Embed Size (px)
Citation preview
The role of inpatient physicians in medical education has become an increasingly important topic as more academic healthcenters turn to the hospitalist model. The Association of Professors of Medicine invited National Association of InpatientPhysicians co-founders Winthrop F. Whitcomb, MD, and John R. Nelson, MD, to discuss how to prepare physicians to serveas hospitalists as well as how hospitalists can participate in training internal medicine residents.
To extend the debate, Jonathan C. Weissler, MD, will provide another perspective on the hospitalist issue next month.
The Role of Hospitalists in Medical Education
HOSPITALISTS AND MEDICALEDUCATION
The rapid growth of physicians practicing as hospi-talists has raised a number of new issues and chal-lenges that need to be addressed to ensure that
physicians continue to provide the best care for patientsand prepare physicians-in-training to provide such care.While some observers regard the addition of the hospi-talist model as a valuable innovation in care delivery, oth-ers see it as a liability for patients and physicians. None-theless, few disagree that hospitalists are likely to remainan important part of the United States health care systemfor the foreseeable future.
The increasing number of practicing hospitalistspoints to the need for careful consideration of whetherthey have been trained appropriately for their work andof modifying future training accordingly. Opinions re-garding optimal residency training for hospitalists havebeen offered by other authors (1–3).
This commentary is shaped by a combined 16 years offull-time hospitalist practice in nonacademic communityhospitals and through involvement in the National Asso-ciation of Inpatient Physicians (NAIP), the professionalsociety for hospitalists. This article addresses the size ofthe hospitalist work force; the role of hospitalists as edu-cators; how to train physicians to best accomplish thetasks of a hospitalist; and the role of NAIP in educatinghospitalists.
THE SIZE OF THE HOSPITALISTWORKFORCE
One problem in any discussion of hospitalist practice isthe lack of a single accepted definition of a hospitalist.Robert Wachter, MD (4), has proposed that a hospitalistis a physician who “spends at least 25% of his or herprofessional time serving as the physician-of-record forinpatients, during which time he or she accepts ‘hand-offs’ of hospitalized patients from primary care providers,
returning the patients to their primary care provider atthe time of hospital discharge.” Even using a more restric-tive definition of a hospitalist—a physician who devotesmore than 50% of his or her clinical time as physician ofrecord for hospitalized patients—an estimated 4,000physicians would qualify as hospitalists today, based onthe NAIP database. Although accurate historical num-bers of hospitalists are unavailable, there were probablyonly 300 to 500 in practice as recently as 1995. Jon D.Lurie, MD, and colleagues (5) estimated that if presenttrends continue, there could eventually be 10,000 to30,000 hospitalists in practice in the United States. Ed-ward O’Neil, PhD, and Rulin (6) predicted a range of3,000 to 30,000 hospitalists ultimately, depending on howmany patients each hospitalist could see daily, how manyhospitals have hospitalists, and whether they see surgicalpatients.
A question for debate is how rapidly the number ofhospitalists will reach projected numbers. The increase inhospitalists is likely to slow within 3 to 5 years; it will be 10to 20 years before the numbers reach the above projec-tions. In addition, it is unlikely that the hospitalist modelwill ever completely replace the traditional model of pri-mary care physicians (PCPs) seeing patients in the officeand hospital. Indeed, it is desirable for hospitalists andPCPs in traditional practice (office and hospital care) towork beside one another in the hospital. Each group canbenefit from the experiences and perspectives of theother.
Presently, the demand for hospitalists outstrips thesupply of physicians to fill the positions. However, thissituation will likely be reversed in the near future as aresult of increasing popularity of the hospitalist careertrack and an anticipated decrease in the rate of growth ofnew hospitalist positions.
