Embed Size (px)
DESCRIPTION
The Vertebral Column
Citation preview

The The SPINESPINE

Review of Relevant Review of Relevant AnatomyAnatomy
Functional Components:Functional Components:
1.1. Anterior PillarsAnterior Pillars
2.2. Posterior PillarsPosterior Pillars
Functional Unit:Functional Unit:
Motions:Motions: SagittalSagittal FrontalFrontal TransverseTransverse Ant/ Post shearAnt/ Post shear Lateral shearLateral shear DistractionDistraction

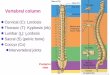
The Vertebral ColumnThe Vertebral Column
> central bony pillar of the body> central bony pillar of the body > provides a base of support for the head > provides a base of support for the head
and internal organs; a stable base for the and internal organs; a stable base for the attachments of ligaments, bones, and attachments of ligaments, bones, and muscles of the UE, rib cage, pelvis, muscles of the UE, rib cage, pelvis,
> a link between the UE and LE> a link between the UE and LE > protects the spinal cord> protects the spinal cord

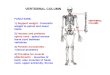
StructureStructure
33 short bones called 33 short bones called vertebrae and 23 IV vertebrae and 23 IV disksdisks
5 regions5 regions > cervical (7)> cervical (7) > thoracic ( 12)> thoracic ( 12) > lumbar ( 5)> lumbar ( 5) > sacral ( 5)> sacral ( 5) > coccygeal ( 4)> coccygeal ( 4)

Primary and Seconday Primary and Seconday CurvesCurves
Primary curves ( thoracic and sacral)Primary curves ( thoracic and sacral) “ “ posterior convexity, anterior concavity”posterior convexity, anterior concavity” ( kyphotic curves)( kyphotic curves) Secondary curves (cervical and lumbar)Secondary curves (cervical and lumbar) “ “ posterior concavity, anterior convexityposterior concavity, anterior convexity ( lordotic curves)( lordotic curves)

General characteristics of General characteristics of vertebravertebra
Typical vertebra hasTypical vertebra has Anteriorly : rounded Anteriorly : rounded bodybody Posteriorly: Posteriorly: vertebral archvertebral arch
a. pedicles (sides of the arch)a. pedicles (sides of the arch) B. laminae ( posteriorly located)B. laminae ( posteriorly located) 7 processes7 processes ( 1 spinous, 2 transverse, 4 articular)( 1 spinous, 2 transverse, 4 articular)
Vertebral foramenVertebral foramen

General characteristics of General characteristics of vertebravertebra

7 processes7 processes
4 4 articulararticular and 3 and 3 nonarticularnonarticular NONARTICULARNONARTICULAR A. (1) spinous process or spine (directed A. (1) spinous process or spine (directed
posteriorly )posteriorly ) B. (2) transverse processes ( directed laterally)B. (2) transverse processes ( directed laterally) > arise from the junction of pedicles and > arise from the junction of pedicles and
laminaelaminae > serves as levers> serves as levers > receives attachments of muscles and > receives attachments of muscles and
ligamentsligaments

7 processes…7 processes…
ARTICULARARTICULAR ( vertically arranged) ( vertically arranged) A. (2) superior articular A. (2) superior articular B. (2) inferior articular B. (2) inferior articular 2 superior articular processes of one arch 2 superior articular processes of one arch
articulate with the 2 inferior articular processes articulate with the 2 inferior articular processes of the arch above forming of the arch above forming two synovial joints two synovial joints
IV foramen IV foramen – formed by superior notch of one – formed by superior notch of one vertebra and inferior notch of an adjacent vertebra and inferior notch of an adjacent vertebra; transmits the spinal nerves and blood vertebra; transmits the spinal nerves and blood vesselsvessels

Characteristics of a Characteristics of a typical cervical vertebratypical cervical vertebra
Transverse processes has a foramen Transverse processes has a foramen transversarium for passage of vertebral artery transversarium for passage of vertebral artery and veinsand veins
Spines are small and bifidSpines are small and bifid Body is small and broad from side to sideBody is small and broad from side to side Vertebral foramen is large and triangularVertebral foramen is large and triangular Superior articular processesSuperior articular processes have facets that have facets that
face face backward and upwardbackward and upward; ; inferior have facetsinferior have facets that face that face downward and forwarddownward and forward

