Embed Size (px)
Citation preview

c o m p u t e r m e t h o d s a n d p r o g r a m s i n b i o m e d i c i n e 9 2 ( 2 0 0 8 ) 249–256
journa l homepage: www. int l .e lsev ierhea l th .com/ journa ls /cmpb
The reconstruction and application of virtual Chinesehuman female
Yuan Yuan, Lina Qi, Shuqian Luo ∗
College of Biomedical Engineering, Capital Medical University,100069 Beijing, PR China
a r t i c l e i n f o
Article history:
Received 27 November 2007
Received in revised form 7 May 2008
Accepted 23 May 2008
Keywords:
Virtual Chinese human female
number 1
Reconstruction
a b s t r a c t
The virtual human is an interactive computer model integrating anatomical, biophysi-
cal, physiological and biomechanical characteristics of human being. The virtual Chinese
human female number 1 (VCH-F1) is a high-resolution dataset of a standard Chinese female.
This paper covers our 5-year work with VCH-F1 dataset. We will introduce the reconstruc-
tion of VCH-F1 three-dimensional (3D) model and our efforts to put this dataset into practical
task such as the construction of the health sciences educational facilities, the research about
the mechanism of acupuncture and the realization of virtual image-guided neurosurgery.
Our experience with this work demonstrates a broad scope and variety of applications of
VCH-F1 dataset in medicine and biology. Further works still need to be done to make this
VCH clinic
Virtual acupuncture
I
dataset a routine clinical tool.
© 2008 Elsevier Ireland Ltd. All rights reserved.
1
Ticaohhggtpcgu
P
Chinese human female number 1 (VCH-F1) [7]. The total sec-tions amount to 8556 and the slice thickness is 0.2 mm. The
0d
mage-guided neurosurgery
. Introduction
he Virtual human is an interactive computer model integrat-ng anatomical, biophysical, physiological and biomechanicalharacteristics of human being. The information could benatomical, physical and functional depending on the devel-pment of the dataset [1]. The evolutionary stages of virtualuman could be classified into three generations: visibleuman, physical human and physiological human. The firsteneration aims at the visualization of three-dimensional (3D)eometric anatomical structures while the other two are withhe purpose of the analysis and simulation of the physicalroperties as well as physiologic characteristics. Each suc-eeding generation is more complex, integrating the preceding
eneration and following a chronological development basedpon technical limitations of the time [2].∗ Corresponding author at: College of Biomedical Engineering, Capital MR China. Tel.: +86 10 83911566.
E-mail addresses: [email protected] (Y. Yuan), [email protected]/$ – see front matter © 2008 Elsevier Ireland Ltd. All rights resoi:10.1016/j.cmpb.2008.05.011
The National Library of Medicine (NLM) in the USA estab-lished the Visible Human Project (VHP) in 1994 [3]. In 1994and 1995, Health Science Center of the University of Coloradoestablished the first male and female dataset [4]. In March2001, Ajou University in Korea and Korea Institute of Scienceand Technology Information established Visible Korea Human(VKH) [5]. China has the largest population in the world,which urges the establishment of virtual human databasebearing the specific features of the Chinese people. The project“Digitalized Virtual Chinese Human” started in 2001 and inFebruary 2003, the dataset of one female was established inSouthern Medical University with the catalog number virtual
edical University, No. 10 Xitoutiao, You An Men, 100069 Beijing,
org (S. Luo).
dataset was then sent to our laboratory (Medical Image Labo-ratory, MIL) in Capital Medical University for further process.
erved.

s i n
250 c o m p u t e r m e t h o d s a n d p r o g r a mChinese visible human (CVH) is another project started by theThird Military Medical University at the same time as oursin 2001. In 2002, the first CVH-male database was establishedwith 2518 total sections and varied thicknesses of 1.0 mm,0.5 mm and 0.1 mm [6].
