Embed Size (px)
Citation preview

11
Maria Said, HMS 3Gillian Lieberman, MD
The Solitary Pulmonary NoduleThe Solitary Pulmonary Nodule
Maria Said, Harvard Medical School Year IIIGillian Lieberman, MD
Maria Said, Harvard Medical School Year IIIMaria Said, Harvard Medical School Year IIIGillian Lieberman, MDGillian Lieberman, MD
March 2004

22
Maria Said, HMS 3Gillian Lieberman, MD
ObjectivesObjectives
I.I. Present a Patient: discuss normal lung Present a Patient: discuss normal lung anatomy and pathology notedanatomy and pathology noted
II.II. Differential Diagnosis for Small Differential Diagnosis for Small Pulmonary Nodules (Pulmonary Nodules (SPNsSPNs) with some ) with some examples from the BIDMCexamples from the BIDMC
III.III. Assessing Assessing SPNsSPNs and the role of and the role of additional imaging or testsadditional imaging or tests

33
Maria Said, HMS 3Gillian Lieberman, MD
ObjectivesObjectives
I.I. Present a Patient: discuss normal lung Present a Patient: discuss normal lung anatomy and pathology notedanatomy and pathology noted
II.II. Differential Diagnosis for Small Differential Diagnosis for Small Pulmonary Nodules (Pulmonary Nodules (SPNsSPNs) with some ) with some examples from the BIDMCexamples from the BIDMC
III.III. Assessing Assessing SPNsSPNs and the role of and the role of additional imaging or testsadditional imaging or tests

44
Maria Said, HMS 3Gillian Lieberman, MD
Ms. GBMs. GB
HPI: 72 yr old woman with history of recurrent HPI: 72 yr old woman with history of recurrent breast cancer presented with a coughbreast cancer presented with a cough
PMH: Breast cancer PMH: Breast cancer s/ps/p mastectomy 1981mastectomy 1981Recurrence chest in wall 1988Recurrence chest in wall 1988HysterectomyHysterectomyCholestecystectomyCholestecystectomy
Meds: Meds: TamoxifenTamoxifen, , PrevacidPrevacid, Lipitor, Mylanta, Lipitor, MylantaAllergies: codeineAllergies: codeine

55
Maria Said, HMS 3Gillian Lieberman, MD
Mrs. GB’s Chest XMrs. GB’s Chest X--RayRay
PACS, BIDMC
AirwayBonesCardiacDiaphragmEverything elseFieldsGastric BubbleHilum

66
Maria Said, HMS 3Gillian Lieberman, MD
Mrs. GB’s CTMrs. GB’s CT
A CT helps us answer three big questions unanswered by CXRa) Is it solitary?b) What does it really look like?c) Are there abnormal lymph nodes?
PACS, BIDMC

77
Maria Said, HMS 3Gillian Lieberman, MD
Small Pulmonary NodulesSmall Pulmonary Nodules
Single Single radiologicallyradiologically visible lesion that is visible lesion that is less than 3cm and surrounded by lung less than 3cm and surrounded by lung parenchyma. parenchyma. 150,000 new solitary pulmonary nodules 150,000 new solitary pulmonary nodules are discovered every yearare discovered every year1 in 500 chest radiographs will reveal an 1 in 500 chest radiographs will reveal an SPNSPNApproximately 50% of these will be Approximately 50% of these will be malignantmalignant

88
Maria Said, HMS 3Gillian Lieberman, MD
ObjectivesObjectives
I.I. Present a Patient: discuss normal lung Present a Patient: discuss normal lung anatomy and pathology notedanatomy and pathology noted
II.II. Differential Diagnosis for Small Differential Diagnosis for Small Pulmonary Nodules (Pulmonary Nodules (SPNsSPNs) with some ) with some examples from the BIDMCexamples from the BIDMC
III.III. Assessing Assessing SPNsSPNs and the role of and the role of additional imaging or testsadditional imaging or tests

99
Maria Said, HMS 3Gillian Lieberman, MD
The DifferentialThe Differential
VVascularascularIInfectiousnfectiousTTraumaraumaAAutoimmune, Inflammatoryutoimmune, InflammatoryMMetabolicetabolicIIatrogenic, drugsatrogenic, drugsNNeoplasticeoplasticCCongenital, cardiacongenital, cardiac