THE HOSPITALIST AS EDUCATOR
The hospitalist model offers distinct advantages for edu-cating housestaff and students. These advantages are con-
q1999 by Excerpta Medica, Inc. 0002-9343/99/$–see front matter 305All rights reserved. PII S0002-9343(99)00234-X
APM Association of Professors of Medicine
ferred by the hospitalist’s availability in inpatient teach-ing settings and expertise in caring for hospitalized pa-tients. Early experience with hospitalists as facultysupport this notion, with the University of California,San Francisco, School of Medicine finding that overallhousestaff satisfaction with hospitalists as teachers wascomparable to the traditional service (7). In the samestudy, the housestaff indicated that they learned moreabout cost effectiveness and comparable amounts ofpathophysiology under a hospitalist system as comparedwith a traditional arrangement (7). Another study dem-onstrated equivalent resident satisfaction with hospitalistattendings versus other faculty members (8), and a thirdstudy found a marked improvement in supervision ofprocedures with hospitalist attendings (9).
Hospitalist teaching positions are being added to de-partments of internal medicine at many teaching pro-grams. Despite this growth, critics point to potentiallyundesirable consequences of hospitalists serving as teach-ing attendings. As hospital lengths of stay decrease, in-hospital educational opportunities are compressed. Withhospitalist attendings, this challenge is compounded byteachers who often have no knowledge of a patient priorto hospitalization. And with little or no contact with pa-tients following discharge, some elements of the educa-tional process may be diminished (10). However, fearsthat hospitalist attendings might decrease the autonomyof residents because of their increased presence on theward and that subspecialty training of fellows might becompromised owing to decreases in the number of con-sultations by hospitalists are not supported by existingdata (7). Although hospitalist attendings are an impor-tant addition to teaching programs, residents should haveexposure to non-hospitalist attendings as well.
COMPONENTS OF HOSPITALISTTRAINING
Despite predictions of a large hospitalist workforce in thefuture, rapid and sweeping changes in residency trainingaimed at incorporating more inpatient experience areunwarranted and could be deleterious. Residents des-tined for careers as hospitalists need significant exposureto the outpatient setting to understand what can reason-ably be done for patients outside the hospital and to ap-preciate the psychosocial aspects of a patient’s illness be-fore and after hospitalization. Furthermore, because hos-pitalists and outpatient physicians work together closelyin patient care, preservation of a common training base isimportant.
Limited data contribute to the widespread opinion thatgeneral clinical skills in traditional internal medicinetraining receive appropriate emphasis for future work asa hospitalist (2). However, one must remember that all
existing data on the hospitalist model emerge from phy-sicians who have had traditional residency or subspecialtytraining. Thus, one cannot argue that changing the wayhospitalists are trained is required to bring about the ben-efits presently associated with hospitalists. However, it isclear that the addition of new areas of competence willserve hospitalists well.
A 1998 survey of NAIP members revealed that geriat-rics, neurology, and perioperative medicine were impor-tant for practice as a hospitalist but not adequately em-phasized in training (2). Other areas regarded as inade-quately covered in training were health economics andutilization management, quality improvement, coordi-nation of care between settings, and management of ter-minally ill patients.
