis prodrome. All participants in this study
were treatment-seeking to some degree, whether they
wished to obtain assessment, psychotherapy, psychi-
atric services, or bsecond opinionsQ regarding psychi-
atric diagnoses, and most were already receiving
mental health services.
We emphasize distress and treatment-seeking in
defining psychotic and prodromal syndromes because
several recent studies have shown that psychotic
experiences commonly occur in the general popula-
tion outside of a diagnosable psychotic disorder. In an
unselected general population sample, 18.1% of adults

R.L. Loewy et al. / Schizophrenia Research 79 (2005) 117–125 123
reported some type of psychotic experience in their
lifetime that was not characterized by distress or
treatment-seeking, while only 1.5% of the sample was
diagnosed with psychotic disorder (Hanssen et al.,
2003). In another investigation, high school students
reported unusual psychotic-like experiences at rates
far beyond the prevalence of psychotic-spectrum
disorders (McGorry et al., 1995). Recently, we found
that when a large sample of undergraduate college
students completed the PQ, 43% of the sample scored
above the cutoff suggested in the present paper (8 or
more positive symptom items), although only 2%
rated at least 8 items as distressing, and a negligible
proportion of the sample reported previously seeking
mental health services (Loewy et al., in preparation).
These studies underscore the importance of distin-
guishing between unusual experiences and true
symptoms or disorder, which must be complemented
by distress and/or an effect on role functioning. A
version of the PQ modified to assess level of distress
and treatment seeking is currently under development
to investigate the possibility of wider screening in
non-clinical settings, such as schools and general
medical facilities.
The PQ is not diagnostic but, rather, is intended
for use as a tool to pre-select patients for more
intensive interviewing. We suggest a careful
approach when screening young people for prodro-
mal psychosis to minimize unnecessary stigma,
confusion, anxiety, and potential treatment with
antipsychotic medications (Peterson, 2000; Post,
2001; Rosen, 2000; Yung and McGorry, 1997).
Informing patients, their families and their clinicians
of the nature of their risk status in a clear and
understandable manner ensures that they receive
accurate information without undue alarm. All
parties should be informed that this screening
measure is not diagnostic and that it has a margin
of error. They can be encouraged to return for further
assessment if there is any future change in symptoms
and/or functioning, and they can be provided with a
description of psychotic symptoms to help track
potential worsening of symptoms. It is possible that
some apparently false negative cases on the PQ are
defined as bprodromalQ on the SIPS but will not
actually become fully psychotic. For included
patients (i.e., SIPS positive cases), the SIPS and
PQ are administered at multiple follow-up time
points, which will allow us to examine this question
in future analyses.
One limitation of the PQ is that all the items are
keyed in the btrueQ direction, thereby subjecting scoresto the effects of response bias, or the tendency to
respond in one direction. Response bias can be
influenced by personality factors such as agreeable-
ness, social desirability, demand characteristics of the
research environment, or cognitive processes engaged
when completing the questionnaire (Krosnick, 1999;
Peltier and Walsh, 1990). However, positive symptom
items on the PQ were constructed to describe specific
experiences of prodromal symptoms that are not
easily phrased in the negative direction, such as bIsometimes feel that things I see on television or read
in the newspaper have a special meaning for me.Q Inthat case, positively keyed items increase validity
because respondents are more likely to understand the
item accurately than when it is phrased in a negative
direction (Schrieshem and Hill, 1981). Therefore, a
positively keyed questionnaire seemed the best
approach to facilitate accurate responses.
Participants who were classified as neither pro-
dromal nor psychotic often reported symptoms con-
sistent with the negative and affective symptoms that
characterize the prodromal phase of psychosis, with-
out the positive symptoms sufficient to warrant a
prodromal or psychotic diagnosis according to the
COPS/POPS. However, the only diagnostic instru-
ment administered at intake was the SIPS. Because
the SIPS is a highly detailed, time-intensive interview
measure, staff costs and patient burden precluded the
completion of an additional clinical interview (e.g.,
SCID) with subjects already known to be ineligible
for the larger CAPPS study. Therefore, we are unable
to provide DSM-IV diagnoses for these excluded
subjects. Of the 39 patients diagnosed as putatively
prodromal at intake, 33 have agreed to follow-up
assessment within our clinic and 6 of these patients
have been followed for a full 2 years. Consequently,
we are not yet able to provide an accurate estimate of
the psychosis transition rate within our sample.