A great deal of work has been attempted by the researchersall over the world to serve visible human datasets in educa-tionally and clinically useful ways. Internationally, Universityof Colorado’s Health Sciences Center built Center for HumanSimulation, a website to offer viewing sample images, prod-ucts and browser about VHP [8]. In Germany, UniversityMedical Center Hamburg-Eppendorf established the VoxelMan, a high-resolution 3D volume-based anatomic datasetwith broad extension such as surgery simulators and virtualbody models delivered from visible human male [9]. The MayoClinic’s Virtual Reality Assisted Surgery Program and Biomed-ical Imaging Resource also used the visible human datasetin their research about VR technology in medicine [10]. E.Y.S.Chao from Orthopedic Biomechanics Laboratory in Johns Hop-kins University also made use of visible human dataset tofacilitate his biomechanical analyses [11]. In China, the ThirdMilitary Medical University established the Chinese visiblehuman project dedicated in data acquisition and visualiza-tion, and merits special distinction. So far, they have reportedfive human datasets [12].
There are so many technical and clinical groups workingin virtual human project, and a great deal of excellent workhas been done. The work of VCH-F1 has the following char-acteristics. By comparison with the widely used VHP femaledataset, the VCH-F1 specimen’s body shape was normal andcan represent the Chinese population while the VHP female’suterus and ovaries were atrophied because of old age. Thenormal anatomical model is of great significance for our fur-ther research. We have worked on image segmentation andreconstruction based on the VCH-F1 dataset for nearly 5 years.Until now, 184 structures of the human body were segmentedand 3D reconstructed. In China, our work is one of the mostcomprehensive works in this area.
This paper is the extended version of the MIMI 2007 Con-ference oral presentation titled Preliminary Application of theFirst Digital Chinese Human. Since then, we did some fur-ther researches. Based on our previous works, VCH clinic, aneducational facility in medical sciences was implemented.The VCH clinic includes the anatomical atlas module, themotion simulation module, the virtual endoscopy module as
well as the games and exam module. We did more researchon image-guided neurosurgery as well. User-friendly interfacewas designed to help the doctors get the location and structureof the focus better.Table 1 – Main parameters of VCH-F1 dataset
Items Photo sections
Sections 8556Section thickness 0.2 mmResolution 3024 × 2016Data size 149.2 GBInstrument Fuji Fine Pix S2 Pro
b i o m e d i c i n e 9 2 ( 2 0 0 8 ) 249–256
In this paper, we will introduce the reconstruction ofVCH-F1 3D model and our efforts to put this dataset intopractical task such as the construction of the health scienceseducational facilities, the research about the mechanismof acupuncture and the realization of image-guided neuro-surgery. Section 2 focuses on the reconstruction of the VCH-F13D model. Section 3 describes the application of VCH-F1dataset to various areas. Section 4 makes concluding remarksand discusses the potential future work by using our researchresult.
2. Reconstruction of VCH-F1
A correct and detailed anatomical model is the basis ofsophisticated simulation of any operation. Highly realisticvisualization of large dataset is a great challenge in the recon-struction of VCH-F1. Pre-processing on this data, includingimage registration, background removal and image segmen-tation, is necessary for 3D modeling. The properly preparedand normalized dataset proved to be effective and efficientin the recent modeling and is expected to be so in the futureresearch.
2.1. Raw data
The VCH-F1 dataset contained digital photographs ofanatomic sections, CT images and MR images. The specimenwas a 19-year-old female who died of food poisoning. Thecadaver was first CT and MR scanned. It was then frozen at−70 ◦C and cryomacrotomed into 8556 slices with the thick-ness of 0.2 mm. Every slice was captured with digital camera.The process took 3 months in total, and the total datasetamounted to 149.7 GB [7]. Table 1 demonstrates the mainparameters of VCH-F1 dataset. The following works describedare based on the digital photo sections.
