Embed Size (px)
Citation preview

The Society of Cardiothoracic Surgeons of Great Britain and Ireland
Fifth National Adult Cardiac Surgical Database Report2003
Improving outcomes for patients
Compiled by
Bruce E. KeoghKBE BSc MD FRCS FECS FETCSSociety of Cardiothoracic Surgeons
Robin Kinsman BSc PhDDendrite Clinical Systems Ltd

The Society of Cardiothoracic Surgeons of Great Britain and Ireland
Fifth National Adult Cardiac Surgical
Database Report 2003
Improving outcomes for patients
Compiled by
Prof. Bruce Keogh Dr Robin Kinsman
KBE BSc MD FRCS FESC FETCS BSc PhD
Society of Cardiothoracic Surgeons Dendrite Clinical Systems Ltd

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
2
The Society of Cardiothoracic Surgeons of
Great Britain and Ireland
gratefully acknowledge the assistance of
Dendrite Clinical Systems Ltd
for
data harvesting, data aggregation,
data analysis, risk modelling
and publishing this report.
Dendrite Clinical Systems Ltd is registered
under the Data Protection Act
Data Protection Act Register Number
Y33 54 136
This document is proprietary information that is protected by copyright. All rights reserved. No part of this document may be photocopied, stored in a retrieval system, transmitted in any form or by any means, electronic, mechanical, photocopying, recording or otherwise, without the permission of the publishers and without prior written consent from the Society of Cardiothoracic Surgeons of Great Britain and Ireland, the Royal College of Surgeons, 35/43 Lincoln’s Inn Fields, London, WC2A 3PN.
Windows and Excel are registered trademarks of the Microsoft Corporation.
Crystal Reports is a registered trademark of Crystal Decisions.
The Patient Analysis & Tracking System is a registered trademark of Axis Clinical Software Inc.
July 2004 Edition. A catalogue record for this book is available from the British Library. ISBN 1-903968-09-7
© 2004 Dendrite Clinical Systems Ltd and the Society of Cardiothoracic Surgeons of Great Britain and Ireland. All rights reserved.
Published by:
Dendrite Clinical Systems Ltd, 59A Bell Street, Henley-on-Thames, Oxfordshire RG9 2BA, United Kingdom
Contact details: Phone: +44 1491 411 288, Fax: +44 1491 411 377, E-mail: [email protected]
£60.00 €90.00
Printed and Bound by CPL Associates
ABC

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
3
Executive summary
• This report documents the nature of contemporary cardiac surgery practice in the United Kingdom and Ireland.
• Cardiac surgery in the UK and Ireland is safe by international standards
• The operative mortality rate for all major operation groups continues to fall despite a worsening casemix.
• Coronary surgery activity has settled at about 25,000 cases a year. Combined valve and coronary surgery continues to increase with over 3,000 combined operations performed in the financial year 2002-2003.
• Analysis of contemporary risk profiles of cardiac surgery patients shows that surgeons are presented with patients of increasing complexity year-on-year; this trend is quite marked.
• This report focuses on coronary surgery, which represents about 70% of cardiac surgical activity. Our results for coronary surgery are comparable with the best in the world and continue to improve:
• We are better at treating the elderly. The proportion of patients over 75 years old has increased by more than 4½-fold over the last decade. During the last 5 years the mortality in this group has fallen by 35%.
• We are better at treating diabetics. The proportion of diabetic patients has risen from 15% to 22% since 1997, but the operative mortality has fallen from 5.4% to 2.6% a reduction of 50%.
• We are better at treating women with heart disease. Around the world women have a higher operative mortality than men, but this has fallen by over 30% in the UK and Ireland since 1997.
• We are better at treating people with high blood pressure. The proportion of patients with high blood pressure has risen from 48% in 1998 to 65% in 2003. During this time the mortality for these patients has fallen from 2.8% to 2.1%. A reduction of 25%.
• We are better at treating patients with very sick and weak hearts. About 10% of patients have very weak hearts. With improving techniques the operative mortality for this group has been reduced by 30% over the last 5 years.
• Two-thirds of coronary surgery patients are overweight or frankly obese.
• Only 70% of coronary bypass operations are elective. There is marked variation between hospitals in the proportion of elective and urgent operations. The operative mortality for non-elective coronary cases is twice as high as for elective patients. This is not changing.
• Patients who have had a previous heart attack are almost twice as likely to die at the time of surgery compared with people who have not had a heart attack.
• For the first time in the UK surgical results for individual surgeons have been analysed for a mainstream specialty in the UK. With the statistical methodology employed, all surgeons meet acceptable standards over the three financial years 2001-2003.
• Data submission for basic activity and mortality for coronary surgery is voluntary but complete for all consultant surgeons in the UK.
• Data capture of variables that allow for comparisons in casemix between institutions and surgeons is incomplete preventing reliable and meaningful risk adjusted comparisons.
• Crude mortality, not adjusted for casemix, has therefore been used for comparative analyses.
• A surgeon’s crude mortality naturally fluctuates from year to year.
• The level of variation in crude mortality between surgeons is less than that seen in New York or New Jersey where similar data are published.

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
4
Preface Mr Patrick Magee President of the Society of Cardiothoracic Surgeons of Great Britain and Ireland
The first National Adult Cardiac Surgical Database Report was produced in 1996. It consisted of a stapled pamphlet with data from 12 centres. Since then we have come a long way. This report of over 340 pages is an almost complete record of contemporary cardiac surgical practice in the UK today. It provides a mine of information, which will be of value to surgeons, patients and those interested in healthcare.
The information is compiled from several data sources each of which brings a different perspective to our understanding of national practice. The UK Cardiac Surgical Register tells us exactly how many different operations were performed in 2002/2003 and what the results were in each unit. Data from The National Adult Cardiac Surgical Database on over 210,000 patients paints a picture of how patient populations have changed over the last decade and how they vary between different units in the UK. The UK Heart Valve Registry data provides long-term mortality data on patients undergoing heart valve replacement in the UK over the last 15 years.
Information of this nature is interesting enough on its own. However, following events in Bristol we have also focussed on how to measure performance. Within the specialty we have developed ways of measuring and predicting the risk of surgery both within the UK and internationally. We have applied this knowledge to give better informed consent to our patients and to monitor our own performance and compare it with others. These techniques are clearly described in the report and are applicable to many other specialties.
The last couple of years have engendered considerable unease as we have struggled over how best to present individual surgeon’s results. Although we know every surgeon’s results for coronary surgery our data is not yet good enough to allow us to cater for variations in casemix, which can be very different. An experienced surgeon is likely to operate on different patients to a less experienced surgeon. We have done the best we can with the available data. The methodology and its rationale are clearly described. All consultant surgeons have contributed voluntarily to this endeavour, which is a mark of our commitment to transparency and quality. We remain concerned, however, that unless this process is handled properly patients will suffer if surgeons feel compelled to avoid the higher risk patients.
This report is a remarkable achievement, which would not have been possible without the encouragement, vision and support of many. Dr Peter Walton of Dendrite Clinical Systems has been instrumental in establishing this Blue Book and has fully supported this project over the years. Robin Kinsman has personally merged and checked all the submitted data and brought increasing intellectual independence and scrutiny to the process of data management and analysis.
Bruce Keogh has provided leadership and encouragement as this process has evolved over the years, but in addition has put in endless hours analysing and preparing the information for presentation. This impressive document is evidence of this effort. Finally, of course, none of this would be possible without the enthusiastic participation and support of the members of the Society of Cardiothoracic Surgeons.

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
5
Foreword Mr James Roxburgh Secretary of the Society of Cardiothoracic Surgeons of Great Britain and Ireland
A quarter of a century ago the Society of Cardiothoracic Surgeons of Great Britain and Ireland agreed to collect raw mortality data for a wide range of cardiac and thoracic surgical procedures. The idea was that all units would submit unit specific data to the Society who would then collate the data and publish annual mortality figures. It was expected that units would then compare these national figures with their own and look for variations and if there was cause for concern, subject their own results to a more detailed review. However as The Bristol Inquiry showed simple collection of the data was not enough, we needed to be more proactive and monitor performance centrally 1. There can have been few surgeons who did not feel that during The Bristol Inquiry we were hung by our own petard when it came to data collection! What had started out as an innovative and ground-breaking project was used as a stick to beat us with; but far from cowering under the pressure of the press coverage and the politicians we have slowly but surely built up a performance review mechanism that is second to none.
It has been said that by publishing individual performance indicators for Consultant Cardiac Surgeons we have crossed the Rubicon; this is indeed true but we have done so flanked by our involvement in two major projects, the NCEPOD study into deaths following first-time coronary artery surgery, and the cardiac surgical component of the Central Cardiac Audit Database (CCAD). The NCEPOD study is a detailed examination of all deaths following surgery for first-time coronary artery surgery over a 3-year period and will involve some 1500 patients. The study will gather information about the patient’s treatment from their first presentation to hospital through up to the events surrounding the death. The outcome of cardiac surgery is multi-factorial and this project is, we believe, the first of its kind to be undertaken anywhere in the world; since it is a joint undertaking with an organisation with a proven track record in the analysis of peri-operative deaths. The CCAD study will allow near real-time submission of data to a central database that will then feed back to the units comparative figures of their performance against national values. This will involve the submission of around 150 data points for every single cardiac surgical procedure undertaken in the United Kingdom, this high volume of data will allow units to receive comparative data on a whole variety of performance indicators such as death, complication rates and length of stay. It will also provide information about the case-mix of unit workload, an important factor in understanding outcome measures. The information from these projects will of course be published in future editions of the Blue Book and will be a unique resource of high quality performance indicators that are available to the public and the profession alike.
The sporting cliché There is no 'i' in team should be borne in mind when discussing the release of surgeon-specific data. The outcome of a cardiac surgical procedure is par excellence an example of teamwork. There are many factors; such as the patient’s general condition, the other medical staff (cardiologists, anaesthetists, intensivists and junior medical staff), the post-operative care (nurses, physiotherapists, pharmacists etc.), the hospital facilities (infection rates, physical plant) and so on, that can have a bearing on the surgical outcome that it is invidious to name an individual as responsible for the success or failure of a cardiac surgical operation. In this day and age many of these factors are simply outside the day-to-day control of the Consultant Surgeon. We have though not used this argument to refuse to publish individual performance figures but hope that the format in which it is published underlines the need to examine surgical outcomes on a unit basis. The result the major projects that are currently underway will, I believe, persuade most people that unit-specific data is of more use to the patients and the public as a whole. The Society has monitored the results of surgeons on an individual basis for over 5 years and will of course continue to do so. Many of the techniques used in performance monitoring and risk management have been developed in the aviation industry; and it has been argued that the airline pilot/passenger and the surgeon/patient relationships are synonymous in risk management terms. However I would argue that that the patient’s journey through hospital is analogous to a holiday abroad rather than a single airline flight. One would no more blame or praise the pilot for the hotel, weather or food than one should hold an individual surgeon accountable for the functioning of the whole hospital. We must take a system-based approach to these complex matters and not one directed towards an individual. The performance individuals within that system must of course be monitored and the Society of Cardiothoracic Surgeons has been responsible for the review of Consultant Cardiac Surgical performance for over 5 years, the results have not, until now, been published.
Cardiac surgery in the United Kingdom can justly claim to be world leaders in the way it provides high quality meaningful performance data to the profession and public alike. It is now high time that other high volume interventional specialities demonstrated their commitment to performance review and the public presentation of this information.

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
6
Acknowledgements to key contributors
SCTS Executive Committee 2002 -2003
Member Position Tenure City
Mr Pat Magee President 2004-2006 London
Prof. Bruce Keogh President-elect 2004-2006 London
Mr James Roxburgh Secretary 2004-2009 London
Mr Babulal Sethia Treasurer 2004-2009 London
Mr Graham Cooper Meeting Secretary 2000-2005 Sheffield
Mr Peter Goldstraw Chairman, Specialist Advisory Committee on Higher Surgical Training
1999-2005 London
Mr Andrew Murday Chairman, Intercollegiate Examination Board 2004-2007 Glasgow
Mr Leslie Hamilton Cardiothoracic Dean 1999-2004 Newcastle
Mr Jonathan Hyde Young Consultants’ Representative 2002-2004 Brighton
Mr Christopher Munsch Cardiothoracic Tutor, Royal College of Surgeons of England
2000-2004 Leeds
Mr Alfred Wood Representing the Republic of Ireland From 2003 Dublin
Mr Michael Lewis Trainees’ Representative 2002- Birmingham
Mr Steven Hunter Elected member 2002-2005 Middlesbrough
Mr Alan Faichney Elected member 2002-2005 Glasgow
Mr Simon Kendall Elected member 2003-2006 Middlesbrough
Mr Richard Page Elected member 2003-2006 Liverpool
Mr Stephen Livesey Elected member 2004-2007 Southampton
Mr Graham Venn Elected member 2004-2007 London
Ms Jacqueline Nicol Nursing Representative 2004-2007 Glasgow
Recent Executive Committee members contributing to the development of this report
Member Position Tenure City
Mr Colin Hilton President 2002-2004 Newcastle
Mr Jim Monro President 2000-2002 Southampton
Mr Andrew Murday Chairman, Intercollegiate Examination Board 2001-2004 Glasgow
Mr Terence Lewis Elected member 2000-2003 Plymouth
Mr Robert Bonser Elected member 2001-2004 Birmingham
Mr Mark Jones Elected member 2001-2004 Manchester
Mr Sam Nashef Elected member 1999-2002 Papworth
Mr David Luke Representing the Republic of Ireland Till 2003 Dublin
All UK surgeons
This report would not have been possible without the ongoing support of the members of the Society who have generously submitted their heart surgery data for analysis.
Other contributors who deserve acknowledgement
Dr Alan Bailey, who co-founded and managed the Cardiac Surgical Register for the last 25 years; Dr Roger Boyle, the National Director for Heart Disease in England; Dr Jill Pell, Chairman of the Scottish Cardiac Registers Steering Committees; Mr Martin Old, project manager of CCAD; Mrs Maria Shortis, founder of Constructive Dialogue for Clinical Accountability, for ensuring that the issues of clinical excellence and patient safety remain central to our endeavours.

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
7
Data managers
Data management 2003 CITY HOSPITAL
Surgical audit lead Data manager
Aberdeen Royal Infirmary Mr El Shafei Ms E Anderson
Belfast Royal Victoria Hospital Mr A Graham Ms B Scullion
Birmingham Queen Elizabeth Hospital Mr B Keogh (to 2003) Mr D Pagano (2004)
Ms V Barnett
Blackpool Victoria Hospital Mr J Au Ms C Malpas
Brighton Royal Sussex County Hospital Mr A Forsyth Mrs J Gayfer
Bristol Royal Infirmary Mr A Bryan Mr D Finch
Cardiff University Hospital of Wales Prof. U Von Oppell Ms C Bray
Cork Cork University Hospital Mr A O’Donnell Ms M Delaney
Coventry Walsgrave Hospital Mr R Patel Mrs A Nugent
Dublin Mater Misericordiae Mr A E Wood Mr P Marsden
Dublin St James’s Hospital Miss E McGovern Ms A Hughes
Edinburgh Royal Infirmary Mr W Walker Mr A Deegan
Glasgow Royal Infirmary Mr A Murday Ms A McOuat
Glasgow Western Infirmary Mr G Berg Ms M Kinnaird
Hull Castle Hill Hospital Mr L Guvendik Mr N Richards
Leeds General Infirmary Mr P Kay Mr J Peckover
Leicester Glenfield Hospital Mr T Spyt Mr P Stafford
Liverpool Cardiothoracic Centre Mr B Fabri Mr A Ward
London Guy's & St Thomas’ Hospitals Mr J Roxburgh None
London Hammersmith Hospital Mr P Punjabi Ms S Krikler
London Harefield Hospital Mr A Khaghani Mr P Kimberley
London King's College Hospital Mr J Desai Mr J Omigie
London London Bridge Hospital Mr G Venn Mrs L Katsumbe
London The Heart Hospital Mr D Lawrence Mr M Curtis
London Royal Brompton Hospital Mr N Moat Mr P Kimberley
London Bart’s and the London Mr A Wood Mr N Silverside
London St George's Hospital Mr J Smith Dr O Valencia
London St Mary's Hospital Mr B Glenville (to 2003) Mr R Stanbridge (2004)
None
Manchester Royal Infirmary Mr D Keenan Ms S Chaisty
Manchester Wythenshawe Hospital Mr B Bridgewater Mr S Bullough
Middlesbrough South Cleveland Hospital Mr A Owens Ms T Smailes
Newcastle Freeman Hospital Mr S Barnard Ms S Jamieson
Nottingham City Hospital Mr I Mitchell Mr M Whitworth
Oxford John Radcliffe Hospital Mr C Ratnatunga Mr C Evans
Papworth Papworth Hospital Mr S Nashef Ms S Powell
Plymouth Derriford Hospital Mr A Marchbank Mrs K Caley
Sheffield Northern General Hospital Mr D Hopkinson Ms J Daly Ms L Kirk
Southampton Southampton General Hospital Mr S Livesey Ms A Green
Stoke-on-Trent N Staffordshire Royal Infirmary Mr C Smallpeice Mrs J O’Bree
Swansea Morriston Hospital Mr A Youhana None

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
8
Summary of contents
This report is divided into the following sections:
1. Acknowledgements to key contributors (page 6-7).
2. Preface and foreword from the President and the Secretary of the Society (pages 4-5).
3. Introductory section (pages 13-38).
Regional perspectives on data issues, progress against the Bristol Royal Infirmary Inquiry Report and basic information for patients.
4. The United Kingdom Cardiac Surgical Register (pages 40-59).
The UK Cardiac Surgical Register was established in 1977 to collect activity and mortality data for all cardiac surgery conducted in NHS hospitals in the UK.
The UK Cardiac Surgical Register was terminated in 2003 and has been replaced by the National Adult Cardiac Surgical Database.
5. Report from the United Kingdom Heart Valve Registry (pages 60-71).
The UK Heart Valve Registry was established in 1986 to collect data on all heart valve implants in the NHS and to track those patients for re-operation and death. Mortality tracking is conducted through the Office of National Statistics (England, Scotland & Wales) and the Central Services Agency (Northern Ireland).
6. The National Adult Cardiac Surgical Database (pages 72-212).
The National Adult Cardiac Surgical Database was established as a pilot project in 1994 and first reported in 1996. It aims to collect detailed information on all patients undergoing heart surgery in the UK. This section focuses on coronary surgery and describes the national patient population, how this population changes over time and how it varies between hospitals. It also describes how changes in surgical practice and surgical techniques have resulted in ever-improving outcomes for patients.
7. Principles of risk measurement and stratification for coronary surgery (pages 213-243).
This section describes ways of measuring surgical risk in a way that is of value to for individual patients and also for measuring performance.
8. Missing data (pages 234-239).
9. Performance indicators and the presentation of surgical results (pages 244-263).
This is another new section. It provides information on performance for both units and surgeons.
10. Institutional and individual surgeon performance (pages 264-309).
11. Long-term follow-up for patients with different risk factors (pages 310-318).
This is a new section made possible by the linkage between a test centre and the Central Cardiac Audit Database to provide long-term mortality tracking through the Office of National Statistics. This adds an entirely new dimension to the potential for analyses that are available on the national data, and will further aid the decision-making process for both patients and surgeons.
12. Appendices (pages 320-340)
A detailed table of contents can be found on the following pages.

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
9
Table of contents
Executive summary 3 Preface 4 Foreword 5 Acknowledgements to key contributors 6
SCTS Executive Committee 2002 -2003 6 Data managers 7
Summary of contents 8 Introduction 13 Perspective from the English Department of Health 14 The value of national data collection: a Scottish perspective 15 A cautionary note on the interpretation of surgical results 16 Background to the Society’s data-collection initiatives 17
Harmonising datasets for the CCAD 23 Difficulties in data collection 25 The National Service Framework for Coronary Heart Disease 28
Audit requirements defined within the National Service Framework 28 Milestones relating to clinical audit 28
Progress against the Bristol Royal Infirmary Inquiry Report 29 The need for data validation 31 Collaboration between the SCTS and the NCEPOD 33 Improving informed consent 34 Informing patients and the public 35 Basic principles of cardiac surgery 36
Valvular heart disease 36 Coronary artery disease 36 Surgical correction of valvular and coronary artery disease 36 Types of bypass grafts 37
The United Kingdom Cardiac Surgical Register (UKCSR) 40 Overall trends in cardiac surgery since 1977 40 Trends in coronary artery bypass surgery since 1977 41 Trends in valve surgery since 1977 42 UKCSR: Data for financial year 2003 43
UKCSR: summary data financial year 2003 43 UKCSR: single open valve operations financial year 2003 44 UKCSR: multiple open valve operations financial year 2003 44 UKCSR: miscellaneous operations for IHD financial year 2003 45 UKCSR: miscellaneous operations for acquired heart disease financial year 2003 46 UKCSR: cardiac surgical activity by centre financial year 2003 47 UKCSR: results by centre financial year 2003; first-time isolated CABG 50 UKCSR: results by centre financial years 2001-2003; first-time isolated CABG 51 UKCSR: results by centre financial year 2003; first-time isolated AVR 52 UKCSR: results by centre financial years 2001-2003; first-time isolated AVR 53
Don’t jump to conclusions 54 Comparison of different sources of data on isolated CABG procedures 56
Final transition from the UKCSR to the NACSD 57

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
10
The United Kingdom Heart Valve Registry (UKHVR) 60 Background 60 Data collection 60 Follow up data 61
Re-operation 61 Notification of death 61
Feedback information 61 Publication 62 Research output from the HVR 62
The National Adult Cardiac Surgical Database (NACSD) 72 Introduction to the database 72 Contributing centres and trusts 72
Contributing centres 73 Data harvest, import, merge and analysis methodology 74
Data collection facilities by centre as at June 2004 76 General cardiac surgical outcomes 77
Mortality rate by procedure 77 Post-operative stay 78
Valve surgery 79 General 79 Aortic valve surgery 80 Mitral valve surgery 82 Mitral valve replacement and repair 84
Coronary artery bypass surgery 87 Age 89 Gender 98 Size – body surface area and body mass index 104 Priority 110 Ejection fraction 116 Previous myocardial infarctions (MIs) 122 Percutaneous coronary intervention (PCI) 132 Left main stem (LMS) disease 134 Previous surgery 140 Diabetes 148 Hypertension 154 Peripheral vascular disease (PVD) 160 Renal disease 166 Angina 172 Dyspnoea (breathlessness) 178 Interactions between risk factors 184
Re-operation for post-operative bleeding 186 Re-operation for post-operative bleeding by procedure 186 Re-operation for post-operative bleeding after isolated CABG 188
Aspects of coronary surgery practice in the UK and Ireland 195 Number of bypass grafts 195 The use of arterial grafts 197 Protecting the heart during coronary surgery 201
Influence of myocardial protection technique on mortality 203 On- and off-pump CABG 204

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
11
International comparisons 205 United Kingdom, Ireland and the USA 210
Evolution of risk factors in coronary bypass surgery 211 Experience from the Society of Thoracic Surgeons National Database (1980-2000) 211 Development of trends 211 Practical considerations 211 Conclusions 212
Risk stratification for coronary surgery 214 What risks are attached to my operation? 214 The Parsonnet score 215
Parsonnet score distributions through time 215 Mortality by Parsonnet score 217 Completeness of Parsonnet score 218
The EuroSCORE 219 EuroSCORE distributions through time 220 Mortality by EuroSCORE 221 Completeness of EuroSCORE data 222
The Logistic EuroSCORE 223 Logistic EuroSCORE distributions through time 223 Mortality by Logistic EuroSCORE 224 Completeness of logistic EuroSCORE data 225
Bayesian modelling 226 What do Bayes tables do? 226 Two Bayesian risk models for isolated coronary artery bypass surgery 227 Simple (5-factor) Bayes model for isolated CABG 228 Complex (9-factor) Bayes model for isolated CABG 228 Adoption of the complex Bayes model 229
The complex Bayes score 230 Complex Bayes score distributions through time 230 Mortality by complex Bayes score 232 Completeness of the complex Bayes score data 233
Missing data 234 Missing simple Bayes variables 234 Missing complex Bayes variables 236 Missing EuroSCORE variables 238
Testing a risk scoring system 240 Receiver Operating Characteristic (ROC) curve 240 Calibration plot 240
Comparisons of risk scoring systems 241 ROC curve areas 241 Calibration 242
Performance indicators and the presentation of surgical results 244 The application of risk stratification 244
Why do we need statistical analysis at all? 244 Setting a benchmark threshold for comparison 245 The graphical presentation of results 245
Average outcomes over a given timeframe 245 Ranking analyses 245 Funnel plots 247
Sequential analyses 249 Standard CUSUM 249 Setting control limits around CUSUM curves 251

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
12
Variable Life-Adjusted Display (VLAD) 253 Plotting cumulative risk 253 The VLAD plot 253 Risk Adjusted CUSUM (RA-CUSUM) 256 Sequential probability ratio testing (SPiRiT) 258 Beyond mortality 260
Institution- and individual-surgeon performance 264 A general perspective on the publication of cardiac surgical results 264
Different data-sources tell different stories 277 Hospital Episode Statistics 280 Paul Ayling, Clinical Senior Lecturer in Epidemiology and Public Health, Assistant Director 280 Dr Foster Unit at Imperial College 280 Background to the publication of individual surgeon’s performance against standards 281
Why publish individual surgeon’s results? 281 The way forward 282 Could crude mortality be presented? 283 Examining institutional influences on outcomes 285 Key points in interpreting the hospital tables including surgeons’ performance 286
Long-term follow up through the Central Cardiac Audit Database 310 Appendices 320
Governance arrangements for adult cardiac surgical audit components 321 The Parsonnet score 324 The EuroSCORE 325 The simple (5-factor) CABG Bayes score 326 The complex (9-factor) CABG Bayes score 327 Facts of life the figures can hide 328 Guidelines for the audit of cardiothoracic surgical practice 330 Quality accreditation programme for adult cardiac surgery 332 The minimum dataset 335
References 348

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
13
Intro
du
ctory sectio
n
Introduction Prof. Bruce Keogh Co-ordinator, UK Cardiac Surgical Register and National Adult Cardiac Surgical Database
This is the most authoritative and comprehensive public documentation of national contemporary cardiac surgical practice available anywhere in the world.
It is authoritative because it has been primarily written by surgeons for surgeons, but in such a way that we believe will be of interest and value to non-medical readers. It is based on professionally collected data with surgically relevant analyses determined by constructive feedback, comment and support from the whole cardiothoracic surgical community in the UK and Ireland. We hope that this authority is strengthened by an open and transparent approach, which acknowledges the flaws and deficiencies in the data and the limitations this imposes on both the analyses and their interpretation.
It is comprehensive because it includes:
• Data from over 210,000 individual patient records.
• Data capture from 100% of NHS centres from England, Scotland, Wales and Northern Ireland.
• Increasing contributions from the Republic of Ireland and the private sector.
This fifth edition builds on previous editions with some new innovations:
• Long-term survival data with tracking through the Central Cardiac Audit Database (CCAD).
• New data from the UK Heart Valve Registry.
• 25-year trend data on activity and hospital mortality for different types of operations.
• 10-year trend data on risk factors.
• Presentation of volume and outcome graphs for both institutions and surgeons.
• Individual named surgeons’ reports.
We continue to publish unadjusted mortality data for coronary bypass and aortic valve replacement surgery for every NHS unit in the UK. This year the unit results are supplemented with an analysis of the results of coronary bypass surgery for every consultant surgeon within the UK. For this we have used crude mortality, unadjusted for casemix, because our data is not yet good enough to apply casemix adjustment to every surgeon’s practice. We also have some concerns around the accuracy of risk adjustment statistics when applied to small individual practices. Nevertheless, we are the first mainstream specialty to have achieved consensus on how to scrutinise individual surgeons’ results, and the first to publish how those results relate to transparent standards. This represents a level of professional maturity, which should be reassuring to our patients.
However, our patients should also be reassured by other information presented in the book. Our national results compare very favourably with international standards and continue to improve. As our patients become older so our results for elderly patients improve (see pages 90-91), as we treat more people with diabetes so the results for diabetic patients improve (see pages 148-149) and as we increasingly understand how to protect the heart itself from the insult of major surgery so the results of surgery for patients with very weak hearts improve (see page 117).
We are now working with the Healthcare Commission, the Central Cardiac Audit Database and the Heart Team in England to develop a robust mechanism for data validation (see pages 31-32). The data feels right, but tighter focus on data quality is essential if we are to engage in safe and sometimes sensitive comparative analyses (see pages 264-309).
The importance of accurate data was highlighted by the Bristol Royal Infirmary Inquiry Report 2 and the Government’s response 3. The SCTS concurs with this important principle as reported in The Times 4, the BMJ 1, 5 6 Heart 7 and in a comprehensive report of a joint study with the Nuffield Trust, the RAND organisation and the California Office of Statewide Health Planning and Development 8, 9 in which the methodology was defined. Clearly the level of validation will determine how the data can be used.
The publication of this book and previous reports reflects considerable effort, enthusiasm and commitment from a cohesive body of clinicians and managers in a successful collaboration with Dendrite Clinical Systems who have provided the data management expertise. This report demonstrates that where vision and determination exist it is possible to collect, merge, analyse and present national information for a whole specialty. Such information is the essential bedrock for ensuring safe and effective clinical governance and improving outcomes for our patients.

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
14
Intr
od
uct
ory
sec
tio
n
Perspective from the English Department of Health Dr Roger Boyle National Director for Heart Disease, England
The last report from the National Audit Cardiac Surgical Database showed quite clearly how the Society of Cardiothoracic Surgeons was leading the way in making clinical outcome data available to the general public. This report shows for the first time, tables that identify individual surgeons in a fashion that allows patients to be reassured that their surgeon meets the professional standards set by the Society while, at the same time, avoids the pitfalls of year-on-year fluctuations in outcome data. This is vitally important since, in the past, where concerns have been raised about individual centres and surgeons, the solutions have been found not in problems with individuals but in the management of the whole system in the complex settings that cardiac centres have become.
The last 12 months has seen further major progress towards improving cardiac services in England. Major capital schemes are underway across the land to improve the clinical setting in which our patients are to be treated and waiting times have continued to improve. No patient waits more than 6 months now for coronary bypass surgery and we are on target to achieve a maximum wait of 3 months by April 2005. At the time of writing there are, on average, just 19 patients waiting for each of our consultant cardiac surgeons.
Another point that is important to highlight is the extremely high standard of care that is being offered in this country. Despite ever-increasing complexity of case-mix, the mortality rates here compare favourably with those anywhere in the world. This is a tribute to the high standards of training being made available in Britain and to the commitment to quality that the Society of Cardiothoracic Surgeons promulgates.
There are challenges ahead. More and more cardiologists are finding ways of treating cases by angioplasty leaving a much more complex series of patients for surgeons to tackle. There will be inevitable effects on outcomes as well as length of stay in ICU and in hospital overall. These changes will need to be factored in as we move to the collection of risk stratified data into the servers of the Central Cardiac Audit Database (CCAD). This developing system already contains some 500,000 episodes of care, mostly admissions with heart attack but increasingly admissions for bypass surgery and angioplasty. Soon it will be possible to track not just the mortality rates after an event but also event-free survival, probably a much better measure of quality.

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
15
Intro
du
ctory sectio
n
The value of national data collection: a Scottish perspective Dr Jill Pell Consultant in Public Health, Greater Glasgow NHS Board Chairman of the Scottish Cardiac Registers Steering Committees
Since 1996, we have collected data prospectively on all adult cardiac surgery procedures performed in Scottish NHS hospitals. The following year, we set up a second register to collect data on all percutaneous coronary interventions performed in Scottish NHS hospitals. In 2000, we expanded the interventional cardiology register to include diagnostic catheterisation and, in the last year, we have started to receive data from private hospitals.
We have separate steering committees for the cardiac surgery and cardiology registers. However, we have long recognised that the distinction is relatively meaningless in the clinical setting where patients may be considered for or undergo both surgery and percutaneous intervention. Therefore, since 1997, the cardiac surgeons have distributed their annual report to interventional cardiologists and vice versa. This year we took a further step towards full integration by producing our first annual report to cover cardiac surgery, percutaneous intervention and coronary angiography.
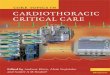
In Scotland, we are fortunate that data on all admissions to hospitals have been collected routinely since 1981. Since the inception of our cardiac registers, we have linked our data to the national hospital admission database and death certificate data to provide follow-up information on events such as myocardial infarction, readmission to hospital, re-investigation, repeat procedures and survival. As a result, we have been able to monitor trends in outcome over time, by procedure and between different sub-groups of patients. We have been able to demonstrate, for example, that the well-recognised improvements in in-hospital mortality following coronary artery bypass grafting have translated into statistically significant improvements in longer-term survival (see figure below).
There are a number of benefits to having a Scottish register, such as linkage to routine data sources, fostering local ownership and therefore improvements in data quality, and ensuring that decisions on service developments are evidence-based. However, Scottish clinicians are also aware of the importance of contributing data to the UK registers, such as the Society of Cardiothoracic Surgeons’ database, in order to provide better benchmarking for use in clinical audit and governance. Also, there is much to be gained from sharing ideas and experience of how best to analyse, present and disseminate data. Therefore, as in previous years, the Scottish cardiac registers are pleased to contribute to this important report.
Isolated CABG: Actuarial survival curves for Scotland (n=8,181)
1997-1998 1999-2000 2001-2002
80%
82%
84%
86%
88%
90%
92%
94%
96%
98%
100%
0 200 400 600 800 1,000 1,200 1,400 1,600 1,800 2,000
Time after operation / days
Surv
ival
rat
e

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
16
Intr
od
uct
ory
sec
tio
n
A cautionary note on the interpretation of surgical results Prof. Tom Treasure, Guy’s and St Thomas’ Hospital, London
Simplistic data may disadvantage patients as well as surgeons
UK cardiac surgeons are entitled to feel proud of the quantity and quality of data that are available and the innovative ways in which our data are presented. The UK Cardiac Surgical Register was a professional initiative started years before the buzzwords clinical audit, the quality agenda and clinical governance were coined 10 and a very long time before CHI, CHAI and NICE were invented. The objectives of the founding fathers of the UK Register were clear: to improve standards. Without the need to pillory anyone it was possible for us all to see the sort of results that were being achieved nationally and to judge whether results in our own units were about the same, better, or worse. It was not the way of things to make public exposés but it would be a mistake to think that the hospitals of Britain were populated by gung-ho surgeons who would carry on regardless, putting lives at risk. Not all the thoracic surgeons of the 1950s made the successful transition to open heart surgery. Not all of the cardiothoracic surgeons of the sixties and seventies took to coronary surgery. In the 1980s it became much less acceptable to do a few congenital operations in children amongst a largely adult practice. Many unpublicised decisions were made on the basis of reflective reading of the annual reports. Some surgeons made these decisions for themselves; others reached a policy in discussion with colleagues; and some had the decision made for them because the clinical referrals were deliberately steered in another direction. Local policies were informed by the data provided in the Register, which we surgeons would seize and scrutinise as it came through the letterbox each year. That unpublicised but quietly effective process is not well known and not remembered. Unfortunately it did not always work that way. What will be remembered are the instances where that process of introspection has let us down and surgeons have had to be publicly forced to stop.
During what I like to refer to as the Bristol show trial some credit was given to cardiac surgeons for collecting data, but we were criticised for making them anonymous. Now the identity and reputation of the surgeon is on the line at the outset. The problem with legislation designed to stop the same thing happening again is that the rules may change practice in a way that was not anticipated. A well-known example is the legislation following the scandalous behaviour of the London landlord of the early 1960s, Rachman (who has given his name to the word Rachmanism, listed in the Oxford English Dictionary). New laws were drafted to protect poor tenants from an unscrupulous and, in that case, a brutal landlord. The law gave to the tenant such security that well intentioned private property owners willing to let a flat, a bed sitter, or the basement of a house now too large for them, would not take the chance. Instead of improving the situation for the tenants, rented property became scarce and more expensive.
The rules under which we now must live and work are being made to stop Bristol happening again and there is no point beating about the bush for Bristol is named by everyone in politics, the press, and the profession. I fear we are already seeing the Rachman effect. As we use surgeon specific outcome data to try to improve things for the patients we actually make things worse. There is no doubt in the mind of any cardiologist that I have talked to that it is much harder to persuade a surgeon to take on the more risky coronary cases. There are patients who we predict have a slim chance of survival without surgery who willingly accept a 20% or 30% risk. Now let us look at that from the point of view of say a surgeon with a mixed cardiothoracic practice, other duties and three or four half day operating sessions a week and a share of the on call rota. Suppose the coronary operations number 50 in the year. Every death is 2%, three deaths in the year makes 6%, and that is the trigger for the cautionary word. Knowing the 95% confidence limits of 3/50 (1.25% to 16.6%) does not make the problem go away. The figures 1.25% to 16.6% span the best but also the very worst of contemporary outcomes. In journalists’ terms 6% is twice the national average mortality and that bald statement, without risk adjustment, is the one that the Medical Director and the Chief Executive may be given. It does not take a mathematician to tell us that it is a dumb use of statistics. These are the rules that were intended to protect patients from the imagined coterie of unskilled surgeons who are as arrogant as they are reckless. It is in the higher risk cases that we make the biggest impact on survival and yet the new rules may deprive these patients of care. We must count but we must use the numbers intelligently. Data sets should not supplant common sense.

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
17
Intro
du
ctory sectio
n
Background to the Society’s data-collection initiatives
The Society of Cardiothoracic Surgeons has a 25-year history of voluntary data collection and analysis, which is described in detail below:
Society of Cardiothoracic Surgeons Parallel Initiatives
UK Cardiac Surgical Register See page 40 Established 1977 by Sir Terence English and Dr Alan Bailey
Basic activity and outcome data of 250 categories of adult cardiac operations. Data received from 100% of UK NHS and all Republic of Ireland units. Aggregated national data fed back to each unit to allow comparisons of local results with national average. Discontinued in 2003 to encourage focus on the National Adult Cardiac Surgical Database. Since 1997 this has included individual surgeon’s results for coronary surgery. This will continue until the Central Cardiac Audit Database is fully functional and can take over this role. Funded by Society membership.
UK Thoracic Surgical Register Established 1978 by Prof. Hugoe Matthews and Dr Alan Bailey. Currently administered by Prof. Tom Treasure
Basic activity and outcome data on many categories of adult thoracic surgical procedures. Data from 100% of NHS cardiothoracic and thoracic surgical units. Funded by Society membership.
UK Heart Valve Registry See page 60 Established 1986 by Professor Ken Taylor
Initially funded by the English Department of Health but more recently by the Commission for Health Improvement and then the Healthcare Commission. Collects patient details on about 60-65% of all heart valve patients in the UK. Linkage to the Office of National Statistics (England, Scotland & Wales) and the Central Services Agency (Northern Ireland) provides long-term mortality tracking now approaching 20 years. Unique international resource. Funding withdrawn 2004.
National Adult Cardiac Surgical Database See page 72 Established 1994 by Mr Bruce Keogh and Dr Peter Walton
The basis of this report. 100% of NHS units contribute individual patient data. Compatible with American, European and other international initiatives.
No external funding.
Central Cardiac Audit Database See page 23 Pilot established 1996. Funded by the English Department of Health through the Healthcare Commission and administered by the NHS Information Authority Managed by Dr David Cunningham and Mr Martin Old
Collects patient orientated data from 100% of UK paediatric cardiac surgical units and provides mortality tracking through the Office of National Statistics. Will become data collection route for all cardiac procedures and will incorporate the UK Heart Valve Registry and the National Adult Cardiac Surgical Database. Society will continue to merge and analyse Scottish, Welsh and Irish data for its members and the public.
Funded by the Healthcare Commission in England.

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
18
Intr
od
uct
ory
sec
tio
n
The history and principles of data collection by the Society
Patients have a right to good surgery. They also have a right to informed consent so they can make the right decision. It is our responsibility to provide appropriate information so that all parties understand the basis on which a decision for surgery is made. Similarly, the purchasers with constrained budgets and difficult decisions will also benefit from quantitative information on the nature of the patient population being referred for and undergoing cardiac surgery. We cannot provide this information without robust local and national data.
…
In principle the model for a successful national database is simple. There are two basic aspects. Firstly, each contributing unit should collect all variables in the agreed dataset for each and every patient. The data should be collected in a system allowing data export in a predefined format. Merging of the data centrally is then easily manageable. Secondly, the data should be robust and validated.
Introduction to 1999-2000 Report
The Society of Cardiothoracic Surgeons has a long history of national data collection. In 1977 Sir Terence English established the UK Cardiac Surgical Register, which collected activity and mortality data on all cardiac operations performed in NHS units in the UK. Although simple in concept, the process represented the first attempt in Britain by any speciality to collect national activity and outcome data. These data were unit specific, but were not in any way risk-stratified which limited its value for statistically valid outcome comparisons.
In 1986 Professor Ken Taylor and Mr John Dark (senior) set up the UK Heart Valve Registry. This was a unique visionary step forward. It was different in several ways.
• Firstly, data on heart valve implantation was to be collected not by surgeons, but by an independent nominated person working in the cardiac surgical operating theatres in each unit.
• Secondly, the form requesting information, including patient identifiers was no longer than one side of A4 paper
• Thirdly, using the patient identifiers the data was linked to the Office of National Statistics so the patients could be flagged up on the system when they died. This provided the basis for the first long-term follow up of valve surgery patients in the world
• Finally, the system allowed identification of re-operations
This provided us with a unique resource, which has provided insight into a number of aspects of valve surgery and patient survival.
In 1994 the Society of Cardiothoracic Surgeons recognised the need to collect comprehensive data on patients undergoing cardiac and thoracic surgery and supported a proposal to develop a patient orientated National Adult Cardiac Surgical Database to replace the UK Cardiac Surgical Register over a ten year timeframe starting from 1996. At that time there were signs of a move away from simple, aggregated data to patient-by-patient data. This move had been driven by the fact that aggregated data could not be used to give the same detailed analysis options that patient-specific data would afford. The current dataset includes demographic data, procedural data and outcome data for each patient. The reasons for collecting more comprehensive data were becoming increasingly clear. Firstly, there was growing public and political interest on both sides of the Atlantic in cardiac surgical outcomes. In the United States there was clear evidence that misconception of operative risks was a leading cause of malpractice actions. Secondly, the Society of Thoracic Surgeons in the United States had shown that hospitals, cardiologists and in some cases surgeons, were ignorant of the changing patterns of patient populations undergoing coronary surgery and that this perpetuated the professional and public misconception that coronary surgery carried little or no risk. Finally, the release of raw mortality data on Medicare patients into the public domain in the late 1980s by the Healthcare Financing Administration without respect for any of the known patient-specific risk factors or co-morbidities created considerable concern within the cardiothoracic community. Then in 1990 Newsday successfully sued the New York Department of Health under the Freedom of Information Law to release risk adjusted surgeon specific outcome data starting the trend towards the public reporting of surgical outcomes.
Contemporaneously in the UK the purchaser – provider split in healthcare provision provided some parallels with developments in the United States. The similarities indicated that if we were to succeed in the new

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
19
Intro
du
ctory sectio
n
healthcare market we would need to understand the nature of our own patient population in the United Kingdom and have a grasp of surgical outcomes for patients with differing severities of illness. The Society of Thoracic Surgeons in the US had responded by establishing a National Cardiothoracic Surgical Database with an agreed comprehensive dataset in 1989-1990. It seemed sensible that we should not re-invent the wheel and we therefore agreed, through the Standards of Care Committee and the Executive Committee, a reduced version of the US dataset, which was broadly compatible with existing databases in the UK.
Recognition of the requirement for an agreed dataset and national database has been slow in some quarters. However, momentum has grown recently, in part as a response to events in Bristol, but mainly as surgeons and healthcare administrators recognise the value of comprehensive data collection for understanding severity of illness, resource allocation and outcome analysis. This enthusiasm has been complemented by the government’s initiative on clinical governance, which further emphasises the surgeon’s duty to understand the quality of care he is providing.
This report demonstrates significant progress in this endeavour. We have clearly shown that electronic downloading of anonymous patient specific data from centres that collect such data is feasible. However, there is much to do and enormous opportunities remain. The issues that we must focus our attention on are the same issues that were outlined in the 1999-2000 Report:
• Standardising data collection.
• Ensuring data collection from all units.
• Developing and understanding the strengths and limitations of methods for measuring and comparing differences in casemix.
• Recognising the difference between hospital mortality and quality.
• Producing sensitive quality indicators to help improve the quality of hospital care.
• Tracking long-term follow-up of patients.
• Building a national resource for the Society and its members and patients and their families.
Standardising data collection
There are still considerable differences in the datasets collected by different units. These differences need to be ironed out if we are to realise the potential benefits of the National Adult Cardiac Surgical Database project. In England and Wales we have had considerable support in this endeavour through the National Service Framework for Coronary Heart Disease (NSF) launched in March 1999 and the CCAD project. The NSF document outlines the requirements for hospital audits, one of which is risk adjusted mortality following coronary artery bypass surgery. This is supported further by the inclusion in the NSF document (Chapter 5, pages 24–40) of the Society’s recommended dataset, which is designed to facilitate stratification for casemix. Furthermore, the NSF imposes a timeframe for collection of this data. Milestone 3 states that:
… by April 2002, in every local network of cardiac care hospitals … should have clinical audit data no more than 12 months old that describes the relevant audit criteria. Where relevant these data are derived from participation in national audits.
Unfortunately the NSF recommendations do not apply to the whole of the UK, so national differences in datasets may persist. This can be accommodated by a mapping process, termed correspondence, but a common dataset would ultimately bring more value to all participants.
The recommended dataset was agreed by the Society Executive in 1996. It was modified slightly in September 2002 with a view to implementation of the changes in April 2003. It has been designed not only to allow stratification of patients according to severity of illness using most current algorithms, but also to track changes in surgical practice, explore specific aspects of surgical training and to examine outcomes. Although a smaller dataset would be easier to collect, it would be of less and less value in the longer term. Relatively simple analyses of the data in the National Adult Cardiac Surgical Database have demonstrated that there are interesting and significant trends in various risk factors over time. Not all of these trends could have been predicted when the project was first launched, and the exclusion of one or more risk factors might have meant that these trends would have remained permanently hidden (see changing risk factors, page 211).
It would also mean that the UK data would be less compatible with parallel, evolving international initiatives, with the implication that useful international comparisons might not be possible. The current dataset is reasonably comparable to the new Society of Thoracic Surgeons (USA) dataset both in terms of size and detail. It is also compatible with the European and US cardiac surgical databases, and the well-established UK Heart Valve Registry. As such, the current dataset should serve to facilitate good clinical audit and governance within each unit and provide comparative national data for benchmarking, through this report.

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
20
Intr
od
uct
ory
sec
tio
n
Any central database is only as reliable as its component parts. Therefore, data validation is a key issue for all of the people who use the data. This will include surgeons who wish to compare their local populations against a national standard and benchmark their results against their peers, but also the patients and relatives of patients who wish to glean information pertinent to their forthcoming operations. Data could be validated at any one of several points in the process, but there is no substitute for good, regular internal review and validation. Without an individual dedicated to those tasks it is unlikely, if not impossible, to accumulate reliable data. These internal review processes must be subject to external scrutiny, in the same way that all commercial financial accounts are independently audited. The value of this was highlighted in a study conducted with the Nuffield Trust, the Rand Organisation and the California Department of Health, which has been published elsewhere 5, 9.
The long-term success of this database project is dependent on development and co-operation at several levels.
• At a local level each unit should collect the Society’s recommended dataset on all patients who undergo cardiac surgery.
• The data should be collected and maintained in a computer-based system that allows for an electronic export of the data, in a format that the Society has defined in conjunction with the CCAD. The definitions of the data fields and the export specifications are available on both the Society and CCAD websites.
Separate databases kept by individual surgeons are not helpful. Such an approach makes downloading of data and validation more difficult and time consuming and suggests a lack of commitment to integrated audit within the unit.
Ensuring data collection from all units
This has now been achieved. What we have not achieved is consistent quality of data from all units.
This will take a couple of years to resolve. It will be helped by the reminder of the obligation to collect this data in a letter from the Minister of Health, Chairman of the Academy of Medical Royal Colleges and the President of our Society coupled with the inclusion in the Healthcare Commission’s performance ratings of coronary surgery outcomes and thrombolysis data collected for the Royal College of Physicians Myocardial Infarction National Audit Project.
Understanding the value of risk models
A variety of scoring systems are available for measuring variations in severity of illness. Although our specialty leads the way in risk stratification modelling there is increasing recognition that no scoring system will ever be completely predictive of outcome, particularly in high risk patients, for three reasons. Firstly, we do not yet fully understand the basis of the pathophysiological response to surgery or factors influencing an individual patient's physiological reserve. Secondly, some of the major risk factors are not easily quantifiable or definable and are therefore omitted from most scoring systems. A typical example would be the state of the coronary arteries. To quote Parsonnet 11, What may be identified as severe and diffuse disease by one surgeon may be considered relatively routine and non-intimidating by another. Thirdly, some high risk patients may be difficult to characterise and the statistical denominators are relatively small. Nevertheless, both the EuroSCORE and Bayes models provide a useful yardstick when examining mortality in groups of patients. The Parsonnet system, which is still often quoted, is becoming outdated. Current UK practice results in a mortality of around a third of that predicted by the Parsonnet score, but this will decrease with time - in part because practice is improving and in part because the weighting of the preoperative risk variables changes with time. Indeed, the essence of responsible surgical audit is to understand and attack the most influential risk factors in order to reduce their impact. As a result there is accumulating evidence that the influence of previously important risk factors is being reduced towards the mean (see page 211). Taken to a natural conclusion, the currently used variables will be of reduced value for risk stratification in a decade’s time. So we must get smarter. The variables that we measure now (gender, diabetes, hypertension etc.) are simply an expression of our genes, which are our underlying blueprint. Risk stratification will move towards the inclusions of clever molecular and genetic analyses of what influences a patient’s ability to withstand pathophysiological turmoil inflicted by surgical stress.
Effective, conventional risk modelling must be an iterative process; it is this that has prompted some groups to explore alternative, more contemporary and locally appropriate scoring system. We should exercise caution in the construction and interpretation of local risk models and we must understand the balance between an accurate and a useful risk model. An accurate risk model accurately predicts an outcome. At one extreme an accurate local risk model could be constructed using data from a single individual or unit with poor results, reliably predict those results, and then be used to lull the participants into a false sense of security. Although accurate and helpful for predicting local outcome, such a model would have limited value for comparative purposes. A genuinely useful risk model is one that reliably predicts an outcome but is based on, and applicable to, a wider constituency, thereby facilitating reasonable and meaningful

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
21
Intro
du
ctory sectio
n
comparisons between individuals or units. Local risk modelling has value in that it caters for immeasurable local influences, which may not pertain elsewhere. Thus a hierarchy of risk models at different levels, based on single units, several units in a region, along with a nationally based model, should allow accurate local analysis and comparisons while also providing the substrate for dissecting and understanding local variations in the process of surgical care. But again, to be of value, all models should rely on the same definitions for their variables.
In-hospital mortality and quality of care
The definition of quality in surgery is difficult and was first considered by Florence Nightingale in the UK and Ernst Codman in the USA, but both were ahead of their time and were to some extent ostracised for their efforts, which were perceived by some as threatening 12. The issue of how to measure quality remains perplexing, but it is an issue, which we must grasp if we are to retain the respect and confidence of those we seek to treat. The concept of quality in cardiac surgery should encompass the whole hospital journey, from the time the patient walks through the front door for his or her preliminary assessment to the time of discharge from the post surgical outpatient clinic and beyond. Individual surgical performance constitutes only a small, albeit important, part of this process. Surgeon specific mortality data collected by the Society of Cardiothoracic Surgeons clearly indicates that surgeons in the same unit tend to have similar mortalities, highlighting the importance of additional local influences on surgical outcomes. Such influences may include the socio-economic status of the catchment area, severity of cardiac illness, prevalence of co-morbidities, threshold of referral from both the general practitioner and the cardiologist, threshold of acceptance by the surgeons, standards of anaesthesia, surgery, and intensive care, adequacy of facilities and staffing levels, attitude to training, interpersonal relationships between staff, and architectural dispersion within the unit. Any one of these can influence surgical outcome and it is clear that hospital mortality is not necessarily a measure of overall quality but is simply a rough guide to the success of the surgical episode. An appreciation of quality begins when the patient has recovered from the trauma of surgery and asks, was it all worth it? If the answer is yes, then added value can be measured by how long the answer remains yes. A favourable answer to these questions depends as much, if not more, on appropriate referral and acceptance as it does on the technical quality of surgery and postoperative management.
Innovative quality indicators
Mortality is a very coarse measure of outcome and quality. It has the advantage of being easy to understand, measure and validate. But to the patient other outcomes, such as a stroke, may feel as bad or even worse. In order to spot changes or differences in practices analysis of other outcomes may be more sensitive. For example, re-opening for bleeding, insertion of an intra-aortic balloon pump, prolonged ventilation, or a new requirement for dialysis may, in a patient who survives, be deemed to represent a near miss. Measuring a constellation of such outcomes may provide a more sensitive measure of quality of practice. The downside is that early intervention, such as return to theatre for bleeding or insertion of an intra-aortic balloon pump, may be avoided to try and reduce the number of near misses. This issue is discussed by Geoff Berg on pages 260-261.
Public reporting of outcome data
Public reporting of outcome data remains a sensitive issue, but times and attitudes are changing. We must prepare ourselves for the abolition of anonymity and the public reporting of surgeon specific risk-stratified outcome data. Our specialty will lead the way, but only when we have a robust system that can withstand scrutiny. There are many talented individuals within our Society and I am sure that we will be able to develop a system of detailed reporting that is agreeable to surgeons, patients, politicians and the media alike.
In this edition we take a major step forward and cross the Rubicon by publishing a list of surgeons’ names and indicate how many coronary operations they perform and whether their results meet standards agreed by the Society of Cardiothoracic Surgeons and the Department of Health. There will be those within and without the specialty who will be critical for different reasons. They don’t like the concept, they don’t like the methodology or they just think we haven’t gone far enough. We ask those potential detractors to be temperate in the expression of their comment and to bear in mind that the shift toward publishing data on individual surgeons is entirely voluntary and driven by a fragile professional consensus, without any external funding or support. If criticism is voiced in an unconstructive way the delicate balance between anxiety and the desire to be seen to be moving forward will be destabilised and the good will and trust of honest surgeons might be shattered.
This is a complicated area, but the generic issues have been succinctly summarised in a Nuffield Trust publication Dying to know: Public release of information about quality of healthcare. This report concludes with some policy recommendations based on the review of US experience of public disclosure. They were presented to Mr Frank Dobson, the then Secretary of State for Health, in July 1999 and circulated to key policy makers and health advisers in the UK and are outlined below:

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
22
Intr
od
uct
ory
sec
tio
n
1. The intended purpose or purposes of public disclosure should be made clear to all stakeholders.
2. Public disclosure should be seen as an evolutionary process, becoming progressively more sophisticated and comprehensive over time.
3. Public disclosure should be seen as one component of clinical governance.
4. Provider organisations should be a key audience for information about performance.
5. The financial cost of implementing a national policy on public disclosure is likely to be significant and should be considered alongside the benefits.
6. Specific educational initiatives for target audiences should be implemented alongside public disclosure.
7. Health professionals and their representative bodies should be fully involved in the process of public disclosure.
8. Both process and outcome measures of quality should be published.
9. Outcome indicators must be risk adjusted.
10. Public disclosure should be accompanied by a strategy for monitoring the benefits and unintended consequences.
11. Public disclosure should be accompanied by possible explanations for the variations reported.
12. A research and development programme focusing on the generation and evaluation of public performance data should be supported by the NHS R&D Directorate.
Building a national resource
The success of any collaborative venture depends on co-ownership by all parties. This database has grown as a result of the efforts of many contributing surgeons. So the database should be available and useful to those who have contributed. We have therefore agreed a mechanism for data release and publication. Firstly all graphs in this report are downloadable from www.scts.org in Acrobat™ format. Secondly, contributors may seek additional data for presentation or publication. Application forms and rules for data release, determined by the Society’s Executive Committee, are also available on the Society’s website.
The Society of Cardiothoracic Surgeons continues to lead the medical and surgical specialties in the UK in the arena of data collection and outcome measures. This is not just fortuitous; it is the result of the vision, effort, generosity and openness of a large number of surgeons and allied professionals. The production of a report of this nature represents a huge commitment of effort at many levels. Although we have received considerable encouragement from a number of quarters this has stopped short of any form of direct financial assistance and we therefore thank Dendrite Clinical Systems for helping us initiate, develop and sustain this important endeavour.

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
23
Intro
du
ctory sectio
n
The Central Cardiac Audit Database
In the early 1990s the Department of Health was inundated with requests for funding cardiac related audit projects. They therefore established a working group to look at ways cardiac data collection could be co-ordinated between interested parties. This group recommended that the datasets of interested specialist groups should be harmonised and mechanisms for on-line, real time data submission and viewing should be explored. The vision was that patient data would be entered at the time of a procedure and passed down the line in an encrypted format to a Central Cardiac Audit Database (CCAD). The patient’s progress would then be tracked through the database so that additional procedures would be flagged and mortality verified through the Office of National Statistics. This would provide accurate information on re-interventions (which might be performed in another hospital) and mortality allowing a greater understanding of natural disease processes and the impact of interventions. Thus the central server would hold merged data from contributing centres, which would be visible to contributors and provide benchmarking measures. These data would be available to the participating specialist associations for analysis and the production of specialty related reports. A pilot project with six centres was established in 1995 and reported in 2000. Reliable data collection was not achieved, mainly for technical reasons related to data transmission, but a number of lessons were learned.
The project has since been placed under the umbrella of the National Clinical Audit Support Programme within the NHS Information Authority. The National Clinical Audit Support Programme is responsible for promoting clinical audit in cancer and coronary heart disease; it is currently directed by Mr Martin Old.
CCAD has several modules. The congenital heart disease module collects and links data from cardiological and surgical interventions in children with heart disease. The Myocardial Infarction National Audit Project (MINAP) collects data on patients admitted to over 250 trusts in England and is administered on behalf of the Royal College of Physicians by the CCAD. The Society has now agreed to use the CCAD as the main route of data collection from local databases for the National Adult Cardiac Surgical Database in England and Wales.
The CCAD will provide an internationally unique opportunity for understanding the impact of both surgical and non-surgical interventions for acquired heart disease. Its strength lies in the linkage with the Office of National Statistics for long-term mortality tracking which will help us understand who will benefit most from which intervention. Herein lies the added value over and above existing initiatives in this country and abroad.
However, a process of this nature also brings dilemmas. If it is to retain the confidence of the public and the media there must be some element of independence from clinicians. Equally if it is to retain the confidence of clinicians, whose performance may be judged through such a system, it must be guided by clinicians, a principle agreed by the Secretary of State and Chief Medical Officer. Failure to observe this strategy will result in continued and unnecessary duplicate data collection with different groups expressing varying degrees of confidence in different initiatives.
With responsibility for funding shifting to the Healthcare Commission, this principle has been enshrined in the tripartite governance arrangements between the Society, the Commission and the Department of Health (see page 321).
In the meantime, the Society must continue with existing initiatives, which cover the whole of the United Kingdom and Ireland.
Harmonising datasets for the CCAD
There have been three forces at work to encourage us to make a few quite significant changes to the 1996 dataset. These changes were made at a meeting of clinical audit leads at a meeting in Birmingham in September 2002, with a view to implementation from April 2003.
The first has been an international influence. The original dataset was a hybrid of existing datasets in the UK combined with the original dataset compiled by the Society of Thoracic Surgeons (STS) in the US. Since then the United States dataset has been modified based on their extensive experience. The new STS dataset has been adopted widely across the globe. In particular, it has been adopted by the European Association for Cardio-Thoracic Surgery as the European standard. It has also been adopted in Japan, Australasia, Canada and several South American countries. With this in mind we have modified the dataset to increase compatibility with our international colleagues, which will facilitate international comparisons. A key example of this is the development of the EuroSCORE risk stratification system, which is being widely adopted across Europe and which requires pre-operative variables not included in the previous SCTS, or current STS, datasets.

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
24
Intr
od
uct
ory
sec
tio
n
The second influence has been data quality. Whilst the collection of pre-operative data has steadily improved, the collection of post-operative complication and morbidity data has been pretty poor. This is related to the difficulty of collecting information after the event and problems with defining some outcomes. So we are now down to four outcomes: in-hospital death, stroke, new dialysis and re-operations, all of which are not only relevant but relatively easy to define. This should make the data collection much simpler.
The third substantial influence has come from a variety of national NHS information initiatives. The strategic aim within the NHS is to ensure that information can be transferred seamlessly, where properly authorised, across sectors. So, within this strategy the CHD Information Strategy in England aims to integrate a variety of information streams relating to the treatment of heart disease. These streams range from chest pain clinics and myocardial infarction information to waiting times for angiography and outcomes from surgery or angioplasty. In order to make this information useful to clinicians we have had to harmonise our old existing dataset with that of the more recent Myocardial Infarction National Audit Project (MINAP) and that of the British Cardiovascular Intervention Society and also the longstanding UK Heart Valve Registry. Although this will be painful for some centres, in the longer term it will facilitate patient tracking within the CCAD and outcomes analysis across the board.
With greater reliance on electronic data transfer it is increasingly important that uniform clinical and technical standards are enforced across the NHS. In order to enable this, the following principles apply:
• Where possible, existing standards will be adopted. New standards will be developed only where there are none already available, and where there is a defined business need.
• Standards must be implementable, and therefore need to be tested in use before adoption, and must be agreed only where there are measures which can be used to test for conformance.
• Higher authorities will normally take precedence. In other words, the standards set out in the Government Interoperability Framework, and the various e-Government guidelines will be adopted in preference to any health specific standards. Where there is a need for health specific standards, then established international standards will be adopted rather than developing new ones.
To implement these principles four national Standards Boards have been established:
• The Information Standards Board (ISB) will oversee the whole standards process, setting priority areas for standardisation and approving proposals. The ISB is accountable to the National Information Policy Board.
• The Clinical Data Standards Board is responsible for agreeing clinical standards, in areas such as terms (e.g. SNOMED Clinical Terms) and clinical messages. They will be most concerned with the use of standards on the care of individual patients/clients and the human behavioural implications.
• The Technical Standards Board is responsible for agreeing technical standards to be applied.
• The Management Information Standards Board is responsible for agreeing dataset and other performance assessment data requirements. They are most concerned with the organisational and population aspects of the use of standards.
Our new dataset as part of the harmonised CCAD dataset, will, where necessary, be passed through the appropriate approval process, but we will not allow this to hinder the progress of data submission to CCAD.
From the Society’s professional standpoint the international considerations are the most important. We represent England, Scotland, Wales and the whole of Ireland and we therefore look to standardisation of the dataset across all these countries.

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
25
Intro
du
ctory sectio
n
Difficulties in data collection especially in adult congenital heart disease
Mr Leslie Hamilton Consultant Paediatric and Adult Cardiac Surgeon, Freeman Hospital, Newcastle-upon-Tyne
The challenges to collection of high-quality data on cardiac surgical patients are well known. However, patients with congenital heart disease pose particular problems. A major difficulty has been a lack of international agreement on what to call individual congenital heart defects meaning that coding systems could not be developed. From the surgical viewpoint this was finally overcome in 2000 when the proceedings of the International and Nomenclature Database Conferences for Paediatric Cardiac Surgery were published 13.
A further difficulty is that congenital heart defects are in fact not isolated entities but part of a spectrum – for example Tetralogy merges into double outlet right ventricle which merges into transposition with ventricular septal defect. Thus it is sometimes difficult to classify accurately the diagnosis of an individual patient.
Operative survival rates for children undergoing surgery for congenital heart defects in early childhood have improved over the years and we are now seeing an increasing number of adults with congenital heart disease. In addition, some congenital heart defects (e.g.s, atrial septal defect and coarctation) only become apparent in adulthood. Thus the population of adults with congenital heart disease coming for surgery are in two groups – those who have had previous surgery in childhood and require re-operation for a variety of reasons and those adults presenting de novo. The former group are usually dealt with by the paediatric cardiac surgeon who undertook the original surgery, whereas the latter group often have their investigations undertaken by adult cardiologists and are then referred to adult surgeons who in earlier years had training in congenital heart disease.
This dichotomy poses a particular problem in data collection for adults with congenital heart disease. Those undergoing surgery in the adult practice of a paediatric cardiac unit will have their operations recorded in the National Paediatric and Congenital Database (CCAD – Central Cardiac Audit Database). Adult patients undergoing surgery in adult cardiac units (who are not connected to CCAD) have their data recorded in the Society of Cardiothoracic Surgeons National Database. Our challenge for the future is to merge these two databases into a single high-quality source of information on adults undergoing surgery for congenital heart disease.

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
26
Intr
od
uct
ory
sec
tio
n

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
27
Intro
du
ctory sectio
n
Evolving quality improvement initiatives

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
28
Intr
od
uct
ory
sec
tio
n
The National Service Framework for Coronary Heart Disease
As part of the modernisation programme for the National Health Service the Government is developing a series of National Service Frameworks to improve the quality and consistency of services in a number of priority areas, one of which is coronary heart disease. These frameworks will apply specifically to England and Wales.
The National Service Framework for Coronary Heart Disease was published on 6th March 2000 following extensive consultation with professionals involved in the treatment of heart disease. The consultation process was conducted through an external reference group co-chaired by Professor Sir George Alberti (Past-President of the Royal College of Physicians) and Dr Graham Winyard (Director of Health Services, NHS Executive). Ms Elaine Griffiths and Professor Ken Taylor were the cardiac surgical members of the group.
The NSF has set 12 standards for the prevention, diagnosis and treatment of heart disease, which are to be implemented over a ten-year period. Milestones are defined to mark progress with each standard.
The NSF comprises seven chapters related to the twelve standards:
• Reducing heart disease in the population (standards one and two).
• Preventing CHD in high risk patients in primary care (standards three and four).
• Treating heart attacks and other acute coronary syndromes (standards five, six and seven).
• Investigating and treating stable angina (standard eight).
• Revascularisation (standards nine and ten).
• Managing heart failure (standard eleven).
• Cardiac rehabilitation (standard twelve).
Chapter Five specifically addresses coronary revascularisation and the associated mandatory audit requirements.
Audit requirements defined within the National Service Framework
• Annual number of coronary artery bypass operations performed in each centre.
• Annual number of coronary artery bypass operations performed by each trained surgeon.
• Number of trained surgeons per centre.
• Number and % of successful coronary artery bypass operations by lesion type and by operator.
• Risk adjusted number and % of people dying after coronary artery bypass surgery before discharge from hospital by surgeon and by centre (this indicator will be replaced as soon as possible by risk adjusted 30 day and one year mortality rates by trust).
• Number and % of people discharged alive following coronary artery bypass operations prescribed aspirin and/or statin.
Milestones relating to clinical audit
Milestone 1
By October 2000, hospitals should have an effective means for setting hospital-wide clinical standards for common conditions and have an approach for determining whether these standards are being met.
Milestone 3
By April 2002, in every local network of cardiac care hospitals … should have clinical audit data no more than 12 months old that describes the relevant audit criteria.
The Society of Cardiothoracic Surgeons’ agreed dataset was published in Chapter 5 of the NSF and provides a template to allow hospital Trusts to fulfil the audit requirements of the NSF for Coronary Heart Disease.

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
29
Intro
du
ctory sectio
n
Progress against the Bristol Royal Infirmary Inquiry Report
Issues relating to the collection and validation of data, the transformation of data into information and the subsequent public release of that information
In June 1998 the Government announced the establishment of an inquiry into the management and care of children receiving complex cardiac surgery at the Bristol Royal Infirmary between 1984 and 1995. The inquiry was asked not only to reach conclusions about the events at Bristol, but also to make recommendations, drawn from its analysis of those events, which could help secure high quality care across the NHS. The report of this inquiry was published on 18th July 2001.
The report with 198 recommendations was a landmark in the history of the NHS and prompted a detailed response from the Department of Health in January 2002 accompanied by a comprehensive debate in the House of Commons.
The report was extremely wide-ranging covering areas such as how healthcare professionals should interact with patients, health service leadership, competency of professionals, standards and safety of clinical care, public and patient involvement in individual and wider healthcare issues and specific matters relating to the care of children in the NHS. Through the report ran a common thread of improvement through openness and accountability supported by robust and honest information for patients, their families and all involved in running healthcare services.
This thread is highlighted by the following paraphrased recommendations relating to data and information processing which relate to the nature of this report in the future.
145 Clinical audit should be compulsory for all healthcare professionals providing clinical care and the requirement to participate in it should be included as part of the contract of employment.
See our audit guidelines on page 330.
148 The dual system of collecting data in separate administrative and clinical systems is wasteful and anachronistic.
This recommendation poses a dilemma for our specialty. We do not want to lose time or momentum. We are keen to continue developing our data collection and patient information initiatives. The philosophical problem of fragmented data collection is also a very real practical issue, which will be solved technologically in time. In the meantime, we are pleased to be working collaboratively with the NHS Information Authority and the National Clinical Audit Support Programme, on the Central Cardiac Audit Database Project.
See page 23.
149 / 150 Steps should be taken nationally and locally to build the confidence of clinicians in the data recorded in the Patient Administration Systems (PAS) in trusts (which is subsequently aggregated nationally to form the Hospital Episode Statistics).
The Hospital Episode Statistics (HES) database should be supported as a major national resource, which can be used reliably, with care, to undertake the monitoring of a range of healthcare outcomes.
151 Systems for clinical audit and monitoring rely on accurate and complete data. Competent staff trained in clinical coding and supported in their work are required. The status, training and professional qualifications of clinical coding staff should be improved.
Proper validation of data is essential, particularly if it is to be used for personal comparisons. In New York State this is considered the most important component of the whole process (Personal communication; Dr Mark Chassin, Commissioner of Health for New York in the early days of public release of surgeon specific results). This is reflected in the fact that validation and audit of the data takes almost 3 years. It is in the interests of patients, surgeons, politicians and the service as a whole that we take a similar responsible approach to certain aspects of our analyses and public disclosure programme.

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
30
Intr
od
uct
ory
sec
tio
n
152 There should be a system of incentives and penalties to encourage better data quality.
We agree. This is why we are publishing missing data by unit in this report.
153 Indicators of performance should be comprehensible to the public as well as to healthcare professionals.
154 Good IT systems, which facilitate data collection, validation and provide aggregated feedback are required.
As part of the Central Cardiac Audit Database Project we will be developing on-line data collection on cardiac surgery in the UK with real-time feedback of results against national standards to all units and surgeons. No such system exists anywhere else in the world.
27 & 155 Patients must be able to obtain information as to the relative performance of the trust … and consultant units within the trust.
In December 2001 the Department of Health wrote to all consultants in England, with the support of the BMA, to inform them of the intention to use available data to publish performance information at a consultant level in time. The presentation of individual surgeon specific outcome data in cardiac surgery is a sensitive issue, mainly because outcomes are dependent on so many people and influences over which or whom surgical consultants have little or no influence. The key to success is innovative presentation of validated data in such a way that it is meaningful to the public, patients and physicians, is fair to surgeons, does not disenfranchise risky patients and encourages innovative research.
This report goes a considerable way to addressing these recommendations.
The Society of Cardiothoracic Surgeons wholeheartedly supports these recommendations but currently harbours major reservations over the reliability of both our own data and the Hospital Episode Statistics (see pages 277-280), which are not yet fit for this purpose.
We have therefore decided to analyse individual surgeon’s results for coronary surgery and to publish where each individual lies relative to agreed statistical standards. Because of the nature of the data, casemix cannot be taken into account and therefore we have not used a numerical presentation (see pages 264-309).