1010
Maria Said, HMS 3Gillian Lieberman, MD
The DifferentialThe Differential
VV: : ArteriovenousArteriovenous malformation, Infarct, Hematomamalformation, Infarct, HematomaII: : TuberculosisTuberculosis, Fungal, , Fungal, Round PneumoniaRound Pneumonia, Abscess, Dog , Abscess, Dog Heartworm (Heartworm (DirofilariaDirofilaria immitisimmitis))TT: : ----AA: Rheumatoid arthritis, Wegener : Rheumatoid arthritis, Wegener granulomatosisgranulomatosisMM: : ----II: : ----NN: : MalignantMalignant (Primary pulmonary carcinoma, Primary pulmonary (Primary pulmonary carcinoma, Primary pulmonary lymphoma, Primary pulmonary lymphoma, Primary pulmonary carcinoidcarcinoid tumor, Solitary Metastasis tumor, Solitary Metastasis and Benign (and Benign (HamartomaHamartoma, , ChondromaChondroma))CC: Bronchial : Bronchial atresiaatresia, , SequestrationSequestrationOOther: External object, ther: External object, PseudotumorPseudotumor (fluid in fissure), (fluid in fissure), AtelectasisAtelectasis

1111
Maria Said, HMS 3Gillian Lieberman, MD
Patient 1: TBPatient 1: TB
PACS, BIDMC

1212
Maria Said, HMS 3Gillian Lieberman, MD
Patient 2: Round Pneumonia Patient 2: Round Pneumonia
PACS, BIDMC

1313
Maria Said, HMS 3Gillian Lieberman, MD
Patient 3: Multiple nodules on CT Patient 3: Multiple nodules on CT cause unknowncause unknown
PACS, BIDMC

1414
Maria Said, HMS 3Gillian Lieberman, MD
Patient 4: Pulmonary sequestration Patient 4: Pulmonary sequestration
PACS, BIDMC

1515
Maria Said, HMS 3Gillian Lieberman, MD
ObjectivesObjectives
I.I. Present a Patient: discuss normal lung Present a Patient: discuss normal lung anatomy and pathology notedanatomy and pathology noted
II.II. Differential Diagnosis for Small Differential Diagnosis for Small Pulmonary Nodules (Pulmonary Nodules (SPNsSPNs) with some ) with some examples from the BIDMCexamples from the BIDMC
III.III. Assessing Assessing SPNsSPNs and the role of and the role of additional imaging or testsadditional imaging or tests

1616
Maria Said, HMS 3Gillian Lieberman, MD
Assessing Likelihood of MalignancyAssessing Likelihood of Malignancy
1.1. AgeAge2.2. History, underlying risk factorsHistory, underlying risk factors3.3. Size of lesionSize of lesion4.4. Border characteristicsBorder characteristics5.5. Calcification of lesionCalcification of lesion6.6. CavitationCavitation of lesionof lesion7.7. Presence of fat in lesionPresence of fat in lesion8.8. Growth rate of lesionGrowth rate of lesion

1717
Maria Said, HMS 3Gillian Lieberman, MD
1. Age1. Age
In one series, the percentage of In one series, the percentage of solitary nodules due to solitary nodules due to malignancy wasmalignancy was
3% in patients between 353% in patients between 35--393915% between ages 40 and 4915% between ages 40 and 4943% between ages 50 and 5943% between ages 50 and 5950% or higher at age 60 or above50% or higher at age 60 or above
Erasmus JJ, Connolly JE, McAdams HP, Erasmus JJ, Connolly JE, McAdams HP, RoggliRoggli VL. Solitary Pulmonary Nodules: Part I. Morphologic VL. Solitary Pulmonary Nodules: Part I. Morphologic Evaluation for Differentiation of Benign and Malignant Lesions. Evaluation for Differentiation of Benign and Malignant Lesions. RadiographicsRadiographics 2000;20:432000;20:43--58.58.