However, we expect to examine the predictive
validity of the PQ once a greater number of patients
in our sample have been followed for a sufficient
period of time.
Evaluation of sample characteristics is crucial in
determining the utility of a clinical measure such as

R.L. Loewy et al. / Schizophrenia Research 79 (2005) 117–125124
the PQ. Patients with attenuated prodromal syn-
dromes represent the largest portion of the validation
samples for the SIPS (Miller et al., 2003), the
CAARMS (Yung et al., 2003), and the present study
(85%), and may represent the prodromal patients
most likely to seek treatment (Davidson and Weiser,
2004). Therefore, the validity of the PQ as assessed
in this study refers largely to accurate identification
of attenuated prodromal syndromes. Definitions of
the prodrome are likely to change with time as
researchers refine the symptom criteria and identify
additional factors that predict psychosis (Knowles
and Sharma, 2004; Lencz et al., 2004; Yung et al.,
2004). As such, future versions of the PQ may
reflect those changes once their predictive power is
established. For now, the definition of the schizo-
phrenia prodrome used in the present study repre-
sents the best current attempts in the field to define
at-risk syndromes.
According to these preliminary results, the PQ
shows promise as a simple and cost-effective way to
screen for prodromal and previously undiagnosed
psychotic symptoms in clinic-referred populations.
While the PQ shows good agreement with concurrent
diagnoses of putatively bprodromalQ or psychotic
syndromes, its predictive validity has not yet been
investigated. The present findings indicate that further
validation studies of the PQ are warranted, and
therefore, data collection for the current study is
ongoing and expanding. These additional data will
allow us to accrue a larger validation sample size
adequate for factor analyses and item analyses. We
intend to use the results of these analyses to reduce the
number of items on the PQ in order to improve
efficiency of administration.
References
Addington, J., 2004. The diagnosis and assessment of individuals
prodromal for schizophrenic psychosis. CNS Spectr. 9 (8),
588–594.
Davidson, M., Weiser, M., 2004. Prodromal schizophrenia: the
dilemma of prediction and early intervention. CNS Spectr. 9 (8),
578.
Hanssen, M., Peeters, F., Krabbendam, L., Radstake, S., Verdoux,
H., van Os, J., 2003. How psychotic are individuals with non-
psychotic disorders? Soc. Psychiatry Psychiatr. Epidemiol. 38
(3), 149–154.
Heinssen, R.K., Cuthbert, B.N., Breiling, J., Colpe, L.J., Dolan-
Sewell, R., 2003. Overcoming barriers to research in early
serious mental illness: issues for future collaboration. Schizophr.
Bull. 29 (4), 737–745.
Knowles, L., Sharma, T., 2004. Identifying vulnerability markers in
prodromal patients: a step in the right direction for schizophre-
nia prevention. CNS Spectr. 9 (8), 595–602.
Krosnick, J.A., 1999. Survey research. Annu. Rev. Psychol. 50,
537–567.
Lencz, T., Smith, C., Auther, A., Correll, C., Cornblatt, B., 2004.
Nonspecific and attenuated negative symptoms in patients at
clinical high-risk for schizophrenia. Schizophr. Res. 68 (1),
37–48.
Loewy, R.L., Riese, S.R., Johnson, J.K., and Cannon, T.D., in
preparation. How unusual are unusual experiences? Self-report
of attenuated psychotic symptoms in a college population.
Manuscript submitted for publication.
McGorry, P.D., McFarlane, C., Patton, G.C., Bell, R., Hibbert,
M.E., Jackson, H.J., Bowes, G., 1995. The prevalence of
prodromal features of schizophrenia in adolescence: a prelimi-
nary survey. Acta Psychiatr. Scand. 92 (4), 241–249.