2.2. Background removal
The RGB cross-sectional images with high color contrastbetween the human body and the surrounding blue embed-ding agency allowed us to remove the background easily. Withthe simple operation of the three-color components R + G − B,the background removal was accomplished.
2.3. Data reduction
For the ease of handling, the bmp format anatomic sections ofVCH-F1 were reformatted to jpeg (optimised Huffman codes).
CT MRI
1718 8011 mm 2 mm512 × 512 512 × 512429.5 MB 200.5 MBSOMATOM PLUS 4 MAGNETOM Vision Plus 1.5 T

c o m p u t e r m e t h o d s a n d p r o g r a m s i n b i o m e d i c i n e 9 2 ( 2 0 0 8 ) 249–256 251
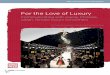
Fig. 1 – VisChinese is an image browser of the normalized dataset. The upper left axial view is the normalized data. Theu derep
Ww50ndassa
2
Rcwdtmtuaatmlpt
sns
pper right coronal view and lower left sagittal view are renicture is from the CT data of VCH-F1.
e decided to restrict the resolution of 2400 × 1600 pixels2,hich provided not only a reduction of the data to
.44 GB, but also normalized the size of each voxel to
.2 cm × 0.2 cm × 0.2 cm. Before 3D reconstruction, the dataeeded to be reduced again to 480 × 320 pixels2. Though someetailed color information was lost by the compression. Aftercomparison of the segmentation results with the recon-
tructed 3D models between the reduced and unreducedource data within local areas, we found such a loss did notffect the results.
.4. Image registration
egistration was desired to bring all images into spatial syn-hrony before 3D reconstruction. Before the VCH-F1 specimenas frozen, four fiducial markers were located in the embed-ing agency to facilitate image registration. Considering thathe mismatch between slices was mainly caused by the slight
ovement of camera during the 3-month data acquisition andhe computing expense to align the 8556 slices, we decided tose a method based on rigid transform, shortest distance, andffine transform. We designed a semi-automatic registrationpproach to align the sequential images with the followinghree steps. Step 1: use rigid transform and shortest distance
ethod to do coarse registration. Step 2: smooth the markines with a low-pass filter. Step 3: use affine transform to dorecise registration. Powell method was used as an optimiza-ion algorithm [13].
All the steps above supplied us with a normalized datasetuitable for 3D visualization. An image browser named VisChi-ese contained the normalized digital photo sections andome relative data was produced in our lab as shown in Fig. 1.
d from the normalized data real-time. The lower right
2.5. Image segmentation
Segmentation was an essential step to achieve accurate3D model. In our work, the methods to distinguish indi-vidual organs from one another varied with the practicaltask. For the structures with clear and high contrast bound-ary, for example, the bone, the skin and the perfusedblood vessels, we realized automated segmentation withregion growing method. Inner organs such as liver andstomach could be segmented semi-automatically. However,because of the complexity of the anatomical structure of thehuman body, in most cases, we had to go back to manualsegmentation.
To achieve such large amount of segmentation, we groupedthe main organs and structures of the whole body into 11smaller projects listed in Table 2. The whole work was dis-tributed to the students who had finished their anatomicalclasses and was done under the direction of anatomists inCapital Medical University.
