Embed Size (px)
Citation preview

The Thyroid NoduleThe Thyroid Nodule
郝 立 智 醫 師郝 立 智 醫 師永康榮民醫院新陳代謝科永康榮民醫院新陳代謝科
N Engl J Med 2004; 351:1764-1771, Oct 21, 2004.
Laszlo Hegedüs, M.D. Department of Endocrinology and Metabolism, Odense University Hospital, DK-5000 Odense,
Denmark.

HLJ
Outline• Case Presentation• The Clinical Problem • Strategies and Evidence • History and Physical Examination • Laboratory Investigations • Imaging of the Thyroid Nodule Radionuclide Scanning SONO Other Methods • Fine-Needle Aspiration Biopsy • Tx of the Solitary Thyroid Nodule Levothyroxine Surgery Radioiodine Percutaneous Ethanol Injection • Areas of Uncertainty • Guidelines from Professional Societies • Conclusions and Recommendations

HLJ
Case Presentation• A 42-year-old woman presents with a palpable mass
on the left side of her neck. She has no neck pain and no symptoms of thyroid dysfunction.
• Physical examination reveals a solitary, mobile thyroid nodule, 2 cm by 3 cm, without lymphadenopathy.
• The p't has no family history of thyroid disease and no history of external irradiation.
• Which investigations should be performed?• Assuming that the nodule is benign, which, if any,
Tx should be recommended?

HLJ
The Clinical Problem (1) • In the United States, 4 to 7 % of the adult population have a
palpable thyroid nodule. However, only 1 of 20 clinically identified nodules is malignant.
• This corresponds to 2 to 4 per 100,000 people per year, constituting only 1 % of all cancers and 0.5 % of all cancer deaths.
• Nodules are more common in women and increase in frequency with age and with decreasing iodine intake.
• The prevalence is much greater with the inclusion of nodules that are detected by SONO or at autopsy.
• By the latter assessment, 50 % of 60-year-old persons have thyroid nodules.

HLJ
The Clinical Problem (2)• The clinical spectrum ranges from the incidental,
asymptomatic, small, solitary nodule, in which the exclusion of cancer is the major concern, to the large, partly intrathoracic nodule that causes pressure symptoms, for which Tx is warranted regardless of cause.
• The most common diagnoses and their approximate distributions are colloid nodules, cysts, and thyroiditis (in 80 % of cases); benign follicular neoplasms (in 10 to 15 %); and thyroid carcinoma (in 5 %).

HLJ
The Clinical Problem (3)
• Management of a solitary thyroid nodule remains controversial.
• This review will focus on the management of a solitary thyroid nodule that is detected on physical examination, regardless of the finding of additional nodules by radionuclide scanning or SONO, since such a finding does not alter the risk of cancer.

HLJ
Strategies and Evidence History and Physical Examination (1)
• The history and physical examination remain the diagnostic cornerstones in evaluating the p't with a thyroid nodule and may be suggestive of thyroid carcinoma (Table 1).
• However, a minority of p'ts with malignant nodules have suggestive findings, which often also occur in benign thyroid disorders.
• There is also substantial variation among practitioners in evaluating nodules, a finding that may explain why an increasing number of thyroid specialists use imaging as part of the evaluation.

HLJ

HLJ
Strategies and Evidence History and Physical Examination (2)
• The risk of thyroid cancer seems nearly as high in incidental nodules (<10 mm), the majority of which escape detection by palpation, as in larger nodules.
• The vast majority of these microcarcinomas do not grow during long-term follow-up and do not cause clinically significant thyroid cancer. The fact that SONO detects nodules (a third of which are more than 20 mm in diameter) in up to 50 % of p'ts with a normal neck examination underscores the low specificity and sensitivity of clinical examination.
• When two or more risk factors that indicate a high clinical suspicion, the likelihood of cancer approaches 100 %.
• In such cases, biopsy is still useful to guide the type of surgery (Figure 1).

HLJ
Figure 1. Algorithm for the Cost-Effective Evaluation and Tx
of a Clinically Detectable Solitary Thyroid Nodule. • In the case of a strong clinical suspicion of cancer, surgery is
recommended, regardless of the results of fine-needle aspiration biopsy (FNAB). In the case of a suppressed serum thyrotropin, thyroid scintigraphy should be performed, since a functioning nodule almost invariably rules out cancer.
• In the case of a nondiagnostic FNAB, a repeated biopsy yields a satisfactory aspirate in 50 % of cases.
• If SONO reveals additional nodules that are more than 10 mm in diameter, FNAB could be performed on one other nodule, in addition to the one that is clinically detectable. The therapeutic options shown cover both solid and cystic nodules.
• In the case of a recurrent cyst, the possibilities of Tx are repeated FNAB, surgery, and ethanol injection. I do not recommend levothyroxine therapy for the thyroid nodule.