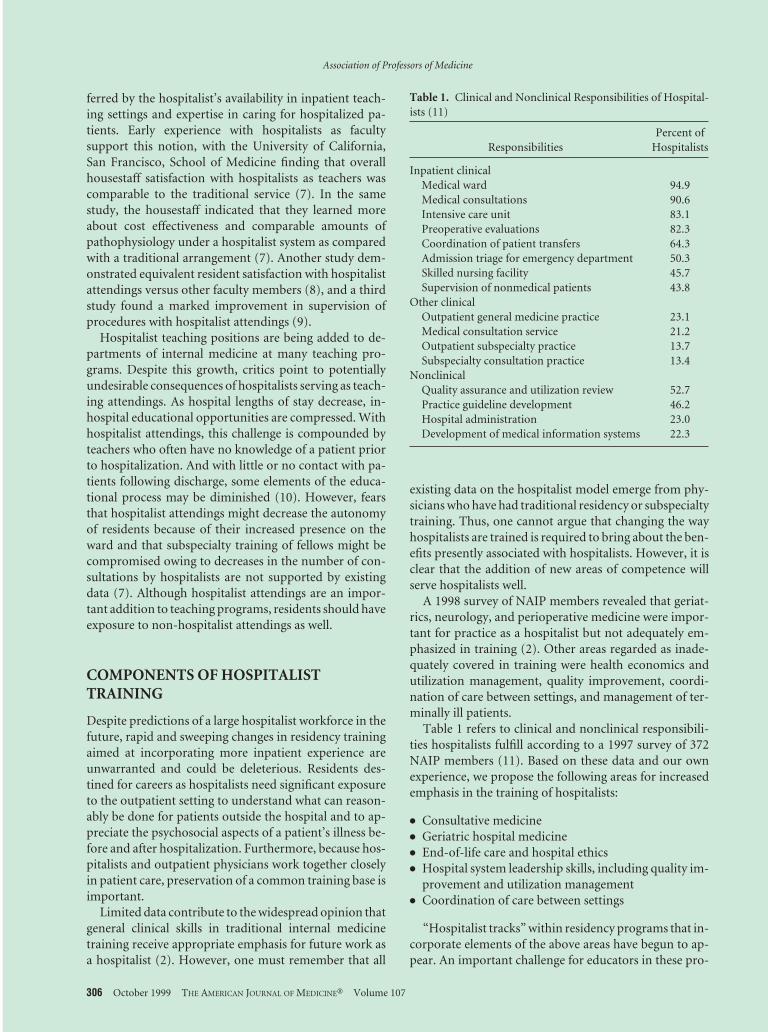
Table 1 refers to clinical and nonclinical responsibili-ties hospitalists fulfill according to a 1997 survey of 372NAIP members (11). Based on these data and our ownexperience, we propose the following areas for increasedemphasis in the training of hospitalists:
● Consultative medicine● Geriatric hospital medicine● End-of-life care and hospital ethics● Hospital system leadership skills, including quality im-
provement and utilization management● Coordination of care between settings
“Hospitalist tracks” within residency programs that in-corporate elements of the above areas have begun to ap-pear. An important challenge for educators in these pro-
Table 1. Clinical and Nonclinical Responsibilities of Hospital-ists (11)
ResponsibilitiesPercent of
Hospitalists
Inpatient clinicalMedical ward 94.9Medical consultations 90.6Intensive care unit 83.1Preoperative evaluations 82.3Coordination of patient transfers 64.3Admission triage for emergency department 50.3Skilled nursing facility 45.7Supervision of nonmedical patients 43.8
Other clinicalOutpatient general medicine practice 23.1Medical consultation service 21.2Outpatient subspecialty practice 13.7Subspecialty consultation practice 13.4
NonclinicalQuality assurance and utilization review 52.7Practice guideline development 46.2Hospital administration 23.0Development of medical information systems 22.3
Association of Professors of Medicine
306 October 1999 THE AMERICAN JOURNAL OF MEDICINEt Volume 107

grams will be to avoid overly customized training for hos-pitalists to avoid a schism between the disciplines ofinpatient and outpatient care. Also, because existing re-quirements in residency training may leave little room foraddition of new material, an opportunity exists for fel-lowship and other post-residency training in some or allof these areas.
Consultative MedicineConsultative medicine—ranging from perioperativemedicine and consultation to obstetrics-gynecology, psy-chiatry, rehabilitation, and other services—is a naturalarea for hospitalists because of their availability for timelyassessment and follow-up (12). For some surgical pa-tients, hospitalists serve as the attending-of-record, inwhich the surgeon performs the operative interventionand acts as consultant for postoperative surgical care, butthe hospitalist is responsible for the overall care of thepatient. In other institutions, hospitalists serve as “co-managers” of surgical patients, acting as a partner withthe surgeon for all care outside the operating room. Pre-liminary data support this model’s effectiveness in reduc-ing utilization of resources, improving outcomes, andproviding value to surgeons and referring physicians(13). In many cases, hospitalists become the de facto co-managers of surgical and other patients because of theiravailability to the ward.