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
31
Intro
du
ctory sectio
n
The need for data validation Mr Ben Bridgewater, Mr Brian Fabri and Mr Mark Jones Consultant Cardiothoracic Surgeons, Wythenshawe Hospital, Manchester
This edition of the National Adult Cardiac Surgery Database report contains a huge amount of data about procedures, risk factors and outcomes of cardiac surgery. The last year has seen a move towards routine collection of data by all cardiac surgical units in the UK and increasingly in the Republic of Ireland. Apart from a limited project sponsored by the Nuffield Trust the data included in this report has not been subject to systematic, external validation.
The dataset on pages 335-247 has been agreed and recommended by the SCTS as the minimum dataset. The SCTS considers that it is the professional responsibility for units to collect and submit the data to the Central Cardiac Audit Database part of the National Clinical Audit Support Programme (NCASP) sponsored and funded by the Healthcare Commission. It will be the role of the Central Cardiac Audit Database (CCAD) to collect, collate, analyse and disseminate results of submissions. This process will be overseen by a group that has representatives from the SCTS, the Healthcare Commission and the Department of Health (DoH; see page 321). The Healthcare Commission has jurisdiction for audit only in England. However, the principles developed and the tools produced to support audit should be of use for the whole Society of Cardiothoracic Surgeons of Great Britain and Ireland.
One of the concerns about using data about health care activity and outcomes has been that of data quality. For example, studies on data submission in 2000-2001 revealed discrepancies between the total number of isolated first time coronary bypass operations submitted by each unit via the Cardiac Surgical Register or the more detailed Adult Cardiac Surgical Database submission 14 – the average difference between the totals was 4% ranging from 0% to 30% between the units. Although, these discrepancies have improved to a difference of 2.8% the range is still 0-29% due largely to 3 hospitals (see page 51). Other concerns have been expressed about the accuracy of data from Hospital Episode Statistics, which have been used by the DoH and the Dr Foster organisation for benchmarking performance (see page 277).
As well as problems with simply counting the number of operations, analyses in this and the previous copy of the Blue Book have shown high levels of missing data for many of the fields required for accurate risk stratification, which prevents meaningful comparative analyses (see page 234). The advent of analysis and publication of surgeon-specific mortality has highlighted these issues further.
There have been several pieces of work published recently on validation of this type of data. The Nuffield-Rand collaboration 15 looked at the accuracy of submitted and independently validated data at 10 units in the UK. The findings were that overall there was a high correlation between the two, but that the quality of data improved following a period of training. The CCAD paediatric project, which was centrally funded and well resourced, has a rigorous validation system in place and recently published results 16 showing differences between submitted and validated data, with 2.6% of actual cases omitted from unit returns. There were also a significant number of discrepancies between submitted mortality and that detected independently by the Office of National Statistics. Whilst this seems to be a problem for data in paediatric surgery, the discrepancies in mortality for adult cardiac surgery are small with one death under reported in 16,000 operations and one false death reported (CCAD pilot project report, Commission for Health Improvement, Jan 2004)
After numerous discussions by members of the Society in business meetings, the executive, the tripartite oversight group, and meetings of clinical audit leads it is thought imperative to introduce a system of data validation. It is felt that all units should be validated, and the process should be as robust as possible given existing resource. There is a spectrum of views amongst members about how this should be done. The final methodology will be a pragmatic solution determined by cost and practicality. Thanks to input from the Healthcare commission it is hoped that there will be some additional personnel to provide training and support validation from next year.
The following outlines, for discussion, a proposed system of validation that would seem to be achievable in the time course required, within the resource available.
Who will do the validation?
The SCTS already has a quality accreditation program (QAP). This was established by Sam Nashef and is now headed up by Mark Jones (see pages 332-333). The remit of this programme is to look at the data collection systems in place within a unit and to ensure that they have appropriate mechanisms for measuring activity by surgeon, assessing casemix, achieving risk stratification, benchmarking and dealing with poor performance. Any unit can seek quality accreditation, but this is not mandatory. To date 8 units have been through the process (see pages 333). It is envisaged that the existing QAP will undertake the proposed validation visits, which will be mandatory and focus on data collection, completeness and accuracy, rather

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
32
Intr
od
uct
ory
sec
tio
n
than the other governance issues. The visits will be undertaken by a joint team including personnel from the Healthcare commission and surgeons representing the SCTS. What will be validated?
The most important part of generating accurate and complete data is to have good processes in place within a unit. There are a number of different models that have achieved this and it does not seem appropriate for the SCTS to impose a single model on all centres. What all successful models have in common are clinicians with an interest in data collection, dedicated audit personnel, appropriate IT support and a good system of internal validation
The role of the validation visits will be two fold
• To look independently at the data submitted by the unit to CCAD
• To study the systems in place to ensure accurate data collection
The visiting team will be given access to the data submitted by the unit to be visited. This will be available online via the CCAD software. This is currently being developed and it is planned that the software will generate views of data which will be both routinely available online to each unit at all times, and be available to the visiting team for the purposes of a visit.
The software will show:
• Discrepancies between submitted mortality and mortality independently generated from the Office of National Statistics.
• The Incidence of missing data for the various fields required for risk stratification, and a summary figure on data quality, the data quality index.
• Logic checks on the data such as whether the operation date fails to fall between the dates of admission and discharge or if the recorded operation is a valve and grafts and the submitted record fails to contain data for both valve and graft surgery.
• Information about the incidence of the various risk factors compared to pooled national data to help look for evidence of systematic gaming.
The team will then visit the unit, having been previously informed by a questionnaire completed by that unit, to look at the systems in place for internal validation including:
• Personnel and IT support for data collection.
• That database activity is routinely validated against independent records of activity
• That mortality is validated against mortuary records or some other independent source.
• Evidence of feedback mechanisms so that they can be sure each consultant has an opportunity to check their own activity and that discrepancy, where found, are corrected.
There have been numerous debates over recent years about the advisability of independent external checking of database activity against log books and sampling case notes to compare extracted with submitted data. With current levels of resource we will not be able to check activity independently, and whilst some sampling of case notes may be ideal, this is labour intensive and data from the Nuffield Rand study suggest these correlations are generally high. The processes suggested here should help to generate accurate case numbers, surgeon attribution, casemix, and validated mortality.
What will be the outcome of a visit?
The leader of the visiting team will be responsible for producing a report, structured under the various appropriate headings. The report will be sent to the audit lead and clinical director of the unit, the Chief executive of the Trust and the secretary of the SCTS, and will be available on the Healthcare commission website. Reports will also be reviewed at the Tripartite group, but is planned that further action would only be taken in exceptional circumstances.
Who will be validated?
It is proposed that all units in the United Kingdom and Ireland will be visited over a 2-year period. It is proposed that those units that have received the SCTS quality accreditation stamp will be excluded from the first year of visit. It is also felt that those units with a high level of missing data in this addition of the Blue Book should be targeted in the first wave of visits, and the tripartite oversight group will define the criteria.

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
33
Intro
du
ctory sectio
n
Collaboration between the SCTS and the NCEPOD Mr Steven Livesey, Consultant Cardiothoracic Surgeon, Southampton General Hospital
This fifth report of the Society of Cardiothoracic Surgeons National Adult Cardiac Surgical Database paints a detailed picture of cardiothoracic practice in the United Kingdom. However it has become increasingly apparently that numerical data alone do not represent the complete story. The era of publication of outcome data specific to individual cardiac surgeons is almost upon us; the arguments for and against this have been well rehearsed but the momentum is unstoppable and most cardiothoracic surgeons have accepted this as part of practice in the 21st century. Our focus is now on how to use this data, which is freely available, to improve cardiac surgical practice. Professor Tom Treasure 17 (updated version on page 16) outlines some of the pitfalls inherent in interpreting surgical results which are presented as simple mortality statistics, as well as some of the unwarranted consequences of operating in this era – in particular the willingness of surgeons to operate – or not – on high risk cases. These are often the patients who stand to gain the most from successful cardiac surgery and it would be regrettable if such patients were not offered appropriate treatment because a surgeon feared appearing at the wrong end of a league table. It is well recognised that the small proportion of high risk patients is responsible for most of the differences in mortality between surgeons 18.
It has thus become clear that we need to develop beyond our reliance on numbers and statistics to tell the story of an individual’s practice. Only by knowing the details behind a mortality statistic is it possible for cardiac surgeons as a whole to learn from it. I believe surgeons and anaesthetists will generally welcome this as an opportunity to explain some of the factors behind their mortality statistics, be they clinical, environmental or organisational.
Cardiothoracic surgical practice has been subjected to periodic review in the past by the National Confidential Enquiry into Peri-operative Deaths (NCEPOD), as the organisation used to be known. Questionnaires were sent to surgeons and anaesthetists involved in the care of a random sample of patients who had died in the peri-operative period. The Society participated in this process by nominating advisors who reviewed the returned questionnaires and made comment on any unusual or noteworthy circumstances. However, the questionnaires were designed largely for a general surgical practice and although NCEPOD helped stimulate many improvements in the practice of surgeons in general, such as the provision of emergency theatres and were able to highlight the relatively junior level of doctors involved in out-of-hours care, the reports were not particularly helpful to cardiac surgeons who faced a very different set of problems. However we viewed the process as a useful one and are keen to refine the system to better suit cardiac surgical practice.
With this in mind the Society is collaborating with the National Confidential Enquiry into Patient Outcome and Deaths to develop a method for assessing standards in cardiac surgery as they relate to individual patients. The basis for this process will be an in depth study of all patients who died within thirty days of a first time, isolated coronary artery bypass graft operation (this would have given a study cohort of 511 patients in 2000 - 2001). The study will review all aspects of the patient’s care from diagnosis through referral to surgery; to the preoperative and operative care and through postoperative care to local audit processes. Not only will clinical details be reviewed, but any constraints encountered in the patient’s journey through treatment such as adequacy or inadequacy of diagnostic information, the impact of waiting lists, availability of intensive care and high dependency beds etc. will also be examined. Details of patients’ care will be reviewed against an agreed set of standards, which are currently being developed by an expert group.
The main output of the study will be an annual report published with future editions of this report. NCEPOD also plans to produce individual reports on each case and intends to offer feedback to individual surgeons or anaesthetists. NCEPOD would continue to use its agreed process for dealing with cases which give cause for concern and would advise Medical Directors that feedback had been given. No information on individual cases would be passed to the Society of Cardiothoracic Surgeons.
It is planned to roll out the study this year with a study of patients having CABG in the financial year 2004 - 2005. The Society and NCEPOD hope that cardiac surgeons and the public alike will welcome this development, which shows our continuing commitment to transparency and accountability in cardiac surgical practice.

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
34
Intr
od
uct
ory
sec
tio
n
Improving informed consent Mr David Richens Consultant Cardiothoracic Surgeon, Nottingham City Hospital Internal Professional Surgical Advisor to the Ombudsman
The Society of Cardiothoracic Surgeons has begun a new initiative in partnership with the Health Service Ombudsman looking at consent.
The stimulus for this is that issues relating to consent underpin a significant number of the complaints received by the Ombudsman after an adverse outcome following surgery. The basis of such complaints usually relates to two main areas: communication and documentation.
There has been a shift in the legal understanding of informed consent over recent years from a doctor-centred approach to a patient-centred approach. Previously how much information should be given before intervention was judged by the Bolam principle, i.e., it was determined by the doctor. The importance of patient focussed consent emerged in the Bristol Inquiry and in 1998 the GMC published Seeking patient’s consent: the ethical considerations followed by the DoH Reference Guide to Consent for Examination or Treatment in 2001. These booklets introduced the concept of the reasonable patient in order to determine how much information should be supplied.
The collaborative project between the Society and the Health Service Ombudsman described here aims to improve the quality of informed consent in cardiac surgery. The specific area of cardiac surgery is particularly suitable as cardiac surgeons are keen to progress this issue and the technical data contained within this Blue Book lend themselves to the production of speciality specific guidelines on what generic processes should be followed and what specific risks should be quoted to patients considering surgery in order to inform the patient and protect the surgeon.
Preliminary work has already been done to obtain the support and participation of the Healthcare Commission, the DoH and the General Medical Council (GMC). It is intended to produce a standard setting model that can be used to develop similar guidance more widely across all interventional specialities. Such guidance would take full account of, and stand alongside, that which has already been produced by the DoH and the GMC. The guidance will be practical, concise and easily understood by patients and their advisors. This will:
• Help patients understand the risks and benefits of surgery.
• Reduce exposure of clinicians to unnecessary complaints and litigation.
• Provide a framework for decision making in Health Service Ombudsman jurisdiction.
To achieve these outcomes the guidance is intended to be available both as a booklet for distribution and electronically. The guidance will be published by OPHSO and it is anticipated it will have the following components:
• Advice on good communication, including alternatives to treatment.
• Advice on good documentation, including use of the consent form.
• Advice to clinicians on how to behave if an adverse event occurs.
• A Ready Reckoner of surgical risk for the common cardiac surgical procedures.
The participation of, and endorsement by, representative patient groups and legal experts in the development of the guidance will be essential to achieve success. Their early and continued involvement will ensure the good practice is patient focussed and will provide legal assurance. They are being engaged in the development of the product and their endorsement of the final version will be sought.
A first cast of the technical detail has been already been agreed between the Health Service Ombudsman and the Society of Cardiothoracic Surgeons. Following incremental consultation and endorsement with patient groups, legal experts and other agencies such as the Healthcare Commission and the GMC there will be review and sign off by the Society by December 2004. It is then planned to hold a delivery event in the Spring of 2005 attended by all interested parties where there is sign off and launch of the final product.

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
35
Intro
du
ctory sectio
n
Informing patients and the public Mr Colin Hilton Past-President, Society of Cardiothoracic Surgeons of Great Britain and Ireland Prof. Bruce Keogh Co-ordinator, UK Cardiac Surgical Register and National Adult Cardiac Surgical Database
When Dr Foster first published their league tables of cardiac surgical results in the Times we were not happy. We felt threatened – cardiac surgical data was our business! But we soon learned that we were not communicating our endeavours to the public. We lacked that expertise.
So, we joined forces with Dr Foster and set about writing a small book aimed at providing expert information for patients with heart trouble. This book provides expert information in an easily digestible form, by combining our specialist knowledge with Dr Foster’s skills in communication.
When a patient discovers that he or she has heart disease it can feel like a death sentence. Anyone in this situation has a multitude of questions:
What is it that I have got?
What are my chances?
Am I going to die?
What can be done for me?
Who can I turn to?
The ensuing anxiety and fear make it difficult to remember what is told to them. There was a need for information in an easily understood form that the patients could study at their leisure.
It does not answer every question but should act as a guide and help patients in their dealings with their doctors. In the new NHS patients will have choices and we believe that this book will help provide the information upon which they can base their decisions.
Written by:
Ben Bridgewater, Wythenshawe Hospital
Elaine Griffiths, Cardiothoracic Centre, Liverpool
Leslie Hamilton, Freeman Hospital, Newcastle
Colin Hilton, Freeman Hospital, Newcastle
Bruce Keogh, Queen Elizabeth Hospital, Birmingham
Patrick Magee, Barts and the London
James Roxburgh, St Thomas’ Hospital, London
Jane Smith, medical journalist
This guide is available online at: www.Amazon.co.uk

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
36
Intr
od
uct
ory
sec
tio
n
Basic principles of cardiac surgery
The heart can be seen as a mechanical device designed to pump blood around the body. Like any pump that pumps liquid it requires two particular sets of components. Firstly, a series of one-way valves to ensure the blood goes in one direction, and secondly a fuel-supply to provide the energy for pumping. The heart has its own fuel lines, the coronary arteries, which provide oxygen and nutrients for the heart muscle. The heart is, in fact, two pumps. The right side receives blood from the body which it pumps through the lungs, where the blood picks up oxygen, and back to the left side of the heart where the blood now containing new oxygen is then pumped around the whole body. The left side of the heart is stronger because it has to pump blood further.
Valvular heart disease
The heart is a muscle pump, which contains four one-way valves to ensure blood flows in one direction. These valves may become narrowed (stenotic) or leaky (regurgitant) and one or more may need to be repaired or replaced.
The right side of the heart contains two valves: the tricuspid valve where blood enters the main pumping chamber, the right ventricle, and the pulmonary valve where the blood leaves the right ventricle to go to the lungs. Similarly when blood returns from the lungs it enters the main pumping chamber, the left ventricle, through the mitral valve and is then pumped out of the heart through the aortic valve. All this requires energy, which is delivered to the heart muscle in the form of nutrients and oxygen by the coronary arteries.
The aortic valve The mitral valve
Coronary artery disease
The coronary arteries may become narrowed or blocked reducing the blood supply to the heart muscle depriving the heart of oxygen (ischaemia) and giving rise to chest pain (angina). A heart attack (myocardial infarction) occurs when the reduction in oxygen supply is so bad that a portion of heart muscle dies. This may go unnoticed or be so severe that the person dies. Varying degrees of oxygen deprivation may impair the pumping efficiency of the heart. Ejection fraction is a term used to describe how well a heart is functioning. A good heart ejects 50-70% of blood from its main pumping chamber with each beat. Decreasing percentages therefore indicate hearts in worse condition.
Surgical correction of valvular and coronary artery disease
Surgery of the heart is best conducted on a heart that is still and empty of blood. This is effected by artificially pumping blood around the body with a heart lung machine (cardiopulmonary bypass) and stopping the heart either electrically or with a chemical solution for the duration of the operation.

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
37
Intro
du
ctory sectio
n
In a coronary artery bypass graft operation (CABG) a blood vessel is taken from elsewhere in the body, cut to an appropriate length and then one end is plumbed into the diseased coronary artery upstream of the narrowing and the other end downstream of the narrowing, hence the term bypass graft. This restores the blood supply to the area of heart normally supplied by the diseased artery. The number of grafts constructed in any operation depends on the number of diseased coronary arteries. These operations may have to be repeated some time later if the disease in the coronary arteries becomes worse, or if the bypass graft itself becomes narrowed. A repeat operation is more difficult to perform and carries a greater risk to the patient than the initial operation.
Types of bypass grafts
Bypass grafts can be constructed from either arteries or veins. Arteries are blood vessels that convey high-pressure blood, containing oxygen and nutrients, away from the heart to the rest of the body. The aorta, the main artery of the body, is about an inch in diameter. The coronary arteries are the first branches off the aorta, and are about 1-2 mm in diameter. Arteries divide into smaller and smaller branches in order to reach all parts of the body; finally, they become microscopic capillaries.
Once blood has passed through the tissues and organs of the body, the small blood vessels join to form larger blood vessels called veins, which convey the blood, now depleted of oxygen and nutrients, back to the heart. These vessels are of a different structure to arteries, mainly because the blood, after passing through the tiny capillaries in the tissues, is at a fraction of the pressure.
On the whole, each bypass graft requires about 6-7 inches of additional blood vessel. It is easier to find such lengths of vein than it is to find such lengths of artery. Particularly in the leg there is one vein, the long saphenous vein, that runs near the surface of the skin, from ankle to groin, and it is easily removed. For these reasons, the long saphenous vein is the most commonly used blood vessel in the construction of bypass grafts.
There are also two arteries in the chest, which normally provide blood to the breastbone, the left and right internal mammary arteries. These arteries can be detached, cut at one end, swung down and attached to a diseased coronary artery, downstream of the narrowing. However, they are not long enough to reach all of the coronary arteries. Of theses two arteries, it is the left internal mammary artery that is used most often. As it is an artery, it is accustomed to arterial blood pressures, and it is also the same diameter as the coronary arteries. It seldom suffers any narrowing itself. This combination of factors makes it an excellent bypass graft. Therefore, it is generally used to bypass the left anterior descending coronary artery, which is the most important artery of the heart. For the reasons above, the left internal mammary artery also lasts longer than a vein bypass graft.
Veins are most commonly used to bypass the other coronary arteries. However, there is a slowly growing trend towards the use of more arteries for these grafts as well, such as the right internal mammary artery, the radial artery from the arm and another artery that normally provides blood to the stomach.
An internal mammary artery bypass graft A saphenous vein bypass graft

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
38
Intr
od
uct
ory
sec
tio
n
Operations on the heart valves are a little more complicated because the valves are deep inside the heart and therefore the heart must be opened in order to gain access to the valves.
The two most common valves to be replaced or repaired are the aortic and mitral valves. These have very different structures as seen below.
Two common types of aortic valve An open and closed mitral valve
Each of the valves can be either replaced or repaired. A valve can usually be replaced with a bioprosthesis (another animal valve), homograft (a human valve) or most commonly a mechanical valve. Common abbreviations are used for valve replacements: aortic valve, AVR; mitral valve, MVR; tricuspid valve TVR and pulmonary valve PVR.
A typical mechanical heart valve replacement A typical tissue bioprosthetic heart valve
replacement made from a pig’s heart valve
There is no perfect substitute for your own heart valve. There are advantages and disadvantages to each type of replacement. Although mechanical valves last longer blood clot tends to form around the hinge mechanism so patients are required to take warfarin indefinitely to reduce the risk of clot. The dose needs to be carefully controlled: too low and clots form, too high and the patient bleeds too easily. The need for indefinite warfarin is usually eliminated by the use of a bioprosthesis made from natural tissues. But because these tissues are not living the valves wear out more quickly and don’t last as long. Therefore, they are generally reserved for older patients or those who wish to avoid warfarin. Trends in the use of heart valves in the UK can be found pages 65-66.
Despite being simple in concept these are major operations that carry a variable risk to the patient.
Additional details on the different types of heart operations can be found on the US Society of Thoracic Surgeons website at: www.sts.org/section/stspatientinfo

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
39
The UK Cardiac Surgical Register established 1977

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
40
UK
Car
dia
c Su
rgic
al R
egis
ter
The United Kingdom Cardiac Surgical Register (UKCSR)
The UK Cardiac Surgical Register was established in 1977, by Sir Terence English and Dr Alan Bailey, under the auspices of the Society of Cardiothoracic Surgeons of Great Britain and Ireland 10. The Register collects annual cardiac surgical activity and mortality data from each NHS cardiothoracic surgical centre and until recently was divided into three sections:
• Surgery for acquired heart disease with detailed breakdown by operation sub category.
• Surgery for congenital heart disease: discontinued from 2000.
• Surgeon-specific activity and mortality data for index procedures.
A nominated individual within each centre takes responsibility for entering the required data onto a form. This form is then returned to the Secretary of the Society who passes the data to Dr Alan Bailey, an independent physician, for aggregation and analysis. Each member of the Society is then sent a copy of the collated data for their own use. Over the years this data has provided useful information on national trends in cardiac surgery, but it makes no allowance for variations in casemix. The data collected includes:
• All cardiac operations performed in NHS hospitals only.
• All NHS or privately funded operations within NHS hospitals.
The data excludes:
• All patients, NHS or private, operated on within the private sector.
Mortality is defined as mortality on the same admission.
Overall trends in cardiac surgery since 1977
The provision of cardiac surgery has grown steadily in the United Kingdom over the last twenty years, with a plateau over the last few years. This growth is largely confined to surgery for coronary artery disease (ischaemic heart disease). This is the result of growing evidence demonstrating the efficacy of coronary artery surgery for both relief of symptoms and prolongation of life coupled with an increase in resources.
UKCSR: Trends in cardiac surgery (n=646,292)
CABG All valves Congenital
0
5
10
15
20
25
Year
Tho
usa
nd
s o
f op
erat
ion
s

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
41
UK
Card
iac Surg
ical Reg
ister
Professional confidence in the benefits of cardiac surgical procedures has resulted in sicker patients being referred for surgery 19. Despite this, the operative survival for all types of surgery has improved over the years, as illustrated in the following graphs, which demonstrate a steady decrease in operative mortality for coronary and valve surgery from 1977 to the late 1980s, after which the mortality and survival rates have remained relatively constant.
Trends in coronary artery bypass surgery since 1977
Over the last few years in the UK ninety-seven in every hundred patients has survived their coronary bypass operation and the vast majority of these people will have enjoyed a substantial improvement in lifestyle. Many will have had their life prolonged.
UKCSR: Activity and mortality trends for isolated coronary surgery (n=386,745)
Number of operations Mortality rate
In 1996-1997 two large centres did not send in their data to the register. An estimate has been employed using activity data from these centres for the preceding and following years. The adult cardiac surgical data returns are complete for the following years, including 2000-2001.
Between 1997 and 1993 the reporting of this information was based on calendar years (1997 etc.); from 1994 onwards a switch to financial years (1994-1995 etc.) was made in recognition that these data would be useful for managers and commissioners of care.
0
4
8
12
16
20
24
28
Year
Tho
usa
nd
s o
f op
erat
ion
s
0%
1%
2%
3%
4%
5%
6%
7%
Cru
de m
ortality rate

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
42
UK
Car
dia
c Su
rgic
al R
egis
ter
Trends in valve surgery since 1977
Operations for heart valve disease, also produce dramatic improvements, because the heart can pump more effectively; because hearts with valve disease are often sicker and the valves are deep within the heart the operations tend to carry a higher risk than isolated coronary bypass operations. The mortality rates for isolated valve surgery (upper graph) and combined valve and coronary operations (lower graph) have fallen over the last 25 years in the UK.
UKCSR: Activity and mortality trends for isolated heart valve surgery (n=131,899)
Number of operations Mortality rate
UKCSR: Activity and mortality trends for combined heart valve and coronary bypass surgery (n=44,082)
Number of operations Mortality rate
0
1
2
3
4
5
6
7
Year
Tho
usa
nd
s o
f op
erat
ion
s
3%
4%
5%
6%
7%
8%
9%
10%
Cru
de m
ortality rate
0
1
2
3
4
5
Year
Tho
usa
nd
s o
f op
erat
ion
s
7%
9%
11%
13%
15%
17%
Cru
de m
ortality rate

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
43
UK
Card
iac Surg
ical Reg
ister
UKCSR: Crude survival after mitral, aortic and double valve procedures
Mitral Aortic Double
UKCSR: Data for financial year 2003
The preceding graphs represent the first level of analysis, but hide the relatively complex nature of procedural data that is collected. By way of illustration the section for acquired heart disease from the 2002-2003 report for the UK Cardiac Surgical Register is summarised below:
UKCSR: summary data financial year 2003 exluding all congenital heart surgery operations
Number Died % Survival % Mortality
Isolated coronary artery bypass surgery 25,277 495 98.0% 2.0%
Isolated valve surgery 6,125 264 95.7% 4.3%
Combined coronary and valve surgery 3,333 253 92.4% 7.6%
Other operations for ischaemic heart disease 374 62 83.4% 16.6%
Miscellaneous 1,773 233 86.9% 13.1%
Total 36,882 1,307 96.5% 3.5%
In keeping with the Society’s commitment to clinical governance, the Register was extended in 1997-1998 to include activity and outcome data on all individual surgeons for isolated, first-time coronary surgery in adult cardiac surgery. All surgeons submit their results for analysis and comparison with their peers. Patients should be encouraged to discuss risks and benefits of an operation with their surgeon and should not feel awkward about asking their surgeon for his experience and results with any operation. Over the last three years cardiothoracic surgeons have each performed an average of 111 isolated coronary bypass operations per year. The table above indicates that this represents about 70% of a surgeon’s operative activity; so, most surgeons will be performing about 160 major cardiac operations a year. In addition, many also perform major lung surgery. Contrary to popular belief there is no meaningful relationship between the volume of operations performed and the outcome of surgery for individual consultants (see pages 307-308).
82%
84%
86%
88%
90%
92%
94%
96%
98%
Year
Cru
de
surv
ival
rat
e

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
44
UK
Car
dia
c Su
rgic
al R
egis
ter
UKCSR: single open valve operations financial year 2003
WITHOUT CABG WITH CABG
Initial Repeat Initial Repeat
No. Died % No. Died % No. Died. % No. Died %
Valvotomy/repair 9 0 0.0 10 1 10.0 10 1 10.0 2 0 0.0
Mechanical valve 1,466 30 2.0 151 10 6.6 684 42 6.1 33 5 15.2
Bioprosthesis 1,856 78 4.2 114 11 9.6 1,594 112 7.0 47 11 23.4
Homograft 22 1 4.5 8 0 0.0 4 0 0.0 4 2 50.0
Autograft 14 0 0.0 0 NA NA 0 NA NA 0 NA NA
Ao
rtic
Aortic total 3,367 109 3.2 283 22 7.8 2,292 155 6.8 86 18 20.9
Valvotomy/repair 681 9 1.3 40 2 5.0 357 22 6.2 8 0 0.0
Mechanical valve 684 33 4.8 201 20 10.0 251 17 6.8 33 3 9.1
Bioprosthesis 183 14 7.7 33 5 15.2 122 15 12.3 9 0 0.0
Homograft 0 NA NA 0 NA NA 0 NA NA 0 NA NA
Other 1 0 0.0 0 NA NA 0 NA NA 0 NA NA
Mit
ral
Mitral total 1,549 56 3.6 274 27 9.9 730 54 7.4 50 3 6.0
Valvotomy/repair 13 1 7.7 4 1 25.0 3 2 66.7 0 NA NA
Mechanical valve 5 0 0.0 3 1 33.3 0 NA NA 0 NA NA
Bioprosthesis 7 1 14.3 5 1 20.0 0 NA NA 0 NA NA
Other 0 NA NA 3 0 0.0 0 NA NA 0 NA NA Tric
usp
id
Tricuspid total 25 2 8.0 15 3 20.0 3 2 66.7 0 NA NA
Single valve total 4,941 167 3.4% 572 52 9.1 3,025 211 7.0 136 21 15.4
UKCSR: multiple open valve operations financial year 2003
WITHOUT CABG WITH CABG
Initial Repeat Initial Repeat
No. Died % No. Died % No. Died. % No. Died %
Mitral & Aortic 346 15 4.3 78 11 14.1 110 13 11.8 8 1 12.5
Mitral & Tricuspid 99 9 9.1 23 2 8.7 36 5 13.9 7 0 0.0
Aortic & Triscupid 8 1 12.5 4 1 25.0 2 0 0.0 1 0 0.0
Other double valves 7 0 0.0 5 0 0.0 1 0 0.0 1 1 100.0
Double total 460 25 5.4 110 14 12.7 149 18 12.1 17 2 11.8
Triple total 28 4 14.3 8 2 25.0 6 1 16.7 0 NA NA
Other multiple 0 NA NA 6 0 0.0 0 NA NA 0 NA NA
Total multiple 488 29 5.9 124 16 12.9 155 19 12.3 17 2 11.8
Total single 4,941 167 3.4 572 52 9.1 3,025 211 7.0 136 21 15.4
Valve total 5,429 196 3.40 696 68 3.40 3,180 230 3.40 153 23 3.40

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
45
UK
Card
iac Surg
ical Reg
ister
UKCSR: miscellaneous operations for IHD financial year 2003
No. Died Mortality %
Excision infarct/aneurysm 190 16 8.4
Repair post-infarct VSD 49 18 36.7
Other 41 2 4.9
Gra
fts
and
o
ther
p
roce
du
res
Total 280 36 12.9
Excision infarct/aneurysm 29 3 10.3
Repair VSD 65 23 35.4
Pro
ced
ure
s w
ith
ou
t g
raft
s
Total 94 26 27.7

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
46
UK
Car
dia
c Su
rgic
al R
egis
ter
UKCSR: miscellaneous operations for acquired heart disease financial year 2003
No. Died Mortality %
Category 1 i 315 40 12.7
Category 2 ii 27 2 7.4
Category 4 iii 161 31 19.3
Category 5iv 179 13 7.3
Other replacement of total aortic arch 51 11 21.6
Surgery for traumatic aortic transection 21 6 28.6
Other replacement of descending aorta 66 6 9.1
Aortic surgery
Thoraco-abdominal aortic replacement 24 7 29.2
Heart 18 3 16.7
Great vessels 2 0 0.0
Ruptured thoracic aorta 2 0 0.0
Lung 0 NA NA
Other 1 0 0.0
Trauma surgery
Unclassified operations for trauma 18 3 16.7
Heart transplant 128 15 11.7
Heart & lung transplant 19 2 10.5
One lung transplant 57 7 12.3
Transplant surgery
Two lung transplant 61 3 4.9
Myxoma 93 3 3.2 Tumour surgery Other 43 0 0.0
Valve surgery Repair paraprosthetic leak 12 0 0.0
Ventricular 9 5 55.6 Dysrhythmias
Atrial ± valve replacement 75 4 5.3
Pulmonary embolectomy 11 3 27.3
Pericardectomy 64 15 23.4
Other 334 57 17.1
i Aortic root with coronary reimplantation +/- ascending aortic replacement +/- partial aortic arch replacement ii Aortic root with coronary reimplantation and total arch replacement iii Isolated ascending aorta + separate aortic valve resuspension +/- partial aortic arch replacement iv Isolated ascending aorta + separate aortic valve replacement +/- partial aortic arch replacement

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
47
UK
Card
iac Surg
ical Reg
ister
UKCSR: cardiac surgical activity by centre financial year 2003 (excluding congenital heart surgery, pulmonary and oesophageal procedures)
The following section presents information on isolated first-time CABG and isolated first-time aortic valve replacement operations. These data illustrate a number of different points, amongst which:
• There is a wide variation in the number of operations performed at each of the centres:
• 494 performed at Nottingham City Hospital versus
• 1,876 performed at the Papworth Hospital.
• Despite this difference the results for coronary surgery are excellent in both centres with no difference in operative mortality:
• 1.9% at Nottingham City Hospital (99% Cl: 1.0-3.4%).
• 1.9% at Papworth Hospital (99% CI: 1.4-2.7%).
• The proportion of cases that are isolated, first-time CABG operations also varies:
• 48.3% at Glenfield Hospital, Leicester versus
• 78.9% at Morriston Hospital, Wales.
• Again the proportion of cases has no impact on the results of coronary surgery; both Glenfield and Morriston have excellent results:
• 1.1% mortality rate at Glenfield Hospital (99% CI: 0.6-1.9%).
• 1.4% at Morriston Hospital (99% CI: 0.7-2.5%).
• Mortality rates for coronary surgery in different units range from 0.4-3.7%; this compares very favourably with the most recently published data from New York where the range of mortality rates for similarly sized hospitals ranged from 0.3-5.0% 20. Such variations are normal and in keeping with international experience.
These differences are illustrated in the graphs and tables on the following pages.

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
48
UK
Car
dia
c Su
rgic
al R
egis
ter
UKCSR: Activity by centre (n=36,882)
First-time CABG First-time AVR Other
0 250 500 750 1,000 1,250 1,500 1,750 2,000
King Edward VII M idhurst
Nottingham City Hospital
St M ary's Hospital London
M orriston Hospital Swansea
Aberdeen Royal Infirmary
King's College Hospital London
Walsgrave Hospital Coventry
Edinburgh Royal Infirmary
Hammersmith Hospital London
Royal Victoria Hospital Belfast
University Hospital o f Wales Cardiff
Royal Sussex County Hospital
Harefield Hospital M iddlesex
Glasgow Royal Infirmary
John Radcliffe Hospital Oxford
Glasgow Western Infirmary
Southampton General Hospital
Royal Brompton Hospital London
The Heart Hospital London
Victoria Hospital B lackpool
Derriford Hospital P lymouth
Queen Elizabeth Hospital B irmingham
Castle Hill Hospital Hull
Bristo l Royal Infirmary
Northern General Hospital Sheffield
St George's Hospital London
N Staffordshire Royal Infirmary
Glenfield Hospital Leicester
James Cook Uni Hosp'l M iddlesbrough
Wythenshawe Hospital M anchester
Freeman Hospital Newcastle
M anchester Royal Infirmary
Guy's & St Thomas' Hospitals London
Bart’s and the London
Leeds General Infirmary
Cardiothoracic Centre Liverpool
Papworth Hospital
Cen
tre
Number of operations

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
49
UK
Card
iac Surg
ical Reg
ister
UKCSR: Proportions of coronary and aortic valve surgery by centre (n=36,882)
First-time CABG First-time AVR Other
0% 20% 40% 60% 80% 100%
Glenfield Hospital Leicester
Southampton General Hospital
University Hospital o f Wales Cardiff
Papworth Hospital
Harefield Hospital M iddlesex
Walsgrave Hospital Coventry
Queen Elizabeth Hospital B irmingham
Guy's & St Thomas' Hospitals London
Freeman Hospital Newcastle
Royal Victoria Hospital Belfast
Royal Brompton Hospital London
Edinburgh Royal Infirmary
John Radcliffe Hospital Oxford
Nottingham City Hospital
Wythenshawe Hospital M anchester
Derriford Hospital P lymouth
King's College Hospital London
Cardiothoracic Centre Liverpool
Bristo l Royal Infirmary
Hammersmith Hospital London
The Heart Hospital London
Victoria Hospital B lackpool
Bart’s and the London
Northern General Hospital Sheffield
M anchester Royal Infirmary
Royal Sussex County Hospital
St George's Hospital London
James Cook Uni Hosp'l M iddlesbrough
Glasgow Western Infirmary
St M ary's Hospital London
Glasgow Royal Infirmary
Castle Hill Hospital Hull
Leeds General Infirmary
King Edward VII M idhurst
Aberdeen Royal Infirmary
N Staffordshire Royal Infirmary
M orriston Hospital Swansea
Cen
tre
Proportion of operations

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
50
UK
Car
dia
c Su
rgic
al R
egis
ter
UKCSR: results by centre financial year 2003; first-time isolated CABG
CITY HOSPITAL Number Mortality and 99% CI
Survival
Aberdeen Royal Infirmary 508 1.6% (0.6-3.9%) 98.4%
Belfast Royal Victoria Hospital 455 3.1% (1.5-6.1%) 96.9%
Birmingham Queen Elizabeth Hospital 655 2.7% (1.5-5.0%) 97.3%
Blackpool Victoria Hospital 683 1.5% (0.6-3.3%) 98.5%
Brighton Royal Sussex County Hospital 610 3.0% (1.6-5.4%) 97.0%
Bristol Royal Infirmary 736 1.4% (0.6-3.1%) 98.6%
Cardiff University Hospital of Wales 487 1.6% (0.6-4.0%) 98.4%
Coventry Walsgrave Hospital 424 1.9% (0.7-4.6%) 98.1%
Edinburgh Royal Infirmary 471 3.0% (1.4-5.9%) 97.0%
Glasgow Royal Infirmary 660 2.1% (1.0-4.2%) 97.9%
Glasgow Western Infirmary 692 1.7% (0.8-3.6%) 98.3%
Hull Castle Hill Hospital 782 1.3% (0.5-2.9%) 98.7%
Leeds General Infirmary 1,128 0.9% (0.4-2.0%) 99.1%
Leicester Glenfield Hospital 566 0.4% (0.1-1.9%) 99.6%
Liverpool Cardiothoracic Centre 1,155 1.9% (1.1-3.3%) 98.1%
London Guy’s & St Thomas’ Hospitals 809 1.6% (0.8-3.3%) 98.4%
London Hammersmith Hospital 494 2.2% (1.0-4.8%) 97.8%
London Harefield Hospital 501 2.6% (1.2-5.3%) 97.4%
London King's College Hospital 472 1.7% (0.6-4.2%) 98.3%
London The Heart Hospital 679 2.7% (1.4-4.8%) 97.3%
London Royal Brompton Hospital 609 0.7% (0.2-2.3%) 99.3%
London Barts and the London 936 1.3% (0.6-2.7%) 98.7%
London St George's Hospital 815 1.7% (0.8-3.4%) 98.3%
London St Mary's Hospital 446 2.2% (0.9-5.0%) 97.8%
Manchester Royal Infirmary 862 2.3% (1.3-4.1%) 97.7%
Manchester Wythenshawe Hospital 800 1.4% (0.6-3.0%) 98.6%
Middlesbrough James Cook University Hospital 847 1.5% (0.7-3.1%) 98.5%
Midhurst King Edward VII 119 2.5% (0.5-10.0%) 97.5%
Newcastle Freeman Hospital 755 2.4% (1.3-4.4%) 97.6%
Nottingham City Hospital 324 2.8% (1.1-6.4%) 97.2%
Oxford John Radcliffe Hospital 624 3.7% (2.1-6.3%) 96.3%
Papworth Papworth Hospital 1,080 2.0% (1.2-3.5%) 98.0%
Plymouth Derriford Hospital 685 1.8% (0.8-3.7%) 98.2%
Sheffield Northern General Hospital 791 0.9% (0.3-2.3%) 99.1%
Southampton Southampton General Hospital 527 1.9% (0.8-4.3%) 98.1%
Stoke-on-Trent North Staffordshire Royal Infirmary 894 1.9% (1.0-3.6%) 98.1%
Swansea Morriston Hospital 523 0.8% (0.2-2.7%) 99.2%
Total 24,604 1.8% (0.8-3.8%) 98.2%
These results demonstrate the excellent and internationally competitive survival rates for cardiac surgery in the United Kingdom. The variation observed is quite normal and will fluctuate from year to year. These are basic survival rates and do not take into account the age or severity of illness of the patients undergoing surgery because accurate and complete information on all patients in every unit is not yet available.

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
51
UK
Card
iac Surg
ical Reg
ister
UKCSR: results by centre financial years 2001-2003; first-time isolated CABG
CITY HOSPITAL Number Mortality and 99% CI
Survival
Aberdeen Royal Infirmary 1,336 1.5% (0.8-2.7%) 98.5%
Belfast Royal Victoria Hospital 1,391 2.3% (1.4-3.6%) 97.7%
Birmingham Queen Elizabeth Hospital 1,772 3.3% (2.3-4.6%) 96.7%
Blackpool Victoria Hospital 1,944 1.8% (1.2-2.8%) 98.2%
Brighton Royal Sussex County Hospital 1,420 3.0% (2.0-4.4%) 97.0%
Bristol Royal Infirmary 2,276 1.3% (0.8-2.1%) 98.7%
Cardiff University Hospital of Wales 1,337 2.1% (1.3-3.4%) 97.9%
Coventry Walsgrave Hospital 1,794 2.5% (1.7-3.7%) 97.5%
Edinburgh Royal Infirmary 1,723 2.1% (1.3-3.2%) 97.9%
Glasgow Royal Infirmary 1,904 2.6% (1.8-3.8%) 97.4%
Glasgow Western Infirmary 2,155 1.9% (1.3-2.8%) 98.1%
Hull Castle Hill Hospital 1,993 1.9% (1.2-2.9%) 98.1%
Leeds General Infirmary 3,197 1.3% (0.8-1.9%) 98.7%
Leicester Glenfield Hospital 1,966 1.1% (0.6-1.9%) 98.9%
Liverpool Cardiothoracic Centre 3,121 1.8% (1.3-2.5%) 98.2%
London Guy’s & St Thomas’ Hospitals 2,598 1.8% (1.3-2.7%) 98.2%
London Hammersmith Hospital 1,615 2.6% (1.7-3.9%) 97.4%
London Harefield Hospital 1,721 2.1% (1.3-3.2%) 97.9%
London King's College Hospital 1,521 2.2% (1.4-3.4%) 97.8%
London The Heart Hospital 1,637 3.8% (2.7-5.2%) 96.2%
London Royal Brompton Hospital 2,037 1.2% (0.7-2.1%) 98.8%
London Barts and the London 3,078 1.3% (0.9-2.0%) 98.7%
London St George's Hospital 2,222 2.6% (1.8-3.6%) 97.4%
London St Mary's Hospital 1,384 2.8% (1.8-4.3%) 97.2%
Manchester Royal Infirmary 2,371 1.9% (1.3-2.8%) 98.1%
Manchester Wythenshawe Hospital 2,475 1.8% (1.2-2.6%) 98.2%
Middlesbrough James Cook University Hospital 2,440 1.6% (1.0-2.4%) 98.4%
Midhurst King Edward VII 443 2.0% (0.8-4.7%) 98.0%
Newcastle Freeman Hospital 2,400 2.6% (1.9-3.6%) 97.4%
Nottingham City Hospital 1,005 1.9% (1.0-3.4%) 98.1%
Oxford John Radcliffe Hospital 1,874 2.9% (2.1-4.1%) 97.1%
Papworth Papworth Hospital 3,049 1.9% (1.4-2.7%) 98.1%
Plymouth Derriford Hospital 2,193 1.6% (1.1-2.5%) 98.4%
Sheffield Northern General Hospital 2,060 1.2% (0.7-2.0%) 98.8%
Southampton Southampton General Hospital 1,880 1.9% (1.2-2.9%) 98.1%
Stoke-on-Trent North Staffordshire Royal Infirmary 2,143 2.1% (1.4-3.1%) 97.9%
Swansea Morriston Hospital 1,387 1.4% (0.7-2.5%) 98.6%
Total 72,862 2.0% (1.3-3.0%) 98.0%
These results demonstrate the excellent and internationally competitive survival rates for cardiac surgery in the United Kingdom. The variation observed is quite normal and will fluctuate from year to year. These are basic survival rates and do not take into account the age or severity of illness of the patients undergoing surgery because accurate and complete information on all patients in every unit is not yet available.

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
52
UK
Car
dia
c Su
rgic
al R
egis
ter
UKCSR: results by centre financial year 2003; first-time isolated AVR
CITY HOSPITAL Number Mortality and 99% CI
Survival
Aberdeen Royal Infirmary 58 5.2% (1.0-19.4%) 94.8%
Belfast Royal Victoria Hospital 108 2.8% (0.5-11.0%) 97.2%
Birmingham Queen Elizabeth Hospital 133 2.3% (0.4-9.0%) 97.7%
Blackpool Victoria Hospital 55 5.5% (1.0-20.3%) 94.5%
Brighton Royal Sussex County Hospital 86 5.8% (1.7-16.8%) 94.2%
Bristol Royal Infirmary 99 0.0% (0.0-3.0%) 100.0%
Cardiff University Hospital of Wales 69 2.9% (0.3-14.6%) 97.1%
Coventry Walsgrave Hospital 67 3.0% (0.4-15.0%) 97.0%
Edinburgh Royal Infirmary 77 2.6% (0.3-13.2%) 97.4%
Glasgow Royal Infirmary 64 4.7% (0.9-17.8%) 95.3%
Glasgow Western Infirmary 79 3.8% (0.7-14.7%) 96.2%
Hull Castle Hill Hospital 93 1.1% (0.1-9.4%) 98.9%
Leeds General Infirmary 107 3.7% (0.9-12.4%) 96.3%
Leicester Glenfield Hospital 184 1.1% (0.1-5.8%) 98.9%
Liverpool Cardiothoracic Centre 172 1.7% (0.3-7.1%) 98.3%
London Guy’s & St Thomas’ Hospitals 132 4.5% (1.5-12.3%) 95.5%
London Hammersmith Hospital 75 8.0% (2.6-20.7%) 92.0%
London Harefield Hospital 74 8.1% (2.6-21.0%) 91.9%
London King's College Hospital 64 7.8% (2.3-21.9%) 92.2%
London The Heart Hospital 106 2.8% (0.5-11.2%) 97.2%
London Royal Brompton Hospital 95 2.1% (0.3-10.9%) 97.9%
London Barts and the London 100 6.0% (1.9-15.9%) 94.0%
London St George's Hospital 70 5.7% (1.4-18.3%) 94.3%
London St Mary's Hospital 34 5.9% (0.7-27.0%) 94.1%
Manchester Royal Infirmary 87 1.1% (0.1-10.0%) 98.9%
Manchester Wythenshawe Hospital 113 0.9% (0.0-7.8%) 99.1%
Middlesbrough James Cook University Hospital 76 1.3% (0.1-11.3%) 98.7%
Midhurst King Edward VII 13 7.7% (0.3-47.2%) 92.3%
Newcastle Freeman Hospital 109 3.7% (0.9-12.2%) 96.3%
Nottingham City Hospital 34 5.9% (0.7-27.0%) 94.1%
Oxford John Radcliffe Hospital 116 1.7% (0.2-9.0%) 98.3%
Papworth Papworth Hospital 187 5.3% (2.3-11.7%) 94.7%
Plymouth Derriford Hospital 106 2.8% (0.5-11.2%) 97.2%
Sheffield Northern General Hospital 98 2.0% (0.2-10.5%) 98.0%
Southampton Southampton General Hospital 120 0.8% (0.0-7.4%) 99.2%
Stoke-on-Trent North Staffordshire Royal Infirmary 64 3.1% (0.4-15.6%) 96.9%
Swansea Morriston Hospital 43 0.0% (0.0-6.7%) 100.0%
Total 3,367 3.2% (0.6-12.8%) 96.8%
These results demonstrate the excellent and internationally competitive survival rates for cardiac surgery in the United Kingdom. The variation observed is quite normal and will fluctuate from year to year. These are basic survival rates and do not take into account the age or severity of illness of the patients undergoing surgery because accurate and complete information on all patients in every unit is not yet available.

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
53
UK
Card
iac Surg
ical Reg
ister
UKCSR: results by centre financial years 2001-2003; first-time isolated AVR
CITY HOSPITAL Number Mortality and 99% CI
Survival
Aberdeen Royal Infirmary 159 4.4% (1.6-11.1%) 95.6%
Belfast Royal Victoria Hospital 314 3.2% (1.3-7.1%) 96.8%
Birmingham Queen Elizabeth Hospital 267 2.6% (0.9-6.8%) 97.4%
Blackpool Victoria Hospital 160 6.3% (2.7-13.5%) 93.7%
Brighton Royal Sussex County Hospital 191 4.7% (1.9-10.7%) 95.3%
Bristol Royal Infirmary 304 2.3% (0.8-6.0%) 97.7%
Cardiff University Hospital of Wales 202 3.0% (1.0-8.2%) 97.0%
Coventry Walsgrave Hospital 218 3.7% (1.4-8.9%) 96.3%
Edinburgh Royal Infirmary 280 3.2% (1.3-7.4%) 96.8%
Glasgow Royal Infirmary 211 5.2% (2.3-11.0%) 94.8%
Glasgow Western Infirmary 253 2.8% (1.0-7.1%) 97.2%
Hull Castle Hill Hospital 247 2.8% (1.0-7.3%) 97.2%
Leeds General Infirmary 331 4.2% (2.1-8.3%) 95.8%
Leicester Glenfield Hospital 462 1.5% (0.5-4.0%) 98.5%
Liverpool Cardiothoracic Centre 413 1.9% (0.7-4.8%) 98.1%
London Guy’s & St Thomas’ Hospitals 393 3.1% (1.4-6.3%) 96.9%
London Hammersmith Hospital 199 4.0% (1.5-9.7%) 96.0%
London Harefield Hospital 231 6.1% (3.0-11.7%) 93.9%
London King's College Hospital 179 4.5% (1.7-10.7%) 95.5%
London The Heart Hospital 252 5.6% (2.7-10.8%) 94.4%
London Royal Brompton Hospital 294 2.4% (0.8-6.2%) 97.6%
London Barts and the London 299 5.0% (2.5-9.6%) 95.0%
London St George's Hospital 182 7.1% (3.4-14.1%) 92.9%
London St Mary's Hospital 129 3.9% (1.1-11.5%) 96.1%
Manchester Royal Infirmary 216 1.9% (0.4-6.4%) 98.1%
Manchester Wythenshawe Hospital 330 3.0% (1.3-6.7%) 97.0%
Middlesbrough James Cook University Hospital 221 2.3% (0.6-6.9%) 97.7%
Midhurst King Edward VII 52 1.9% (0.1-16.0%) 98.1%
Newcastle Freeman Hospital 311 2.3% (0.8-5.8%) 97.7%
Nottingham City Hospital 117 2.6% (0.5-10.2%) 97.4%
Oxford John Radcliffe Hospital 291 2.7% (1.0-6.7%) 97.3%
Papworth Papworth Hospital 506 4.5% (2.6-7.7%) 95.5%
Plymouth Derriford Hospital 311 1.0% (0.2-4.0%) 99.0%
Sheffield Northern General Hospital 236 1.3% (0.2-5.2%) 98.7%
Southampton Southampton General Hospital 343 1.5% (0.4-4.5%) 98.5%
Stoke-on-Trent North Staffordshire Royal Infirmary 171 2.9% (0.8-8.8%) 97.1%
Swansea Morriston Hospital 135 2.2% (0.4-8.9%) 97.8%
Total 9,410 3.2% (1.2-7.7%) 96.8%
These results demonstrate the excellent and internationally competitive survival rates for cardiac surgery in the United Kingdom. The variation observed is quite normal and will fluctuate from year to year. These are basic survival rates and do not take into account the age or severity of illness of the patients undergoing surgery because accurate and complete information on all patients in every unit is not yet available.

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
54
UK
Car
dia
c Su
rgic
al R
egis
ter
Don’t jump to conclusions
When considering the preceding and following data two issues need to be understood:
• The data is not risk adjusted and therefore does not cater for differences in casemix between hospitals.
• It is conventional to present surgical results as an average over three years so that any random fluctuations from year to year are ironed out. This practice is adopted by New York State, Pennsylvania, New Jersey, the English Department of Health and Dr Foster.
• This means that if there has been a run of high mortality, for whatever reason, it will take two or three years for any improvement to be registered in the averaged three-year results.
The funnel plot below shows the operative mortality for isolated aortic valve replacements at all NHS units in the United Kingdom. The level of observed variation is normal for this sort of crude data.
The principles and mathematics surrounding funnel plots are explained in detail on page 247.
First-time aortic valve replacement: Funnel plot on crude mortality data by centres for financial years 2001-2003(n=9,410)
Overall rate 99 % lower alert 99 % lower alert Centre
99.9% lower alarm 99.9% lower alarm
0%
1%
2%
3%
4%
5%
6%
7%
8%
9%
10%
0 100 200 300 400 500
Number of cases
Cru
de
mo
rtal
ity
rate

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
55
UK
Card
iac Surg
ical Reg
ister
Over a three-year period both the Queen Elizabeth Hospital in Birmingham and the Heart Hospital in London had a mortality for coronary surgery of more than 3%. The Heart Hospital received considerable adverse publicity as a result. In neither case was this difference statistically significant on either basic or risk adjusted mortality data from UK practice as a whole. Both hospitals collect good data on their patients. Neither hospital’s performance was significantly different from that expected given the complexity of cases, but the Heart Hospital results have improved following a move to dedicated premises in 2002.
First-time CABG: Crude mortality data by centre for financial years 2001-2003(n=72,862)
Overall rate 99 % lower alert 99 % lower alert Centre
99.9% lower alarm 99.9% lower alarm
First-time isolated CABG: Observed and predicted mortality rates using a modified EuroSCORE as the predictor; financial years 2001-2003(n=1,797 and n=1,612 respectively)
Queen Elizabeth Hospital - Observed Queen Elizabeth Hospital - Predicted
The Heart Hospital - Observed The Heart Hospital - Predicted
0%
1%
2%
3%
4%
5%
6%
7%
8%
9%
2001 2002 2003
Financial year
Cru
de
mo
rtal
ity
rate
0%
1%
2%
3%
4%
5%
6%
0 500 1,000 1,500 2,000 2,500 3,000
Number of cases
Cru
de
mo
rtal
ity
rate

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
56
UK
Car
dia
c Su
rgic
al R
egis
ter
Comparison of different sources of data on isolated CABG procedures in the financial year 2003
CITY HOSPITAL UK Cardiac Surgical Register
National Adult Cardiac Surgical
Database
Aberdeen Royal Infirmary 512 509
Belfast Royal Victoria Hospital 455 323
Birmingham Queen Elizabeth Hospital 661 661
Blackpool Victoria Hospital 698 695
Brighton Royal Sussex County Hospital 624 623
Bristol Royal Infirmary 755 750
Cardiff University Hospital of Wales 504 503
Coventry Walsgrave Hospital 438 438
Edinburgh Royal Infirmary 481 481
Glasgow Royal Infirmary 674 672
Glasgow Western Infirmary 701 700
Hull Castle Hill Hospital 800 802
Leeds General Infirmary 1,146 925
Leicester Glenfield Hospital 592 574
Liverpool Cardiothoracic Centre 1,187 1,181
London Guy’s & St Thomas’ Hospitals 849 815
London Hammersmith Hospital 517 516
London Harefield Hospital 522 522
London King's College Hospital 485 485
London The Heart Hospital 694 692
London Royal Brompton Hospital 633 633
London Barts and the London 966 907
London St George's Hospital 839 839
London St Mary's Hospital 466 428
Manchester Royal Infirmary 908 908
Manchester Wythenshawe Hospital 809 803
Midhurst King Edward VII 122 0
Middlesbrough James Cook University Hospital 862 772
Newcastle Freeman Hospital 791 785
Nottingham City Hospital 330 327
Oxford John Radcliffe Hospital 635 622
Papworth Papworth Hospital 1,115 1,118
Plymouth Derriford Hospital 706 700
Sheffield Northern General Hospital 805 803
Southampton Southampton General Hospital 562 542
Stoke-on-Trent North Staffordshire Royal Infirmary 905 899
Swansea Morriston Hospital 528 485
Total 25,277 24,438

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
57
UK
Card
iac Surg
ical Reg
ister
Final transition from the UKCSR to the NACSD
Dual data collection systems can be helpful, but are also time consuming. The Society of Cardiothoracic Surgeons agreed in 1996 to replace the United Kingdom Cardiac Surgical Register (UKCSR) with a patient-orientated database that was to become the National Adult Cardiac Surgical Database (NACSD), and anticipated that this would take 10 years. Both systems have been running in tandem for some years, but now that there is reasonable correlation between the two systems we have decided to abandon the UKCSR and focus our attention on developing the database.
The table on the previous page shows that the database captures 96.7% of all coronary surgical activity reported to the UKCSR.
The graph below shows that, in general, fewer cases are recorded in the database than in the UKCSR. There is a striking similarity between the returns to the Register and the Database for most of the centres; only three of the 37 centres have a reporting difference of more than 10% (see previous page; highlighted in brown in the chart).
This close correlation seems to support the strategy of focussing all our future attention on the one system that brings the added value of a wealth of information on individual-patient characteristics, which will allow more and more meaningful analyses.
UKCSR: Isolated CABG activity; UKCSR versus NACSD by centre; financial year 2003
Centre Identical match
10% more than UKCSR 20% more than UKCSR
NACSD 10% less than UKCSR 20% less than UKCSR
Since 1977 we have relied on returns to the UK Cardiac Surgical Register (UKCSR) for tracking national activity. We have now abandoned the UKCSR to focus on our Adult Cardiac Surgical Database (NACSD). This was easier information to collect than that required by our National Database. As a result there is a discrepancy in counts between the two systems, which is marked for about a third of units. This will need early resolution to ensure the integrity of our national data.
300
400
500
600
700
800
900
1,000
1,100
1,200
300 400 500 600 700 800 900 1,000 1,100 1,200
Numbers in the UKCSR
Nu
mb
ers
in t
he
NA
CSD

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
58
UK
Car
dia
c Su
rgic
al R
egis
ter
The graph below details the level of discrepancy for each unit in the UK.
UKCSR: Isolated CABG activity; UKCSR versus NACSD by centre; financial year 2003
Fewer in CSR returns Fewer in NACSD returns
1,146
455
862
966
528
466
849
562
592
635
809
905
791
706
1,187
755
-50 0 50 100 150 200 250
Leeds General Infirmary
Royal Victoria Hospital Belfast
James Cook Uni Hosp'l M iddlesbrough
Bart's and the London
M orriston Hospital Swansea
St M ary's Hospital London
Guy's & St Thomas's Hospitals London
Southampton General Hospital
Glenfield Hospital Leicester
John Radcliffe Hospital Oxford
Wythenshawe Hospital M anchester
N Staffordshire Royal Infirmary
Freeman Hospital Newcastle
Derriford Hospital P lymouth
Cardiothoracic Centre Liverpool
Bristo l Royal Infirmary
Nottingham City Hospital
Victoria Hospital B lackpool
Aberdeen Royal Infirmary
The Heart Hospital London
Northern General Hospital Sheffield
Glasgow Royal Infirmary
University Hospital o f Wales Cardiff
Royal Sussex County Hospital
Hammersmith Hospital London
Glasgow Western Infirmary
Walsgrave Hospital Coventry
St George's Hospital London
Royal Brompton Hospital London
Queen Elizabeth Hospital B irmingham
M anchester Royal Infirmary
King's College Hospital London
Harefield Hospital M iddlesex
Edinburgh Royal Infirmary
Papworth Hospital
Castle Hill Hospital Hull
Cen
tre
Difference between NACSD and UKCSR

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
59
The UK Heart Valve Registry established 1986

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
60
UK
Hea
rt V
alve
Reg
istr
y
The United Kingdom Heart Valve Registry (UKHVR) Prof. Ken Taylor and Ms Maria Edwards
This is the first year that data from the UK Heart Valve Registry have been included in this report. The UK Heart Valve Registry is the oldest national registry in the world providing long-term mortality tracking.
Background
In 1985, discussions took place between the UK Department of Health (then the Department of Health & Social Security) and representatives of the Society of Cardiothoracic Surgeons of Great Britain & Ireland. Agreement was reached to set up a national registry for all artificial heart valves implanted through the National Health Service (NHS) hospitals within the UK. Three important decisions were reached:
1. The Registry would be funded by the Department of Health.
2. Individual patient and clinician confidentiality would be maintained.
3. Participating centres would receive an annual report.
The Registry office was set up in the Cardiac Surgical Unit of the Hammersmith Hospital, London under the direction of Professor Ken Taylor. Each implanting NHS cardiac surgical unit was asked to nominate a link person in that centre who would co-ordinate the centre's data collection, and be the contact person for the central registry office. A Freepost mail service was set up to facilitate transfer of registration forms.
From the outset the emphasis was on achieving maximal co-operation from the UK centres and aim for completeness of patient registration. The data required for the registration form are therefore intentionally brief and simple to obtain. The form comprises patient identification details, surgeon and hospital identification and considerable detail on the implanted valve including each valve’s unique serial number. The Registry began data collection prospectively from 1st January 1986, with no attempt being made to obtain retrospective data. Patients are traced through the Office for National Statistics (England, Scotland & Wales) and the Central Services Agency (Northern Ireland) thus providing unique mortality information.
Although the Registry has historically collected data from NHS cardiac centres only, because of the overriding need to be able to identify all patients at risk after heart valve replacement surgery, the Registry now collects data from some private cardiac surgical units in the UK.
The UK Heart Valve Registry uses a database called the Patient Analysis & Tracking System, from Dendrite Clinical Systems, (PATS) to record patient and valve details. The PATS system is a clinical information management tool, which has allowed the Registry to create its own database based on its requirements. In addition to the storage of information, the PATS system is able to track and analyse patient data over time, conduct analysis of specific demographic or clinical data so that entire populations may be studied, tabulate data, compute averages and calculate patient survival curves. This flexibility and capacity to carry out such tasks is essential as the Registry is increasingly undertaking analyses on this population.
Data collection
In the first ten years of the Heart Valve Registry's existence, the registration form and the method of inputting the data remained unchanged. However, as a result of changing technology and the need to discover more about trends in heart valve disease and replacement surgery, the Registry introduced a modified version of the registration form in 1996.
Although the new form contains more questions, its design is such that it will take less time to complete. A registration form is usually completed at the time of implant by a nominated member of staff at the implanting centre. However, this person’s background is not necessarily clinical. Thus, the form has been designed with this in mind. Whoever completes the form is asked to shade the option(s), which corresponds to the answer or, to write only minimal information in the boxes provided. Each centre has received a set of guidelines on how to complete the form and are actively encouraged to contact the Registry for help should they have any problems or queries about how to do this. All participating centres are sent batches of blank forms upon request and each has its own unique hospital identifier number, known only to the Heart Valve Registry.
The completed forms are input into the database system manually on a daily basis. Regular and stringent validation and maintenance checks are carried out on the database to ensure correctness and completeness of data.

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
61
UK
Heart V
alve Reg
istry
Follow up data
The Registry does not seek to obtain sequential follow-up data on patients apart from the occurrence of death and re-operation.
Re-operation
Re-operation is recorded by a new registration form completed for each valve operation subsequent to the initial registered valve replacement. Although the Registry data lack information on inter-current events not leading to re-operation or death, this limitation was accepted from the planning stage as inevitable in order to maintain simplicity and completeness of data collection, rather than risk reduced co-operation and incomplete data from all UK implanting centres.
Notification of death
All patients entered into the database are flagged for follow-up by either the Office for National Statistics (ONS; patients living in England, Scotland & Wales only) or the Central Services Agency (CSA; patients living in Northern Ireland). Among the many functions of these two agencies is to receive and process the death certificates for all persons dying within the UK.
At the end of every quarter (i.e., last day of March, June, September and December) a list of patient details entered onto the Heart Valve Registry’s PATS database system during the last quarter is sent to the ONS and CSA respectively. This is done in two different ways. The ONS' system is fully computerised and so, the Heart Valve Registry is able to download its last quarter's information onto disk and send this via the postal system. The CSA however, uses the more traditional card system which entails the Heart Valve Registry sending a batch of cards, each containing one patient's demographic details, to the CSA via the postal service.
Both agencies flag each valve replacement patient's details on the national mortality computer and thus, whenever a patient who has been flagged subsequently dies, death certification details are copied back to the Heart Valve Registry. The ONS notifies the Heart Valve Registry of a patient's death by sending to the office a copy of the certified death certificate. The CSA notify the Registry by returning the patient's card stamped with the patient’s date of death. This card is then sent to a second agency in Northern Ireland (Registrar for Deaths) and a request is made for a copy of the certified death certificate.
The link with these agencies therefore provides the Registry with the date and certified cause(s) of death, including date and place of death and post-mortem information (if carried out) for each heart valve replacement patient.
Feedback information
All participating centres can request at any time information about their own centre's performance. This information can be provided either in paper format or on computer disk. A centre may not however, receive any information about another centre's implant history or performance.
An annual report has been produced by the Heart Valve Registry since 1986 under UK Crown Copyright and has been distributed to the Department of Health as well as participating centres. The report provides information on the previous year's performance in terms of number of valves implanted, the sex and age of patients, the valve site and type i.e., mechanical versus bioprosthetic. In addition, it offers some comparative analysis with previous years as well as reports on survival of patients within one calendar year after implant.
An oral report has also been given each year at the annual meeting of the UK Society of Cardiothoracic Surgeons.

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
62
UK
Hea
rt V
alve
Reg
istr
y
Publication
The contribution of the UK Heart Valve Registry data to the knowledge of valve surgery is being increasingly recognised in scientific presentations and publications. Thus, the database is a unique information resource for patient demographics, short and long-term outcomes and heart valve performance.
The UK Heart Valve Registry data are increasingly being used extensively by numerous authors of papers; book chapters have also cited UK Heart Valve Registry data with suitable acknowledgment.
Research output from the HVR
1. UK Heart Valve Registry Annual Report - each year since 1986 Crown Copyright.
2. Annual Report to the Society of Cardiothoracic Surgeons of Great Britain and Ireland - each year since 1986.
3. Taylor KM. The clinical aspects of heart valve replacements. Engineering in medicine 1987; 16: 63-65.
4. Taylor KM. Acute failure of artificial heart valves. BMJ (leading article) 1988; 297:996-7.
5. Taylor KM. The UK Heart Valve Registry in Current topics in heart valve surgery 1990; ed. WH Bain ICR London.
6. Taylor KM. Heart valve surgery in the UK: present practice and future trends. Brit. Heart J. 1991; 66: 335-6.
7. Taylor KM, Gray SA, Livingstone S, Brannan JJ. The UK Heart Valve Registry. J. Heart Valve Dis 1992; 1: 152-59.
8. Taylor KM. Fatigue and wear in prosthetic heart valves - a surgeon's perspective. J. Heart Valve Dis 1996; 5 (supp): 57-8.
9. Taylor KM. Overview: A cardiac surgeon’s perspective. J of Heart Valve Dis 1996; 5 (supp I) S7-S8.
10. Azimakopoulos G, Edwards MB, Brannan JJ, Taylor KM. Survival and cause of death after mitral valve replacement in patients aged 80 years and over: Collective results from the UK Heart Valve Registry. Eur J of Cardiothoracic Surg 1996; 11:922-928.
11. Taylor KM. The United Kingdom Heart Valve Registry: the first 10 years. Heart (editorial) 1997; 77 (4): 295-6.
12. Asimakopoulos G, Edwards MB, Taylor KM. Aortic valve replacement in patients aged 80 years and over: survival and cause of death based on 1100 cases. Collective results from the UK Heart Valve Registry. Circulation 1997; 96 (10): 3403-08.
13. Edwards MB, Ratnatunga CP, Dore CJ and Taylor KM. Operative mortality and long term survival following surgery for prosthetic endocarditis: A study from the UK Heart Valve Registry Eur J Cardiothoracic Surg 1998; 14: 156-164.
14. Ratnatunga CP, Edwards MB, Dore CJ and Taylor KM. Tricuspid Valve Replacement: UK Heart Valve Registry. Mid Term Results. Comparative Study between mechanical and biological prostheses. Annals of Thoracic Surgery 1998; 66: 1940-1947.
15. Edwards MB. Prosthetic heart valves implanted in the United Kingdom 1986 to 1997. Second edition. UK Heart Valve Registry, London 1998.
16. Weerasinghe A, Edwards MB, Taylor KM. The First Redo Heart Valve Replacement: 10 Year Analysis. Circulation 1999; 99: 655-658.
17. Edwards MB, Taylor KM. A profile of valve replacement in the UK (1986-1997): A study from the UK Heart Valve Registry. J Heart Valve Dis 1999; 8: 697-701.
18. Edwards MB. UK trends in heart valve replacement surgery. Action for Biomaterials 2000; 4: 16.
19. Edwards MB, Taylor KM. 25 years of heart valve replacements: The UK experience. A guide to types, models and MRI safety. UK Heart Valve Registry, London, 2000.
20. Edwards MB, Taylor KM, Shellock FG. Prosthetic heart valves: Evaluation of magnetic field interactions, heating and artifacts at 1.5 Tesla. JMRI 2000; 12: 363-369.

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
63
UK
Heart V
alve Reg
istry
21. Edwards MB. UK trends in heart valve replacement surgery. Action for Biomaterials 2000; 4: 16.
22. Edwards MB, Taylor KM. Cohort survery of heart valve replacement patients: does the valve card scheme have room for improvement ? BMJ 2001; 323: 429-430.
23. Edwards MB, Ordidge RJ, Thomas DL, Hand JW, Taylor KM. Translational and rotational forces on heart valves subjected to ex vivo testing to a 4.7 T MR system. J Magn Reson Imaging 2002; 16: 653-659.
24. Edwards MB, Taylor KM. Outcomes of valvular surgery in nonagenarians. Ann Thorac Surg 2003; 75: 830-834.
25. Edwards MB, Taylor KM. Differences between 30-day and 365-day mortality following heart valve replacement surgery. Ann Thorac Surg 2003; 76: 482-486.
26. Edwards MB, Taylor KM. Outcomes of valvular surgery in nonagenarians (response to letter - in press) Ann Thorac Surg 2004.
27. JPA Puvimanasinghe, JJM Takkenberg, MJC Eijkemans, MB Edwards, EW Steyerberg LA van Herwerden, KM Taylor, GL Grunkemeier, JDF Habbema and AJJC Bogers. A comparison of prognosis after aortic valve replacement with a mechanical valve or bioprosthesis using microsimulation. (in press) Heart 2004.
28. Edwards MB, Ordidge RJ, Hand JW, Taylor KM, Young IR. Assessment of magnetic field (4.7 T) induced forces on prosthetic heart valves and annuloplasty rings (in press).
29. Edwards MB. A guide to types, models and MRI safety of heart valves and annuloplasty rings implanted in the United Kingdom 1974–2003. United Kingdom Heart Valve Registry, London, 2004.

