Embed Size (px)
Citation preview
665 GROUP B STREPTOCOCCUS INFECTION INDUCES TROPHOBLAST APOPTOSISOZLEM EQUILS1, KELLY DORAN2, JAMES MCGREGOR3, CALVIN HOBEL4, 1Universityof California, Pediatrics, Los Angeles, California, 2University of California,San Diego, Pediatrics, San Diego, California, 3University of Southern Califor-nia, Obstetrics and Gynecology, Los Angeles, California, 4University of Cali-fornia, Los Angeles, Los Angeles, California
OBJECTIVE: Group B streptococci (GBS) is one of the leading causes ofprematurity, and neonatal infection. Here, we assessed the cytotoxic effect ofGBS infection on trophoblasts.
STUDY DESIGN: We used JEG3 syncytiotrophoblast and 3A first trimestercytotrophoblast cell lines and either infected them with GBS or treated themwith GBS extract. In order to assess whether trophoblast invasion wasnecessary for GBS induced trophoblast death, we infected JEG3 cells withinvasiveness associated gene (iag) mutant GBS. In order to assess the effect ofB-hemolysin on GBS induced torphoblast death, we treated JEG3 cells withGBS extract obtained from B-hemolysin mutant GBS. Trophoblast death wasassessed by measuring supernatant lactate dehydrogenase release. Cell inva-sion was assessed by microscopic examination.
RESULTS: We observed that in JEG3 syncytiotrophoblast and 3A firsttrimester cytotrophoblast cell lines both infection with GBS and treatmentwith GBS cell wall extract induced cell death as compared to uninfected andmedia treated cells respectively. We observed that iagGBS was poorly invasivein trophoblasts as compared to wild type bacteria; however iagGBS infectionwas significantly cytotoxic in JEG3 trophoblast cells. We observed thattreatment of JEG3 trophoblast cells with cell extract from B-hemolysindeleted mutant was not cytotoxic.
CONCLUSION: Trophoblasts provide a barrier between fetal circulation andplacenta. Our data suggests that GBS invades and induces trophoblast celldeath; which may impair fetal-placental barrier and consequently allowbacterial penetrance into fetal circulation. GBS-induced trophoblast deathmay provide an alternative mechanism for GBS-pathogenesis in neonatal GBSinfection as well as preterm delivery.
666 PYELONEPHRITIS DURING PREGNANCY: A CAUSE FOR AN ACQUIRED DEFICIENCYOF PROTEIN Z JYH KAE NIEN1, DEBRA HOPPENSTEADT2, OFFER EREZ3,JIMMY ESPINOZA3, ELEAZAR SOTO3, JUAN PEDRO KUSANOVIC3, CHONGJAI KIM4, POOJA MITTAL3, JAWED FAREED2, JOAQUIN SANTOLAYA3,ROBERTO ROMERO1, 1Perinatology Research Branch, NICHD, NIH, DHHS,Bethesda, Maryland, 2Loyola University Medical Center, Department of Pa-thology, Maywood, Illinois, 3Wayne State University School of Medicine, De-partment of Obstetrics and Gynecology, Detroit, Michigan, 4Wayne StateUniversity School of Medicine, Department of Pathology, Detroit, Michigan
OBJECTIVE: Pyelonephritis during pregnancy has a more severe course thanin the non-pregnant state. This has been attributed to the susceptibility ofpregnant women to the Schwartzman Reaction (DIC). An acquired protein Zdeficiency has been reported when there is excessive thrombin activity. The aimof this study was to determine whether pyelonephritis results in changes in thematernal plasma protein Z concentrations.
STUDY DESIGN: A cross sectional study was designed and protein Z plasmaconcentrations were compared between normal pregnant women (n=71) andpregnant women with pyelonephritis (n=43), matched for gestational age.Protein Z plasma concentrations were measured by ELISA. Non-parametricstatistics were used for analysis.
RESULTS: 1) There was no change in plasma protein Z concentrations withadvancing gestational age in normal pregnant women; and 2) patients withpyelonephritis had a significantly lower median plasma concentration ofprotein Z than patients with a normal pregnancy (median 2.1 ml/ml, range 0.4-3.2 vs. median 2.4 ml/ml, range 1.1-3.4; p=0.029).
CONCLUSION: Pyelonephritis during pregnancy is associated with lowerconcentrations of protein Z. The most likely explanation for this observation isenhanced thrombin activity, which is known to cause an acquired protein Zdeficiency. This state can contribute to the severity of pyelonephritis duringpregnancy (e.g., development of ARDS).
667 THE ROLE OF FETAL VIRAL INFECTION IN THE DEVELOPMENT OF ADVERSEPREGNANCY OUTCOMES CATHERINE GIBSON1, ALASTAIR MACLENNAN1,PAUL GOLDWATER2, ERIC HAAN3, KEVIN PRIEST4, GUSTAAF DEKKER5, 1AdelaideUniversity, Obstetrics and Gynaecology, Adelaide, South Australia, Australia,2Women’s and Children’s Hospital, Microbiology and Infectious Diseases,Adelaide, South Australia, Australia, 3Women’s and Children’s Hospital, De-partment of Genetic Medicine, Adelaide, South Australia, Australia, 4Depart-ment of Health, Epidemiology Branch, Adelaide, South Australia, Australia,5Adelaide University, Maternal Medicine, Adelaide, South Australia,Australia
OBJECTIVE: To investigate the role of fetal viral infection in the develop-ment of a range of adverse pregnancy outcomes, including pregnancy-inducedhypertensive disorders (PIHD), antepartum haemorrhage (APH), intrauterinegrowth restriction !10th percentile (IUGR) and preterm birth (PTB).