2.6. Three-dimensional visualization
In 3D reconstruction, besides traditional surface and volumerendering methods, we used inverted cast-ray method to scanvolume data space. The difference from traditional volumerendering was that in this method, the rays stopped at the firstencountered object, and methods discussed in our publishedpaper [13] was used to render the point at the segmented bor-
derline. This method made the high-resolution visualizationof distinct surfaces possible.The surface rendering was accomplished with march-ing cubes method programmed with visualization tool kit

252 c o m p u t e r m e t h o d s a n d p r o g r a m s i n b i o m e d i c i n e 9 2 ( 2 0 0 8 ) 249–256
Table 2 – Reconstructed anatomical structures of VCH-F1
Anatomical structures Components
SkinBones Skull, sternum, spine, ribs, clavicles, scapulas, humeri, radiuses, ulnas, palm bones, hip bones, femurs,
patellae, fibulas, tibias and feetMuscles Temporalis, semispinalis capitis, splenius capitis, sternocleidomastoid, orbicularis oculi, orbicularis oris,
masseter, levator labil superioris, latissmus dorsi, rhomboideus, teres major/minor, obliquus internusabdominis, obliquus externus abdominis, rectus abdominis, superaspinatus, infraspinatus, subscapularis,serratus anterior, erector spinae, trapezius, pectoralis major/minor, psoas major, biceps brachii, brachialis,triceps brachii, coracobrachialis, deltoid, branchioradialis, flexor carpi ulnaris, flexor pollicis longus, extensorcarpi radialis longus and brevis, flexor carpi radialis, extensor digiti minimi, pronator teres, flexor digitorumsuperficialis/profundus, extensor digitorum, anconeus, dorsal interossei, flexor pollicis brevis, abductorpollicis brevis, adductor pollicis, semitendinosus, semimembranosus, adductor longus, adductor magnus,sartorius, gracilis, quadriceps femoris, gluteus maximus, soleus, gastrocnemius, peroneus longus, flexorhallucis longus, tibialis posterior/anterior, extensor digitorum longus and extensor hallucis longus
Brain Cerebrum, cerebellum, brain stem, lateral ventricle, caudate nucleus and lentiform nucleusHeart Pericardium and ventricles
SpleenUrinary system Kidneys and urinary bladderRespiratory system Lungs, trachea and principal bronchiDigestive system Esophagus, stomach, liver, gallbladder, pancreas and intestine
lusomin
in, he
Reproductive system Uterus, ovaries, oviducts and follicuArteries and veins Ascending aorta, thoracic aorta, abd
cava, inferior vena cava, femoral ve
(VTK). To improve the realistic effect without much com-putational expense, texture mapping was applied to themodel in software Maya 6.5. Fig. 2 shows some 3D visu-
alization results. So far, almost all the main anatomicalstructures of the whole body have been segmented and recon-structed. Table 2 lists all the structure contained in our VCH-F13D model.Fig. 2 – Reconstruction of the main anatomical structures of VCHsimplified Hall model, (c) the surface model of organs, (d) the sur
al aorta, renal artery, femoral artery, obturator artery, superior venapatic veins and renal veins
3. Applications
3.1. VCH clinic
Traditionally, knowledge about the human body is repre-sented in books and atlases. Since 1990s, high IT technology
-F1. (a) The result with Lambert model, (b) the result withface model of muscles and (e) the surface model of skeleton.

c o m p u t e r m e t h o d s a n d p r o g r a m s i n b i o m e d i c i n e 9 2 ( 2 0 0 8 ) 249–256 253
Fig. 3 – Interfaces of VCH clinic. (a) The normal display of the brain with introduction given on the board, (b) the detailedd bilint aw p
dccpmoFtacm
dmemv
3Abstpitvpi
3Vsaat
isplay of the brain with the name of the substructure givenhe inner structure, (d) the virtual exam game, (e) the 3D jigs
evelopment has allowed more powerful and versatileomputer-based representations of knowledge [10]. Besidesommon health information and knowledge, the use of com-uter technology may provide an alternative instructionalode for health science teaching and learning. With the help
f this atlas, students may obtain knowledge more efficiently.urther more, immersion into a virtual environment facilitateshe exploration of a scene of 3D medical objects or tomogramsnd the examination of pathological regions. Thus, physiciansan recognize topological coherencies in a much faster andore natural way [14].A Health Science Education Software, VCH Clinic, was
esigned based on the model of VCH-F1. It was accomplishedainly with the software Virtools Dev 3.0, a development
ngine for 3D visualization and interactivity [15]. Three mainodules were included in our VCH Clinic: 3D anatomy atlas,
irtual endoscopy, and the motion simulation.