HLJ

HLJ

HLJ
Laboratory Investigations (1) • Because clinical examination is not sensitive for identifying thyroid
dysfunction, laboratory evaluation of thyroid function is routinely warranted.• The only biochemical test routinely needed is serum thyrotropin level. If this
level is subnormal, free thyroxine or free triiodothyronine should be measured to document the presence and degree of hyperthyroidism.
• 10 % of p'ts with a solitary nodule have a suppressed level of serum thyrotropin, which suggests a benign hyperfunctioning nodule.
• If the serum thyrotropin is elevated, a serum antithyroperoxidase Ab should be obtained to confirm Hashimoto's thyroiditis.
• However, the finding of an elevated level does not obviate the need for a FNAB, since the practitioner must rule out a coexisting cancer, including lymphoma, which accounts for only 5 % of thyroid cancers but is associated with Hashimoto's thyroiditis.
• Nearly all p'ts with thyroid cancer are euthyroid.

HLJ
Laboratory Investigations (2)• If a p't has a family history of medullary thyroid cancer or
multiple endocrine neoplasia type 2, a basal serum calcitonin should be obtained; an elevated level suggests medullary thyroid cancer.
• Before surgery is performed, investigation for primary hyperparathyroidism and pheochromocytoma should be carried out.
• Serum calcitonin is not routinely measured in p'ts who have no suggestive family history, since medullary carcinoma is present in only about 1 of 250 p'ts with a thyroid nodule.

HLJ
Imaging of the Thyroid Nodule Radionuclide Scanning (1)
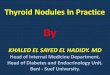
• Radionuclide scanning, which is performed much more commonly in Europe than in the United States, may be used to identify whether a nodule is functioning (Figure 2).
• A functioning nodule, with or without suppression of extranodular uptake, is nearly always benign, whereas a nonfunctioning nodule, constituting approximately 90 % of nodules, has a 5 % risk of being malignant.
• Thus, in the p't with a suppressed level of serum thyrotropin, radionuclide confirmation of a functioning nodule may obviate the need for biopsy.

HLJ
Imaging of the Thyroid Nodule Radionuclide Scanning (2)
• A scan can also indicate whether a clinically solitary nodule is a dominant nodule in an otherwise multinodular gland and can reveal substernal extension of the thyroid.
• A scan can be performed with iodine-123, iodine-131, or technetium-99m–labeled pertechnetate.
• Iodine isotopes, which are both trapped and bound organically in the thyroid, are preferred, since 3 to 8 % of nodules that appear functioning on pertechnetate scanning may appear nonfunctioning on radioiodine scanning, and a few of those nodules may be thyroid cancers.
• A scan cannot be used to measure the size of a nodule accurately.

HLJ
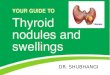
Figure 2. Scintigram of a Solitary Functioning Nodule in the Right Thyroid Lobe.
• Scintigraphy that was performed with the use of technetium-99m–labeled pertechnetate shows suppression of extranodular uptake in thyroid tissue.

HLJHegedus, L. N Engl J Med 2004;351:1764-1771
Scintigram of a Solitary Functioning Nodule in the Right Thyroid Lobe

HLJ
Imaging of the Thyroid Nodule SONO (1)
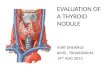
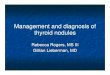
• SONO can accurately detect nonpalpable nodules, estimate the size of the nodule and the volume of the goiter, and differentiate simple cysts, which have a low risk of being malignant, from solid nodules or from mixed cystic and solid nodules, which have a 5 % risk of being malignant (Figure 3).
• SONO also provides guidance for diagnostic procedures (e.g., fine-needle aspiration biopsy) as well as therapeutic procedures (e.g., cyst aspiration, ethanol injection, or laser therapy) and facilitates the monitoring of the effects of Tx.