Typical cervical vertebraTypical cervical vertebra

Characteristics of the Characteristics of the atypical cervical vertebraeatypical cervical vertebrae( C1, C2, and C7)( C1, C2, and C7)
C1 atlas ( supports the globe of the head)C1 atlas ( supports the globe of the head) > s body and spinous process> s body and spinous process > has anterior and posterior arch> has anterior and posterior arch > has a lateral mass on each side with > has a lateral mass on each side with
articular surfaces on its upper surface for articular surfaces on its upper surface for articulation with the occipital articulation with the occipital condyles(condyles(atlanto-occipitalatlanto-occipital joints joints))

Characteristics of the Characteristics of the atypical cervical vertebraeatypical cervical vertebrae( C1, C2, and C7)….( C1, C2, and C7)….
C2 axis ( epistropheus)C2 axis ( epistropheus) > has peglike odontoid process> has peglike odontoid process
C7 (vertebra prominens)C7 (vertebra prominens) > has the longest spinous process and not bifid> has the longest spinous process and not bifid > transverse process is large> transverse process is large > foramen transversarium is small and > foramen transversarium is small and
transmits the vertebral vein or veins.transmits the vertebral vein or veins.

Atypical vertebraeAtypical vertebrae

Characteristics of a Typical Characteristics of a Typical Thoracic VertebraThoracic Vertebra
Body is medium size and heart shapedBody is medium size and heart shaped Vertebral foramen is small and circularVertebral foramen is small and circular Spines are long and inclined downwardSpines are long and inclined downward Costal facets are present on the sides of the Costal facets are present on the sides of the
bodies for articulation with the head of the ribsbodies for articulation with the head of the ribs Costal facets are present on the transverse Costal facets are present on the transverse
processes for articulation with the tubercles of processes for articulation with the tubercles of the ribs( T11 and 12 have no facets on the the ribs( T11 and 12 have no facets on the transverse processes)transverse processes)
Superior articular processesSuperior articular processes facets – facets – backward backward and laterallyand laterally
Inferior articular processesInferior articular processes facets – facets – forward forward and mediallyand medially

Typical thoracic vertebraTypical thoracic vertebra

Characteristics of a Characteristics of a Typical Lumbar VertebraTypical Lumbar Vertebra
Body is large and kidney shapedBody is large and kidney shaped Pedicles are strong and directed backwardPedicles are strong and directed backward Laminae are thickLaminae are thick Vertebral foramina are triangularVertebral foramina are triangular Transverse processes are long and slenderTransverse processes are long and slender Spinous processes are short, flat, and Spinous processes are short, flat, and
quadrangular and project backwardquadrangular and project backward Articular surfaces of the Articular surfaces of the superior articular superior articular
process face mediallyprocess face medially Inferior articular processes face laterallyInferior articular processes face laterally


comparisoncomparison

Regional variations in Regional variations in vertebral structurevertebral structure
cervical thoraciccervical thoracic lumbar lumbar
Body small heart-shaped kidneyBody small heart-shaped kidney
Arch Arch

Slant and Direction of Facet JointsSlant and Direction of Facet JointsA.A. Cervical- frontal planeCervical- frontal plane
B.B. ThoracicThoracic Upper thoracic: frontal planeUpper thoracic: frontal plane Lower thoracic: sagittal planeLower thoracic: sagittal plane
C.C. Lumbar- sagittal planeLumbar- sagittal plane

SacrumSacrum
5 vertebrae fused together to form 5 vertebrae fused together to form wedge-shaped bonewedge-shaped bone
Concave anteriorlyConcave anteriorly Upper border articulates with L5Upper border articulates with L5 Inferior border articulates with coccyxInferior border articulates with coccyx Lateral border articulates with 2 iliac Lateral border articulates with 2 iliac
bones ( sacroiliac joints)bones ( sacroiliac joints)