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
64
UK
Hea
rt V
alve
Reg
istr
y
UKHVR: Age trends
>70 year-olds Average age
Between 1986 and 2001 the proportion of patients over seventy years old has risen from 12.4 to 41.7%. This has practical implications because patients over the age of seventy tend to receive a different type of artificial valve than younger patients.
There are two different types of valve that are commonly inserted surgically:
Mechanical valves are made of entirely artificial material; because of this there is a tendency for blood to form clots on the mechanism. These clots may inhibit the valve mechanism preventing the valve from working properly, or, very rarely, they may break off and travel to the brain, sometimes causing a stroke. To prevent this happening, patients with an artificial valve need to take a drug called warfarin, which prevents the blood forming clots easily.
For patients who may not want to take warfarin, or the elderly where warfarin is better avoided if possible a different type of valve is commonly used.
Biological or tissue valves are made from animal material. Because they are made from natural tissue blood clot forming on the valve is much less of a problem and warfarin is not required, except sometimes for a short period after surgery. This type of valve does not tend to last as long as mechanical valves. Therefore they tend to be used more commonly in elderly patients over the age of seventy, who will put less stress on the valve and in whom warfarin is less desirable (because older people bruise and bleed more easily than younger people).
Over the years the technology for preserving and making tissue valves improved and some surgeons feel that reserving these valves for patients over the age of 70 is conservative. Many surgeons, particularly in America, are now using 65 as the cut off age.
10%
14%
18%
22%
26%
30%
34%
38%
42%
46%19
86
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
Financial year
Pro
po
rtio
n o
f pat
ien
ts o
ver
the
age
of 7
0 y
ears
58
59
60
61
62
63
64
65
66
67
Averag
e age / years

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
65
UK
Heart V
alve Reg
istry
UKHVR: Trends in implants used over time by age group (n=79,662)
≤70 years old; mechanical implant ≤70 years old; biological implant
>70 years old; mechanical implant >70 years old; biological implant
The increasing confidence in the newer tissue valves is reflected in the slowly increasing proportion of younger and older patients receiving biological implants.
UKHVR: Type of implant (n=94,553)
Mechanical Bioprosthesis Homograft
The increased confidence in biological valves, coupled with the increasing age of the patient population, is reflected in the increasing proportion of biological valves overall.
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
Financial year
Po
rpo
rtio
n o
f op
erat
ion
sw
ith
in a
ge
bra
cket
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
Financial year
Pro
po
rtio
n o
f im
pla
nts

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
66
UK
Hea
rt V
alve
Reg
istr
y
UKHVR: Type of mechanical implant (n=32,354)
Porcine Pericardial
The improved technology for making and preserving different types of biological valves is reflected in the increasing usage of pericardial valves made from the heart lining of cattle. Porcine valves are generally natural pig valves with artificial supports. Both valves work very well.
UKHVR: Type of mechanical implant (n=61,621)
Single leaflet Bileaflet Ball
There are many different types of mechanical heart valves, which fall into three broad categories: single-leaflet, bileaflet or ball-and-cage. The bileaflet valves are now the most commonly used valves in the UK.
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
Financial year
Po
rpo
rtio
n o
fb
iolo
gic
al im
pla
nts
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
Financial year
Pro
po
rtio
n o
fm
ech
anic
al im
pla
nts

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
67
UK
Heart V
alve Reg
istry
UKHVR: Type of valves replaced or repaired (n=87,343)
Aortic Mitral Tricuspid
There has been a slow but steady increase in the proportion of aortic valve surgery over the last 15 years, related largely to degenerative aortic valve narrowing associated with age.
UKHVR: Number of valves replaced or repaired (n=87,343)
Single Double Triple
The proportion of patients requiring double or triple valve replacement continues to fall, presumably as a result of better public health and the elimination of rheumatic disease in childhood which affects the heart valves later in life.
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%19
86
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
Financial year
Pro
po
rtio
n o
f op
erat
ion
s
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
Financial year
Pro
po
rtio
n o
f op
erat
ion
s

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
68
UK
Hea
rt V
alve
Reg
istr
y
UKHVR: Age trends by valve site
Aortic Mitral
The proportion of patients over the age of seventy having aortic valve surgery is slowly climbing, while the proportion undergoing mitral valve surgery is falling. This is possibly due to earlier intervention in mitral valve patients with increasing confidence in mitral valve repair techniques.
UKHVR: Long-term survival by site of valve replaced or repaired
First-time aortic valve First-time mitral valve
Repeat aortic valve Repeat mitral valve
18%
20%
22%
24%
26%
28%
30%
32%
34%19
86
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
Financial year
Pro
po
rtio
n o
f mit
ral v
alve
pat
ien
ts a
ged
ove
r 7
0 y
ears
66%
68%
70%
72%
74%
76%
78%
80%
82%
Pro
po
rtion
of ao
rtic valvep
atients ag
ed o
ver 70
years
0%
5%
10%
15%
20%
25%
30%
35%
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
Financial year
30
-day
mo
rtal
ity
rate

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
69
UK
Heart V
alve Reg
istry
UKHVR: Long-term survival by site of valve replaced or repaired
Aortic Mitral Tricuspid
Operative mortality for mitral valve surgery is generally higher than for aortic valve surgery, but after the early period long-term survival is similar.
UKHVR: Long-term survival by number of valves replaced or repaired
Single Double
20%
30%
40%
50%
60%
70%
80%
90%
100%
0 2 4 6 8 10 12 14 16 18
Time after surgery / years
Surv
ival
rat
e
30%
40%
50%
60%
70%
80%
90%
100%
0 2 4 6 8 10 12 14 16 18
Time after operation / years
Surv
ival
rat
e

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
70
UK
Hea
rt V
alve
Reg
istr
y
UKHVR: Long-term survival by gender
Male Female
Although the early operative mortality for women is slightly higher, the long-term survival for men and women is the same.
UKHVR: Long-term survival by age
≤69 years old >69 years old
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
0 2 4 6 8 10 12 14 16 18
Time after surgery / years
Surv
ival
rat
e
30%
40%
50%
60%
70%
80%
90%
100%
0 2 4 6 8 10 12 14 16 18
Time after surgery / years
Surv
ival
rat
e

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
71
UK
Heart V
alve Reg
istry
The UK National Adult Cardiac Surgical Database
established 1996

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
72
NA
CSD
- In
tro
du
cto
ry
The National Adult Cardiac Surgical Database (NACSD)
Introduction to the database
The Cardiac Surgical Register described in the preceding pages is unique in that it has provided activity and outcome data for UK cardiac surgery for over a quarter of a century. Although a national register of procedures is essential there is a growing demand to increase the breadth of data collected in order to form a patient orientated rather than a procedure orientated database. The driving force for this development has derived from the shift towards evidence-based practice, the need for more information for patients and their families in the light of changing attitudes to informed consent and increasing interest in understanding which patients will require which resources and matching patients to available resources. Therefore, it seems natural to progress from a procedure-orientated database to a more comprehensive patient-orientated database. Almost a third of the population die from coronary artery disease and cardiac surgery offers the potential for considerable symptomatic and prognostic benefit to a large number of people. Healthcare professionals and purchasers are becoming increasingly interested in understanding who will benefit the most and at what cost in terms of both risk (mortality and complications) and resources. Therefore, a simple bean counting exercise is no longer enough. The Society of Cardiothoracic Surgeons is encouraging the collection of comprehensive and standardised data across the UK and Ireland to enable a greater understanding of national practice.
Contributing centres and trusts
On 31st March 2003 there were 39 NHS hospitals in 36 trusts undertaking adult cardiac surgery in the United Kingdom (see next page). Of these 38 (100%) have contributed data of varying quality to the National Database. All Scottish centres also contribute to the Scottish National Cardiac Surgery Register, which has a slightly different dataset, but is robust and validated (see page 15). We are also pleased to include the data from St James’s Hospital in Dublin and we anticipate that additional Irish hospitals will be in a position to submit data in the near future. In addition, data of varying quality from 7 private hospitals are also included.
Growth of the National Adult Cardiac Surgical Database (n=211,033)
Procedures Centres
0
20,000
40,000
60,000
80,000
100,000
120,000
140,000
160,000
180,000
200,000
1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003
Financial year
Cu
mu
lati
uve
nu
mb
er o
f p
roce
du
res
0
5
10
15
20
25
30
35
40
45
50
Nu
mb
er of cen
tres

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
73
NA
CSD
- Intro
du
ctory
Contributing centres
City Hospital Contributor Total number of procedures submitted
Aberdeen Royal Infirmary Yes 2,340
Belfast Royal Victoria Hospital Yes 5,730
Birmingham Queen Elizabeth Hospital Yes 6,370
Blackpool Victoria Hospital Yes 1,304
Brighton Royal Sussex County Hospital Yes 2,603
Bristol Royal Infirmary Yes 7,900
Cardiff University Hospital of Wales Yes 4092
Coventry Walsgrave Hospital Yes 9,026
Dublin St James’s Hospital Yes 1,793
Edinburgh Royal Infirmary Yes 731
Glasgow Golden Jubilee Hospital Yes 246
Glasgow Royal Infirmary Yes 3,679
Glasgow Western Infirmary Yes 5,142
Hull Castle Hill Hospital Yes 7,009
Leeds General Infirmary Yes 10,946
Leicester Glenfield Hospital Yes 6,067
Liverpool Cardiothoracic Centre Yes 9,208
London Guy’s & St Thomas’ Hospitals Yes 12,899
London Hammersmith Hospital Yes 2,415
London Harefield Hospital Yes 5,789
London King's College Hospital Yes 10,239
London The Heart Hospital Yes 4,741
London Royal Brompton Hospital Yes 5,557
London Barts and the London Yes 4,902
London St George's Hospital Yes 11,392
London St Mary's Hospital Yes 569
Manchester Royal Infirmary Yes 6,059
Manchester Wythenshawe Hospital Yes 6,840
Middlesbrough James Cook University Hospital Yes 7,220
Newcastle Freeman Hospital Yes 7,859
Nottingham City Hospital Yes 3,418
Oxford John Radcliffe Hospital Yes 1,983
Papworth Papworth Hospital Yes 11,569
Plymouth Derriford Hospital Yes 2,215
Sheffield Northern General Hospital Yes 2072
Southampton Southampton General Hospital Yes 4,563
Stoke-on-Trent North Staffordshire Royal Infirmary Yes 7,711
Swansea Morriston Hospital Yes 3,382
Private hospital groups
BUPA 5 Hospitals Yes 854
HCA International 2 Hospitals Yes 2,599
Total 47 hospitals 211,033

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
74
NA
CSD
- In
tro
du
cto
ry
Data harvest, import, merge and analysis methodology
Each cardiothoracic surgery centre across England, Scotland, Wales, Northern Ireland and in the Irish Republic was invited to submit a data file of consecutive patient records to the National Adult Cardiac Surgical Database either in the format of the Society of Cardiothoracic Surgeons’ (SCTS) minimum dataset or as close to that format as is possible. For the purpose of confidentiality and compliance with the Data Protection Act, data files were anonymised for surgeon and patient identifiers as part of the process. These files were then collated on behalf of the SCTS at Dendrite’s head office and were loaded onto a secure server.
The schematic on the opposite page shows the current data-flow paths.
Where the source data files originated from hospital based Dendrite database systems (32 hospitals) the files were simply copied across onto the central server as discrete individual registries. For those hospitals using either an alternative proprietary or generic third-party database systems (15 hospitals) the data files were loaded into an Import Manager Module program that converted the files to a compatible format for merging into the central database. The process of importing data involved careful, individually tailored mapping of the data files on a field-by-field basis. This process created a series of interim registries as shown in the schematic on the facing page. Each interim registry represented an exact copy of the source data files, but now all on one standard software platform.
Before final merging the data a further mapping process was undertaken. This involved corresponding data from the interim registries across a series of identical final source registries. Before this step was undertaken a series of data logic and data validation checks were made to ensure that erroneous data (e.g. negative lengths of stays) were identified and where possible corrected or eliminated. Once these checks were completed, the subsequent correspondence mapping process ensured that the data structure across each of the final source registries was harmonised and uniform so that the data could then be merged and analysed easily. The merging process is essentially an automated process and converted the data into one huge data-file of over 210,000 complete patient records (approximately 40,000,000 data items) ready for analysis.
Data merging, manipulation and analyses were performed using in-house Dendrite software, the Patient Analysis and Tracking System software, Microsoft Excel™ and Crystal Decisions’ Crystal Reports™ using an object link to the Dendrite software. Where possible, data from all entries and all hospitals were used for the basic aggregate data analysis and inter-hospital comparisons.
For the purpose of demonstrating the capability for long-term follow-up (see pages 310-319) a data file was sent directly from one centre to the Central Cardiac Audit Database (CCAD) for long-term mortality tracking by the Office of National Statistics (ONS).
It is proposed, in the future, that once a successful pilot programme for the CCAD project has been completed, to then link all English and Welsh cardiothoracic surgery centres directly to CCAD. This means that the SCTS National Adult Cardiac Surgical Database will eventually take data feeds from CCAD (for all English and Welsh centres) together with follow up data. The relationship between CCAD and units in Scotland, Northern Ireland and the Republic of Ireland remains unclear.
The diagram opposite shows how data for this report were collected and merged. In the future input from English and Welsh centres will feed directly into CCAD.

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
75
NA
CSD
- Intro
du
ctory
Schematic to show the current data-flow paths for the National Adult Cardiac Surgical Database

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
76
NA
CSD
- In
tro
du
cto
ry
Data collection facilities by centre as at June 2004
City Hospital Networked, multi-user collection system in theatres
Computer system
Dedicated cardiac surgical
data-manager
Aberdeen Royal Infirmary No In-house Part-time
Belfast Royal Victoria Hospital Yes Dendrite No
Birmingham Queen Elizabeth Hospital Yes Dendrite Yes
Blackpool Victoria Hospital Yes Dendrite Yes
Brighton Royal Sussex County Hospital Yes Dendrite Yes
Bristol Royal Infirmary Yes Dendrite Yes
Cardiff University Hospital of Wales Yes Dendrite Yes
Cork Cork University Hospital Yes Dendrite Yes
Coventry Walsgrave Hospital Yes Dendrite Yes
Dublin Mater Misericordiae Yes Dendrite Yes
Dublin St James’s Hospital Yes Dendrite Yes
Edinburgh Royal Infirmary No In-house Yes
Glasgow Royal Infirmary Yes In-house Part-time
Glasgow Western Infirmary Yes SCAN Yes
Hull Castle Hill Hospital Yes Dendrite Yes
Leeds General Infirmary Yes Dendrite Shared
Leicester Glenfield Hospital Yes Dendrite Yes
Liverpool Cardiothoracic Centre Yes In-house Yes
Guy’s & St Thomas’ Hospitals
Guy's Hospital Yes No
London
St Thomas’ Hospital Yes
Tomcat & Dendrite No
London Hammersmith Hospital Yes Dendrite Shared
London King's College Hospital Yes Dendrite Yes
London The Heart Hospital Yes Dendrite Yes
Royal Brompton & Harefield NHS Trust
Harefield Hospital Yes Dendrite Yes
London
Royal Brompton Hospital Yes Dendrite Yes
London Barts and the London Yes Dendrite Yes
London St George's Hospital Yes Dendrite Yes
London St Mary's Hospital No In-house No
Manchester Royal Infirmary Yes In-house Yes
Manchester Wythenshawe Hospital Yes Datacam Yes
Middlesbrough James Cook University Hospital Yes In-house Yes
Newcastle Freeman Hospital Yes Dendrite Yes
Nottingham City Hospital Yes SUMMIT Yes
Oxford John Radcliffe Hospital Yes Datacam Shared
Papworth Papworth Hospital Yes In-house Yes
Plymouth Derriford Hospital Yes iSoft Yes
Sheffield Northern General Hospital Yes CIMS Yes
Southampton Southampton General Hospital Yes In-house Yes
Stoke-on-Trent North Staffordshire Royal Infirmary Yes Dendrite Yes
Swansea Morriston Hospital Yes Dendrite No

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
77
NA
CSD
– Gen
eral ou
tcom
es
General cardiac surgical outcomes
Mortality rate by procedure
The graphs below show improving hospital survival for all main types of surgery over the last few years.
Crude survival and mortality by procedure (n=181,677)
Isolated CABG All CABG Isolated valve CABG & valve
82%
84%
86%
88%
90%
92%
94%
96%
98%
100%
1996 1997 1998 1999 2000 2001 2002 2003
Financial year
Cru
de
surv
ival
rat
e
0%
2%
4%
6%
8%
10%
12%
1996 1997 1998 1999 2000 2001 2002 2003
Financial year
Cru
de
mo
rtal
ity
rate

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
78
NA
CSD
– G
ener
al o
utc
om
es
Post-operative stay
The proportion of patients staying in hospital for longer than two weeks following major heart surgery has slowly increased over the last decade. There will be many reasons for this, but an increasing elderly patient population and an increasing proportion of combined valve and coronary operations will be two significant reasons.
Post-operative stay by financial year (n=184,397)
<8 days 8-14 days 15-21 days >21 days
Post-operative stay by procedure for financial year 2003 (n=36,312)
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
1994 1995 1996 1997 1998 1999 2000 2001 2002 2003
Financial year
Per
cen
tag
e o
f pat
ien
ts
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
CABG, Valve & Other
Other
Valve & Other
CABG & Other
CABG & Valve
Valve alone
CABG alone
Pro
ced
ure
Proportion of patients

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
79
NA
CSD
– Valve su
rgery
Valve surgery
General
Although the average age of patients undergoing aortic valve surgery remained relatively stable over the last 7 years, there is a suggestion of the beginnings of an upward trend in patients’ age over the last 3-4 years. The average age of patients having combined aortic valve and coronary operations is considerably higher because both aortic valve disease and coronary artery disease are commoner in older patients; the average age for this group of patients has also increased in the period since the financial year 2000.
The survival of patients undergoing isolated aortic valve replacement is good, with over 96% of patients leaving hospital alive. Even more encouraging is the improvement in survival for patients undergoing combined aortic valve replacement and coronary surgery, who tend to be both older and sicker.
In the box and whisker plots the patients’ stay is considered in percentiles. The box represents the length-of-stay for the middle-half of all patients (25th-75th centiles) e.g., the box for patients undergoing aortic valve surgery in 1994 covers stays of 6-10 days. The whiskers indicate the length-of-stay range for the middle 80% (10th-90th centiles): in the financial year 2003 90% of all aortic valve surgery patients were discharged by 18 days. The median length-of-stay is the same for patients undergoing both isolated aortic valve and aortic valve surgery in combination with coronary surgery, but the spread is much greater when combined aortic valve and coronary bypass surgery is required.
Mitral valve disease generally has a greater deleterious impact on the heart and general health than aortic valve disease. In the past, rheumatic fever in childhood predisposed to mitral valve disease in adulthood; this was the main reason for mitral valve surgery. Since the advent of effective antibiotics, rheumatic fever has become very rare in the UK and now age-related degeneration of the mitral valve is becoming the predominant reason for surgery.
The two conditions are generally amenable to different types of surgery. Rheumatic mitral valve disease tends to require that the valve is replaced with an artificial valve. On the other hand degenerative mitral valve disease is often amenable to repair. This means that not only does the patient keep their own valve, but they are less likely to suffer valve related complications down the line.
Over the years mitral valve surgery has been more risky than aortic valve surgery largely due to rheumatic valve disease. Isolated mitral valve operations carried, on average, an operative mortality of about 5%, which would rise to about 10% when coronary bypass grafting was also required.
Mitral valve patients are generally sicker than aortic valve patients so, not surprisingly, the overall spread of post-operative length-of-stay is greater as shown in the box-and-whisker plots, however, this remained relatively static over the last few years. Combined mitral valve surgery and coronary bypass surgery is a much bigger and more complex operation than isolated mitral valve replacement or repair and therefore patients generally stay in hospital a little longer after such an operation.
However, things are changing. A combination of changing disease processes and improved surgical techniques has meant that more vales are being repaired with better and better results. The operative mortality when a valve can be repaired is well under 2% as opposed to about 6% when a replacement is required. The benefit of repair over replacement is retained even when additional coronary surgery is required at the same time (see page 85). The benefits of repair over replacement are also reflected in a reduced postoperative hospital stay.

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
80
NA
CSD
– V
alve
su
rger
y
Aortic valve surgery
The average age of patients undergoing isolated aortic valve replacement has remained pretty static over the last 7-8 years. On the other hand, the average age of patients having combined aortic valve replacement and coronary surgery has steadily risen. Despite this the operative mortality has remained relatively constant.
Aortic valve: Average age by procedure; bars denote standard errors (n=27,879)
AV AV & CABG
Aortic valve: Crude mortality by procedure (n=25,751)
AV AV & CABG
0%
1%
2%
3%
4%
5%
6%
7%
8%
9%
10%
1997 1998 1999 2000 2001 2002 2003
Financial year
Cru
de
mo
rtal
ity
rate
60
62
64
66
68
70
72
1994 1995 1996 1997 1998 1999 2000 2001 2002 2003
Financial year
Ave
rag
e ag
e / y
ears

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
81
NA
CSD
– Valve su
rgery
The increasing age of patients having combined aortic valve and coronary surgery is reflected in the longer post-operative length of stay seen in the last 4-5 years. The post-operative length of stay for isolated aortic valve patients has remained constant.
The median post-operative lengths of stay are slightly longer than in the US where the median is 7 days for both groups.
Isolated aortic valve: Post-operative stay (n=16,046)
Median 25th-75th percentile 10th and 90th percentiles
Aortic valve and CABG: Post-operative stay (n=10,017)
Median 25th-75th percentile 10th and 90th percentiles
4
6
8
10
12
14
16
18
20
1994 1995 1996 1997 1998 1999 2000 2001 2002 2003
Financial year
Len
gth
-of-
stay
/ d
ays
4
6
8
10
12
14
16
18
20
Leng
th-o
f-stay / days
4
6
8
10
12
14
16
18
20
22
24
1994 1995 1996 1997 1998 1999 2000 2001 2002 2003
Financial year
Len
gth
-of-
stay
/ d
ays
4
6
8
10
12
14
16
18
20
22
24
Leng
th-o
f-stay / days

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
82
NA
CSD
– V
alve
su
rger
y
Mitral valve surgery
The average age of mitral valve patients has not changed much over the last few years. On average patients having combined mitral valve and coronary surgery are 5 years older than those having isolated mitral valve surgery. The operative mortality for both groups has slowly fallen over the years.
Mitral valve: Average age by procedure; bars denote standard errors (n=12,871)
MV MV & CABG
Mitral valve: Crude mortality by procedure (n=11,867)
MV MV & CABG
0%
2%
4%
6%
8%
10%
12%
14%
16%
18%
20%
1997 1998 1999 2000 2001 2002 2003
Financial year
Cru
de
mo
rtal
ity
rate
59
61
63
65
67
69
1994 1995 1996 1997 1998 1999 2000 2001 2002 2003
Financial year
Ave
rag
e ag
e / y
ears

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
83
NA
CSD
– Valve su
rgery
The post-operative length of stay for mitral valve patients has remained relatively constant. A median stay of 8 days for isolated mitral valve surgery and 10 days for combined mitral and coronary surgery is longer than the respective 7 and 9 days reported in the US.
Isolated mitral valve: Post-operative stay (n=8,498)
Median 25th-75th percentile 10th and 90th percentiles
Mitral valve and CABG: Post-operative stay (n=3,063)
Median 25th-75th percentile 10th and 90th percentiles
0
5
10
15
20
25
30
35
1994 1995 1996 1997 1998 1999 2000 2001 2002 2003
Financial year
Len
gth
-of-
stay
/ d
ays
0
5
10
15
20
25
30
35
Leng
th-o
f-stay / days
4
6
8
10
12
14
16
18
20
22
24
1994 1995 1996 1997 1998 1999 2000 2001 2002 2003
Financial year
Len
gth
-of-
stay
/ d
ays
4
6
8
10
12
14
16
18
20
22
24
Leng
th-o
f-stay / days

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
84
NA
CSD
– V
alve
su
rger
y
Mitral valve replacement and repair
In the past, rheumatic fever in childhood predisposed to mitral valve disease in adulthood; this was the main reason for mitral valve surgery. Since the advent of effective antibiotics, rheumatic fever has become very rare in the UK and now age-related degeneration of the mitral valve is becoming the predominant reason for surgery.
The two conditions are generally amenable to different types of surgery. Rheumatic mitral valve disease tends to require that the valve is replaced with an artificial valve. On the other hand degenerative mitral vale disease is often amenable to repair. This means that not only does the patient keep their own valve, but they are also less likely to suffer valve related complications down the line.
There is good evidence that repairing, rather than replacing the mitral valve where possible is better for the patient.
Demonstrably better results for mitral valve repair as opposed to replacement have resulted in more patients being referred for surgery where investigations show that repair is feasible.
Isolated mitral valve: Age categories by procedure (n=4,297)
<56 years 56-60 years 61-65 years
66-70 years 71-75 years >75 years
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
2001 2002 2003 2001 2002 2003
Replacement Repair
Mitral valve procedure & Financial year
Per
cen
tag
e o
f pat
ien
ts

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
85
NA
CSD
– Valve su
rgery
The operative mortality for mitral valve replacement and repair has fallen noticeably over the last few years. Mitral valve repair has an operative mortality less than one-third that of mitral valve replacement and less than that for isolated, first time coronary surgery.
Even when combined with coronary surgery repair offers an advantage over replacement.
Isolated mitral valve: Crude mortality for patients by procedure (n=5,447)
MV replacement MV repair
Mitral valve and CABG: Crude mortality by procedure (n=2,433)
MV replacement MV repair
0%
2%
4%
6%
8%
10%
12%
2000 2001 2002 2003
Financial year
Cru
de
mo
rtal
ity
rate
0%
2%
4%
6%
8%
10%
12%
14%
16%
18%
20%
2000 2001 2002 2003
Financial year
Cru
de
mo
rtal
ity
rate

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
86
NA
CSD
– V
alve
su
rger
y
Patients who have had a mitral valve repair will spend less time in hospital than those who have had a replacement.
The graph below shows that 50% of mitral repair patients have been discharged sooner than 50% of valve replacement patients, who in turn are discharged sooner than patients who have had combined mitral and coronary surgery.
So, mitral valve repair, where feasible, offers a lower operative mortality and a shorter length of hospital stay.
Mitral valve: Post-operative stay by procedure (n=4,232)
Isolated MV repair Isolate MV replacement
MV repair & CABG MV replacement & CABG
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
0 2 4 6 8 10 12
Post-operative stay / days
Cu
mu
lati
ve p
rop
ort
ion
of p
atie
nts
dis
char
ged

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
87
NA
CSD
– CA
BG
surg
ery risk factors
Coronary artery bypass surgery
The remainder of this report focuses on coronary surgery since this constitutes the vast majority (about 70%) of adult cardiac surgery. Coronary artery bypass surgery is perhaps one of the best-documented and understood surgical procedures 21 and as such has attracted attention as a marker or sentinel operation for surgical performance 22, 23. Despite the fact that over 25,000 coronary operations are performed each year in the United Kingdom, and the raw mortality has been well documented over the years in the UK Cardiac Surgical Register, the national patient characteristics had not been well defined until the 1999-2000 report.
This section of the report takes our analyses a few steps further.
Firstly, it attempts to illustrate some of the complexities of national data collection by documenting missing, unconfirmed, unmapped or incomplete data for each centre in the UK.
Secondly, it documents the enormous variation in the characteristics of patient-populations undergoing surgery in different hospitals. The raw mortality reported for coronary artery bypass surgery is largely dependent on casemix. Some hospitals will operate on older patients; some will serve populations where there are more diabetics or more people with lung disease. All of these factors contribute to the risk of surgery for the individual patient and the reported results for a particular centre.
Finally, this section of the report will confirm the slowly changing characteristics of patients undergoing coronary surgery demonstrated in previous reports and illustrate the impact of the following patient related variables on hospital outcome:

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
88
NA
CSD
– C
AB
G s
urg
ery
risk
fact
ors
Sections on coronary surgery
Risk factors
• Age 89
• Gender 98
• Patient size 104
• Priority (degree of urgency) 110
• Ejection fraction 116
• Previous myocardial infarctions (MIs) 122
• Percutaneous coronary intervention (PCI) 132
• Left main stem (LMS) disease 134
• Previous surgery 140
• Diabetes 148
• Hypertension 154
• Peripheral vascular disease (PVD) 160
• Renal disease 166
• Angina 172
• Dyspnoea (breathlessness) 178
Interactions between risk factors 184
• Mortality, ejection fraction and dyspnoea 184
• Mortality, age and renal disease 185
Re-operation for post-operative bleeding 186
Aspects of coronary surgery practice 195
• Number of bypass grafts 195
• The use of arterial grafts 197
• Protecting the heart during coronary surgery 201
• On- and off-pump CABG 204
International comparisons 205
Evolution of risk factors 211

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
89
NA
CSD
– CA
BG
surg
ery risk factors
Age
Key points from age analyses
• Age is one of the best-recorded variables; in the last five years for the 107,287 patients represented in the database age was not recorded for only 175patients, equivalent to just 0.2%.
• If current trends are maintained the average age of patients presenting for coronary surgery will go up by another 2 years over the next five years.
• Over the last decade the proportion of patients over 75 has increased from 2.2% to 10.0%.
• Almost 30% of patients are over 70 years old, which represents a doubling over the last decade.
• Older patients stay longer in hospital after their operation and this appears to be increasing.
• Although older patients have a higher post-operative mortality rate; outcomes have improved steadily for all age groups over the last 5 years, most noticeably in the oldest age groups.
• The operative mortality for patients over the age of 75 has fallen from 7.2% in 1999 to 4.7% in 2003, representing a reduction of 35% over 5 years.
• The age spectrums are similar in the NHS and the private sector.
Average age
The current trend is that the average age of coronary surgery patients is increasing at the rate of two years every five years. Although this trend is steady and sustained, there are still differences between centres; the breadth of this difference was 5 years in 2003 as shown in a later graph.
Isolated CABG: average age; bars denote standard error (n=144,333)
57
58
59
60
61
62
63
64
65
1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003
Financial year
Ave
rag
e ag
e / y
ears

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
90
NA
CSD
– C
AB
G s
urg
ery
risk
fact
ors
Age categories
Over the last decade the proportion of patients over 75 has increased from 2.2% to 10.0%. Almost 30% of patients are over 70 years old, which represents a doubling over the last decade. This is important, as increasing age is one of the most important predictors of outcome and resource-utilisation.
Isolated CABG: Age categories (n=140,641)
<56 years 56-60 years 61-65 years
66-70 years 71-75 years >75 years
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
1994 1995 1996 1997 1998 1999 2000 2001 2002 2003
Financial year
Per
cen
tag
e o
f pat
ien
ts

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
91
NA
CSD
– CA
BG
surg
ery risk factors
Mortality and age
The most noticeable improvements in outcomes over the last 5 years have been in the older age groups, for example, mortality for patients over the age of 75 has fallen from 7.2% in 1999 to 4.7% in 2003, representing a reduction of 35%.
Financial year
1999 2000 2001 2002 2003
<56 1.1% (n=3,453)
1.1% (n=3,910)
1.1% (n=4,177)
1.1% (n=4,272)
0.8% (n=4,579)
56-60 1.4% (n=2,732)
1.0% (n=3,018)
1.2% (n=3,378)
1.1% (n=3,421)
0.9% (n=3,820)
61-65 2.0% (n=3,450)
1.8% (n=3,929)
1.9% (n=4,420)
1.6% (n=4,521)
1.5% (n=4,794)
66-70 2.7% (n=3,421)
2.5% (n=3,998)
2.3% (n=4,730)
2.0% (n=4,803)
1.9% (n=5,356)
71-75 3.9% (n=2,363)
3.4% (n=3,048)
3.6% (n=3,517)
3.1% (n=3,994)
3.1% (n=4,693)
>75 7.2% (n=1,019)
5.4% (n=1,421)
6.0% (n=1,802)
5.3% (n=2,168)
4.7% (n=2,590)
Ag
e at
su
rger
y / y
ears
Unconfirmed 0.0% (n=18)
9.1% (n=11)
0.0% (n=8)
0.0% (n=35)
1.0% (n=102)
Isolated CABG: Crude mortality by age category (n=106,797)
<56 years 56-60 years 61-65 years
66-70 years 71-75 years >75 years
0%
1%
2%
3%
4%
5%
6%
7%
8%
1999 2000 2001 2002 2003
Financial year
Cru
de
mo
rtal
ity
rate

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
92
NA
CSD
– C
AB
G s
urg
ery
risk
fact
ors
Isolated CABG: Crude survival by age category for financial year 2003 (n=25,832))
These graphs demonstrate that patients greater than 75 years old are two-and-a-half times more likely to succumb from surgery than patients 10 years younger and almost six times more likely to die than patients under the age of 60 years. This is very relevant given the difference in age spectrum between units illustrated on the following two pages, and must be borne in mind when viewing the basic mortality statistics on pages 50 and 51, which take no account of age or any other risk factors.
Isolated CABG: Crude mortality by age category for financial year 2003 (n=25,832)
0%
1%
2%
3%
4%
5%
6%
<56 56-60 61-65 66-70 71-75 >75
Age at surgery / years
Cru
de
mo
rtal
ity
rate
91%
92%
93%
94%
95%
96%
97%
98%
99%
100%
<56 56-60 61-65 66-70 71-75 >75
Age at surgery / years
Cru
de
surv
ival
rat
e

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
93
NA
CSD
– CA
BG
surg
ery risk factors
Age and NHS centres
Isolated CABG: Age categories by centre for financial year 2003 (n=24,978)
<56 years 56-60 years 61-65 years
66-70 years 71-75 years >75 years
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
N Staffordshire Royal Infirmary
Glasgow Western Infirmary
Northern General Hospital Sheffield
Golden Jubilee Hospital Glasgow
Royal Victoria Hospital Belfast
University Hospital o f Wales Cardiff
Queen Elizabeth Hospital B irmingham
M anchester Royal Infirmary
Leeds General Infirmary
King's College Hospital London
Glasgow Royal Infirmary
Walsgrave Hospital Coventry
Wythenshawe Hospital M anchester
Hammersmith Hospital London
Victoria Hospital B lackpool
St James's Hospital Dublin
Guy's & St Thomas' Hospitals London
Edinburgh Royal Infirmary
Aberdeen Royal Infirmary
James Cook Uni Hosp'l M iddlesbrough
M orriston Hospital Swansea
Bristo l Royal Infirmary
John Radcliffe Hospital Oxford
Cardiothoracic Centre Liverpool
Harefield Hospital London
Freeman Hospital Newcastle
St M ary's Hospital London
The Heart Hospital London
Nottingham City Hospital
Castle Hill Hospital Hull
Royal Brompton Hospital London
Glenfield Hospital Leicester
Barts and the London
St George's Hospital London
Derriford Hospital P lymouth
Southampton General Hospital
Royal Sussex County Hospital
Papworth Hospital
Cen
tre
Percentage of patients

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
94
NA
CSD
– C
AB
G s
urg
ery
risk
fact
ors
Average age by centre
Isolated CABG: Average age by centre for financial year 2003; bars denote standard error (n=24,978)
60 61 62 63 64 65 66 67 68
Glasgow Western Infirmary
Royal Victoria Hospital Belfast
N Staffordshire Royal Infirmary
Northern General Hospital Sheffield
Glasgow Royal Infirmary
Golden Jubilee Hospital Glasgow
University Hospital o f Wales Cardiff
Queen Elizabeth Hospital B irmingham
St James's Hospital Dublin
Leeds General Infirmary
M anchester Royal Infirmary
King's College Hospital London
Hammersmith Hospital London
James Cook Uni Hosp'l M iddlesbrough
Wythenshawe Hospital M anchester
Edinburgh Royal Infirmary
Guy's & St Thomas' Hospitals London
Victoria Hospital B lackpool
Walsgrave Hospital Coventry
M orriston Hospital Swansea
Nottingham City Hospital
Freeman Hospital Newcastle
Aberdeen Royal Infirmary
St M ary's Hospital London
The Heart Hospital London
John Radcliffe Hospital Oxford
Bristo l Royal Infirmary
Cardiothoracic Centre Liverpool
Royal Brompton Hospital London
Castle Hill Hospital Hull
Harefield Hospital London
Barts and the London
Glenfield Hospital Leicester
St George's Hospital London
Derriford Hospital P lymouth
Southampton General Hospital
Royal Sussex County Hospital
Papworth Hospital
Cen
tre
Average age at surgery / years

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
95
NA
CSD
– CA
BG
surg
ery risk factors
Missing, unconfirmed or unmapped age data
Isolated CABG: Missing age data by centre for financial year 2003 (n=25,067)
0% 5% 10% 15% 20% 25%
Aberdeen Royal Infirmary
Barts and the London
Victoria Hospital B lackpool
Bristo l Royal Infirmary
Cardiothoracic Centre Liverpool
Castle Hill Hospital Hull
Derriford Hospital P lymouth
Edinburgh Royal Infirmary
Freeman Hospital Newcastle
Glasgow Royal Infirmary
Glasgow Western Infirmary
Glenfield Hospital Leicester
Golden Jubilee Hospital Glasgow
Guy's & St Thomas' Hospitals London
Hammersmith Hospital London
Harefield Hospital London
John Radcliffe Hospital Oxford
King's College Hospital London
Leeds General Infirmary
M anchester Royal Infirmary
N Staffordshire Royal Infirmary
Northern General Hospital Sheffield
Nottingham City Hospital
Papworth Hospital
Queen Elizabeth Hospital B irmingham
Royal Brompton Hospital London
Royal Sussex County Hospital
Southampton General Hospital
St George's Hospital London
St James's Hospital Dublin
The Heart Hospital London
University Hospital o f Wales Cardiff
Walsgrave Hospital Coventry
Wythenshawe Hospital M anchester
James Cook Uni Hosp'l M iddlesbrough
St M ary's Hospital London
M orriston Hospital Swansea
Royal Victoria Hospital Belfast
Cen
tre
Percentage entries with missing data

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
96
NA
CSD
– C
AB
G s
urg
ery
risk
fact
ors
Age and private centres; Age and County
This year, for the first time, we include a series of graphs that focus on the patient-populations in the private sector. This is intended to encourage and promote the collection of data on all cardiac surgery operations performed in the UK. This chart indicates that there is a high degree of similarity between the two groups of patients in terms of age.
Isolated CABG: Age categories by centre for financial year 2003 (Private Hospital n=934)
<56 years 56-60 years 61-65 years
66-70 years 71-75 years >75 years
Isolated CABG: Age categories by country for financial year 2003 (n=24,975)
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
All NHS
All private
BUPA Hospital Washington
BUPA Hospital Bristol
London Bridge Hospital
BUPA Hospital Leicester
BUPA Cambridge Lea Hospital
BUPA Chalybeate Southampton
The Harley Street Clinic
Cen
tre
Percentage of patients
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
England
Wales
Ireland
Scotland
Co
un
try
Percentage of patients

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
97
NA
CSD
– CA
BG
surg
ery risk factors
Post-operative stay and age
Older patients stay longer in hospital after their operation. The length-of-stay for older patients appears to be increasing. Given the increasing proportion of older patients this will have implications for healthcare providers in the future.
Financial year
1999 2000 2001 2002 2003
<56 7.4 (n=3,127)
7.5 (n=3,603)
7.2 (n=3,916)
7.1 (n=4,120)
7.1 (n=4,318)
56-60 7.7 (n=2,496)
7.8 (n=2,774)
7.5 (n=3,163)
7.7 (n=3,294)
7.4 (n=3,625)
61-65 8.0 (n=3,078)
8.2 (n=3,610)
7.9 (n=4,163)
8.0 (n=4,340)
8.1 (n=4,588)
66-70 8.6 (n=3,095)
9.0 (n=3,711)
8.9 (n=4,398)
8.9 (n=4,576)
8.7 (n=5,079)
71-75 9.2 (n=2,137)
9.4 (n=2,820)
9.7 (n=3,258)
9.9 (n=3,839)
10.3 (n=4,456)
>75 10.2 (n=927)
10.3 (n=1,302)
10.6 (n=1,673)
11.3 (n=2,081)
11.3 (n=2,427)
Ag
e at
su
rger
y / y
ears
Unconfirmed 6.9 (n=8)
18.6 (n=10)
7.2 (n=6)
6.4 (n=18)
8.8 (n=20)
Isolated CABG: Average post-operative stay by age; bars denote standard errors (n=99,994)
<56 56-60 61-65 66-70 71-75 >75
6
7
8
9
10
11
12
1999 2000 2001 2002 2003
Financial year
Po
st-o
per
ativ
e st
ay /
day
s

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
98
NA
CSD
– C
AB
G s
urg
ery
risk
fact
ors
Gender
Key points from gender analyses
• Gender is another well-recorded variable; in the last five years for the 107,287 patients represented in the database gender was not recorded for only 85, equivalent to less than 0.1%.
• Women have consistently comprised about 20% of isolated coronary surgery patients.
• There are notable differences in the proportion of female patients in NHS hospitals; the rates varied from 11.8% to 24.7% in 2003.
• The proportion of female patients increases with increasing age from 13.7% in the under 50s to 31.7% in the over 80s.
• Women have worse outcomes; with an operative mortality which has consistently been 1.0-1.5% greater than men over the last 5 years.
• On average, women spend an extra day in hospital after their operation than men, although this may be related to age.
Gender distribution
Women have consistently comprised about 20% of isolated coronary artery bypass surgery patients. There has been little or no change in this pattern over the last 8 years.
At the lower end of the age-scale, in the pre-menopausal age group of <50 years, only 13.7% of the isolated coronary artery bypass surgery patients are female, whereas at the upper end of the spectrum, in the over-eighty age-group, the proportion of females more than doubles to 31.7% of the total.
Isolated CABG: Gender distributions (n=133,592)
0%
5%
10%
15%
20%
25%
30%
35%
<51 51-55 56-60 61-65 66-70 71-75 76-80 >80
Age at surgery / years
Per
cen
tag
e fe
mal
e p
atie
nts

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
99
NA
CSD
– CA
BG
surg
ery risk factors
Mortality and gender
Women have consistently suffered a higher operative mortality than men. Over the years the gap has narrowed slightly both in the USA and the UK. The reason for the higher operative mortality in women remains an enigma. There are some immediately apparent possibilities: the first is that women intrinsically respond differently to the surgery in some way; the second is that, on the whole, women are smaller than men, which means that their coronary arteries are smaller making the operation a little more difficult; a third contributing factor is that, proportionally, there are relatively more women in the older age brackets, so age may also play an important role in creating this difference in operative risk.
Some aspects of these hypotheses were explored and published in the 2000-2001 NACSD report and led to the conclusion that size was probably the most important determinant of risk between the genders.
Financial year
1997 1998 1999 2000 2001 2002 2003
Male 2.8% (n=6,454)
2.3% (n=10,728)
2.2% (n=13,050)
2.0% (n=15,399)
2.0% (n=17,618)
1.9% (n=18,445)
1.8% (n=20,798)
Female 4.8% (n=1,681)
3.8% (n=2,733)
3.6% (n=3,405)
3.1% (n=3,935)
3.5% (n=4,413)
2.9% (n=4,768)
2.8% (n=5,055)
Gen
der
Unconfirmed 0.0% (n=3)
NA
0.0% (n=1)
0.0% (n=1)
0.0% (n=1)
0.0% (n=1)
2.5% (n=81)
Isolated CABG: Crude mortality by gender (n= 128,482)
Male Female
0%
1%
2%
3%
4%
5%
6%
1997 1998 1999 2000 2001 2002 2003
Financial year
Cru
de
mo
rtal
ity
rate

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
100
NA
CSD
– C
AB
G s
urg
ery
risk
fact
ors
Gender and NHS centres
Isolated CABG: Proportion of female patients by centre for financial year 2003 (n=24,986)
0% 5% 10% 15% 20% 25% 30%
Royal Victoria Hospital Belfast
St M ary's Hospital London
Golden Jubilee Hospital Glasgow
Royal Brompton Hospital London
University Hospital o f Wales Cardiff
Derriford Hospital P lymouth
Leeds General Infirmary
King's College Hospital London
M orriston Hospital Swansea
Walsgrave Hospital Coventry
Papworth Hospital
Royal Sussex County Hospital
Nottingham City Hospital
Guy's & St Thomas' Hospitals London
Barts and the London
Hammersmith Hospital London
Bristo l Royal Infirmary
John Radcliffe Hospital Oxford
Cardiothoracic Centre Liverpool
Southampton General Hospital
N Staffordshire Royal Infirmary
The Heart Hospital London
St James's Hospital Dublin
Castle Hill Hospital Hull
Queen Elizabeth Hospital B irmingham
Edinburgh Royal Infirmary
Freeman Hospital Newcastle
Northern General Hospital Sheffield
Harefield Hospital London
James Cook Uni Hosp'l M iddlesbrough
M anchester Royal Infirmary
Glenfield Hospital Leicester
Glasgow Western Infirmary
Aberdeen Royal Infirmary
Wythenshawe Hospital M anchester
St George's Hospital London
Glasgow Royal Infirmary
Victoria Hospital B lackpool
Cen
tre
Percentage female patients

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
101
NA
CSD
– CA
BG
surg
ery risk factors
Missing, unconfirmed or unmapped gender data
Isolated CABG: Missing gender data by centre for financial year 2003 (n=25,067)
0% 2% 4% 6% 8% 10% 12% 14% 16% 18% 20%
Wythenshawe Hospital M anchester
Walsgrave Hospital Coventry
University Hospital o f Wales Cardiff
The Heart Hospital London
St James's Hospital Dublin
St George's Hospital London
Southampton General Hospital
Royal Sussex County Hospital
Royal Brompton Hospital London
Queen Elizabeth Hospital B irmingham
Papworth Hospital
Nottingham City Hospital
Northern General Hospital Sheffield
N Staffordshire Royal Infirmary
M orriston Hospital Swansea
M anchester Royal Infirmary
Leeds General Infirmary
John Radcliffe Hospital Oxford
James Cook Uni Hosp'l M iddlesbrough
Harefield Hospital London
Hammersmith Hospital London
Golden Jubilee Hospital Glasgow
Glenfield Hospital Leicester
Glasgow Western Infirmary
Glasgow Royal Infirmary
Freeman Hospital Newcastle
Derriford Hospital P lymouth
Castle Hill Hospital Hull
Cardio thoracic Centre Liverpool
Bristo l Royal Infirmary
Victoria Hospital B lackpool
Barts and the London
Aberdeen Royal Infirmary
Guy's & St Thomas' Hospitals London
St M ary's Hospital London
Edinburgh Royal Infirmary
King's College Hospital London
Royal Victoria Hospital Belfast
Cen
tre
Percentage entries with missing data

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
102
NA
CSD
– C
AB
G s
urg
ery
risk
fact
ors
Gender and private centres; Gender and country
Isolated CABG: Proportion of female patients by centre for financial year 2003 (Private Hospital n=944)
Isolated CABG: Proportion of female patients by country for financial year 2003 (n=24,986)
0% 5% 10% 15% 20% 25% 30%
All NHS
All private
BUPA Hospital Bristol
The Harley Street Clinic
BUPA Hospital Leicester
BUPA Hospital Washington
London Bridge Hospital
BUPA Cambridge Lea Hospital
BUPA Chalybeate Southampton
Cen
tre
Percentage female patients
0% 5% 10% 15% 20% 25%
Scotland
England
Ireland
Wales
Co
un
try
Percentage female patients

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
103
NA
CSD
– CA
BG
surg
ery risk factors
Gender and post-operative stay
Women tend to have a longer post-operative hospital stay. This is probably due to the fact that women are generally older at the time of surgery and have smaller coronary arteries, which means the operations are a little more technically demanding.
Financial year
1999 2000 2001 2002 2003
Male 8.2 (n=11,789)
8.4 (n=14,231)
8.3 (n=16,483)
8.4 (n=17,721)
8.5 (n=19,666)
Female 8.6 (n=3,078)
9.1 (n=3,598)
9.0 (n=4,093)
9.2 (n=4,546)
9.4 (n=4,828)
Gen
der
Unconfirmed 7.0 (n=1)
9.0 (n=1)
6.0 (n=1)
5.0 (n=1)
7.3 (n=19)
Isolated CABG: Average post-operative stay by gender; bars denote standard errors (n=100,033)
Male Female
8.0
8.2
8.4
8.6
8.8
9.0
9.2
9.4
9.6
1999 2000 2001 2002 2003
Financial year
Len
gth
of s
tay
/ day
s

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
104
NA
CSD
– C
AB
G s
urg
ery
risk
fact
ors
Size – body surface area and body mass index
Key points from analyses of patients’ size
• Body surface area (BSA) is more closely associated with operative mortality than body mass index (BMI).
• Small body surface area is associated with increased post-operative mortality.
• Smaller body surface area is associated with higher rates of post-operative bleeding (see page 192).
Body surface area (BSA) distributions
Body surface area is a function of the patient’s height and weight, and is calculated for adults as follows:
BSA = 7.184 × 10-3 × m0.425 × h0.725
where
BSA - Body surface area in m2
m - patient’s mass in kg
h - patient’s height in cm
Isolated CABG: Body surface area by gender; financial years 1999-2003 (n=97,885)
Male Female
0%
5%
10%
15%
20%
25%
<1.
40
1.40
-1.4
9
1.50
-1.5
9
1.60
-1.6
9
1.70
-1.7
9
1.80
-1.8
9
1.90
-1.9
9
2.00
-2.0
9
2.10
-2.1
9
2.20
-2.2
9
2.30
-2.3
9
2.40
-2.4
9
>2.
49
Body surface area / m2
Per
cen
tag
e o
f pat
ien
ts

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
105
NA
CSD
– CA
BG
surg
ery risk factors
Mortality and BSA
Small size as measured by body surface area (BSA) has a greater negative influence than large size. In a previous edition we have shown that this is equally true for both men and women. We also showed that the gender difference disappeared when BSA was taken into account.
It is likely that the increased mortality for smaller patients relates in part to the technical difficulty of constructing bypass grafts to very small coronary arteries and in part due to the greater impact of such major surgery on a smaller person.
Gender
Male Female Unconfirmed
<1.70 3.8% (n=3,696)
3.6% (n=8,624)
0.0% (n=3)
1.70-1.79 2.9% (n=8,147)
3.2% (n=4,814)
0.0% (n=3)
1.80-1.89 2.2% (n=15,445)
2.4% (n=3,358)
0.0% (n=3)
1.90-1.99 1.6% (n=18,960)
2.0% (n=1,839)
16.7% (n=6)
2.00-2.09 1.5% (n=15,942)
2.2% (n=692)
0.0% (n=3)
>2.09 1.5% (n=15,933)
1.9% (n=364)
0.0% (n=3)
Bo
dy
surf
ace
area
/ m
2
Unconfirmed 2.4% (n=7,187)
4.2% (n=1,885)
1.6% (n=64)
Isolated CABG: Crude mortality by body surface area and gender; financial years 1999-2003 (n=97,814)
Male Female
0.0%
0.5%
1.0%
1.5%
2.0%
2.5%
3.0%
3.5%
4.0%
4.5%
<1.70 1.70-1.79 1.80-1.89 1.90-1.99 2.00-2.09 >2.09
Body Surface Area / m2
Cru
de
mo
rtal
ity
rate

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
106
NA
CSD
– C
AB
G s
urg
ery
risk
fact
ors
Operative mortality, which is higher for smaller people, has fallen by 12% over the last 5 years for the smallest patients, those with a BSA of less than 1.7.
Financial year
1999 2000 2001 2002 2003
<1.70 4.0% (n=1,889)
3.7% (n=2,182)
3.6% (n=2,572)
3.6% (n=2,780)
3.5% (n=2,900)
1.70-1.89 2.9% (n=4,745)
2.6% (n=5,611)
2.8% (n=6,771)
2.5% (n=6,996)
2.1% (n=7,647)
1.90-2.39 1.8% (n=7,808)
1.7% (n=9,465)
1.6% (n=10,997)
1.5% (n=11,792)
1.4% (n=12,841)
>2.39 0.9% (n=211)
1.6% (n=129)
2.0% (n=153)
1.3% (n=157)
1.1% (n=189)
Bo
dy
surf
ace
area
/ m
2
Unconfirmed 2.9% (n=1,803)
2.3% (n=1,948)
3.1% (n=1,539)
2.6% (n=1,489)
3.1% (n=2,357)
Isolated CABG: Crude mortality by body surface area (n=96,996)
<1.70 1.70-1.89 1.90-2.39
0%
1%
2%
3%
4%
5%
1999 2000 2001 2002 2003
Financial year
Cru
de
mo
rtal
ity
rate

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
107
NA
CSD
– CA
BG
surg
ery risk factors
Body mass index (BMI) distributions
Body mass index is used as a measure of whether or not a person is overweight. The BMI is used as a guideline only. It is not foolproof.
A healthy weight is reflected in a BMI of less than 25; a BMI of 25 or greater is considered overweight; thirty or more is considered obese and 35 or more represents morbid obesity.
In the UK, three-quarters of coronary surgery patients are overweight and over one quarter are obese; less than one-quarter are of normal weight for their size.
Body mass index is a function of the patient’s height and weight, and is calculated as follows:
BMI = m2 ÷ h
where
BMI - Body mass index
m - patient’s mass in kg
h - patient’s height in cm
Financial year
1999 2000 2001 2002 2003
Underweight <20.0 285 257 297 302 321
Normal 20.0-24.9 3,766 4,107 4,797 4,891 5,220
Overweight 25.0-29.9 7,130 8,568 9,784 10,261 11,077
Obese 30.0-34.9 2,814 3,581 4,454 4,895 5,501
Morbidly obese ≥35.0 636 853 1,143 1,344 1,486
Bo
dy
mas
s in
dex
Unconfirmed 1,830 1,974 1,574 1,733 2,406
Isolated CABG: Body mass index (n=91,919)
Underweight Normal Overweight Obese Morbidly obese
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
1999 2000 2001 2002 2003
Financial year
Per
cen
tag
e o
f pat
ien
ts

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
108
NA
CSD
– C
AB
G s
urg
ery
risk
fact
ors
Mortality and BMI
Financial years 1999-2003
Financial year
Male Female Unspecified
Underweight <20.0 4.9% (n=869)
6.8% (n=592)
0.0% (n=1)
Normal 20.0-24.9 2.2% (n=17,775)
3.9% (n=4,992)
0.0% (n=4)
Overweight 25.0-29.9 1.8% (n=39,019)
2.6% (n=7,763)
0.0% (n=9)
Obese 30.0-34.9 1.6% (n=16,716)
2.6% (n=4,501)
16.7% (n=6)
Morbidly obese ≥35.0 2.2% (n=3,634)
3.0% (n=1,818)
0.0% (n=1)
Bo
dy
mas
s in
dex
Unconfirmed 2.4% (n=7,297)
4.1% (n=1,910)
1.6% (n=64)
Isolated CABG: Crude mortality by body mass index and gender; financial years 1999-2003 (n=97,679)
Male Female
0%
1%
2%
3%
4%
5%
6%
7%
8%
9%
10%
Underweight Normal Overweight Obese Morbidly obese
Body Mass Index
Cru
de
mo
rtal
ity
rate

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
109
NA
CSD
– CA
BG
surg
ery risk factors
As with body surface area, underweight patients have a higher operative mortality than heavier patients.
Financial year
1999 2000 2001 2002 2003
Underweight <20.0 5.3% (n=285)
7.0% (n=257)
5.7% (n=297)
6.0% (n=302)
4.7% (n=321)
Normal 20.0-24.9 2.8% (n=3,763)
2.6% (n=4,107)
2.7% (n=4,796)
2.4% (n=4,891)
2.6% (n=5,214)
Overweight 25.0-29.9 2.2% (n=7,129)
1.9% (n=8,567)
2.1% (n=9,778)
2.0% (n=10,261)
1.5% (n=11,056)
Obese 30.0-34.9 1.9% (n=2,813)
2.0% (n=3,580)
2.0% (n=4,452)
1.7% (n=4,895)
1.6% (n=5,483)
Morbidly obese ≥35.0 2.8% (n=636)
3.0% (n=853)
2.2% (n=1,142)
2.3% (n=1,343)
2.4% (n=1,479)
Bo
dy
mas
s in
dex
Unconfirmed 2.9% (n=1,830)
2.2% (n=1,971)
3.0% (n=1,567)
2.5% (n=1,522)
3.1% (n=2,381)
Isolated CABG: Crude mortality by body mass index (n=91,822)
Underweight Normal Overweight Obese Morbidly obese
0%
1%
2%
3%
4%
5%
6%
7%
8%
9%
10%
1999 2000 2001 2002 2003
Financial year
Cru
de
mo
rtal
ity
rate

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
110
NA
CSD
– C
AB
G s
urg
ery
risk
fact
ors
Priority
Key points from the priority analyses
• The proportions of elective and non-elective cases have remained stable over the last 8 years.
• Priority remains an important determinant of outcome.
• There is significant variation in the percentage of elective cases between centres.
• Non-elective patients remain in hospital longer after their operation.
Priority distribution
The national percentage of patients requiring urgent surgery has remained relatively constant over the last 8 years. Since the difference between elective and urgent surgery is clearly understood, local variation is likely to be real and probably reflects a combination of differences in clinical strategies for the management of unstable angina and available surgical resources. It also reflects local confidence in surgical waiting list management. Note that the UK database conforms to the definitions of urgency used worldwide by the cardiothoracic community, which are at variance with the national CEPOD and NHS definitions.
Financial year
1996 1997 1998 1999 2000 2001 2002 2003
Elective 3,039 5,274 9,279 11,591 13,167 15,260 16,529 18,750
Urgent 1,101 2,253 3,385 4,213 4,680 5,961 6,103 6,507
Emergency 234 372 475 496 532 617 585 511
Salvage 10 19 22 58 115 118 87 95 Op
erat
ive
pri
ori
ty
Unconfirmed 627 226 303 103 846 93 122 148
Isolated CABG: Operative priority (n=130,914)
Elective Urgent Emergency Salvage
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
1996 1997 1998 1999 2000 2001 2002 2003
Financial year
Per
cen
tag
e o
f pat
ien
ts

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
111
NA
CSD
– CA
BG
surg
ery risk factors
Mortality and priority
Operative priority has a major influence on surgical risk. Urgent cases such as in-hospital referrals have an operative mortality, which is approximately twice that of elective patients admitted from home. Genuine emergency surgery is 4-5 times as risky as routine surgery. This is similar to the North American experience.
Financial year
1999 2000 2001 2002 2003
Elective 1.7% (n=11,589)
1.5% (n=13,166)
1.3% (n=15,254)
1.3% (n=16,426)
1.4% (n=18,686)
Urgent 3.3% (n=4,211)
3.1% (n=4,679)
3.6% (n=5,958)
3.4% (n=6,014)
2.9% (n=6,495)
Emergency 9.7% (n=495)
10.0% (n=532)
10.7% (n=617)
9.5% (n=577)
10.6% (n=510)
Salvage 32.8% (n=58)
20.0% (n=115)
22.0% (n=118)
25.3% (n=87)
10.5% (n=95) O
per
ativ
e p
rio
rity
Unconfirmed 3.9% (n=103)
1.8% (n=843)
1.2% (n=85)
1.8% (n=110)
0.7% (n=148)
Isolated CABG: Crude mortality by operative priority (n=105,682)
Elective Urgent Emergency
0%
2%
4%
6%
8%
10%
12%
14%
1999 2000 2001 2002 2003
Financial year
Cru
de
mo
rtal
ity
rate

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
112
NA
CSD
– C
AB
G s
urg
ery
risk
fact
ors
Priority and NHS centres
Isolated CABG: Operative priority by centre for financial year 2003 (n=24,923)
Elective Urgent Emergency Salvage
0% 20% 40% 60% 80% 100%
St James's Hospital Dublin
M orriston Hospital Swansea
Bristo l Royal Infirmary
University Hospital o f Wales Cardiff
Southampton General Hospital
John Radcliffe Hospital Oxford
St George's Hospital London
Barts and the London
James Cook Uni Hosp'l M iddlesbrough
Walsgrave Hospital Coventry
Queen Elizabeth Hospital B irmingham
Hammersmith Hospital London
King's College Hospital London
The Heart Hospital London
Derriford Hospital P lymouth
St M ary's Hospital London
Glenfield Hospital Leicester
Victoria Hospital B lackpool
M anchester Royal Infirmary
Edinburgh Royal Infirmary
Leeds General Infirmary
Freeman Hospital Newcastle
N Staffordshire Royal Infirmary
Aberdeen Royal Infirmary
Royal Sussex County Hospital
Guy's & St Thomas' Hospitals London
Castle Hill Hospital Hull
Glasgow Royal Infirmary
Royal Victoria Hospital Belfast
Nottingham City Hospital
Papworth Hospital
Wythenshawe Hospital M anchester
Royal Brompton Hospital London
Glasgow Western Infirmary
Cardiothoracic Centre Liverpool
Harefield Hospital London
Northern General Hospital Sheffield
Golden Jubilee Hospital Glasgow
Cen
tre
Percentage of patients

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
113
NA
CSD
– CA
BG
surg
ery risk factors
Missing, unconfirmed or unmapped priority data
Isolated CABG: Missing operative priority data by centre for financial year 2003 (n=25,067)
0% 5% 10% 15% 20%
Wythenshawe Hospital M anchester
Walsgrave Hospital Coventry
University Hospital o f Wales Cardiff
St James's Hospital Dublin
St George's Hospital London
Southampton General Hospital
Royal Sussex County Hospital
Royal Brompton Hospital London
Queen Elizabeth Hospital B irmingham
Papworth Hospital
Northern General Hospital Sheffield
N Staffordshire Royal Infirmary
M anchester Royal Infirmary
Leeds General Infirmary
King's College Hospital London
James Cook Uni Hosp'l M iddlesbrough
Harefield Hospital London
Hammersmith Hospital London
Guy's & St Thomas' Hospitals London
Glenfield Hospital Leicester
Glasgow Royal Infirmary
Freeman Hospital Newcastle
Edinburgh Royal Infirmary
Derriford Hospital P lymouth
Castle Hill Hospital Hull
Cardio thoracic Centre Liverpool
Victoria Hospital B lackpool
Bristo l Royal Infirmary
Glasgow Western Infirmary
Nottingham City Hospital
Aberdeen Royal Infirmary
The Heart Hospital London
Golden Jubilee Hospital Glasgow
Barts and the London
St M ary's Hospital London
John Radcliffe Hospital Oxford
M orriston Hospital Swansea
Royal Victoria Hospital Belfast
Cen
tre
Percentage entries with missing data

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
114
NA
CSD
– C
AB
G s
urg
ery
risk
fact
ors
Priority and private centres; Priority and country
As might be expected, there are many fewer non-elective operations performed in the private sector.
Isolated CABG: Operative priority by centre for financial year 2003 (Private Hospital n=940)
Elective Urgent Emergency Salvage
Isolated CABG: Operative priority by country for financial year 2003 (n=24,923)
Elective Urgent Emergency Salvage
0% 20% 40% 60% 80% 100%
All NHS
All private
London Bridge Hospital
BUPA Hospital Bristol
BUPA Hospital Washington
BUPA Hospital Leicester
BUPA Chalybeate Southampton
BUPA Cambridge Lea Hospital
The Harley Street Clinic
Cen
tre
Percentage of patients
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Wales
Ireland
England
Scotland
Co
un
try
Percentage of patients

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
115
NA
CSD
– CA
BG
surg
ery risk factors
Priority and post-operative stay
Priority of surgery has a powerful influence on the post-operative stay as indicated in the table and graph below.
Financial year
1999 2000 2001 2002 2003
Elective 7.9 (n=10,551)
8.1 (n=12,057)
8.0 (n=14,388)
8.2 (n=15,842)
8.3 (n=17,783)
Urgent 9.0 (n=3,727)
9.3 (n=4,357)
9.2 (n=5,446)
9.4 (n=5,738)
9.3 (n=6,126)
Emergency 10.5 (n=450)
10.3 (n=494)
11.1 (n=558)
11.0 (n=551)
13.6 (n=470)
Salvage 10.7 (n=57)
10.4 (n=108)
9.5 (n=116)
8.9 (n=85)
8.5 (n=90) O
per
ativ
e p
rio
rity
Unconfirmed 9.1 (n=83)
8.7 (n=814)
7.4 (n=69)
9.0 (n=52)
11.5 (n=44)
Isolated CABG: Average post-operative stay by operative priority; bars denote standard errors (n=98,538)
Elective Urgent Emergency
7
8
9
10
11
12
13
14
15
1999 2000 2001 2002 2003
Financial year
Po
st-o
per
ativ
e st
ay /
day
s

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
116
NA
CSD
– C
AB
G s
urg
ery
risk
fact
ors
Ejection fraction
Key points from the ejection fraction analyses
• Ejection fraction is a standard measure of the heart’s efficiency.
• The percentage of patients with poor heart function has remained relatively stable over time.
• Heart function remains one of the most important predictors of post-operative outcomes.
• Patients with poor heart function are five times more likely to die after their operation than patients with good heart function.
Heart function is measured by the heart’s ejection fraction. With each heartbeat the heart ejects a certain amount of blood. If it ejects more than 50% of blood from the main pumping chamber with each beat it is functioning well and is said to have a good ejection fraction. If it ejects less than 50% then its function is impaired. The lower the ejection fraction the greater the functional impairment. An ejection fraction of less than 30% represents very poor heart function; an ejection fraction between 30-50% represents moderate or fair heart function.
Ejection fraction distribution
The following table and graph shows that over the years the distribution of patients with good, fair / moderate and poorly functioning hearts has remained relatively constant.
Financial year
1996 1997 1998 1999 2000 2001 2002 2003
Good 2,912 4,721 8,056 10,149 11,385 13,964 14,752 16,344
Fair 1,144 2,139 3,511 4,182 5,060 6,018 6,033 6,698
Poor 260 488 756 1,016 1,234 1,459 1,424 1,464
Ejec
tio
n
frac
tio
n
Unconfirmed 695 796 1,141 1,114 1,661 608 1,217 1,505
Isolated CABG: Ejection fraction (n=125,169)
Good Fair Poor
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
1996 1997 1998 1999 2000 2001 2002 2003
Financial year
Per
cen
tag
e o
f pat
ien
ts

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
117
NA
CSD
– CA
BG
surg
ery risk factors
Mortality and ejection fraction
Chapter 6 of the National Service Framework for Coronary Heart Disease encourages the diagnosis and treatment of patients with heart failure. Heart failure is a clinical syndrome caused by a reduction in the heart’s ability to pump blood around the body. In about 70% of patients the cause is coronary artery disease, which in some cases will be amenable to surgery. Improved diagnosis and treatment of heart failure will, therefore, have resource implications for surgical centres.
The table below clearly outlines the difference in operative mortality between patients with good heart function and those with poor heart function. There is a fairly consistent five-fold increase in mortality when the ejection fraction is less than 30%.
Financial year
1999 2000 2001 2002 2003
Good 1.4% (n=10,146)
1.4% (n=11,384)
1.4% (n=13,959)
1.2% (n=14,752)
1.2% (n=16,306)
Fair 3.0% (n=4,180)
2.7% (n=5,059)
3.0% (n=6,014)
2.8% (n=6,033)
2.7% (n=6,687)
Poor 9.4% (n=1,016)
7.8% (n=1,234)
8.3% (n=1,458)
8.9% (n=1,423)
6.4% (n=1,463)
Ejec
tio
n fr
acti
on
Unconfirmed 3.6% (n=1,114)
2.0% (n=1,658)
3.2% (n=601)
2.3% (n=1,006)
2.4% (n=1,478)
Isolated CABG: Crude mortality by ejection fraction (n=101,114)
Good Fair Poor
Note on the opposite page the wide variation in the distribution of ejection fraction between centres (the John Radcliffe Hospital did not submit data on ejection fraction).
0%
2%
4%
6%
8%
10%
12%
1999 2000 2001 2002 2003
Financial year
Cru
de
mo
rtal
ity
rate

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
118
NA
CSD
– C
AB
G s
urg
ery
risk
fact
ors
Ejection fraction and NHS centres
Isolated CABG: Ejection fraction by centre for financial year 2003 (n=23,677)
Good Fair Poor
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Papworth Hospital
M orriston Hospital Swansea
Glasgow Royal Infirmary
St M ary's Hospital London
University Hospital o f Wales Cardiff
King's College Hospital London
Glenfield Hospital Leicester
Nottingham City Hospital
St James's Hospital Dublin
Cardiothoracic Centre Liverpool
Hammersmith Hospital London
Royal Victoria Hospital Belfast
Bristo l Royal Infirmary
Northern General Hospital Sheffield
Guy's & St Thomas' Hospitals London
Barts and the London
Southampton General Hospital
The Heart Hospital London
Glasgow Western Infirmary
Edinburgh Royal Infirmary
N Staffordshire Royal Infirmary
Derriford Hospital P lymouth
St George's Hospital London
Golden Jubilee Hospital Glasgow
Walsgrave Hospital Coventry
Victoria Hospital B lackpool
Wythenshawe Hospital M anchester
Royal Sussex County Hospital
Queen Elizabeth Hospital B irmingham
Aberdeen Royal Infirmary
Royal Brompton Hospital London
M anchester Royal Infirmary
Castle Hill Hospital Hull
Freeman Hospital Newcastle
Leeds General Infirmary
James Cook Uni Hosp'l M iddlesbrough
Harefield Hospital London
John Radcliffe Hospital Oxford
Cen
tre
Percentage of patients

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
119
NA
CSD
– CA
BG
surg
ery risk factors
Missing, unconfirmed or unmapped ejection fraction data
Isolated CABG: Missing ejection fraction data by centre for financial year 2003 (n=25,067)
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Wythenshawe Hospital M anchester
Walsgrave Hospital Coventry
St James's Hospital Dublin
Southampton General Hospital
Royal Sussex County Hospital
Royal Brompton Hospital London
N Staffordshire Royal Infirmary
M anchester Royal Infirmary
Leeds General Infirmary
Harefield Hospital London
Hammersmith Hospital London
Glasgow Western Infirmary
Cardiothoracic Centre Liverpool
Victoria Hospital B lackpool
Freeman Hospital Newcastle
Edinburgh Royal Infirmary
Aberdeen Royal Infirmary
University Hospital o f Wales Cardiff
Queen Elizabeth Hospital B irmingham
Castle Hill Hospital Hull
Golden Jubilee Hospital Glasgow
Glasgow Royal Infirmary
Bristo l Royal Infirmary
Nottingham City Hospital
James Cook Uni Hosp'l M iddlesbrough
St M ary's Hospital London
The Heart Hospital London
King's College Hospital London
Derriford Hospital P lymouth
St George's Hospital London
Papworth Hospital
Barts and the London
M orriston Hospital Swansea
Guy's & St Thomas' Hospitals London
Northern General Hospital Sheffield
Royal Victoria Hospital Belfast
Glenfield Hospital Leicester
John Radcliffe Hospital Oxford
Cen
tre
Percentage entries with missing data

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
120
NA
CSD
– C
AB
G s
urg
ery
risk
fact
ors
Ejection fraction and private centres; Ejection fraction and country
There is considerable variation between the reported ejection fractions from different centres, which may be real or may relate to varying methods of estimating ejection fraction. The importance of this difference is that a low ejection fraction is associated with a higher operative mortality and morbidity.
Isolated CABG: Ejection fraction by centre for financial year 2003 (Private Hospital n=829)
Good Fair Poor
Isolated CABG: Ejection fraction by country for financial year 2003 (n=23,677)
Good Fair Poor
0% 20% 40% 60% 80% 100%
All NHS
All private
BUPA Cambridge Lea Hospital
BUPA Hospital Leicester
London Bridge Hospital
BUPA Chalybeate Southampton
The Harley Street Clinic
BUPA Hospital Washington
BUPA Hospital Bristol
Cen
tre
Percentage of patients
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Wales
Ireland
Scotland
England
Co
un
try
Percentage of patients

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
121
NA
CSD
– CA
BG
surg
ery risk factors
Ejection fraction and post-operative stay
Patients with good heart function have greater reserves to withstand the insult of major surgery and are therefore likely to recover more quickly than patients with impaired heart function. This is reflected in both the operative mortality / survival and the post-operative length-of-stay.
On average patients with significantly impaired heart function take three days longer to recover than patients with good heart function.
Financial year
1999 2000 2001 2002 2003
Good 7.8 (n=9,178)
8.0 (n=10,321)
7.9 (n=12,914)
8.1 (n=14,013)
8.2 (n=15,589)
Fair 8.7 (n=3,886)
8.9 (n=4,755)
8.9 (n=5,768)
9.1 (n=5,784)
9.1 (n=6,260)
Poor 10.3 (n=946)
10.9 (n=1,163)
10.9 (n=1,403)
11.5 (n=1,374)
11.1 (n=1,369)
Ejec
tio
n fr
acti
on
Unconfirmed 8.6 (n=858)
8.9 (n=1,591)
8.6 (n=492)
8.2 (n=1,097)
9.6 (n=1,295)
Isolated CABG: Average post-operative stay by ejection fraction; bars denote standard errors (n=94,723)
Good Fair Poor
7.0
7.5
8.0
8.5
9.0
9.5
10.0
10.5
11.0
11.5
12.0
1999 2000 2001 2002 2003
Financial year
Ave
rag
e p
ost
-op
erat
ive
stay
/ d
ays

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
122
NA
CSD
– C
AB
G s
urg
ery
risk
fact
ors
Previous myocardial infarctions (MIs)
Key points from the previous myocardial infarction analyses
• Heart attacks tend to result in impaired heart function, which is associated with worse outcomes.
• In the most recent year’s data, patients who had had one or more heart attacks had a reduced survival rate: 97.4% versus 98.5% for patients who had not had a heart attack.
Previous MI distributions
A heart attack (Myocardial Infarction or MI) occurs when one of the coronary arteries becomes blocked and some heart muscle dies as a result. The hazard of a myocardial infarction is that it irreversibly damages heart muscle and, if large enough, also reduces life expectancy. Sufficiently severe or multiple infarctions will also reduce the ejection fraction so the information presented in this section should to some extent reflect the information in that section. Nearly half of patients presenting for surgery have had a previous heart attack. Some centres only note the presence of a previous infarction, not how many have occurred.
Financial year
1996 1997 1998 1999 2000 2001 2002 2003
No previous MI 2,019 3,488 5,761 7,918 9,537 11,059 12,123 13,920
Previous MI 1,878 3,387 5,742 6,534 8,138 10,153 10,340 11,073
Pre
vio
us
MI
Unconfirmed 1,114 1,269 1,961 2,009 1,665 837 963 1,018
Isolated CABG: Previous MIs (n=123,070)
No MI Previous MI
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
1996 1997 1998 1999 2000 2001 2002 2003
Financial year
Per
cen
tag
e o
f pat
ien
ts

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
123
NA
CSD
– CA
BG
surg
ery risk factors
Mortality and previous MIs
Because a MI weakens the heart it is less able to withstand the rigours of surgery so the operative mortality is higher.
Financial year
1999 2000 2001 2002 2003
No MI 2.0% (n=7,915)
1.8% (n=9,532)
1.8% (n=11,048)
1.6% (n=12,044)
1.5% (n=13,882)
Previous MI 3.1% (n=6,532)
2.9% (n=8,138)
2.9% (n=10,147)
2.8% (n=10,251)
2.6% (n=11,042)
Pre
vio
us
MI
Unconfirmed 2.0% (n=2,009)
1.8% (n=1,665)
2.4% (n=837)
1.5% (n=919)
1.7% (n=1,010)
Isolated CABG: Crude mortality by previous MIs (n=100,531)
No MI Previous MI
0.0%
0.5%
1.0%
1.5%
2.0%
2.5%
3.0%
3.5%
4.0%
1999 2000 2001 2002 2003
Financial year
Cru
de
mo
rtal
ity
rate

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
124
NA
CSD
– C
AB
G s
urg
ery
risk
fact
ors
Previous MIs and NHS centres
The white bar below is a proxy for No MI, since one hospital does not collect MI data in the agreed dataset.
Isolated CABG: Previous MI by centre for financial year 2003 (n=24,435)
No MI Previous MI
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
James Cook Uni Hosp'l M iddlesbrough
King's College Hospital London
M orriston Hospital Swansea
Nottingham City Hospital
University Hospital o f Wales Cardiff
Derriford Hospital P lymouth
Aberdeen Royal Infirmary
Glasgow Western Infirmary
Leeds General Infirmary
St James's Hospital Dublin
Barts and the London
The Heart Hospital London
Northern General Hospital Sheffield
Hammersmith Hospital London
Glasgow Royal Infirmary
Royal Victoria Hospital Belfast
Royal Sussex County Hospital
N Staffordshire Royal Infirmary
St George's Hospital London
M anchester Royal Infirmary
Glenfield Hospital Leicester
Edinburgh Royal Infirmary
Freeman Hospital Newcastle
Cardiothoracic Centre Liverpool
Papworth Hospital
Wythenshawe Hospital M anchester
Guy's & St Thomas' Hospitals London
Walsgrave Hospital Coventry
Southampton General Hospital
Bristo l Royal Infirmary
Queen Elizabeth Hospital B irmingham
Royal Brompton Hospital London
Harefield Hospital London
Victoria Hospital B lackpool
John Radcliffe Hospital Oxford
Castle Hill Hospital Hull
St M ary's Hospital London
Golden Jubilee Hospital Glasgow
Cen
tre
Percentage of patients