The involvement of hospitalists in primarily nonmed-ical cases is especially important in patients with multiplecomorbidities and challenging social and ethical issues,when the nonmedical attending physician may not be asavailable or as skilled in managing specific problems asthe hospitalist. Whether as physician-of-record, consul-tant, or comanager, skills in consultative medicine areessential for the hospitalist.
Geriatric Hospital MedicineA substantial and increasing proportion of hospitalizedpatients is elderly. While representing only 13% of theAmerican population, individuals aged 65 years andolder account for 31% of hospital discharges and 42% ofinpatient hospital days (14). As a result, a large portion ofhospitalist practice is devoted to care of the elderly.
As the discipline of geriatrics has matured, it has be-come clear that the elderly have unique needs during hos-pitalization, presentations of disease are often atypical,and the use of technology for diagnosis and treatment has
greatly increased risks against which benefits must beweighed. Leipzig and colleagues (15) have articulated cer-tain competencies in geriatrics (Table 2) that should berequired of all hospitalists.
End-of-Life Care and Hospital EthicsIn the United States, more than 60% of adults die in hos-pitals (16). Hospitalized patients are known to spend alarge part of their last days in pain and exposed to aggres-sive measures despite their wishes (17). This realizationsupports widespread observations that physicians arepoorly trained in the care of the dying.
Thus, a major opportunity exists to bring about sys-tematic change in the way care is delivered to the dyingpatient for physicians who practice hospital medicine.Three competencies in end-of-life care have been identi-fied (Table 3) (18). Skill in common ethical issues thatarise in the hospital is also important for hospitalists (19).
Hospital System Leadership SkillsAn important benefit of hospitalists lies in their ability tobe “good citizens” of the hospital. The hospitalist is ide-ally suited to understand and improve systems of carewithin the hospital, which have historically suffered froma lack of systematic study and physician involvement. Tothat end, training in health care system improvement,including the skills of quality improvement and outcomemeasurement, are necessary tools for hospitalists (20,21).
Because the cost of hospital care in the United States islarge (22) and payers are invested in controlling thesecosts, physicians practicing hospital medicine are underincreasing pressure to limit utilization of hospital re-sources. At the same time, it is the responsibility of thephysician to manage utilization with the best interests ofthe patient in mind. Thus, training in cost-effective deci-sion making, appropriate use of hospital admission andcontinued inpatient stay, and the capability of care deliv-ery in nonacute settings is needed for hospitalists (Table4).
Coordination of Care Between SettingsAn inherent weakness of the hospitalist model is the lon-gitudinal discontinuity of care that results from having aphysician who practices solely in the hospital setting. Be-cause of this “modularization” of care, emphasis must beplaced on understanding how various loci of care inter-relate (23).
Table 2. Geriatric Competencies for Hospitalists (15)
Atypical presentations of common diseasesGeriatric pharmacologyRisks, prevention, and interventions for geriatric syndromesSkills for interdisciplinary teamworkIntegration of medical evidence with patient values
Table 3. Competencies in End-of-Life Care for Hospitalists(17)
Communicating about illness and death with patients andloved ones
Palliating symptomsProviding psychosocial support
Association of Professors of Medicine
October 1999 THE AMERICAN JOURNAL OF MEDICINEt Volume 107 307

The experience of countries that have long employed ahospitalist-like model supports the idea that a “voltagedrop” of information flow between care settings is a realphenomenon and underscores the need for added train-ing in this area (24). Skills in information managementare important and should include an understanding ofwhat information referring physicians need, how theywant it transmitted, and when they need it (25). Duringresidency training, time spent in nonhospital settings, in-cluding the outpatient clinic, emergency department,skilled nursing facility, hospice, and home, is importantto learn how to coordinate care effectively as patientsmove in and out of the hospital.