Miller, T.J., McGlashan, T.H., Woods, S.W., Stein, K., Driesen, N.,
Corcoran, C.M., Hoffman, R., Davidson, L., 1999. Symptom
assessment in schizophrenic prodromal states. Psychiatr. Q. 70
(4), 273–287.
Miller, T.J., McGlashan, T.H., Rosen, J.L., Somjee, L., Markovich,
P.J., Stein, K., Woods, S.W., 2002. Prospective diagnosis of the
initial prodrome for schizophrenia based on the Structured
Interview for Prodromal Syndromes: preliminary evidence of
interrater reliability and predictive validity. Am. J. Psychiatry
159 (5), 863–865.
Miller, T.J., McGlashan, T.H., Rosen, J.L., Cadenhead, K.,
Ventura, J., McFarlane, W., Perkins, D.O., Pearlson, G.D.,
Woods, S.W., 2003. Prodromal assessment with the
Structured Interview for Prodromal Syndromes and the
Scale of Prodromal Symptoms: predictive validity, interrater
reliability, and training to reliability. Schizophr. Bull. 29 (4),
703–715.
O’Toole, B.I., 2000. Screening for low prevalence disorders. Aust.
N. Z. J. Psychiatry 34, S39–S46 (Suppl.).
Peltier, B.D., Walsh, J.A., 1990. An investigation of response bias in
the Chapman Scales. Educational and Psychological Measure-
ment 50 (4), 803–815.
Peterson, D.R., 2000. The ethics of research into schizophrenia
prevention: a carer’s perspective. Aust. N. Z. J. Psychiatry 34,
S201–S203 (Suppl.).
Post, S.G., 2001. Preventing schizophrenia and Alzheimer disease:
comparative ethics. Schizophr. Res. 51 (1), 103–108.
Raine, A., 1991. The SPQ: a scale for the assessment of schizotypal
personality based on DSM-III-R criteria. Schizophr. Bull. 17 (4),
555–564.
Rosen, A., 2000. Ethics of early prevention in schizophrenia. Aust.
N. Z. J. Psychiatry 34, S208–S212 (Suppl.).
SAS Version 8.2 [Computer Software], 1999. SAS Institute Inc.,
Cary, NC.
Schoonjans, F., 2005. MedCalc (version 7.4.1.0) [Computer
Software]. MedCalc Software, Mariakerke, Belgium.

R.L. Loewy et al. / Schizophrenia Research 79 (2005) 117–125 125
Schrieshem, C.A., Hill, K.D., 1981. Controlling acquiescence
response bias by item reversals: the effect on questionnaire
validity. Educ. Psychol. Meas. 41, 1101–1114.
Yung, A.R., McGorry, P.D., 1996. The prodromal phase of first-
episode psychosis: past and current conceptualizations. Schiz-
ophr. Bull. 22 (2), 353–370.
Yung, A.R., McGorry, P.D., 1997. Is pre-psychotic intervention
realistic in schizophrenia and related disorders? Aust. N. Z. J.
Psychiatry 31 (6), 799–805.
Yung, A.R., Phillips, L.J., McGorry, P.D., McFarlane, C.A.,
Francey, S., Harrigan, S., Patton, G.C., Jackson, H.J., 1998.
Prediction of psychosis. A step towards indicated prevention of
schizophrenia. Br. J. Psychiatry 172 (33), 14–20 (Suppl.).
Yung, A.R., Phillips, L.J., Yuen, H.P., Francey, S.M., McFarlane,
C.A., Hallgren, M., McGorry, P.D., 2003. Psychosis prediction:
12-month follow up of a high-risk (bprodromalQ) group.
Schizophr. Res. 60 (1), 21–32.
Yung, A.R., Phillips, L.J., Yuen, H.P., McGorry, P.D., 2004. Risk
factors for psychosis in an ultra high-risk group: psychopathol-
ogy and clinical features. Schizophr. Res. 67 (2–3), 131–142.
Zweig, M.H., Campbell, G., 1993. Receiver-operating characteristic
(ROC) plots: a fundamental evaluation tool in clinical medicine.
Clin. Chem. 39 (4), 561–577.