.1.1. Three-dimensional anatomy atlas3D anatomy atlas based on virtual reality technology has
een basically developed in our lab. In this atlas, the anatomictructure of a whole body was shown. The model could beransformed, rotated, zoomed in, zoomed out or made trans-arent depending on the user’s need. Related knowledge and
nformation were also involved in this atlas, such as 2D pic-ures, movies and text introductions. Two little games, theirtual examination and jigsaw puzzle of skeleton were alsorovided to boost the students’ curiosity and interest in learn-
ng (Fig. 3(a)–(e)).
.1.2. Virtual endoscopyirtual endoscopy (VE) describes a new method of diagno-
is, using computer processing of 3D image datasets (suchs those from CT or MRI scans) to provide simulated visu-lizations of patient-specific organs similar or equivalent tohose produced by standard endoscopic procedures [2]. Con-gually, (c) the outer structure made transparent to presentuzzle and (f) virtual endoscopy in recta.
ventional endoscope is invasive and often uncomfortable forpatients and sometimes has serious side effects such as per-foration, infection and hemorrhage. VE visualization avoidsthese risks and can minimize difficulties and decrease mor-bidity when used before actual endoscopic procedures. Inaddition, many body regions not suitable with real endoscopecan be explored with VE. The VCH-F1 datasets allow us withgood opportunity to set foot in this field. As a preliminarywork, the flythrough path was drawn by fitting B-spline to thekey points located manually. Fig. 3(f) indicates a fly through inrecta.
3.1.3. Motion simulationPhysical human is the second stage of the whole developmentof VCH-F1 as mentioned in Section 1. Research on this issuehas started in our lab recently. The accurate human motionsimulation is of great practical significance. For instance, insports, the analysis and simulation of outstanding athletescan help coaches train their players. We accomplished the pre-liminary human motion simulation with the software 3DSMax7.0 and Virtools Dev 3.0.
In the motion simulation part of VCH clinic, the skeleton ofVCH-F1 could walk on the ground and make different gestures.All the motion data were acquired by two Avenir CCD lenses.Each motion had both front view and side view shot syn-chronously. These video clips were then converted to imagesequences, imported to the software 3DSMax and matched tothe VCH-F1 model.
What’s more, a motion simulation of the Olympic hurdlechampion Xiang-Liu was accomplished. This is a primitiveattempt in motion simulation with VCH-F1 model. In thiswork, we reconstruct the 3D motion of Xiang-Liu. The origi-
nal data was a monocular video clip of the Man’s hurdle racein Athens 2004 Olympic games. We firstly matched the fig-ure of the skeleton and muscle integrated model (SMI model)of VCH-F1 with Xiang-Liu’s figure by doing which we got
254 c o m p u t e r m e t h o d s a n d p r o g r a m s i n b i o m e d i c i n e 9 2 ( 2 0 0 8 ) 249–256
Fig. 4 – Motion simulation of VCH-F1. (a) The motion sequence of SMILX hurdling and (b) the comparison of the hurdlevelocity between Xiang-Liu and SMILX where the black broken line indicated the velocity of Xiang-Liu and the reddemonstrate SMILX. (For interpretation of the references to color in this figure legend, the reader is referred to the web
tion when Zu-San-Li was acupunctured (Fig. 5). The excitationenhanced and suppressive regions in brain were displayed inred and green color on the brain 3D model.
Fig. 5 – The demonstration of virtual acupuncture on
version of the article.)
the skeleton and muscle integrated Liu Xiang model (SMILXmodel). By using the key frame technology, we then recon-structed the whole hurdle action. The detailed process wasdescribed in Ref. [16]. We recorded the velocity of every hur-dle stride of SMILX model and compared it with Xiang-Liu’shurdle clearance velocity (the result was shown in Fig. 4(b)).The result indicated the practicability of motion simulationwith VCH-F1 model. More works are needed in the opti-mization methods to minimize the error and to make themotion simulation based on VCH-F1 model to assist the sportstraining.