1818
Maria Said, HMS 3Gillian Lieberman, MD
2. History2. History
SmokingSmokingAsbestosAsbestosPreviously diagnosed Previously diagnosed malignancymalignancyFeverFever
45 year old woman with bladder cancer, nodule was metastasis
Erasmus JJ, Connolly JE, McAdams HP, Erasmus JJ, Connolly JE, McAdams HP, RoggliRoggli VL. Solitary Pulmonary Nodules: Part I. Morphologic VL. Solitary Pulmonary Nodules: Part I. Morphologic Evaluation for Differentiation of Benign and Malignant Lesions. Evaluation for Differentiation of Benign and Malignant Lesions. RadiographicsRadiographics 2000;20:432000;20:43--58.58.

1919
Maria Said, HMS 3Gillian Lieberman, MD
3. Size of lesion3. Size of lesion
The smaller the nodule, the more likely it is The smaller the nodule, the more likely it is to be benign.to be benign.
Caveat: 80% of benign nodules are less Caveat: 80% of benign nodules are less than 2 cm, but 15% of malignant nodules than 2 cm, but 15% of malignant nodules are less than 1 cm.are less than 1 cm.

2020
Maria Said, HMS 3Gillian Lieberman, MD
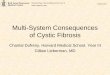
4. Border Characteristics4. Border Characteristics
Non-small cell cancer in a 63 year-old woman
Erasmus JJ, Connolly JE, McAdams HP, Erasmus JJ, Connolly JE, McAdams HP, RoggliRoggli VL. Solitary Pulmonary Nodules: Part I. Morphologic VL. Solitary Pulmonary Nodules: Part I. Morphologic Evaluation for Differentiation of Benign and Malignant Lesions. Evaluation for Differentiation of Benign and Malignant Lesions. RadiographicsRadiographics 2000;20:432000;20:43--58.58.
Benign lesions tend to Benign lesions tend to be smooth and be smooth and discrete. Malignant discrete. Malignant lesions have irregular, lesions have irregular, lobulatedlobulated, or , or spiculatedspiculated borders.borders.
Caveat: 21% malignant Caveat: 21% malignant nodules have well nodules have well defined margins.defined margins.

2121
Maria Said, HMS 3Gillian Lieberman, MD
5. Calcification of Lesion5. Calcification of LesionBenign:Benign:•• Diffuse, homogeneous calcificationDiffuse, homogeneous calcification•• Central calcification (Central calcification (granulomagranuloma))•• Laminated (concentric) calcification (Laminated (concentric) calcification (granulomagranuloma))•• “Popcorn” calcification (“Popcorn” calcification (hamartomahamartoma))Malignant:Malignant:•• EccentricEccentric
•• AmorphousAmorphous
Caveat: 38%Caveat: 38%--63% benign nodules are not calcified63% benign nodules are not calcified

2222
Maria Said, HMS 3Gillian Lieberman, MD
5. Calcification5. Calcification
Chondrohamartoma(popcorn)
Non-small cell cancer(amorphous)
Erasmus JJ, Connolly JE, McAdams HP, Erasmus JJ, Connolly JE, McAdams HP, RoggliRoggli VL. Solitary Pulmonary Nodules: Part I. Morphologic VL. Solitary Pulmonary Nodules: Part I. Morphologic Evaluation for Differentiation of Benign and Malignant Lesions. Evaluation for Differentiation of Benign and Malignant Lesions. RadiographicsRadiographics 2000;20:432000;20:43--58.58.

2323
Maria Said, HMS 3Gillian Lieberman, MD
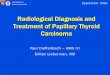
6. 6. CavitationCavitation
Benign Benign cavitarycavitary nodules have smooth, thin nodules have smooth, thin walls (<4mm).walls (<4mm).
Malignant nodules have thick, irregular walls Malignant nodules have thick, irregular walls (>16 mm)(>16 mm)
Caveat: There is a great deal of overlap.Caveat: There is a great deal of overlap.

2424
Maria Said, HMS 3Gillian Lieberman, MD
6. 6. CavitationCavitation
Non-small cell lung cancer in a 61 yr old woman (thick wall)
Aspergillus infection in a 48 yr old man with leukemia (thin wall)
Erasmus JJ, Connolly JE, McAdams HP, Erasmus JJ, Connolly JE, McAdams HP, RoggliRoggli VL. Solitary Pulmonary Nodules: Part I. Morphologic VL. Solitary Pulmonary Nodules: Part I. Morphologic Evaluation for Differentiation of Benign and Malignant Lesions. Evaluation for Differentiation of Benign and Malignant Lesions. RadiographicsRadiographics 2000;20:432000;20:43--58.58.