STUDY DESIGN: The newborn screening cards of 717 cases and 609 controlswere tested for viral RNA and DNA from enteroviruses and herpesvirusesusing polymerase chain reaction (PCR). The herpesviruses were detected usingtwo PCRs, one detecting nucleic acids from HSV-1, HSV-2, EBV, CMV andHHV-8, hereafter designated Herpes group A viruses, and the other detectingnucleic acids from VZV, HHV-6 and HHV-7, hereafter designated Herpesgroup B viruses.
RESULTS: Detection of cytomegalovirus (CMV) DNA was significantlyassociated with preterm birth !28 weeks gestation (OR 1.62, 95% CI 1.02-2.57). The risk of developing PIHD was increased in the presence of Herpesgroup B viruses (OR 3.57, 95% CI 1.10-11.70), CMV (OR 3.89, 95% CI 1.67-9.06), any herpesvirus (OR 5.70, 95% CI 1.85-17.57) and any virus (OR 5.17,95% CI 1.68-15.94). Viral infections were not associated with IUGR or APHwithout hypertension; the combined presence of pre-existing hypertension andany herpesvirus was significantly associated with growth-restriction (OR 5.70,95% CI 1.17-27.73).
CONCLUSION: Exposure to in utero viral infection is significantly associatedwith very preterm birth !28 weeks gestation, and also with pregnancy-induced hypertensive disorders, but not with IUGR or APH.
668 HIVNET 024: NEUTROPHILIC AND MONONUCLEAR PLACENTAL INFILTRATION,ANTIBIOTICS AND OUTCOME IN AN AFRICAN POPULATIONROBERT GOLDENBERG1, VICTOR MUDENDA2, ELIZABETH BROWN3, TAHA TAHA4,EPHATA KAAYA5, 1University of Alabama at Birmingham, Obstetrics/Gynecol-ogy, Birmingham, Alabama, 2University Teaching Hospital, Pathology, Lu-saka, Zambia, 3Fred Hutchinson Cancer Research Center, Seattle,Washington, 4Johns Hopkins University, Baltimore, Maryland, 5MuhimbiliUniversity, Pathology, Dar es Salaam, Tanzania
OBJECTIVE: Histologic chorioamnionitis (HCA), usually defined as neu-trophilic infiltration (NI) of the chorioamnion (CA), is associated with pretermbirth (PTB), lower birthweights (BWT) and earlier gestational ages (GA).Antibiotics have not consistently reduced PTB. Fewer studies have evaluatedNI in other placental sites or mononuclear infiltration (MI) at any site andtheir relationship to antibiotic use or PTB. Our goal is to evaluate therelationship of NI and MI to pregnancy outcome.
STUDY DESIGN: A randomized trial of antibiotics to reduce PTB andperinatal HIV transmission was conducted at 4 African sites with negativeresults. Both HIV-infected (n=2098) and uninfected (n=335) women weregiven metronidazole 250 mg and erythromycin 250 mg at 20-24 wks tid for 7days and metronidazole 250 mg and ampicillin 500 mg q 4 hrs during labor, oridentical placebos. At delivery, the CA, decidua, umbilical cord and villi wereevaluated for NI and MI.
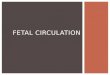
RESULTS: NI was common in the decidua (18%) and CA (28%) but less soin the cord (7%) and villi (0.1%). MI was common in the decidua (43%) andCA (34%) but not in the cord (0.1%) or villi (0.2%). NI in the membranes (29vs 23% p!0.05) was more common in HIV infected women as was MI (35 vs29% p=0.07). Decidual MI was associated with fewer PTB (20.1 vs 24.3%p=0.03) and longer time from randomization to delivery (p=0.04). Therelationship between NI at various sites and outcome are shown in the table()p!0.05). Antibiotics did not decrease NI or MI at any site.
Cord Membranes Decidua
Outcome No NI NI No NI NI No NI NI
BWT(g)(x) 2999 2779* 3005 2926* 3003 2898*GA(x) 39.0 38.2* 39.0 38.9 39.1 38.4*PTB ! 32 wks (%) 2.5 7.0* 2.4 4.0 2.2 6.1*PTB ! 37 wks (%) 21.7 32.4* 22.0 23.7 21.2 28.3*BWT ! 1500 g (%) 1.3 4.9* 1.2 2.5* 1.0 4.7*BWT ! 2500 g (%) 11.6 23.2* 10.9 16.5* 11.4 17.0*
CONCLUSION: NI, but not MI, in the cord, decidua, and CA is associatedwith PTB at various GA cutoffs and BWT !1500g and !2500g, as well asdecreased mean BWT and GA. HIV-infected women are more likely to haveNI, perhaps explaining part of the poorer outcomes in those women.Antibiotics do not decrease NI or MI.
S188 SMFM Abstracts

![Maternal and fetal predictors of fetal viral load and ... · strain-specific, in-house quantitative reverse transcrip-tion polymerase chain reaction (qRT-PCR) [19] in gilt serum (0,](https://img.pdfslide.net/doc/110x75/5f05bb5f7e708231d4146c9e/maternal-and-fetal-predictors-of-fetal-viral-load-and-strain-specific-in-house.jpg)