3.2. Virtual acupuncture
Acupuncture is an important aspect of traditional Chinesemedicine because of its magic curative effect, simple opera-tion, low cost, and few side effects. Though acupuncture ispracticed all over the world, the accurate description of themechanism is still unclear. The construction of the completelyhuman dataset and the development of 3D visualization tech-nology make it possible to integrate the traditional practicewith modern medical theory. We attempted to use VCH-F1model to demonstrate the corresponding effect of cerebralmetabolic function induced by puncturing the Zu-San-Li (oneof the most frequently used acupuncture points, and is alsonamed STOMACH-36 or St 36). This is the first step to addfunctional data of real human being to VCH-F1.
The pathological data we used were positron emissiontomography (PET) images acquired on six young and healthymale volunteers by Neuroinformatics Center of PLA GeneralHospital in Beijing. Though functional magnetic resonanceimaging (fMRI) has been increasingly used for understand-ing the specific central mechanism of acupuncture in normalhuman subjects, PET, as a long-used cerebral homodynamicstudy method still provides irreplaceable quantitative mea-surement of cerebral blood flow (CBF) in vivo. Process of dataacquisition is detailed in Ref. [17].
We then use the software statistical parametric map-ping (SPM) [18] to localize brain areas with both increasedand decreased metabolic changes relative to the baselineand found that the excitement was strengthened in the
regions of gyrus precentralis and postcentralis, the foresideof right lobus temporalis and gyrus frontalis inferior [19].These results indicated that acupuncturing Zu-San-Li mightincrease glucose metabolism in pain related brain regionswhile metabolic changes were also seen in different parts ofthe autonomic nerve system, which is correlated to gastricfunction [17].
A serial of axial images of VCH-F1 lower limbs were markedaccording to the localization of acupuncture points in tradi-tional Chinese medicine and based on this, meridian lineswere created by B-spline fitting method [20]. Combining all thefunctional and anatomical information mentioned above, a 3Datlas was developed to demonstrate the change of brain func-
Zu-San-Li (St 36) point. The left image shows thereconstructed Meridians on the right leg and the position ofZu-San-Li (St 36) point. The right image demonstrates thereflection in brain regions when Zu-San-Li is acupunctured.

c o m p u t e r m e t h o d s a n d p r o g r a m s i n b i o m e d i c i n e 9 2 ( 2 0 0 8 ) 249–256 255
Fig. 6 – Reconstruction with the improved marching cubes algorithm. (a) Reconstruction of vessel label datasets. Thec b) VCi
3
Ilrtnymstadg
samaiiststMoi
tuiiFb
tOmit[
onglobated blocked vessels indicate cerebral hemorrhage. (mage-guided neurosurgery.
.3. Image-guided neurosurgery
mage-guided neurosurgery became indispensable over theast few years. By using image-guided technology, a neu-osurgeon could preserve normal tissue while maximizinghe resection of lesions during cortical surgery. Image-guidedeurosurgery incorporates medical image process and anal-sis techniques, medical image 3D visualization techniques,odern robotics and modern medicine. Image-guided neuro-
urgery strives to enhance the surgeon’s capability, to decreasehe invasiveness of surgical procedures and increase theirccuracy and safety. VCH-F1, as an integrated and detailedataset of human body, offers us an opportunity in image-uided neurosurgery research.
A novel automatic segmentation algorithm for brain tis-ue segmentation was schemed out. This method integratednisotropic diffusion filter, statistical threshold, mathematicalorphological operations, fuzzy connectedness and geodesic
ctive contour model (GACM). Moreover, we introduced a newdea for deformation driven by a Euclidean distance field ofmage edge in GACM. This method first generated a coarseegmentation of interest structure of brain using statisticalhreshold and mathematical morphology, and then refined theegmentation result using GACM driven by a Euclidean dis-ance field of image edge. The algorithm was evaluated usingontreal phantom dataset of brain, and the results show that
ur method is effective and robust when random noise andntensity inhomogeneities exist.