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
125
NA
CSD
– CA
BG
surg
ery risk factors
Missing, unconfirmed or unmapped previous MI data
Isolated CABG: Missing previous MI data by centre for financial year 2003 (n=25,067)
0% 10% 20% 30% 40% 50% 60% 70% 80% 90%
Wythenshawe Hospital M anchester
Walsgrave Hospital Coventry
St James's Hospital Dublin
St George's Hospital London
Southampton General Hospital
Royal Sussex County Hospital
Royal Brompton Hospital London
Queen Elizabeth Hospital B irmingham
Papworth Hospital
Northern General Hospital Sheffield
M anchester Royal Infirmary
Harefield Hospital London
Hammersmith Hospital London
Guy's & St Thomas' Hospitals London
Glasgow Western Infirmary
Glasgow Royal Infirmary
Edinburgh Royal Infirmary
Derriford Hospital P lymouth
Cardiothoracic Centre Liverpool
Victoria Hospital B lackpool
Aberdeen Royal Infirmary
Leeds General Infirmary
N Staffordshire Royal Infirmary
The Heart Hospital London
Bristo l Royal Infirmary
Castle Hill Hospital Hull
Golden Jubilee Hospital Glasgow
University Hospital o f Wales Cardiff
King's College Hospital London
Freeman Hospital Newcastle
Nottingham City Hospital
James Cook Uni Hosp'l M iddlesbrough
M orriston Hospital Swansea
Glenfield Hospital Leicester
Barts and the London
John Radcliffe Hospital Oxford
Royal Victoria Hospital Belfast
St M ary's Hospital London
Cen
tre
Percentage entries with missing data

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
126
NA
CSD
– C
AB
G s
urg
ery
risk
fact
ors
Previous MIs and private centres; Previous MI and country
Isolated CABG: Previous MI by centre for financial year 2003 (Private Hospital n=905)
No MI Previous MI
Isolated CABG: Previous MI by country for financial year 2003 (n=24,088)
No MI Previous MI
0% 20% 40% 60% 80% 100%
All NHS
All private
BUPA Hospital Leicester
BUPA Hospital Washington
BUPA Chalybeate Southampton
BUPA Hospital Bristol
BUPA Cambridge Lea Hospital
London Bridge Hospital
The Harley Street Clinic
Cen
tre
Percentage of patients
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Wales
Ireland
Scotland
England
Co
un
try
Percentage of patients

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
127
NA
CSD
– CA
BG
surg
ery risk factors
Previous MIs and post-operative stay
Because a heart attack weakens the heart it is less resilient so it takes longer to recover from an operation. Not surprisingly patients who have had a previous heart attack(s) spend longer in hospital recovering after their operation.
Financial year
1999 2000 2001 2002 2003
No MI 8.1 (n=7,358)
8.2 (n=8,947)
8.1 (n=10,795)
8.3 (n=11,888)
8.4 (n=13,471)
Previous MI 8.5 (n=6,422)
8.8 (n=7,665)
8.7 (n=9,510)
9.0 (n=10,016)
8.9 (n=10,595)
Pre
vio
us
MI
Unconfirmed 8.1 (n=1,088)
8.7 (n=1,218)
8.8 (n=272)
8.6 (n=364)
10.3 (n=447)
Isolated CABG: Average post-operative stay by previous MI; bars denote standard errors (n=96,667)
No MI Previous MI
7.8
8.0
8.2
8.4
8.6
8.8
9.0
9.2
1999 2000 2001 2002 2003
Financial year
Ave
rag
e p
ost
-op
erat
ive
stay
/ d
ays

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
128
NA
CSD
– C
AB
G s
urg
ery
risk
fact
ors
Number of previous MIs
Almost a half (50%) of all patients have had a heart attack before having coronary surgery. One-in-twenty patients have had two or more.
Financial year
1996 1997 1998 1999 2000 2001 2002 2003
None 2,019 3,488 5,761 7,918 9,537 11,059 12,123 13,920
One 1,416 2,293 4,233 4,827 6,259 7,460 7,965 8,418
Two or more 406 389 650 943 1,197 1,435 1,486 1,473
Nu
mb
er o
f p
revi
ou
s M
Is
Unconfirmed 1,170 1,974 2,820 2,773 2,347 2,095 1,852 2,200
Isolated CABG: Number of previous MIs (n=116,675)
None One Two or more
0%
10%
20%
30%
40%
50%
60%
1996 1997 1998 1999 2000 2001 2002 2003
Financial year
Per
cen
tag
e o
f pat
ien
ts

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
129
NA
CSD
– CA
BG
surg
ery risk factors
Mortality and number of previous MIs
Since heart attacks weaken the heart it is not surprising that the operative risk of surgery increases with each heart attack.
Financial year
1999 2000 2001 2002 2003
None 2.0% (n=7,915)
1.8% (n=9,532)
1.8% (n=11,048)
1.6% (n=12,044)
1.5% (n=13,882)
One 2.9% (n=4,825)
2.5% (n=6,259)
2.5% (n=7,455)
2.6% (n=7,893)
2.4% (n=8,392)
Two or more 4.0% (n=943)
4.3% (n=1,197)
5.0% (n=1,434)
4.5% (n=1,469)
3.1% (n=1,468) N
um
ber
of
pre
vio
us
MI
Unconfirmed 2.3% (n=2,773)
2.3% (n=2,347)
2.7% (n=2,095)
1.7% (n=1,808)
2.5% (n=2,192)
Isolated CABG: Mortality by number of previous MIs (n=95,756)
None One Two or more
0%
1%
2%
3%
4%
5%
6%
7%
1999 2000 2001 2002 2003
Financial year
Cru
de
mo
rtal
ity
rate

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
130
NA
CSD
– C
AB
G s
urg
ery
risk
fact
ors
Timing of the most recent MI
The preceding few pages have shown that almost a half of patients have suffered a heart attack at some point prior to coronary surgery. The vast majority of these heart attacks occurred over one month prior to surgery. However, a small percentage of patients have suffered a heart attack within one month of their surgery, and a tiny number will have required urgent or emergency surgery with 24 hours of their heart attack.
The timing of surgery in relation to the timing of the most recent heart attack has a profound effect on the results of surgery. Surgery within 24 hours of a heart attack is extremely risky, and is generally reserved for patients where there is no other alternative. Most surgeons’ preference is to delay surgery until the heart has had time to recover from the insult of a heart attack, because the heart is then healthier and the risk of surgery considerably lessened.
This point is clearly demonstrated on the following page.
Financial year
1999 2000 2001 2002 2003
No MI 7,918 9537 1,1059 12,123 1,3920
<6 hours 29 41 45 39 35
6-24 hours 61 60 76 58 64
1-30 days 956 1,108 1,281 1,396 1,639
>30 days 4,245 5,210 6,659 6,397 7,074
Last MI timing unconfirmed 1,243 1,719 2,092 2,450 2,261 Tim
ing
of l
ast
MI
Previous MI unconfirmed 2,009 1,665 837 963 1,018
Isolated CABG: Timing of the most recent MI (n=91,030)
<6 hours 6-24 hours 1-30 days >30 days
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
1999 2000 2001 2002 2003
Financial year
Per
cen
tag
e o
f pat
ien
ts w
ho
hav
e h
ad
a M
I an
d t
imin
g is
kn
ow
n

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
131
NA
CSD
– CA
BG
surg
ery risk factors
Mortality by timing of the most recent MI
The second chart demonstrates that, over the last 5 years at least, the difference in post-operative mortality between MIs that are less than 6 hours old and MIs that are 6-24 hours old is marginal. The overall picture demonstrates that surgery within 24 hours of a prior MI is extremely risky: approximately 11 times the risk for patients who have not had any prior MI and 7 times the risk for patients who had their last MI more than 30 days before their coronary surgery.
Isolated CABG: Crude mortality by timing of last MI (n=93,473)
No MI <1 day 1-30 days >30 days
Isolated CABG: Crude mortality by timing of last MI; financial years 1999-2003 (n=36,463)
0%
2%
4%
6%
8%
10%
12%
14%
16%
18%
20%
<6 hours 6-24 hours 1-30 days >30 days
Time since last MI
Cru
de
mo
rtal
ity
rate
0%
5%
10%
15%
20%
25%
1999 2000 2001 2002 2003
Time since last MI
Cru
de
mo
rtal
ity
rate

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
132
NA
CSD
– C
AB
G s
urg
ery
risk
fact
ors
Percutaneous coronary intervention (PCI)
Timing of prior PCI
Medical technology has advanced considerably over the last few years and it is now possible to treat a substantial number of patients without surgery. One option involves passing a special type of balloon into the narrowing of a coronary artery, inflating the balloon to widen the narrowing and then splinting the widened artery open with a stent. This type of procedure is generally referred to as Percutaneous Transluminal Coronary Angioplasty (PTCA), or, increasingly, Percutaneous Coronary Intervention (PCI). These sorts of procedures are now extremely successful and safe, and patients only have to spend a day or two in hospital after which they can immediately resume normal activities.
Numbers of PCI and CABG procedures; data from BCIS and SCTS (n=578,810)
PCI CABG
In many cases this procedure will eliminate the need for surgery, in some it will delay the need for some years. In a few, the procedure will precipitate problems necessitating urgent or emergency surgery. The proportion of patients requiring urgent surgery is steadily falling. The graph below shows that where the percentage of patients undergoing PCI within 24 hours of surgery has been recorded, it has fallen by 50% from 1% to less than 0.5% of surgical practice over the last 8 years; this is against a background of an ever-increasing numbers of patients having PCI. However, if urgent surgery is required the operative mortality remains high at about 10-15%.
0
5
10
15
20
25
30
35
40
45
50
1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003
Financial year
Nu
mb
er o
f pro
ced
ure
s / t
ho
usa
nd
s

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
133
NA
CSD
– CA
BG
surg
ery risk factors
Isolated CABG: Previous PCI and timing of failed PCI (n=111,729)
PCI <=24 hours before surgery
PCI >24 hours before surgery
PCI timing unknown
Mortality by timing of prior PCI
The table below clearly outlines the difference in operative mortality between patients requiring urgent versus delayed surgery following previous cardiological intervention for coronary disease.
Financial year
1999 2000 2001 2002 2003
No PCI 2.3% (n=12,422)
2.1% (n=14,997)
2.2% (n=18,227)
2.0% (n=19,619)
1.9% (n=21,413)
PCI ≤24 hours before surgery
11.1% (n=45)
16.2% (n=37)
19.5% (n=41)
14.0% (n=43)
11.4% (n=44)
PCI >24 hours before surgery
3.2% (n=31)
0.0% (n=44)
0.0% (n=34)
2.8% (n=72)
3.2% (n=62)
PCI timing unknown 3.0% (n=605)
2.6% (n=833)
2.8% (n=1,022)
2.9% (n=1,186)
1.6% (n=1,346) O
per
ativ
e p
rio
rity
Unconfirmed 2.7% (n=3,353)
2.3% (n=3,424)
2.4% (n=2,708)
1.9% (n=2,294)
2.3% (n=3,069)
0%
1%
2%
3%
4%
5%
6%
1996 1997 1998 1999 2000 2001 2002 2003
Financial year
Per
cen
tag
e o
f pat
ien
ts

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
134
NA
CSD
– C
AB
G s
urg
ery
risk
fact
ors
Left main stem (LMS) disease
Key points from the left main stem disease analyses
• Left main stem disease is associated with poorer outcomes.
• Patients with left main stem disease are almost twice as likely to die after their operation.
• Patients with left main stem disease stay longer in hospital after their operation.
• The difference in post-operative stay for patients with and without left main stem disease has increased over the last 4 years.
LMS disease distributions
The proportion of patients with left main stem disease has increased over the last 5 years, from 13.4-21.4%, which represents a 60% increase. The reasons for this increase are unclear but might be due to the fact that more and more patients without left main stem disease are having narrowings in their coronary arteries treated with angioplasty rather than surgery.
Surgery is still the preferred treatment option for patients with left main stem disease.
Financial year
1996 1997 1998 1999 2000 2001 2002 2003
No LMS disease 3,805 5,072 9,455 12,562 13,224 16,170 17,013 17,661
LMS disease 660 738 1,401 1,937 2,814 3,462 3,871 5,006
LMS
dis
ease
Unconfirmed 546 2,334 2,608 1,962 3,302 2,417 2,542 3,344
Isolated CABG: LMS disease (n=114,851)
No LMS LMS disease
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
1996 1997 1998 1999 2000 2001 2002 2003
Financial year
Per
cen
tag
e o
f pat
ien
ts

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
135
NA
CSD
– CA
BG
surg
ery risk factors
Mortality and LMS disease
The reductions in mortality over the last few years are most likely to be associated with improvements in both surgical techniques and post-operative care.
Financial year
1999 2000 2001 2002 2003
No LMS disease 2.3% (n=12,558)
2.0% (n=13,222)
2.0% (n=16,162)
1.8% (n=17,012)
1.6% (n=17,611)
LMS disease 3.6% (n=1,936)
3.3% (n=2,814)
3.6% (n=3,459)
3.3% (n=3,871)
3.0% (n=5,003)
LMS
dis
ease
Unconfirmed 2.7% (n=1,962)
2.3% (n=3,299)
2.4% (n=2,411)
2.1% (n=2,331)
2.4% (n=3,316)
Isolated CABG: Crude mortality by LMS disease (n=63,652)
No LMS disease LMS disease
0.0%
0.5%
1.0%
1.5%
2.0%
2.5%
3.0%
3.5%
4.0%
4.5%
5.0%
1999 2000 2001 2002 2003
Financial year
Cru
de
mo
rtal
ity
rate

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
136
NA
CSD
– C
AB
G s
urg
ery
risk
fact
ors
LMS disease and NHS centres
Isolated CABG: LMS disease by centre for financial year 2003 (n=21,903)
No LMS disease LMS disease
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Edinburgh Royal Infirmary
Freeman Hospital Newcastle
Glenfield Hospital Leicester
St George's Hospital London
Castle Hill Hospital Hull
Glasgow Royal Infirmary
Walsgrave Hospital Coventry
Royal Victoria Hospital Belfast
Southampton General Hospital
Harefield Hospital London
Wythenshawe Hospital M anchester
Barts and the London
St James's Hospital Dublin
University Hospital o f Wales Cardiff
Derriford Hospital P lymouth
Royal Brompton Hospital London
Queen Elizabeth Hospital B irmingham
Bristo l Royal Infirmary
N Staffordshire Royal Infirmary
King's College Hospital London
Cardiothoracic Centre Liverpool
Victoria Hospital B lackpool
Aberdeen Royal Infirmary
The Heart Hospital London
Guy's & St Thomas' Hospitals London
Leeds General Infirmary
M anchester Royal Infirmary
Glasgow Western Infirmary
Royal Sussex County Hospital
Nottingham City Hospital
James Cook Uni Hosp'l M iddlesbrough
Northern General Hospital Sheffield
M orriston Hospital Swansea
Hammersmith Hospital London
St M ary's Hospital London
Papworth Hospital
John Radcliffe Hospital Oxford
Golden Jubilee Hospital Glasgow
Cen
tre
Percentage of patients

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
137
NA
CSD
– CA
BG
surg
ery risk factors
Missing, unconfirmed or unmapped LMS disease data
Isolated CABG: LMS disease data by centre for financial year 2003 (n=25,067)
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Wythenshawe Hospital M anchester
Walsgrave Hospital Coventry
St James's Hospital Dublin
Royal Brompton Hospital London
Queen Elizabeth Hospital B irmingham
N Staffordshire Royal Infirmary
M anchester Royal Infirmary
Glasgow Western Infirmary
Edinburgh Royal Infirmary
Cardiothoracic Centre Liverpool
Victoria Hospital B lackpool
Southampton General Hospital
Guy's & St Thomas' Hospitals London
Castle Hill Hospital Hull
Derriford Hospital P lymouth
Aberdeen Royal Infirmary
Freeman Hospital Newcastle
Nottingham City Hospital
Royal Sussex County Hospital
University Hospital o f Wales Cardiff
The Heart Hospital London
Glasgow Royal Infirmary
King's College Hospital London
James Cook Uni Hosp'l M iddlesbrough
St George's Hospital London
Hammersmith Hospital London
Harefield Hospital London
M orriston Hospital Swansea
Northern General Hospital Sheffield
Leeds General Infirmary
Bristo l Royal Infirmary
Barts and the London
Glenfield Hospital Leicester
Royal Victoria Hospital Belfast
St M ary's Hospital London
Papworth Hospital
John Radcliffe Hospital Oxford
Golden Jubilee Hospital Glasgow
Cen
tre
Percentage entries with missing data

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
138
NA
CSD
– C
AB
G s
urg
ery
risk
fact
ors
LMS disease and private centres; LMS and country
In line with many of the previous analyses, the incidence of left main stem disease is different between the NHS and private-patient populations.
Isolated CABG: LMS disease by centre for financial year 2003 (Private Hospital n=764)
No LMS disease LMS disease
Isolated CABG: LMS disease by country for financial year 2003 (n=21,903)
No LMS disease LMS disease
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
All NHS
All private
London Bridge Hospital
BUPA Hospital Bristol
BUPA Hospital Washington
BUPA Cambridge Lea Hospital
The Harley Street Clinic
BUPA Chalybeate Southampton
BUPA Hospital Leicester
Cen
tre
Percentage of patients
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Ireland
Scotland
England
Wales
Co
un
try
Percentage of patients

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
139
NA
CSD
– CA
BG
surg
ery risk factors
LMS disease and post-operative stay
Patients with left main stem disease stay longer in hospital after their operation.
The difference in post-operative stay for patients with and without left main stem disease has increased over the last 4 years
Financial year
1999 2000 2001 2002 2003
No LMS disease 8.2 (n=11,256)
8.5 (n=11,959)
8.3 (n=15,025)
8.5 (n=16,163)
8.5 (n=17,168)
LMS disease 8.6 (n=1,683)
8.8 (n=2,611)
8.7 (n=3,260)
9.1 (n=3,705)
9.1 (n=4,707)
LMS
dis
ease
Unconfirmed 8.4 (n=1,929)
8.5 (n=3,260)
8.6 (n=2,292)
8.6 (n=2,400)
9.1 (n=2,638)
Isolated CABG: Average post-operative stay by LMS disease; bars denote standard errors (n=87,537)
No LMS LMS disease
8.0
8.2
8.4
8.6
8.8
9.0
9.2
9.4
1999 2000 2001 2002 2003
Financial year
Ave
rag
e p
ost
-op
erat
ive
stay
/ d
ays

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
140
NA
CSD
– C
AB
G s
urg
ery
risk
fact
ors
Previous surgery
Key points from the previous heart surgery analyses
• The percentage of patients who had had some kind of previous heart surgery steadily fell over the last 4 years from 3.9% to 2.5%.
• Previous heart surgery remains a major risk factor, increasing the risk of post-operative death around three-fold.
• Most patients who had had a previous cardiac operation had their first operation over six years earlier.
• In recent years previous heart surgery has been associated with an increased and increasing post-operative stay.
Previous surgery distributions
Following a heart operation the heart becomes encased in scar tissue. This makes a re-operation technically more challenging for the surgeon and more risky for the patient. Over the years the number of patients undergoing repeat heart surgery has remained relatively constant at 3-4%. However, there is a striking variation between centres. On an encouraging note, the operative mortality for repeat surgery appears to be falling as surgical techniques improve, nevertheless it still attracts a three-fold increase in operative mortality.
Financial year
1996 1997 1998 1999 2000 2001 2002 2003
No previous surgery 4,436 7,277 12,400 15,429 18,365 20,384 22,508 25,030
Previous surgery 146 289 502 630 642 681 655 640
Pre
vio
us
surg
ery
Unconfirmed 429 578 562 402 333 984 263 341
Isolated CABG: Previous surgery (n=130,014)
No previous surgery Previous surgery
80%
82%
84%
86%
88%
90%
92%
94%
96%
98%
100%
1996 1997 1998 1999 2000 2001 2002 2003
Financial year
Per
cen
tag
e o
f pat
ien
ts

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
141
NA
CSD
– CA
BG
surg
ery risk factors
Mortality and previous surgery
Previous heart surgery remains a major risk factor, increasing the risk of post-operative death about three-fold.
This is related to the fact that after surgery the heart become encased in scar tissue and is sometimes adherent to the back of the sternum (or breastbone) making reopening of the sternum very hazardous. Even when the reopening is successful the heart structures, including the coronary arteries can sometimes be extremely difficult to identify. Added to this is the fact that the patient’s coronary artery disease is always worse at the re-operation than it was at the first operation.
Financial year
1999 2000 2001 2002 2003
No previous surgery 2.2% (n=15,424)
2.1% (n=18,363)
2.1% (n=20,375)
2.0% (n=22,333)
1.9% (n=24,959)
Previous surgery 7.8% (n=630)
5.8% (n=642)
7.3% (n=681)
4.4% (n=655)
6.4% (n=640)
Pre
vio
us
surg
ery
Unconfirmed 2.2% (n=402)
3.6% (n=330)
3.0% (n=976)
3.1% (n=226)
2.7% (n=335)
Isolated CABG: Crude mortality by previous surgery (n=104,702)
No previous surgery Previous surgery
0%
2%
4%
6%
8%
10%
12%
1999 2000 2001 2002 2003
Financial year
Cru
de
mo
rtal
ity
rate

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
142
NA
CSD
– C
AB
G s
urg
ery
risk
fact
ors
Previous surgery and NHS centres
Isolated CABG: Previous surgery by centre for financial year 2003 (n=24,740)
No previous surgery Previous surgery
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
John Radcliffe Hospital Oxford
Wythenshawe Hospital M anchester
Royal Victoria Hospital Belfast
Aberdeen Royal Infirmary
N Staffordshire Royal Infirmary
Queen Elizabeth Hospital B irmingham
Derriford Hospital P lymouth
Northern General Hospital Sheffield
Leeds General Infirmary
Glasgow Western Infirmary
King's College Hospital London
The Heart Hospital London
James Cook Uni Hosp'l M iddlesbrough
Edinburgh Royal Infirmary
M orriston Hospital Swansea
Victoria Hospital B lackpool
Castle Hill Hospital Hull
Royal Sussex County Hospital
Glasgow Royal Infirmary
Bristo l Royal Infirmary
Nottingham City Hospital
Cardio thoracic Centre Liverpool
St George's Hospital London
Papworth Hospital
St James's Hospital Dublin
Barts and the London
University Hospital o f Wales Cardiff
Walsgrave Hospital Coventry
Guy's & St Thomas' Hospitals London
Glenfield Hospital Leicester
Royal Brompton Hospital London
Hammersmith Hospital London
Golden Jubilee Hospital Glasgow
Freeman Hospital Newcastle
Harefield Hospital London
Southampton General Hospital
M anchester Royal Infirmary
St M ary's Hospital London
Cen
tre
Percentage of patients

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
143
NA
CSD
– CA
BG
surg
ery risk factors
Missing, unconfirmed or unmapped previous surgery data
Isolated CABG: Missing previous surgery data by centre for financial year 2003 (n=25,067)
0% 5% 10% 15% 20% 25%
Wythenshawe Hospital M anchester
Walsgrave Hospital Coventry
University Hospital o f Wales Cardiff
St George's Hospital London
Royal Sussex County Hospital
Royal Brompton Hospital London
Queen Elizabeth Hospital B irmingham
Papworth Hospital
Nottingham City Hospital
M anchester Royal Infirmary
James Cook Uni Hosp'l M iddlesbrough
Glasgow Royal Infirmary
Castle Hill Hospital Hull
Cardio thoracic Centre Liverpool
Aberdeen Royal Infirmary
N Staffordshire Royal Infirmary
Glasgow Western Infirmary
Victoria Hospital B lackpool
Glenfield Hospital Leicester
Edinburgh Royal Infirmary
St James's Hospital Dublin
Freeman Hospital Newcastle
Leeds General Infirmary
The Heart Hospital London
Royal Victoria Hospital Belfast
Hammersmith Hospital London
Bristo l Royal Infirmary
Southampton General Hospital
Guy's & St Thomas' Hospitals London
Golden Jubilee Hospital Glasgow
Northern General Hospital Sheffield
Derriford Hospital P lymouth
King's College Hospital London
St M ary's Hospital London
Harefield Hospital London
Barts and the London
M orriston Hospital Swansea
John Radcliffe Hospital Oxford
Cen
tre
Percentage entries with missing data

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
144
NA
CSD
– C
AB
G s
urg
ery
risk
fact
ors
Previous surgery and private centres; Previous surgery and country
Isolated CABG: Previous surgery by centre for financial year 2003 (Private Hospital n=930)
No previous surgery Previous surgery
Isolated CABG: Previous surgery by country for financial year 2003 (n=24,740)
No previous surgery Previous surgery
0% 20% 40% 60% 80% 100%
All NHS
All private
BUPA Hospital Washington
BUPA Cambridge Lea Hospital
BUPA Hospital Bristol
BUPA Hospital Leicester
London Bridge Hospital
BUPA Chalybeate Southampton
The Harley Street Clinic
Cen
tre
Percentage of patients
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Wales
England
Ireland
Scotland
Co
un
try
Percentage of patients

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
145
NA
CSD
– CA
BG
surg
ery risk factors
Previous surgery and post-operative stay
Although repeat coronary operations are more difficult as reflected by the increased operative mortality, the average post-operative length-of-stay is only one day greater than that for patients having their first operation.
Financial year
1999 2000 2001 2002 2003
No previous surgery 8.2 (n=14,150)
8.5 (n=17,052)
8.4 (n=19,809)
8.6 (n=21,451)
8.6 (n=23,652)
Previous surgery 9.7 (n=596)
9.6 (n=593)
9.1 (n=670)
9.3 (n=623)
9.8 (n=584)
Pre
vio
us
surg
ery
Unconfirmed 7.7 (n=122)
8.9 (n=185)
7.9 (n=98)
8.7 (n=194)
9.4 (n=277)
Isolated CABG: Average post-operative stay by previous surgery; bars denote standard errors (n=99,180)
No previous surgery Previous surgery
8.0
8.5
9.0
9.5
10.0
10.5
1999 2000 2001 2002 2003
Financial year
Ave
rag
e p
ost
-op
erat
ive
stay
/ d
ays

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
146
NA
CSD
– C
AB
G s
urg
ery
risk
fact
ors
Timing of previous surgery
Coronary artery disease can be treated by medications, cardiological interventions or surgery. The nature of surgery is explained on pages 36-38. The success of a coronary operation depends on the extent of disease in the original coronary arteries and how well the bypass grafts bear up over time. The graph below illustrates a number of points.
Firstly, a small proportion of patients require a repeat operation within one year. This is not surprising given the complex technical aspects of surgery involving stitching bypass grafts onto arteries that are only 1 to 2 mm in diameter and are, in many cases, both diseased and friable.
Secondly, and most encouragingly, the graph demonstrates that the vast majority of patients undergoing repeat surgery do so seven or more years after the first operation, most commonly 10-12 years later. This is in keeping with the best results published in the international literature.
These data are based on patients undergoing surgery some years ago, but things have changed. There is an increasing use of one or more arterial grafts and drug therapy after surgery has improved considerably. It is therefore reasonable to assume that the longevity of bypass grafts will continue to improve.
Isolated CABG: Time from previous cardiac operation to current CABG operation (n=2,294)
The chart on the following page takes the same data and presents it in a different fashion; it is easier to see how long it is before 50% of all recorded re-operations have been performed (approximately 11 years after the previous operation).
0%
1%
2%
3%
4%
5%
6%
7%
8%
9%
0 1 2 3 4 5 6 7 8 9
10 11 12 13 14 15 16 17 18 19 20 21 22
>22
Time from previous cardiac operation / years
Per
cen
tag
e o
f re-
op
erat
ion
s

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
147
NA
CSD
– CA
BG
surg
ery risk factors
The frequency distribution plot shown below is simply another way of presenting the same data plotted in the chart on the previous page. It makes it easier to visualise the time by which any given proportion of re-operations have been performed; for example 50% of all re-operations had occurred by 11 years.
Isolated CABG: Time from previous cardiac operation to current CABG operation (n=2,294)
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
0 2 4 6 8
10 12 14 16 18 20 22
Time from previous cardiac operation / years
Cu
mu
lati
ve p
erce
nta
ge
of r
e-o
per
atio
ns

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
148
NA
CSD
– C
AB
G s
urg
ery
risk
fact
ors
Diabetes
Key points from the diabetes analyses
• A little over one fifth of patients undergoing coronary surgery had diabetes.
• Over the last seven years the proportion of patients undergoing coronary surgery presenting with diabetes has increased by fifty percent.
• Despite the effects of diabetes on coronary artery disease, improved post-operative management has decreased the impact of diabetes on outcome; over the past six year the post-operative mortality rate for diabetic patients has more than halved.
• Diabetics tend to spend 1.5 days longer in hospital than patients who do not have diabetes.
Diabetes distributions
Diabetes is a serious condition in which the body cannot utilise glucose efficiently. Glucose is the main food substance of cells in the body. A naturally occurring hormone called insulin enables glucose to enter cells where it is used. Diabetic patients do not produce enough insulin, so glucose cannot enter the body’s cells efficiently. Diabetes may lead to significant health problems such as heart disease, stroke, renal failure, peripheral vascular disease and sometimes blindness.
Diabetes is becoming a more common condition worldwide; this is reflected in the steadily increasing percentage of patients with diabetes undergoing coronary surgery. It can affect people of all ages in every population; socially disadvantaged groups in affluent societies and people from certain ethnic communities (especially those of South Asian, African and Afro-Caribbean descent) are particularly prone to diabetes.
Financial year
1996 1997 1998 1999 2000 2001 2002 2003
No diabetes 3,821 6,438 10,400 12,790 14,851 17,546 18,588 20,087
Diabetes 652 1,061 1,882 2,592 3,139 3,880 4,654 5,592
Dia
bet
es
Unconfirmed 538 645 1,182 1,079 1,350 623 184 332
Isolated CABG: Diabetes (n=127,973)
No diabetes Diabetes
60%
65%
70%
75%
80%
85%
90%
95%
100%
1996 1997 1998 1999 2000 2001 2002 2003
Financial year
Per
cen
tag
e o
f pat
ien
ts

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
149
NA
CSD
– CA
BG
surg
ery risk factors
Mortality and diabetes
There has been a marked improvement in the outcome of coronary surgery for diabetics over the last six with a 52% reduction in mortality from 5.4% to 2.6%
Financial year
1997 1998 1999 2000 2001 2002 2003
No diabetes 2.9% (n=6,433)
2.3% (n=10,398)
2.3% (n=12,786)
2.1% (n=14,850)
2.2% (n=17,539)
1.9% (n=18,435)
1.8% (n=20,028)
Diabetes 5.4% (n=1,060)
3.8% (n=1,881)
3.2% (n=2,591)
2.9% (n=3,138)
3.0% (n=3,878)
3.0% (n=4,604)
2.6% (n=5,577)
Dia
bet
es
Unconfirmed 2.6% (n=645)
3.0% (n=1,182)
2.6% (n=1,079)
1.9% (n=1,347)
2.8% (n=615)
2.3% (n=175)
1.5% (n=329)
Isolated CABG: Crude mortality by diabetes (n=123,198)
No diabetes Diabetes
0%
1%
2%
3%
4%
5%
6%
7%
1997 1998 1999 2000 2001 2002 2003
Financial year
Cru
de
mo
rtal
ity
rate

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
150
NA
CSD
– C
AB
G s
urg
ery
risk
fact
ors
Diabetes and NHS centres
Isolated CABG: Diabetes by centre for financial year 2003 (n=24,778)
No diabetes Diabetes
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Aberdeen Royal Infirmary
St James's Hospital Dublin
Royal Victoria Hospital Belfast
Glasgow Royal Infirmary
Victoria Hospital B lackpool
Northern General Hospital Sheffield
Golden Jubilee Hospital Glasgow
Edinburgh Royal Infirmary
Derriford Hospital P lymouth
N Staffordshire Royal Infirmary
Bristo l Royal Infirmary
Glasgow Western Infirmary
Castle Hill Hospital Hull
Papworth Hospital
Southampton General Hospital
James Cook Uni Hosp'l M iddlesbrough
Wythenshawe Hospital M anchester
Royal Sussex County Hospital
Nottingham City Hospital
Guy's & St Thomas' Hospitals London
M orriston Hospital Swansea
M anchester Royal Infirmary
King's College Hospital London
Cardiothoracic Centre Liverpool
Harefield Hospital London
Freeman Hospital Newcastle
Glenfield Hospital Leicester
University Hospital o f Wales Cardiff
Leeds General Infirmary
Walsgrave Hospital Coventry
John Radcliffe Hospital Oxford
Barts and the London
Queen Elizabeth Hospital B irmingham
The Heart Hospital London
St George's Hospital London
Royal Brompton Hospital London
Hammersmith Hospital London
St M ary's Hospital London
Cen
tre
Percentage of patients

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
151
NA
CSD
– CA
BG
surg
ery risk factors
Missing, unconfirmed or unmapped diabetes data
Isolated CABG: Missing diabetes data by centre for financial year 2003 (n=25,067)
0% 5% 10% 15% 20% 25% 30% 35% 40%
Wythenshawe Hospital M anchester
Walsgrave Hospital Coventry
St James's Hospital Dublin
Southampton General Hospital
Royal Sussex County Hospital
Royal Brompton Hospital London
Queen Elizabeth Hospital B irmingham
Papworth Hospital
Northern General Hospital Sheffield
N Staffordshire Royal Infirmary
M anchester Royal Infirmary
Harefield Hospital London
Hammersmith Hospital London
Guy's & St Thomas' Hospitals London
Glasgow Western Infirmary
Edinburgh Royal Infirmary
Derriford Hospital P lymouth
Cardiothoracic Centre Liverpool
Victoria Hospital B lackpool
Aberdeen Royal Infirmary
Leeds General Infirmary
Freeman Hospital Newcastle
Glasgow Royal Infirmary
James Cook Uni Hosp'l M iddlesbrough
Bristo l Royal Infirmary
Castle Hill Hospital Hull
The Heart Hospital London
John Radcliffe Hospital Oxford
University Hospital o f Wales Cardiff
King's College Hospital London
Golden Jubilee Hospital Glasgow
St M ary's Hospital London
Nottingham City Hospital
St George's Hospital London
Barts and the London
M orriston Hospital Swansea
Glenfield Hospital Leicester
Royal Victoria Hospital Belfast
Cen
tre
Percentage entries with missing data

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
152
NA
CSD
– C
AB
G s
urg
ery
risk
fact
ors
Diabetes and private centres; Diabetes and country
Isolated CABG: Diabetes by centre for financial year 2003 (Private Hospital n=901)
No diabetes Diabetes
Isolated CABG: Diabetes by country for financial year 2003 (n= 24,778)
No diabetes Diabetes
0% 20% 40% 60% 80% 100%
All NHS
All private
BUPA Hospital Washington
BUPA Cambridge Lea Hospital
BUPA Hospital Bristol
BUPA Chalybeate Southampton
The Harley Street Clinic
BUPA Hospital Leicester
London Bridge Hospital
Cen
tre
Percentage of patients
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
England
Wales
Scotland
Ireland
Co
un
try
Percentage of patients

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
153
NA
CSD
– CA
BG
surg
ery risk factors
Diabetes and post-operative stay
In general, diabetics tend to spend a day and a half longer in hospital than non-diabetics which has resource management implications given the ever-growing proportion of diabetic patients undergoing coronary surgery.
Financial year
1999 2000 2001 2002 2003
No diabetes 8.0 (n=12,217)
8.3 (n=13,963)
8.1 (n=16,695)
8.3 (n=17,706)
8.3 (n=19,148)
Diabetes 9.4 (n=2,455)
9.6 (n=2,960)
9.7 (n=3,703)
9.8 (n=4,441)
9.7 (n=5,182)
Dia
bet
es
Unconfirmed 10.4 (n=196)
8.8 (n=907)
10.3 (n=179)
8.6 (n=121)
11.8 (n=183)
Isolated CABG: Average post-operative stay by diabetes; bars denote standard errors (n=98,470)
No diabetes Diabetes
7.5
8.0
8.5
9.0
9.5
10.0
10.5
1999 2000 2001 2002 2003
Financial year
Ave
rag
e p
ost
-op
erat
ive
stay
/ d
ays

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
154
NA
CSD
– C
AB
G s
urg
ery
risk
fact
ors
Hypertension
Key points from the hypertension analyses
• There continues to be a slow but steady increase in the proportion of hypertensive patients over the last 8 years, from 44% to 65%; this probably represents a combination of the effects of a continually aging population and better diagnosis and treatment of hypertension.
• In the 2003 data the difference in mortality between hypertensive and non-hypertensive was almost abolished.
• Hypertension remains a minor risk factor for adverse post-operative outcomes.
Hypertension distributions
Financial year
1996 1997 1998 1999 2000 2001 2002 2003
No hypertension 2,402 3,969 6,380 7,316 7,944 8,995 8,757 9,003
Hypertension 2,087 3,551 5,939 8,065 10,013 12,540 14,516 16,616
Hyp
erte
nsi
on
Unconfirmed 522 624 1,145 1,080 1,383 514 153 392
Isolated CABG: Hypertension (n=128,093)
No hypertension Hypertension
0%
10%
20%
30%
40%
50%
60%
70%
1996 1997 1998 1999 2000 2001 2002 2003
Financial year
Per
cen
tag
e o
f pat
ien
ts

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
155
NA
CSD
– CA
BG
surg
ery risk factors
Mortality and hypertension
Financial year
1999 2000 2001 2002 2003
No hypertension 2.2% (n=7,314)
1.6% (n=7,944)
2.0% (n=8,991)
1.7% (n=8,677)
1.8% (n=8,979)
Hypertension 2.7% (n=8,062)
2.7% (n=10,011)
2.6% (n=12,533)
2.4% (n=14,400)
2.1% (n=16,568)
Hyp
erte
nsi
on
Unconfirmed 2.3% (n=1,080)
2.0% (n=1,380)
3.1% (n=508)
2.2% (n=137)
1.6% (n=387)
Isolated CABG: Crude mortality by hypertension (n=103,479)
No hypertension Hypertension
0.0%
0.5%
1.0%
1.5%
2.0%
2.5%
3.0%
3.5%
1999 2000 2001 2002 2003
Financial year
Cru
de
mo
rtal
ity
rate

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
156
NA
CSD
– C
AB
G s
urg
ery
risk
fact
ors
Hypertension and NHS centres
Isolated CABG: Hypertension by centre for financial year 2003 (n=24,729)
No hypertension Hypertension
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Royal Victoria Hospital Belfast
Glasgow Royal Infirmary
Northern General Hospital Sheffield
Edinburgh Royal Infirmary
Southampton General Hospital
St James's Hospital Dublin
N Staffordshire Royal Infirmary
Victoria Hospital B lackpool
Glasgow Western Infirmary
Leeds General Infirmary
University Hospital o f Wales Cardiff
Cardio thoracic Centre Liverpool
Golden Jubilee Hospital Glasgow
Bristo l Royal Infirmary
The Heart Hospital London
James Cook Uni Hosp'l M iddlesbrough
M anchester Royal Infirmary
Queen Elizabeth Hospital B irmingham
Derriford Hospital P lymouth
Papworth Hospital
M orriston Hospital Swansea
Aberdeen Royal Infirmary
Royal Sussex County Hospital
Freeman Hospital Newcastle
John Radcliffe Hospital Oxford
Nottingham City Hospital
Barts and the London
St George's Hospital London
Harefield Hospital London
Castle Hill Hospital Hull
Wythenshawe Hospital M anchester
Royal Brompton Hospital London
St M ary's Hospital London
King's College Hospital London
Guy's & St Thomas' Hospitals London
Hammersmith Hospital London
Glenfield Hospital Leicester
Walsgrave Hospital Coventry
Cen
tre
Percentage of patients

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
157
NA
CSD
– CA
BG
surg
ery risk factors
Missing, unconfirmed or unmapped hypertension data
Isolated CABG: Missing hypertension data by centre for financial year 2003 (n=25,067)
0% 5% 10% 15% 20% 25% 30% 35%
Wythenshawe Hospital M anchester
Walsgrave Hospital Coventry
St James's Hospital Dublin
Southampton General Hospital
Royal Sussex County Hospital
Royal Brompton Hospital London
Papworth Hospital
M anchester Royal Infirmary
James Cook Uni Hosp'l M iddlesbrough
Harefield Hospital London
Hammersmith Hospital London
Guy's & St Thomas' Hospitals London
Glasgow Western Infirmary
Freeman Hospital Newcastle
Edinburgh Royal Infirmary
Derriford Hospital P lymouth
Cardiothoracic Centre Liverpool
Victoria Hospital B lackpool
Aberdeen Royal Infirmary
Queen Elizabeth Hospital B irmingham
Bristo l Royal Infirmary
Leeds General Infirmary
The Heart Hospital London
Northern General Hospital Sheffield
Castle Hill Hospital Hull
N Staffordshire Royal Infirmary
Glasgow Royal Infirmary
University Hospital o f Wales Cardiff
St M ary's Hospital London
King's College Hospital London
Nottingham City Hospital
Golden Jubilee Hospital Glasgow
John Radcliffe Hospital Oxford
St George's Hospital London
Barts and the London
M orriston Hospital Swansea
Glenfield Hospital Leicester
Royal Victoria Hospital Belfast
Cen
tre
Percentage entries with missing data

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
158
NA
CSD
– C
AB
G s
urg
ery
risk
fact
ors
Hypertension and private centres; Hypertension and country
Isolated CABG: Hypertension by centre for financial year 2003 (Private Hospital n=890)
No hypertension Hypertension
Isolated CABG: Hypertension by country for financial year 2003 (n= 24,729)
No hypertension Hypertension
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
All NHS
All private
The Harley Street Clinic
BUPA Chalybeate Southampton
BUPA Hospital Washington
BUPA Cambridge Lea Hospital
BUPA Hospital Bristol
BUPA Hospital Leicester
London Bridge Hospital
Cen
tre
Percentage of patients
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
England
Wales
Scotland
Ireland
Co
un
try
Percentage of patients

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
159
NA
CSD
– CA
BG
surg
ery risk factors
Hypertension and post-operative stay
Although there is no significant difference in mortality between people with high or normal blood pressure, patients with high blood pressure tend to remain in hospital for a day longer.
Financial year
1999 2000 2001 2002 2003
No hypertension 8.0 (n=6,973)
8.2 (n=7,422)
8.1 (n=8,457)
8.0 (n=8,329)
8.2 (n=8,596)
Hypertension 8.4 (n=7,697)
8.7 (n=9,470)
8.6 (n=11,981)
8.9 (n=13,848)
8.9 (n=15,673)
Hyp
erte
nsi
on
Unconfirmed 10.8 (n=198)
8.9 (n=938)
10.1 (n=139)
9.5 (n=91)
11.0 (n=244)
Isolated CABG: Average post-operative stay by hypertension; bars denote standard errors (n=98,446)
No hypertension Hypertension
7.5
8.0
8.5
9.0
9.5
1999 2000 2001 2002 2003
Financial year
Ave
rag
e p
ost
-op
erat
ive
stay
/ d
ays

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
160
NA
CSD
– C
AB
G s
urg
ery
risk
fact
ors
Peripheral vascular disease (PVD)
Key points from the peripheral vascular disease analyses
• This condition is present in about 10% of coronary surgery patients.
• Generally, peripheral vascular disease is associated with a doubling in post-operative mortality rate.
• On average patients with peripheral vascular disease spend about 2 days longer in hospital after their operation.
PVD distributions
Peripheral vascular disease is a term used to describe the presence of blood vessel narrowings in arteries of the body other than the coronary arteries of the heart. The narrowings are caused by atheroma, which is deposition of fatty and cholesterol like substances in the walls of the arteries. Not everyone who has coronary artery disease will have peripheral vascular disease. However, when vascular disease is present it may affect the blood supply to the legs, the kidneys, the gut or the brain. This is relevant because there are quite large fluctuations in blood pressure during a heart operation and when the blood pressure drops the blood flow through tissues or organs affected by vascular disease will fall. This may result in temporary or permanent damage to parts of the body sensitive to reductions in blood flow e.g.s, the kidneys or brain.
Financial year
1996 1997 1998 1999 2000 2001 2002 2003
No PVD 2,645 5,566 9,763 11,994 14,839 18,131 20,027 22,426
PVD 396 605 1,080 1,587 1,805 2,421 2,682 3,099
PV
D
Unconfirmed 1,970 1,973 2,621 2,880 2,696 1,497 717 486
Isolated CABG: PVD (n=119,066)
No PVD PVD
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
1996 1997 1998 1999 2000 2001 2002 2003
Financial year
Per
cen
tag
e o
f pat
ien
ts

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
161
NA
CSD
– CA
BG
surg
ery risk factors
Mortality and PVD
For the reasons outlined on the previous page, patients with peripheral vascular disease are, on average, twice as likely to die than patients without diseased peripheral blood vessels.
Financial year
1999 2000 2001 2002 2003
No PVD 2.2% (n=11,991)
2.1% (n=14,837)
2.0% (n=18,125)
1.8% (n=19,874)
1.7% (n=22,360)
PVD 4.7% (n=1,585)
3.6% (n=1,805)
4.4% (n=2,420)
4.0% (n=2,647)
4.2% (n=3,094) P
VD
Unconfirmed 2.4% (n=2,880)
2.1% (n=2,693)
2.6% (n=1,487)
2.3% (n=693)
1.5% (n=480)
Isolated CABG: Crude mortality by PVD (n=98,738)
No PVD PVD
0%
1%
2%
3%
4%
5%
6%
1999 2000 2001 2002 2003
Financial year
Cru
de
mo
rtal
ity
rate

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
162
NA
CSD
– C
AB
G s
urg
ery
risk
fact
ors
PVD and NHS centres
Isolated CABG: PVD by centre for financial year 2003 (n=24,622)
No PVD PVD
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Nottingham City Hospital
Golden Jubilee Hospital Glasgow
Royal Brompton Hospital London
Royal Victoria Hospital Belfast
The Heart Hospital London
M orriston Hospital Swansea
Harefield Hospital London
Glasgow Royal Infirmary
N Staffordshire Royal Infirmary
St George's Hospital London
Glenfield Hospital Leicester
Bristo l Royal Infirmary
Derriford Hospital P lymouth
Barts and the London
Northern General Hospital Sheffield
Queen Elizabeth Hospital B irmingham
Papworth Hospital
Edinburgh Royal Infirmary
Walsgrave Hospital Coventry
Castle Hill Hospital Hull
Wythenshawe Hospital M anchester
Hammersmith Hospital London
Glasgow Western Infirmary
Cardiothoracic Centre Liverpool
Aberdeen Royal Infirmary
Southampton General Hospital
Victoria Hospital B lackpool
Royal Sussex County Hospital
James Cook Uni Hosp'l M iddlesbrough
M anchester Royal Infirmary
Freeman Hospital Newcastle
John Radcliffe Hospital Oxford
University Hospital o f Wales Cardiff
King's College Hospital London
Guy's & St Thomas' Hospitals London
St M ary's Hospital London
Leeds General Infirmary
St James's Hospital Dublin
Cen
tre
Percentage of patients

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
163
NA
CSD
– CA
BG
surg
ery risk factors
Missing, unconfirmed or unmapped PVD data
Isolated CABG: Missing PVD data by centre for financial year 2003 (n=25,067)
0% 5% 10% 15% 20% 25% 30% 35%
Wythenshawe Hospital M anchester
Walsgrave Hospital Coventry
University Hospital o f Wales Cardiff
St James's Hospital Dublin
St George's Hospital London
Southampton General Hospital
Royal Sussex County Hospital
Royal Brompton Hospital London
Papworth Hospital
M anchester Royal Infirmary
Guy's & St Thomas' Hospitals London
Glasgow Western Infirmary
Glasgow Royal Infirmary
Freeman Hospital Newcastle
Edinburgh Royal Infirmary
Derriford Hospital P lymouth
Cardiothoracic Centre Liverpool
Victoria Hospital B lackpool
James Cook Uni Hosp'l M iddlesbrough
Aberdeen Royal Infirmary
Bristo l Royal Infirmary
N Staffordshire Royal Infirmary
Harefield Hospital London
Castle Hill Hospital Hull
The Heart Hospital London
Leeds General Infirmary
Golden Jubilee Hospital Glasgow
King's College Hospital London
Northern General Hospital Sheffield
Nottingham City Hospital
Queen Elizabeth Hospital B irmingham
Hammersmith Hospital London
St M ary's Hospital London
M orriston Hospital Swansea
Barts and the London
John Radcliffe Hospital Oxford
Glenfield Hospital Leicester
Royal Victoria Hospital Belfast
Cen
tre
Percentage entries with missing data

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
164
NA
CSD
– C
AB
G s
urg
ery
risk
fact
ors
PVD and private centres; PVD and country
Isolated CABG: PVD by centre for financial year 2003 (Private Hospital n=903)
No PVD PVD
Isolated CABG: PVD by country for financial year 2003 (n=24,622)
No PVD PVD
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
All NHS
All private
BUPA Hospital Bristol
The Harley Street Clinic
BUPA Hospital Leicester
BUPA Hospital Washington
BUPA Cambridge Lea Hospital
BUPA Chalybeate Southampton
London Bridge Hospital
Cen
tre
Percentage of patients
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Ireland
England
Wales
Scotland
Co
un
try
Percentage of patients

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
165
NA
CSD
– CA
BG
surg
ery risk factors
PVD and post-operative stay
On average patients with peripheral vascular disease stay a day and a half longer in hospital after their operation than patients without peripheral vascular disease.
Financial year
1999 2000 2001 2002 2003
No PVD 8.1 (n=11,922)
8.3 (n=14,095)
8.2 (n=17,855)
8.4 (n=19,551)
8.4 (n=21,298)
PVD 9.1 (n=1,574)
10.2 (n=1,713)
9.8 (n=2,270)
10.2 (n=2,524)
10.2 (n=2,929) P
VD
Unconfirmed 8.5 (n=1,372)
8.9 (n=2,022)
9.7 (n=452)
9.7 (n=193)
10.8 (n=286)
Isolated CABG: Average post-operative stay by PVD; bars denote standard errors (n=95,731)
No PVD PVD
8.0
8.5
9.0
9.5
10.0
10.5
11.0
1999 2000 2001 2002 2003
Financial year
Ave
rag
e p
ost
-op
erat
ive
stay
/ d
ays

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
166
NA
CSD
– C
AB
G s
urg
ery
risk
fact
ors
Renal disease
Key points from the pre-operative renal disease analyses
• Just less than 2% of coronary surgery patients have some sort of kidney disease.
• The incidence, whilst small, has shown an increase over the last seven years.
• The presence of renal disease increases mortality-risk by five to six times.
• On average, patients with renal disease spend an extra five to six days in hospital after their operation; this is true even for mild renal impairment.
Renal disease distributions
The kidneys serve to excrete the body’s toxic waste products. If they are failing or functioning inefficiently then they do not excrete all the waste products, so the level of a substance in the blood called creatinine begins to climb. The normal level is less than 140 μmol l-1. For the purposes of this analysis a level greater than 200 μmol l-1 in the blood is considered elevated. As kidneys fail and the level reaches 500-700 μmol l-1 then dialysis with a kidney machine is required.
Financial year
1996 1997 1998 1999 2000 2001 2002 2003
No renal disease 2,912 5,903 10,305 14,008 15,922 18,832 20,801 22,724
Elevated creatinine 17 59 105 173 173 267 257 245
Dialysis 21 18 44 58 68 68 80 100
Other renal disease 0 11 5 12 14 18 22 32
Ren
al d
isea
se
Unconfirmed 2,061 2,153 3,005 2,210 3,163 2,864 2,266 2,910
Isolated CABG: Renal disease (n=113,274)
No renal disease Elevated creatinine
Dialysis Other renal disease
95%
96%
97%
98%
99%
100%
1996 1997 1998 1999 2000 2001 2002 2003
Financial year
Per
cen
tag
e o
f pat
ien
ts

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
167
NA
CSD
– CA
BG
surg
ery risk factors
Mortality and renal disease
Although coronary surgery for patients with renal disease is relatively uncommon, this condition has a profound effect on the patient’s survival and post-operative length-of-stay, as illustrated on the following pages. For this reason the impact of renal disease is taken into account in most risk stratification systems. It is clear that even a moderately elevated creatinine may be associated with post-operative difficulty.
The presence of renal disease increases the risk of mortality by five to six times.
Financial year
1999 2000 2001 2002 2003
No renal disease 2.2% (n=13,579)
2.0% (n=15,504)
2.1% (n=18,492)
1.9% (n=20,284)
1.8% (n=21,792)
Elevated creatinine 14.1% (n=156)
15.7% (n=159)
8.6% (n=245)
12.2% (n=246)
9.6% (n=240)
Dialysis 12.3% (n=57)
4.7% (n=64)
4.5% (n=66)
8.2% (n=73)
16.7% (n=90)
Other renal disease 0.0% (n=11)
0.0% (n=14)
22.2% (n=18)
0.0% (n=20)
0.0% (n=28)
Ren
al d
isea
se
Unconfirmed 2.9% (n=2,209)
2.6% (n=2,050)
3.6% (n=1,843)
3.1% (n=1,175)
3.1% (n=1,463)
Isolated CABG: Crude mortality by renal disease (n=91,047)
No renal disease Elevated creatinine Dialysis
0%
5%
10%
15%
20%
25%
1999 2000 2001 2002 2003
Financial year
Cru
de
mo
rtal
ity
rate

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
168
NA
CSD
– C
AB
G s
urg
ery
risk
fact
ors
Renal disease and NHS centres
Isolated CABG: Renal disease by centre for financial year 2003 (n=22,215)
No renal disease Elevated creatinine Dialysis Other renal disease
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
James Cook Uni Hosp'l M iddlesbrough
Walsgrave Hospital Coventry
John Radcliffe Hospital Oxford
St M ary's Hospital London
Glenfield Hospital Leicester
Barts and the London
University Hospital o f Wales Cardiff
Edinburgh Royal Infirmary
Glasgow Western Infirmary
Hammersmith Hospital London
Guy's & St Thomas' Hospitals London
Royal Victoria Hospital Belfast
Royal Brompton Hospital London
Castle Hill Hospital Hull
Southampton General Hospital
St George's Hospital London
Nottingham City Hospital
Freeman Hospital Newcastle
Bristo l Royal Infirmary
The Heart Hospital London
Royal Sussex County Hospital
Derriford Hospital P lymouth
Leeds General Infirmary
Queen Elizabeth Hospital B irmingham
St James's Hospital Dublin
Papworth Hospital
N Staffordshire Royal Infirmary
M orriston Hospital Swansea
Harefield Hospital London
Victoria Hospital B lackpool
Northern General Hospital Sheffield
King's College Hospital London
Wythenshawe Hospital M anchester
M anchester Royal Infirmary
Cardiothoracic Centre Liverpool
Golden Jubilee Hospital Glasgow
Glasgow Royal Infirmary
Aberdeen Royal Infirmary
Cen
tre
Percentage of patients

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
169
NA
CSD
– CA
BG
surg
ery risk factors
Missing, unconfirmed or unmapped renal disease data
Isolated CABG: Missing renal disease data by centre for financial year 2003 (n=25,067)
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
University Hospital o f Wales Cardiff
St George's Hospital London
Royal Brompton Hospital London
Queen Elizabeth Hospital B irmingham
Papworth Hospital
N Staffordshire Royal Infirmary
Harefield Hospital London
Hammersmith Hospital London
Guy's & St Thomas' Hospitals London
Edinburgh Royal Infirmary
Derriford Hospital P lymouth
Southampton General Hospital
Glasgow Western Infirmary
Castle Hill Hospital Hull
Freeman Hospital Newcastle
Northern General Hospital Sheffield
Bristo l Royal Infirmary
The Heart Hospital London
Wythenshawe Hospital M anchester
Victoria Hospital B lackpool
M anchester Royal Infirmary
St James's Hospital Dublin
St M ary's Hospital London
Nottingham City Hospital
Leeds General Infirmary
Cardiothoracic Centre Liverpool
Barts and the London
John Radcliffe Hospital Oxford
Glenfield Hospital Leicester
King's College Hospital London
Royal Sussex County Hospital
M orriston Hospital Swansea
Walsgrave Hospital Coventry
Royal Victoria Hospital Belfast
James Cook Uni Hosp'l M iddlesbrough
Aberdeen Royal Infirmary
Glasgow Royal Infirmary
Golden Jubilee Hospital Glasgow
Cen
tre
Percentage entries with missing data

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
170
NA
CSD
– C
AB
G s
urg
ery
risk
fact
ors
Renal disease and private centres; Renal disease and country
Isolated CABG: Renal disease by centre for financial year 2003 (Private Hospital n=886)
No renal disease Elevated creatinine Dialysis Other renal disease
Isolated CABG: Renal disease by country for financial year 2003 (n=22,215)
No renal disease Elevated creatinine Dialysis Other renal disease
80% 82% 84% 86% 88% 90% 92% 94% 96% 98% 100%
Scotland
Wales
Ireland
England
Co
un
try
Percentage of patients
80% 84% 88% 92% 96% 100%
All NHS
All private
The Harley Street Clinic
BUPA Hospital Washington
BUPA Cambridge Lea Hospital
BUPA Hospital Bristol
BUPA Hospital Leicester
BUPA Chalybeate Southampton
London Bridge Hospital
Cen
tre
Percentage of patients

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
171
NA
CSD
– CA
BG
surg
ery risk factors
Renal disease and post-operative stay
On average, patients with renal disease spend an extra five to six days in hospital after their operation; this is true even for mild renal impairment.
Financial year
1999 2000 2001 2002 2003
No renal disease 8.1 (n=13,865)
8.4 (n=15,059)
8.3 (n=18,615)
8.4 (n=20,400)
8.5 (n=21,451)
Elevated creatinine 12.1 (n=161)
13.6 (n=164)
13.6 (n=244)
16.0 (n=244)
14.0 (n=220)
Dialysis 7.6 (n=51)
13.2 (n=70)
12.0 (n=72)
15.4 (n=85)
12.1 (n=97)
Other renal disease 10.0 (n=12)
10.4 (n=14)
6.4 (n=17)
7.6 (n=21)
9.1 (n=31)
Ren
al d
isea
se
Unconfirmed 9.6 (n=779)
8.7 (n=2,523)
9.1 (n=1,629)
9.6 (n=1,518)
9.3 (n=2,714)
Isolated CABG: Average post-operative stay by renal disease; bars denote standard errors (n=90,893)
No renal disease Elevated creatinine Any renal disease
8
9
10
11
12
13
14
15
16
17
18
1999 2000 2001 2002 2003
Financial year
Ave
rag
e p
ost
-op
erat
ive
stay
/ d
ays

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
172
NA
CSD
– C
AB
G s
urg
ery
risk
fact
ors
Angina
Key points from the angina analyses
• The proportion of patients presenting for cardiac surgery with severe angina continues to show a year-on-year decrease.
• Severe angina is associated with increased post-operative stay; patients with the severest angina stay 1.5 days longer than do patients with little or no angina.
• Severe angina more than doubles post-operative mortality.
Angina distributions
Based on the evidence from large trials, coronary surgery is performed both for the relief of angina and the prolongation of life. The accepted scoring system for the classification of angina is the Canadian Cardiovascular Society (CCS) grading system; the greater the CCS score, the more severe the angina.
For the patient, angina is at best worrying and at worst crippling. The graphs below demonstrate the continuing high proportion of patients presenting for surgery with severe angina. Nevertheless, the trend is towards improvement, with a diminishing population of patients with very bad angina undergoing surgery. This is coupled with an increase in the proportion of patients with less severe angina coming to surgery.
Financial year
1996 1997 1998 1999 2000 2001 2002 2003
CCS 0 92 98 142 219 440 688 729 956
CCS 1 320 404 581 881 1,176 1,412 2,029 3,465
CCS 2 1,071 1,702 3,177 4,241 5,478 6,798 6,754 8,070
CCS 3 1,966 2,634 4,560 5,468 6,251 7,439 7,904 8,236
CCS 4 991 1,528 2,467 2,914 3,256 3,996 4,442 4,068
An
gin
a
Unconfirmed 571 1,778 2,537 2,738 2,739 1,716 1,568 1,216
Isolated CABG: Angina class (n=119,043)
CCS 0 CCS 1 CCS 2 CCS 3 CCS 4
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
1996 1997 1998 1999 2000 2001 2002 2003
Financial year
Per
cen
tag
e o
f pat
ien
ts

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
173
NA
CSD
– CA
BG
surg
ery risk factors
Mortality and angina
On the whole, the worse the angina, the higher the operative risk.
Angina is heart pain due to cramp, which occurs when the heart muscle is not receiving an adequate supply of blood. Very sick or dead heart muscle does not register pain and does not function as well following surgery. This explains why patients with no or very little angina, but with disease bad enough to warrant surgery, have a relatively high operative mortality.
Financial year
1999 2000 2001 2002 2003
CCS 0-1 1.9% (n=1,100)
1.8% (n=1,616)
1.5% (n=2,099)
1.4% (n=2,706)
1.5% (n=4,402)
CCS 2 1.3% (n=4,240)
1.3% (n=5,477)
1.5% (n=6,796)
1.1% (n=6,724)
1.0% (n=8,047)
CCS 3 2.1% (n=5,467)
2.2% (n=6,251)
2.1% (n=7,434)
2.0% (n=7,832)
2.2% (n=8,215)
CCS 4 4.5% (n=2,911)
4.2% (n=3,255)
4.5% (n=3,995)
4.3% (n=4,402)
3.8% (n=4,058)
An
gin
a
Unconfirmed 3.0% (n=2,738)
2.2% (n=2,736)
2.3% (n=1,708)
1.9% (n=1,550)
2.3% (n=1,212)
Isolated CABG: Crude mortality by angina class (n=97,027)
CCS 0-1 CCS 2 CCS 3 CCS 4
0%
1%
2%
3%
4%
5%
6%
1999 2000 2001 2002 2003
Financial year
Cru
de
mo
rtal
ity
rate

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
174
NA
CSD
– C
AB
G s
urg
ery
risk
fact
ors
Angina and NHS centres
Isolated CABG: Angina class by centre for financial year 2003 (n=23,891)
CCS 0-1 CCS 2 CCS 3 CCS 4
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
St James's Hospital Dublin
University Hospital o f Wales Cardiff
M orriston Hospital Swansea
James Cook Uni Hosp'l M iddlesbrough
Queen Elizabeth Hospital B irmingham
Cardiothoracic Centre Liverpool
Freeman Hospital Newcastle
Wythenshawe Hospital M anchester
Aberdeen Royal Infirmary
Bristo l Royal Infirmary
Glasgow Royal Infirmary
Royal Victoria Hospital Belfast
Glasgow Western Infirmary
St George's Hospital London
Nottingham City Hospital
Edinburgh Royal Infirmary
Leeds General Infirmary
Northern General Hospital Sheffield
Victoria Hospital B lackpool
John Radcliffe Hospital Oxford
Glenfield Hospital Leicester
M anchester Royal Infirmary
Walsgrave Hospital Coventry
Barts and the London
King's College Hospital London
N Staffordshire Royal Infirmary
Royal Sussex County Hospital
Guy's & St Thomas' Hospitals London
Derriford Hospital P lymouth
Castle Hill Hospital Hull
Hammersmith Hospital London
Harefield Hospital London
Royal Brompton Hospital London
Golden Jubilee Hospital Glasgow
The Heart Hospital London
Southampton General Hospital
Papworth Hospital
St M ary's Hospital London
Cen
tre
Percentage of patients

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
175
NA
CSD
– CA
BG
surg
ery risk factors
Missing, unconfirmed or unmapped angina data
Isolated CABG: Missing angina class data by centre for financial year 2003 (n=25,067)
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Walsgrave Hospital Coventry
St James's Hospital Dublin
Royal Sussex County Hospital
Royal Brompton Hospital London
Queen Elizabeth Hospital B irmingham
Papworth Hospital
M anchester Royal Infirmary
Glasgow Western Infirmary
Glasgow Royal Infirmary
Freeman Hospital Newcastle
Edinburgh Royal Infirmary
Castle Hill Hospital Hull
Cardio thoracic Centre Liverpool
Victoria Hospital B lackpool
N Staffordshire Royal Infirmary
Southampton General Hospital
Harefield Hospital London
Bristo l Royal Infirmary
The Heart Hospital London
Guy's & St Thomas' Hospitals London
Aberdeen Royal Infirmary
Wythenshawe Hospital M anchester
James Cook Uni Hosp'l M iddlesbrough
Derriford Hospital P lymouth
King's College Hospital London
Leeds General Infirmary
University Hospital o f Wales Cardiff
Northern General Hospital Sheffield
Hammersmith Hospital London
St George's Hospital London
John Radcliffe Hospital Oxford
Glenfield Hospital Leicester
Barts and the London
Nottingham City Hospital
M orriston Hospital Swansea
Royal Victoria Hospital Belfast
Golden Jubilee Hospital Glasgow
St M ary's Hospital London
Cen
tre
Percentage entries with missing data

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
176
NA
CSD
– C
AB
G s
urg
ery
risk
fact
ors
Angina and private centres; Angina and country
Isolated CABG: Angina class by centre for financial year 2003 (Private Hospital n=904)
CCS 0-1 CCS 2 CCS 3 CCS 4
Isolated CABG: Angina class by country for financial year 2003 (n= 23,891)
CCS 0-1 CCS 2 CCS 3 CCS 4
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
All NHS
All private
BUPA Hospital Leicester
The Harley Street Clinic
London Bridge Hospital
BUPA Hospital Bristol
BUPA Hospital Washington
BUPA Chalybeate Southampton
BUPA Cambridge Lea Hospital
Cen
tre
Percentage of patients
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
England
Scotland
Ireland
Wales
Co
un
try
Percentage of patients

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
177
NA
CSD
– CA
BG
surg
ery risk factors
Angina and post-operative stay
The worse a patient’s angina before the operation, the longer they are likely to stay in hospital after their operation.
Financial year
1999 2000 2001 2002 2003
CCS 0-1 7.4 (n=1,076)
8.0 (n=1,574)
7.6 (n=2,065)
8.3 (n=2,688)
8.4 (n=4,280)
CCS 2 7.6 (n=4,057)
7.9 (n=5,205)
7.8 (n=6,522)
8.0 (n=6,483)
7.9 (n=7,749)
CCS 3 8.3 (n=5,206)
8.6 (n=5,730)
8.5 (n=6,941)
8.6 (n=7,425)
8.8 (n=7,982)
CCS 4 9.2 (n=2,772)
9.6 (n=3,054)
9.5 (n=3,717)
9.6 (n=4,193)
9.9 (n=3,941)
An
gin
a
Unconfirmed 8.5 (n=1,757)
8.5 (n=2,267)
8.8 (n=1,332)
8.9 (n=1,479)
10.3 (n=561)
Isolated CABG: Average post-operative stay by angina class; bars denote standard errors (n=92,660)
CCS 0-1 CCS 2 CCS 3 CCS 4
7.0
7.5
8.0
8.5
9.0
9.5
10.0
1999 2000 2001 2002 2003
Financial year
Ave
rag
e p
ost
-op
erat
ive
stay
/ d
ays

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
178
NA
CSD
– C
AB
G s
urg
ery
risk
fact
ors
Dyspnoea (breathlessness)
Key points from the dyspnoea analyses
• There has been an increase in breathlessness amongst coronary surgery patients over the last six years from about 50% in 1996 to a peak of 70% in 2002.
• The increase in the proportion of breathless patients is due to an increase in mild breathlessness.
• Breathlessness is associated with a higher risk of post-operative mortality; double the risk for severe breathlessness and four times the risk for very severe breathlessness.
• Breathless patients stay longer in hospital after their operation.
Dyspnoea distributions
Dyspnoea is the medical term for breathlessness. This is a fairly subjective symptom that may be due to a variety of causes, but is generally related to cardiac disease or lung disease. It is graded according to the New York Heart Association Classification, along similar lines to the classification for angina. In essence, patients with NYHA class 1 have very mild shortness-of-breath that does not restrict normal activity; at the other end of the scale, class 4 dyspnoea is breathlessness at rest or on any normal physical activity.
Financial year
1996 1997 1998 1999 2000 2001 2002 2003
NYHA 1 2,228 2,821 4,073 4,845 5,884 6,773 6,638 7,435
NYHA 2 1,229 2,118 4,119 5,214 6,830 7,673 8,622 9,780
NYHA 3 799 2,089 3,206 3,601 4,130 5,151 5,314 5,460
NYHA 4 144 359 506 723 720 833 1,010 927 Dys
pn
oea
Unconfirmed 611 757 1,560 2,078 1,776 1,619 1,842 2,409
Isolated CABG: Dyspnoea grade (n=121,254)
NYHA 1 NYHA 2 NYHA 3 NYHA 4
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
1996 1997 1998 1999 2000 2001 2002 2003
Centre
Per
cen
tag
e o
f pat
ien
ts

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
179
NA
CSD
– CA
BG
surg
ery risk factors
Mortality and dyspnoea
Pre-operative breathlessness indicates trouble with the heart, the lungs or both heart and lungs. Not surprisingly, it is therefore associated with an increasing mortality; as breathlessness increases so mortality increases. Note the dramatic increase in mortality associated with marked breathlessness.
Shortness-of-breath may be due to either lung or heart disease, both of which influence the risk of heart surgery; when due to poor heart function it has a very significant impact on surgical mortality (see page 184).
Financial year
1999 2000 2001 2002 2003
NYHA 1 2.0% (n=4,844)
1.9% (n=5,883)
1.9% (n=6,769)
1.4% (n=6,638)
1.4% (n=7,416)
NYHA 2 2.2% (n=5,212)
1.6% (n=6,830)
1.8% (n=7,672)
1.7% (n=8,621)
1.5% (n=9,760)
NYHA 3 2.9% (n=3,600)
3.0% (n=4,130)
2.9% (n=5,147)
2.8% (n=5,314)
2.5% (n=5,448)
NYHA 4 5.4% (n=722)
7.5% (n=719)
6.1% (n=833)
7.2% (n=1,010)
5.7% (n=926)
Dys
pn
oea
Unconfirmed 2.5% (n=2,078)
1.8% (n=1,773)
2.7% (n=1,611)
1.9% (n=1,631)
3.0% (n=2,384)
Isolated CABG: Crude mortality by dyspnoea grade (n=97,494)
NYHA 1 NYHA 2 NYHA 3 NYHA 4
0%
1%
2%
3%
4%
5%
6%
7%
8%
9%
10%
1999 2000 2001 2002 2003
Financial year
Cru
de
mo
rtal
ity
rate

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
180
NA
CSD
– C
AB
G s
urg
ery
risk
fact
ors
Dyspnoea and NHS centres
Isolated CABG: Dyspnoea grade by centre for financial year 2003 (n=22,697)
NYHA 1 NYHA 2 NYHA 3 NYHA 4
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Papworth Hospital
The Heart Hospital London
King's College Hospital London
St George's Hospital London
Royal Victoria Hospital Belfast
Queen Elizabeth Hospital B irmingham
Royal Brompton Hospital London
Hammersmith Hospital London
Guy's & St Thomas' Hospitals London
Derriford Hospital P lymouth
Southampton General Hospital
Castle Hill Hospital Hull
Leeds General Infirmary
Harefield Hospital London
Cardiothoracic Centre Liverpool
Barts and the London
Northern General Hospital Sheffield
Royal Sussex County Hospital
Golden Jubilee Hospital Glasgow
N Staffordshire Royal Infirmary
M anchester Royal Infirmary
Edinburgh Royal Infirmary
Victoria Hospital B lackpool
Glenfield Hospital Leicester
Wythenshawe Hospital M anchester
Walsgrave Hospital Coventry
Bristo l Royal Infirmary
James Cook Uni Hosp'l M iddlesbrough
University Hospital o f Wales Cardiff
Freeman Hospital Newcastle
M orriston Hospital Swansea
St James's Hospital Dublin
Nottingham City Hospital
Glasgow Royal Infirmary
Glasgow Western Infirmary
Aberdeen Royal Infirmary
St M ary's Hospital London
John Radcliffe Hospital Oxford
Cen
tre
Percentage of patients

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
181
NA
CSD
– CA
BG
surg
ery risk factors
Missing, unconfirmed or unmapped dyspnoea data
Isolated CABG: Dyspnoea grade class data by centre for financial year 2003 (n=25,067)
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Walsgrave Hospital Coventry
St James's Hospital Dublin
Southampton General Hospital
Royal Sussex County Hospital
Royal Brompton Hospital London
Queen Elizabeth Hospital B irmingham
Papworth Hospital
M anchester Royal Infirmary
Guy's & St Thomas' Hospitals London
Glasgow Western Infirmary
Freeman Hospital Newcastle
Edinburgh Royal Infirmary
Victoria Hospital B lackpool
Cardio thoracic Centre Liverpool
N Staffordshire Royal Infirmary
Bristo l Royal Infirmary
The Heart Hospital London
Harefield Hospital London
Aberdeen Royal Infirmary
University Hospital o f Wales Cardiff
Wythenshawe Hospital M anchester
Castle Hill Hospital Hull
King's College Hospital London
Northern General Hospital Sheffield
Derriford Hospital P lymouth
Hammersmith Hospital London
Leeds General Infirmary
St George's Hospital London
M orriston Hospital Swansea
Glasgow Royal Infirmary
Glenfield Hospital Leicester
Barts and the London
Golden Jubilee Hospital Glasgow
Nottingham City Hospital
Royal Victoria Hospital Belfast
James Cook Uni Hosp'l M iddlesbrough
St M ary's Hospital London
John Radcliffe Hospital Oxford
Cen
tre
Percentage entries with missing data