HLJ
Imaging of the Thyroid Nodule SONO (2)
• In one study, among p'ts who had been referred for evaluation of a palpable thyroid abnormality, SONO altered the clinical management in two thirds of cases, mainly by identifying nodules that were smaller than 1 cm (which were not considered to require further evaluation) in 20 % of the p'ts and by discovering additional nodules (which required biopsy) in 24 % of the p'ts.
• Characteristics revealed by SONO — such as hypoechogenicity, microcalcifications, irregular margins, increased nodular flow visualized by Doppler, and, especially, the evidence of invasion or regional lymphadenopathy — are associated with an increased risk of cancer
• SONO findings cannot reliably distinguish between benign and cancerous lesions.

HLJHegedus, L. N Engl J Med 2004;351:1764-1771
Cross-Sectional Ultrasonogram Showing a Solid, Hypoechoic Nodule (Dark Gray) in the Right Thyroid Lobe

HLJ
Other Methods • CT and MRI also cannot reliably differentiate between
malignant and benign nodules. These tests are rarely indicated in the evaluation of a nodule.
• An exception is in the diagnosis and evaluation of substernal goiters, since these imaging techniques can assess the extent of the goiter more precisely than can other techniques and can evaluate tracheal compression.
• Evaluation of glucose metabolism by positron-emission tomography using fludeoxyglucose (fluorodeoxyglucose) F 18 may help in distinguishing benign from malignant nodules, but its use is limited by cost and accessibility and it cannot replace biopsy.

HLJ
Prevalence and Risk of Cancer of Focal Thyroid Incidentaloma Identified by 18F-Fluorodeoxyglucose Positron Emission Tomography for Metastasis
Evaluation and Cancer Screening in Healthy Subjects • We performed a retrospective review of 18F-fluorodeoxyglucose
positron emission tomography (FDG-PET) examination to determine the prevalence of thyroid FDG-PET incidentaloma in a p't group evaluated for metastasis of cancer and in a group of healthy subjects who underwent voluntary cancer screening.
• We also evaluated the risk of malignancy in focal thyroid FDG-PET incidentaloma and its association with standard uptake values (SUVs) (maximum and greater than 0.75 threshold).
• A total of 1330 subjects underwent FDG-PET for metastasis evaluation (n = 999) and cancer screening (n = 331). Twenty-nine of 1330 subjects (2.2%) showed focal (n = 21) or diffuse (n = 8) thyroid FDG-PET incidentaloma.
J Clin Endocrinol Metab 2003;88:4100-4104.

HLJ
• No significant difference in the prevalence of thyroid FDG-PET incidentaloma between the two groups (19 of 999 vs. 10 of 331; P > 0.05). Four of 15 focal incidentalomas (26.7%) whose histological diagnoses were available showed papillary thyroid cancer. The maximum SUV (16.5 ± 4.70) and greater than 0.75 threshold SUV (14.2 ± 5.3) of malignant lesions were significantly higher than those of benign tumors (6.5 ± 3.8 and 4.9 ± 3.0; P < 0.05).
• In conclusion, thyroid FDG-PET incidentaloma has prevalence of 2.2%, and its prevalence was not different according to the purpose of the FDG-PET.
• The focal thyroid FDG-PET incidentaloma carries a high risk of malignancy, especially in cases with high SUVs.
• Therefore, focal thyroid FDG-PET incidentaloma with high SUVs warrants a pathological diagnostic procedure if it changes a p't’s Tx plan or prognosis.
J Clin Endocrinol Metab 2003;88:4100-4104.

HLJ
Fine-Needle Aspiration Biopsy (1)
• Independent of morphology, FNA provides the most direct and specific information about a thyroid nodule.
• It is performed on an outp't basis, is relatively inexpensive, and is easy to learn.
• Complications are rare and primarily involve local discomfort.• The use of anticoagulants or salicylates does not preclude biopsy. • In centers with experience in FNA, the use of this technique has
been estimated to reduce the number of thyroidectomies by 50 %, to roughly double the surgical confirmation of carcinoma, and to reduce the overall cost of medical care by 25 %, as compared with surgery performed on the basis of clinical findings alone.

HLJ
Fine-Needle Aspiration Biopsy (2)• FNA has diagnostically useful results in about 80 % of cases,
typically with two to four passes of the needle.• The number of cases in which sufficient samples are obtained
increases if aspiration is guided by SONO, especially in nodules that are partly cystic, and repeated biopsy reduces by half the rate of insufficient samples (to about 10 %).
• The diagnostic accuracy of FNA depends on the way in which suspicious lesions are handled. Viewing them as "positive" increases sensitivity (rate of false negative results, 1 %), but decreases specificity.
• If FNA reveals a follicular neoplasm (which occurs in 15 % of nodules, of which only 20 % turn out to be malignant), radionuclide scanning should be performed.