Though VCH-F1 dataset includes detailed image data ofhe brain, more pathological data are still needed in the sim-lation of real patients. It is generally recognized that the
ncorporation and effective utilization of MRA informationn image-guided surgery environment is very important [21].our MRA volume datasets from Navy General Hospital haveeen used to evaluate this algorithm.
For 3D reconstruction of labeled ROI data after segmenta-ion, an improved marching cubes algorithm was presented.nly the boundary voxels were smoothed for surface nor-
al calculation, this choice avoided using of Gaussian filtern all image space. Using the edge flag buffer and point posi-ion interpolation, the redundant point storage was avoided22]. The improved marching cubes algorithm was practiced
H-F1 acted as a “virtual patient” in our demonstration of
in the image-guided neurosurgery system of the neurosurgicaldepartment of Navy General Hospital, Beijing. Fig. 6 presentsthe visualization results of four vessel label datasets acquiredfrom MRA images in which the conglobated blocked structuresof the vessels indicate the location of cerebral hemorrhage,and such information is significant for surgeons while makingsurgical plan.
4. Conclusion and future work
In this paper, the progress of reconstruction and preliminaryapplication of VCH-F1 dataset are presented. During the 5years since the VCH-F1 dataset were sent to us, our lab hasdone a lot in the reconstruction of high-resolution 3D modelof the whole body and in the attempt to bring this data andthe technology into various practical issue. The achievement,weakness and the lesson we have learned are summed up asfollows.
In the reconstruction of VCH-F1 model, though we haveestablished almost all the main structures of the humanbody with approved quality, the model is by far not sufficientto demonstrate the entire human anatomical characteris-tics completely. In order to achieve this, more accurate andeffective segmentation is in demand. In our work, segmenta-tion is almost done manually or semi-automatically. VCH-F1datasets provides rich opportunities in researches of variousaspects. Our applications of VCH-F1 3D model, the healthscience facility VCH clinic, the virtual acupuncture and theimage-guided neurosurgery demonstrate a broad scope andvariety of applications of VCH-F1 dataset in medicine and bio-logical research. All these works are based on the accurate andhigh-quality 3D model of VCH-F1, though the quality may varyaccording to different practical tasks.
We have spent more than 4 years in segmentation andreconstruction. The various applications of VCH-F1, not onlythe model but also the related methodology, in differentareas have also taken the start. More efforts are still in need
to achieve new segmentation methods with more accuracy,robustness as well as effectiveness to achieve a more pre-cise anatomical model. Powerful computers are also in needto realize the higher-resolution display. Since human body is
s i n
r
resonance angiography, IEEE Comput. Graph. Appl. 12 (1992)12–13.
256 c o m p u t e r m e t h o d s a n d p r o g r a m
such a complex system and each individual is different, moredata are needed, from anatomical to functional, from macro tomicro and from physiological to psychological. The researchon virtual Chinese human is still in its infant stage and notfully qualified for the routine clinical use. However, furtherresearches for a more realistic and vivid simulation of humanbeing as well the more effective clinical application has beenmade possible with VCH-F1 dataset.
Conflict of interest statement
None.
Acknowledgements
Our sincere thankfulness goes to the donor of VCH-F1 andher relatives, whose support made all of the works possible.This research was supported by National “863” Develop-ment Project of High-Tech Research. The grant numbers are2001AA231031 and 2002AA231021. We would like to thankProf. Shizhen Zhong and his team for their excellent workon data acquisition of VCH-F1. We also want to express ouracknowledgement to all the people involved in this project.
e f e r e n c e s
[1] S.Q. Luo, Research of Virtual Chinese Human FemaleDataset, CJKMI 2004, Nogaya, Japan, 2004, pp. 89–91.