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
182
NA
CSD
– C
AB
G s
urg
ery
risk
fact
ors
Dyspnoea and private centres; Dyspnoea and country
Isolated CABG: Dyspnoea grade by centre for financial year 2003 (Private Hospital n=905)
NYHA 1 NYHA 2 NYHA 3 NYHA 4
Isolated CABG: Dyspnoea grade by country for financial year 2003 (n=22,697)
NYHA 1 NYHA 2 NYHA 3 NYHA 4
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
All NHS
All private
BUPA Hospital Bristol
The Harley Street Clinic
BUPA Hospital Leicester
London Bridge Hospital
BUPA Hospital Washington
BUPA Chalybeate Southampton
BUPA Cambridge Lea Hospital
Cen
tre
Percentage of patients
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
England
Ireland
Wales
Scotland
Co
un
try
Percentage of patients

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
183
NA
CSD
– CA
BG
surg
ery risk factors
Dyspnoea and post-operative stay
Post-operative recovery may be hampered by pre-operative breathlessness as indicated by prolonged stay in hospital after the operation associated with increasing levels of breathlessness.
Financial year
1999 2000 2001 2002 2003
NYHA 1 7.7 (n=4,538)
7.9 (n=5,576)
7.8 (n=6,721)
7.9 (n=6,493)
8.1 (n=7,144)
NYHA 2 8.2 (n=4,999)
8.4 (n=6,438)
8.3 (n=7,572)
8.4 (n=8,459)
8.5 (n=9,428)
NYHA 3 8.8 (n=3,534)
9.2 (n=3,811)
9.0 (n=5,082)
9.5 (n=5,240)
9.3 (n=5,302)
NYHA 4 10.1 (n=337)
11.1 (n=494)
9.5 (n=714)
10.1 (n=692)
10.4 (n=823)
Dys
pn
oea
Unconfirmed 8.5 (n=413)
8.8 (n=714)
8.5 (n=1,083)
9.0 (n=1,313)
9.0 (n=379)
Isolated CABG: Average post-operative stay by dyspnoea grade; bars denote standard errors (n=94,470)
NYHA 1 NYHA 2 NYHA 3 NYHA 4
7.5
8.0
8.5
9.0
9.5
10.0
10.5
11.0
1999 2000 2001 2002 2003
Financial year
Ave
rag
e p
ost
-op
erat
ive
stay
/ d
ays

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
184
NA
CSD
– C
AB
G s
urg
ery
risk
fact
ors
Interactions between risk factors
Mortality, ejection fraction and dyspnoea
Coronary surgery can improve heart function in some cases; however, when poor heart function is associated with moderate or severe breathlessness, the surgery carries a very high risk: almost 14 times the risk for a patient with a good heart and no breathlessness.
Financial years 2001-2003
Ejection fraction Mortality rate
(Count; 95% CI)
Good Fair Poor Unconfirmed
NYHA 1-2 1.0% (n=31,499; 0.9-1.1%)
2.3% (n=12,155; 2.0-2.6%)
6.4% (n=2,242; 5.4-7.5%)
1.5% (n=980; 0.9-2.6%)
NYHA 3 1.6% (n=9,341; 1.4-1.9%)
3.3% (n=4,860; 2.9-3.9%)
7.8% (n=1,451; 6.5-9.3%)
1.6% (n=257; 0.5-4.2%)
NYHA 4 3.6% (n=1,373; 2.7-4.8%)
6.6% (n=897; 5.1-8.5%)
13.8% (n=458; 10.8-17.3%)
12.2% (n=41; 4.6-27.0%) D
ysp
no
ea
Unconfirmed 1.4% (n=2,804; 1.0-1.9%)
3.8% (n=822; 2.6-5.4%)
11.4% (n=193; 7.4-17.0%)
2.9% (n=1,807; 2.2-3.8%)
Isolated CABG: Crude mortality by ejection fraction and dyspnoea grade; financial years 2001-2003 (n=64,276)
NYHA 1-2 NYHA 3 NYHA 4
0%
2%
4%
6%
8%
10%
12%
14%
16%
18%
Good Fair Poor
Ejection fraction
Cru
de
mo
rtal
ity
rate

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
185
NA
CSD
– CA
BG
surg
ery risk factors
Mortality, age and renal disease
The interaction between age, renal disease and post-operative mortality is outlined below. The table shows a trend of increasing risk with greater age and with impaired renal function.
Financial years 2001-2003
Renal disease Mortality rate
(Count; 95% CI)
None Elevated creatinine
Dialysis Other Unconfirmed
<51 0.7% (n=5,045; 0.5-1.0%)
4.3% (n=47; 0.7-15.7%)
2.8% (n=36; 0.1-16.2%)
8.3% (n=12; 0.4-40.2%)
1.4% (n=627; 0.7-2.8%)
51-60 1.0% (n=15,821; 0.8-1.1%)
8.4% (n=107; 4.2-15.8%)
6.7% (n=75; 2.5-15.5%)
8.0% (n=25; 1.4-27.5%)
1.1% (n=1,852; 0.7-1.8%)
61-70 1.7% (n=25,020; 1.6-1.9%)
5.4% (n=277; 3.2-9.0%)
7.9% (n=101; 3.7-15.5%)
4.2% (n=24; 0.2-23.1%)
2.4% (n=3,202; 1.9-3.0%)
>70 3.4% (n=16,134; 3.2-3.7%)
14.2% (n=352; 10.8-18.4%)
24.6% (n=57; 14.5-38.0%)
0.0% (n=7; 0.0-34.8%)
5.5% (n=2,214; 4.6-6.5%)
Ag
e / y
ears
Unconfirmed 0.0% (n=73; 0.0-4.0%)
NA NA NA 1.4% (n=72; 0.1-8.5%)
Isolated CABG: Crude mortality by age and renal disease category; financial years 2001-2003 (n=63,072)
None Elevated creatinine Dialysis
0%
5%
10%
15%
20%
25%
30%
35%
40%
<51 51-60 61-70 >70
Age at surgery / years
Cru
de
mo
rtal
ity

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
186
NA
CSD
– C
AB
G s
urg
ery
po
st-o
per
ativ
e b
leed
ing
Re-operation for post-operative bleeding
Re-operation for post-operative bleeding by procedure
This is the first time data on re-operation for post-operative bleeding in this database have been analysed. Some hospitals either did not supply suitable data on bleeding and therefore these analyses are based on only 21 hospitals’ data.
Heart operations are major procedures and it is not surprising that in some cases bleeding can be difficult to control and may, on occasion, mean return to the operating theatre to stop persistent bleeding. There is always some bleeding and this is why tubes are left in the chest after an operation so that excess blood can drain in bottles. If the drainage is excessive the surgeon may decide to take the patient back to the operating theatre.
Troublesome bleeding may come from a variety of sources some of which are related to the residual effects of drugs taken by the patient before the operation that are intended to prevent clotting e.g.s Warfarin, aspirin. Bleeding may also come from the wound and tissues surrounding the heart, but the surgeon will always want to reassure himself that the bleeding is not coming from joins in bypass grafts or suture lines in the heart. Generally, the more complex the operation the more likely it is that there will be problems with bleeding.
Re-operation for post-operative bleeding
No Yes Unconfirmed
CABG only 62,712 2,138 1,396
CABG & Valve 7,246 532 270
CABG, Valve & Other 502 46 26
CAB & Other 1,571 103 66
Valve only 13,739 840 505
Valve & Other 1,800 197 113
Other 507 199 533
Pro
ced
ure
Unconfirmed 47 0 46
Re-operation for post-operative bleeding; financial years 1999-2003 (n=94,132)
No re-operation Re-operation
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
CAB only
Valve only
CAB & Other
CAB & Valve
Other
CAB, Valve & Other
Valve & Other
Pro
ced
ure
Percentage of patients

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
187
NA
CSD
– CA
BG
surg
ery po
st-op
erative bleed
ing
Re-operation for post-operative bleeding; financial years 1999-2003 (n=94,132)
Valve operations involve sizable incisions into either the main blood vessel leaving the heart or heart itself, consequently the bleeding rates are higher for valve surgery than for isolated coronary bypass surgery. A combination of valve surgery and bypass surgery results in an even higher rate of return to the operating theatre for control of bleeding.
Re-operation for post-operative bleeding for isolated aortic and mitral operations; financial years 1999-2003 (n=19,598)
Aortic valve replacement
Mitral valve replacement Mitral valve repair
0% 2% 4% 6% 8% 10% 12%
CAB only
Valve only
CAB + Other
CAB + Valve
Other
CAB + Valve + Other
Valve + Other
Pro
ced
ure
Re-operation for bleeding rate
0%
1%
2%
3%
4%
5%
6%
7%
8%
9%
Valve only CAB & Valve
Procedure
Re-
op
erat
ion
for
ble
edin
g r
ate

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
188
NA
CSD
– C
AB
G s
urg
ery
po
st-o
per
ativ
e b
leed
ing
Re-operation for post-operative bleeding after isolated CABG
Re-operations for post-operative bleeding and financial year
There is not discernible trend in bleeding rates over time for isolated coronary operations. The rate of return to theatre for the control of bleeding is consistently 3.0-3.5%.
Re-operation for post-operative bleeding
No Yes Unconfirmed
1999 10,212 347 257
2000 11,865 392 312
2001 13,370 444 174
2002 13,663 491 170
Fin
anci
al y
ear
2003 13,602 464 483
Isolated CABG: Re-operation for post-operative bleeding (n=64,850)
0.0%
0.5%
1.0%
1.5%
2.0%
2.5%
3.0%
3.5%
4.0%
1999 2000 2001 2002 2003
Financial year
Re-
op
erat
ion
for
ble
edin
g r
ate

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
189
NA
CSD
– CA
BG
surg
ery po
st-op
erative bleed
ing
Re-operation for post-operative bleeding and centre
The funnel plot below shows that most centres fall within the normal, expected range of return to theatre for bleeding.
One centre, highlighted in blue, appears to be performing particularly well; this would bear further analysis.
Isolated CABG: Funnel plot on re-operation for bleeding rate for 21 centres; financial year 2003 (n=14,066)
Overall rate 99.9 % lower alert 99.9 % lower alert Centre
99.99% lower alarm 99.99% lower alarm
0%
1%
2%
3%
4%
5%
6%
7%
8%
9%
10%
0 200 400 600 800 1,000 1,200
Number of cases
Re-
op
erat
ion
for
ble
edin
g r
ate

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
190
NA
CSD
– C
AB
G s
urg
ery
po
st-o
per
ativ
e b
leed
ing
Re-operation for post-operative bleeding and age
Older people generally bruise and bleed more easily; it is, therefore, not surprising that older people suffer more bleeding problems following heart surgery, as shown in the graph below.
Re-operation for post-operative bleeding
No Yes Unconfirmed
<56 16,241 454 1,859
56-60 12,569 407 1,318
61-65 16,013 561 1,611
66-70 16,278 598 1,270
71-75 12,009 544 720
>75 5,848 291 286 Ag
e at
su
rger
y / y
ears
Unconfirmed 26 5 30
Isolated CABG: Re-operation for post-operative bleeding by age; financial years 1999-2003 (n=64,846)
0%
1%
2%
3%
4%
5%
6%
<56 56-60 61-65 66-70 71-75 >75
Age at surgery / years
Re-
op
erat
ion
for
ble
edin
g r
ate

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
191
NA
CSD
– CA
BG
surg
ery po
st-op
erative bleed
ing
Re-operation for post-operative bleeding, age and gender
Re-operation for post-operative bleeding
Male Female Unspecified
No
Yes
Un
con
firm
ed
No
Yes
Un
con
firm
ed
No
Yes
Un
con
firm
ed
<56 14,001 413 1,622 2,236 41 235 4 0 2
56-60 10,587 356 1,105 1,979 51 211 3 0 2
61-65 13,002 471 1,296 3,008 90 312 3 0 3
66-70 12,465 463 974 3,810 135 290 3 0 6
71-75 8,750 424 525 3,258 120 194 1 0 1
>75 4,127 218 224 1,718 73 62 3 0 0 Ag
e at
su
rger
y / y
ears
Unconfirmed 22 5 25 3 0 5 1 0 2
Isolated CABG: Re-operation for post-operative bleeding by age and gender; financial years 1999-2003 (n=64,829)
Male Female
0%
1%
2%
3%
4%
5%
6%
<56 56-60 61-65 66-70 71-75 >75
Age at surgery / years
Re-
op
erat
ion
for
ble
edin
g r
ate

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
192
NA
CSD
– C
AB
G s
urg
ery
po
st-o
per
ativ
e b
leed
ing
Re-operation for post-operative bleeding, BSA and gender
Re-operation for post-operative bleeding
Male Female Unspecified
No
Yes
Un
con
firm
ed
No
Yes
Un
con
firm
ed
No
Yes
Un
con
firm
ed
<1.70 2,205 143 54 5,257 209 103 1 0 0
1.70-1.79 4,910 235 94 3,047 60 58 2 0 0
1.80-1.89 9,448 387 202 2,118 45 33 3 0 0
1.90-1.99 11,774 395 208 1,183 23 24 5 0 1
2.00-2.09 9,862 322 176 444 9 7 3 0 0
2.10-2.19 5,781 137 89 140 6 1 1 0 0
2.20-2.29 2,529 55 49 33 1 1 1 0 0
2.30-2.39 993 12 24 9 0 0 1 0 0
>2.39 436 8 4 3 1 0 0 0 0
Bo
dy
surf
ace
area
/ m
2
Unconfirmed 1,975 70 210 548 20 58 0 0 0
Isolated CABG: Re-operation for post-operative bleeding by BSA; financial years 1999-2003 (n=61,789)
0%
1%
2%
3%
4%
5%
6%
<1.7 1.70-1.79 1.80-1.89 1.90-1.99 2.00-2.09 2.10-2.19 2.20-2.29 2.30-2.39 >2.39
Body surface area / m2
Re-
op
erat
ion
for
ble
edin
g r
ate

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
193
NA
CSD
– CA
BG
surg
ery po
st-op
erative bleed
ing
Re-operation for post-operative bleeding and bypass time
It is well documented that the longer a patient is connected to the heart-lung machine (bypass machine) the more difficulty the surgeon faces trying to control bleeding at the end of the operation. Despite this, the re-opening for bleeding rate remains less than 4%, except for those extremely difficult cases, where the bypass time has exceeded 3 hours. Thankfully, this represents a tiny percentage of our patients.
Isolated CABG: Re-operation for post-operative bleeding by bypass time; financial years 1999-2003 (n=52,562)
Isolated CABG: Bypass time in patients where re-operation for bleeding data are recorded; financial years 1999-2003 (n=52,562)
0%
2%
4%
6%
8%
10%
12%
<31 31-60 61-90 91-120 121-150 151-180 >180
Bypass time / min
Re-
op
erat
ion
for
ble
edin
g r
ate
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
<31 31-60 61-90 91-120 121-150 151-180 >180
Bypass time / min
Per
cen
tag
e o
f pat
ien
ts

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
194
NA
CSD
– C
AB
G s
urg
ery
po
st-o
per
ativ
e b
leed
ing
Re-operation for post-operative bleeding and mortality
Re-operation for post-operative bleeding
No Yes Unconfirmed
Alive 61,473 1,967 1,300
Died 1,188 170 88
Pat
ien
t st
atu
s
Unconfirmed 51 1 8
Isolated CABG: Re-operation for bleeding by patient status; 1999-2003 (n=64,798)
Isolated CABG: Mortality by re-operation for bleeding; 1999-2003 (n=64,798)
0%
2%
4%
6%
8%
10%
12%
14%
16%
Alive Dead
Patient status at discharge
Re-
op
erat
ion
for
ble
edin
g r
ate
0%
1%
2%
3%
4%
5%
6%
7%
8%
9%
10%
No re-operation Re-operation
Post-operative re-operation for bleeding
Mo
rtal
ity
rate

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
195
CA
BG
surg
ery practice
Aspects of coronary surgery practice in the UK and Ireland
Number of bypass grafts
During the second half of the 1990s there has been a steady reduction in the proportion of patients receiving four bypass grafts, with a concomitant increase in the proportion receiving two or three grafts. This may reflect the worsening pattern of coronary artery disease being considered for surgery, with fewer arteries being suitable for grafting. The marked variation between centres will be the result of different patient populations combined with differences in surgical philosophy and practice.
UKCSR: Number of grafts used in first-time isolated CABG procedures by financial year (n=188,534)
1 graft 2 grafts 3 grafts
4 grafts 5 grafts >5 grafts
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
1996 1997 1998 1999 2000 2001 2002 2003
Financial year
Per
cen
tag
e o
f pat
ien
ts

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
196
CA
BG
su
rger
y p
ract
ice
UKCSR: Number of grafts used in first-time isolated CABG procedures by centre for financial year 2003 (n=24,604)
1 graft 2 grafts 3 grafts
4 grafts 5 grafts >5 grafts
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Harefield Hospital M iddlesex
Castle Hill Hospital Hull
Bristo l Royal Infirmary
Queen Elizabeth Hospital B irmingham
Glasgow Western Infirmary
Aberdeen Royal Infirmary
Northern General Hospital Sheffield
John Radcliffe Hospital Oxford
Walsgrave Hospital Coventry
The Heart Hospital London
Nottingham City Hospital
Glenfield Hospital Leicester
King Edward VII M idhurst
Guy's & St Thomas' Hospitals London
Southampton General Hospital
Royal Sussex County Hospital
Wythenshawe Hospital M anchester
Leeds General Infirmary
Glasgow Royal Infirmary
King's College Hospital London
Edinburgh Royal Infirmary
Royal Brompton Hospital London
Royal Victoria Hospital Belfast
James Cook Uni Hos'l M iddlesbrough
Derriford Hospital P lymouth
Hammersmith Hospital London
St George's Hospital London
St M ary's Hospital London
Papworth Hospital
Victoria Hospital B lackpool
Bart's and the London
Cardiothoracic Centre Liverpool
Freeman Hospital Newcastle
N Staffordshire Royal Infirmary
University Hospital o f Wales Cardiff
M orriston Hospital Swansea
M anchester Royal Infirmary
Cen
tre
Percentage of patients

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
197
CA
BG
surg
ery practice
The use of arterial grafts
It has been clearly demonstrated that patients who receive a left internal mammary artery graft (LIMA) to the left anterior descending coronary artery (LAD) enjoy better symptomatic relief and a longer life expectancy than patients who receive a vein graft to that coronary artery. As a result, a LIMA graft to the LAD has become standard practice, with vein grafts being applied to other coronary arteries as required.
The graph below illustrates the steady increase in the percentage of patients undergoing isolated coronary surgery and receiving at least one arterial graft. This will generally represent the proportion of patients receiving a LIMA to the LAD since this is the most commonly applied arterial graft.
Arterial graft usage in isolated CABG; Data from UKCSR up to 2000-2001 and from NACSD thereafter
One or more arteries Two or more arteries Three or more arteries
More recently there has been gradually accumulating evidence to suggest that additional benefit may be conferred by additional arterial rather than venous bypass grafts. If this evidence holds up to scrutiny we must expect to see an increasing proportion of patients with 2 or more arterial bypass grafts and ultimately an increasing proportion of patients receiving only arterial grafts.
The decision to use multiple arterial grafts in any patient generally results in a longer and more technically demanding operation than the current standard operation of one LIMA graft to the LAD with additional venous grafts as required. If this trend continues it will mean that additional operating theatre facilities and surgeons will be required to perform the same number of operations.
The second half of the 1990s saw a slow but steady increase in the number of patients undergoing total arterial revascularisation, with one-fifth of all patients receiving two or more arterial grafts. This rate is high by international standards.
The 2000-2001 report showed there was considerable variation between centres, which we thought would reduce as the available evidence on the relative benefits of this strategy has become clearer.
Information on the use of arterial grafts by different institutions is less complete this year since we have shifted the prime mode of data collection from the UKCSR to the National Adult Cardiac Surgical Database.
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
1985
1986
1987
1988
1989
1990
1991
1992
1993
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3Year
Per
cen
tag
e o
f pat
ien
ts

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
198
CA
BG
su
rger
y p
ract
ice
After a steady rise in arterial graft usage since 1985, and increasing enthusiasm for the use of more than one arterial graft since the mid 1990s, we have now reached a plateau.
UKCSR: Arterial graft usage in first-time isolated CABG by total number of grafts used
1 graft 2 grafts 3 grafts 4 grafts
UKCSR: Arterial graft usage in first-time isolated CABG by total number of grafts used
2 grafts 3 grafts 4 grafts
0%
5%
10%
15%
20%
25%
30%
1996 1997 1998 1999 2000 2001 2002 2003
Financial year
Per
cen
tag
e o
f pat
ien
ts
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
1996 1997 1998 1999 2000 2001 2002 2003
Financial year
Per
cen
tag
e o
f pat
ien
ts

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
199
CA
BG
surg
ery practice
This graph demonstrates the varying use of at least one arterial graft per operation between centres. The data on this is complete for 95% or more of all patients in all centres except Barts & the London (88% complete, shaded dark) and James Cook University Hospital in Middlesbrough (excluded).
First-time isolated CABG: Patients receiving one or more arterial grafts; financial year 2003 (n=20,154)
50% 60% 70% 80% 90% 100%
Leeds General Infirmary
The Heart Hospital London
Wythenshawe Hospital M anchester
Castle Hill Hospital Hull
Northern General Hospital Sheffield
Glasgow Western Infirmary
Southampton General Hospital
Victoria Hospital B lackpool
Bart's and the London
M orriston Hospital Swansea
M anchester Royal Infirmary
Derriford Hospital P lymouth
Nottingham City Hospital
Guy's & St Thomas' Hospitals London
Walsgrave Hospital Coventry
Freeman Hospital Newcastle
Glenfield Hospital Leicester
King's College Hospital London
N Staffordshire Royal Infirmary
Queen Elizabeth Hospital B irmingham
University Hospital o f Wales Cardiff
Bristo l Royal Infirmary
Royal Sussex County Hospital
Cardio thoracic Centre Liverpool
Royal Brompton Hospital London
Papworth Hospital
Hammersmith Hospital London
Edinburgh Royal Infirmary
St George's Hospital London
Harefield Hospital M iddlesex
Cen
tre
Percentage of patients

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
200
CA
BG
su
rger
y p
ract
ice
First-time isolated CABG: Change in the proportion of patients receiving one or more arterial grafts; financial year 2001 versus 2003 (n=40,833)
More in 2003 Fewer in 2003
-5% 0% 5% 10% 15% 20%
Castle Hill Hospital Hull
M anchester Royal Infirmary
Derriford Hospital P lymouth
Royal Brompton Hospital London
Nottingham City Hospital
Guy's & St Thomas' Hospitals London
Southampton General Hospital
Bristo l Royal Infirmary
St George's Hospital London
Papworth Hospital
Cardio thoracic Centre Liverpool
Northern General Hospital Sheffield
Queen Elizabeth Hospital B irmingham
King's College Hospital London
N Staffordshire Royal Infirmary
Glenfield Hospital Leicester
University Hospital o f Wales Cardiff
Wythenshawe Hospital M anchester
Freeman Hospital Newcastle
Bart's and the London
Royal Sussex County Hospital
Harefield Hospital M iddlesex
Glasgow Western Infirmary
Hammersmith Hospital London
Edinburgh Royal Infirmary
Leeds General Infirmary
Walsgrave Hospital Coventry
Victoria Hospital B lackpool
M orriston Hospital Swansea
The Heart Hospital London
Cen
tre
Percentage of patients in 2003 lesspercentage of patients in 2001

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
201
CA
BG
surg
ery practice
Protecting the heart during coronary surgery
During surgery on the heart it is common to stop the heart to make it easier to suture the bypass grafts onto to the coronary arteries, which are only 1.5mm in diameter. During this time the function of the heart and lungs is taken over by a heart-lung or cardiopulmonary bypass machine.
The heart can be stopped using several different methods. In general, a mixture of potassium and magnesium with some other chemicals is infused into the coronary arteries. This mixture can be carried in either blood or a clear saline like solution. These solutions are called cardioplegia and are referred to as either blood or crystalloid cardioplegia respectively.
The heart can also be stopped electrically and this is referred to as cardiac arrest with ventricular fibrillation. In the graph below it is labelled Non cardioplegia to distinguish this technique from blood or crystalloid cardioplegia.
NACSD: Isolated CABG: Myocardial protection (n=90,923)
Blood cardioplegia Crystalloid cardioplegia Blood & crystalloid cardioplegia
Non-cardioplegia Off-bypass
More recently engineering technology has evolved to produce stabilisers, which can hold the coronary arteries still during suturing. This eliminates the need to chemically or electrically stop the heart and therefore the need for a heart lung machine. This is referred to as off-bypass or off-pump coronary surgery.
Although off-pump coronary surgery appears to confer some benefits by eliminating the need for a bypass machine, the technology, although good, is still not perfect or appropriate for all cases. It is also quite difficult to learn, consequently many surgeons continue to use the established, safe techniques with which they are more familiar.
The proportion of patients in the UK undergoing off-pump coronary surgery (17%, 2003) is similar to Australia (16%, 2002) and the USA (21.6%, 2003).
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
1999 2000 2001 2002 2003
Financial year
Per
cen
tag
e o
f op
erat
ion
s

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
202
CA
BG
su
rger
y p
ract
ice
Extensive scientific studies examining subtle changes in the heart suggest that blood cardioplegia is better than crystalloid cardioplegia. This is reflected in the growing proportion of patients receiving blood rather than crystalloid cardioplegia.
NACSD: Isolated CABG: Myocardial protection (n=48,253)
Blood cardioplegia Crystalloid cardioplegia
50%
55%
60%
65%
70%
75%
80%
85%
90%
95%
100%
1999 2000 2001 2002 2003
Financial year
Per
cen
tag
e o
f op
erat
ion
sp
erfo
rmed
usi
ng
car
dio
ple
gia

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
203
CA
BG
surg
ery practice
Influence of myocardial protection technique on mortality
The graph below is difficult to interpret because the choice of myocardial protection technique can be influenced by a number of subtle technical considerations related to individual cases. Nevertheless, there appears to be no real difference between cardioplegia (blood or crystalloid) and electrical arrest.
The apparent lower mortality for off-bypass surgery is misleading because if difficulties are encountered during this type of surgery then the patient is connected to a heart lung machine and cardioplegia administered to make the operation technically easier and to rest the heart; this is called conversion. If a patient subsequently dies the death is registered as on-bypass usually with cardioplegia.
NACSD: Isolated CABG: Crude mortality rate by myocardial protection (n=90,439)
Blood cardioplegia Crystalloid cardioplegia
Non-cardioplegia Off-bypass
0%
1%
2%
3%
4%
5%
6%
1997 1998 1999 2000 2001 2002 2003
Financial year
Cru
de
mo
rtal
ity
rate

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
204
CA
BG
su
rger
y p
ract
ice
On- and off-pump CABG
UKCSR: On- and off-pump isolated CABG by centre; financial years 2000-2003 (n=56,065)
On-pump Off-pump
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
M orriston Hospital Swansea
Leeds General Infirmary
Queen Elizabeth Hospital B irmingham
Glasgow Royal Infirmary
James Cook Uni Hosp'l M iddlesbrough
Glasgow Western Infirmary
Hammersmith Hospital London
Freeman Hospital Newcastle
The Heart Hospital London
King Edward VII M idhurst
Bart's and the London
Guy's & St Thomas' Hospitals London
Northern General Hospital Sheffield
N Staffordshire Royal Infirmary
Nottingham City Hospital
Derriford Hospital P lymouth
Castle Hill Hospital Hull
Southampton General Hospital
Wythenshawe Hospital M anchester
Glenfield Hospital Leicester
Royal Sussex County Hospital
University Hospital o f Wales Cardiff
Papworth Hospital
Aberdeen Royal Infirmary
Edinburgh Royal Infirmary
Royal Victoria Hospital Belfast
Royal Brompton Hospital London
King's College Hospital London
John Radcliffe Hospital Oxford
Victoria Hospital B lackpool
Walsgrave Hospital Coventry
St George's Hospital London
Cardiothoracic Centre Liverpool
M anchester Royal Infirmary
Bristo l Royal Infirmary
Harefield Hospital M iddlesex
St M ary's Hospital London
Cen
tre
Percentage of patients

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
205
NA
CSD
– CA
BG
surg
ery Intern
ation
al com
pariso
ns
International comparisons
A number of other countries have developing clinical databases, which contain information on enough patients to allow us to draw some comparisons between the natures of patients undergoing surgery in different countries.
Information for this section is drawn from a number of sources:
• The UK National Adult Cardiac Surgical Database, which includes data from the UK and Republic of Ireland (this report).
• The European Association for Cardio-Thoracic Surgery Adult Cardiac Surgical Database, which includes data from the national societies of, amongst others, Norway, France and Italy 24.
• The US Society of Thoracic Surgeons Adult Cardiac Database 25.
All of these databases include data on a variety of different operations (see chart below), but most of the graphs presented in this section relate only to coronary artery bypass surgery.
Some comparisons are not yet possible because of different data definitions or different published analyses. These issues are slowly being resolved around the world.
Procedures performed 1999-2003 (n=163,757)
CABG Valve CABG + Valve
CABG + Other Valve + Other CABG + Valve + Other
Other
In different countries surgeons have different practices. In the UK surgeons link cardiac and thoracic (mainly lung) surgery. In other countries, the lung and other thoracic work is carried out by general surgeons and cardiac surgeons operate only on the heart, aorta and peripheral blood vessels (e.g. legs); this type of surgery is denoted by the upper, black parts of the histograms above. In the UK peripheral vascular surgery is performed largely by dedicated, vascular surgeons who do not operate on the heart nor on adjacent large blood vessels.
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
France Italy Norway UK Ireland
Country
Per
cen
tag
e o
f op
erat
ion
s

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
206
NA
CSD
– C
AB
G s
urg
ery
Inte
rnat
ion
al c
om
par
iso
ns
Isolated CABG: Average age; 1999-2003 (n=866,374)
Isolated CABG: Gender; 1999-2003 (n=865,903)
59
60
61
62
63
64
65
66
67
Ireland UK Norway France USA Italy
Country
Ave
rag
e ag
e / y
ears
0%
5%
10%
15%
20%
25%
30%
Ireland Norway UK Italy France USA
Country
Per
cen
tag
e fe
mal
e p
atie
nts

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
207
NA
CSD
– CA
BG
surg
ery Intern
ation
al com
pariso
ns
Isolated CABG: Diabetes; 1999-2003 (n= 854,874)
Isolated CABG: Obesity; 1999-2003 (n=851,393)
0%
5%
10%
15%
20%
25%
30%
35%
40%
Norway Ireland UK Italy France USA
Country
Per
cen
tag
e o
f pat
ien
tsw
ith
dia
bet
es
0%
5%
10%
15%
20%
25%
30%
35%
40%
Italy Norway France Ireland UK USA
Country
Per
cen
tag
e o
bes
e p
atie
nts

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
208
NA
CSD
– C
AB
G s
urg
ery
Inte
rnat
ion
al c
om
par
iso
ns
Isolated CABG: Morbid obesity; 1999-2003 (n= 843,700)
Isolated CABG: Ejection fraction; 1999-2003 (n=808,807)
0%
2%
4%
6%
8%
10%
12%
14%
Italy Norway France Ireland UK USA
Country
Per
cen
tag
e o
f mo
rbid
lyo
bes
e p
atie
nts
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
Ireland USA UK Italy France Norway
Country
Per
cen
tag
e o
f pat
ien
tsw
ith
go
od
eje
ctio
n fr
acti
on

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
209
NA
CSD
– CA
BG
surg
ery Intern
ation
al com
pariso
ns
Isolated CABG: Average post-operative stay; 1999-2003 (n=845,407)
0
1
2
3
4
5
6
7
8
9
10
USA Ireland UK Italy France
Country
Ave
rag
e p
ost
-op
erat
ive
stay
/ d
ays

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
210
NA
CSD
– C
AB
G s
urg
ery
Inte
rnat
ion
al c
om
par
iso
ns
United Kingdom, Ireland and the USA
The crude mortality for coronary surgery in the UK is a little lower than that in the USA. However, the patient population in the USA is slightly older with a greater proportion of women, diabetics, smokers and patients with lung disease. In addition there are more morbidly obese patients.
This again highlights the hazards of drawing conclusions from crude mortality data where patient characteristics have not been taken onto account. Methods for taking these factors into account (risk stratification) are discussed in detail in the following pages.
Isolated CABG: UK-USA risk factor comparisons; financial year 2003 (n=172,822)
UK and Ireland United States of America
First-time isolated CABG: UK-USA crude mortality comparisons (n≈1,690,000)
UK and Ireland United States of America
1.0%
1.5%
2.0%
2.5%
3.0%
3.5%
4.0%
1994 1995 1996 1997 1998 1999 2000 2001 2002 2003
Year
Cru
de
mo
rtal
ity
rate
0% 10% 20% 30% 40% 50% 60% 70% 80% 90%
Previous surgery
Elective surgery
Peripheral vascular disease
Hypertension
NYHA IV
Respiratory disease
Current smoker
Diabetes
Morbidly obese
Female
>65 years old
Fact
or
Percentage of patients

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
211
NA
CSD
– CA
BG
surg
ery Intern
ation
al com
pariso
ns
Evolution of risk factors in coronary bypass surgery Prof. Fred Edwards Chairman of the United States National Adult Cardiac Surgery Database
Experience from the Society of Thoracic Surgeons National Database (1980-2000)
The field of coronary artery bypass grafting (CABG) has undergone considerable change in the last two decades. Most surgeons sense that their patient population carries progressively higher risk with each passing year, yet operative mortality has remained quite stable. Certainly we must quantify these important observations to define the issues as clearly as possible.
The Society of Thoracic Surgeons National Cardiac Surgery Database, commonly called the STS Database, contains detailed peri-operative information on more than one million patients, thereby making it the largest cardiac surgery database in the United States. This information has been used to analyse the trends in risk factors and outcomes for patients undergoing isolated CABG from 1980 - 2000. Where 2000 data were not available, 1998 or 1999 data were extrapolated to calendar year 2000.
Development of trends
In the early 1980s, coronary bypass surgery was enjoying a golden period characterized by operative mortality rates typically in the range of 1–2%. The vast majority of cases were elective, single vessel bypasses were not uncommon, and elderly patients were usually not offered surgical options. Some 5 or 6 years later, however, the landscape had dramatically changed. The improvements in myocardial protection permitted safe surgery to be extended to the elderly as well as those with severely compromised ventricular function. Urgent and emergent operations became common, and redo procedures began to occupy a significant part of the operating schedule. Patients having the lowest operative risk were being treated with percutaneous catheter interventions, thereby removing them from the CABG population. Not surprisingly, the operative mortality for coronary artery bypass grafting CABG rose from 1-2% to around 5-6%. More patients were leaving the hospital alive and well, but a significant number of patients that previously would have died on the medicine ward were instead dying post-operatively in the surgical intensive care unit.
Practical considerations
Operative mortality (OM), of course, is one of the most important trends to follow. There is some value in tracking the raw, unadjusted OM, but there is general agreement that mortality is best analysed with tools that make appropriate adjustments of patient risk. The STS Database has developed statistical tools that are designed to account for individual patient risk. Initially models were developed using Bayesian theory to predict the probability of operative death associated with CABG 26, 27, 28 but subsequent models were derived from multivariate logistic regression techniques 29, 30, 31.
Unadjusted CABG mortality has varied significantly over this period of time. After the accentuated peak in the mid-1980s, there has been a progressive decline to approximately 3% today. This allows an opportunity to examine the quality of operative care provided over that time. There is a general perception that patient risk factors have become more unfavourable in the last 15 years. If that is true and the OM has dropped, one might logically conclude that better care is being provided to our patients.
In fact, an examination of well-accepted risk factors shows that there has been a progressive rise in patient age, re-operations, left main coronary artery disease, renal failure, and non-elective surgery.
The average ejection fraction has progressively fallen. Subjectively, one would be prompted to conclude that the patients are indeed at higher risk today. One would also assume that the risk models would reflect this by showing a progressively higher predicted mortality for each successive year. Surprisingly, when the risk models for each year are used to determine the predicted OM, there is virtually no change over the last two decades.
We were surprised to find that none of the other risk factors demonstrated a significant increase in odds ratio. In other words, virtually all risk factors either remained stable or diminished in importance over the last twenty years. As shown below, the landscape of risk factors has dramatically changed over this time.

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
212
NA
CSD
– C
AB
G s
urg
ery
Inte
rnat
ion
al c
om
par
iso
ns
Evolution of risk factor influence on operative mortality
1980s 2000
In 1980, there were several risk factors that clearly stood out as compelling markers for patient risk. Presently, however, we find a much more homogeneous array of odds ratios. The trend suggests that we are approaching a point at which there will be few, if any outstanding risk factors and patient death following CABG will be almost a random event. If we do, in fact, reach such a state, risk modelling will be virtually impossible.
We may, however, still conclude that patient care has improved. It is almost certainly the improvement in patient care that has produced the drop in odds ratios, which in turn has produced the drop in predicted and observed operative mortality.
Conclusions
• In the USA CABG mortality has reached a plateau of approximately 2-3%.
• The frequency of traditionally recognized risk factors is increasing.
• The impact of these risk factors is decreasing.
• Prediction of CABG outcomes will be more difficult in the future.
0 1 2 3 4 5 6 7 8
3-vessel disease
Smoking
COAD
Cerebrovascular disease
Hypertension
Peripheral vascular disease
Age>70
Left main stem disease
Female Gender
Redo surgery
Renal impairment
Ejection fraction
Emergency
Ris
k fa
cto
r
Odds ratio for operative mortality

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
213
NA
CSD
– CA
BG
surg
ery risk stratification
Adjusting for risk Estimating risk for patients &
presenting risk adjusted analyses

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
214
NA
CSD
– C
AB
G s
urg
ery
risk
str
atif
icat
ion
Risk stratification for coronary surgery
What risks are attached to my operation?
Surgery of the heart is now very common and is widely regarded as the best understood and most scientifically based branch of surgery. In the NHS alone over 35,000 heart operations are performed every year with results as good as anywhere in the world.
Many things in life carry some degree of risk, which we intuitively understand. Assessments of financial and political risks populate every Sunday newspaper. A few things such as war, childbirth, dangerous sports, travel and surgery carry very real risks to life and limb, which cannot be escaped. The vast majority of patients undergoing heart surgery whistle through their operation and recovery phase with little difficulty. A few will have some minor problems, which are normal, and a small proportion will suffer quite significant complications such as a stroke or death.
Not all patients are the same. The challenge is to identify patients who are at a potentially higher risk from surgery so that the potential risks and benefits can be discussed with the patient on an informed basis before any operation.
The risk that any one patient will not survive surgery is dependent on a number of different factors, some of which can be quantified, such as age, gender and the existence of specific comorbidities. Risk scoring systems attempt to take account of these risk factors and convert them into a numeric risk score, which represents the probability of death or some other outcome for an individual. The higher the score, the greater the predicted risk. However, low risk is not the same as no risk.
Although we can now work out a probability of death, we cannot say exactly which patient will survive or die. If we assess 100 patients and apply a risk scoring system we can estimate that, say, 3 patients will die. Unfortunately we cannot yet say with certainty which three; if we could we would not operate on them. For each of the 100 individuals we can calculate a probability of death or survival using the types of scoring systems described on the following pages.
If we are to reduce the risk of surgery for our patients it is imperative that we explore and understand the factors that contribute to that risk. For example, understanding the impact of diabetes has prompted considerable effort to minimise its impact and this is reflected in the steadily reducing influence of diabetes on outcome.
Over the years a variety of risk stratification systems have evolved using logistic regression and Bayes modelling techniques 32, 33, 34; these range from simple additive systems 11, 35, 36, 37 to highly complex statistical algorithms, which provide the basis for rational and meaningful comparisons of outcomes between groups of patients, institutions 38 and ultimately individual surgeons.

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
215
NA
CSD
– CA
BG
surg
ery risk stratification
The Parsonnet score
Key points from Parsonnet score analyses
• The Parsonnet score was the first widely used risk-scoring system for cardiac surgery; it was developed in 1985.
• It requires data on 16 variables.
• Increased Parsonnet score still correlates with increased risk.
• There has been a reduction in low risk patients and an increase in higher risk patients over the last 5 years.
• The Parsonnet score substantially over-predicts risk for today’s patients.
• The score can be calculated for over half of the patients in the NACSD.
The components that comprise the additive Parsonnet scoring system are detailed in an Appendix at the end of this report. For those who are unfamiliar with this scoring system, a score for each patient is calculated before the operation and the greater the score, the greater the mortality risk. In the paper published by Parsonnet in 1985, patients in the low risk group (Parsonnet score of 0 to 4) had an average mortality of 1%, patients in the elevated risk group (Parsonnet score of 5 to 9) had an average mortality of 5%, and so on up the scale. The distribution of patients between the five Parsonnet score groups is usually such that most patients have low scores, and as the risk score increases so the number of patients with that score falls.
The Parsonnet score can be calculated using all the parameters that Parsonnet described, or by using only the rigidly defined parameters i.e., excluding the subjective catastrophic states and other rare circumstances (see Appendices). The second, more stringent approach, which excludes the ill-defined components, was applied to those data entries where all the appropriate data were available to generate a centrally calculated Parsonnet score. From this point onwards, the Parsonnet score referred to will be that centrally calculated version, so that any comparisons will be made in the knowledge that there has been standardisation.
Parsonnet score distributions through time
Isolated CABG: Parsonnet score distributions (n=55,744)
0-4 5-9 12-14 15-19 >19
0%
10%
20%
30%
40%
50%
60%
1999 2000 2001 2002 2003
Financial year
Per
cen
tag
e o
f pat
ien
ts

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
216
NA
CSD
– C
AB
G s
urg
ery
risk
str
atif
icat
ion
The graph on the preceding page clearly shows that the proportion of lower risk patients is falling and the proportion of higher risk patients is rising.
This is reflected in the graph below, which shows that the average Parsonnet score has risen by 2 over the last six years. This is equivalent to an increase in predicted mortality of almost 1% over this period.
Isolated CABG: Average Parsonnet score by gender (n=65,593)
Male Female All
4
5
6
7
8
9
10
1997 1998 1999 2000 2001 2002 2003
Financial year
Ave
rag
e P
arso
nn
et s
core

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
217
NA
CSD
– CA
BG
surg
ery risk stratification
Mortality by Parsonnet score
The Parsonnet score is now very inaccurate at predicting mortality. However, if the score is divided by 3 it gives a reasonable prediction of operative mortality for contemporary practice in the United Kingdom and Ireland.
Financial year
1999 2000 2001 2002 2003
0-4 1.1% (n=4,523)
0.6% (n=4,589)
0.9% (n=5,626)
0.8% (n=5,601)
0.6% (n=5,796)
5-9 2.5% (n=2,216)
2.3% (n=2,400)
2.1% (n=3,177)
1.9% (n=3,280)
1.4% (n=3,555)
10-14 4.2% (n=1,196)
4.2% (n=1,362)
3.4% (n=1,866)
3.0% (n=2,155)
2.5% (n=2,398)
15-19 6.5% (n=495)
6.6% (n=653)
4.2% (n=945)
4.2% (n=1,107)
4.9% (n=1,244)
>19 11.9% (n=134)
8.9% (n=191)
10.2% (n=343)
11.4% (n=404)
7.7% (n=481)
Par
son
net
sco
re
Unconfirmed 2.6% (n=7,892)
2.3% (n=10,140)
2.5% (n=10,075)
2.1% (n=10,667)
2.1% (n=12,460)
Isolated CABG: Mortality by Parsonnet score for financial year 2003 (n=13,474)
Observed Predicted
0%
5%
10%
15%
20%
25%
30%
0-4 5-9 10-14 15-19 >19
Parsonnet score
Mo
rtal
ity
rate

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
218
NA
CSD
– C
AB
G s
urg
ery
risk
str
atif
icat
ion
Isolated CABG: Mortality by Parsonnet score (n=55,737)
0-4 5-9 10-14 15-19 >19
Completeness of Parsonnet score
The Parsonnet score used in this report has 16 variables; if even a single one of these is missing then the patient’s score cannot be determined with absolute confidence. The graph below indicates the percentage of patients with one or more required variables for calculation of the complete Parsonnet score absent from their data.
Isolated CABG: Patients without a complete Parsonnet score (n=107,287)
0%
2%
4%
6%
8%
10%
12%
14%
1999 2000 2001 2002 2003
Financial year
Mo
rtal
ity
rate
0%
10%
20%
30%
40%
50%
60%
1999 2000 2001 2002 2003
Financial year
Per
cen
tag
e o
f pat
ien
ts w
ho
can
no
t b
e fu
lly s
core
d

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
219
NA
CSD
– CA
BG
surg
ery risk stratification
The EuroSCORE
Key points from the EuroSCORE analyses
• The EuroSCORE is a simple additive risk scoring system based on contemporary European data (including British data).
• Calculation of the EuroSCORE for a patient undergoing isolated coronary requires the collection of 13 clinical factors.
• Sixty percent of patients fall into the two lowest risk categories.
• Like all risk scoring systems, it is less accurate for very ill patients.
• Even when certain assumptions are allowed, in the financial year ending March 2003, the EuroSCORE could not be calculated for 30% of patient-entries because of missing, unconfirmed or unmappable data.
Since the development of the Parsonnet risk model, the specialty has moved forward and although most of the risk variables in the Parsonnet system remain pertinent their relative impact on mortality has changed. More recently another system based on a pan-European patient population has been described in order to make the system more applicable to European patients 36, 39. The principle is much the same, but some of the risk factors and their weightings are different, making allowance for advances in surgical practice and a different patient population.
We have calculated the EuroSCORE for a group of coronary artery bypass patients from the current data in the National Adult Cardiac Surgical Database (see appendices). A total of 63,623 patient-entries fulfilled all the criteria required to determine the EuroSCORE over the last five years. One assumption was made in the calculation: all previous cerebro-vascular accidents (CVA) were taken as an indication that there was neurological dysfunction. The EuroSCORE is a more direct measure of operative mortality than the Parsonnet score. Most patients have a score of between 0 or 3, which approximates to a risk of death in the range 0-3%. This is in keeping with the average mortality rate for contemporary coronary artery bypass surgery.

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
220
NA
CSD
– C
AB
G s
urg
ery
risk
str
atif
icat
ion
EuroSCORE distributions through time
The vast majority of patients (83%) fall in the 0-5 EuroSCORE risk bracket.
Isolated CABG: Modified EuroSCORE distributions (n=64,051)
0-1 2-3 4-5 6-7 8-9 >9
Isolated CABG: Average modified EuroSCORE score by gender (n=70,174)
Male Female All
0%
5%
10%
15%
20%
25%
30%
35%
1999 2000 2001 2002 2003
Financial year
Per
cen
tag
e o
f pat
ien
ts
2.0
2.5
3.0
3.5
4.0
4.5
5.0
1997 1998 1999 2000 2001 2002 2003
Financial year
Ave
rag
e m
od
ifie
d E
uro
SCO
RE

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
221
NA
CSD
– CA
BG
surg
ery risk stratification
Mortality by EuroSCORE
Over the last 5 years the EuroSCORE, along with other models, has become less accurate and is starting to noticeably over-predict mortality, especially in the mid-range. At the upper end, which is a relatively small proportion of patients, it under-predicts mortality.
Financial year
1999 2000 2001 2002 2003
0-1 0.3% (n=2,243)
0.4% (n=3,047)
0.6% (n=3,676)
0.5% (n=4,211)
0.3% (n=4,311)
2-3 1.0% (n=2,323)
1.2% (n=3,349)
1.1% (n=4,347)
0.9% (n=4,967)
0.9% (n=5,409)
4-5 2.1% (n=1,518)
2.1% (n=2,377)
1.7% (n=3,154)
1.9% (n=3,665)
1.8% (n=4,245)
6-7 5.3% (n=655)
4.2% (n=1,095)
4.1% (n=1,457)
3.8% (n=1,713)
3.2% (n=2,042)
8-9 6.1% (n=264)
7.1% (n=421)
8.6% (n=544)
6.9% (n=652)
6.3% (n=773)
>9 17.5% (n=160)
18.3% (n=218)
18.5% (n=378)
16.8% (n=405)
16.1% (n=378)
Mo
dif
ied
Eu
roSC
OR
E
Unconfirmed 2.8% (n=9,293)
2.4% (n=8,828)
2.5% (n=8,476)
2.4% (n=7,601)
2.3% (n=8,776)
Isolated CABG: Mortality by modified EuroSCORE for financial year 2003 (n=17,158)
Observed Predicted
0%
2%
4%
6%
8%
10%
12%
14%
16%
18%
20%
0-1 2-3 4-5 6-7 8-9 >9
Modified EuroSCORE
Mo
rtal
ity
rate

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
222
NA
CSD
– C
AB
G s
urg
ery
risk
str
atif
icat
ion
Isolated CABG: Mortality by modified EuroSCORE (n=63,997)
0-1 2-3 4-5 6-7 8-9 >9
Completeness of EuroSCORE data
The modified EuroSCORE used in this report has 13 variables; as with the calculation of the Parsonnet score, even if one of these variables is missing then the patient’s score cannot be determined with absolute confidence. The graph below reveals the percentage of patients with one or more required variables for calculation of the complete EuroSCORE absent from their data.
Isolated CABG: Patients without a complete EuroSCORE (n=107,287)
0%
5%
10%
15%
20%
25%
1999 2000 2001 2002 2003
Financial year
Mo
rtal
ity
rate
0%
10%
20%
30%
40%
50%
60%
1999 2000 2001 2002 2003
Financial year
Per
cen
tag
e o
f pat
ien
ts w
ho
can
no
t b
e fu
lly
sco
red

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
223
NA
CSD
– CA
BG
surg
ery risk stratification
The Logistic EuroSCORE
Key points from the logistic EuroSCORE analyses
• This modification of the EuroSCORE uses the same 13 components as the additive EuroSCORE.
• Fifty percent of patients have a predicted risk of less than 2%.
• The score identifies a year-on-year increase in risk.
• This score over-predicts for the highest risk patients as opposed to the additive EuroSCORE that under-predicts for these patients.
Logistic EuroSCORE distributions through time
The logistic EuroSCORE 40 uses exactly the same data items as the EuroSCORE (see appendix) to predict a patient’s risk, but uses a non-integer weighting for each risk factor rather than simple integer values; for example, if the patient is female then 0.3304052 is added rather than 1 point as used in the classic, additive EuroSCORE model. Once all the appropriate weightings have been added together, the patient’s predicted risk is calculated by plugging this number into a relatively complex mathematical formula.
The hope was that this version of the EuroSCORE would generate even more accurate predictions than the classic, additive EuroSCORE.
Full details of the weightings and the equation are given at www.euroscore.org/logisticEuroSCORE.htm.
Isolated CABG: Modified logistic EuroSCORE distributions (n=64,051)
<1.0% 1.0-1.9% 2.0-2.9% 3.0-4.9% 5.0-9.9% >9.9%
0%
5%
10%
15%
20%
25%
30%
35%
1999 2000 2001 2002 2003
Financial year
Per
cen
tag
e o
f pat
ien
ts

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
224
NA
CSD
– C
AB
G s
urg
ery
risk
str
atif
icat
ion
Mortality by Logistic EuroSCORE
Financial year
1999 2000 2001 2002 2003
<1.0% 0.1% (n=1,255)
0.4% (n=1,606)
0.5% (n=1,948)
0.2% (n=2,320)
0.2% (n=2,397)
1.0-1.9% 0.7% (n=2,450)
0.7% (n=3,523)
0.8% (n=4,394)
0.8% (n=4,989)
0.6% (n=5,169)
2.0-2.9% 1.8% (n=1,296)
1.5% (n=1,988)
1.5% (n=2,627)
0.9% (n=3,050)
1.2% (n=3,468)
3.0-4.9% 2.0% (n=1,127)
2.4% (n=1,717)
1.7% (n=2,316)
2.2% (n=2,622)
2.0% (n=3,127)
5.0-9.9% 5.8% (n=669)
4.5% (n=1,129)
4.9% (n=1,496)
4.1% (n=1,743)
3.3% (n=2,052)
>9.9% 10.7% (n=366)
11.6% (n=544)
13.0% (n=775)
11.9% (n=889)
10.9% (n=945) M
od
ifie
d L
og
isti
c Eu
roSC
OR
E
Unconfirmed 2.8% (n=9,293)
2.4% (n=8,828)
2.5% (n=8,476)
2.4% (n=7,601)
2.3% (n=8,776)
Isolated CABG: Mortality by modified logistic EuroSCORE for financial year 2003 (n=17,158)
Observed Predicted
0%
2%
4%
6%
8%
10%
12%
14%
16%
18%
20%
<1.0 1.0-1.9 2.0-2.9 3.0-4.9 5.0-9.9 >9.9
Modified logistic EuroSCORE
Mo
rtal
ity
rate

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
225
NA
CSD
– CA
BG
surg
ery risk stratification
Isolated CABG: Mortality by modified logistic EuroSCORE (n=63,997)
0-1 2-3 4-5 6-7 8-9 >9
Completeness of logistic EuroSCORE data
The modified logistic EuroSCORE used in this report has 13 variables; as with the calculation of the additive EuroSCORE, just one missing variable can preclude the calculation of the score with absolute confidence. The graph below indicates the percentage of patients with one or more required variables for calculation of the complete logistic EuroSCORE absent from their data.
Isolated CABG: Patients without a complete logistic EuroSCORE (n=107,287)
0%
2%
4%
6%
8%
10%
12%
14%
1999 2000 2001 2002 2003
Financial year
Mo
rtal
ity
rate
0%
10%
20%
30%
40%
50%
60%
1999 2000 2001 2002 2003
Financial year
Per
cen
tag
e o
f pat
ien
ts w
ho
can
no
t b
e fu
lly s
core
d

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
226
NA
CSD
– C
AB
G s
urg
ery
risk
str
atif
icat
ion
Bayesian modelling
The sciences ... mainly make models. By a model is meant a mathematical construct, which, with the addition of certain verbal interpretations, describes observed phenomena. The justification of such a mathematical construct is that it is expected to work.
John Van Neumann
Risk stratification is a method of delimiting sub-populations within a cohort that have different risks of a particular outcome, based upon severity of illness and comorbidity. Using such an approach, it is possible to make fair comparisons between different institutions or different surgeons. Comparisons of individual institutions’ or individual surgeons’ outcome rates could also be made against agreed standards using this method. The Bayesian approach is one method of risk stratification.
What do Bayes tables do?
The Bayes table approach is a particularly simple way of building a risk stratification system from a database. Based solely on tables relating outcomes to single risk factors, the probability of an adverse outcome can be estimated for a patient with any combination of risk factors.
The method is based on the repeated use of Bayes theorem, which is a basic formula in probability theory, first discovered by the Rev. Thomas Bayes, a non-conformist minister from Tunbridge Wells, which was published posthumously in 1763 (Thomas Bayes having died in 1761; his grave lies in Bunhill Fields in London, only yards from the Royal Statistical Society). Bayes theorem tells us how the probability of an event should be revised when additional relevant evidence is obtained.
The following is an example of the way in which this may be applied to clinical data. Suppose the outcome of interest is post-operative death, and we have information on both post-operative status and age. The data might be shown as in the table below:
Table of fictitious, example data
S: Survivors D: Deaths Total
A: 70-79 years old 90 30 120
not A: all other ages 810 70 880
Ag
e g
rou
pin
g
Total 900 100 1,000
The notation used within the table is such that S represents survival, D represents death, A represents patients in the age grouping 70-79 years old and not A represents all other patients.
A probability of an event is calculated as the number of events in a group (post-operative deaths) divided by the total number in that same group. For example, the probability of death, p(D), for the entire group is 100 / (100 + 900) = 0.10. Such rates can also be expressed in percentage terms, and the percentage rate is obtained by multiplying the probability by a factor of 100. In this example, the percentage mortality rate is [100 / (900 + 100)] × 100 = 0.10 × 100 = 10%. The probability of survival, p(S), is 900 / (100 + 900) = 0.90, which may also be expressed as 90%.
A probability of 1.00 (100%) means that the event always occurs, whereas a probability of 0.00 (0%) means that the event never occurs. Since either death or survival must occur, the sum of the probability of survival and the probability of death must be equal to 1. This idea may be expressed as the formula:
p(D) + p(S) = 1
This implies that the probability of survival can be calculated as:
p(S) = 1 - p(D)
The odds on death is defined as the probability of death divided by the probability of survival:
Odds (D) = p(D) / p(S) = p(D) / [1 - p(D)]

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
227
NA
CSD
– CA
BG
surg
ery risk stratification
In the above example, the odds on death for the whole group is p(D) / [1 - p(D)] = 0.1 / [ 1 – 0.10] = 1 / 9 or, in betting parlance, 9 to 1 against death. An assessment of these odds based on no patient-specific data is known as the prior odds.
The odds on D may be converted to a probability using the following formula:
p(D) = Odds (D) / [1 + Odds(D)]
Suppose that we now wish to take into account the age of the patient, which falls in the range 70-79 years old (designated A). The probability of death in this group is denoted p(D | A) = 30 / (90 + 30) = 30 / 120 = 0.25 or 25%. This is known as the posterior probability. The odds on death in this group is p(D | A) / p(S | A) = 0.25 / 0.75 = 1 / 3 = 0.33 or 3 to 1 against death. This is known as the posterior odds.
Bayes theorem is the formula that provides the link between the prior and posterior odds:
posterior odds = prior odds × likelihood ratio
where the likelihood ratio expresses how much more likely it is that a patient with such an age should fall amongst those who die rather than those who survive. From the above, the likelihood ratio = p(A | D) / p(A | S) = [(30 / 100) / (90 / 900)] = 0.30 / 0.10 = 3, i.e., this age group is 3 times more common in those who die than those who survive. Thus, Bayes theorem suggests that the posterior odds = 3 × prior odds = 3 × (0.10 / 0.90) = 3 × 0.11 = 0.33. Using the conversion formula described above, this corresponds to a probability of 0.25 or 25%, which matches the probability obtained by direct examination of the data in the table.
The Bayes tables (see Appendices) give detailed information on Bayesian risk models.
Items of evidence in a Bayes model might include many different risk factors that affect the outcome, such as age, left ventricular ejection fraction, urgency and so on. The calculation of risk for a specific patient is updated each time a new item of evidence is added. This simple procedure is, however, making the crucial assumption that each item of evidence is contributing independent information concerning the chances of the outcome; technically, we are assuming that the items of evidence are conditionally independent given the true outcome. This assumption is most likely to be appropriate if careful clinical sense has been used in selecting the predictive factors that do not convey similar evidence. Failure to select predictive factors in this way may result in predictions that are over-confident.
It is important to note that the score is calculated irrespective of omissions in the data. It is possible to calculate a Bayes score whether all, some or none of the risk factors are known. The Bayes score is adjusted for each item of evidence, and will more accurately reflect the true risk if all the relevant data are known.
Two Bayesian risk models for isolated coronary artery bypass surgery
In the 1999-2000 report we described two Bayesian models to predict in-hospital mortality from the data on isolated coronary artery bypass surgery: a simple, 5-factor Bayes model and a complex, 9-factor Bayes model. Simple risk models can produce acceptable results, but more complex risk models may give better results. These two risk models were generated in an attempt to test this hypothesis.
The aim was to generate risk models that accurately discriminated between patients who died following surgery and patients who survived; this was tested using Receiver Operating Characteristic curve analysis (see below). The risk score should also provide an accurate estimation of the individual patient’s risk; this was tested using calibration curve analyses (see below). Each Bayes model was initially trained on the isolated coronary artery bypass surgery data from the financial year ending 1999, and then tested on the isolated coronary artery bypass surgery data from the financial years ending 1999 and 2000 separately. When results from the ROC curve and calibration plot analyses indicated that the models discriminated well and produced broadly accurate predictions, both were re-calculated on the pooled data from financial years ending 1999 and 2000 (see Appendices).

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
228
NA
CSD
– C
AB
G s
urg
ery
risk
str
atif
icat
ion
Simple (5-factor) Bayes model for isolated CABG
The first model contained only 5 risk factors, in an attempt to provide a reasonably simple predictor of the outcome that all surgeons could use. A minimum of data is needed to calculate the score.
A large number of risk factors were ranked according to their weight of evidence. The weight of evidence for each risk factor was determined as the sum of the products, for each subdivision of the risk factor, of the normalised proportion of patients in the death column and the normalised weight in the Bayes table. In descending order of weight of evidence the risk factors were: Ejection Fraction, Priority, Cardiogenic Shock, Age, Congestive Cardiac Failure, Any pre operative support (determined from the presence of Cardiogenic Shock, IV inotropes, Intra Aortic Balloon Pump, Pre operative Ventilation), Angina class, Angina Symptom Status, IV inotropes, Left Main Stem disease, Intra Aortic Balloon Pump, Number of Previous Operations, IV nitrates, Dyspnoea grade, Pre operative Ventilation, Peripheral Vascular Disease, Renal Dysfunction, Body Surface Area, Previous Myocardial Infarction, Pacemaker, Recent Failed Intervention, Extent of Coronary Disease, Gender, Pulmonary Disease, Cerebrovascular Disease, Diabetes, Hypercholesterolaemia, Hypertension. The patient’s Ejection Fraction adds the greatest weight of evidence, and the presence or absence of Hypertension adds the least weight of evidence.
A series of 5 factor Bayes models were constructed, using various combinations of risk factors, giving preference to those with the greatest weight of evidence. The combination of risk factors that gave the best results was: Age (weight of evidence rank 4), Body Surface Area (weight of evidence rank 18), Ejection Fraction (weight of evidence rank 1), Priority (weight of evidence rank 2) and Previous operations (weight of evidence rank 12) (see Appendices). Calculation of this score requires seven data items: the patient’s date of birth, the date of the operation, the patient’s height and weight, ejection fraction, the urgency of the operation and whether or not the patient had undergone any cardiac surgery previously.
Taking risk factors on the basis of their weight of evidence alone did not give the best results
Complex (9-factor) Bayes model for isolated CABG
The second model contained 9 risk factors: Age (weight of evidence rank 4), Body Surface Area (weight of evidence rank 18), Diabetes (weight of evidence rank 26), Hypertension (weight of evidence rank 28), Left Main Stem disease (weight of evidence rank 10), Ejection Fraction (weight of evidence rank 1), Priority (weight of evidence rank 2), Renal system (weight of evidence rank 17) and Previous operations (weight of evidence rank 12) (see Appendices). Eleven data items are required to calculate this score: the patient’s date of birth, the date of the operation, the patient’s height and weight, the presence or absence of diabetes, hypertension, left main stem disease and renal disease, the patient’s left ventricular ejection fraction, the urgency of the operation and whether or not the patient had undergone any cardiac surgery previously.
As for the simple Bayes model, taking risk factors simply on the basis of their weight of evidence did not give the best results.

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
229
NA
CSD
– CA
BG
surg
ery risk stratification
Adoption of the complex Bayes model
The next, short, section is semi-statistical in nature and will only really be of use to those with a mathematical interest. The net result of all the analyses is that the complex Bayes model appears to be better as a risk model for isolated CABG surgery than the simple model and so was adopted as the Bayes model to be used in further analyses. The benefit of the simple model was that fewer variables were used in its calculation. As more and more variables are added to a risk model, there will be more and more missing data (see pages 234-239). When assembling a risk model one of several compromises that must be made is comparing the model’s accuracy against the ease with which the required data can be collected; there is no point in having a near perfect risk model when the data required cannot be collected on a day-to-day basis.
Extensive analyses of the relative merits of the two Bayesian risk models described above were presented in the last Report. These demonstrated that whilst both models discriminated well, the complex model consistently showed slightly better discrimination than the simple model (ROC area 0.744 for the simple model versus 0.750 for the complex model; data used to build the models).
The complex model also performed a little better in terms of calibration. The chart below shows the difference between the actual ratio of observed to expected and the ratio for a perfect fit between observed and predicted: ( Observed deaths ÷ Predicted deaths ) – 1; a value of 0 would be a perfect match, anything greater than 0 would be too many deaths predicted by the model and less than 0 would be to few deaths predicted; the greater the differences, the poorer the model. The chart demonstrates that, when viewed as a whole, the complex model appears to superior to the simple model.
Isolated CABG: A comparison of the calibration plots for the simple and complex Bayes models; financial years 1999 & 2000 (n=33,392
Simple Bayes model Complex Bayes model
For these reasons, the complex Bayes model was chosen as the Bayes model to be used in further analyses, especially in sequential analyses (see pages 249-259). Detailed results from analyses of using the complex Bayes model will be presented later in this report to allow comparison of this risk modelling technique with other established risk scores, but reference to the simple Bayes model will be confined to a section that demonstrates the relationship between the number of risk factors and missing data.
-0.20
-0.15
-0.10
-0.05
0.00
0.05
0.10
0.15
<1.0 1.0-1.9 2.0-2.9 3.0-4.9 5.0-9.9 >9.9
Risk groups
Dea
ths:
(Ob
serv
ed /
Pre
dic
ted
) - 1

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
230
NA
CSD
– C
AB
G s
urg
ery
risk
str
atif
icat
ion
The complex Bayes score
Key points from complex Bayes score analyses
• The score indicates an overall increase in risk over the last 5 years.
• The complex Bayes score is very accurate, even in higher risk groups.
• The Bayes score now slightly over-predicts risk.
• Mortality for each risk group falls year on year.
Complex Bayes score distributions through time
The Bayes model used here was first described in the 1999 Report. It remains relatively accurate today; it is a useful tool for measuring changes in casemix over time. The graph below shows that a reduction in the percentage of lowest risk cases, matched by an increase in medium risk cases.
Isolated CABG: Complex Bayes score distributions (n=107,287)
<1.0% 1.0-1.9% 2.0-2.9% 3.0-4.9% 5.0-9.9% >9.9%
0%
5%
10%
15%
20%
25%
30%
35%
40%
1999 2000 2001 2002 2003
Financial year
Per
cen
tag
e o
f pat
ien
ts

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
231
NA
CSD
– CA
BG
surg
ery risk stratification
Isolated CABG: Average complex Bayes score by gender (n=128,895)
Male Female All
2.0
2.5
3.0
3.5
1997 1998 1999 2000 2001 2002 2003
Financial year
Ave
rag
e B
ayes
sco
re

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
232
NA
CSD
– C
AB
G s
urg
ery
risk
str
atif
icat
ion
Mortality by complex Bayes score
The calibration plot below, for the complex Bayes score, shows a good fit between observed and predicted risk across the whole range of risk scores.
Financial year
1999 2000 2001 2002 2003
<1.0% 0.6% (n=5,734)
0.5% (n=5,945)
0.5% (n=6,735)
0.5% (n=6,868)
0.4% (n=7,209)
1.0-1.9% 1.5% (n=5,602)
1.4% (n=6,772)
1.2% (n=7,613)
1.0% (n=8,056)
1.2% (n=9,134)
2.0-2.9% 2.7% (n=2,167)
2.5% (n=2,743)
2.6% (n=3,075)
2.0% (n=3,373)
1.8% (n=4,038)
3.0-4.9% 4.9% (n=1,556)
3.4% (n=2,004)
3.5% (n=2,438)
3.7% (n=2,708)
3.1% (n=3,039)
5.0-9.9% 7.0% (n=958)
5.7% (n=1,306)
7.4% (n=1,461)
6.1% (n=1,469)
5.7% (n=1,801)
>9.9% 19.4% (n=439)
16.5% (n=565)
16.3% (n=710)
15.8% (n=740)
15.3% (n=713)
Co
mp
lex
Bay
es s
core
Unconfirmed 0.6% (n=5,734)
0.5% (n=5,945)
0.5% (n=6,735)
0.5% (n=6,868)
0.4% (n=7,209)
Isolated CABG: Mortality by complex Bayes score for financial year 2003 (n=25,934)
Observed Predicted
0%
2%
4%
6%
8%
10%
12%
14%
16%
18%
20%
<1.0% 1.0-1.9% 2.0-2.9% 3.0-4.9% 5.0-9.9% >9.9%
Complex Bayes score
Mo
rtal
ity
rate

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
233
NA
CSD
– CA
BG
surg
ery risk stratification
Isolated CABG: Mortality by complex Bayes score (n=106,971)
<1.0% 1.0-1.9% 2.0-2.9% 3.0-4.9% 5.0-9.9% >9.9%
Completeness of the complex Bayes score data
The complex Bayes score may be calculated whether or not an individual risk factor data item is missing; this means that every isolated CABG entry in the database can have a complex Bayes score. However, the accuracy of the score’s prediction is dependent, to some extent, on the number of risk factor data that are complete.
0%
2%
4%
6%
8%
10%
12%
14%
16%
18%
20%
1999 2000 2001 2002 2003
Financial year
Mo
rtal
ity
rate

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
234
NA
CSD
– C
AB
G s
urg
ery
risk
str
atif
icat
ion
Missing data
Missing data prevents meaningful risk adjusted comparisons between units or surgeons. It also prevents other analyses that may be of value for understanding cardiac surgical practice.
The collection of complete and accurate data is unequivocally the responsibility of the submitting unit (see audit guidelines; appendices this report). This was conveyed to all Trust chairmen in England in a letter dated 29th October 2002 from Lord Philip Hunt (Minister of Health), Prof. Peter Hutton (Chairman of the Academy of Medical Royal Colleges) and Mr Colin Hilton (President of the Society of Cardiothoracic Surgeons).
The number of responses has been very disappointing.
Missing simple Bayes variables
Calculation of the simple Bayes score utilises only 5 variables, determined from 6 data-items; data collection for these data-items is now complete for almost 90% patients. The incomplete data is largely attributable to a small handful of hospitals whose data collection systems are evolving.
Isolated CABG: Missing simple Bayes score variables (n=133,906)
0 1 2 3 >3
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
1996 1997 1998 1999 2000 2001 2002 2003
Financial year
Per
cen
tag
e o
f pat
ien
ts

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
235
NA
CSD
– CA
BG
surg
ery risk stratification
Isolated CABG: Missing simple Bayes score variables; financial year 2003 (n=25,067)
0 1 2 3 >3
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Walsgrave Hospital
St James's Hospital Dublin
Southampton General Hospital
Royal Sussex County Hospital
Royal Brompton Hospital
Leeds General Infirmary
Harefield Hospital
Freeman Hospital
B lackpool Victoria Hospital
Queen Elizabeth Hospital
Hammersmith Hospital
Glasgow Western Infirmary
Derriford Hospital
N Staffordshire Royal Infirmary
Cardiothoracic Centre
University Hospital o f Wales
Bristo l Royal Infirmary
Glasgow Royal Infirmary
King's College Hospital
Northern General Hospital
M anchester Royal Infirmary
Castle Hill Hospital
St George's Hospital
Nottingham City Hospital
Papworth Hospital
Bart's and the London Chest
Golden Jubilee Hospital
Aberdeen Royal Infirmary
M orriston Hospital
Wythenshawe Hospital
Guy's & St Thomas'
Glenfield Hospital
The Heart Hospital
James Cook University Hospital
Royal Victoria Hospital Belfast
Edinburgh Royal Infirmary
St M ary's Hospital
John Radcliffe Hospital
Cen
tre
Percentage of patients

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
236
NA
CSD
– C
AB
G s
urg
ery
risk
str
atif
icat
ion
Missing complex Bayes variables
The chart below shows the effect of the step up from the simple Bayes score that utilises 5 variables to the Complex Bayes score that employs 9 variables.
Isolated CABG: Missing complex Bayes score variables (n=133,906)
0 1 2 3 >3
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
1996 1997 1998 1999 2000 2001 2002 2003
Financial year
Per
cen
tag
e o
f pat
ien
ts

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
237
NA
CSD
– CA
BG
surg
ery risk stratification
Isolated CABG: Missing complex Bayes score variables; financial year 2003 (n=25,067)
0 1 2 3 >3
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Royal Brompton Hospital
Queen Elizabeth Hospital
Southampton General Hospital
Glasgow Western Infirmary
Derriford Hospital
Freeman Hospital
N Staffordshire Royal Infirmary
University Hospital o f Wales
Blackpool Victoria Hospital
St James's Hospital Dublin
Harefield Hospital
Hammersmith Hospital
Castle Hill Hospital
St George's Hospital
M anchester Royal Infirmary
Cardiothoracic Centre
Nottingham City Hospital
Northern General Hospital
Bristo l Royal Infirmary
Wythenshawe Hospital
Leeds General Infirmary
Guy's & St Thomas'
Royal Sussex County Hospital
King's College Hospital
Bart's and the London Chest
Walsgrave Hospital
M orriston Hospital
The Heart Hospital
Glenfield Hospital
Royal Victoria Hospital Belfast
James Cook University Hospital
Edinburgh Royal Infirmary
Aberdeen Royal Infirmary
Glasgow Royal Infirmary
Golden Jubilee Hospital
John Radcliffe Hospital
Papworth Hospital
St M ary's Hospital
Cen
tre
Percentage of patients

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
238
NA
CSD
– C
AB
G s
urg
ery
risk
str
atif
icat
ion
Missing EuroSCORE variables
At present, the EuroSCORE is the agreed risk scoring system for use in the UK. It has been validated worldwide and is acknowledged as being reliable for large inter-group or inter-hospital comparisons.
The EuroSCORE requires the collection of 17 variables for risk measurement in coronary surgery patients. If one variable is missing then the score cannot be calculated reliably. The associated graphs show that on this basis the EuroSCORE could not be calculated on about 35% patients in the financial year 2002-2003. Although this represents a substantial improvement over the years it falls far short of an acceptable level of data collection.
In part this may be due to the fact that some EuroSCORE questions have only recently been added to local databases. Whatever the reason it highlights the need for peer review and data validation visits (see pages 31-32).
Isolated CABG: Missing EuroSCORE variables (n=133,906)
0 1 2 3 >3
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
1996 1997 1998 1999 2000 2001 2002 2003
Financial year
Per
cen
tag
e o
f pat
ien
ts

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
239
NA
CSD
– CA
BG
surg
ery risk stratification
Isolated CABG: Missing EuroSCORE variables; financial year 2003 (n=25,067)
0 1 2 3 >3
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Royal Brompton Hospital
N Staffordshire Royal Infirmary
Glasgow Western Infirmary
Harefield Hospital
University Hospital o f Wales
Bristo l Royal Infirmary
Derriford Hospital
Southampton General Hospital
St James's Hospital Dublin
St George's Hospital
Freeman Hospital
The Heart Hospital
Nottingham City Hospital
Cardio thoracic Centre
Leeds General Infirmary
Guy's & St Thomas'
Royal Sussex County Hospital
M anchester Royal Infirmary
Wythenshawe Hospital
Walsgrave Hospital
Bart's and the London Chest
Castle Hill Hospital
B lackpool Victoria Hospital
Queen Elizabeth Hospital
Royal Victoria Hospital Belfast
Hammersmith Hospital
Glenfield Hospital
Northern General Hospital
Edinburgh Royal Infirmary
Papworth Hospital
Glasgow Royal Infirmary
Golden Jubilee Hospital
James Cook University Hospital
King's College Hospital
St M ary's Hospital
M orriston Hospital
John Radcliffe Hospital
Aberdeen Royal Infirmary
Cen
tre
Percentage of patients

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
240
NA
CSD
– C
AB
G s
urg
ery
risk
str
atif
icat
ion
Testing a risk scoring system
Although there are a number of risk stratification models available, the Parsonnet, EuroSCORE and Bayes scoring systems are used most frequently. The EuroSCORE is a more recent additive model that is under assessment but seems to accurately predict outcomes in contemporary UK practice. Which is the most accurate system? Statisticians have a number of methods for measuring the predictive accuracy of such scoring systems. The Receiver Operating Characteristic (ROC) curve 37, 41 and calibration plots provide useful graphical representation of predictive accuracy.
Receiver Operating Characteristic (ROC) curve
Hanley and McNeil stated (with our insertions square brackets) that the area under the ROC curve:
… represents the probability that a randomly chosen diseased subject [or in this case a deceased patient] is (correctly) rated or ranked with greater suspicion than a randomly chosen non-diseased subject [or in this case a non-deceased patient].
A simplistic reworking of this statement would be that the area represents the probability that the risk predictor (in this report the Parsonnet score, the EuroSCORE or the Bayes score) accurately discriminates between patients who die during surgery and patients who survive surgery. An area of 0.50 indicates that there is no discrimination i.e., individuals in survivor-deceased patient parings are allocated to the correct group by the risk predictor according to chance. An area of 1.00 would indicate that discrimination was perfect, and any intermediate value is a quantitative measure of the ability of the risk predictor to distinguish between survivors and non-survivors. Obviously, the closer the value is to 0.50 the less accurate the discrimination, and the closer to 1.00 the better the discrimination.
Calibration plot
Risk scores must also provide an estimate of the risk for both individual patients and groups of patients. One way to test this component of a risk score is to plot the observed number of events against the predicted number of events, and this is termed a calibration plot. To simplify the procedure, the data can be split into groups, according to risk, and the observed and predicted outcome rates plotted side by side. If the model accurately predicts the outcome, the two should match closely.