HLJ
Fine-Needle Aspiration Biopsy (3)• If such scanning shows a functioning nodule with or without
complete suppression of the rest of the thyroid, surgery can be avoided, since the risk of cancer is negligible.
• In a cystic lesion or one that is a mixture of cystic and solid components, FNA of a possible solid component should be performed, since the risk of cancer is the same as that for a solid nonfunctioning nodule.
• With the exception of calcitonin immunostaining for medullary carcinoma, there are no reliable immunohistologic or molecular tests for distinguishing between benign and malignant nodules.

HLJ

HLJ
Tx of the Solitary Thyroid Nodule• The natural history of solitary thyroid nodules is poorly understood,
mainly because nodules that are suspicious for cancer, cause pressure, or prompt reports of cosmetic problems are rarely left untreated.
• With this reservation, it seems that the majority of benign nonfunctioning nodules grow, particularly those that are solid.
• In one study, 89 % of nodules that were followed for five years increased by 15 % or more in volume. The annual rate of evolution of a solitary functioning nodule into a hyperfunctioning nodule is as high as 6 %; the risk is positively related to the size of the nodule and negatively related to the serum thyrotropin level.
• Table 2 summarizes the advantages and disadvantages of potential Tx options.
• Figure 1 shows a management algorithm.

HLJ

HLJ
Levothyroxine (1)• Tx with levothyroxine at a dose sufficient to keep the serum
thyrotropin below 0.3 mU/l has been suggested as a way to prevent growth of an apparently benign nodule. However, this approach has clear limitations.
• A recent meta-analysis showed no significant difference in the size of nodules after 6 to 12 months of suppressive therapy with levothyroxine, as compared with no Tx, although the size of the nodules decreased by more than 50 % in a larger proportion of levothyroxine-treated p'ts than in p'ts who had no Tx.
• The likelihood of such shrinkage is greater when serum thyrotropin is suppressed to below 0.1 mU/l than it is when the level is below 0.3 mU.

HLJ
Levothyroxine (2)• In a five-year, randomized trial, suppression to below 0.1 mU/l
significantly reduced the frequency with which new nodules developed (i.e., 8 % of p'ts who were treated with levothyroxine as compared with 29 % of untreated p'ts).
• However, therapy with levothyroxine to reduce thyrotropin below 0.1 mU/l is associated with an increased risk of atrial fibrillation, other cardiac abnormalities, and reduced bone density.
• Regrowth of nodules occurs after cessation of therapy.• Levothyroxine has no effect on the recurrence of thyroid cysts
after aspiration.

HLJ
Surgery • The main indications for surgery are clinical or cytologic features
suggestive of cancer or symptoms due to the nodule (Table 1). • If preoperative cytology suggests a benign lesion,
hemithyroidectomy is generally preferred. • Postoperative administration of levothyroxine is indicated only in
cases of hypothyroidism. • When surgery is performed by a specialist, the incidence of
complications is low (i.e., postoperative hypoparathyroidism in 1 % of cases and injuries to the recurrent laryngeal nerve in about 1 %), but the complication rate is higher for less experienced surgeons and those without special training.

HLJ
Radioiodine (1)• Radioiodine is an option for Tx of a functioning nodule,
with or without biochemical hyperthyroidism. • It is contraindicated in pregnant and breast-feeding women. • Normalization of the results of thyroid radionuclide
scanning and the serum thyrotropin level (often referred to as a "cure") is achieved in 75 % of p'ts, and thyroid volume is reduced 40 %, after a single dose of iodine-131 aiming at a level of 100 Gy, independent of pretreatment thyroid function.

HLJ
Radioiodine (2)• Main side effect is hypothyroidism, which occurs in 10 % of p'ts
within five years after Tx and increases in frequency over time. • This risk is unrelated to dose but is greater in p'ts with thyroid
peroxidase antibodies and with iodine uptake in extranodular thyroid tissue.
• Most nodules do not disappear after radioiodine therapy but may become harder on palpation and may reveal unusual cytologic features as a result of irradiation.
• Thyroid function should be checked regularly during the first year and yearly thereafter in order to detect hypothyroidism.
• Nodules are unlikely to grow after radioiodine therapy, but if growth occurs, a biopsy may be warranted.