2525
Maria Said, HMS 3Gillian Lieberman, MD
7. Presence of Fat7. Presence of Fat
The presence of fat The presence of fat (easily assessed on (easily assessed on CT by measuring HU CT by measuring HU units) is a reliable units) is a reliable indicator of a indicator of a hamartomahamartoma..
Erasmus JJ, Connolly JE, McAdams HP, Erasmus JJ, Connolly JE, McAdams HP, RoggliRoggli VL. Solitary Pulmonary Nodules: Part I. VL. Solitary Pulmonary Nodules: Part I. Morphologic Evaluation for Differentiation of Benign and MalignaMorphologic Evaluation for Differentiation of Benign and Malignant Lesions. nt Lesions. RadiographicsRadiographics 2000;20:432000;20:43--58.58.

2626
Maria Said, HMS 3Gillian Lieberman, MD
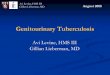
8. Growth Rate8. Growth Rate
Malignant lesions have roughly a doubling time Malignant lesions have roughly a doubling time between approximately a month and a year. between approximately a month and a year. Benign lesions generally have a doubling time Benign lesions generally have a doubling time less than a month and greater than a year.less than a month and greater than a year.
PitfallsPitfalls•• Difficult measuring small lesionsDifficult measuring small lesions•• Doubling refers to volume, not to diameterDoubling refers to volume, not to diameter•• BroncheolalveolarBroncheolalveolar carcinomas and carcinomas and carcinoidcarcinoid
tumors can have DT greater than a year.tumors can have DT greater than a year.

2727
Maria Said, HMS 3Gillian Lieberman, MD
8. Growth Rates8. Growth Rates
Erasmus JJ, McAdams HP, Connolly JE. Solitary Pulmonary Nodules:Erasmus JJ, McAdams HP, Connolly JE. Solitary Pulmonary Nodules: Part II. Evaluation of the Indeterminate Part II. Evaluation of the Indeterminate Nodule. Nodule. RadiographicsRadiographics 2000;20:592000;20:59--66.66.
The upper and lower nodules are growing at the same rate. Because the human eye judges diameter, not volume, the bottom nodule appears to be growing faster.

2828
Maria Said, HMS 3Gillian Lieberman, MD
Further TestingFurther Testing
Radiographic TestingRadiographic TestingCT DensitometryCT DensitometryContrastContrast--Enhanced CT (Enhanced CT (senssens: 95: 95--100%, spec: 70100%, spec: 70--93%)93%)BronchoscopyBronchoscopy ((senssens: 20: 20--80%)80%)PET (lesions with low FDG uptake are typically benign) PET (lesions with low FDG uptake are typically benign) ((senssens: 96.8%, spec: 77.8%): 96.8%, spec: 77.8%)
Invasive TestingInvasive TestingFine needle aspiration (Fine needle aspiration (senssens 8080--95%, spec 5095%, spec 50--88%)88%)ThorascopyThorascopy (video assisted thoracic surgery, or VATS): (video assisted thoracic surgery, or VATS): can be used for diagnosis and excisioncan be used for diagnosis and excisionThoracotomyThoracotomy

2929
Maria Said, HMS 3Gillian Lieberman, MD
How to ProceedHow to Proceed
If probability cancer:If probability cancer:<12% : radiographic follow<12% : radiographic follow--upup
1212--69%: CT and PET scanning69%: CT and PET scanning>69 to 90%: CT followed by either biopsy or surgery>69 to 90%: CT followed by either biopsy or surgery>90%: surgery>90%: surgery
Decision Analysis Model can be used to assess the risk that a nodule is malignant

3030
Maria Said, HMS 3Gillian Lieberman, MD
Mrs. GB’s Pet ScanMrs. GB’s Pet Scan
Courtesy of J. Anthony Parker, MD, PhD

3131
Maria Said, HMS 3Gillian Lieberman, MD
Ms. GB’s Pet ScanMs. GB’s Pet Scan
Courtesy of J. Anthony Parker, MD, PhD

3232
Maria Said, HMS 3Gillian Lieberman, MD
Ms. GB’s Pet ScanMs. GB’s Pet Scan
Courtesy of J. Anthony Parker, MD, PhD

3333
Maria Said, HMS 3Gillian Lieberman, MD
ObjectivesObjectives
I.I. Presented Patient Ms. GB Presented Patient Ms. GB –– nodule nodule found on CXR, followed up by CT and found on CXR, followed up by CT and PETPET
II.II. Explored differential diagnoses include Explored differential diagnoses include infection and other benign causes as infection and other benign causes as well as malignancywell as malignancy
III.III. Discussed assessment of Discussed assessment of SPNsSPNs using using nodule characteristics and additional nodule characteristics and additional radiographic techniquesradiographic techniques