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
241
NA
CSD
– CA
BG
surg
ery risk stratification
Comparisons of risk scoring systems
All the following comparisons use only the data where all scores are present (limitation ∴ set by Parsonnet / EuroSCORE). This is to make the comparisons more valid – comparing like with like, an even playing field; it also has the benefit of selecting entries where the data collection is more complete, which should increase the accuracy of the Bayes score over a situation where all entries are used in the analyses describing the Bayes score’s results.
ROC curve areas
Isolated CABG: Calibration plot chi-squared values for 4 different risk models (n=43,822)
Parsonnet score EuroSCORE
Logistic EuroSCORE Complex Bayes score
0.64
0.66
0.68
0.70
0.72
0.74
0.76
0.78
0.80
0.82
0.84
1999 2000 2001 2002 2003
Financial year
RO
C c
urv
e ar
ea

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
242
NA
CSD
– C
AB
G s
urg
ery
risk
str
atif
icat
ion
Calibration
The chi-squared value is a measure of closely the predicted mortality matches the actual mortality. The smaller the chi-squared value, the better the match.
The key messages are that the match was good for both the EuroSCOREs and the complex Bayes score, but, as time goes by, the match between observed and predicted mortality slowly drifts apart for all the scores.
Isolated CABG: ROC curve areas for 4 different risk models (n=43,819)
Parsonnet score EuroSCORE
Logistic EuroSCORE Complex Bayes score
Chart above with Parsonnet score line removed
0
50
100
150
200
250
300
350
400
450
500
1999 2000 2001 2002 2003
Financial year
Ch
i-sq
uar
ed v
alu
e
0
20
40
60
80
100
120
140
1999 2000 2001 2002 2003
Financial year
Ch
i-sq
uar
ed v
alu
e

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
243
NA
CSD
– CA
BG
surg
ery risk stratification
The preceding graphs indicate that the accuracy of all risk prediction models varies with time, but that the complex Bayes Score is consistently the most accurate model for prediction of death following coronary surgery in the UK. Although this score appears to be more accurate and requires the collection of slightly fewer data-items, it is a little more complicated to calculate than the EuroSCORE.
Isolated CABG: Observed and predicted mortality rate by age for 4 different risk models; financial years 2001-2003 (n=31,296)
Observed
Parsonnet score EuroSCORE
Logistic EuroSCORE Complex Bayes score
Chart above with Parsonnet score bars removed
0%
2%
4%
6%
8%
10%
12%
14%
16%
18%
20%
<56 56-60 61-65 66-70 71-75 >75
Age at surgery / years
Mo
rtal
ity
rate
0%
1%
2%
3%
4%
5%
6%
7%
8%
9%
<56 56-60 61-65 66-70 71-75 >75
Age at surgery / years
Mo
rtal
ity
rate

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
244
NA
CSD
– C
AB
G s
urg
ery
per
form
ance
ind
icat
ors
Performance indicators and the presentation of surgical results
The application of risk stratification
The operative mortality for coronary artery bypass surgery was incorporated into the basket of clinical indicators used by the Department of Health in the NHS Performance Ratings for trusts (see page 267, 269 and 272-274). Several of these clinical indicators are based on data required for the implementation of the National Service Frameworks, which, in the case of coronary heart disease, includes the Society of Cardiothoracic Surgeons recommended dataset.
However, the public release of comparative performance indicators or league tables remains a sensitive issue among clinicians, largely for fear of misinterpretation by the media and patients. In this section we examine some of the more technical aspects of how comparative data can be presented in an easily interpretable fashion, so as to encourage rigorous, but fair, evaluation of clinical performance, whilst highlighting potential pitfalls in interpretation. The most appropriate means of presentation is still a subject of protracted debate, and the current lack of well-validated data provides an opportunity for us to illustrate some of the issues surrounding the presentation of potentially sensitive data. Although based on real data, the following analyses should be taken purely as illustrative, and are simply intended to stimulate discussion.
To this end, the Society is in collaboration with the Nuffield Trust, the RAND organisation and the California Department of Health to draw on the experience of the public release of outcome data in North America. Any additional feedback on ways in which the fairness and objectivity of the presentation might be improved would be welcomed by the Society.
Why do we need statistical analysis at all?
Statistical analysis attempts to allow for the effects of natural variability that arises from inevitable and unpredictable differences between patients and surgeons, as well as between operations and outcomes. Any analysis based only on a limited number of cases will always be subject to errors. If a surgeon operates on two patients and they both survive he has a mortality of 0%, but if one dies he has a statistical operative mortality of 50%. No one would believe that either percentage represented the real risk for patients operated on by that surgeon. Assuming that one of the first two patients died following their operation, the surgeon might then do another 48 operations with no deaths. After the fiftieth operation his mortality would be calculated as 2%. At this point, a reasonable person might guess that this surgeon’s true mortality rate is around 2%, but would not have been prepared to make a guess at his level of performance based on the first two cases. So, the greater the number of cases with known outcomes the more certain one can be of the true risk of an operation under that surgeon. Statisticians cope with this by creating mathematical confidence limits around any outcome based on the number of observations or cases performed. In the example above where one of two patients dies we cannot be absolutely confident that that surgeon’s mortality is 50% but we can be 95% confident that the actual risk lies between 2.7% and 97.3%. By the time the surgeon has done 50 cases with only one death, we can be 95% confident that his real operative mortality lies between 0.1% and 12.0%. So the greater the number of cases, the more accurate the assessment becomes.
In practical terms, we look at data over defined time periods: one year, two years or three years, so that there are a meaningful number of cases to analyse 42. Even so, these short series represent only a snapshot in time, and may not necessarily be representative of overall performance; even if a surgeon or centre had no deaths within the chosen timeframe, we would not necessarily believe that this happy situation would continue forever. Similarly, a short run of bad outcomes should be regarded with caution. It follows that decisions regarding so-called divergent outcomes must take into account random variability and should not be based simply on the observed rate. Casemix must also be considered.
The precision with which comparisons can be made depends primarily on the number of adverse outcomes. Thus, the outcomes of a high risk procedure can be judged with greater statistical certainty using fewer operations than for a low risk procedure. Increasing the denominator, or total number of low risk procedures for analysis, may require:
• Aggregating the number of procedures over time, e.g., three years’ activity may be necessary to obtain enough observations for confident results.
• Combining well-defined, common groups of operations for analysis.
• Using near-miss and deaths as adverse events instead of deaths alone.

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
245
NA
CSD
– CA
BG
surg
ery perfo
rman
ce ind
icators
Setting a benchmark threshold for comparison
Benchmark thresholds may be either absolute or relative.
• Relative thresholds are defined according to statistical measures of overall performance, such as an average or two standard deviations from the average. Taken to its logical conclusion, this approach could penalise everyone above the benchmark at that time, even though there may be neither real nor meaningful difference between their performance and the benchmark. Fifty percent of all people are below average intelligence, 50% of lawyers are below average as are 50% of doctors below average. This is a product of statistics and not a judgement on people, on lawyers or on doctors.
• Absolute thresholds rely on specification of the upper end of acceptable performance, and possibly the lower end of unacceptable performance with a grey area that lies in between.
The graphical presentation of results
The aim of presenting performance data is generally to be able to show normal variation between institutions and identify significant divergence from normal or otherwise defined performance. In this section we describe four general categories of data presentation:
• Average outcome over a given timeframe:
• Crude survival plots or crude mortality plots.
• Observed versus predicted plots.
• Standardised mortality ratio (SMR) plots.
• Volume and outcome control charts:
• Funnel plots 43.
• Spectrum plots.
• Performance trends over time (Statistical process control charts):
• Cumulative Summation charts (CUSUM) 44, 45.
• Risk adjusted trend charts:
• Variable Life Adjusted Display charts (VLAD Plots) 46, 47.
• Risk Adjusted CUSUM 48.
• Sequential Probability Testing Ratio (SPiRiT) 49.
We describe a series of charts that can be used to chart performance or outcomes over time. The most basic charts simply plot the outcome of survival or death for each operation over time. The more sophisticated methods take into account the pre-existing risk of the patient. These are useful for monitoring performance in real time and are commonly used in most cardiac surgical centres. These are described under the following headings:
Average outcomes over a given timeframe
Ranking analyses
The death or survival rates for a number of institutions or individuals are plotted as a histogram and ranked with the best at one end and the worst at the other end. School league tables based on exam results are a typical example. But everyone knows that children attending an academic public school have a better start than kids attending a deprived inner city school. The inner city school may not achieve such good exam results but it may well be a perfectly good, or educationally better, school doing its best with under-privileged children. The same is true of hospitals. There is very clear evidence that some of the best academic and teaching hospitals have higher death rates than ordinary hospitals because they take on worse cases often referred by other local hospitals.

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
246
NA
CSD
– C
AB
G s
urg
ery
per
form
ance
ind
icat
ors
To take account of this variation the patient population at each hospital can be mathematically standardised to take account of variation in age, sex and other variables. This is called risk stratification. Simple risk stratification systems only take account of age and sex. More complicated systems take account of many other variables. The risk adjusted outcomes can be related to observed or actual outcomes to provide a standardised mortality ratio (SMR) or the difference from the expected mortality. However, it would be misleading to claim that statistical procedures can ever fully adjust for pre-existing risk factors.
Observed versus predicted (O vs. E) plots show the observed in-hospital mortality together with the predicted mortality for each centre. Vertical lines may be used to represent 95% confidence limits around the observed mortality rate; these limits show the range where we are 95% confident that the centre’s true mortality rate lies. If the limits for one centre do not overlap with the limits for another centre then it is likely that there is a real difference between the mortality rates in the two centres.
Standardised mortality ratio (SMR) plots show the ratio of observed to predicted mortality (O ÷ E). This method compensates to some extent for casemix, but is highly dependent on the reliability of the method used to adjust for casemix. If the 95% confidence limits around the SMR fail to overlap with SMR = 1, then a real difference between the actual and predicted outcome rates has been identified.
However, by chance alone, like any event that has a random component such as the toss of a coin, one in forty centres (2.5%) will be identified as significantly below average, even if their true performance were within the benchmark level. This indicates the need for caution in interpreting statistically significant results. This technique is essentially testing the hypothesis that all the centres have exactly the same underlying mortality rate which is highly unlikely in the real world.
In addition, the practice of ranking institutions to create league tables has the potential to be extremely misleading, since ranks are notoriously sensitive to chance variability. For this reason, techniques have been developed for placing 95% confidence intervals around observed ranks 50; but this is not always enough. League tables of cardiac units in North America have clearly shown that a unit’s position can vary substantially from one year to the next, more due to the effects of chance than to a change in the quality of care delivered by the centre 42, 51. A typical pattern shows great uncertainty around the observed rank - we can seldom be 95% confident that any particular centre lies in any particular echelon of a league table. The confidence intervals around the ranks are also sensitive to the risk model that is used in the risk adjustment, which adds a further layer of complexity to the interpretation of such graphs.
There is considerable danger in generating spurious false-positive findings when carrying out many comparisons, although statistical techniques do exist for dealing with this phenomenon. One such technique is the Bonferroni adjustment, which essentially widens the confidence intervals that are used to indicate uncertainty, whereas the shrinkage estimation method 52 makes adjustments to all estimates of outcome rates based on an estimate of the expected regression-to-the-mean, pulling them towards the overall average. These methods could, of course, lead to an excess of false-negatives in which genuinely divergent behaviour goes undetected. The Statistician’s phrase regression-to-the-mean describes the tendency for institutions that have been identified as extreme to become less extreme when monitored in the future - put simply, part of the reason for their extremeness was a run of good or bad luck. This simple phenomenon could lead to spurious claims being made about the benefit of interventions to rescue failing institutions. Shrinkage estimation is intended to counter this difficulty.
Perhaps the most important idea is that there is little gained from measuring variability in outcomes unless one can suggest underlying causes and remedial interventions. Someone must always be bottom of any league table, and the vital issue is whether they are truly divergent and, if so, why? Investigating the underlying reasons for variability in outcomes is not straightforward: while adjustment for casemix is, in principle, possible, one must keep in mind that clinicians may respond to individual patient's situations in different but appropriate ways. Investigations must value that clinical skill

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
247
NA
CSD
– CA
BG
surg
ery perfo
rman
ce ind
icators
Funnel plots
Shewhart control charts have been suggested as a means of presenting performance indicator results in the healthcare setting without having to resort to spurious ranking into league tables 53, 54. These plots show observed number of events against volume of cases on a square root scale; unfortunately this format appears unintuitive, obscures the observed event rates, and leads to rather approximate control limits. Applying a small adjustment – plotting the event rates against volume of cases – leads to the so-called funnel plot, which is widely used in meta-analyses to check for publication bias 55 and has also been used to compare mortality rates in paediatric cardiac surgery 56. Exact binomial control limits around the overall event rate are superimposed to indicate possible thresholds for alert and alarm respectively.
Funnel plots discourage inappropriate ranking while providing a strong visual indication of divergent performance or special cause variation. Advantages over the Shewhart control chart approach include the display of the observed event rates, an informal check of the relationship between event rate and volume of cases, an emphasis on the increased variability expected from smaller centres, intuitive choice of axes (hence easy plotting) and exact Binomial control limits easily obtainable from the most popular spreadsheet packages.
The example funnel plot below is not risk adjusted, and therefore has all the problems associated with not comparing like with like.
NACSD: All isolated CABG: Funnel plot on two years’ data by centre; financial years 2002 & 2003 (n=47,859)
Overall rate 99 % lower alert 99% lower alert Centre
99.9% lower alarm 99.9% lower alarm
If we attempt to introduce a level of adjustment for risk, by applying the analysis to a sub-population of patients such as those aged less than 70 undergoing an elective, first-time coronary operation, then the picture changes, as shown overleaf. Sometimes, the changes may be dramatic and, just as with league tables, one analysis cannot provide the whole story.
0%
1%
2%
3%
4%
5%
6%
0 500 1,000 1,500 2,000
Number of cases
Cru
de
mo
rtal
ity
rate

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
248
NA
CSD
– C
AB
G s
urg
ery
per
form
ance
ind
icat
ors
NACSD: First-time, elective isolated CABG for patients aged less than 70 years: Funnel plot on two years’ data by centre; financial years 2002 & 2003 (n=22,941)
Overall rate 99 % lower alert 99 % lower alert Centre
99.9% lower alarm 99.9% lower alarm
The following centres submitted only one year’s data (financial year 2003): Edinburgh Royal Infirmary, Golden Jubilee Hospital Glasgow and St Mary’s Hospital London.
0%
1%
2%
3%
4%
5%
6%
0 200 400 600 800 1,000 1,200
Number of cases
Cru
de
mo
rtal
ity
rate

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
249
NA
CSD
– CA
BG
surg
ery perfo
rman
ce ind
icators
Sequential analyses
Standard CUSUM
The standard CUSUM chart plots a cumulative number of events against time 44. In the context of heart surgery, an event might be an adverse outcome, such as post-operative death, and time might be defined by the date-order in which operations were performed, the operative sequence. Most frequently, the adverse outcome in these kinds of analyses is an operative death. In order to standardise the timeframes, the first operation would be given the operative sequence number of 1, the second operation would be given a operative sequence number of 2 and so on.
The calculation of the standard CUSUM value is relatively simple. Each of the observed outcomes is given a numerical value: the adverse outcome is given a value of 1 and other outcomes are given a value of 0; these values are equal to the outcome rate for the individual patients. These values are then summed across the operative sequence to give the CUSUM value. In mathematical notation, this would be:
∑Δ=
=
=np
ppnC
1
n is the number of operations in the sequence
Cp is the CUSUM value at operation number p; the observed number of adverse outcomes
Δp is the observed outcome for the patient at operation number p
These CUSUM values can be plotted against a predicted outcome rate, in order to visualise differences between observed and predicted outcome rates. To calculate the predicted CUSUM value the predicted outcome rate is first converted to probability. For a 5% risk, the probability of an adverse outcome would be 0.05, for a 10% risk the probability of an adverse outcome would be 0.10, and so on. These probabilities are summed across the operative sequence in much the same way as the observed outcome rates, but, for the purposes of charting, they are rounded down to the nearest whole number. For example, taking a series of 99 operations where each patient has a 1% risk of the adverse outcome, the corresponding probability of the adverse outcome would be 0.01 for each patient. Summing these probabilities over the series of 99 operations would give a predicted CUSUM value of 0.99. For charting purposes this would be rounded down to 0. If one more patient were added to the series, also with a 1% risk of the adverse outcome, the predicted CUSUM would then be 0.99 + 0.01 = 1.00. On the chart, the predicted CUSUM value would now be 1. This explains the stepped appearance of both the observed and predicted CUSUM plots. In mathematical notation the predicted CUSUM would be:
∑=
=
=np
ppnP
1int δ
Pn is the predicted CUSUM value at operation number p; the predicted number of adverse outcomes
δp is the predicted outcome rate for the patient at operation number p
The following chart shows the observed and predicted cumulative number of adverse outcomes for all isolated CABG procedures performed by one of the contributing centres over a two-year period. An adverse outcome was defined as death for this particular chart. The cumulative risk across this series of 640 operations, according to the complex CABG Bayes score, is 15 patients i.e., 15 patient deaths are predicted.
It is possible that the observed number of deaths is greater than the predicted number of deaths at some points along the curve, and less than the predicted number of deaths at other points, but for this centre the number of deaths is consistently less than the predicted number of deaths. The end-point of the curve shows that there were 3 patient deaths less than predicted. This sort of visual representation of data is sensitive to the point at which the analysis commences, and the point at which the analysis ends. It is important to bear this in mind whenever examining these charts.

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
250
NA
CSD
– C
AB
G s
urg
ery
per
form
ance
ind
icat
ors
Isolated CABG: Standard CUSUM plots for financial year 2001 for the North Staffordshire Royal Infirmary (n=640)
Observed
Predicted Parsonnet EuroSCORE
Logistic EuroSCORE Complex Bayes
The results of this technique are heavily dependant on the risk model that is used as the predictor of the adverse outcome. Any risk score that has been designed to predict the adverse outcome of interest could be used in the calculations that create these curves. For example, in cardiac surgery risk scores such as the Parsonnet score, the EuroSCORE and Bayes scores are often employed.
In Parsonnet’s original paper a Parsonnet score of between 0 and 4 carried an average operative mortality risk of 1%, a Parsonnet score of between 5 and 9 carried an average operative mortality risk of 5%, and so on up the risk score scale. Each time a surgeon operates on a patient with a Parsonnet score of between 0 and 4 there is, according to Parsonnet’s original data, a 1% chance that the patient will die. If a surgeon operates on 100 such patients then Parsonnet would predict that one patient would die; the cumulative risk in this series is one patient death.
However, the predicted values quoted in Parsonnet’s original paper are now out of date as practice in cardiac surgery has moved on, and, as a result, the observed mortality rate for each of the Parsonnet score groups has fallen. Any risk adjusted analysis of current mortality rates that employed the Parsonnet score as the predictor of death would tend to over-estimate the risk. In such an analysis, the observed mortality rate would tend to appear much lower than the predicted rate.
So, the exact position of the standard CUSUM curve with respect to the predicted number of adverse outcomes is greatly affected by the risk score that is used and the probability of death attached to that score. This applies equally to the VLAD and the Risk Adjusted CUSUM plots that follow. All of the following charts employ the complex CABG Bayes score as the predictor of death, since this is a contemporary, risk score that has been shown to reflect recent outcome rates across the UK; in the case of the complex CABG Bayes score the predicted risk is equal to the value of the score.
A note of caution: these visual representations provide useful tools to highlight trends that may need closer examination. In the format above, it cannot be used to determine a statistically significant departure from expected performance nor statistically significant differences between hospitals or surgeons. Furthermore, no risk score will be able to account for all the risk factors that may affect outcomes. Each will contain the most frequently encountered and measurable risk factors that impinge on the outcome they intend to predict. However, if only one surgically relevant risk factor that is absent from the risk model occurs frequently within the patient population of a hospital (or a surgeon) and not in the patient populations of other hospitals (or surgeons), then these plots will not paint an entirely accurate or fair picture. The complex CABG Bayes score is the best available approximation to the true risk at the present time. Even the Risk Adjusted CUSUM method should be used as an indicator and not as the final word in comparative mortality analyses.
0
5
10
15
20
25
30
35
40
100 200 300 400 500 600
Sequence
Cu
mu
lati
ve s
um
/ p
atie
nts

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
251
NA
CSD
– CA
BG
surg
ery perfo
rman
ce ind
icators
Setting control limits around CUSUM curves
Using a standard CUSUM chart it is possible to identify deviations from a predicted outcome rate. It is useful to have some preset criteria for formally specifying that a deviation from a steady rate has taken place. These criteria are defined in statistical terms, and the choice of test is very important. Straightforward, standard tests of statistical significance after every operation are not appropriate. This would constitute multiple testing, and statisticians have determined that the results from these tests are misleading. Sequential testing techniques were developed during the 1940s in an attempt to avoid these problems of multiple testing.
It is possible to draw two extra boundary lines on the standard CUSUM chart: an alert line and an alarm line. If the CUSUM line crosses either of these boundary lines there is an indication that the observed outcome rate has exceeded a pre-determined target rate, po. The mortality rate in the data used to generate the CUSUM chart above was 2.3%, so po might be set to 0.023. In order to avoid too many false alarms, a number of other parameters must be set: the first is a fixed chance that the CUSUM line will cross a boundary when the true outcome rate is still po; this parameter is designated a, and is usually either 0.05, for a 5% chance, or 0.01, for a 1% chance. The next parameter is another outcome rate that is important to detect, which is designated p1; it may be a higher outcome rate or a lower outcome rate, depending on whether the test is designed to look for worsening or improvement in performance. In the sample data used previously, the actual mortality rate was 2.3%, so a higher rate might be set at 3.3% and a lower rate might be set at 1.3%. Finally, the power of the analysis must be set, which defines the chance of correctly rejecting the target rate in favour of p1, according to the other criteria that have been set; this is denoted 1 -b. The power of these analyses is typically set to 80%, which means that b would be, in probability terms, 0.20.
In order to calculate the positions of the boundary lines from these parameters, a number of components are needed:
⎥⎦⎤
⎢⎣⎡ −
=α
β1loga
⎥⎦
⎤⎢⎣
⎡=
0
1logppP
⎥⎦⎤
⎢⎣⎡
−=
αβ
1logb
⎥⎦
⎤⎢⎣
⎡−−
=11
1logppQ o
QPQs+
=
Finally, the boundaries can be calculated for each point along the curve; again n is the number of the operation in the sequence:
alert boundary
⎟⎟⎠
⎞⎜⎜⎝
⎛+
−⋅=QPbsnalert
alarm boundary
⎟⎟⎠
⎞⎜⎜⎝
⎛+
+⋅=QPasnalarm
This chart shows that none of the boundary lines, as defined above, are crossed. This means that there is neither a worsening in the mortality rate nor an improvement. Different parameters would give different results.

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
252
NA
CSD
– C
AB
G s
urg
ery
per
form
ance
ind
icat
ors
Isolated CABG: Standard CUSUM plot with limits for financial year 2001 for North Staffordshire Royal Infirmary (n=640)
Observed
Improvement Alert Alarm
Worsening Alert Alarm
This method simply takes a pre-defined outcome rate and determines whether or not the observed rate deviates from this rate. This method is not risk adjusted and therefore will not take account of any changes in casemix over time.
5
10
15
20
25
100 200 300 400 500 600
Sequence
Cu
mu
lati
ve s
um
/ p
atie
nts

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
253
NA
CSD
– CA
BG
surg
ery perfo
rman
ce ind
icators
Variable Life-Adjusted Display (VLAD)
As with the standard CUSUM method, VLAD analysis 46, 47 can be used to examine any event rate as long as a suitable predictor exists for that event. For the purposes of the examples and charts in this section, an event was defined as death.
Plotting cumulative risk
This plot always has an upward trend and illustrates the cumulative risk over the operative sequence. Application and extension of this method can be used to calculate the cumulative risk associated with any group of patients using any suitable risk score. The following equation describes this approach:
∑=
=
=np
ppn
1δρ
n is the number of operations in the sequence
δp is the predicted outcome rate for the patient at operation number p
ρn is the cumulative risk when the operation sequence is n
This kind of plot allows a visual comparison of predicted, cumulative risk from different sources, be they different hospitals or different surgeons. The curve is not shown, as it is not a necessary component of the VLAD analysis; the comparison of observed and predicted outcome rates is contained entirely in the VLAD itself.
The VLAD plot
This curve attempts to provide a visual representation of performance against the predicted outcome rate. It may trend up or down over time.
Effectively, when the analysis begins the VLAD-value, which has units of patients, is set to zero. If a patient survives their operation, overall VLAD-value increases in a manner that relates to the patient’s mortality risk. If the patient had a risk of 60% then the value increases by 0.6 patients, if the patient had a risk of 10% VLAD-value increases by 0.1 patients and so on. However, if the patient dies following the operation then the VLAD-value decreases. For the patient with a predicted mortality risk of 10% the decrease would be 0.9 patients, whereas for the patient with a risk of 60% the decrease would be only 0.4 patients. The death of a high risk patient is therefore appropriately weighted.
With each operation VLAD-value increases or decreases according to the risk of the operation, and at various times the net value will be positive, negative or zero. An overall positive value implies that more patients have survived than one would expect according to the risk model, whereas an overall negative value implies that more patients have died than expected. A zero value is exactly what the risk model predicts. Transitions from overall positive to overall negative values and back again are commonplace, and reflect the nature of normal surgical practice. The mathematical description of this concept is as follows:
∑ Δ=
=
−=Ρnp
pppn
1δ
n is the number of operations in the sequence
δp is the predicted outcome rate for the patient at operation number p
Δn is the observed outcome rate for the patient at operation number p
Pn VLAD-value, the cumulative difference between the expected and observed outcome rates

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
254
NA
CSD
– C
AB
G s
urg
ery
per
form
ance
ind
icat
ors
An observed mortality rate can have a value of either 1 (certainty of death) or 0 (certainty of survival). If a patient has a 1% risk of dying then the value of δp will be 0.01, if a patient has a 5% risk of dying then the value of δp will be 0.05, and so on. If a surgeon operates on a patient with a mortality risk 1% and this patient survives then the positive value is:
0.01 (chance of death) - 0 (survival) = 0.01 patients
The VLAD-value for a series of 99 such patients would be 0.99 patients. Should the one-hundredth patient also survive then the VLAD-value is 1.00, or 1 patient fewer than expected. If, however, the one-hundredth patient dies, then the VLAD-value for this patient is:
0.01 (chance of death) - 1 (death) = -0.99 patients
Adding this value to the cumulative VLAD-value already determined for the previous 99 patients, all of whom survived, is 0.00. This is exactly the number deaths predicted by the risk model.
The VLAD shows, over the operative sequence, the number of patient-deaths fewer than expected where the values are positive, or greater than expected where the values are negative. As with the CUSUM chart above, the chart below uses the complex CABG Bayes score as the predictor of outcome for a group of isolated CABG patients from one of the contributing centres.
The end-point on the VLAD that employs the complex CABG Bayes score has an overall VLAD-value of 3 patients, or 3 patient-deaths fewer than predicted. At various points along the curve, the overall VLAD-value may rise above or below zero patients. The conclusions drawn from these analyses are, in part, dependent on the point in time at which the analysis starts and finishes.
Isolated CABG: VLAD plots for financial year 2001 for the North Staffordshire Royal Infirmary (n=640)
Parsonnet EuroSCORE Predicted
Logistic EuroSCORE Complex Bayes
In this format, it is not possible to determine statistical deviation from the predicted outcome rate. As with the standard CUSUM chart, it is important to remember that the shape of the curve and the end-points are dependant on the risk score that has been used in the calculations. An inappropriate or inaccurate risk score will produce misleading results.
-202468
101214161820222426
0 100 200 300 400 500 600
Sequence
VLA
D v
alu
e / p
atie
nts

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
255
NA
CSD
– CA
BG
surg
ery perfo
rman
ce ind
icators
Isolated CABG: VLAD plots for financial year 2001 for the North Staffordshire Royal Infirmary (n=640)
EuroSCORE Logistic EuroSCORE
Complex Bayes Predicted
The charts above show outcome results for one centre; the results are consistently better than predicted. It is quite normal for a VLAD curve to fluctuate either side of the expected line as in the chart reproduced from last year’s report below:
Isolated CABG: One centre’s VLAD plot for financial years 1999-2000 (n=2,221)
-2
0
2
4
6
8
10
12
0 100 200 300 400 500 600
Sequence
VLA
D v
alu
e / p
atie
nts
-10
-8
-6
-4
-2
0
2
4
6
0 500 1,000 1,500 2,000
Sequence
VLA
D v
alu
e / p
atie
nts

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
256
NA
CSD
– C
AB
G s
urg
ery
per
form
ance
ind
icat
ors
Risk Adjusted CUSUM (RA-CUSUM)
The standard CUSUM method may be used to monitor changes in surgical outcome rates, but suffers in that it does not adjust for risk. This means that it may signal either an alert or an alarm simply because an increase in the number of high risk patients having operations produces a concomitant increase in the number of deaths. VLAD analyses are risk adjusted, but this approach has no robust method for signalling significant deviations from the predicted outcome rate. A Risk Adjusted CUSUM (RA-CUSUM) method 48 has been developed that comprises the best components of the standard CUSUM and the VLAD, and although the calculations associated with this approach are a little more daunting than those used in the previous two methods, the underlying principles are the same. Those overwhelmed by the statistics in the previous sections should skip this section.
The method utilises odds ratios for its calculations. As described previously in the section on Bayes modelling, odds ratios may be calculated as the probability of event over the probability of an alternate event. Therefore, using our previous notation, the odds on having an adverse outcome for an individual patient are calculated as:
( )pp
δδ−1
Initially two hypotheses must be set: the first is HO, which is the outcome rate that we wish to test. This could be set to the level of current practice. The second, alternative hypothesis, HA defines the deviation from HO to be detected. Either increases in the outcome rate or decreases in the outcome rate may be detected. There is an odds ratio associated with each of these hypotheses; the odds ratio associated with HO is denoted ORO, and the odds ration associated with HA is ORA. Using our previous notation:
O
OOOR
δδ
= and
O
AAOR
δδ
=
δo is the probability of the adverse outcome under HO
δA is the probability of the adverse outcome under HA
If HA is set such that a doubling in the rate is to be examined, δA is clearly 2; if HA is intended to look for a halving in the rate, δA is 0.5. The method repeatedly tests HO against HA. Under HO the odds on an adverse outcome for an individual patient, OpO are:
( )ppO
pO
ORO
δδ
−
⋅=
1
The corresponding probability of an adverse outcome for this same patient is:
( )[ ]pOp
pOpO OR
ORδδ
δδ
⋅+−
⋅=
1
Under HA the odds on an adverse outcome for an individual patient, OpA are:
( )ppA
pA
ORO
δδ
−
⋅=
1
And, the corresponding probability of an adverse outcome for this same patient is:
( )[ ]pAp
pApA OR
ORδδ
δδ
⋅+−
⋅=
1

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
257
NA
CSD
– CA
BG
surg
ery perfo
rman
ce ind
icators
A log-likelihood ratio can then be calculated for each patient; it is denoted Wn. The form of the calculation depends on the actual outcome for that patient. If the patient does not have the adverse outcome, the calculation is:
⎥⎥⎦
⎤
⎢⎢⎣
⎡
⋅+−
⋅+−=
pAp
pOpn OR
ORW
δδδδ
11
log
If the patient has the adverse outcome, the calculation is modified to:
( )( ) ⎥
⎥⎦
⎤
⎢⎢⎣
⎡
⋅⋅+−
⋅⋅+−=
OpAp
ApOpn OROR
ORORW
δδδδ
11
log
Essentially, the method plots a cumulative value against time, in a similar way as the two previous methods. The difference comes in the way that that value is calculated. A cumulative Χ-value is calculated for tests intended to look for deterioration in the outcome rate, and a Ζ-value for tests intended to look for an improvement. These values are described by the formulæ:
( )ntn W+Χ=Χ −1,0max and ( )ntn W−Ζ=Ζ −1,0min
The max and min components of the formulæ simply mean that Χn is set to zero unless Χn-1 was positive, in which case it is calculated from Χn-1 and Wn, and Ζn is set to zero unless Ζn-1 was positive, in which case it is calculated from Ζn-1 and Wn.
Isolated CABG: RA-CUSUM plots for financial years 2001-2003 for the North Staffordshire Royal Infirmary; risk predicted by complex Bayes score (n=1,520)
Test for deterioration Test for improvement
Doubling alarm Halving alarm
In the chart shown above, an adverse outcome was set as a post-operative death and the probability of the adverse outcome was the complex CABG Bayes score.
Alarm lines, parallel to the x-axis, can be drawn on the chart, to indicate when the observed value signals either a significant deterioration or an improvement in outcome rates. The calculation of the position of these alarm lines is complex, and beyond the scope of this report. It is just as important to look for significant improvements in the outcome rate as it is to look for deteriorations, as good practice should be examined and disseminated.
-5
-4
-3
-2
-1
0
1
2
3
4
5
0 200 400 600 800 1000 1200 1400
Operative sequence
RA
-CU
SUM
val
ue

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
258
NA
CSD
– C
AB
G s
urg
ery
per
form
ance
ind
icat
ors
Sequential probability ratio testing (SPiRiT)
The fundamental problem with many sequential analysis techniques is that they cannot indicate significant deviation from predicted outcome rates without falling foul of the problems associated with multiple testing (when a true null hypothesis is certain to be eventually rejected). The sequential probability ratio testing (SPiRiT) plot is a sequential technique that can perform this function without such problems 49.
Below is an example of a risk adjusted version of the classical sequential probability ratio test that was developed for quality control of military supplies in the Second World War. It takes the form of a simple adaptation of a cumulative observed – predicted (O – E) plot. Instead of plotting cumulative O – E, accumulations of the following over the operative sequence are plotted:
Outcome
No event Event
Doubling of predicted )1ln( ip+− )1ln()2ln( ip+−
Test
Halving of predicted ⎟⎠⎞
⎜⎝⎛ −
21ln ip ⎟
⎠⎞
⎜⎝⎛ −+
21ln)2ln( ip
where
pi predicted rate for the ith patient
The formulae in the table are specific results for tests that look for a doubling in the predicted rate and a halving in the predicted rate. There are approximations for theses tests:
test for a doubling (0.69 × observed rate for patient i) – predicted rate for patient i
test for a halving (0.69 × observed rate for patient i) – (predicted rate for patient i ÷ 2)
In statistical terms, we are looking at two hypotheses, the null hypothesis, HO, and the alternative hypothesis, H1, and determining which is true. In the test for a doubling in the predicted rate the null hypothesis is that the rate is exactly as predicted and the alternative hypothesis is that the rate is double that predicted. In the test for halving the null hypothesis is that the observed rate is half that predicted and the alternative hypothesis is that the rate is as predicted. These are tests that are relatively simple to understand, but the technique can be applied to other differences between observed and predicted rates.
Each test produces a line that can trend up or down over time; it is possible to set control limits around these curves that run parallel to the x-axis of the chart. When the test curves cross the control limits then we can make some statements about accepting or rejecting the test hypotheses. Essentially, when the test curve for a doubling in the predicted rate crosses the upper control limit HO can be rejected, which means that excess mortality has been detected; when this test curve crosses the lower control limit then HO can be accepted, which means that performance is as predicted. When the test-curve for a halving in the predicted rate crosses the upper limit H1 can be rejected – there has not been a halving in the predicted rate. When the test curve for a halving in the predicted rate crosses the lower boundary HO can be accepted – there has been a halving in the predicted rate (all of these judgements are subject to the parameters used to set the control limits). As with the CUSUM curve with control limits above, the following chart has both alert and alarm control limits that represent different levels of confidence.
To simplify the charts for this report the upper and lower limits for both tests have been set so that they are identical and suitably colour-coded; when the orange test curve crosses the red control limits doubling has been detected and when the dark green test curve for a halving in the predicted rate crosses the green control limits a halving in the rate has been detected.

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
259
NA
CSD
– CA
BG
surg
ery perfo
rman
ce ind
icators
The position control limits are set according to the following formulae:
⎥⎦⎤
⎢⎣⎡
−=
αβ
1loga ⎥⎦
⎤⎢⎣⎡ −
=α
β1logb
where
a upper control limit
b lower control limit
α probability of rejecting HO when it is true (classical Type I error)
β probability of rejecting H1 if it is true (classical Type II error)
Whilst these are generalised formulae, when comparing many (n) individuals Bonferroni suggests using α=β=0.10/n for an alert line and α=β=0.01/n for an alarm line. Such an approach was used in the following chart:
Isolated CABG: SPiRiT plot for financial years 2001-2003 for the North Staffordshire Royal Infirmary; risk predicted by complex Bayes score (n=1,520)
Test for deterioration Test for improvement
Halving i Alert Alarm
Doubling i Alert Alarm
This plot demonstrates not only if there has been a significant deviation from predicted outcome rates but also when significance was attained. When control limits are crossed the analysis should begin again to retain the sensitivity of the test.
i Limits for the test set according to Bonferroni adjustment for 36 inter-centre comparisons.
-12
-9
-6
-3
0
3
6
9
12
0 200 400 600 800 1,000 1,200 1,400 1,600
Sequence
SPiR
iT v
alu
e

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
260
NA
CSD
– C
AB
G s
urg
ery
per
form
ance
ind
icat
ors
Beyond mortality Application of VLAD to the outcome of death ± near-miss-of-death
Mr Geoffrey Berg Consultant Cardiothoracic Surgeon, Western Infirmary, Glasgow
Mortality is a readily measurable end-point but may represent a poor indicator of quality of care, cost-effectiveness or use of resources. Our present mortality data does not differentiate the average surgeon delivering stable patients from theatre from the poor surgeon who has the back up of a good intensive care centre clawing patients back from the brink. Using death following first-time coronary artery surgery as a benchmark for a surgeon’s performance, even with risk stratification, is not sensitive due to the overall low mortality rate.
VLAD plots for 5 surgeons from one contributing centre using the Parsonnet score as the predictor of risk (n=5,405)
Morbidity following cardiac surgery is much more common, but it is more difficult to collect accurate data. Although many units are collating post-operative complication data, there are no requirements to publish these data. Numerous fixed scoring systems have been developed for cardiac surgery patients but there may be problems in applying these systems to different populations. Not only may patient demographics differ between countries but also within countries. A system developed in one timeframe may not be accurate in a different timeframe due to advances in surgical technique and post-operative management, or due to changes in resources. These systems also do not take account of local expertise.
For these reasons our centre developed a local system of risk stratification to be used in conjunction with established systems – to measure death and near-miss-of-death. To try and define an easy measurement of major morbidity following cardiac surgery we developed a series of measurements to record near-miss-of-death. This has been incorporated into a computer system so that the risk of death or near-miss-of-death can be estimated pre-operatively.
The development of various post-operative complications will often lead to prolonged ventilation or intensive care stay and initially we selected ventilation time, intensive care stay and time-to-discharge as a measure of near-miss-of-death. Although this incorporated many of the common post-operative complications such as stroke and peri-operative myocardial infarction, there were a number of important events that it missed. Intra-aortic balloon pump inserted post-operatively, acute renal failure, cardiac arrest and patient returned to theatre for a new cardiac procedure were added to ventilation greater than 72 hours, intensive care stay greater than 96 hours and discharge from hospital greater than 12 days.
-8
0
8
16
24
32
40
48
56
64
72
80
0 200 400 600 800 1,000 1,200 1,400
Sequence
Cu
mu
lati
ve V
LAD
val
ue
/ pat
ien
ts

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
261
NA
CSD
– CA
BG
surg
ery perfo
rman
ce ind
icators
If a patient had any of these events during the post-operative stay, they were classified as having a near-miss-of-death. This near miss event can then be counted and used as part of the audit process. Using Bayesian analysis, a scoring system can be developed and patients can be risk stratified for near-miss-of-death pre-operatively. This system has demonstrated some interesting findings; less than 10% of our coronary patients have a near-miss-of-death but over 20% of our valve patients do. Nearly 30% of our coronary patients with poor pre-operative left ventricular function either die or have a near-miss-of-death. We have found that obese patients have a lower mortality than average but an average risk of near-miss-of-death. As shown below cumulative risk adjusted plots can be made and may be more sensitive in highlighting consultants’ or trainees’ performance.
Cumulative risk adjusted mortality and morbidity plots for 5 surgeons from one contributing centre using a locally-derived Bayes score as the predictor of risk
(n=5,405)
It is possible to collect and audit post-operative morbidity using agreed definitions. All the units in Scotland submit their results to the Scottish Audit of Cardiac Surgery. Thirty-one post-operative data fields are included (using CCAD definitions). The results are published and are made known to our purchasers and referring physicians. Patients are now aware that adverse events happen in hospitals but are also aware that many of them are preventable. If we want to improve our overall outcomes we must move on from measuring and reporting mortality and record and report morbidity, late mortality and even relief of symptoms.
-40
-30
-20
-10
0
10
20
30
40
0 200 400 600 800 1,000 1,200 1,400
Sequence
Cu
mu
lati
ve r
isk
adju
sted
mo
rtal
ity
and
mo
rbid
ity
valu
e / p
atie
nts

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
262
NA
CSD
– In
stit
uti
on
an
d in
div
idu
al p
erfo
rman
ce

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
263
NA
CSD
– Institu
tion
and
ind
ividu
al perfo
rman
ce
Institution and individual surgeon performance without risk adjustment

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
264
NA
CSD
– In
stit
uti
on
an
d in
div
idu
al p
erfo
rman
ce
Institution- and individual-surgeon performance
A general perspective on the publication of cardiac surgical results in the post Bristol era
The mathematics behind the development of fair and meaningful comparative methodologies of healthcare performance is not trivial and it remains an evolving science 57, 58.
Florence Nightingale was one of the first in the UK to promote the collection, statistical analysis and public release of institutional surgical outcome data. When she published her league tables of London Hospitals in the mid 19th century she received acclaim in some quarters but was ostracised in others 59. Ultimately the league tables were deemed to be based on unreliable data and subject to institutional gaming and were not continued after her death. Nothing has changed. In the early 1900s Ernest Codman in the USA suggested that hospitals in general and surgeons in particular should measure and report their results. More importantly he believed that they should keep measures of the longer-term outcomes of surgical procedures so that institutions and surgeons could be compared on the basis of their end results. Not only did he feel that this would improve the delivery of the right care to the right patients by institutions but he also believed that the availability of such figures would enable patient choice. Whereas Nightingale had largely adopted a data based statistical approach Codman had recognised that hospitals must deliver service, teaching and research and that quality in any one of these areas was dependent upon quality in the other areas. To help him formulate his ideas he sought the views of industrial engineers who helped him perceive the hospital as a production system - an amalgam of clinical and non-clinical processes. Although not widely accepted, Codman’s views helped the American College of Surgeons develop their hospital standardisation programme in 1913 addressing five relatively benign aspects of hospital performance including the organisation and qualifications of medical staff, policies regarding professional work in the hospital, the medical records and clinical facilities. In 1919 at an American College of Surgeons conference the Director of the College reported that only 89 of 692 surveyed hospitals with more than 100 beds had met the newly agreed ACS standards. But the real message lies in the professional concern surrounding the anonymity of the hospitals that could not meet the standards. Leaders of the ACS who were concerned that hospital identities might become public met together at midnight in the basement of the Waldorf Astoria and fed the original reports into the hotel incinerator.
But times are changing. Medical science and technology are advancing. Improvements in information technology have seen an explosion in the amount of medical information available to all citizens through a multitude of sources, particularly on the World Wide Web 60, 61, 62, 63.64, 65,66 This has changed the relationship between physicians and patients irreversibly and for the better. People understand their medical problems and treatments better; their expectations are higher. They no longer overlook inequities of access to care, unfair waiting times or clinical quality issues. They want to be partners in their treatments. They are concerned about the safety and quality of care they receive, and this has been heightened by a number of high profile incidents in the NHS In the late 1980s and early 1990s which culminated in the Bristol Royal Infirmary Inquiry into the excessive mortality and morbidity of children undergoing heart surgery in that institution.
So, with growing concern over clinical and administrative standards in the wider NHS, open benchmarking of clinical outcomes and institutional performance became a high profile issue contributing to the introduction of the concept of clinical governance outlined in the white paper A First Class Service published in 1997. This document set out a package of proposals to support the delivery of more consistent and higher quality care to patients. The aim was to drive performance improvement by setting measurable national standards, through National Service Frameworks and the National Institute for Clinical Excellence and providing an environment for improving local clinical care through clinical governance. This would be underpinned by improved professional self-regulation and development and monitoring of standards through the Commission for Health Improvement, the NHS Performance Assessment Framework and the National Survey of Patient and User Experience. These were quite wide-ranging proposals and represented the first attempt to understand and measure the quality of service offered by the NHS since it inception 50 years previously - a remarkable deficiency of the biggest organisation in the UK.
In order to measure the quality of any service industry some sort benchmarking and performance assessment is the first step and is unavoidable. The NHS Performance Assessment Framework, published in April 1999, introduced a standardised approach to assessing performance in the NHS by encouraging measurement across six interdependent areas: Fair Access, Effective Delivery, Efficiency, sensitive and convenient User / Carer Experience, clinical outcomes and health improvement for the local population.

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
265
NA
CSD
– Institu
tion
and
ind
ividu
al perfo
rman
ce
The Performance Assessment Framework (PAF)
The health authority PAF comprises six areas of performance:·
• Health improvement.
• Fair access.
• Effective delivery of appropriate health care.
• Efficiency.
• Patient/carer experience.
• Health outcomes of NHS care.
The PAF for NHS hospital trusts is similar but only has four areas:
• Clinical effectiveness and outcomes.
• Efficiency.
• Patient/carer experience.
• Capacity & capability.
The assessment process is embryonic and evolving rapidly. There are various sources of comparative data - each with its own statistical methodology, advantages and disadvantages. In June 1999 the first sets of High Level Performance Indicators (HLPIs) and Clinical Indicators (CIs) were published.
The next few paragraphs describe the evolution of these indicators and show how cardiac surgical outcome measures have become incorporated into the wider assessment of NHS performance in England.
Department of Health high-level performance indicators
The high-level performance indicators were health authority indicators drawn from existing indicator sets including the Public Health Common Data Set and from evolving sources, such as the Clinical Indicators. Their stated aims were:
• To provide information to the public about performance in their local health services.
• To provide a basis for benchmarking performance of NHS organisations.
• To encourage the sharing of comparative information between NHS organisations.
• To promote the spreading of good practice within the NHS.
Department of Health Clinical Indicators
In the summer of 1999 the DoH released information on Clinical Indicators, providing information about individual NHS hospital Trusts, grouped into different types of Trusts. These were:
• In-hospital premature deaths.
• 30-day peri-operative mortality - emergency surgery admission.
• 30-day peri-operative mortality - non-emergency surgery admission.
• In-hospital mortality following fractured neck of femur.
• In-hospital premature deaths (30-day mortality following acute myocardial infarction).
• Health Outcomes of NHS health care 28-day emergency re-admission.
• Rate of discharge to usual place of residence following acute stroke within 56 days of emergency admission for patients 50 years or older.
• Rate of discharge to usual place of residence within 28 days of emergency admission with fractured neck of femur.
In an attempt to be even handed and reduce spurious variability, the deaths of high risk cases transferred to specialist units from another hospital were attributed to the Trust where surgery first occurred. The clinical indicators attracted a surprisingly subdued response from the public and media largely because the media and public exhibited greater than anticipated sophistication in recognising the weaknesses inherent in the data and difficulties in the analyses. Trusts, however, expended enormous effort in justifying areas of under performance to regional offices and health authorities.
Although most would agree that the 1999 Clinical Indicators were a valiant first attempt in the 50-year history of the NHS to measure and benchmark clinical quality nationally, there remain issues of credibility which revolve around data quality and difficulties in adjustment for casemix.
The indicators published in summer 2002 appeared as part of the Performance Star Ratings system. This system used performance indicators and any relevant assessments made by the clinical governance reviews

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
266
NA
CSD
– In
stit
uti
on
an
d in
div
idu
al p
erfo
rman
ce
conducted by the Commission for Health Improvement to give NHS organisations an overall performance rating.
The NHS Performance Indicators
In July 2000 an updated and expanded set of high-level performance indicators were combined with the clinical indicators into one analytical exercise to produce the NHS Performance Indicators. These indicators attempted to address each of the six areas defined in the Performance Assessment Framework.
In reality, the acute trust indicators consisted of the established Clinical Indicators described above, but these were supplemented with a set of Health Authority Indicators illustrated in the table below, divided into the six PAF areas.
Health improvement Patient / Carer experience of the NHS
Deaths from all causes (ages 15-64) Patients who wait less than 2 hours for emergency admission (through A & E)
Deaths from all causes (ages 65-74) Cancelled operations
Deaths from cancer Delayed discharge
Deaths from all circulatory diseases First outpatient appointments for which patient did not attend
Suicide rates Outpatients seen within 13 weeks of GP referral
Deaths from accidents Patients satisfaction
Serious injury from accidents
Fair access
Percentage of those on waiting list waiting 18 months or more
Inpatient waiting list Health Outcomes of NHS health care (Part 1)
Adult dental registrations Conceptions below age 18
Early detection of cancer Decayed, missing or filled teeth in five year old children
Cancer waiting times Readmission to hospital following discharge
Number of GPs Emergency admissions of older people
Practice availability Emergency psychiatric re-admissions
Elective Surgery rates Stillbirths and infant mortality
Surgery rates - Coronary heart disease
Effective Delivery of Appropriate Health care Health Outcomes of NHS health care (Part 2)
Childhood immunisations Breast cancer survival
Inappropriately used surgery Cervical cancer survival
Acute care management Lung cancer survival
Chronic care management Colon cancer survival
Mental health in primary care Deaths in hospital following surgery (emergency)
Cost effective prescribing Deaths in hospital following surgery (non-emergency)
Returning home following treatment for a stroke Deaths in hospital following a heart attack (ages 35-74)
Returning home following treatment for a fractured hip Deaths in hospital following a fractured hip
Efficiency
Day case rate
Length of stay
Maternity unit costs
Mental health unit costs
Generic prescribing
By 2002 the Trust level performance indicators had grown considerably and included a much wider range of measures including some key service standards defined in the National Service Frameworks along with a broader range of clinical indicators to try and reflect the quality of treatment that patients received.
Of particular relevance to our specialty was the inclusion of institutional 30-day mortality rates for coronary artery bypass surgery in both the Trust and Health Authority Indicators. In addition the Health Authority indicators had grown to include survival rates for lung cancer and the number of organ donors per million

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
267
NA
CSD
– Institu
tion
and
ind
ividu
al perfo
rman
ce
population. These indicators were grouped into the four NHS Performance Assessment Framework (PAF) areas for NHS hospital Trusts: Clinical effectiveness and outcomes; Efficiency; Patient/carer experience and Capacity & capability.
PAF area
No. February 2002, Detailed Indicator Name
i Percentage of patients discharged back to usual place of residence within 56 days of emergency admission to hospital with a stroke, aged 50 and over (age and sex standardised)
ii Percentage of patients discharged back to usual place of residence within 28 days of emergency admission to hospital with a hip fracture, aged 65 and over (age and sex standardised)
iii Emergency readmissions to hospital within 28 days of discharge (all ages), as a percentage of live discharges (age and sex standardised)
iv Emergency readmissions to hospital within 28 days of discharge following treatment for a fractured hip, as a percentage of live hip fracture discharges (age and sex standardised)
v Emergency readmissions to hospital within 28 days of discharge following a stroke, as a percentage of live stroke discharges (age and sex standardised)
vi Deaths within 30 days of surgery for non-elective admissions to hospital, per 100,000 patients (age and sex standardised, includes deaths in hospital and after discharge)
vii Deaths within 30 days of a Coronary Artery Bypass Graft (CABG), per 100,000 patients (age and sex standardised, includes deaths in hospital and after discharge)
viii Deaths within 30 days of emergency admission to hospital with a hip fracture, of patients aged 65 and over, per 100,000 patients (age and sex standardised, includes deaths in hospital and after discharge)
A
ix Deaths within 30 days of a stroke, per 100,000 patients (age and sex standardised, includes deaths in hospital and after discharge)
Institutional measures: Efficiency i Day case rate. Ratio of observed to expected day case rate for a basket of 25 procedures, adjusted for
differences in casemix
ii Length of stay. Ratio of observed to expected length of stay, adjusted for differences in casemix
iii Reference costs. Index comparison of the actual cost of a trust's activity with the same activity using national average costs
B
iv Missed outpatient appointments. Percentage of first outpatients appointments for which patient did not attend
Institutional measures: Patient and carer experience i Six-month inpatient waits. Percentage of patients waiting less than 6 months for an inpatient admission
ii Thirteen-week outpatient waits. Percentage of patients seen within 13 weeks of GP written referral for first outpatient appointment
iii Two-week breast cancer waits. Percentage of patients seen within 2 weeks of urgent GP referral for suspected breast cancer to outpatient appointment with specialist
iv Trolley waits. Percentage of patients admitted through A&E not placed in a bed on a ward within 4 hours of decision to admit
v Complaints. Percentage of written complaints for which a local resolution was completed within 4 weeks
vi Cancelled operations. Elective admissions that are cancelled at the last minute for non-clinical reasons as a percentage of elective admissions
vii Cancelled operations not admitted within a month. Patients not admitted within one month of last minute cancellation as a percentage of elective admissions
C
viii Hospital Cleanliness. Whole hospital score for cleanliness, formulated against PEAT visits
Institutional measures: Capacity & capability i Junior doctors' hours. Percentage of Junior Doctors complying in full with the New Deal on Junior
Doctors' Hours
ii Vacancy rate - Qualified Allied Health Professionals. Three month vacancies expressed as a percentage of three month vacancies plus staff in post
iii Vacancy rate - Qualified nursing, midwifery & health visiting staff. Three month vacancies expressed as a percentage of three month vacancies plus staff in post
iv Vacancy rate – Consultants. Consultants three month vacancies expressed as a percentage of three month vacancies plus staff in post
v Sickness absence rates. Amount of time lost through absences as a percentage of staff time available for directly employed NHS staff
vi Clinical negligence. Level of compliance against Clinical Negligence Scheme for Trusts (CNST) risk management standards
D
vii Data quality. Summary measure of Hospital Episode Statistics (HES) data quality for NHS trusts with inpatient activity

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
268
NA
CSD
– In
stit
uti
on
an
d in
div
idu
al p
erfo
rman
ce
The indicators published in February 2002 re-appeared in July, along with some new ones, as part of the Performance Star Ratings system. This system uses performance indicators and any relevant assessments made by CHI to give NHS organisations an overall performance rating.
The NHS Performance Ratings in England
The performance indicators provided stand-alone feedback to Trusts of their performance in the described areas. They did not try to provide an overall picture of a Trust’s performance relative to others. The NHS performance ratings were designed to provide a public, high-level summary of the overall performance of NHS organisations by mathematically modelling their overall performance and allocating a relative score to each trust. Trusts in England were place into one of four categories with the highest levels of performance being awarded a three star rating and the lowest a zero star rating
In October 2001 the Department of Health released the first NHS Performance Ratings confined to non-specialist acute NHS hospital Trusts (general hospitals). A poor performance rating did not necessarily mean that a trust was failing to provide a good standard of care to its patients but simply that the overall patient experience was unsatisfactory.
By summer 2002 things had evolved even further. The analysis covered all NHS Trusts in England including Acute Trusts, Specialist Trusts, Ambulance Trusts and indicative ratings for Mental Health Trusts. Primary Care Organisations (PCOs) were the subject of a parallel publication, describing their performance against a range of other indicators. As they are relatively new NHS bodies (nearly 60% came into existence as recently as April 2002) PCOs will receive their first overall Star ratings in 2003, based on their performance during 2002 & 2003.
The 2002 ratings were tougher, for example the key target on waiting times for cancer treatment was extended to cover all types of cancer not just breast cancer. They also incorporated a broader set of indicators and took into account CHI assessments of Trusts’ clinical governance arrangements. In addition the methodology was slightly different. Previously to be a 3-star Trust the institution had to reach all key targets and be in the top 50% of all Trusts for the 3 focus areas. This year a Trust had to fulfil the key targets and not be in the bottom 20% of all Trusts for any key focus area and be in the top 50% of all Trusts for 2 out of 3 of the focus areas.
All acute Trusts were assessed on their performance during 2001 & 2002 against a number of key targets and a larger number and range of indicators shown in the table below.
Key targets Eighteen-month inpatient waits The total number of breaches over the year
Fifteen-month inpatient waits Number of patients waiting more than 15 months for an inpatient admission
Twenty six-week outpatient waits Number of patients waiting more than 6 months (26 weeks) for an outpatient appointment
Twelve-hour trolley waits Number of patients waiting more than 12 hours for admission via A&E
Cancelled operations Number of operations cancelled for non-clinical reasons on the day of, or after, admission divided by Total number of elective admissions
Two-week cancer waits Proportion of patients seen for first outpatient appointment within 2 weeks when urgently referred by their GP with suspected cancer, and the referral being received by the NHS Trust within 24 hours
Improving working lives Trusts asked if they have completed/made progress towards completing their self assessment through peer review of the National Audit Instrument and have an agreed regional window for accreditation to IWL practice status given 1, else 0.
Hospital cleanliness Each organisation is assigned the lowest score from their component hospitals PEAT inspection score.
Financial management The indicator looks at the achievement of financial balance in 2001 & 2002 without the need of unplanned financial support (provided by the DoH or others) to cover financial difficulties or a potential deficit. Other intelligence, e.g. audit reports, may also impact on the assessment.

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
269
NA
CSD
– Institu
tion
and
ind
ividu
al perfo
rman
ce
Clinical focus Clinical negligence The standards cover a range of aspects some organisational, some focusing on clinical
practice. The standards are drawn from a range of services including the findings and recommendations of the Confidential Enquiries. Each standard comprises a number of separate criteria, addressing different aspects of the subject. These are organised into one of three levels. Level one criteria represent the basic elements of a clinical risk management framework; levels two and three are more demanding and concern the implementation and integration into practice of policies and procedures, monitoring, and acting on the results.
Death within 30 days of surgery (non-elective admissions)
The indirectly age and sex-standardised rate of deaths occurring in hospital and after discharge between 0 and 29 days (inclusive) of non-elective operative procedure per 100,000 continuous inpatient (CIP) spells.
Death within 30 days of a heart bypass operation
The indirectly age and sex-standardised rate of deaths occurring in hospital and after discharge between 0 and 29 days (inclusive) of a coronary artery bypass procedure per 100,000 continuous inpatient (CIP) spells. Details at: http://www.doh.gov.uk/performanceratings/2002/s_127.doc
Emergency readmission to hospital following discharge for adults and / or children
The indirectly age and sex-standardised percent of emergency admission to any hospital in England occurring within 28 days (7 days for children) of the last, previous discharge from hospital, for all ages (0-15, children).
Emergency readmission to hospital following treatment for a fractured hip
Emergency readmissions to hospital within 28 days of discharge following treatment for a fractured hip, as a percentage of live hip fracture discharges (age and sex standardised)
Emergency readmission to hospital following treatment for a stroke
Emergency readmissions to hospital within 28 days of discharge following a stroke, as a percentage of live stroke discharges (age and sex standardised)
Returning home following hospital treatment for fractured hip
Percentage of patients discharged back to usual place of residence within 28 days of emergency admission to hospital with a hip fracture, aged 65 and over (age and sex standardised)
Returning home following hospital treatment for stroke
Percentage of patients discharged back to usual place of residence within 56 days of emergency admission to hospital with a stroke, aged 50 and over (age and sex standardised)
Patient focus Six month inpatient waits Number of inpatients who had been waiting less than 6 months for inpatient treatment at
quarter end divided by Number of patients on inpatient’s waiting list, expressed as a percentage.
Total inpatient waits The difference between the actual number of patients waiting for an inpatient appointment at end of Q4 2001 / 2 and the expected number of patients waiting for an inpatient appointment at the end of Q4 2001 / 2 divided by Expected number of patients waiting for an inpatient appointment at the end of Q4 2001 / 2.
Thirteen week outpatient waits Number of outpatients seen within 13 weeks of GP written referral divided by Total number of outpatients seen following GP written referral, expressed as a percentage.
Total time in A&E Number of patients waiting less than 4 hours in A&E divided by the Total number of attendances in A&E
Cancelled operations not admitted within a month
Number of patients not readmitted within one month of operation cancelled for non-clinical reasons on the day of, or after, admission as a percentage of the total number of elective admissions
Heart operation waits Number of patients waiting more than 12 months for a CABG plus Number of patients waiting more than 12 months for a PTCA
Breast cancer treatment Number of patients treated within one month of diagnosis of breast cancer divided by Number of patients treated with a diagnosis of breast cancer
Delayed discharges Total number of patients (all ages) occupying an acute hospital bed with delayed discharge divided by Total number of patients (all ages) occupying an acute hospital bed. Average of snapshots taken where data present
Inpatient survey - Coordination of care
The combined score (out of 100) for question within the dimension covering questions around organisation of emergency care, admissions process, conflicting information, member of clinical staff in coordinating role
Inpatient Survey - Environment and facilities
The combined score (out of 100) for question within the dimension covering questions around cleanliness, quality and amount of food
Inpatient Survey - Information and education
The combined score (out of 100) for questions around medical staff's responses to questions, explanations of medication, possible problems during convalescence
Inpatient Survey - Physical and emotional needs
The combined score (out of 100) for questions around noise, adequate control of pain, assistance during mealtimes, support from clinical staff on anxieties
Inpatient Survey - Prompt Access The combined score (out of 100) for questions around waiting
Inpatient survey - Respect and dignity The combined score (out of 100) for questions around privacy for discussion, examination and treatment, mixed sex facilities and whether patient was treated with dignity and respect

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
270
NA
CSD
– In
stit
uti
on
an
d in
div
idu
al p
erfo
rman
ce
Capacity and capability focus Data quality This indicator, which is currently based on Hospital Episode Statistics (HES) data, provides a
measure of the quality and reliability of the data underlying many of the Performance Indicators and serves as a proxy for assessing the general quality of data for each organisation. The Data Quality Indicator is being further developed to measure the accuracy of clinical coding from Trusts.
Staff opinion survey Average score for a series of ten questions scored 1-5 with 5 being the positive end of the scale.
Junior doctors' hours % of junior doctors complying in full with the New Deal on Junior Doctors' hours (working a maximum 56 hour week)
Sickness absence rate The amount of time lost through absences, divided by Available staff time for all staff.
Information governance Numerator Field/Indicator Value: Summed performance across 18 audit areas (each scored out of 2) to give a total score out of 36. The 18 audit areas are: 1.Info for Patients/Clients, 2.Staff Code, 3.Induction Procedures, 4.Training Needs, 5.Training Provision, 6.Staff Contracts, 7.Contracts with Other Organisations., 8.Info Flows, 9.Data Ownership, 10.Safe Havens, 11.Protocols, 12.Security Policy Document, 13.Security Responsibilities, 14.Risk Assessment, 15.Security Incidents, 16.Security Monitoring, 17.User Responsibilities, 18.Controlling Access
It is important to be aware that the approach uses high level summary data and cannot go into every area in depth.
The 2003 star ratings were produced under the jurisdiction of the Commission for Health Improvement (CHI). The Department of Health retained the responsibility for setting priorities and key targets for the ratings, but CHI was responsible for the development of the methodology and publication of the ratings.
Clinical Governance reports from the Commission for Health Improvement
The Commission for Health Improvement (CHI) was set up by the government to examine the quality of patient care in the NHS across England and Wales. CHI started operating on 1st April 2000 and had a programme underway which aimed at reducing variations in care in the NHS. In time all NHS organisations would be assessed by CHI and the findings made public. A CHI review examined the effectiveness of the NHS organisation's clinical governance arrangements by assessing the management, provision and quality of service provided by the organisation. Reports from the Commission for Health Improvement would have an increasingly important bearing on the performance rating of local NHS organisations.
The information from CHI's reviews were used in determining poorly performing (zero star) and high-performing leading (three star) NHS organisations. CHI reviews would be taken into account for those trusts where a report had been published since the last ratings were calculated.
CHI also investigated serious service failures in the NHS when requested by the Secretary of State for Health in England and the National Assembly for Wales. Examples included the investigation of cardiothoracic transplant services at St George’s Hospital in London 67, the West of London Breast Screening Service at Hammersmith Hospitals NHS Trust 68 and an investigation into the employment of locum consultants 69.
Through these processes CHI informed the NHS on best practice and ensured that the NHS was following national guidelines. CHI and the Audit Commission commenced a review soon to be published of the level of implementation of the National Service Framework for Coronary Heart Disease. This is due to report towards the end of 2004, but now under the jurisdiction of the Healthcare Commission.

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
271
NA
CSD
– Institu
tion
and
ind
ividu
al perfo
rman
ce
The Healthcare Commission (Commission for Healthcare Audit and Inspection)
The Healthcare Commission (Commission for Healthcare Audit and Inspection) replaced CHI on 1st April 2004 and inherited production of the performance rating system including assessment of outcomes following coronary surgery for hospitals in England.
The main difference between the Healthcare Commission and CHI is that the Healthcare Commission’s responsibilities have been extended to include the private sector and mental health. This makes sense given the blurring of the margins between the NHS and the private sector.
The Commission’s main statutory functions laid out in the Health and Social Care Act 2003 include:
• Conducting reviews and investigations of the provision of healthcare and the arrangements to promote and protect public health, including studies aimed at improving the economy, efficiency and effectiveness of the NHS.
• Promoting the co-ordination of reviews and assessments undertaken by other bodies.
• Publishing information about the state of healthcare across the NHS and the independent sector, including the results of national clinical audits.
• Reviewing the quality of data relating to health and healthcare.
The statutory requirements of the Healthcare Commission in England only include:
• Reviewing the performance of each local NHS organisation and awarding an annual rating for that performance.
• Regulating the independent healthcare sector through annual registration and inspection.
• Reviewing complaints about NHS bodies that they have not been able to resolve locally through their own complaints processes.
• Publishing surveys of the views of patients and staff.
Government ministers retain responsibility for setting overall priorities for the NHS, which in turn determine key targets and certain performance indicators included in the performance ratings. On 22nd July 2004, acute, specialist, ambulance, mental health and primary care trusts (PCTs) in England received performance ratings (star ratings), assessing performance during the year ending 31st March 2004.
The key targets were:
• 12-hour waits for emergency admission via A&E post decision to admit.
• All cancers: 2-week wait.
• Financial management.
• Hospital cleanliness.
• Improving working lives.
• Outpatient and elective (inpatient and daycase) booking.
• Outpatients waiting longer than the standard.
• Patients waiting longer than the standard for elective admission.
• Total time in A&E: 4 hours or less.

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
272
NA
CSD
– In
stit
uti
on
an
d in
div
idu
al p
erfo
rman
ce
The balanced scorecard indicators for 2004
These indicators were chosen to provide a balance across a broad range of areas. The balanced scorecard indicators, including details of the rationale, the data source, the data period and technical specifications are available on the Healthcare Commission website.
The balanced scorecard indicators are:
• A&E emergency admission waits (4 hours).
• Adult inpatient and young patient surveys: access and waiting.
• Adult inpatient and young patient surveys: better information, more choice.
• Adult inpatient and young patient surveys: building closer relationships.
• Adult inpatient and young patient surveys: clean, comfortable, friendly place to be.
• Adult inpatient and young patient surveys: safe, high-quality, coordinated care.
• Better Hospital Food.
• Breast cancer: 1 month diagnosis to treatment.
• Breast cancer: 2 month GP urgent referral to treatment.
• Cancelled operations.
• Child protection.
• Clinical governance composite indicator.
• Clinical negligence.
• Composite of participation in audits (see following pages).
• Consultant appraisal.
• Day case patient booking.
• Deaths following a heart bypass operation (see following pages).
• Deaths following selected non-elective surgical procedures.
• Delayed transfers of care.
• Emergency readmission following discharge (adults).
• Emergency readmission following discharge for a fractured hip.
• HES & Workforce datasets: data quality on ethnic group.
• Indicator on stroke care.
• Infection control.
• Information governance.
• Junior doctors' hours.
• Patient complaints.
• Patients waiting longer than standard for revascularisation.
• Six month inpatient waits.
• Staff opinion survey: health, safety and incidents.
• Staff opinion survey: human resource management.
• Staff opinion survey: staff attitudes.
• Thirteen week outpatients.
• Thrombolysis – 30-minute door-to-needle time from MINAP.
• Winning Ways - processes and procedures.
It is clear that very few of the indicators above are useful measures of clinical quality. They are generally measures of organisational process. The exceptions are: deaths following CABG, thrombolysis time and, to a lesser extent, infection control.

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
273
NA
CSD
– Institu
tion
and
ind
ividu
al perfo
rman
ce
Healthcare Commission performance ratings 2004; CABG data based on the calendar year 2003
Acute Trusts performing cardiac surgery in England
20
04
ra
tin
g
CA
BG
Clin
ical
au
dit
Barts and The London NHS Trust ** 3 5
Blackpool, Fylde and Wyre Hospitals NHS Trust *** 3 5
Brighton and Sussex University Hospitals NHS Trust nil 3 5
Central Manchester and Manchester Children's University Hospitals NHS Trust *** 3 5
Guy's and St Thomas' NHS Trust *** 3 5
Hammersmith Hospitals NHS Trust *** 2 5
Hull and East Yorkshire Hospitals NHS Trust * 3 5
King's College Hospital NHS Trust *** 3 5
Leeds Teaching Hospitals NHS Trust * 3 5
Nottingham City Hospital NHS Trust *** 3 5
Oxford Radcliffe Hospital NHS Trust ** 2 5
Papworth Hospital NHS Trust ** 3 5
Plymouth Hospitals NHS Trust * 3 5
Royal Brompton and Harefield NHS Trust *** 3 5
Sheffield Teaching Hospitals NHS Trust *** 3 5
South Manchester University Hospitals NHS Trust *** 3 5
South Tees Hospitals NHS Trust * 3 5
Southampton University Hospitals NHS Trust *** 3 5
St George's Healthcare NHS Trust ** 3 5
St Mary's NHS Trust ** 3 5
The Cardiothoracic Centre - Liverpool NHS Trust *** b 5
The Newcastle upon Tyne Hospitals NHS Trust ** 3 5
United Bristol Healthcare NHS Trust ** 3 5
University College London Hospitals NHS Trust *** 3 3
University Hospital Birmingham NHS Trust *** 3 5
University Hospital of North Staffordshire NHS Trust ** 3 5
University Hospitals Coventry and Warwickshire NHS Trust ** 3 5
University Hospitals of Leicester NHS Trust Nil 3 5
The performance rating system is not designed to reflect clinical quality. It is designed to measure the organisational processes underpinning largely non-clinical service for patients. One exception is deaths following CABG.
Performance ratings are often misinterpreted by public and media as a measure of the quality of clinical care provided by an organisation, which can lead to all kinds of unfair adverse publicity 70.