HLJ

HLJ
Percutaneous Ethanol Injection (1)• A number of studies have suggested a benefit of SONO guided
ethanol injection in the Tx of benign functioning and nonfunctioning solid thyroid nodules as well as cystic nodules.
• The mechanism of effect involves coagulative necrosis and small-vessel thrombosis.
• The procedure requires prior documentation of benign cytology, skill, and experience; drawbacks include local pain and a potential risk of serious side effects (Table 2).
• There are few data from controlled trials to support this approach.

HLJ
Tx of solitary autonomous thyroid nodules by percutaneous ethanol injection (PEI): results of an Italian multicenter
study. The Multicenter Study Group
• PEI has been proposed for the therapy of autonomously functioning thyroid nodules. In 1992, an Italian multicenter study was undertaken to confirm the usefulness and the feasibility of this procedure.
• The study included 429 p'ts: 242 (56.4%) were affected by a toxic adenoma (TA) and 187 (43.5%) by pretoxic adenoma (PTA).
• FT4, FT3 and TSH were measured before and 3, 6, 12 months after the end of tx; thyroid ultrasound and thyroid scintiscan were performed in the majority of p'ts before and after tx.
J Clin Endocrinol Metab 1996;81:3261-3264.

HLJ
• P'ts underwent 2-12 sessions of PEI under sonographic guidance (median 4). The total amount of ethanol administered per p't (1.5 mL/mL nodular volume) was 2-50 mL (mean +/- SD, 17 +/- 9 mL), and the amount per each injection was 1-8 mL (3.2 +/- 1.3 mL).
• Tx was judged successful when both TSH and free thyroid hormone returned within the normal range and recovery of tracer uptake in extranodular tissue was observed at scintiscan, at any time during the follow-up period.
• Tx was considered unsuccessful when no change was observed at scintiscan and/or serum TSH remained less than 0.4 mU/L.
• A successful tx was achieved in 66.5% TA and in 83.4% PTA, when assessed after a 12-month follow-up. In all cases a reduction of the nodular size was observed. Almost all positive results were obtained in nodules whose initial volume was less than 15 mL; large nodules responded less favorably.

HLJ
• Tx was generally well tolerated, only transient side-effects, mainly local pain at the time of injection, were observed.
• Once normalization of scintigraphic image and of FT4, FT3 and TSH was achieved, no recurrence of hyperthyroidism nor development of hypothyroidism were observed for the length of the study.
• In conclusion, PEI for tx of autonomously functioning thyroid nodules is effective and safe. Better results are obtained in p'ts with PTA than TA, particularly when the initial volume of the nodule is less than or equal to 15 mL.
• PEI may be considered as an alternative to surgery and to radioiodine for Tx of autonomously functioning thyroid nodules.
J Clin Endocrinol Metab 1996;81:3261-3264.

HLJ
Percutaneous Ethanol Injection (2)• Available data suggest that multiple injections of ethanol (a median
of four) can achieve a complete cure (i.e., a normalization of results of radionuclide scanning and serum thyrotropin measures) in two thirds of p'ts with hyperfunctioning nodules and three quarters of p'ts with functioning nodules without hyperthyroidism.
• In solid nonfunctioning nodules that are solitary and cytologically benign, a single ethanol injection has been shown to reduce the volume of nodules by 50 %. Additional ethanol injections have only a limited effect.
• Recently, data from a preliminary study suggested that the use of laser photocoagulation may be as effective as ethanol injection, with fewer adverse effects. However, controlled trials are needed.

HLJ
Effect of ultrasound-guided interstitial laser photocoagulation on
benign solitary solid cold thyroid nodules – a randomised study • Aim: To evaluate the efficacy of US-guided interstitial laser photocoagulation
(ILP) on thyroid function, nodule size and p't satisfaction in benign solitary solid cold thyroid nodules by comparing one ILP session with no tx in a prospective randomised study.
• Materials and methods: Thirty euthyroid outp'ts with a benign solitary solid and a scintigraphically cold thyroid nodule causing local discomfort were assigned to one session of ILP (n = 15) or observation (n = 15) and followed for 6 months. Thyroid nodule volume and total thyroid volume were assessed by US and thyroid function was determined by routine assays before and during follow-up. Pressure and cosmetic complaints before and at 6 months were evaluated on a visual analogue scale. ILP was performed under US guidance and with an output power of 2.5–3.5 W.
European Journal of Endocrinology, 2005-3, Vol 152, Issue 3, 341-345