3434
Maria Said, HMS 3Gillian Lieberman, MD
ReferencesReferences
Erasmus JJ, Connolly JE, McAdams HP, Erasmus JJ, Connolly JE, McAdams HP, RoggliRoggli VL. Solitary Pulmonary Nodules: Part I. Morphologic VL. Solitary Pulmonary Nodules: Part I. Morphologic Evaluation for Differentiation of Benign and Malignant Lesions. Evaluation for Differentiation of Benign and Malignant Lesions. RadiographicsRadiographics 2000;20:432000;20:43--58.58.
Erasmus JJ, McAdams HP, Connolly JE. Solitary Pulmonary Nodules:Erasmus JJ, McAdams HP, Connolly JE. Solitary Pulmonary Nodules: Part II. Evaluation of the Part II. Evaluation of the Indeterminate Nodule. Indeterminate Nodule. RadiographicsRadiographics 2000;20:592000;20:59--66.66.
OstOst D, Fein AM, D, Fein AM, FeinsilverFeinsilver SH. The Solitary Pulmonary Nodules. N SH. The Solitary Pulmonary Nodules. N EnglEngl J Med 2003;348(25): 2535J Med 2003;348(25): 2535-- 2542.2542.
Shaffer K. Role of Radiology for Imaging and Biopsy of Solitary Shaffer K. Role of Radiology for Imaging and Biopsy of Solitary Pulmonary Nodules. Chest Pulmonary Nodules. Chest 1999;116(6):519S1999;116(6):519S--522S.522S.
SwensenSwensen SJ, Silverstein MD, SJ, Silverstein MD, EdellEdell ES, et al. Solitary pulmonary nodules: clinical prediction modeES, et al. Solitary pulmonary nodules: clinical prediction model l versus physicians. Mayo versus physicians. Mayo ClinClin Proc 1999;74:319Proc 1999;74:319--29.29.
SwensenSwensen SJ, Silverstein MD, SJ, Silverstein MD, IlstrupIlstrup DM, DM, SchleckSchleck CD, CD, EdellEdell ES. The probability of malignancy in solitary ES. The probability of malignancy in solitary pulmonary nodules: application to small pulmonary nodules: application to small radiologicallyradiologically indeterminate nodules. Arch Intern Med indeterminate nodules. Arch Intern Med 1997; 157: 8491997; 157: 849--55.55.
Weinberger SE. Differential diagnosis and evaluation of the soliWeinberger SE. Differential diagnosis and evaluation of the solitary pulmonary nodules. Up to Date. tary pulmonary nodules. Up to Date. http://individual.uptodateonline.com/application/topic/print.asphttp://individual.uptodateonline.com/application/topic/print.asp?file?file=misclung/23359&type==misclung/23359&type=A&selA&sel ectedTitleectedTitle=1~9.=1~9.
YankelevitzYankelevitz DF, DF, HenschkeHenschke CI. Lung Cancer: Small Solitary Pulmonary Nodules. Radiologic CCI. Lung Cancer: Small Solitary Pulmonary Nodules. Radiologic Clinics of linics of North America 2000;38(3):471North America 2000;38(3):471--78.78.

3535
Maria Said, HMS 3Gillian Lieberman, MD
AcknowledgmentsAcknowledgments
Special thanks to:Special thanks to:•• J. Anthony Parker, MD, PhDJ. Anthony Parker, MD, PhD•• Joseph Barry, MDJoseph Barry, MD•• Phillip Phillip BoiselleBoiselle, MD, MD•• Larry Barbaras Larry Barbaras •• Gillian Lieberman, MD Gillian Lieberman, MD •• Pamela Pamela LepkowskiLepkowskifor their help and support.for their help and support.