SHOULD INPATIENT MEDICINE BECOMEA SPECIALTY?
In time, it will be beneficial to have a formal certificationpathway to demonstrate competence in inpatient medi-cine. Certification and specialty designation will helpmaintain high standards in inpatient care and serve as aguide for continuing medical education for hospitalists.Because the hospitalist model is sometimes viewedmerely as a more expedient form of practice that benefitspayers, the casual observer might erroneously concludethat it has been invented by managed care solely to serveits financial interests. Certification will help to maintainthe focus on providing excellent care for patients, not juston economics and efficiency.
The American Board of Internal Medicine (ABIM)does not regard inpatient medicine as a specialty yet andhas no immediate plans to develop steps to certify hospi-talists (26). However, as the field of inpatient medicinedevelops a research base and an identified set of compe-tencies, it will be appropriate for ABIM and the AmericanBoard of Family Practice to develop a hospitalist certify-ing examination with NAIP’s input. Although there isconcern that a specialty certification for hospitalists willresult in the elimination of hospital privileges for physi-cians who are not so designated, this event is unlikely tohappen even if the number of certified hospitalists growssignificantly because of the large number of PCPs whowill wish to care for their hospitalized patients. Still, it isappropriate to delay the creation of a certification path-way until there is general agreement on the compositionof the hospitalist skill set.
NAIP’S ROLE IN EDUCATINGHOSPITALISTS
In its mission to meet the needs of hospitalists and theirpatients, NAIP has chosen three areas of focus for its ac-tivities: education, advocacy, and the support of investi-gation in inpatient medicine. To date, the association hasdevoted many of its educational resources to organiza-tional and political matters of importance to hospitalists.In coming years, NAIP will increase attention to clinicaltopics as hospitalists become well established in thehealth care system.
NAIP’s role in education will be to work with its mem-bers, other specialties, and health care institutions to de-fine a skill set for hospitalists and offer meaningful pro-grams to attain this expertise. As the professional societyfor hospitalists, NAIP has and will continue to have aunique role in the education of the new specialist. Weanticipate the establishment and expansion of a range ofeducational opportunities, including national and re-gional conferences, online and written materials (such asa journal), and interactive training modules designed toteach the skills outlined above. In addition, formal recog-nition of educational achievement will be an importantfunction of the organization.
NAIP aims to be a resource for academic health centers(AHCs) that have hospitalists. To date, it has offered andsupported several programs on hospitalists and training.In the future, NAIP will seek to establish positions on theappropriate content and structure of training programsfor hospitalists. Clearly defined guidelines for educationwill promote a uniform approach by the nation’s AHCsfor hospitalist training.
Winthrop F. Whitcomb, MDJohn R. Nelson, MD
Dr. Whitcomb and Dr. Nelson are co-presidents of theNational Association of Inpatient Physicians. Dr. Whit-comb is the director of the inpatient medicine service atMercy Hospital in Springfield, Massachusetts; Dr. Nelsonis a hospitalist in Gainesville, Florida.
REFERENCES1. Wartman SA, Silver AL, Walerstein SJ, et al. The hospitalist
movement: an education and research agenda. New Med. 1999;3:11–16.
2. Fenton CL, Plauth WH, Pantilat SZ, Wachter RM. Training forhospital-based practice: do we need a specialized curriculum? Pre-sented at the SGIM Annual Meeting, San Francisco, May 1, 1999.Abstract.
3. Hauer KE, Flanders SA, Wachter RM. A model hospital medicineresidency track. Presented at the NAIP Second Annual Meeting,New Orleans, April 21, 1999.