Structure and Function of the IV DiskStructure and Function of the IV Disk
The Annulus FibrosusThe Annulus Fibrosus fibrocartilage and collagenfibrocartilage and collagen provides tensile strength provides tensile strength restrain various spinal motionrestrain various spinal motion fibers of the inner layer blend with the nucleus fibers of the inner layer blend with the nucleus
pulposuspulposus firmly attached to the adjacent vertebra and to firmly attached to the adjacent vertebra and to
one anotherone anotherSupported by ligaments Supported by ligaments

Structure and Function of the IV DiskStructure and Function of the IV Disk
The Nucleus PulposusThe Nucleus Pulposus gelatinous mass gelatinous mass with loosely aligned fibers. with loosely aligned fibers. high concentration of proteoglycanshigh concentration of proteoglycans Fluid Mechanics In the SpineFluid Mechanics In the Spine
evenly distribute pressureevenly distribute pressure transport for nutrients transport for nutrients normally: NP does not move in a healthy disknormally: NP does not move in a healthy disk
The Cartilaginous End-PlatesThe Cartilaginous End-Plates encircled by the apophyseal ring of the encircled by the apophyseal ring of the
respective vertebral bodyrespective vertebral body nutrition diffuses from marros of the vertebral bodies to nutrition diffuses from marros of the vertebral bodies to
the disk via the endplatesthe disk via the endplates

LigamentsLigaments

Intervertebral diskIntervertebral disk

LigamentsLigaments
1. Intersegmental – 1. Intersegmental – binds a anumber of binds a anumber of vertebrae into a unitvertebrae into a unit
2. Intrasegmental – 2. Intrasegmental – binds an individual or binds an individual or adjacent vertebrae adjacent vertebrae togethertogether

Intersegmental ligamentsIntersegmental ligaments Anterior Longitudinal ligamentAnterior Longitudinal ligament Dense band along anterior and lateral surface Dense band along anterior and lateral surface
of the vertebral bodies from sacrum to C2of the vertebral bodies from sacrum to C2 Atlanto-occipital ligament – extension from C2 Atlanto-occipital ligament – extension from C2
to occiputto occiput Tensile strength Tensile strength High cervical, lower thoracic, lumbar regionsHigh cervical, lower thoracic, lumbar regions Compressed in flexion, stretch in flexion and Compressed in flexion, stretch in flexion and
slack in neutral positionslack in neutral position 2x as strong as the PLL2x as strong as the PLL

IntersegmentalIntersegmental
2. Posterior Longitudinal ligament2. Posterior Longitudinal ligamentRuns within the vertebral canal along Runs within the vertebral canal along
posterior surfaces of the vertebral bodies posterior surfaces of the vertebral bodies from C2 to sacrumfrom C2 to sacrum
Tectorial membrane – ligament that Tectorial membrane – ligament that extends to the occiputextends to the occiput
Stretched in flexion, slack in extensionStretched in flexion, slack in extension

IntersegmentalIntersegmental
Supraspinous ligamentSupraspinous ligament Runs along the tips of the spinous process Runs along the tips of the spinous process
from C7 to sacrumfrom C7 to sacrum ““Ligamentum nuchae” in the cervical regionLigamentum nuchae” in the cervical region Ligaments on the lumbar level merge with the Ligaments on the lumbar level merge with the
insertion of lumbar musclesinsertion of lumbar muscles Stretched in flexionStretched in flexion Its fiber resist separation of the spinous Its fiber resist separation of the spinous
processes during forward flexion processes during forward flexion

Intrasegmental ligamentsIntrasegmental ligaments
Ligamentum flavumLigamentum flavum thick, elastic ligament on the posterior thick, elastic ligament on the posterior
surface of vertebral canalsurface of vertebral canalRuns from C2 to sacrum connecting Runs from C2 to sacrum connecting
laminae of adjacent vertebraelaminae of adjacent vertebraeStrongest in the lower thoracic and Strongest in the lower thoracic and
weakest in midcervicalweakest in midcervical

Intrasegmental ligamentsIntrasegmental ligaments Interspinous ligamentInterspinous ligamentWell developed only in lumbar area from Well developed only in lumbar area from
base of spinous process to anotherbase of spinous process to anotherStretch in forward flexion and slack in Stretch in forward flexion and slack in
extensionextension Intertransverse ligamentIntertransverse ligamentWell developed only in lumbar areaWell developed only in lumbar areaStretch in lateral bendingStretch in lateral bending