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
274
NA
CSD
– In
stit
uti
on
an
d in
div
idu
al p
erfo
rman
ce
Legend
Star
rat
ing
s
http://ratings2004.healthcarecommission.org.uk/ Trusts with the highest levels of performance are awarded a performance rating of three stars;
Trusts that are performing well overall, but have not quite reached the same consistently high standards, are awarded a performance rating of two stars; Trusts where there is some cause for concern regarding particular areas of performance are awarded a performance rating of one star; Trusts that have shown the poorest levels of performance against the indicators or little progress in implementing clinical governance are awarded a performance rating of zero stars. Where a Trust has a low rating based on poor performance on a number of key targets and indicators, this does not necessarily mean that a hospital is unsafe, does not contain some very good clinical services or that the staff are not working hard in often difficult circumstances. It does mean that performance must be improved in a number of key areas. A zero-star trust is one which either fails against the key targets or is considered to have poor clinical governance
Dea
ths
afte
r C
AB
G
This indicator is based on continuous inpatient spells, covering all consecutive episodes of hospital care for individual patients during one continuous period, even if they involve transfers to other hospitals. Spells and deaths are attributed to the trust where the first relevant operation took place. It is standardised to take into account differences between types of patients (age, sex, method of admission – elective, non-elective) treated in a particular trust and those across England as a whole. The indicator uses the first bypass operation when there is more than one operation mentioned, except where the bypass occurs after a coronary artery widening procedure (angioplasty) or alongside a heart valve operation. Pooled data are presented for calendar years 2001, 2002 and 2003. The pooled three-year data are used for standardisation. The rate is presented as an indirectly age, sex and method of admission standardised rate per 100,000. Numerator (number of deaths) Number of continuous inpatient spells identified in the denominator where the patient dies in hospital or after discharge, between 0-29 days (inclusive) after the first eligible procedure in a spell. Data on deaths after discharge are obtained from the Office for National Statistics (ONS) and linked to the HES data. Denominator (relevant patient spells) Number of continuous inpatient spells where there was at least one Coronary Artery Bypass Graft (CABG) procedure (OPCS 4 codes K40-K46) in any operation field in the spell, except where the CABG occurs after a Percutaneous Transluminal Coronary Angioplasty (PTCA) procedure (OPCS 4 codes K49-K50 other than K50.2 and K50.3) or alongside a heart valve procedure (OPCS 4 codes K25-K38). A spell may include more than one operative procedure. Day cases are excluded. The fields used to construct this indicator include sex, episode start date, episode order, episode end date, method of admission, date of admission, discharge date, method of discharge, discharge destination, age at start of episode, operative procedure, source of admission, and main specialty. Effect of case-mix and severity A number of factors outside the control of hospitals, such as the socio-economic mix of local populations and events prior to hospitalisation, may contribute to the variation shown by the indicators. Differences in case-mix, beyond that accounted for by the standardisation, concurrent illnesses, the differing complexity of operations and other potential risk factors also contribute to the variation. Current data do not allow assessment of severity of illness and seriousness of operations across continuous inpatient spells, hence adjustment of the indicators for variations in these is not possible.
Co
mp
osi
te o
f par
tici
pat
ion
in a
ud
its Contribution to:·
• Myocardial Infarction National Audit Programme (MINAP) (Financial Year 2003/04)·
• National Confidential Enquiry into Patient Outcome and Death (April 2003 - December 2003) Part 1 The number of months a Trust has submitted data to NCEPOD for the months April 2003 to December 2003. The value will be a score between 0 and 9. Part 2: Whether a trust has participated in the MINAP audit. Participation is defined as the Royal College of Physicians (RCP) assessing that there has been a meaningful level of the relevant AMI activity in the Trust submitted to MINAP for the financial period 2003/04. The Trust will score 9 points for a 'Yes' and 0 points for 'No'. Overall Indicator: Parts 1 and 2 are added together to give a score of 0 to 18.] Score banding <15 = 1 (Poor), Greater than or equal to 15 but less than 18 = 3, Greater than or equal to 18 = 5 (Good)

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
275
NA
CSD
– Institu
tion
and
ind
ividu
al perfo
rman
ce
Joined-up inspection
The Healthcare Commission is the lead healthcare regulator and will work closely with other regulators and inspecting bodies to reduce the burden of visits, data requests and regulation on healthcare organisations. A concordat has been signed by: the Healthcare Commission, Audit Commission, Commission for Social Care Inspection, Mental Health Act Commission, Health and Safety Executive, National Audit Office, NHS Estates, NHS Litigation Authority, Academy of Medical Royal Colleges and Postgraduate Medical Education and Training Board (PMETB).
The concordat aims to achieve greater consistency and cohesion in the inspection of health and healthcare. However, while closer alignment of methodologies may often be beneficial, the intention is not to impose a single inspection methodology or to diminish existing methodologies that best meet the needs of services for which they have been developed. Equally the concordat does not affect the statutory remit of individual inspecting bodies.
The full text of the concordat is available on the Healthcare Commission website. Certain specific objectives will pertain to the work outlined in this report, particularly the sharing of data and the transparency of the data validation and Quality Accreditation visits:
• As inspecting bodies develop their annual plans and reports, they share them with other inspecting bodies to assist the development of coordinated programmes of work, including, where necessary, inspection methodologies.
• Inspecting bodies consider the suitability of existing data sets and maximise their legitimate use of information from other inspecting bodies.
• Inspecting bodies coordinate their core data, information and developmental requirements.
• Subject to agreed protocols (e.g., regarding the use of confidential personal information), inspecting bodies share relevant information with each other to ensure there is no duplication of data collection and that maximum value is obtained from the information collected.
• Inspecting bodies coordinate their inspections, reviews and monitoring activity and, where appropriate, develop shared methodologies and inspect jointly. They develop mechanisms to support these procedures.
• Subject to their statutory remit, inspecting bodies develop reliance on the results of reviews carried out by other competent organisations. They aim to avoid replicating inspections in areas that have been inspected recently by others. To support this process, inspecting bodies will demonstrate the robustness of their processes and findings.
• Inspecting bodies publish clear methodologies, including evidence, value-based assessments and statistical tools that are used to reach conclusions. Subject to any statutory changes, revisions to standards and/or criteria are published in advance and timescales given for consultation and implementation.
• Arrangements made for determining the number of inspectors, their location, skills, background, cultural mix and cultural understanding are documented and monitored. Selection criteria are clearly stated, applied fairly, reviewed regularly and available publicly.
• Inspecting bodies ensure that inspectors are suitably trained and subject to certification where relevant. The continuing competence of inspectors is reviewed regularly and inspectors are properly supported to retain and develop the necessary skill and knowledge.
On the same day the 2004 star ratings were released (22nd July 2004) the Secretary of State announced some significant changes to the disposition of Arm’s Length Review Bodies. The Healthcare Commission would take on the main role of the Mental Health Act Commission, which would be abolished.
The National Clinical Assessment Authority would be brought into the National Patient Safety Agency, which will also support high quality independent ethical review of all research that could affect patients. The NPSA will also take over responsibility for the national confidential enquiries from NICE. This will not affect our study of coronary surgery deaths (see page 33).

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
276
NA
CSD
– In
stit
uti
on
an
d in
div
idu
al p
erfo
rman
ce
Dr Foster
In January 2001 the independent company Dr Foster, in conjunction with the Sunday Times, produced the first Dr Foster’s Good Hospital Guide. This guide presented key information on waiting lists and facilities for every trust in the ÚK. Most controversially it produced a league table of all hospitals with more than 300 beds by mortality index, and commented on the link between hospital mortality levels and ratio of doctors to beds. This mortality index differed from the DoH Clinical Indicator number 1 in four main respects. Firstly, the Dr Foster figures included emergency as well as elective cases. Secondly in that it accounted to a greater extent for case mix. Mortality rates were not just standardised for age and sex, as per the DoH clinical indicators. They also took into account the top 80 diagnoses, which led to about 80% of hospital deaths. Thirdly, Dr Foster only considered in-hospital deaths, rather than deaths within 30 days. Fourthly, Dr Foster’s study ignored transferred cases altogether because of the issues apparent in their inclusion in the DoH Clinical Indicators.
Although the DoH Clinical Indicators 71 and the Dr Foster Good Hospital Guide 60 are both available on the web the Dr Foster guide is designed for more public viewing and includes details of hospital facilities and consultant staff.
In November 2001 Dr Foster and the DoH published league tables of hospital mortality for coronary surgery by unit. There was concern within the clinical community that these tables would be misleading and therefore result in high risk patients being denied surgery. The Society of Cardiothoracic Surgeons agreed a response at an extraordinary general meeting held on 9th November and this was published alongside the league tables in the Times on 19th November 2001 (see appendix)
The National Casemix Office
The National Casemix Office produces a benchmarking tool: the Performance Analysis Toolkit which allows any English Trust to compare itself with any other English Trust using a variety of indicators such as readmission rates or length of stay. It does not include mortality. It is based on admission spells. So what is an admission spell? When patients are admitted under a given consultant the time they spend under that consultant is described as a Finished Consultant Episode. Some patients spend time under more than one consultant during an admission to hospital. For example a patient may be admitted through A & E with diabetes under a general physician (physician A) who then refers the patient to a diabetologist the next day (physician B). The diabetologist may refer the patient to a cardiologist for an angiogram of the heart (physician C). The whole admission consists of three FCEs, which constitute a single admission spell.
The wider variety of indicators to review makes it easier to build a full picture about a potential comparator. Healthcare Resource Groups (HRGs) and their trim points are now recalculated based on the predominant diagnosis or treatment over the whole spell making the data more clinically relevant. Trusts perceive the data as being out of date; the 2000 / 2001 data has only recently been released.
CHKS
CHKS is a private company that provides benchmarking comparisons against 8 peer hospitals. This source has two advantages over Golden Bullets and the Casemix Office: the data are more up to date and include information on deaths. However, data from peer hospitals is aggregated so data from individual Trusts cannot be seen. Furthermore, data is provided by specialty, but Trusts split work between specialties in a variety of different ways that make some comparisons less helpful.

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
277
NA
CSD
– Institu
tion
and
ind
ividu
al perfo
rman
ce
Different data-sources tell different stories
The DoH, CHI, Healthcare Commission, CHKS, National Casemix Office and Dr Foster analyses are produced using Hospital Episode Statistics (HES) which are dependent on corporate information systems, which were never designed to capture detailed clinical data and are therefore dependent to some extent on subjective interpretation by clinical coders. As a result the system does not have the embedded functionality to enable risk stratification to a level now demanded by the cardiac surgical community. This is one of the reasons why each cardiac surgery unit has invested in a dedicated clinical information system and also why the national database initiative described in this report is so important.
There is also concern in the clinical community, reinforced by independent analyses from the Audit Commission, that the Hospital Episode Statistics are not accurate in term of counting procedures. The graph below indicates the variance between the number of first-time coronary bypass operations in different hospitals in England recorded by the hospitals’ administrative systems and used for the CHI star ratings and the number of operations recorded by the surgeons in those hospitals and submitted to the Cardiac Surgical Register.
This graph illustrates reasonable statistical correlation between the count of operations recorded in the UKCSR and HES data, with the difference being less than 10% for most hospitals.
Strikingly there are three hospitals (Brighton, Blackpool and Middlesbrough) where the HES count is less than a third of that recorded by surgeons in the UKCSR. It is unlikely that any hospital performed less than 1,000 coronary operations in three years. Analysis of the underlying methodology when such differences become apparent will help to improve all data sources.
First-time isolated CABG: UKCSR versus CHI-HES analysis; 2000-2002 (UKCSR n=52,476; CHI-HES n=51,294)
Centre Identical match
10% more than UKCSR 10% less than UKCSR
20% more than UKCSR 20% less than UKCSR
40% more than UKCSR 40% less than UKCSR
500
1,000
1,500
2,000
2,500
3,000
3,500
4,000
500 1,000 1,500 2,000 2,500 3,000 3,500 4,000
Numbers in the UKCSR
Nu
mb
ers
in t
he
CH
I-H
ES a
nal
ysis

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
278
NA
CSD
– In
stit
uti
on
an
d in
div
idu
al p
erfo
rman
ce
Dr Foster and CHI used slightly different methodologies for analysing the HES data. A comparison between the Dr Foster count and that recorded by surgeons in the UKCSR shows a relative undercount by Dr Foster analysts. This is because Dr Foster have adopted a philosophy of excluding any cases where there is any suggestion in the HES coding that they may be more complicated than straightforward first-time coronary operations.
Once again the statistical correlation is good but the counts are different.
The complexities of analysing these data are outlined by Dr Paul Aylin, Senior Lecturer at Imperial College, on page 280 below.
First-time isolated CABG: UKCSR versus Dr Foster-HES analysis; 2000-2002 (UKCSR n=60,150; Dr Foster-HES n=40,961)
Centre Identical match
10% more than UKCSR 10% less than UKCSR
20% more than UKCSR 20% less than UKCSR
40% more than UKCSR 40% less than UKCSR
Throughout these comparative charts data referred as UKCSR used financial years to demark the data, as did that referred to as Dr Foster-HES data; the CHI-HES analysis used calendar years to sub-divide the data, which may explain a small component of the observed differences.
0
500
1,000
1,500
2,000
2,500
3,000
3,500
0 500 1,000 1,500 2,000 2,500 3,000 3,500
Numbers in the UKCSR
Nu
mb
ers
in t
he
Dr
Fost
er-H
ES a
nal
ysis

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
279
NA
CSD
– Institu
tion
and
ind
ividu
al perfo
rman
ce
This graph clearly illustrates the difficulty of accurately counting the number of coronary operations performed in England using the Hospital Episode Statistics. Both Dr Foster and CHI work from the same dataset using slightly different methodologies, which give slightly different answers.
For some analyses these differences are not important. For others they may be crucial. It is incumbent on clinicians to work with and help analysts working on this highly complex dataset. Such help should start at the base hospital where clinicians should take greater responsibility for the accuracy of data recorded for their own specialties. Clinicians can no longer abrogate responsibility for the quality of mainstream NHS corporate data.
Similarly it is incumbent on organisations engaging in this sort of analysis to engage specialist clinical expertise to help develop the inclusion and exclusion criteria, the analytical methodologies and caveats for interpretation.
It is only with this sort of collaborative approach that we will improve the data quality to a level that will engender widespread confidence in the analyses. This is even more relevant in specialties where there are subtle coding differences between quite different clinical diagnoses and procedures.
Several cardiac surgical units now use their clinical databases to facilitate local coding and data entry into hospital administrative data systems. This is a good symbiotic relationship of benefit to all parties. It ensures better administrative data whilst allowing the clinicians to analyse their own data locally in ways that are more interesting to them.
First-time isolated CABG: CHI-HES versus Dr Foster-HES analyses; 2000-2002 (CHI-HES n=51,294; Dr Foster-HES n=35,366)
Centre Identical match
10% more than CHI-HES analysis 10% less than CHI-HES analysis
20% more than CHI-HES analysis 20% less than CHI-HES analysis
40% more than CHI-HES analysis 40% less than CHI-HES analysis
500
1,000
1,500
2,000
2,500
3,000
3,500
4,000
500 1,000 1,500 2,000 2,500 3,000 3,500 4,000
Numbers in the CHI-HES analysis
Nu
mb
ers
in t
he
Dr
Fost
er-H
ES a
nal
ysis

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
280
NA
CSD
– In
stit
uti
on
an
d in
div
idu
al p
erfo
rman
ce
Hospital Episode Statistics Paul Ayling, Clinical Senior Lecturer in Epidemiology and Public Health, Assistant Director Dr Foster Unit at Imperial College
Hospital Episode Statistics (HES) is a complex dataset and requires considerable processing before it can be analysed. HES data have been used to identify outliers for the Bristol Inquiry 72, 73 and are being increasingly used for other purposes including the monitoring of deaths in hospital 74. Originally designed for administrative purposes, a key feature of HES is that it is based on finished consultant episodes. These are defined as a continuous episode of care under a single consultant team. There may be several episodes within an admission, which need to be linked in order to determine the outcome on discharge. Further linkage can be carried out between admissions in the same patient to track transfers and readmissions to other NHS hospitals.
Comparisons of HES analyses with other sources will result in differences for a number of reasons. An obvious feature of HES is that they are published by financial year (in these comparisons, for the years 1999-2000 to 2001-2002). Any comparison with data published by calendar year will inevitably result in differences.
Within each episode of care, there is now the provision to record up to 14 diagnoses and up to 12 procedures. Differences in whether an operation is coded in the first or a subsequent episode within an admission, and where it appears within an episode may again result in differences between HES analyses and other datasets.
Selection criteria may also differ between analyses. For the Dr Foster figures, care is taken to exclude operations where mention is made of other complicating procedures such as valve replacements, which are associated with a higher risk of death and inclusion of which may result in unfair comparisons between centres.
HES data only record events occurring within NHS hospitals. Deaths occurring at home are not recorded. This will be remedied in the near future, when the results of a Department of Health exercise to link HES with ONS death registration data will be made available to researchers. The Dr Foster Unit at Imperial does make an effort to track patients transferred to other NHS institutions such as community hospitals.
Data quality is an issue in any dataset. Errors in coding, missing outcomes and duplicate records do exist within HES. Careful data cleaning prior to analysis can to some extent get around duplicate records and inconsistent coding but some records will be excluded from mortality analyses because of missing fields. Problems with miscoding are more difficult to deal with, although the choice of suitably broad categories of procedure codes can help to minimise the effect of miscoding between narrow categories of operation 75. Missing operations and coding of diagnoses to vague symptoms cannot be dealt with within an analysis and may result in undercounting. These are best tackled at source and feeding back results to Trusts is one way to highlight shortfalls in recording.
In summary, there are a number of reasons for differences between analyses of HES and other data sources. The extent to which these impact on an analysis will depend on the purposes for which it is carried out. Closer collaboration between clinicians, coders and researchers will help to minimise or explain differences. Anecdotal evidence suggests that increased interest in HES by clinicians is leading to better quality data. Greater clinical input into appropriate selection and exclusion criteria will lead to more comparable analyses and comparison of data sets at an individual level might help to identify potential improvements in both systems.

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
281
NA
CSD
– Institu
tion
and
ind
ividu
al perfo
rman
ce
Background to the publication of individual surgeon’s performance against standards
As events in Bristol unravelled cardiac surgeons tried to redress perceived deficiencies in their approach to national data collection and audit 76. The first step was to produce an unambiguous set of guidelines on the practical aspects of how to collect appropriate data and implement effective audit in cardiac surgical units (see appendix).
The second step was to try and work out how to measure surgical performance.
Our thesis was that every patient had the right to expect his surgery to be performed by a surgeon whose results were not statistically worse than the average after casemix had been taken into account. Unfortunately 50% of surgical units in the country did not even have the capacity to collect the data required for the rudimentary risk stratification in use at that time, which meant that we had to resort to methodologies relying on crude mortality data alone.
So at the 1998 annual meeting of the Society of Cardiothoracic Surgeons it was agreed, following animated discussion, to institute the collection of surgeon specific activity and in-hospital mortality data for index procedures. Several index procedures were chosen:
• mortality following correction of aortic coarctation or isolated VSD repair for paediatric surgeons.
• mortality following lobectomy for lung cancer for thoracic surgeons 77.
• mortality following isolated, first time coronary surgery for general cardiothoracic surgeons.
The idea was that the Society would approach any surgeon whose crude or raw mortality was greater than 2 standard deviations above the mean, seek clarification and offer help where appropriate. In-hospital mortality was chosen because it was relatively easy to collect, could be validated and included all patients who died in hospital, not just those within a certain timeframe. Furthermore, it was used by reporting systems in New York, Pennsylvania and New Jersey. It is also meaningful to the public. Despite reservations over the use of raw data and fear over how the process might evolve, we embarked on a journey, which we felt was a professional and measured response to growing public concerns. Progress on such projects is usually incremental and in any future reviews the retrospectoscope should take in the panorama of the day.
In 1998 cardiac surgeons were anxious. They were fearful that in the shadow of Bristol, Chief Executives would have a low threshold for suspension, which could unjustly derail the career and income of a perfectly competent surgeon. These fears were not without foundation. At that time nearly 5% of all consultant cardiac surgeons were either suspended or under investigation usually based on spurious claims of surgical ineptitude (only one has subsequently been upheld). Nevertheless, such was the recognition of the importance of this venture that compliance among consultant surgeons for data submission has been 100% from that time. From our data we have learnt two things. Firstly, there is no meaningful relationship between volume and outcome for individual surgeons. Secondly, when surgeons have been reviewed multiple issues of process and organisation, rather than technical, surgical ability, have usually been the underlying problem. Because of this, we have this year agreed a mechanism to engage the medical director or chief executive of any trust where a surgeon is under review.
The Kennedy report clearly stated that
patients must be able to obtain information as to the relative performance of the trust… and consultant units within the trust.
But, in most surgical specialties, a consultant unit is an easily identifiable individual. This led to an increasing belief that the interests of the public and patients would be served by publication of both unit and individual surgical performance in the form of postoperative mortality.
Why publish individual surgeon’s results?
A detailed analysis by the Nuffield Trust has shown that the arguments for and against publication are finely balanced 78. They describe three models of public release.
The public accountability model sees public disclosure as a public responsibility irrespective of the consequences. Proponents argue that the public good will be served by openness and that the release of data, in conjunction with appropriate education and the ensuing debate will help clarify important societal issues.

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
282
NA
CSD
– In
stit
uti
on
an
d in
div
idu
al p
erfo
rman
ce
A market orientated model assumes that the provision of comparative data on quality will allow informed and willing consumers to drive quality improvement through selective purchasing or utilisation.
A professionally orientated model, which is the focus of this article, assumes an intrinsic desire on behalf of health professionals to improve their practice. This is generally motivated by a desire to maintain autonomy in the face of greater governmental regulation. Providing data on variations gives credibility to the professional bodies that are seen to attenuate their often secretive, protective and self serving image. The data act as a catalyst to identify and solve problems and publication turns up the heat to enable the catalyst to work.
The apparent benefits of the cardiac surgery reporting program in New York had been well publicised 79, 80, 81, 82. The claims were that this system of public reporting was transparent and that the associated scrutiny had resulted in an improvement in the quality of care reflected in a demonstrable reduction in post-operative mortality. Counter-claims suggested that this reduction in mortality was no greater than that seen across the rest of the US and that in a litigious climate the data required protracted, detailed auditing and validation so the data when finally published 3 years after the fact, were no longer relevant. Furthermore, there was a feeling in the US cardiac surgical community that an unintended negative consequence of public disclosure was that surgeons were protecting their results by avoiding higher risk cases if they felt they were sailing too close to the wind 83, 84, 85, 86. The improvement in mortality was easy to demonstrate. The avoidance of high risk surgery was less easy to demonstrate because of the subjective and immeasurable nature of the clinical decision making process in these complex patients. This is a real irony, because the evidence suggests that patients are the one group who pay little attention to these data. Even in the US where surgeon specific data are published patients pay little attention to the information. What they really want is an operation in a hospital close to home and as soon as possible 87, 88, 89.
Public disclosure of hospital and surgeon-specific data in other specialties has been less high profile, but will gain increasing importance 90, 91.
In 2000 a survey of cardiac surgeons conducted independently by Newsnight in the UK showed that 80% of surgeons were in favour of the principle of public disclosure but 90% of surgeons thought that high risk cases were already being avoided in anticipation of the publication of results. There was also anxiety over what any published figures might mean. The surgeon plays an important role in surgical outcome, but so does the anaesthetist, the intensive care physician and the ITU nurse. Surgical results are influenced by the socio-economic status of the local population, severity of cardiac illness, prevalence of co-morbidities, threshold of referral from both the general practitioner and the cardiologist, threshold of acceptance by the surgeons, standards of anaesthesia, surgery, and intensive care, adequacy of facilities and staffing levels, attitude to training, interpersonal relationships between staff, and architectural dispersion within the unit. So the concept of fingering the surgeon was perceived as unfair 92. This was further accentuated by the perception that US surgeons have more control over selecting the team with whom they work. In the NHS, unlike the private sector, surgeons have little or no say over the appointment of other team members. These concerns had been reflected in the Veterans Administration (the biggest healthcare provider in the US) decision to discourage the generation of surgeon specific risk adjusted outcomes because they felt it was not possible to separate the performance of a surgeon from that of his or her institution, because quality is highly dependent on institutional systems 93, 94. However, the opposing argument is that it is the doctors who are best placed to change institutional processes that influence outcome and they are therefore a logical target 95.
The way forward
By January 2002 the temperature had risen. The surgical community recognised the inevitability of some kind of public disclosure. Given this inevitability, we were keen to become world leaders in this area. We were supported by the Royal College of Anaesthetists and the Association of Cardiothoracic Anaesthetists who, although concerned, were,
in agreement that data on anaesthetists should be treated exactly the same as surgeons
and should be subject to the same rules of public disclosure 96.
The National Service Framework for coronary heart disease which included a clinical cardiac surgery dataset and clear recommendations for comparative audit had been published two years earlier and launched by the Prime Minister at the Royal College of Surgeons. This had subsequently spawned a national CHD Information Strategy 97, which mandated collection of the surgical clinical dataset 98 originally developed by the Society of Cardiothoracic Surgeons in 1996. The aim was to harmonise data collection between cardiology, cardiac surgery and other administrative systems so that everyone had ownership of, and was working from, the same base dataset and the same definitions. We agreed that the best way forward would be to develop a professionally driven, independently validated system for measuring and presenting surgical outcomes. The formula was simple: the NHS would provide the infrastructure and the surgical community

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
283
NA
CSD
– Institu
tion
and
ind
ividu
al perfo
rman
ce
would provide the data and be responsible for developing meaningful analyses and presentation. In order to retain the confidence of surgeons, the public and the healthcare regulators, the project would be overseen jointly by the surgical community, the then Commission for Health Improvement (now the Healthcare Commission) and the Department of Health. The data collection process would shift from the Society of Cardiothoracic Surgeons to the Central Cardiac Audit Database (CCAD), part of the National Clinical Audit Support Programme within the NHS Information Authority 99. The added value would be that this system would provide mortality tracking through the Office of National Statistics. This would enable us to start analysing and understanding the factors influencing long-term survival rather than focussing solely on early post-operative mortality. This is particularly relevant given the observation that the hazard of early death following coronary artery surgery remains elevated for 60-90 days 100. This should lead to an appreciation of which kinds of patients benefit most from which operation and so contribute significantly to the overall quality of care and more specifically to the basis of informed consent.
In the light of Bristol and changing public attitudes we thought carefully about ways to present the data. We agreed that in time we would base any risk adjusted comparative analyses on lower risk cases alone, which would mean that surgeons still felt able to tackle more complex and difficult cases without unnecessary apprehension. The wisdom of this strategy was recently highlighted by a publication in the BMJ, which confirmed that risk stratification systems, which may be pretty good at predicting risk in large institutional groups of patients are much less reliable in high risk cases at an individual surgeon level. More importantly this study defined the level of predicted risk above which we should exclude patients from comparative analyses. We have more recently agreed to exclude patients enrolled in recognised peer reviewed high risk clinical trials, but we will still publish the number of patients entered into these trials in order to encourage recruitment into innovative research and to give credit to those surgeons who choose to take part in such studies. This has become particularly relevant for studies of coronary revascularisation for poor left ventricular function or heart failure where the surgical risk is high but the benefits in terms of long-term symptoms and survival can be improved dramatically.
This was an ambitious programme. Our dataset which had been established in 1996 had to be changed in order to accommodate NHS data standards, units had to be connected to the CCAD through secure connections and the transmission specifications for the clinical data required standardisation and testing. Locally, data managers were appointed and networked computer systems were put in place. The first data trickled into CCAD in October 2003, which unfortunately was far too late for the production of validated risk adjusted surgeon specific results in 2004.
We began to consider other options. We knew that the quality of data in our existing database would not support robust comparative analyses 101. We knew the Hospital Episode Statistics were being used to monitor individual surgeon’s activity in a number of other specialties and that outcome data were only the press of a button away 102. In October 2002, we had published unadjusted mortality for coronary and aortic valve surgery for every unit in the UK, which had attracted very little attention 103. But we had also been collecting individual surgeon’s unadjusted mortality data for some years. Could we analyse and present this data constructively?
Could crude mortality be presented?
The way such data are presented is determined by the reason for publication. There are several reasons for publishing outcome data but the two key reasons are to either facilitate patient choice or to demonstrate safety. Publishing for patient choice requires detailed comparative, risk adjusted tables of outcome published in some sort of rank order. Publishing to indicate whether a surgeon is safe or not is less complicated and certainly less contentious. This requires agreeing a threshold of unacceptable mortality and then revealing where each individual surgeon’s results lie relative to that threshold. This is analogous to the blood alcohol level test to determine fitness to drive a car – one is either above or below the agreed or legal limit.

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
284
NA
CSD
– In
stit
uti
on
an
d in
div
idu
al p
erfo
rman
ce
Actual versus predicted mortality for 2001-2003 using a 9-factor Bayes model built on 2000 data shows that most deaths occur in higher risk patients.
SCTS Complex CABG Bayes score
Observed Predicted
Alive Dead Total Mortality rate Dead
Mortality rate
<1.0% 20,467 91 20,558 0.4% 144.7 0.7%
1.0-1.9% 23,834 271 24,105 1.1% 339.2 1.4%
2.0-2.9% 9,913 217 10,130 2.1% 245.7 2.4%
3.0-4.9% 7,656 262 7,918 3.3% 302.3 3.8%
5.0-9.9% 4,288 293 4,581 6.4% 307.8 6.7%
>9.9% 1,765 333 2,098 15.9% 373.7 17.8%
All 67,923 1,467 69,390 2.1% 1713.3 2.5%
Actual versus predicted mortality for 2001-2003 using a modified EuroSCORE to maximise the number of scorable patients.
EuroSCORE
Observed Predicted
Alive Dead Total Mortality rate Dead
Mortality rate
0-1 11,998 53 12,051 0.4% 60.3 0.5%
2-3 14,450 134 14,584 0.9% 367.4 2.5%
4-5 10,784 194 10,978 1.8% 486.6 4.4%
6-7 4,989 189 5,178 3.7% 330.2 6.4%
8-9 1,819 140 1,959 7.1% 163.6 8.4%
>9 953 195 1,148 17.0% 133.8 11.7%
All 44,993 905 45,898 2.0% 1542.0 3.4%
Therefore, in the absence of risk adjustment it is reasonable that the threshold should be considerably higher than it is when risk adjustment is employed. So how did we set the limits?
In industry 99.9% confidence limits (3 Standard Deviations; SD) limits are commonly used for manufacturing quality control processes where materials and processes are standardised. Sadly, this level of standardisation does not hold for cardiac surgical patients who can be very diverse. This is our justification for widening the limits to 99.99% to take this additional, inherent variation into consideration. We propose to use these limits as our basis for publication of individual surgeon’s results. In the absence of risk adjustment, for the purposes of safety we will consider any surgeon whose mortality is within 99.99% confidence limits (4 SD) over an aggregated three-year period as meeting transparent and defined standards.
Surgeons who have been in post for less than three years will be analysed similarly for one or two years. Those whose mortality lies within 99.99% Cls will be said to meet SCTS standards, those whose mortality lies below and outside these limits will be said to exceed SCTS standards and those above with a high mortality will be annotated as does not meet SCTS standards
Despite these agreed standard for the publication of results we will continue to use a more stringent set of limits to initiate an internal assessment, setting an annual mortality rate of greater than 2 SD above the mean as the trigger for local clinical governance review. The problem with this approach is that there will always be 2.5% of the consultant body under review. We need to destigmatise the review process and re-educate trusts to understand and accept the new order. This is intended to be a constructive process and must not be allowed to become a trigger for criticism, blame or ill-considered actions. The process of stringent annual reviews should ensure that no surgeon ever breaches the higher alarm limit (99.99% confidence limit) over a three-year period.
The use of data that is not risk adjusted is still very controversial, but its value is being increasingly recognised. The use of a single risk adjusted number to summarise a surgeon’s results runs the risk of lending a level of spurious credibility to an analysis that does not take into account the impact of influences,

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
285
NA
CSD
– Institu
tion
and
ind
ividu
al perfo
rman
ce
which are not patient related. To many the number will simply represent the final analysis 104 105. On the other hand data that are not risk adjusted simply say, Take a closer look at the bigger picture. It inevitably invokes a review process of which detailed, risk stratified analysis is only a part. No blame can be righteously appointed until a full review has taken place.
Examining institutional influences on outcomes
In order to remain credible we can no longer do this alone. We must collaborate with other agencies. We have therefore embarked on a joint project with the National Confidential Enquiry into Patient Outcomes and Deaths (NCEPOD) to review all deaths after first-time coronary surgery. This will bring both independence and expertise into the study of patient, surgical and institutional factors which influence outcome. This information will help us to determine those organisational features that improve both the patient experience and surgical outcome (see page 33).
Our proposed mode of presentation using crude data is an interim measure while we improve our ability to collect complete data suitable for risk stratification. This will take time. Through the wider Nuffield Trust (UK) and RAND (USA) collaborative programme on quality measurement and improvement in healthcare we have undertaken a rigorous, independent review of the quality of data in the clinical databases of ten units in England. This has shown serious but remediable deficiencies in data quality. The study has led to a series of recommendations on data collection including the requirement for a permanent cycle of independent external monitoring and validation by an independent source before release 106. Until then it would be irresponsible to publish any numerical mortality data against an individual surgeon.
This system is not perfect, it is a first step, which has, opened a door that other branches of medicine will need to enter 107. Most importantly we hope we have opened a more general debate around the relative influence of individual physicians and institutional influences on patient outcomes and how this relationship translates to transparent public accountability.

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
286
NA
CSD
– In
stit
uti
on
an
d in
div
idu
al p
erfo
rman
ce
Key points in interpreting the hospital tables including surgeons’ performance
Coronary artery surgery is the commonest procedure performed by cardiac surgeons and is therefore a pragmatic barometer of quality and performance. Meaningful analysis and presentation is fraught with difficulty. This is a first attempt.
There are some specific points to bear in mind when reviewing the following tables:
1. Most deaths occur in higher risk cases.
2. More senior and experienced surgeons tend to have more varied surgical practice so they often perform a smaller number of coronary operations. This is illustrated in the table below from a fairly typical six-surgeon unit. So the number of coronary operations is not necessarily a useful measure of experience or competence.
Type of operations performed by time as Consultant
CABG Valve CAB + Valve
Congenital Aortic Others
3. There is, therefore, a higher proportion of senior, experienced surgeons or surgeons with varied casemix at the lower end of the volume spectrum (see pages 307-308). These surgeons often also perform proportionally fewer straightforward elective coronary operations with a greater proportion of their coronary surgery workload coming from in-house urgent referrals when they are on call.
4. Data submission is entirely voluntary.
5. Compliance among consultant surgeons has been 100% since inception in 1998.
6. Results are presented by hospital because quality of care is affected by organisational influences.
7. Where a surgeon performs private practice within an NHS institution those patients are included in the analysis. However, most surgeons perform their private practice in private hospitals and this data has not been collected. This is a shortcoming that will be resolved in time.
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
2 3 8 12 13 15
Years as a Consultant
Per
cen
tag
e o
f op
erat
ion
s

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
287
NA
CSD
– Institu
tion
and
ind
ividu
al perfo
rman
ce
In the following section, hospitals appear in the following order:
CITY HOSPITAL Trust
Aberdeen Royal Infirmary Grampian University Hospitals
Belfast Royal Victoria Hospital Royal Hospitals
Birmingham Queen Elizabeth Hospital University Hospital Birmingham NHS Trust
Blackpool Victoria Hospital Blackpool, Fylde and Wyre Hospitals NHS Trust
Brighton Royal Sussex County Hospital Brighton and Sussex University Hospitals NHS Trust
Bristol Royal Infirmary United Bristol Healthcare NHS Trust
Cardiff University Hospital of Wales Cardiff and Vale NHS Trust
Coventry Walsgrave Hospital University Hospitals Coventry and Warwickshire NHS Trust
Edinburgh Royal Infirmary Lothian University Hospitals NHS Trust
Glasgow Royal Infirmary North Glasgow University Hospitals
Glasgow Western Infirmary North Glasgow University Hospitals
Hull Castle Hill Hospital Hull and East Yorkshire Hospitals NHS Trust
Leeds General Infirmary Leeds Teaching Hospitals NHS Trust
Leicester Glenfield Hospital University Hospitals of Leicester NHS Trust
Liverpool The Cardiothoracic Centre Cardiothoracic Centre – Liverpool NHS Trust
London Guy’s & St Thomas’ Hospitals Guy's and St Thomas' Hospital NHS Trust
London Hammersmith Hospital Hammersmith Hospitals NHS Trust
London Royal Brompton Hospital Royal Brompton and Harefield NHS Trust
London Harefield Hospital Royal Brompton and Harefield NHS Trust
London King's College Hospital Kings College Hospital NHS Trust
London The Heart Hospital University College London Hospitals NHS Trust
London Barts and the London Hospitals Barts and the London NHS Trust
London St George's Hospital St George’s Healthcare NHS Trust
London St Mary's Hospital St Mary’s NHS Trust
Manchester Royal Infirmary Central Manchester and Manchester Children’s University Hospitals NHS Trust
Manchester Wythenshawe Hospital South Manchester University Hospitals NHS Trust
Middlesbrough James Cook University Hospital South Tees Hospitals NHS Trust
Newcastle Freeman Hospital Newcastle upon Tyne Hospitals NHS Trust
Nottingham City Hospital Nottingham City Hospital NHS Trust
Oxford John Radcliffe Hospital Oxford Radcliffe Hospitals NHS Trust
Papworth Papworth Hospital Papworth Hospital NHS Foundation Trust
Plymouth Derriford Hospital Plymouth Hospitals NHS Trust
Sheffield Northern General Hospital Sheffield Teaching Hospitals NHS Trust
Southampton Southampton General Hospital Southampton University Hospitals NHS Trust
Stoke-on-Trent North Staffordshire Royal Infirmary University Hospital of North Staffordshire NHS Trust
Swansea Morriston Hospital Swansea NHS Trust

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
288
NA
CSD
– In
stit
uti
on
an
d in
div
idu
al p
erfo
rman
ce
Aberdeen: Royal Infirmary www.show.scot.nhs.uk/guh/hospitals/ari/ari.htm
Chief Executive: Mr Alex Cumming Hospital Telephone: 01224 681 818
Trust star rating 2003 / 2004 NA/ NA Networked data collection system No
SCTS Quality accreditation No Dedicated surgical data manager Part-time
Operations Mortality Survival
Isolated CABG 1,336 1.5% (99% CI: 0.8-2.7%) 98.5% 2001-2003
Isolated AVR 159 4.4% (99% CI: 1.6-11.1%) 95.6%
Isolated CABG 508 1.6% (99% CI: 0.6-3.9%) 98.4% 2003
Isolated AVR 58 5.2% (99% CI: 1.0-19.4%) 94.8%
Surgeons performing coronary surgery CABG per year
SCTS review of results
Buchan Cardiothoracic 116 Meets SCTS standards (three years)
Cockburn Cardiothoracic 61 Meets SCTS standards (three years)
El-Shafei Adult cardiac 158 Meets SCTS standards (three years)
Gibson Adult cardiac 59 Meets SCTS standards (one years)
Jeffrey Adult cardiac 116 Meets SCTS standards (three years)
Belfast: Royal Victoria Hospital www.royalhospitals.org
Chief Executive: Mr William McKee Hospital Telephone: 028 9024 0503
Trust star rating 2003 / 2004 NA/ NA Networked data collection system Yes
SCTS Quality accreditation No Dedicated surgical data manager No
Operations Mortality Survival
Isolated CABG 1,391 2.3% (99% CI: 1.4-3.6%) 97.7% 2001-2003
Isolated AVR 314 3.2% (99% CI: 1.3-7.1%) 96.8%
Isolated CABG 455 3.1% (99% CI: 1.5-6.1%) 96.9% 2003
Isolated AVR 108 2.8% (99% CI: 0.5-11.0%) 97.2%
Surgeons performing coronary surgery CABG per year
SCTS review of results
Campalani Adult cardiac 110 Meets SCTS standards (three years)
Danton Adult/Paediatric 76 Meets SCTS standards (two years)
Gladstone Adult/Paediatric 63 Meets SCTS standards (three years)
Graham Cardiothoracic 59 Meets SCTS standards (three years)
MacGowan Adult cardiac 103 Meets SCTS standards (three years)

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
289
NA
CSD
– Institu
tion
and
ind
ividu
al perfo
rman
ce
Birmingham: Queen Elizabeth Hospital www.uhb.nhs.uk
Chief Executive: Mr Mark Britnell Hospital Telephone: 0121 472 1311
Trust star rating 2003 / 2004 / Networked data collection system Yes
SCTS Quality accreditation No Dedicated surgical data manager Yes
Operations Mortality Survival
Isolated CABG 1,772 3.3% (99% CI: 2.3-4.6%) 96.7% 2001-2003
Isolated AVR 267 2.6% (99% CI: 0.9-6.8%) 97.4%
Isolated CABG 655 2.7% (99% CI: 1.5-5.0%) 97.3% 2003
Isolated AVR 133 2.3% (99% CI: 0.4-9.0%) 97.7%
Surgeons performing coronary surgery CABG per year
SCTS review of results
Bonser Adult cardiac 84 Meets SCTS standards (three years)
Graham Adult cardiac 109 Meets SCTS standards (three years)
Keogh Adult cardiac 80 Meets SCTS standards (three years)
Pagano Adult cardiac 101 Meets SCTS standards (one year)
Rooney Adult cardiac 130 Meets SCTS standards (two years)
Wilson Adult cardiac 124 Meets SCTS standards (three years)
Blackpool: Victoria Hospital www.blackpool-victoria.nhs.uk
Chief Executive: Mr Roy Male CBE Hospital Telephone: 01253 300 000
Trust star rating 2003 / 2004 / Networked data collection system Yes
SCTS Quality accreditation No Dedicated surgical data manager Yes
Operations Mortality Survival
Isolated CABG 1,944 1.8% (99% CI: 1.2-2.8%) 98.2% 2001-2003
Isolated AVR 160 6.3% (99% CI: 2.7-13.5%) 93.7%
Isolated CABG 683 1.5% (99% CI: 0.6-3.3%) 98.5% 2003
Isolated AVR 55 5.5% (99% CI: 1.0-16.8%) 94.5%
Surgeons performing coronary surgery CABG per year
SCTS review of results
Au Cardiothoracic 145 Meets SCTS standards (three years)
Duncan Cardiothoracic 152 Meets SCTS standards (three years)
Millner Cardiothoracic 180 Meets SCTS standards (three years)
Sogliani Cardiothoracic 49 Meets SCTS standards (two years)

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
290
NA
CSD
– In
stit
uti
on
an
d in
div
idu
al p
erfo
rman
ce
Brighton: Royal Sussex County Hospital www.brighton-healthcare.nhs.uk
Chief Executive: Mr Stuart Welling Hospital Telephone: 01273 696 955
Trust star rating 2003 / 2004 / Nil Networked data collection system Yes
SCTS Quality accreditation No Dedicated surgical data manager Yes
Operations Mortality Survival
Isolated CABG 1,420 3.0% (99% CI: 2.0.4.4%) 97.0% 2001-2003
Isolated AVR 191 4.7% (99% CI: 1.7-10.7%) 95.3%
Isolated CABG 610 3.0% (99% CI: 1.6-5.4%) 97.0% 2003
Isolated AVR 86 5.8% (99% CI: 1.7-16.8%) 94.2%
Surgeons performing coronary surgery CABG per year
SCTS review of results
Forsyth Adult cardiac 176 Meets SCTS standards (three years)
Hyde Adult cardiac 95 Meets SCTS standards (two years)
Pugsley Adult cardiac 118 Meets SCTS standards (three years)
Trivedi Adult cardiac 141 Meets SCTS standards (three years)
Bristol: Royal Infirmary www.ubht.nhs.uk
Chief Executive: Mr Ron Kerr Hospital Telephone: 0117 929 0666
Trust star rating 2003 / 2004 Nil / Networked data collection system Yes
SCTS Quality accreditation Yes Dedicated surgical data manager Yes
Operations Mortality Survival
Isolated CABG 2276 1.3% (99% CI: 0.8-2.1%) 98.7% 2001-2003
Isolated AVR 304 2.3% (99% CI: 0.8-6.0%) 97.7%
Isolated CABG 736 1.4% (99% CI: 0.6-3.1%) 98.6% 2003
Isolated AVR 99 0.0% (99% CI: 0.0-3.0%) 100.0%
Surgeons performing coronary surgery CABG per year
SCTS review of results
Angelini Adult cardiac 106 Meets SCTS standards (three years)
Ascione Cardiothoracic 76 Meets SCTS standards (one year)
Bryan Adult cardiac 144 Meets SCTS standards (three years)
Ciulli Adult cardiac 159 Meets SCTS standards (three years)
Hutter Adult cardiac 138 Meets SCTS standards (three years)
Pawade Adult/Paediatric 39 Meets SCTS standards (three years)
Underwood Adult cardiac 89 Meets SCTS standards (three years)

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
291
NA
CSD
– Institu
tion
and
ind
ividu
al perfo
rman
ce
Cardiff: University Hospital of Wales www.cardiffandvale.wales.nhs.uk
Chief Executive: Mr Hugh Ross Hospital Telephone: 029 2074 7747
Trust star rating 2003 / 2004 NA/ NA Networked data collection system Yes
SCTS Quality accreditation No Dedicated surgical data manager Yes
Operations Mortality Survival
Isolated CABG 1,337 2.1% (99% CI: 1.3-3.4%) 97.9% 2001-2003
Isolated AVR 202 3.0% (99% CI: 1.0-8.2%) 97.0%
Isolated CABG 487 1.6% (99% CI: 0.6-4.0%) 98.4% 2003
Isolated AVR 69 2.9% (99% CI: 0.3-14.6%) 97.1%
Surgeons performing coronary surgery CABG per year
SCTS review of results
Azzu Adult cardiac 80 Meets SCTS standards (three years)
Butchart Cardiothoracic 35 Meets SCTS standards (three years)
Kulatilake Cardiothoracic 83 Meets SCTS standards (three years)
O'Keefe Cardiothoracic 136 Meets SCTS standards (two years)
von Oppell Adult cardiac 83 Meets SCTS standards (two years)
Coventry: Walsgrave Hospital www.uhcw.nhs.uk
Chief Executive: Mr David Roberts Hospital Telephone: 024 7660 2020
Trust star rating 2003 / 2004 / Networked data collection system Yes
SCTS Quality accreditation No Dedicated surgical data manager Yes
Operations Mortality Survival
Isolated CABG 1,794 2.5% (99% CI: 1.7-3.7%) 97.5% 2001-2003
Isolated AVR 218 3.7% (99% CI: 1.4-8.9%) 96.3%
Isolated CABG 424 1.9% (99% CI: 0.7-4.6%) 98.1% 2003
Isolated AVR 67 3.0% (99% CI: 0.4-15.0%) 97.0%
Surgeons performing coronary surgery CABG per year
SCTS review of results
Briffa Cardiothoracic 116 Meets SCTS standards (three years)
Dimitri Cardiothoracic 136 Meets SCTS standards (three years)
Norton Cardiothoracic 123 Meets SCTS standards (three years)
Patel Cardiothoracic 102 Meets SCTS standards (three years)
Rosin Cardiothoracic 121 Meets SCTS standards (three years)

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
292
NA
CSD
– In
stit
uti
on
an
d in
div
idu
al p
erfo
rman
ce
Edinburgh: Royal Infirmary www.show.scot.nhs.uk/rie
Chief Executive: Mr James Barbour Hospital Telephone: 0131 536 1000
Trust star rating 2003 / 2004 NA/ NA Networked data collection system No
SCTS Quality accreditation No Dedicated surgical data manager Yes
Operations Mortality Survival
Isolated CABG 1,723 2.1% (99% CI: 1.3-3.2%) 97.9% 2001-2003
Isolated AVR 280 3.2% (99% CI: 1.3-7.4%) 96.8%
Isolated CABG 471 3.0% (99% CI: 1.4-5.9%) 97.0% 2003
Isolated AVR 77 2.6% (99% CI: 0.3-13.2%) 97.4%
Surgeons performing coronary surgery CABG per year
SCTS review of results
Brackenbury Cardiothoracic 120 Meets SCTS standards (three years)
Campanella Adult cardiac 121 Meets SCTS standards (three years)
Mankad i Adult/Paediatric 94 Meets SCTS standards (three years)
Prasad Adult cardiac 142 Meets SCTS standards (three years)
Walker Cardiothoracic 44 Meets SCTS standards (three years)
Zamvar Cardiothoracic 110 Meets SCTS standards (three years)
i Now Adult Cardiac only

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
293
NA
CSD
– Institu
tion
and
ind
ividu
al perfo
rman
ce
Glasgow: North Glasgow University Hospitals www.show.scot.nhs.uk/ngt
Chief Executive: Mr Tim Davison
Glasgow Royal Infirmary
Hospital Telephone: 0141 211 4000
Trust star rating 2003 / 2004 NA Networked data collection system Yes
SCTS Quality accreditation Pending Dedicated surgical data manager Yes
Operations Mortality Survival
Isolated CABG 1,904 2.6% (99% CI: 1.8-3.8%) 97.4% 2001-2003
Isolated AVR 211 5.2% (99% CI: 2.3-11.0%) 94.8%
Isolated CABG 660 2.1% (99% CI: 1.0-4.2%) 97.9% 2003
Isolated AVR 64 4.7% (99% CI: 0.9-17.8%) 95.3%
Glasgow Western Infirmary
Hospital Telephone: 0141 211 2000
Trust star rating 2003 / 2004 NA Networked data collection system Yes
SCTS Quality accreditation Yes Dedicated surgical data manager Yes
Operations Mortality Survival
Isolated CABG 2,155 1.9% (99% CI: 1.3-2.8%) 98.1% 2001-2003
Isolated AVR 253 2.8% (99% CI: 1.0-7.1%) 97.2%
Isolated CABG 692 1.7% (99% CI: 0.8-3.6%) 98.3% 2003
Isolated AVR 79 3.8% (99% CI: 0.7-14.7%) 96.2%
Surgeons performing coronary surgery CABG per year
SCTS review of results
Berg Adult cardiac 160 Meets SCTS standards (three years)
Butler Cardiothoracic 147 Meets SCTS standards (three years)
Colquhoun Cardiothoracic 131 Meets SCTS standards (three years)
Craig Cardiothoracic 107 Meets SCTS standards (three years)
Faichney Cardiothoracic 109 Meets SCTS standards (three years)
Kirk Cardiothoracic 88 Meets SCTS standards (three years)
MacArthur Adult/Paediatric 83 Meets SCTS standards (three years)
Murday Adult cardiac 118 Meets SCTS standards (three years)
Nkere Adult cardiac 126 Meets SCTS standards (three years)
Pathi Adult cardiac 171 Meets SCTS standards (three years)
Pollock Adult/Paediatric 34 Meets SCTS standards (three years)
Wheatley Adult cardiac 31 Meets SCTS standards (three years)

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
294
NA
CSD
– In
stit
uti
on
an
d in
div
idu
al p
erfo
rman
ce
Hull: Castle Hill Hospital www.hey.nhs.uk
Chief Executive: Mr Stephen Greep Hospital Telephone: 01482 875 875
Trust star rating 2003 / 2004 / Networked data collection system Yes
SCTS Quality accreditation No Dedicated surgical data manager Yes
Operations Mortality Survival
Isolated CABG 1,993 1.9% (99% CI: 1.2-2.9%) 98.1% 2001-2003
Isolated AVR 247 2.8% (99% CI: 1.0-7.3%) 97.2%
Isolated CABG 782 1.3% (99% CI: 0.5-2.9%) 98.7% 2003
Isolated AVR 93 1.1% (99% CI: 0.1-9.4%) 98.9%
Surgeons performing coronary surgery CABG per year
SCTS review of results
Cale Cardiothoracic 184 Meets SCTS standards (three years)
Cowen Cardiothoracic 107 Meets SCTS standards (three years)
Griffin Cardiothoracic 206 Meets SCTS standards (three years)
Guvendik Cardiothoracic 172 Meets SCTS standards (three years)
Leeds: General Infirmary www.leedsth.nhs.uk
Chief Executive: Mr Neil McKay Hospital Telephone: 0113 243 2799
Trust star rating 2003 / 2004 / Networked data collection system Yes
SCTS Quality accreditation No Dedicated surgical data manager Shared
Operations Mortality Survival
Isolated CABG 3,197 1.3% (99% CI: 0.8-1.9%) 98.7% 2001-2003
Isolated AVR 331 4.2% (99% CI: 2.1-8.3%) 95.8%
Isolated CABG 1,128 0.9% (99% CI: 0.4-2.0%) 99.1% 2003
Isolated AVR 107 3.7% (99% CI: 0.9-12.4%) 96.3%
Surgeons performing coronary surgery CABG per year
SCTS review of results
Kaul Adult cardiac 233 Meets SCTS standards (three years)
Kay Adult cardiac 137 Meets SCTS standards (three years)
McGoldrick Adult cardiac 156 Meets SCTS standards (three years)
Munsch Adult cardiac 132 Meets SCTS standards (three years)
Nair Adult cardiac 144 Meets SCTS standards (three years)
O'Regan Adult cardiac 141 Meets SCTS standards (three years)
Watterson Adult/Paediatric 79 Meets SCTS standards (three years)

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
295
NA
CSD
– Institu
tion
and
ind
ividu
al perfo
rman
ce
Leicester: Glenfield Hospital www.uhl-tr.nhs.uk
Chief Executive: Dr Peter Reading Hospital Telephone: 0116 287 1471
Trust star rating 2003 / 2004 Nil / Nil Networked data collection system Yes
SCTS Quality accreditation No Dedicated surgical data manager Yes
Operations Mortality Survival
Isolated CABG 1,966 1.1% (99% CI: 0.6-1.9%) 98.9% 2001-2003
Isolated AVR 462 1.5% (99% CI: 0.5-4.0%) 98.5%
Isolated CABG 566 0.4% (99% CI: 0.1-1.9%) 99.6% 2003
Isolated AVR 184 1.1% (99% CI: 0.1-5.8%) 98.9%
Surgeons performing coronary surgery CABG per year
SCTS review of results
Firmin Adult/Paediatric 82 Meets SCTS standards (three years)
Galinanes Adult cardiac 87 Meets SCTS standards (three years)
Hadjinikolaou Adult cardiac 130 Meets SCTS standards (two years)
Hickey Adult/Paediatric 121 Meets SCTS standards (three years)
Leverment Cardiothoracic 52 Meets SCTS standards (three years)
Sosnowski Adult cardiac 89 Meets SCTS standards (three years)
Spyt Adult cardiac 138 Meets SCTS standards (three years)
Liverpool: Cardiothoracic Centre www.ctc.nhs.uk
Chief Executive: Mr Mike Bone Hospital Telephone: 0151 228 1616
Trust star rating 2003 / 2004 / Networked data collection system Yes
SCTS Quality accreditation Yes Dedicated surgical data manager Yes
Operations Mortality Survival
Isolated CABG 3,121 1.8% (99% CI: 1.3-2.5%) 98.2% 2001-2003
Isolated AVR 413 1.9% (99% CI: 0.7-4.8%) 98.1%
Isolated CABG 1,155 1.9% (99% CI: 1.1-3.3%) 98.1% 2003
Isolated AVR 172 1.7% (99% CI: 0.3-7.1%) 98.3%
Surgeons performing coronary surgery CABG per year
SCTS review of results
Chalmers Adult cardiac 180 Meets SCTS standards (three years)
Dihmis Adult cardiac 180 Meets SCTS standards (three years)
Fabri Adult cardiac 111 Meets SCTS standards (three years)
Griffiths Adult cardiac 133 Meets SCTS standards (three years)
Mediratta Cardiothoracic 150 Meets SCTS standards (three years)
Pullan Adult cardiac 147 Meets SCTS standards (three years)
Rashid Adult cardiac 133 Meets SCTS standards (three years)

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
296
NA
CSD
– In
stit
uti
on
an
d in
div
idu
al p
erfo
rman
ce
London: Guy’s & St Thomas’ Hospitals www.guysandstthomas.nhs.uk
Chief Executive: Dr Jonathan Michael Hospital Telephone: 020 7188 7188
Trust star rating 2003 / 2004 / Networked data collection system Yes
SCTS Quality accreditation No Dedicated surgical data manager No
Operations Mortality Survival
Isolated CABG 2,598 1.8% (99% CI: 1.3-2.7%) 98.2% 2001-2003
Isolated AVR 393 3.1% (99% CI: 1.4-6.3%) 96.9%
Isolated CABG 809 1.6% (99% CI: 0.8-3.3%) 98.4% 2003
Isolated AVR 132 4.5% (99% CI: 1.5-12.3%) 95.5%
Surgeons performing coronary surgery CABG per year
SCTS review of results
Anderson Adult cardiac 87 Meets SCTS standards (three years)
Austin Adult cardiac 104 Meets SCTS standards (three years)
Blauth Adult cardiac 96 Meets SCTS standards (three years)
O'Riordan Adult cardiac 164 Meets SCTS standards (three years)
Roxburgh Adult cardiac 105 Meets SCTS standards (three years)
Shabbo Adult cardiac 142 Meets SCTS standards (three years)
Venn Adult cardiac 81 Meets SCTS standards (three years)
Young Adult cardiac 86 Meets SCTS standards (three years)
London: Hammersmith Hospitals www.hhnt.org
Chief Executive: Mr Derek Smith Hospital Telephone: 020 8383 3322
Trust star rating 2003 / 2004 / Networked data collection system Yes
SCTS Quality accreditation Yes Dedicated surgical data manager Shared
Operations Mortality Survival
Isolated CABG 1,615 2.6% (99% CI: 1.7-3.9%) 97.4% 2001-2003
Isolated AVR 199 4.0% (99% CI: 1.5-9.7%) 96.0%
Isolated CABG 494 2.2% (99% CI: 1.0-4.8%) 97.8% 2003
Isolated AVR 75 8.0% (99% CI: 2.6-20.7%) 92.0%
Surgeons performing coronary surgery CABG per year
SCTS review of results
Anderson Cardiothoracic 146 Meets SCTS standards (three years)
Punjabi Cardiothoracic 183 Meets SCTS standards (three years)
Smith Cardiothoracic 138 Meets SCTS standards (three years)
Taylor Adult Cardiac 71 Meets SCTS standards (three years)

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
297
NA
CSD
– Institu
tion
and
ind
ividu
al perfo
rman
ce
London: Royal Brompton and Harefield NHS Trust www.rbh.nthames.nhs.uk
Chief Executive: Mr Gareth Goodier
Royal Brompton Hospital
Chief Executive: Mr Gareth Goodier Hospital Telephone: 020 7352 8121
Trust star rating 2003 / 2004 / Networked data collection system Yes
SCTS Quality accreditation No Dedicated surgical data manager Yes
Operations Mortality Survival
Isolated CABG 2,037 1.2% (99% CI: 0.7-2.1%) 98.8% 2001-2003
Isolated AVR 294 2.4% (99% CI: 0.8-6.2%) 97.6%
Isolated CABG 609 0.7% (99% CI: 0.2-2.3%) 99.3% 2003
Isolated AVR 95 2.1% (99% CI: 0.3-10.9%) 97.9%
Surgeons performing coronary surgery i CABG per year
SCTS review of results
DeSouza Adult cardiac 217 Meets SCTS standards (three years)
Moat Adult cardiac 163 Meets SCTS standards (three years)
Pepper Adult cardiac 111 Meets SCTS standards (three years)
Petrou Adult cardiac 140 Meets SCTS standards (one year)
Sethia Adult/Paediatric 26 Meets SCTS standards (three years)
Shore Adult/Paediatric 77 Meets SCTS standards (three years)
London: Harefield Hospital
Hospital Telephone: 01895 823 737
Trust star rating 2003 / 2004 As above Networked data collection system Yes
SCTS Quality accreditation No Dedicated surgical data manager Yes
Operations Mortality Survival
Isolated CABG 1,721 2.1% (99% CI: 1.3-3.2%) 97.9% 2001-2003
Isolated AVR 231 6.1% (99% CI: 3.0-11.7%) 93.9%
Isolated CABG 501 2.6% (99% CI: 1.2-5.3%) 97.4% 2003
Isolated AVR 74 8.1% (99% CI: 2.6-21.0%) 91.9%
Surgeons performing coronary surgery CABG per year
SCTS review of results
Amrani Adult cardiac 207 Meets SCTS standards (three years)
Dreyfus Adult cardiac 95 Meets SCTS standards (two years)
Gaer Adult cardiac 124 Meets SCTS standards (three years)
Khaghani Adult cardiac 111 Meets SCTS standards (three years)
i Includes coronary operations performed at King Edward VII Hospital Midhurst

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
298
NA
CSD
– In
stit
uti
on
an
d in
div
idu
al p
erfo
rman
ce
London: Kings College Hospital www.kingsch.nhs.uk
Chief Executive: Mr Malcolm Lowe-Lauri Hospital Telephone: 020 7737 4000
Trust star rating 2003 / 2004 / Networked data collection system Yes
SCTS Quality accreditation No Dedicated surgical data manager Yes
Operations Mortality Survival
Isolated CABG 1,521 2.2% (99% CI: 1.4-3.4%) 97.8% 2001-2003
Isolated AVR 179 4.5% (99% CI: 1.7-10.7%) 95.5%
Isolated CABG 472 1.7% (99% CI: 0.6-4.2%) 98.3% 2003
Isolated AVR 64 7.8% (99% CI: 2.3-21.9%) 92.2%
Surgeons performing coronary surgery CABG per year
SCTS review of results
Desai Adult cardiac 113 Meets SCTS standards (three years)
El-Gamel Adult cardiac 109 Meets SCTS standards (three years)
John Adult cardiac 134 Meets SCTS standards (three years)
Marrinan Cardiothoracic 102 Meets SCTS standards (three years)
London: The Heart Hospital www.uclh.org
Chief Executive: Mr Robert Naylor Hospital Telephone: 020 7573 8888
Trust star rating 2003 / 2004 / Networked data collection system Yes
SCTS Quality accreditation No Dedicated surgical data manager Yes
Operations Mortality Survival
Isolated CABG 1,637 3.8% (99% CI: 2.7-5.2%) 96.2% 2001-2003
Isolated AVR 252 5.6% (99% CI: 2.7-10.8%) 94.4%
Isolated CABG 679 2.7% (99% CI: 1.4-4.8%) 97.3% 2003
Isolated AVR 106 2.8% (99% CI: 0.5-11.2%) 97.2%
Surgeons performing coronary surgery CABG per year
SCTS review of results
Hayward Cardiothoracic 90 Meets SCTS standards (two year)
Kolvekar Cardiothoracic 148 Meets SCTS standards (three years)
Lawrence Cardiothoracic 143 Meets SCTS standards (one year)
van Doorn Adult Congenital 44 Meets SCTS standards (three years)
Walesby Cardiothoracic 120 Meets SCTS standards (three years)
Yap Adult cardiac 87 Meets SCTS standards (one year)

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
299
NA
CSD
– Institu
tion
and
ind
ividu
al perfo
rman
ce
London: Barts and the London Hospitals www.bartsandthelondon.nhs.uk
Chief Executive: Mr Paul White Hospital Telephone: 020 7377 7000
Trust star rating 2003 / 2004 / Networked data collection system Yes
SCTS Quality accreditation No Dedicated surgical data manager Yes
Operations Mortality Survival
Isolated CABG 3,078 1.3% (99% CI: 0.9-2.0%) 98.7% 2001-2003
Isolated AVR 299 5.0% (99% CI: 2.5-9.6%) 95.0%
Isolated CABG 936 1.3% (99% CI: 0.6-2.7%) 98.7% 2003
Isolated AVR 100 6.0% (99% CI: 1.9-15.9%) 94.0%
Surgeons performing coronary surgery CABG per year
SCTS review of results
Edmonson Cardiothoracic 46 Meets SCTS standards (three years)
Lall Adult cardiac 46 Meets SCTS standards (one year)
Magee Cardiothoracic 72 Meets SCTS standards (three years)
Peters Adult cardiac 56 Meets SCTS standards (one year)
Shipolini Adult cardiac 131 Meets SCTS standards (one year)
Uppal Cardiothoracic 105 Meets SCTS standards (three years)
Weir Cardiothoracic 137 Meets SCTS standards (three years)
Wong Cardiothoracic 126 Meets SCTS standards (three years)
Wood Cardiothoracic 91 Meets SCTS standards (three years)
London: St George’s Hospital www.st-georges.org.uk
Chief Executive: Dr Peter Homa CBE Hospital Telephone: 020 8672 1255
Trust star rating 2003 / 2004 / Networked data collection system Yes
SCTS Quality accreditation No Dedicated surgical data manager Yes
Operations Mortality Survival
Isolated CABG 2,222 2.6% (99% CI: 1.8-3.6%) 97.4% 2001-2003
Isolated AVR 182 7.1% (99% CI: 3.4-14.1%) 92.9%
Isolated CABG 815 1.7% (99% CI: 0.8-3.4%) 98.3% 2003
Isolated AVR 70 5.7% (99% CI: 1.4-18.3%) 94.3%
Surgeons performing coronary surgery CABG per year
SCTS review of results
Chandrasekaran Cardiothoracic 140 Meets SCTS standards (three years)
Jahangiri Adult cardiac 197 Meets SCTS standards (one year)
Kanagasabay Cardiothoracic 98 Meets SCTS standards (two years)
Sarsam Adult cardiac 132 Meets SCTS standards (three years)
Smith Cardiothoracic 100 Meets SCTS standards (three years)

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
300
NA
CSD
– In
stit
uti
on
an
d in
div
idu
al p
erfo
rman
ce
London: St Mary’s Hospital www.st-marys.nhs.uk
Chief Executive: Mr Julian Nettel Hospital Telephone: 020 7866 6666
Trust star rating 2003 / 2004 / Networked data collection system No
SCTS Quality accreditation No Dedicated surgical data manager No
Operations Mortality Survival
Isolated CABG 1,384 2.8% (99% CI: 1.8-4.3%) 97.2% 2001-2003
Isolated AVR 129 3.9% (99% CI: 1.1-11.5%) 96.1%
Isolated CABG 446 2.2% (99% CI: 0.9-5.0%) 97.8% 2003
Isolated AVR 34 5.9% (99% CI: 0.7-27.0%) 94.1%
Surgeons performing coronary surgery CABG per year
SCTS review of results
Casula Cardiothoracic 99 Meets SCTS standards (one year)
Glenville Cardiothoracic 138 Meets SCTS standards (three years)
Stanbridge Cardiothoracic 172 Meets SCTS standards (three years)
Manchester: Royal Infirmary www.cmht.nwest.nhs.uk
Chief Executive: Mr Mike Deegan Hospital Telephone: 0161 276 1234
Trust star rating 2003 / 2004 / Networked data collection system Yes
SCTS Quality accreditation Yes Dedicated surgical data manager Yes
Operations Mortality Survival
Isolated CABG 2,371 1.9% (99% CI: 1.3-2.8%) 98.1% 2001-2003
Isolated AVR 216 1.9% (99% CI: 0.4–4.6%) 98.1%
Isolated CABG 862 2.3% (99% CI: 1.3-4.1%) 97.7% 2003
Isolated AVR 87 1.1% (99% CI: 0.0-10.0%) 98.9%
Surgeons performing coronary surgery CABG per year
SCTS review of results
Grötte Adult cardiac 155 Meets SCTS standards (three years)
Hasan Adult cardiac 198 Meets SCTS standards (three years)
Keenan Adult cardiac 169 Meets SCTS standards (three years)
Odom Cardiothoracic 147 Meets SCTS standards (three years)
Prendergast Adult cardiac 120 Meets SCTS standards (three years)

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
301
NA
CSD
– Institu
tion
and
ind
ividu
al perfo
rman
ce
Manchester: Wythenshawe Hospital www.smuht.nwest.nhs.uk
Chief Executive: Mr Peter Morris Hospital Telephone: 0161 998 7070
Trust star rating 2003 / 2004 Nil / Networked data collection system Yes
SCTS Quality accreditation No Dedicated surgical data manager Yes
Operations Mortality Survival
Isolated CABG 2,475 1.8% (99% CI: 1.2-2.6%) 98.2% 2001-2003
Isolated AVR 330 3.0% (99% CI: 1.3-6.7%) 97.0%
Isolated CABG 800 1.4% (99% CI: 0.6-3.0%) 98.6% 2003
Isolated AVR 113 0.9% (99% CI: 0.0-7.8%) 99.1%
Surgeons performing coronary surgery CABG per year
SCTS review of results
Bridgewater Adult cardiac 94 Meets SCTS standards (three years)
Campbell Adult cardiac 97 Meets SCTS standards (three years)
Carey Adult cardiac 142 Meets SCTS standards (two years)
Deiriyana Cardiothoracic 56 Meets SCTS standards (three years)
Hooper Adult cardiac 93 Meets SCTS standards (three years)
Jones Cardiothoracic 84 Meets SCTS standards (three years)
Waterworth Adult cardiac 114 Meets SCTS standards (three years)
Yonan Adult cardiac 158 Meets SCTS standards (three years)
Middlesbrough: James Cook University Hospital www.southtees.northy.nhs.uk
Chief Executive: Mr Simon Pleydell Hospital Telephone: 01642 850850
Trust star rating 2003 / 2004 / Networked data collection system Yes
SCTS Quality accreditation No Dedicated surgical data manager Yes
Operations Mortality Survival
Isolated CABG 2,440 1.6% (99% CI: 1.0-2.4%) 98.4% 2001-2003
Isolated AVR 221 2.3% (99% CI: 0.6-6.9%) 97.7%
Isolated CABG 847 1.5% (99% CI: 0.7-3.1%) 98.5% 2003
Isolated AVR 76 1.3% (99% CI: 0.1-11.3%) 98.7%
Surgeons performing coronary surgery CABG per year
SCTS review of results
Hunter Adult cardiac 173 Meets SCTS standards (three years)
Kendall Cardiothoracic 254 Meets SCTS standards (three years)
Morritt Cardiothoracic 153 Meets SCTS standards (three years)
Owens Cardiothoracic 102 Meets SCTS standards (one years)
Wallis Cardiothoracic 154 Meets SCTS standards (three years)

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
302
NA
CSD
– In
stit
uti
on
an
d in
div
idu
al p
erfo
rman
ce
Newcastle: Freeman Hospital www.newcastle-hospitals.org.uk
Chief Executive: Mr Leonard R Fenwick Hospital Telephone: 0191 233 6161
Trust star rating 2003 / 2004 / Networked data collection system Yes
SCTS Quality accreditation No Dedicated surgical data manager Yes
Operations Mortality Survival
Isolated CABG 2,400 2.6% (99% CI: 1.9-3.6%) 97.4% 2001-2003
Isolated AVR 311 2.3% (99% CI: 0.8-5.8%) 97.7%
Isolated CABG 755 2.4% (99% CI: 1.3-4.4%) 97.6% 2003
Isolated AVR 109 3.7% (99% CI: 0.9-12.2%) 96.3%
Surgeons performing coronary surgery CABG per year
SCTS review of results
Clark Cardiothoracic 82 Meets SCTS standards (three years)
Dark Adult cardiac 56 Meets SCTS standards (three years)
Forty Cardiothoracic 98 Meets SCTS standards (three years)
Hamilton Adult/Paediatric 37 Meets SCTS standards (three years)
Hasan Adult/Paediatric 37 Meets SCTS standards (three years)
Hilton Cardiothoracic 90 Meets SCTS standards (three years)
Ledingham Adult cardiac 118 Meets SCTS standards (three years)
Pillay Adult cardiac 146 Meets SCTS standards (three years)
Scheuler Adult cardiac 105 Meets SCTS standards (one year)
Tocewicz Adult cardiac 98 Meets SCTS standards (two years)
Nottingham: City Hospital www.ncht.org.uk
Chief Executive: Mr Gerry McSorley Hospital Telephone: 0115 969 1169
Trust star rating 2003 / 2004 / Networked data collection system Yes
SCTS Quality accreditation Yes Dedicated surgical data manager Yes
Operations Mortality Survival
Isolated CABG 1,005 1.9% (99% CI: 1.0-3.4%) 98.1% 2001-2003
Isolated AVR 117 2.6% (99% CI: 0.5-10.2%) 97.4%
Isolated CABG 324 2.8% (99% CI: 1.1-6.4%) 97.2% 2003
Isolated AVR 34 5.9% (99% CI: 0.7-27.0%) 94.1%
Surgeons performing coronary surgery CABG per year
SCTS review of results
Birdi Adult cardiac 41 Meets SCTS standards (two years)
Mitchell Adult cardiac 113 Meets SCTS standards (three years)
Naik Adult cardiac 102 Meets SCTS standards (three years)
Richens Adult cardiac 107 Meets SCTS standards (three years)

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
303
NA
CSD
– Institu
tion
and
ind
ividu
al perfo
rman
ce
Oxford: John Radcliffe Hospital www.oxfordradcliffe.nhs.uk
Chief Executive: Mr Trevor Campbell Davis Hospital Telephone: 01865 741 166
Trust star rating 2003 / 2004 / Networked data collection system Yes
SCTS Quality accreditation No Dedicated surgical data manager Shared
Operations Mortality Survival
Isolated CABG 1,874 2.9% (99% CI: 2.1-4.1%) 97.1% 2001-2003
Isolated AVR 291 2.7% (99% CI: 1.0-6.7%) 97.3%
Isolated CABG 624 3.7% (99% CI: 2.1-6.3%) 96.3% 2003
Isolated AVR 116 1.7% (99% CI: 0.2-9.0%) 98.3%
Surgeons performing coronary surgery CABG per year
SCTS review of results
Armistead Adult cardiac 149 Meets SCTS standards (three years)
Pillai Adult/Paediatric 107 Meets SCTS standards (three years)
Ratnatunga Cardiothoracic 164 Meets SCTS standards (three years)
Taggart Adult cardiac 162 Meets SCTS standards (three years)
Westaby Adult/Paediatric 46 Meets SCTS standards (three years)
Papworth: Papworth Hospital www.papworth-hospital.org.uk
Chief Executive: Mr Stephen Bridge Hospital Telephone: 01480 830541
Trust star rating 2003 / 2004 / Networked data collection system Yes
SCTS Quality accreditation Yes Dedicated surgical data manager Yes
Operations Mortality Survival
Isolated CABG 3,049 1.9% (99% CI: 1.4-2.7%) 98.1% 2001-2003
Isolated AVR 506 4.5% (99% CI: 2.6-7.7%) 95.5%
Isolated CABG 1,080 2.0% (99% CI: 1.2-3.5%) 98.0% 2003
Isolated AVR 187 5.3% (99% CI: 2.3-11.7%) 94.7%
Surgeons performing coronary surgery CABG per year
SCTS review of results
Dunning Adult cardiac 112 Meets SCTS standards (three years)
Jenkins Adult cardiac 118 Meets SCTS standards (two years)
Large Adult cardiac 140 Meets SCTS standards (three years)
Nashef Adult cardiac 140 Meets SCTS standards (three years)
Ritchie Cardiothoracic 187 Meets SCTS standards (three years)
Tsui Adult cardiac 162 Meets SCTS standards (three years)
Wallwork Adult cardiac 100 Meets SCTS standards (three years)
Wells Cardiothoracic 28 Meets SCTS standards (three years)

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
304
NA
CSD
– In
stit
uti
on
an
d in
div
idu
al p
erfo
rman
ce
Plymouth: Derriford Hospital www.derriford.co.uk
Chief Executive: Mr Paul Roberts Hospital Telephone: 01752 777 111
Trust star rating 2003 / 2004 / Networked data collection system Yes
SCTS Quality accreditation No Dedicated surgical data manager Yes
Operations Mortality Survival
Isolated CABG 2,193 1.6% (99% CI: 1.1-2.5%) 98.4% 2001-2003
Isolated AVR 311 1.0% (99% CI: 0.2-4.0%) 99.0%
Isolated CABG 985 1.8% (99% CI: 0.8-3.7%) 98.2% 2003
Isolated AVR 106 2.8% (99% CI: 0.5-11.2%) 97.2%
Surgeons performing coronary surgery CABG per year
SCTS review of results
Allen Cardiothoracic 184 Meets SCTS standards (three years)
Dalrymple-Hay Cardiothoracic 139 Meets SCTS standards (two years)
Kuo Cardiothoracic 94 Meets SCTS standards (three years)
Lewis Adult cardiac 46 Meets SCTS standards (three years)
Marchbank Cardiothoracic 166 Meets SCTS standards (three years)
Unsworth White Cardiothoracic 149 Meets SCTS standards (three years)
Sheffield: Northern General Hospital www.sheffield.nhs.uk
Chief Executive: Mr Andrew Cash Hospital Telephone: 0114 243 4343
Trust star rating 2003 / 2004 / Networked data collection system Yes
SCTS Quality accreditation No Dedicated surgical data manager Yes
Operations Mortality Survival
Isolated CABG 2,060 1.2% (99% CI: 0.7-2.0%) 98.8% 2001-2003
Isolated AVR 236 1.3% (99% CI: 0.2-5.2%) 98.7%
Isolated CABG 791 0.9% (99% CI: 0.3-2.3%) 99.1% 2003
Isolated AVR 98 2.0% (99% CI: 0.2-10.5%) 98.0%
Surgeons performing coronary surgery CABG per year
SCTS review of results
Braidley Adult cardiac 136 Meets SCTS standards (three years)
Cooper Adult cardiac 102 Meets SCTS standards (three years)
Hopkinson Adult cardiac 113 Meets SCTS standards (three years)
Locke Adult cardiac 119 Meets SCTS standards (three years)
Wilkinson Adult cardiac 102 Meets SCTS standards (three years)

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
305
NA
CSD
– Institu
tion
and
ind
ividu
al perfo
rman
ce
Southampton: General Hospital www.suht.nhs.uk
Chief Executive: Mr Simon Jupp (acting) Hospital Telephone: 023 8077 7222
Trust star rating 2003 / 2004 / Networked data collection system Yes
SCTS Quality accreditation No Dedicated surgical data manager Yes
Operations Mortality Survival
Isolated CABG 1,880 1.9% (99% CI: 1.2-2.9%) 98.1% 2001-2003
Isolated AVR 343 1.5% (99% CI: 0.4-4.5%) 98.5%
Isolated CABG 527 1.9% (99% CI: 0.8-4.3%) 98.1% 2003
Isolated AVR 120 0.8% (99% CI: 0.0-7.4%) 99.2%
Surgeons performing coronary surgery CABG per year
SCTS review of results
Barlow Cardiothoracic 92 Meets SCTS standards (three years)
Haw Adult/Paediatric 89 Meets SCTS standards (three years)
Langley Adult/Paediatric 53 Meets SCTS standards (one year)
Livesey Adult cardiac 92 Meets SCTS standards (three years)
Monro Adult/Paediatric 81 Meets SCTS standards (three years)
Ohri Adult cardiac 137 Meets SCTS standards (three years)
Tsang G Cardiothoracic 117 Meets SCTS standards (three years)
Stoke-on-Trent: North Staffordshire Royal Infirmary www.nsht.nhs.uk
Chief Executive: Mr Dave Crowley Hospital Telephone: 01782 715444
Trust star rating 2003 / 2004 / Networked data collection system Yes
SCTS Quality accreditation No Dedicated surgical data manager Yes
Operations Mortality Survival
Isolated CABG 2,143 2.1% (99% CI: 1.4-3.1%) 97.9% 2001-2003
Isolated AVR 171 2.9% (99% CI: 0.8-8.8%) 97.1%
Isolated CABG 894 1.9% (99% CI: 1.0-3.6%) 98.1% 2003
Isolated AVR 64 3.1% (99% CI: 0.4-15.6%) 96.9%
Surgeons performing coronary surgery CABG per year
SCTS review of results
Abid Adult cardiac 51 Meets SCTS standards (one year)
Levine Adult cardiac 209 Meets SCTS standards (three years)
Parmar Cardiothoracic 149 Meets SCTS standards (three years)
Ridley Adult cardiac 149 Meets SCTS standards (three years)
Satur Adult cardiac 128 Meets SCTS standards (one year)
Smallpeice Cardiothoracic 135 Meets SCTS standards (three years)

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
306
NA
CSD
– In
stit
uti
on
an
d in
div
idu
al p
erfo
rman
ce
Swansea: Morriston Hospital www.swansea-tr.wales.nhs.uk
Chief Executive: Ms Jane Perrin Hospital Telephone: 01792 702 222
Trust star rating 2003 / 2004 NA Networked data collection system Yes
SCTS Quality accreditation No Dedicated surgical data manager No
Operations Mortality Survival
Isolated CABG 1,387 1.4% (99% CI: 0.7-2.5%) 98.6% 2001-2003
Isolated AVR 135 2.2% (99% CI: 0.4-8.9%) 97.8%
Isolated CABG 523 0.8% (99% CI: 0.2-2.7%) 99.2% 2003
Isolated AVR 43 0.0% (99% CI: 0.0-6.7%) 100.0%
Surgeons performing coronary surgery CABG per year
SCTS review of results
Argano Adult cardiac 111 Meets SCTS standards (three years)
Ashraf Adult cardiac 166 Meets SCTS standards (three years)
Youhana Adult cardiac 158 Meets SCTS standards (three years)
Locum and other independent surgeons performing more than 30 cases per year
Surgeons performing coronary surgery CABG per year
SCTS review of results
Amer Cardiothoracic 65 Meets SCTS standards (three years)
Bhatnagar Cardiothoracic 74 Meets SCTS standards (three years)
Cherian Cardiothoracic 46 Meets SCTS standards (one year)
Kolocassides Cardiothoracic 79 Meets SCTS standards (two years)
Lund Cardiothoracic 64 Meets SCTS standards (three years)
O’Toole Cardiothoracic 119 Meets SCTS standards (three years)
Sarkhar Cardiothoracic 179 Meets SCTS standards (three years)
Sitaram Cardiothoracic 69 Meets SCTS standards (two years)
Consultant Surgeons currently operating solely in the private sector
Surgeons performing coronary surgery CABG per year
SCTS review of results
Kallis Adult cardiac 95 i Meets SCTS standards (three years)
Pattison Adult cardiac 53 i Meets SCTS standards (three years)
i Includes 2 years-worth of data for operations performed when an NHS Consultant at the Heart Hospital.