Table 4. Hospital System Leadership Skills for Hospitalists
Quality improvementOutcome measurementMultidisciplinary team buildingCost-effective decision makingAppropriate use of acute and nonacute care setting
Association of Professors of Medicine
308 October 1999 THE AMERICAN JOURNAL OF MEDICINEt Volume 107
4. Wachter RM. An introduction to the hospitalist model. Ann InternMed. 1999;130:338 –342.
5. Lurie JD, Miller MS, Lindenauer PK, et al. The potential size of thehospitalist workforce in the United States. Am J Med. 1999;106:441– 445.
6. O’Neil E, Ruhlin C. Health workforce needs of hospitalist basedhealth systems. Presented at The Emerging Role of Hospitalists inAmerican Health Care: A National Conference, San Francisco, De-cember 5– 6, 1997.
7. Wachter RM, Katz P, Showstack J, et al. Reorganizing an academicmedical service: impact on cost, quality, patient satisfaction, andeducation. JAMA. 1998;279:1560 –1565.
8. Palmer HC, et al. The effect of a hospitalist service on patient care inan academic teaching hospital. Presented at the SGIM AnnualMeeting, San Francisco, May 1, 1999. Abstract.
9. Hunt DK, Henderson MC, Badgett RG. Impact of a hospitalistteaching service on internal medicine residency training. Presentedat the SGIM Annual Meeting, San Francisco, May 1, 1999.
10. Schroeder SA, Schapiro R. The hospitalist: new boon for internalmedicine or retreat from primary care? Ann Intern Med. 1999;130:382–387.
11. Lindenauer PK, Pantilat SZ, Katz P, Wachter RM. Hospitalists andthe practice of inpatient medicine: results of a survey of the Na-tional Association of Inpatient Physicians. Ann Intern Med. 1999;130:343–349.
12. Strathy G. Quality of care and the hospitalist. The Hospitalist. 1997;3:3– 4.
13. Macpherson DS, Parenti C, Nee J, et al. An internist joins the sur-gical service: does co-management make a difference? J Gen InternMed. 1994;9:440 – 444.
14. Vital and Health Statistics. Data on Older Americans, 1992. Series 3:
Analytic and Epidemiologic Studies, No. 27. US Department ofHealth and Human Services, Publication 93-1411; 1993.
15. Leipzig RM, Bloom HG, Lavizzo-Mourey R, Cassel CK. Shouldhospitalists be geriatricians? Submitted for publication.
16. Vital Statistics for the United States. 11. Mortality. Washington, DC:National Center for Health Statistics; 1993.
17. Pantilat SZ, Cassel CK. End-of-life issues for the hospitalized pa-tient. Presented at the NAIP Second Annual Meeting, New Orleans,April 21, 1999.
18. The SUPPORT Principal Investigators. The study to understandprognoses and preferences for outcomes and risks of treatments(SUPPORT). JAMA. 1995;274:1591–1598.
19. Lo B. Ethical issues in the hospital. Presented at Management of theHospitalized Patient in the Managed Care Era, San Francisco; April11, 1997.
20. Berwick DM, Nolan TW. Physicians as leaders in improving healthcare: a new series in the Annals of Internal Medicine. Ann InternMed. 1998;128:289 –292.
21. Nolan TW. Understanding medical systems. Ann Intern Med. 1998;128:293–298.
22. Ginzberg E. The changing US health care agenda. JAMA. 1998;279:501–504.
23. Whitcomb WF, Nelson JR. Hospital Interfaces. 2000. In press.24. Isaac DR, et al. The GP-hospital interface: attitudes of general prac-
titioners to tertiary teaching hospitals. Med J Aust. 1997;166:9 –12.25. Pantilat SZ, Lindenauer PK, Katz PP, Wachter RM. Primary care
physician preferences for communication about their inpatientscared for by hospitalists. Presented at the NAIP Second AnnualMeeting, New Orleans, April 21, 1999.
26. Kelley, MA. The hospitalist: a new medical specialty? Ann InternMed. 1999;130:373–375.
Association of Professors of Medicine
October 1999 THE AMERICAN JOURNAL OF MEDICINEt Volume 107 309