Thoracolumbar FasciaThoracolumbar Fascia

OTHER FACTORS THAT INFLUENCE OTHER FACTORS THAT INFLUENCE MOVEMENT MOVEMENT
Slant and Shape of Spinous ProcessSlant and Shape of Spinous Process
Relative size of IV and BodyRelative size of IV and Body
Ribs in the thoracic RegionRibs in the thoracic Region
MusclesMuscles

NEUROMUSCULAR NEUROMUSCULAR FUNCTION: DYNAMIC FUNCTION: DYNAMIC STABILIZATIONSTABILIZATION Muscle control in the Lumbar spineMuscle control in the Lumbar spine
Functions primarily as prime movers and secondary stabilizersFunctions primarily as prime movers and secondary stabilizers Functions as primary stabilizersFunctions as primary stabilizers
Transversus abdominis and IO- isometric contraction, Transversus abdominis and IO- isometric contraction, valsalva maneuver and drawing in maneuvervalsalva maneuver and drawing in maneuver
IO and EO- rotation and side bendingIO and EO- rotation and side bending Rectus abs- flexion and post tiltingRectus abs- flexion and post tilting Quadratus Lumborum- stabilize the spine and ribsQuadratus Lumborum- stabilize the spine and ribs MultifidusMultifidus Intersegmental mmIntersegmental mm ESES Iliopsoas mmIliopsoas mm

Small muscles at the Small muscles at the backback

FEEDFORWARD AND SPINAL STABILITYFEEDFORWARD AND SPINAL STABILITY“ …“ …there are feedforward postural responses there are feedforward postural responses
of all trunk preceding activity in muscles of all trunk preceding activity in muscles that move the extremity”that move the extremity”
“…“…speed or not direction of arm movements speed or not direction of arm movements directly affects activation of TA and IO”directly affects activation of TA and IO”
EFFECTS OF BREATHING ON POSTURE EFFECTS OF BREATHING ON POSTURE AND STABILITYAND STABILITY
Effect of Valsalva maneuverEffect of Valsalva maneuver

POSTURE POSTURE EquilibriumEquilibrium
ankleankleKneeKnee hiphipTrunkTrunkHeadHead
Etiology of Postural ImpairmentsEtiology of Postural ImpairmentsMechanical stressMechanical stress

PAIN SYNDROMES RELATED TO IMPAIRED PAIN SYNDROMES RELATED TO IMPAIRED POSTUREPOSTURE
Postural Fault: deviates from normal alignment but Postural Fault: deviates from normal alignment but has no structural limitationshas no structural limitations
Postural Pain Syndrome: pain that occurs from Postural Pain Syndrome: pain that occurs from mechanical stress when a person maintains a mechanical stress when a person maintains a faulty posture from prolonged periodfaulty posture from prolonged period
Postural Dysfunction: with adaptive shortening of Postural Dysfunction: with adaptive shortening of tissues and mm weaknesstissues and mm weakness
Postural HabitsPostural Habits

COMMON FAULTY POSTURESCOMMON FAULTY POSTURES
Kypholordotic PostureKypholordotic Posture Potential sources of painPotential sources of pain Potential mm Potential mm
impairmentsimpairments Common CausesCommon Causes

COMMON FAULTY POSTURESCOMMON FAULTY POSTURES
SwaybackSwayback Potential sources of Potential sources of
painpain Potential mm Potential mm
impairmentsimpairments Common CausesCommon Causes

COMMON FAULTY POSTURESCOMMON FAULTY POSTURES
Flat Low-Back Flat Low-Back Potential sources of Potential sources of
painpain Potential mm Potential mm
impairmentsimpairments Common CausesCommon Causes

COMMON FAULTY POSTURESCOMMON FAULTY POSTURES
Flat Upper Back and Flat Upper Back and Flat neck postureFlat neck posture
Potential sources of Potential sources of painpain
Potential mm Potential mm impairmentsimpairments
Common CausesCommon Causes