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
307
NA
CSD
– Institu
tion
and
ind
ividu
al perfo
rman
ce
UKCSR: Funnel plot on 3-year isolated CABG data by Consultant; financial years 2001 - 2003 (n=64,488)
Overall rate 99.9 % lower alert 99.9 % lower alert Consultant
99.99% lower alarm 99.99% lower alarm
UKCSR: Funnel plot on 2-year isolated CABG data by Consultant; financial years 2002 - 2003 (n=46,066)
Overall rate 99.9 % lower alert 99.9 % lower alert Consultant
99.99% lower alarm 99.99% lower alarm
0%
1%
2%
3%
4%
5%
6%
7%
8%
9%
10%
0 100 200 300 400 500 600 700 800
Number of cases
Cru
de
mo
rtal
ity
rate
0%
1%
2%
3%
4%
5%
6%
7%
8%
9%
10%
0 100 200 300 400 500
Number of cases
Cru
de
mo
rtal
ity
rate

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
308
NA
CSD
– In
stit
uti
on
an
d in
div
idu
al p
erfo
rman
ce
UKCSR: Funnel plot on 1 year isolated CABG data by Consultant; financial year 2003 (n=24,546)
Overall rate 99.9 % lower alert 99.9 % lower alert Consultant
99.99% lower alarm 99.99% lower alarm
The three preceding graphs illustrate the variability and spread of surgeons’ results from year to year. The range of mortality is greater over one year than over three years. This is an inevitable consequence of random variation and is the reason why New York, Pennsylvania, New Jersey and now the United Kingdom have chosen to publish results using a 3-year average.
More specifically, the graph above shows a single outlier on one year’s data only, who over a three-year period had results that were well within the agreed statistical limits. Nevertheless, the surgeon reported his evolving concerns to his colleagues, the Society and the Trust management who instituted internal and external reviews. Analysis of his performance using appropriately risk stratified data together with a review of the working environment concluded that the unpredicted cluster of deaths was not related in any way to the surgeon’s clinical or operative skills.
We anticipate that our annual review of individual surgeons’ results when combined with the review of contributing organisational issues, which we are undertaking jointly with NCEPOD, that this process will become easier and easier for all concerned (see page 33).
Interestingly, detailed analysis reveals a small statistically significant volume effect in which a 20% increase in workload is associated with a one-twentieth reduction in operative mortality (5% relative reduction, 95% CL: 2-8%). In real terms, this translates to a reduction in operative mortality from 2.0% down to 1.9%, which is negligible in practical terms.
0%
2%
4%
6%
8%
10%
12%
0 50 100 150 200 250 300
Number of cases
Cru
de
mo
rtal
ity
rate

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
309
NA
CSD
– CA
BG
surg
ery follo
w u
p
Long-term follow up through the
Central Cardiac Audit Database

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
310
NA
CSD
– C
AB
G s
urg
ery
follo
w u
p
Long-term follow up through the Central Cardiac Audit Database
The Central Cardiac Audit Database (CCAD) administered by the NHS Information Authority as part of the National Clinical Audit Support Programme will alter the way we collect and present cardiac surgical data first in England and Wales and then in Scotland and Northern Ireland.
Currently the data presented and analysed in this report has been downloaded for analysis without specific patient identifiers. The CCAD mechanism has advanced encryption technology, which enables patient identifiers to be transmitted safely and then used to track the survival of any patient through the Office of National Statistics in England. If a patient has died the date of death is entered automatically into the database. At no point does medical information on that patient leave the database – it is secure.
This tracking of deaths on a regular basis allows us to build up a picture of what happens to different types of patient over the years following surgery. This is valuable because patients are increasingly interested in what their long-term future holds. Soon we will have the answers based on UK practice.
More excitingly, the CCAD will feed this information back to each cardiac surgical centre on-line in real time so they can perform their own analyses.
Units will also be able to see how their data and results compare with the national average for all sorts of operations and groups of patients.
This is an enormous and quite ambitious undertaking and will take time to perfect. Initially, the programme will be driven in England under the jurisdiction of the Healthcare Commission with oversight from a tripartite group composed of representatives from the Healthcare Commission, Department of Health and the Society of cardiothoracic Surgeons (see appendix).
When this system is running it will be the most advanced data collection and performance feedback system in the world.
The following graphs illustrate the potential goldmine of information available for patients and their surgeons. The graphs are based on only one hospital in the UK: Queen Elizabeth Hospital in Birmingham, but similar information should be available to every centre in the England within 18 months.
The following graphs show the percentage of patients surviving for six years following surgery at the Queen Elizabeth Hospital in Birmingham

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
311
NA
CSD
– CA
BG
surg
ery follo
w u
p
Isolated CABG: One centre’s actuarial survival curves by age (n=2,855)
Survival curve Standard error <61 years 61-70 years >70 years
The graph below shows that although women have a higher early mortality (see page 99) their longer-term survival after the early period is no different to that of men.
Isolated CABG: One centre’s actuarial survival curves by gender (n=2,855)
Survival curve Standard error Male Female
60%
65%
70%
75%
80%
85%
90%
95%
100%
0 500 1,000 1,500 2,000
Time after operation / days
Surv
ival
rat
e
60%
65%
70%
75%
80%
85%
90%
95%
100%
0 500 1,000 1,500 2,000
Time after operation / days
Surv
ival
rat
e

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
312
NA
CSD
– C
AB
G s
urg
ery
follo
w u
p
Isolated CABG: One centre’s actuarial survival curves by BSA (n=2,833)
Survival curve Standard error <1.70 m2 1.70-1.99 m2 >1.99 m2
Isolated CABG: One centre’s actuarial survival curves by operative priority (n=2,855)
Survival curve Standard error Elective Urgent Emergency
60%
65%
70%
75%
80%
85%
90%
95%
100%
0 500 1,000 1,500 2,000
Time after operation / days
Surv
ival
rat
e
60%
65%
70%
75%
80%
85%
90%
95%
100%
0 500 1,000 1,500 2,000
Time after operation / days
Surv
ival
rat
e

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
313
NA
CSD
– CA
BG
surg
ery follo
w u
p
Patients who have had a previous heart attack fare less well both in the short- (see page 123) and longer-term. This difference becomes starker if the heart attacks have damaged the heart muscle and reduced the heart function (see page 117).
Isolated CABG: One centre’s actuarial survival curves by ejection fraction (n=2,855)
Survival curve Standard error Good Fair Poor
Isolated CABG: One centre’s actuarial survival curves by incidence of previous MIs (n=2,852)
Survival curve Standard error None One Two or more
60%
65%
70%
75%
80%
85%
90%
95%
100%
0 500 1,000 1,500 2,000
Time after operation / days
Surv
ival
rat
e
60%
65%
70%
75%
80%
85%
90%
95%
100%
0 500 1,000 1,500 2,000
Time after operation / days
Surv
ival
rat
e

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
314
NA
CSD
– C
AB
G s
urg
ery
follo
w u
p
Isolated CABG: One centre’s actuarial survival curves by incidence of previous PCI (n=2,855)
Survival curve Standard error None One or more
Isolated CABG: One centre’s actuarial survival curves by left main stem disease (n=2,855)
Survival curve Standard error No LMS disease LMS disease
60%
65%
70%
75%
80%
85%
90%
95%
100%
0 500 1,000 1,500 2,000
Time after operation / days
Surv
ival
rat
e
60%
65%
70%
75%
80%
85%
90%
95%
100%
0 500 1,000 1,500 2,000
Time after operation / days
Surv
ival
rat
e

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
315
NA
CSD
– CA
BG
surg
ery follo
w u
p
Isolated CABG: One centre’s actuarial survival curves by previous cardiac surgery (n=2,855)
Survival curve Standard error No previous surgery Previous surgery
Isolated CABG: One centre’s actuarial survival curves by diabetes (n=2,855)
Survival curve Standard error No diabetes Diabetes
60%
65%
70%
75%
80%
85%
90%
95%
100%
0 500 1,000 1,500 2,000
Time after operation / days
Surv
ival
rat
e
60%
65%
70%
75%
80%
85%
90%
95%
100%
0 500 1,000 1,500 2,000
Time after operation / days
Surv
ival
rat
e

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
316
NA
CSD
– C
AB
G s
urg
ery
follo
w u
p
Isolated CABG: One centre’s actuarial survival curves by hypertension (n=2,855)
Survival curve Standard error No HT HT
Isolated CABG: One centre’s actuarial survival curves by peripheral vascular disease (n=2,852)
Survival curve Standard error No PVD PVD
80%
82%
84%
86%
88%
90%
92%
94%
96%
98%
100%
0 500 1,000 1,500 2,000
Time after operation / days
Surv
ival
rat
e
60%
65%
70%
75%
80%
85%
90%
95%
100%
0 500 1,000 1,500 2,000
Time after operation / days
Surv
ival
rat
e

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
317
NA
CSD
– CA
BG
surg
ery follo
w u
p
Isolated CABG: One centre’s actuarial survival curves by renal disease (n=2,852)
Survival curve Standard error No renal disease Renal disease
Isolated CABG: One centre’s actuarial survival curves by angina (n=2,855)
Survival curve Standard error CCS 1 & CCS 4 CCS 2 & CCS 3
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
0 500 1,000 1,500 2,000
Time after operation / days
Surv
ival
rat
e
60%
65%
70%
75%
80%
85%
90%
95%
100%
0 500 1,000 1,500 2,000
Time after operation / days
Surv
ival
rat
e

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
318
NA
CSD
– C
AB
G s
urg
ery
follo
w u
p
Isolated CABG: One centre’s actuarial survival curves by dyspnoea (n=2,855)
Survival curve Standard error NYHA 1 NYHA 2 NYHA 3 NYHA 4
Isolated CABG: One centre’s actuarial survival curves by EuroSCORE (n=2,706)
Survival curve Standard error Euroscore 0-1 2-3 4-5 >5
60%
65%
70%
75%
80%
85%
90%
95%
100%
0 500 1,000 1,500 2,000
Time after operation / days
Surv
ival
rat
e
60%
65%
70%
75%
80%
85%
90%
95%
100%
0 500 1,000 1,500 2,000
Time after operation / days
Surv
ival
rat
e

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
319
Ap
pen
dices
Appendices

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
320
Ap
pen
dic
es
Appendices
Society of Cardiothoracic Surgeons
Royal College of Surgeons of England
35-43, Lincoln’s Inn Fields,
London
WC2A 3PE
Richmond House
79 Whitehall
London
SW1A 2NS
29th October 2002
Chairmen of Trust Boards
Cardiac Surgical Centres
Dear Colleague
National Audit of Cardiac Surgery
We are writing to seek your help in ensuring the successful collection of comprehensive data for every patient undergoing heart surgery in England.
The enclosed report published recently by the Society of Cardiothoracic Surgeons with the support of the Academy of Medical Royal Colleges and the Department of Health is an exemplar of clinician-led audit and release of outcome data to the public.
It is vital that the challenging, but essential, task of collecting and validating this data is supported by hospital trusts and local health communities. The report demonstrates clearly that the necessary infrastructure is not in place in some centres.
Funding to support centres in their provision of data collection staff and systems was made available to the NHS this year from the £100 million for the Extending Patient Choice scheme for cardiac surgery. This was made clear to Chief Executives of cardiac surgery centres in letters and at a series of eight regional roadshows undertaken by the Heart Team earlier this year.
The requirement that Trusts should participate fully in national audits is also made explicit in the Performance and Planning Framework published on 2 October. This reinforces the commitment that Trusts would provide surgeon-specific outcome data with the intention of publication in 2004, made as part of the government’s response to the Kennedy Report following the Bristol Inquiry.
I am sure that you will appreciate the important part which reliable outcome data plays in the provision of high quality care for patients. We would be most grateful if you could help to make sure that your own Trust meets these requirements as part of your wider clinical governance agenda and also to report back to us any difficulties that you encounter.
Yours faithfully
Lord Hunt of King’s Heath Parliamentary Under-Secretary of State (Lords), DoH
Professor Peter Hutton Chairman, Academy of Medical Royal Colleges
Mr Colin Hilton President, Society of Cardiothoracic Surgeons of Great Britain and Ireland
7

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
321
Ap
pen
dices
Governance arrangements for adult cardiac surgical audit components of the central cardiac audit database
Introduction
1. This document sets out the governance arrangements, underpinning principles and operational guidelines for the management of the adult cardiac surgical audit components of the Central Cardiac Audit Database (CCAD).
Governance
2. The Chairman of CCAD will be accountable to a Board chaired by the Commission for Healthcare Audit and Inspection (CHAI) known hereafter as the Healthcare Commission for the operation of the cardiac surgical elements of CCAD and the activities of CCAD staff.
3. The Board will consist of six members, two each from the Healthcare Commission, the Society of Cardiothoracic Surgeons of Great Britain and Ireland (SCTS) and the Department of Health (DH). The project manager of the National Clinical Audit Support Programme (NCASP) and the Director of CCAD will attend to advise and observe.
Healthcare Commission Professor Bruce Keogh KBE Chair
Healthcare Commission Dr Jonathan Boyce Member
SCTS Representative Mr James Roxburgh Member
SCTS Representative Mr Ben Bridgewater Member
DoH Representative Dr Roger Boyle Member
DoH Representative Mr Gavin Larner Member
In attendance
NCASP Mr Martin Old
CCAD Dr Tony Rickards and Mr Chris Bell
4. DH representatives will liaise with the devolved national administrations prior to meetings to provide a UK wide Government position at the Board.
5. The board will be able to invite further advisers to attend on an ad hoc basis, for example, for expert statistical or analytical advice.
6. The Board’s decisions will be reached by consensus.
7. The Healthcare Commission will host the meetings and provide secretariat.
8. The Board will meet every quarter. Urgent business requiring speedy resolution can be cleared by e-mail on a consensus basis.
9. The terms of reference, membership and the need for the continuation of the Board will be reviewed annually.
Terms of Reference
10. The Board will have the following terms of reference:
a. to safeguard the confidentiality and security of patient, professional and institutional data, and analyses using that data, including
i. consideration of third party requests for access to or use of data;
ii. consideration of CCAD requests for use or disclosure of data; and
iii. approval of all publications and analyses using the CCAD data.
b. to make CCAD the authoritative source of data on cardiac surgery, by

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
322
Ap
pen
dic
es
i. ensuring adequate resources are available for the collection, validation, analysis and publication of data;
ii. appointing independent expertise to conduct analyses of outcome data;
iii. agreeing arrangements for the validation of data;
iv. promoting timely, accurate and complete submission of data;
c. to provide the Healthcare Commission with the information and analysis needed to give patients and the public clear, accurate, accessible and understandable information on cardiac surgical outcomes;
d. to foster greater understanding of the complexity underlying outcomes data among the public, patients, the media and opinion formers; and
e. to consider proposals for modifications to, or extensions to, the audit dataset.
Underpinning Principles and Operational Guidelines
11. In carrying out its terms of reference, the Board will be guided by the following principles and operational guidelines in addition to the information governance framework defined by the Healthcare Commission:
a. Confidentiality: CCAD, DH, the Healthcare Commission, SCTS and their members and employees will respect the confidentiality of all data and analyses about patients, clinicians or institutions and each will be accountable to their own ethical, regulatory and disciplinary frameworks for any breaches of this principle. In particular:
i. Data or analyses will not be communicated, formally or informally, outside of these organisations, without the explicit consent of any individual or organisation identified and without the approval of the Board;
ii. Should any party wish to use data to demonstrate or promote the work of CCAD, all patients, professionals and institutions should be carefully and effectively anonymised; and
iii. CCAD will log all central uses of local encryption keys with an explanation of their purpose. If technically feasible, CCAD should generate an automatic log when local keys are used. The Board will review this log on a quarterly basis.
b. Respect and Responsibility: All participants in the audit and its governance will show respect for the professionalism of their colleagues and participating organisations. Use and analysis of data should not be used to present an unfair representation of any individual or institution’s performance. Publication of data and analyses will be presented in such a way as to promote greater understanding and improve patient care.
c. Accountability to Patients and the Public: All participants will seek to ensure that use, analysis and publication of data gives patients and the public better information which extends their knowledge and understanding of the profession and the complexity of health care, whilst supporting patients and their families in making decisions about their health and treatment.
d. Supporting Clinical Governance and Improved Performance: The use, analysis and presentation of data needs to be sensitive to the impact it might have on professional behaviour and have due regard to the risks of defensive practice or inhibiting properly consented and appropriate high risk interventions. The effect of clinical audit must remain the improvement of patient care and better outcomes.
e. Independence and Integrity: Data, analyses and publications using the audit need to be perceived as authoritative, impartial and independent and arrangements for validation and analyses will need to ensure this.
f. UK-Wide: Where possible the Board should seek to ensure, working with colleagues in Scotland, Wales and Northern Ireland, that participation in the work of CCAD is facilitated and resourced.
Corporate accountability
The Board will be accountable to the Commission for Healthcare Audit and Inspection through the Director for Information and Analysis, to the Department of Health through the National Director for Heart Disease and to the Society of Cardiothoracic Surgeons through the Secretary of the Society.
James Roxburgh Jonathan Boyce Roger Boyle Secretary, SCTS External Outputs, CHAI National Director for Heart
Disease,

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
323
Ap
pen
dices
Lines of public accountability for the oversight of analysis and publication of the adult cardiac surgical component of the Central Cardiac Audit Database through the Healthcare Commission

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
324
Ap
pen
dic
es
The Parsonnet score
The Parsonnet score was the first simple, validated, additive scoring system for predicting risk in cardiac surgery. It is widely used in the UK, but its weakness is that it allows subjective scoring (variables highlighted in blue). These have been omitted for the centrally calculated score used in this report.
Factor Definition Score
Gender Female 1
Morbid obesity Body Mass Index >35 3
Diabetes Any history of diabetes regardless of duration or treatment. Latent diabetes of pregnancy excluded 3
Hypertension A history of blood pressure greater than 140/90mmHg on two occasions, or lower if on medication
3
Good (50%) 0
Fair (30-49%) 2
LV dysfunction
Poor (<30%) 4
70-74 years old 7
75-79 years old 12
Age
> 80 years old 20
Second operation 5 Re-operation
Third (or more) 10
Intra aortic balloon pump Prior to surgery. Do NOT include IABP’s inserted prophylactically just prior to surgery because these represent post-operative support.
2
Left ventricular aneurysm Aneurysmectomy 5
Within 24 hours of operation 10 Recently failed intervention
>24 hours; operation on same admission 5
Renal Dialysis dependency 10
Catastrophic states e.g.s acute structural defect, cardiogenic shock, acute renal failure 10-50
Pat
ien
t-re
late
d fa
cto
rs
Other rare circumstances e.g.s paraplegia, pacemaker dependency, congenital heart disease in adults, severe asthma
2-10
Systolic PA pressure <60 mmHg 5 Mitral valve surgery
Systolic PA pressure ≥60 mmHg 8
AV pressure gradient ≤120 mmHg 5 Aortic valve surgery
AV pressure gradient >120 mmHg 7
Surg
ery-
rela
ted
fa
cto
rs
CABG at the time of valve surgery 2
In the original paper, an additive score of
• 0-4 translated to an average operative mortality of 1% (low risk)
• 5-9 5% (elevated risk)
• 10–14 9% (significantly elevated risk)
• 15–19 17% (high risk)
• >19 31% (very high risk)
In addition, the impact of the variables used in the Parsonnet score has changed over time. Consequently there is a tendency to over predict operative risk, hence the move to develop newer scoring systems such as the EuroSCORE and the UK Bayes scores illustrated overleaf.

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
325
Ap
pen
dices
The EuroSCORE
The EuroSCORE project, led by Mr Sam Nashef, has recently reported. This is a weighted, additive score similar in concept to the North American Parsonnet score but based on a pan-European sample of cardiac surgical patients and represents a considerable improvement on the Parsonnet score.
Factor Definition Score
Age Per 5 years or part thereof over 60 1
Gender Female 1
Chronic Pulmonary disease Long-term use of bronchodilators or steroids for lung disease 1
Extra cardiac arteriopathy Any one or more of the following: claudication, carotid occlusion or >50% stenosis, previous or planned surgery on the abdominal aorta, limb arteries or carotids
2
Neurological dysfunction Disease severely affecting ambulation or day-to-day functioning 2
Previous cardiac surgery Previous surgery requiring opening of the pericardium
3
Serum creatinine >200 mmol l-1 pre-operatively 2
Active endocarditis Patient still under antibiotic treatment for endocarditis at the time of surgery 3
Pat
ien
t-re
late
d fa
cto
rs
Critical pre-operative state Ventilation before arrival in the anaesthetic room, pre-operative inotropic support, intra aortic balloon counterpulsation (IABP) or pre-operative acute renal failure (anuria or oliguria <10ml/hr)
3
Unstable angina Angina requiring iv nitrates until arrival in the operating room 2
LV dysfunction Moderate (30-50%) 1
Poor (<30%) 3
Recent myocardial infarction <90 days 2
Car
dia
c-re
late
d
fact
ors
Pulmonary hypertension Systolic PA pressure >60 mmHg 2
Emergency Carried out on referral before the beginning of the next working day 2
Other than isolated CABG Major cardiac operation other than or in addition to CABG
2
Surgery on thoracic aorta Ascending, arch or descending aorta 3 Op
erat
ion
-re
late
d fa
cto
rs
Post infarct septal rupture 4

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
326
Ap
pen
dic
es
The simple (5-factor) CABG Bayes score
r i n ii p iii odds iv LR v weight vi
OVERALL 835 33,392 2.5% 0.026 NA -36.63
<56 years old 84 6,626 1.3% 0.013 0.501 -6.92
56-60 years old 70 5,250 1.3% 0.014 0.527 -6.41
61-65 years old 134 6,670 2.0% 0.021 0.799 -2.24
66-70 years old 183 6,730 2.7% 0.028 1.090 0.86
Ag
e
71-75 years old 195 4,952 3.9% 0.041 1.598 4.69
>75 years old 153 2,325 6.6% 0.070 2.747 10.10
<1.7 m2 118 2,941 4.0% 0.042 1.630 4.88
1.70-1.89 m2 201 6,979 2.9% 0.030 1.156 1.45
1.90-2.39 m2 355 16,490 2.2% 0.022 0.858 -1.53
Bo
dy
Surf
ace
Are
a
>2.39 m2 39 2,284 1.7% 0.017 0.677 -3.90
Good EF 317 19,652 1.6% 0.016 0.639 -4.480
Fair EF 248 8,410 2.9% 0.030 1.185 1.70
Ejec
tio
n
frac
tio
n
Poor EF 185 2,044 9.1% 0.100 3.880 13.56
Elective 374 21,098 1.8% 0.018 0.704 -3.52
Urgent 247 8,142 3.0% 0.031 1.220 1.99
Pri
ori
ty
Emergency 126 914 13.8% 0.160 6.235 18.30
None 679 29,278 2.3% 0.024 0.926 -0.77
Pri
or
op
’ns
One or more 87 1,335 6.5% 0.070 2.718 10.00
i number of deaths ii number of operations in the group / sub-group iii probability of death iv odds on death v likelihood ratio vi 10 × ln(likelihood ratio)

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
327
Ap
pen
dices
The complex (9-factor) CABG Bayes score
r i n ii p iii odds iv LR v weight vi
OVERALL 835 33,392 2.5% 0.026 NA -36.63
<56 years old 84 6,626 1.3% 0.013 0.501 -6.92
56-60 years old 70 5,250 1.3% 0.014 0.527 -6.41
61-65 years old 134 6,670 2.0% 0.021 0.799 -2.24
66-70 years old 183 6,730 2.7% 0.028 1.090 0.86
Ag
e
71-75 years old 195 4,952 3.9% 0.041 1.598 4.69
>75 years old 153 2,325 6.6% 0.070 2.747 10.10
<1.7 m2 118 2,941 4.0% 0.042 1.630 4.88
1.70-1.89 m2 201 6,979 2.9% 0.030 1.156 1.45
1.90-2.39 m2 355 16,490 2.2% 0.022 0.858 -1.53
Bo
dy
Surf
ace
Are
a
>2.39 m2 38 2,280 1.7% 0.017 0.661 -4.14
No 162 5,055 3.2% 0.033 1.291 2.55
Dia
bet
es
Yes 559 23,486 2.4% 0.024 0.951 -0.51
No 310 14,776 2.1% 0.021 0.836 -1.80
HT
Yes 462 15,773 2.9% 0.030 1.177 1.63
No 418 19,431 2.2% 0.022 0.857 -1.54
LMS
Yes 138 3,919 3.5% 0.036 1.423 3.53
Good 317 19,652 1.6% 0.016 0.639 -4.47
Fair 248 8,410 2.9% 0.030 1.185 1.70
Ejec
tio
n
frac
tio
n
Poor 185 2,044 9.1% 0.100 3.880 13.56
Elective 374 21,098 1.8% 0.018 0.704 -3.51
Urgent 247 8,142 3.0% 0.031 1.220 1.99
Pri
ori
ty
Emergency 126 914 13.8% 0.160 6.235 18.30
Dialysis 12 138 8.7% 0.095 3.713 13.12
Elevated creatinine 85 1,071 7.9% 0.086 3.361 12.12
Ren
al
dis
ease
None 463 21,778 2.1% 0.022 0.847 -1.66
None 679 29,278 2.3% 0.024 0.926 -0.77
Pri
or
op
’ns
One or more 87 1,335 6.5% 0.070 2.718 10.00
i number of deaths ii number of operations in the group / sub-group iii probability of death iv odds on death v likelihood ratio vi 10 × ln(likelihood ratio)

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
328
Ap
pen
dic
es
Facts of life the figures can hide
A contribution to the public debate from the Executive Committee of the Society of Cardiothoracic Surgeons of Great Britain and Ireland on the impact of the public release of surgical outcome data by Dr Foster. The Times, 19th November 2001.
When you buy a car or house you do your homework first. It would be unthinkable not to study the specifications of the car or to have a structural survey performed on the house. Surprisingly, until very recently, information on how well hospitals perform has not been available to those who need it most. Since the inception of the NHS the assumption has been that our health service offers among the best medical and surgical services in the world; but can this assumption be justified?
The information published today is good news. The Dr Foster analysis independently confirms our evidence that the results of heart surgery are steadily improving despite the fact that we are operating on older and sicker patients. Today’s publication also shows that overall the results of coronary bypass surgery in England are as good as anywhere in the world, but inevitably there is quite a variation in results between hospitals. Experience from North America has shown that this variation is neither surprising nor unusual. For example, between 1995 and 1998 the percentage of patients dying following coronary surgery in different hospitals in New York State ranged from 0.62–4.56% (average 2.27%) compared with 0.8–4.6% in the UK for 1998-2000 (average 2.3%).
A comparison of data between UK and USA national cardiac surgical databases shows that the survival rates for coronary surgery the UK and US are almost identical at 97.6% and 97.3% respectively in 1999. These are extremely good results, but we must remember that heart surgery is a highly technical, complex business ad although we can achieve a relatively low risk for most patients we can never reduce this to no risk.
Today’s league tables are based on the Department of Health’s Hospital Episode Statistics (HES), which were not designed to collect detailed clinical data. The tables try to compensate for differences in patient populations at different hospitals by taking into account the effects of age, gender, urgency of operation and social status or deprivation, but surgeons base decisions for surgery on much more detailed and often subtle clinical information. The way the tables have been constructed is the best that can be expected from the data available, but many other conditions such as underlying heart function, lung function, smoking history, diabetes, obesity, high blood pressure, kidney function and other vascular conditions all have an impact on the risk of a heart operation. These factors must all be taken into account when calculating surgical risk, particularly if meaningful comparisons between units or surgeons are to be made. For example, if a patient has had a heart attack which has significantly reduced his heart function to the point where he is very breathless he is ten times more likely to die during an operation than the average patient, yet he may have the most to gain. Such patients may be seen in some units in greater numbers than in others because some units serve older and sicker populations, or because those units have special expertise; unless such factors are taken into account unfair comparisons may be made. This type of important and clinically relevant information is simply not available in the current NHS information systems. In fact, of the four most important risk factors for coronary bypass surgery (advanced age, emergency status, poor heart function and whether this is a repeat operation), only the first two are accounted for in the published tables.
This needs to be rectified, so we are working closely with the NHS information people to ensure that the right kind of information is collected in all heart surgery units.
We favour publishing measures of how well a centre is working. We don’t think that simply ranking units according to how many patients die is necessarily the best way, because the sickest patients most in need of surgery are those who are most likely to die as a result of the operation and also the most likely to benefit. So we need to work out a better set of measures that don’t penalise units who may be trying very hard for very sick patients in their area.
If we cannot sort this issue out quickly then those units that feel misrepresented by improperly weighted data may find an easy solution by simply avoiding high risk cases as has happened in the United States whenever the state Government imposes a reporting system, rather than working with the professional societies to use the national registry already developed by the American Society of Thoracic Surgeons.
In Pennsylvania a published survey showed that two thirds of surgeons are less willing to operate on higher risk patients because of the Consumer Guide league tables. This is because 85% believe there is inadequate risk adjustment and that mortality is too crude a measure of surgical quality. In addition nearly 60% felt that league tables led to data being manipulated to increase the apparent risk of surgery, a fact that became apparent in New York State. After the first publication of league tables the incidence of lung disease rose from 1.8% to 52.9% and the incidence of unstable angina requiring intravenous treatment rose from 1.9 to 20.8% - all in one year! Clearly this could not have been the result of a sudden upsurge in the incidence of these conditions, but rather to more liberal labelling of patients with these diagnoses.
A survey of New York surgeons in 1998 reported that nearly 40% of surgeons had changed their criteria for accepting patients and over 60% had turned down high risk patients in the preceding year as a result of the

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
329
Ap
pen
dices
public reporting system. In addition, there is evidence of increased referral of high risk cases to the Cleveland Clinic from nearby areas of New York State.
When Newsnight surveyed heart surgeons in this country they found that although 78% of surgeons were in favour of public disclosure of outcomes, 90% felt that the threat of public disclosure had already resulted in high risk patients being turned down for surgery. The irony is that although turning down high risk patients is an easy way to improve your position in the league table, the best surgeons and institutions often have higher mortalities because they are referred and operate on the highest risk patients. Unfortunately some of the key determinants of success or failure, such as the severity and extent of coronary artery disease, are often subtle and not easily measurable.
The Society of Cardiothoracic Surgeons has independently pioneered data collection and analysis to allow such comparisons to be made and we now have some of the best comparative analyses available in the world. Unfortunately some units still do not have the facilities for properly detailed data collection because funding has not been forthcoming. But on the 18th July this year the Secretary of State, Mr Alan Milburn while delivering his ministerial response to the Bristol Royal Infirmary Inquiry to the House of Commons stated:
For data on surgical outcomes to be published, of course, it needs to be robust, rigorous and risk adjusted. That will take inevitably time.
In order to improve our data quality we have been working with the Nuffield Trust to draw on the American experience through the Rand Organisation in the US and the California Department of Health to develop reliable methods of data validation and novel, easily understandable ways of presenting surgical results. Simultaneously we have been working with the Department of Health to get away from the situation where everyone uses different data.
Variations in outcome between units are usually the result of differences in the pattern of heart disease in that area, how soon people are diagnosed and referred for surgery or the hospital environment. Heart surgery is a highly complex process involving a large number of dedicated professionals all working as a team. If the environment isn’t right for any reason then the teamwork will suffer. Given all these factors it is not surprising that noticeable differences in outcome between units is seldom due to the technical quality of the operation, since UK heart surgeons are all trained in the same system. Of course some surgeons will be better than others as in any job. But take a good surgeon and put him in a poor environment with poor teamwork and inadequate support and his results will suffer and vice versa.
The Walsgrave Hospital highlighted in today’s league tables is a case in point. All units and surgeons in the UK voluntarily submit their activity results to the Society of Cardiothoracic Surgeons. When surgeons at the Walsgrave became aware that the centre results did not compare favourably with other units they instituted a variety of changes primarily to the way their patients were assessed prior to surgery. Detailed analysis of their data, following these changes, has shown that their outcomes are much better and are now entirely consistent with overall UK results.
Surgical technique also plays a role. There is clear evidence that using an artery, called the internal mammary artery, from inside the chest, rather than a vein from the leg, to bypass the most important coronary artery in the heart reduces the risk of surgery. In 1999 in the UK 88.5% of patients received at least one internal mammary artery graft as opposed to 79% in the US. Similarly, improved surgical technique and selection of the right patients has reduced the mortality for repeat coronary surgery in the UK from 9.6% in 1997 to 5.5% in 1999. But there have been improvements in other areas as well. We are treating diabetics better. The mortality for diabetics undergoing surgery has fallen from 5.7% in 1996 to 3.2% in 1999 – a 40% improvement in outcome.
We are keen to raise the overall quality of heart surgery and to establish mechanisms to protect patients from unnecessary institutional risk. Equally, we remain clear that any analyses that enter the public domain should be conducted on accurate and relevant data and should be subject to professionally agreed caveats. In keeping with these principles the New York State Department of Health spend almost 3 years validating data before publication; the 1998 data were released earlier this year. In New York, and generally throughout the United States, patients have a choice of where they have their operations. In turn surgeons can generally choose the hospital where they work and the team with whom they work. Neither condition is true in the NHS where patients have little or no choice as to where they are referred for surgery. It is therefore particularly important to get things right in order to prevent misinterpretation and unnecessary distress in an increasingly litigious environment.
Although the current league tables are based on data which have inherent flaws we hope they will force trusts to focus attention on developing accurate and clinically relevant data collection and to use this to analyse, understand and improve the quality of service they offer. League tables should therefore spur us to seek answers to the questions they raise, but it must be recognised they themselves are not the answer. We hope that today’s analysis will at least stimulate debate on how best to measure the quality of heart surgery in the UK.

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
330
Ap
pen
dic
es
Guidelines for the audit of cardiothoracic surgical practice
Background
The Society of Cardiothoracic Surgeons of Great Britain and Ireland was the first professional body to co-ordinate national data collection in the United Kingdom with the introduction of the United Kingdom Thoracic Surgical Register in 1976 and the Cardiac Surgical Register in 1977. These voluntary registers collect simple activity and mortality data from all NHS cardiothoracic and thoracic surgical units in the UK in an anonymous fashion. The evolution of cardiothoracic surgical practice has been attended by an understanding of the influence of cardiac and non-cardiac factors on survival from cardiac and thoracic surgery. Mortality is mainly influenced by severity of illness and associated co-morbidities, but appropriateness of treatment and in-hospital quality of care also play a significant role. It has become clear that greater complexity of surgery in an increasingly diverse population severely undermines the value of simple surgical mortality as a measure of quality of care. Over the last few years various statistical algorithms have become available that relate operative mortality and morbidity to casemix.
A combination of marketplace competition together with public and political awareness has raised vigorous debate on issues relating to quality of care and institutional and individual surgical performance. The Society of Cardiothoracic has chosen to take the initiative and recommend that all cardiothoracic surgical units throughout the UK should undertake regular review of their practice in a risk stratified fashion. We believe that this approach represents good risk management policy for trusts, hospitals, individual units and their surgeons and will raise the overall quality of clinical care.
The implementation of such an approach and the responsible interpretation of the resultant data require national and local agreement and co-ordination of responsibilities.
Individual and institutional responsibilities
The Hospital Trust should provide the hardware, software and personnel to allow patient orientated data collection for risk stratification, and downloading of data into the Society’s National Cardiac and Thoracic Surgical Databases.
The Cardiothoracic Surgical Centres should define the strategy for data collection, collation and presentation, and should dedicate time each month for presentation and discussion of surgical activity and results. The centre should identify one consultant with overall responsibility for co-ordinating and developing the audit programme.
Each Consultant Surgeon must assume full responsibility for collection of complete, accurate and honest data on all cases under his/her care, provided the trust has met the obligations outlined above.
The Society of Cardiothoracic Surgeons of Great Britain and Ireland will provide individual clinicians and trusts with guidance on contemporary standards of care. To this end the Society will:
• define a recommended dataset for each surgical patient.
• develop and provide statistical models enabling individual and group risk prediction and outcome comparison.
• define contemporary levels of performance based on these statistical models.
• circulate an annual audit report to members.
• publish summarised and aggregated data on the internet at www.scts.org
The Royal College of Surgeons Specialist Advisory Committee for Higher Surgical Training will seek evidence during inspections that effective audit meetings have taken place, all surgical staff have attended regularly, appropriate records have been kept and that adequate audit assistance and computer systems are available.

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
331
Ap
pen
dices
Data collection
Data collection remains the joint responsibility of the trust and the Surgeon. To facilitate effective risk stratification data should be collected in line with the appended Minimum Dataset (MDS) defined by the Society of Cardiothoracic Surgeons. The current MDS, and its associated definitions, is compatible with all existing initiatives in the UK such as the UK Heart Valve Registry, the Central Cardiac Audit Database (CCAD) and the British Cardiac Intervention Society database (BCIS). The definitions and data fields are also compatible with evolving European initiatives and the Society of Thoracic Surgeons (USA), American College of Cardiology and the Healthcare Financing Administration (HCFA) in the United States.
The Society strongly encourages collection of the Recommended Dataset that allows robust risk stratification together with tracking of several aspects of surgical practice including surgical training, and measurement of outcomes other than mortality alone.
Data collection strategies must be determined locally. However, algorithms for risk stratification are becoming more complex and numbers of patients will grow. A networked computerised system with good statistical capabilities is recommended.
Data validation
Local validation should be performed by random selection of case notes to reduce gaming / fraud
External validation of data will be performed by the Society on 3-5 yearly cycles. Details of the validation process will be forwarded to individual units.
Audit meetings
Should be held monthly in allocated and dedicated time. All consultants should attend meetings and should take it in turn to chair the meetings and should foster an air of constructive analysis and criticism. Specialist registrars should be involved, as part of their training, and attendance of nursing, technical and other staff should be encouraged. A register of attendance should be kept. The form of presentation and discussion should be agreed and developed locally, but meetings should address:
• Total surgical activity.
• Risk stratified activity.
• Mortality and morbidity.
• Intermittent detailed review of specific issues and outcomes in order to improve practice.
Surgeon-specific review
By unanimous agreement within the speciality surgeon-specific outcome data for marker operations has been returned to the Society of Cardiothoracic Surgeons from 1st April 1997. This will be collected annually in a format defined by the Society and will be collated and analysed as part of the established UK Cardiac and Thoracic Surgical Registers. The President of the Society will seek clarification from any surgeon whose performance lies outside predefined limits. Clearly this clarification will be greatly simplified for all parties if facilities for comprehensive data collection and risk adjustment are in place. If concern persists then the Medical Director of the trust will be contacted and the Society will provide, in conjunction with the Royal College of Surgeons, a discrete and supportive external review by senior cardiothoracic surgeons. The aim of such a visit would be to determine the nature and severity of the perceived problem and to develop a collaborative strategy for resolution of the problem.
In addition to the mandatory return of surgeon-specific data to the Society individuals should continuously review their own progress using risk stratified data. Surgeon-specific data should be reviewed jointly by the consultant surgeons on at least an annual basis. The Society will respond supportively to an approach from a concerned member, his colleagues or the trust recognising that in some instances this may simply be an issue of rebuilding personal or institutional confidence and credibility.
The Society of Cardiothoracic Surgeons of Great Britain & Ireland accords the highest priority to surgical audit and requests that all concerned give due consideration to the value and importance of the professional responsibilities outlined above.

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
332
Ap
pen
dic
es
Quality accreditation programme for adult cardiac surgery Mr Mark Jones, Chairman of the Quality Accreditation Programme
The Quality Accreditation (QA) Programme was established by Sam Nashef and Bruce Keogh; it was intended to provide formal recognition for those units where robust clinical audit was regularly carried out; such audit helps to ensure delivery of a high quality surgical service. The programme was favourably received and endorsed at the AGM of the Society in March 2000.
The Society can be justly proud of its track record in quality monitoring when compared to that of other medical specialities. The national register for adult, paediatric and thoracic surgery procedural mortality has been one of the earliest examples of self-regulation and quality monitoring in any medical field. More recently, the introduction of index procedure mortality data gathering for individual surgeons' performance has expanded the remit of the Society's monitoring system. The development of the Society database for adult cardiac surgery has further enlarged the scope of data gathering and looks set to be the first project to succeed in developing a national, risk stratified database with over 80% of all units currently submitting at least partial data to the project.
Nevertheless, the current medico-political climate allows no room for complacency. The existing systems are valuable, but their value is limited by the absence of data validation and comprehensive data collection and, in the case of the register and index procedural results, also from a lack of a suitable measure of casemix. This is particularly important if surgeons are expected to continue to offer potentially life-saving surgery to high risk patients. This scheme aims to address these issues by offering public recognition of those units in which quality is monitored by a robust system of measurement of risk stratified outcomes with clear performance targets and mechanisms for dealing with underperformance as measured against such targets.
The scheme has two further, important aims. The first is to promote a culture in which quality monitoring as outlined above becomes the norm in surgical practice, thus providing the incentive for hospital management and purchasers to supply the resources necessary for surgical units to qualify for accreditation. The second is to act as a model for extending quality monitoring to other aspects of our own speciality (thoracic surgery, paediatric cardiac surgery and transplantation) and to other surgical and medical specialities.
The basics for QA are simple. In order to be successful a Unit must demonstrate:
• It knows what it is doing (Numbers, types of operations, outcomes).
• It has an idea of what sort of outcomes it thinks are acceptable. (An element of risk stratification with a pre-set target of what would be an acceptable outcome in relation to the risk).
• It knows what to do if the outcomes are not acceptable. (A pre-established mechanism for tackling an under performance with clear cut responsibilities of key individuals and an action plan including re-auditing to ensure the problem is sorted).
Participation
Any centre or hospital performing adult cardiac surgery in Britain and Ireland is eligible to apply for accreditation. Participation is wholly voluntary and the process is only initiated at the request of an individual unit. Members of the Society are encouraged to examine the criteria for accreditation to ensure that their centre has the necessary mechanisms in place before applying and, if not, to take steps to install these mechanisms.

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
333
Ap
pen
dices
Accreditation criteria
The Society must be satisfied that the centre fulfils all of the ten criteria listed below:
1. There are reliable data on the number of adult heart operations performed in the unit.
2. There are reliable data on the number of adult heart operations performed under the care of every consultant surgeon in the unit.
3. There are reliable data on the breakdown of these operations by broad category types, such as coronary surgery, valve surgery, combined coronary and valve surgery and others.
4. There is a valid system of assessing casemix. This can be a simple system, such as one based on age and sex, an additive risk stratification system, such as Parsonnet or EuroSCORE, or a more complex system such a regression analysis system or a Bayesian model. (The collection of the Society minimum dataset is encouraged but this is not a prerequisite to accreditation).
5. There are reliable data on clinical outcome measures. At the very least, these must include hospital or 30-day mortality.
6. There is a preset level of minimum acceptable performance in relation to the casemix measure. This level must be acceptable to the visitors. Examples are mortality within 70% of Parsonnet predicted mortality, or within 2 standard deviations of EuroSCORE predicted mortality.
7. The pre-set minimum acceptable performance must be applied to the unit's performance as a whole as well as to that of individual consultant surgeons.
8. The data on numbers (1, 2, 3, and 5 above) are reliable and can be validated by review of an appropriate sample of case notes or by the presence of a robust local system of data validation.
9. The casemix data (4 above) are reliable and can be validated by review of an appropriate sample of case notes or by the presence of a robust local system of data validation.
10. There is in place a clear and effective mechanism to investigate and appropriately to deal with any performance that falls outside the minimum acceptable performance level (6 above). The mechanism must include identification of the nature of the problem, measures to correct the problem, reassessment after a predetermined period and an action plan to be followed should initial measures fail.
Accreditation
The visitors may make three recommendations to the Executive of the Society: to grant accreditation, to grant accreditation with specific suggestions for improvement or to withhold accreditation, giving reasons and suggestions for achieving accreditation at a later date. The SoCS will consider the visitors' report and recommendations and, if satisfied, will then grant accreditation to the recommended units on behalf of the Society.
Accredited units may make public their accreditation to purchasers, patients and health authorities and may use the Society's quality accreditation logo on notepaper, in correspondence and elsewhere if appropriate.
Accreditation will be valid for a period of five years; continuance will require a further visit.
Which units have been accredited?
The Units deemed to have satisfied these criteria were (in alphabetical order):
• Bristol Royal Infirmary.
• Glasgow Western Infirmary.
• Hammersmith Hospital London.
• Cardiothoracic Centre Liverpool.
• Manchester Royal Infirmary.
• Nottingham City Hospital.
• Papworth Hospital.
The Glasgow Royal Infirmary is currently awaiting a second visit.

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
334
Ap
pen
dic
es
The visits have been both a valuable and constructive exercise and educational for both units and visitors alike. The key impression for visitors was of the enthusiasm and rigor with which the accredited units had embraced quality control. There were different but equally valid approaches to target setting and outcome monitoring. Risk models varied but were broadly based upon the use of Parsonnet or EuroSCORE. Units were able to demonstrate examples of corrective measures to adverse trends based upon robust hospital managerial and clinical governance structures.
Unit ownership of data, its transparency and willingness to submit to external peer-review reflects the maturity of a Department’s approach to quality-control.
The current lack of interest from additional units seeking QA is a concern. This hesitancy may, in time, be countered by, firstly, anxiety surrounding the public release of surgeon-specific outcome data and, secondly, the development of the joint European Cardiovascular and Thoracic Institute of Accreditation (ECTSIA), under the jurisdiction of European Association for Cardio-Thoracic Surgery, the European Society of Thoracic Surgery and the European Society of Cardiovascular Surgery, currently Directed by Mr SAM Nashef.
The fact that many of the audit leads from cardiac surgery centres attended a recent CHAI / CCAD / SCTS meeting in January 2004 at the then CHI headquarters emphasises the concerns these units share about surgical outcomes, the audit process and the validation of data. Involvement of the NHS Information Authority and the Healthcare Commission in this process will only serve to add weight and objectivity.
Further information
For any additional information, or to apply for accreditation, contact:
Mr Mark Jones
Address Consultant Cardiothoracic Surgeon
Wythenshawe Hospital
South Moor Road, Wythenshawe,
Manchester, M23 9LT
Telephone +44 (161) 291 2513
e-mail [email protected]

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
335
Ap
pen
dices
The minimum dataset

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
336
Ap
pen
dic
es

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
337
Ap
pen
dices

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
338
Ap
pen
dic
es

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
339
Ap
pen
dices

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
340
Ap
pen
dic
es

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
341
No
tes
Notes

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
342
No
tes
Notes

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
343
No
tes
Notes

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
344
No
tes
Notes

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
345
No
tes
Notes

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
346
No
tes
Notes

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
347
No
tes
Notes

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
348
Ref
eren
ces
References
1 Keogh B, Dussek J, Watson D, Magee P and Wheatley D. Public confidence and cardiac surgical outcome (Editorial). BMJ 1998; 316 (7147): 1759-20 2 The Report of the Public Inquiry into Children’s Heart Surgery at Bristol Royal Infirmary 1984-1995. The Bristol Royal Infirmary Inquiry, 2001. 3 http://www.doh.gov.uk/bristolinquiryresponse 4 Keogh B. Facts of life the figures can hide. (Viewpoint) The Times, 19 November 2001 5 Fine L, Keogh B, Cretin S, Orlando M and Gould M. How to evaluate and improve the quality and credibility of an outcomes database: validation and feedback study on the UK Cardiac Surgery Experience. BMJ 2003; 326: 25-28 6 Keogh B, Spiegelhalter D, Bailey A, Roxburgh J, Magee P and Hilton C. Towards public disclosure of individual surgeon’s results: the surgeons’ tale. BMJ 2003 (Accepted for publication) 7 Keogh B. Cardiac surgical mortality: the tip of the quality assurance iceberg. (Editorial) Heart. 2000; 84: 7-8. 8 http://www.oshpd.cahwnet.gov/hqad/ccorp/index.htm 9 Fine L, Keogh B, Orlando M, Cretin S and Gould M. Improving the credibility of information on healthcare outcomes. The Nuffield Trust, 2003 10 English TAH, Bailey AR, Dark JF and Williams WG. The UK Cardiac Surgical Register 1977-82 BMJ 1984; 289:1205-8 11 Parsonnet V, Dean D and Bernstein AD (1989). A method of uniform stratification of risk for evaluating the results of surgery in acquired heart disease. Circulation 1989; 79: I3-I12 12 Spiegelhalter D. Surgical audit: statistical lessons from Nightingale and Codman. J R Statist Soc. 1999;162 (Part1): 45-58 13 Annals of Thoracic Surgery 2000; 69: 4 (Suppl) 14 Keogh B and Kinsman R. National adult cardiac surgical database report 2000-2001. London. Society of Cardiothoracic Surgeon of Great Britain and Ireland. 2002. 15 Fine LG, Keogh BE, Cretin S, Orlando M, Gould MM. How to evaluate and improve the quality and credibility of an outcomes database: validation and feedback study on the UK Cardiac Surgery Experience. BMJ 2003; 326: 25-28 16 Gibbs JL, Monro JL, Cunningham D, Rickards A. Survival after surgery or therapeutic catheterisation for congenital heart disease in the United Kingdom: analysis of the central cardiac audit database for 2000-1. BMJ 2004; 328: 611 17 Treasure T. A cautionary note on the interpretation of surgical results. National Adult Cardiac Surgical Database Report 2001–2002 18 Bridgewater B, Grayson AD, Jackson M, Brooks B, Grotte GJ, Keenan DJM, Millner R, Fabri BM, Jones M. Surgeon specific mortality in adult cardiac surgery: comparison between crude and risk stratified data. BMJ 2003; 327: 13-17 19 Clark RE, Edwards FH and Schartz M. Profile of pre-operative characteristics of patients having CABG over the past decade. Ann. Thor. Surg. 1994; 58 1863-5 20 http://www.health.state.ny.us/nysdoh/heart/pdf/1998-2000_cabg.pdf 21 Guidelines and indications for coronary artery bypass graft surgery. A report of the American College of cardiology / American Heart association Task Force on Assessment of Diagnostic and Therapeutic Cardiovascular Procedures (Subcommittee on Coronary artery bypass graft surgery). JACC 1991; 17: 543-89 22 Chassin MR. The Missing, unconfirmed or unmapped ingredient in health reform: quality of care. JAMA 1993; 270: 377-8 23 Chassin MR, Hannan EH, De Buono BA. Benefits and hazards of reporting medical outcomes publicly. New Eng. J. Med. 1996; 334: 394-8

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
349
Referen
ces
24 Keogh B & Kinsman R. First European Adult Cardiac Surgical Database Report. European Association for Cardiothoracic Surgery. 2003 25 Data analyses of the Society of Cardiothoracic Surgeons National Adult Cardiac Surgery Database, Spring 2004 26 Edwards FH, Clark RE, Schwartz M. Coronary artery bypass surgery - results, trends, and risk assessment from The Society of Thoracic Surgeons National Database experience. Ann. Thorac. Surgery 1994; 57: 12-19 27 Grover FL, Shroyer AL, Edwards FH, Pae W, Ferguson TB, Gay WA, Clark RE. Data quality review program: The Society of Thoracic Surgeons Cardiac Surgery Database. Ann. Thorac. Surgery 1996; 62: 1229-31 28 Shroyer AL, Edwards FH, and Grover FL. Updates to the data quality review program: The Society of Thoracic Surgeons Adult Cardiac National Database. Ann. Thorac. Surgery 1998; 65: 1494-7 29 Edwards FH, Grover FL, Shroyer AL, Schwartz M, Bero J. The Society of Thoracic Surgeons National Cardiac Surgery Database: Current risk assessment. Ann. Thorac. Surgery 1997; 63: 903-8 30 Shroyer AL, Grover FL, and Edwards FH. 1995 Coronary artery bypass risk model: The Society of Thoracic Surgeons Adult Cardiac National Database. Ann. Thorac. Surgery 1998; 65: 879-84 31 Edwards FH, Clark RE, Schwartz M. Practical problems in the management of large multi-institutional databases. Ann. Thorac. Surgery 1994; 58: 1841-1844 32 Kennedy JW, Kaiser GC, Fisher LD et al. Multi-variate discriminate analysis of the clinical and angiographic predictors of operative mortality. from CASS J. Thor. Cardiovasc. Surg. 1980; 80: 876 33 Pierpont GL, Kruse M, Ewalds S and Weir EK. Practical problems in assessing risk for coronary artery surgery. J. Thor. Cardiovasc. Surg. 1985; 89: 673-82 34 McCormick JR, Schick EC, McCabe CH, Kronmal RA and Ryan TJ. Determinants of operative mortality and long-term survival in patients with unstable angina. The CASS experience. J Thor Cardiovas. Surg 1985; 89: 683-8 35 Higgins T, Estafanous F, Loop F, Beck G, Blum J and Paranandi L. Stratification of morbidity and mortality outcome by pre-operative risk factors in coronary artery bypass patients. JAMA 1992; 192; 267; 2344-48 36 Nashef SAM, Roques F, Michel P, Guaducheau E, Lemeshow S, Salomon R and The EuroSCORE Study Group (1998). Eurpoean system for cardiac operative risk evaluation (EuroSCORE). Presented to the 12th Annual Meeting of The European Association for Cardio-Thoracic Surgery 37 O’Connor GT, Plume SK, Olmstead EM, et al. Multivariate prediction of in-hospital mortality associated with coronary artery bypass surgery. Circulation 1992; 85: 2110-2118 38 Denvir MA, Lee AJ, Rysdale J, Prescott RJ, Eteiba H, Walker A, Starkey IR and Pell JP. Comparing performance between coronary intervention centres requires detailed case-mix adjusted analysis. Lancet 2004; 26; 177-184. 39 Roques F, Nashef SA, Michel P, Gauducheau E, de Vincentiis C, Baudet E, Cortina J, David M, Faichney A, Gabrielle F, Gams E, Harjula A, Jones MT, Pintor PP, Salamon R and Thulin L. Risk factors and outcome in European cardiac surgery: analysis of the EuroSCORE multinational database of 19,030 patients. Eur. J. Cardiothorac. Surg. 1999; 15: 1: 816-22; discussion 822-3 40 Roques F, Michel P, Goldstone AR, Nashef SA. The logistic EuroSCORE. 2003 Eur Heart J. 24(9): 882-3 41 Hanley JA and McNeil BJ. The meaning and use of the area under a Receiver Operating Characteristic curve. Radiology 1982; 143: 29-36 42 Parry GJ, Gould CR, McCabe CJ, and Tarrow-Mordi WO. Annual league tables of mortality in neonatal intensive care units: longitudinal study. BMJ 1998; 316: 1931-1935 43 Spiegelhalter DJ. Funnel plots for comparing institutional performance. 2004 Submitted.
See www.mrc-bsu.cam.ac.uk/BSUsite/AboutUs/People/davids/funpap.pdf 44 De Leval MR, Francois K, Bull C, Brawn W and Spiegelhalter D. Analysis of a cluster of surgical failures. Application to a series of neonatal arterial switch operations. J. Thor. Cardivasc. Surg. 1994; 107: 914-24 45 Steiner SH, Cook RJ and Treasure T. Monitoring surgical performance using risk adjusted cumulative sum charts. Biostatistics 2001; 2 46 Poloniecki J, Valencia O, Littlejohns P. Cumulative risk adjusted mortality chart for detecting changes in death rate: observational study of heart surgery. BMJ 1998; 316: 1697-1700

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
350
Ref
eren
ces
47 Lovegrove J, Valencia O, Treasure T, Sherlaw-Johnson C, Gallivan S. Monitoring the results of cardiac surgery by variable life adjusted display. Lancet 1997; 350: 1128-30 48 Steiner SH, Cook RJ, Farewell VT and Treasure T. Monitoring surgical performance using risk adjusted cumulative sum charts. Biostatistics 2000; 1: 441-52 49 Spiegelhalter DJ, Grigg O, Kinsman R and Treasure T. Risk adjusted sequential probability ratio tests: applications to Bristol, Shipman and adult cardiac surgery. Quality in Health Care 2003; 15: 7-13 50 Marshall EC and Spiegelhalter DJ. Reliability of league tables of in vitro fertilisation clinics: retrospective analysis of live birth rates. BMJ 1998; 317: 1701-1704 51 Coronary Artery Bypass Surgery in New York State 1992-1996. Albany: New York: New York State Department of Health 1996 52 Christiansen C and Morris C. Improving the statistical approach to healthcare provider profiling. Ann. Int. Med. 1997; 127: 764-768 53 Mohammed MA, Cheng KK, Rouse A, Marshall, T. Bristol, Shipman, and clinical governance: Shewhart's forgotten lessons. Lancet 2001; 357: 463-467 54 Adab P, Rouse A, Mohammed MA, Marshall, T. Performance league tables: the NHS deserves better. BMJ 2002; 324: 95-98 55 Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997; 315: 629-634 56 Stark J, Gallivan S, Lovegrove J, Hamilton JRL, Monro JL, Pollock JCS, Watterson KG. Mortality rates after surgery for congenital heart defects in children and surgeons' performance. Lancet 2000; 355: 1004-1007 57 Christiansen C and Morris C. Improving the ststistical approach to health care provider profiling. Annals Int Med 1997; 127: 764-8 58 Tu J, Sykora K and Naylor C Assessing the outcomes of coronary artery bypass graft surgery: how many risk factors are enough? JACC 1997; 30: 1317-23 59 Spiegelhalter D. Surgical audit: statistical lessons from Nightingale and Codman. J R Statist Soc. 1999; 162 (Part1): 45-58 60 http://www.drfoster.co.uk 61 http://www.nhsdirect.nhs.uk 62 http://www.nhs.uk 63 http://www.bbc.co.uk/health 64 http://www.healthfinder.gov 65 http://www.healthcentre.org.uk 66 http://www.healthinfocus.co.uk 67 http://www.chi.nhs.uk/eng/organisations/london/st_georges/index.shtml 68 http://www.chi.nhs.uk/eng/organisations/london/hammersmith/index.shtml 69 http://www.chi.nhs.uk/eng/report/inv/locum/index.shtml 70 Horton R. Why is Kennedy’s Healthcare Commission damaging NHS care? Lancet 2004; 364; 401-402 71 http://doh.gov.uk/indicat/indicat.htm 72 Aylin P, Alves B, Best N, Cook A, Elliott P, Evans SJW, Lawrence AE, Murray GD, Pollock J, Spiegelhalter D. Comparison of UK paediatric cardiac surgical performance by analysis of routinely collected data 1984-96: was Bristol an outlier? Lancet 2001;358:181-87. 73 Aylin P, Alves B, Cook A, Bennett J, Bottle A, Best N, Catena B, Elliott P. Analysis of Hospital Episode Statistics for the Bristol Royal Infirmary Inquiry. 1999.
Available from: URL: http://www.bristol-inquiry.org.uk/Documents/hes_(Aylin).pdf 74 Poloniecki J, Charalambos S, Bland M, Jones P. Retrospective cohort study of false alarm rates associated with a series of heart operations: the case for hospital mortality monitoring groups. BMJ 2004; 328: 375

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
351
Referen
ces
75 Dixon J, Sanderson C, Elliott P, Walls P, Jones J, Petticrew M. Assessment of the reproducibility of clinical coding in routinely collected hospital activity data: a study of two hospitals. J Pub Health Med 1998; 20 (1) :63-69 76 Public confidence and cardiac surgical outcome (Editorial). Keogh B, Dussek J, Watson D, Magee P and Wheatley D. British Medical Journal 1998; 316 (7147): 1759-20 77 Treasure T, Utley M and Bailey A. Assessment of whether in hospital mortality for lobectomy is a useful standard for the quality of lung cancer surgery: retrospective study. British Medical Journal, 2003; 327: 73-75 78 Marshall M, Sheklle P, Brook R and Leatherman S. Dying to know: Public release of information about quality of healthcare. Nuffield Trust and Rand, 2000 79 Hannan EL, Kilburn H Jr, Racz M, Shields E, Chassin MR. Improving the outcomes of coronary artery bypass surgery in New York State. JAMA 1994; 271: 761-766 80 Hannan EL, Siu AL, Kumar D, Kilburn H Jr, Chassin MR. The decline in coronary artery bypass graft surgery mortality in New York State: the role of surgeon volume. JAMA 1995; 273: 209-213 81 Hannan EL, Kumar D, Racz M, Siu AL, Chassin MR. New York State's Cardiac Surgery Reporting System: four years later. Ann Thorac Surg 1994; 58: 1852-1857 82 Chassin M. R., Hannan E. L., DeBuono B. A. Benefits and Hazards of Reporting Medical Outcomes Publicly. New Eng J Med 1996; 334: 394-398 83 Omoigui N, Annan K, Brown K, Miller D, Cosgrove D, Loop F. Potential explanation for decreased CABG related mortality in New York State: outmigration to Ohio. Circulation 1994; 90: I-93.abstract 84 Eric Schneider and Arnold Epstein. Influence of cardiac surgery performance reports on referral practices and access to care. New Eng J Med 1996; 335: 251-256 85 Is more information better? The effects of report cards on health care providers. National Bureau of Economic Research. Working paper 8697 www.nber.org/papers/w8697 86 Burack J, Impellizzeri P, Homel P and Cunningham J. Public reporting of surgical mortality: a survey of New York State cardiothoracic surgeons. Ann Thorac Surg 199; 68: 1195-1200 87 Schneider E and Epstein A. Use of public performance reports. A survey of patients undergoing cardiac surgery. JAMA 1998; 279: 1638-42 88 Shahian D, Yip W, Westcott G and Johnson J. Selection of a cardiac surgery provider in the managed care era J Thorac Cardiovasc Surg 2000; 120: 978-989 89 Schneider E and Lieberman T. Publicly disclosed information about the quality of healthcare: response of the US public. Quality in Health Care 2001; 10: 96-103 90 Marshall M, Sheklle P, Leatherman S and Brook R.. The public release of performance data. What do we expect to gain? A review of the evidence. JAMA 2000; 283: 1866-1874 91 Hannan E, Radzyner M, Rubin D, Dougherty J and Brennan M. The influence of hospital and surgeon volume on in-hospital mortality for colectomy, gastrectomy and lung lobectomy in patients with cancer Surgery 2002; 131: 6-15 92 B. Keogh. Facts of life the figures can hide. (Viewpoint) The Times, 19 November 2001 93 Khuri SK. Quality, advocacy, healthcare policy and the surgeon. Ann Thorac Surg 2002;74:641-94 94 Albert AA, Walter JA, Arnrich B, Hassanein W, Rosendahl UP, Bauer S, Ennker J. On-line variable live-adjusted displays with internal and external risk adjusted mortalities. A valuable method for benchmarking and early detection of unfavourable trends in cardiac surgery Eur J Cardiothorac Surg 2004; 25: 312-319 95 Chassin MR. Improving the quality of care – Part 3 of 6. N Engl J Med 1996; 335: 1060-1063 96 Bruce Keogh, Personal communication from the Royal College of Anaesthetists, 2002. 97 Department of Health. Coronary Heart Disease Information Strategy. http://www.doh.gov.uk/ipu/strategy/nsf/chdstrat/chdisdoc.htm 98 Chief Executive Bulleting 17th September, 2002. http://www.doh.gov.uk/ipu/ncasp/ncaspadv2.htm 99 Information for IT and the NHS. The National Clinical Audit Support Programme: http://www.doh.gov.uk/ipu/ncasp/index.htm

The Society of Cardiothoracic Surgeons of Great Britain and Ireland National Adult Cardiac Surgical Database Report 2003
352
Ref
eren
ces
100 Sergeant P, Blackstone E and Meyns B. Validation and interdependence with patient-variables of the influence of procedural variables on early and late survival after CABG. K.U. Leuven Coronary Surgery Program. Eur J Cardiothorac Surg 1997, 12, 1-19
101 Fine L, Keogh B, Cretin S, Orlando M and Gould M. How to evaluate and improve the quality and credibility of an outcomes database: validation and feedback study on the UK Cardiac Surgery Experience. British Medical Journal 2003; 326: 25-28 102 Consultants: managing them means measuring them (News focus). Health Service Journal Dec 2002: 10-11 103 Keogh B and Kinsman R. National Adult Cardiac Surgical Database Report 2000-2001 (ISBN 1-903968-04-6) 104 Shahian D, Normand S Torchiana D et al. Cardiac surgery report cards; comprehensive review and statistical critique. Ann Thorac Surg 2001; 72: 2155-2168 105 Lezzoni L. The risks of risk adjustment. JAMA 1997; 278: 1600-1611 106 Fine L, Keogh B, Orlando M, Cretin S and Gould B. Improving the credibility of information on healthcare outcomes. The Nuffield Trust, 2003 107 Speech by Rt Hon Alan Milburn MP, Secretary of State for Health, to the General Medical Council, 20 May 2003