[2] R.A. Robb, Virtual endoscopy: development and evaluationusing the visible human datasets, Comput. Med. ImagingGraph. 24 (2000) 133–151.
[3] M.J. AcKerman, The Visible Human Project: a resource foreducation, Acad. Med. 74 (6) (1999) 667–670.
[4] V. Spizter, M.J. Ackerman, A.L. Scherzinger, D. Whitlock, Thevisible human male: a technical report, Am. Med. Inform.Assoc. 3 (1996) 118–130.
[5] S.P. Jin, S.C. Min, B.H. Sung, S. Byeong-Seok, H.S. Park, VisibleKorean human: its techniques and applications, Clin. Anat.19 (2006) 216–224.
[6] S.X. Zhang, P.A. Heng, Z.J. Liu, L.W. Tan, M.G. Qiu, Q.Y. Li, etal., The Chinese visible human (CVH) datasets incorporate
b i o m e d i c i n e 9 2 ( 2 0 0 8 ) 249–256
technical and imaging advances on earlier digital humans,Anatomy 204 (2004) 165–173.
[7] S.Z. Zhong, L. Yuan, et al., Research report of experimentaldatabase establishment of digitized virtual Chinese No. 1female, J. First Mil. Med. Univ. 23 (2003) 196–200, 209.
[8] Center for Human Simulation,http://www.visiblehuman.org.
[9] Voxel Man, http://www.voxel-man.de.[10] J.J. Camp, B.M. Cameron, D. Blezek, R.A. Robb, Virtual reality
in medicine and biology, Future Gener. Comput. Syst. 14(June) (1998) 91–108.
[11] E.Y.S. Chao, Graphic-based musculoskeletal model forbiomechanical analyses and animation, Med. Eng. Phys. 25(3) (2003) 201–212.
[12] Chinese Visible Human,http://www.chinesevisiblehuman.com/index e.aspx.
[13] G.W. Du, H.Z. Chai, H.Z. Cao, S.Q. Luo, High resolutionvisualization of VCH-female dataset, Proc. SPE 5444 (2003)453–458.
[14] K. Christian, H. Michael, E. Rolf, K.-H. Englmeier, VRinteraction techniques for medical imaging applications,Comput. Methods Programs Biomed. 56 (1998) 65–74.
[15] Virtools, A Dassault Systèmes Technology,http://www.virtools.com.
[16] L.H. Zhu, S.Q. Luo, Motion simulation of digital human withmuscle system, CJKMI 2008, Japan.
[17] X.L. Jin, Y.L. Ma, L. Yin, et al., PET imaging of glucosemetabolic response in human brain induced by stimulationof acupoint ST36, 20th International CODATA Conference,2006, Beijing.
[18] Statistical Parametric Mapping (SPM),http://www.fil.ion.ucl.ac.uk/spm.
[19] X.-P. Han, H.-Z. Cao, W.-D. Ni, et al., Research of extractingand displaying ROI of PET brain functional images, Chin. J.Med. Imaging Technol. 19 (11) (2003) 1459–1461.
[20] Q. Zhong, S.Q. Luo, 3D reconstruction of meridian based ondigital Chinese human-female, J. Capital Univ. Med. Sci., 25(3), 281–283.
[21] D.W. Shattuck, S.R. Sandor-Leahy, R.M. Leahy, et al.,Magnetic resonance image tissue classification using apartial volume model. Volume visualization of magnetic
[22] A.M. Dale, B. Fischl, M.I. Sereno, Cortical surface-basedanalysis. I. Segmentation and surface reconstruction,NeuroImage 9 (1999) 179–194.





![What Can Trigger Chinese Female Self-Objectification: Revealing … · 2018. 4. 27. · to female self-objectification [5]. In daily life, women spend the majority of their waking](https://img.pdfslide.net/doc/110x75/5fea12fd4be9881421294932/what-can-trigger-chinese-female-self-objectification-revealing-2018-4-27-to.jpg)