COMMON FAULTY POSTURESCOMMON FAULTY POSTURES
Forwardhead and Forwardhead and increased thoracic increased thoracic kyphosiskyphosis
Potential sources Potential sources of painof pain
Potential mm Potential mm impairmentsimpairments
Common CausesCommon Causes

COMMON FAULTY POSTURESCOMMON FAULTY POSTURESLower Extremity AsymmetriesLower Extremity Asymmetries CharacteristicsCharacteristics
hip jointhip joint SI jointSI joint lumbar spine lumbar spine
Potential sources of painPotential sources of painShear forces in the SI and hip jt at LLShear forces in the SI and hip jt at LL stenosis at IV foraminastenosis at IV foramina facet compressionfacet compression disc break downdisc break downMm fatigue, spasm and tensionMm fatigue, spasm and tensionLE overuse LE overuse

PATHOLOGY OF THE IV DISKPATHOLOGY OF THE IV DISKINJURY AND DEGENERATION INJURY AND DEGENERATION
1.1. Fatigue Loading and Traumatic RuptureFatigue Loading and Traumatic Rupture
a. Fatigue Breakdowna. Fatigue Breakdown
b. Traumatic Ruptureb. Traumatic Rupture
2. Axial Load2. Axial Load
3. Age3. Age
4. Degenerative Changes4. Degenerative Changes

DISC PATHOLOGIESDISC PATHOLOGIES

COMPRESSION FRACTURECOMPRESSION FRACTURE

DISC HERNIATION AND TISSUE DISC HERNIATION AND TISSUE FLUID STASISFLUID STASIS

DISC HERNIATION DISC HERNIATION

Etiology of S/SxEtiology of S/Sx
1.1. PainPain
2.2. Neurologic s/sxNeurologic s/sx
3.3. Variability of symptomsVariability of symptoms Small posterolateral protrusionSmall posterolateral protrusion Large posterolateral protrusionLarge posterolateral protrusion Large posterior protrusionLarge posterior protrusion Anterior protrusionAnterior protrusion
4.4. Shifting symptomsShifting symptoms
5.5. inflammationinflammation

Herniation Herniation

Objective Clinical FindingsObjective Clinical FindingsA. Lumbar SpineA. Lumbar SpinePosturePosturePreferred position and activityPreferred position and activityForward bending and backward bendingForward bending and backward bending special testspecial test
B. Cervical SpineB. Cervical Spine

Pathology of the Facet JointPathology of the Facet Joint

Common Diagnosis of Facet Jt. Common Diagnosis of Facet Jt. PathologiesPathologies
Sprain / Capsule InjurySprain / Capsule Injury OA, Degenerative Dse., SpondylosisOA, Degenerative Dse., Spondylosis Rheumatoid ArthritisRheumatoid Arthritis Facet Jt. Impingement Facet Jt. Impingement
Common ImpairmentCommon Impairment1.1. PainPain2.2. MobilityMobility3.3. Postural impairmentsPostural impairments4.4. Activities and motionsActivities and motions

SpondylolysisSpondylolysis

SpondylolisthesisSpondylolisthesis


Classification of SpondylolysisClassification of Spondylolysis1.1. Dysplastic: dysplasia in the superior sacral Dysplastic: dysplasia in the superior sacral
facet and inferior facet of L5facet and inferior facet of L5
2.2. Isthmic: Isthmic: LyticLytic ElongatedElongated Acute FractureAcute Fracture
3.3. DegenerativeDegenerative
4.4. TraumaticTraumatic
5.5. PathologicPathologic

S/ Sy of Spondylolysis/ SpondylolithesisS/ Sy of Spondylolysis/ Spondylolithesis
1.1. Compression of nerve rootCompression of nerve root
2.2. Compression of spinal cordCompression of spinal cord
3.3. Exaggerated lumbar lordosisExaggerated lumbar lordosis
4.4. Limited spinal ROMLimited spinal ROM
5.5. Tightness of hip flexor, hamstring and Tightness of hip flexor, hamstring and ankle dorsiflexorsankle dorsiflexors
On Xray: Meyerdings Classification On Xray: Meyerdings Classification depending on degree of advancementdepending on degree of advancement