HLJ
• Results: In the ILP group, the nodule volume decreased from 8.2 ml (6.1; 11.9) (median; quartiles) to 4.8 ml (3.0; 6.6) after 6 months (P = 0.001). The overall median reduction was 44% (37; 52), which correlated with a significant decrease in pressure symptoms as well as cosmetic complaints. In the control group, a non-significant increase in median nodule volume of 7% (0; 34) after 6 months was seen. No major side-effects were seen in the ILP group. There was no correlation between thermal energy deposition and nodule volume reduction. Thyroid function was unaltered throughout.
• Conclusion: US-guided ILP, given as a single tx, resulted in a satisfactory clinical response in the majority of p'ts with a benign solitary solid cold thyroid nodule, and may become a clinically relevant alternative to surgery in selected p'ts.
European Journal of Endocrinology, 2005-3,Vol 152, Issue 3, 341-345

HLJ
Percutaneous Ethanol Injection (3)• In thyroid cysts, the recurrence rate after aspiration is high.• Tetracycline, a sclerosing agent, had no effect in a
randomized study. • Uncontrolled studies have suggested that ethanol injection
may prevent the recurrence of cysts. • A recent randomized, double-blind study involving a six-
month follow-up period reported that 21 of 33 p'ts (64 %) who were treated with ethanol were cured after one session, as compared with 6 of 33 p'ts (18 %) who were treated with saline.

HLJ
Tetracycline for sclerosis of thyroid cysts. A randomized study • In a prospective study, 53 consecutive p'ts with solitary thyroid cysts were
randomized to ultrasonically guided cyst aspiration and subsequent flushing with isotonic saline (n = 30) or tetracycline hydrochloride (n = 23).
• The p'ts were followed up clinically and ultrasonically 1, 3, 6, and 12 months after Tx. If the cyst recurred, a repeated Tx was offered. Cure was defined as the absence of any residual nodule and an ultrasonic cyst volume of less than 1 mL 12 months after the last Tx.
• During follow-up, two p'ts without recurrence after saline tx and six p'ts without recurrence after tetracycline tx developed solid cold nodules.
• Fourteen (47%) of 30 p'ts in the saline group and ten (43%) of 23 p'ts in the tetracycline group were cured (not statistically significant).
• Tetracycline does not seem to offer any advantage over isotonic saline in the tx of thyroid cysts, and some of these p'ts still need thyroid surgery.
Arch Intern Med 1988;148:1116-1118.

HLJ
Tx of Recurrent Thyroid Cysts with Ethanol: A Randomized Double-Blind Controlled Trial
• Thyroid nodules are prevalent; when evaluated by SONO (US), 15–25% of solitary thyroid nodules are cystic or predominantly cystic, and most are benign. Simple aspiration is the tx of choice, but the recurrence rate is 10–80% depending on the number of aspirations and the cyst volume.
• The aim of this study was to evaluate the effect on recurrence rate of benign recurrent thyroid cysts in a double-blind randomized study comparing ethanol instillation with instillation of isotonic saline and subsequent complete emptying.
• Sixty-six consecutive p'ts with recurrent and benign (based on US-guided biopsy) thyroid cysts ( 2 ml) were randomly assigned to either subtotal cyst aspiration, flushing with 99% ethanol, and subsequent complete fluid aspiration (n = 33), or to subtotal cyst aspiration, flushing with isotonic saline, and subsequent complete fluid aspiration (n = 33).
J Clin Endocrinol Metab 2003;88:5773-5777.

HLJ
• In case of recurrence (defined as cyst volume >1 ml) at the monthly evaluations, the tx was repeated but limited to a maximum of three txs.
• Procedures were US-guided, and p'ts were followed for 6 months. Age, sex, number of previous aspirations, pretreatment cyst volume, and serum TSH did not differ in the two groups.
• Cure (defined as a cyst volume 1 ml at the end of follow-up) was obtained in 27 of 33 [82%; confidence interval (CI), 65–93] p'ts treated with ethanol and in 16 of 33 (48%; CI, 31–66) p'ts treated with saline (P = 0.006).

