Embed Size (px)
DESCRIPTION
Part 2 of 3 ||11.20.09 || NeuroSci2 lecture: Regional Neurobiology ||Lecturer: Dr. Tan (?)
Citation preview

THE VENTRICLES, CHOROID PLEXUS, & CEREBROSPINAL
FLUID

DEVELOPMENT
• 3RD WOG – neural canal & central canal• 24 – 26 days closure of the anterior (rostral) &
posterior (caudal) neuropores, respectively• Neural tube lined by differentiating
neuroepithelial cells undergoing cell division that give rise to the ependymal cells lining the mature ventricular system & central canal

5 WEEKS OF GESTATION 6 WEEKS OF GESTATION8.5 WEEKS OF GESTATION
VESICLES VESICLES & VENTRICULAR CAVITY
Cervicalflexure
Pontine flexure
Telencephalic flexure
Cephalic flexure

DEVELOPMENT
2nd & 3rd months of development
FORAMEN OF MAGENDIE & LUSCHKA

DEVELOPMENT CHOROID PLEXUS
- found in both lateral ventricles, III & IV ventricles- artery invaginate thru the tela choroidea giving rise to primordial choroid plexus inside the ventricular system; villi development- begins to secrete CSF by the end of 1st trimester circulating thru the ventricular system & subarachnoid space

DEVELOPMENT CHOROID PLEXUS
- arteries involved in the development of choroid plexus: IV ventricle - branches of posterior inferior cerebellar artery (PICA) III ventricle - branches of medial posterior choroidal artery Lat. ventricle - branches of the lateral posterior choridal artery & the anterior choroidal artery

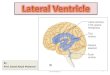
VENTRICLESAnterior horn
Body
Posterior horn
Third ventricle
Inferior horn
CerebralAqueduct(Sylvius)
Fourthventricle
Central canal
Foramen of Magendie
Foramen of Luschka
InterventricularForamen (Monroe)
Atrium, lateral ventricle
*The only openings between the ventricles of the brain and the subarachnoid space surrounding the brain are the foramina of Luschka & Magendie in the fourth ventricle
A/R- corpus callosumM- septum pellucidumL/F- caudate nucleus
A-f. MonroeP- spleniumR- corpus callosumM- septum pellucidumF- fornix,c.plexus, thalamus
R- corpus callosumM- calcarine fissure
R- thin ependymaL- thalamiF- hypo- & subthalamusA- l. terminalis, Ant. Comm.
L- cerebellar peduncleF- rhomboid fossa



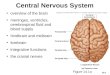
THIRD VENTRICLE BOUNDARY
Supraoptic recess
Infundibular recess
Pinealrecess
Suprapineal recess
Dorsal thalamus &Hypothalamus
Anterior commissure
Lamina terminalis
Tela choroidea (choroid plexus)
Posteriorcommissure
Optic chiasm
Infundibulum

- Cerebral aqueduct of Sylvius or Iter- only 1.5 mm in diam.- contains no choroid plexus- surrounded by a sleeve of gray matter containing small neurons; known as periaqueductal gray or central gray

IV VENTRICLE

-Hemorrhage into the ventricles from ruptured aneurysm, AVM or HPN bleed-Mass lesion obstructing the flow of CSF producing hydrocephalus-Inflammation & infectious process-Congenital anomaly involving the Iter as in stenosis or atresia

(desmosomes)
- Tanycytes: transport substances between ventricles & the blood

EPENDYMOMA - 5% - 6% of all glial neoplasms; originates from the ependymal cells - majority (60%-75%) are located in the posterior fossa - most frequent found in children younger than 5 years of age - signs & symptoms depend on the location of the tumor - characteristic histologic feature is the perivascular rosettes - treatment primarily is surgery followed by focal irradiation

Choroid plexus: - extend from the inferior horn of the lateral ventricle into the atrium (glomus choroideum), along the floor of the body of the lateral ventricle, continues through the interventricular foramen, and attaches to the roof of the III ventricle - it is also found in the IV ventricle attaching to the caudal roof and extends laterally into the foramen of Luschka - the endothelial cells of the capillaries along the layers of the choroid plexus have numerous fenestrations allowing exchange of molecules between blood plasma & the extracellular fluid in the connective tissue

(Zonulae occludentes)
Blood-CSF Barrier


BLOOD-BRAIN-BARRIER - A physiologic barrier to the movement of many substances into or out of the brain - endothelial cells of brain capillaries form a continuous lining membrane joined by numerous tight (occluding) junctions & have no intercellular pores or fenestrations - in turn are surrounded by the end- feet of astrocytes - Normal condition: BBB prohibits movement of high-molecular weight substances (proteins, penicillin, dopamine, vital dyes, etc.) - important in the administration of medicines targeted for the brain

CHOROID PLEXUS• Blood supply to the choroid plexus is via the
choroidal arteries and the posterior cerebellar arteries
• CP in the inferior horn, atrium & body of the lateral ventricle is served by the ant. choroidal artery (br. of ICA) & the lateral posterior choroidal artery (br. of P2)
• CP in the III ventricle is served by the medial posterior choroidal artery (br. Of P2)
• CP in the IV ventricle is served by brs. of the posterior inferior cerebellar artery (PICA)
• CP extending out into the foramen of Luschka into the SAS is served by anterior inferior cerebellar artery (AICA)
BLOOD SUPPLY

Choroid Plexus Tumors: - CP papillomas or carcinomas - common between birth and 10 years - occurs in the IV ventricle in 50%- 60% - signs & symptoms: increased ICP due to hydrocephalus - treatment is by surgery & for the malignant one is a combination of chemotherapy followed by surgery and a combination of chemotherapy & radiation




CEREBROSPINAL FLUID (CSF) - Normal CSF: pressure 70 – 200 mm H2O clear, colorless sugar 45-80 mg% (40%-60% of blood glucose)
protein 15 – 45 mg/dL total/diff. cell count 0-5/ml (leukocytes) average volume 120 ml in adult production 450-500 ml/day - produced by the choroid plexus & absorbed by arachnoid villi or pacchionian bodies found in the superior sagittal sinus back into the circulation

CSF Findings in Various CNS Disorders
DISORDER PRESSURE APPEARANCE GLUCOSE PROTEIN CELLS
Acute
Pyogenic increased cloudy/turbid decreased increased Inc. PMNs
Chronic
TB, Fungal,
Part.Tx M
increased Clear or cloudy decreased increased inc. lymphos
Acute
Viral
Normal or
Mildly inc. Clear, colorless normal
Mildly
increased
Inc.
lymphos
S A H
increased
Bloody, does not clot, super-natant xantho.
normal increased
Plenty of rbcs
Traumatic
tap normal
Bloody, clots spontaneously,
No xantho. normal
4 mg inc. per 5000
rbc
Same as peripheral count


Hydrocephalus: - obstructive hydrocephalus - communicating hydrocephalus - hydrocephalus ex vacuo - normal pressure hydrocephalus (NPH)