HLJ
• In the ethanol group, 21 of 33 (64%) p'ts were cured after one session only, compared with six of 33 (18%) in the saline group (P = 0.002). The number of previous aspirations (P = 0.005) and baseline cyst volume (P = 0.005) had influence on outcome, i.e. the chance of success decreased with the number of previous aspirations and with increasing cyst volume.
• Seven p'ts (21%) treated with ethanol had moderate to severe pain (median duration, 5 min; CI, 2–10), and one had transient dysphonia. Indirect laryngoscopy was performed before and after the last session and was normal in all p'ts.
• We concluded that tx of recurrent thyroid cysts with ethanol is superior to simple aspiration and flushing with saline and devoid of serious side effects.
• Our study demonstrates that flushing with ethanol is a clinically significant nonsurgical alternative for thyroid cysts that recur despite repeat aspirations.
J Clin Endocrinol Metab 2003;88:5773-5777.

HLJ

HLJ
Areas of Uncertainty • There are no data from studies comparing the outcome
and cost-effectiveness of various strategies of evaluating a nodule (e.g., using radionuclide imaging and ultrasonographic guidance for fine-needle aspiration).
• There are also insufficient data comparing the outcome (including quality of life) of various management approaches in the absence of cancer.

HLJ
Guidelines from Professional Societies (1)
• Clinical-practice guidelines were published in 1996 by the American Thyroid Association (www.thyroid.org/professionals/publications/guidelines.html) and American Association of Clinical Endocrinologists (www.aace.com/clin/guidelines/thyroid_nodules.pdf).
• The recommendations of both organizations correspond with those provided here.
• Radionuclide scanning is not routinely recommended, but it is advocated in the case of a suppressed serum thyrotropin or the finding of follicular neoplasia by FNA.

HLJ

HLJ

HLJ
Guidelines from Professional Societies (2)• Thyroid SONO is recommended to guide FNA, especially in
nodules that are small and incidental or are partly cystic or from which primary FNA has yielded insufficient material.
• FNAB of all possibly malignant nodules (which are not defined in the guidelines) is advocated.
• If the cytology is benign, repeated biopsy is seldom indicated.• In the case of a benign nodule, periodic lifelong follow-up every
6 to 24 months (including measurement of serum thyrotropin levels, neck palpation, and FNA in case of growth or other suspicious signs) is recommended.

HLJ
Guidelines from Professional Societies (3)• For a functioning benign nodule, iodine-131 is considered the tx of
choice, with surgery as an alternative, especially if the nodule is very large or partly cystic or if the p't is young;
• Tx is more strongly recommended if the serum thyrotropin is decreased or overt hyperthyroidism is present, because of adverse effects on bone and CV system.
• For a nonfunctional benign nodule, no clear recommendation on the use of levothyroxine, although this therapy is considered contraindicated when the serum thyrotropin is suppressed, in p'ts more than 60 years old, and in postmenopausal women.
• If levothyroxine therapy is used, regular reassessment (the interval is not defined in the guidelines) is recommended, with monitoring of serum thyrotropin, which should be subnormal but measurable.
• The guidelines do not address ethanol injection and laser therapy.

HLJ
Conclusions and Recommendations (1)• For the p't who presents with a nodule, as in the case described in
the vignette, the main concern is to exclude the possibility of thyroid cancer, even though the vast majority of nodules are benign (Figure 1).
• Initial evaluation include measurement of the serum thyrotropin and a FNA, preferably guided by SONO.
• If the p't has a family history of medullary thyroid carcinoma or MEN type 2, the serum calcitonin should also be checked.
• If the thyrotropin is suppressed, radionuclide scanning should be performed.
• In p'ts less than 20 years old, and in the case of a high clinical suspicion for cancer (e.g., follicular neoplasia as diagnosed by FNA and a nonfunctioning nodule revealed on scanning), offer hemithyroidectomy regardless of the results of FNA.

HLJ
Conclusions and Recommendations (2)• In the case of a functioning benign nodule, iodine-131 is generally
the therapy of choice, independent of concomitant hyperthyroidism.
• For nonfunctioning cystic nodules, aspiration and ethanol injection therapy may be considered, and ethanol injection or laser therapy if the nodules are solid, but data to support the use of these therapies are limited.
• My usual approach after documenting benign cytology is to follow the p't yearly with neck palpation and measurement of the serum thyrotropin, with repeated SONO and FNA if evidence of growth.
• I do not recommend levothyroxine therapy to shrink or prevent growth of benign nodules because of the drug's low efficacy and potential side effects.

HLJ