Meyerding’s ClassificationMeyerding’s Classification


Treatment:Treatment: Posttraumatic cases: immobilization for 10-Posttraumatic cases: immobilization for 10-
12 wks12 wksChronic Back PainChronic Back Pain
1. abdominal strengthening1. abdominal strengthening
2. stretching of tight structures2. stretching of tight structures
3. static and dynamic body strengthening3. static and dynamic body strengthening
4. support4. support
5. massage and modalities5. massage and modalities

Lumbar StenosisLumbar Stenosis
condition in which the nerves or the spinal condition in which the nerves or the spinal cord in the spinal canal are "closed in," or cord in the spinal canal are "closed in," or compressed compressed
Causes:Causes: spur formantionspur formantionFacet hypertrophyFacet hypertrophy subluxationsubluxation spondyolisthesisspondyolisthesis congenital presdepositioncongenital presdeposition

Lumbar StenosisLumbar Stenosis

Lumbar Stenosis S/ SxLumbar Stenosis S/ Sx
Central StenosisCentral Stenosis
1.1. Sx produced by standing and walking and Sx produced by standing and walking and relieved by sitting or assuming a flexed relieved by sitting or assuming a flexed spine positionspine position
2.2. PseudoclaudicationPseudoclaudication
3.3. WeaknessWeakness
4.4. Walks in a stooped mannerWalks in a stooped manner
5.5. Walking uphill is easier than walking Walking uphill is easier than walking downhilldownhill

Lumbar Stenosis S/ SxLumbar Stenosis S/ Sx
Lateral Recess SyndromeLateral Recess Syndrome1.1. Intense sciatic painIntense sciatic pain2.2. Mild neurologic defecitMild neurologic defecit3.3. SLR usually negativeSLR usually negative4.4. Little of no low back painLittle of no low back pain
TREATMENTTREATMENT1.Strengtening1.Strengtening2. Stretching2. Stretching3. Passive support3. Passive support

Pathology of Muscle and Soft Pathology of Muscle and Soft TissueTissue
Common Sites Common Sites a.a. CervicalCervical
FlexionFlexion Extension Extension
b.b. LumbarLumbar Common ImpairmentsCommon Impairments
a.a. AcuteAcute Pain and mm guardingPain and mm guarding Pain c mm contraction and stretchPain c mm contraction and stretch Interference c ADLInterference c ADL
b.b. Subacute/ChronicSubacute/Chronic Mm weaknessMm weakness Restricted mobilityRestricted mobility Inadequate spinal control and stabilizationInadequate spinal control and stabilization Poor postural awarenessPoor postural awareness Limited IADL, work and recreational actLimited IADL, work and recreational act

Guidelines for Management of Soft Tissue Guidelines for Management of Soft Tissue and MM Lesionand MM Lesion
1.1. Modulate Pain and Control Edema and Modulate Pain and Control Edema and InflammationInflammationa. Cervical a. Cervical b. lumbarb. lumbar
2. Maintain Mm integrity2. Maintain Mm integritya. Cervical Regiona. Cervical Regionb. Lumbar Regionb. Lumbar Region
3. Maintain mm integrity when there is no mm injury3. Maintain mm integrity when there is no mm injury4. Traction4. Traction

GENERAL GUIDELINES IN MANAGING GENERAL GUIDELINES IN MANAGING SPINAL PROBLEMSSPINAL PROBLEMSAcuteAcute 1.1. Decrease Acute SxDecrease Acute Sx
Modalities, massage, restModalities, massage, rest TractionTraction
2.2. Demonstrate awareness of neck and pelvic Demonstrate awareness of neck and pelvic position and movementposition and movement
Establish the neutral position/ position of bias/ Establish the neutral position/ position of bias/ functional positionfunctional position
a. a. Flexion biasFlexion biasb. Extension biasb. Extension biasc. Nonweight-bearing biasc. Nonweight-bearing bias
Kinesthetic Training Kinesthetic Training a. cervical and scapular motionsa. cervical and scapular motionsb. Pelvic tilts and neutral spineb. Pelvic tilts and neutral spine

GENERAL GUIDELINES IN MANAGING GENERAL GUIDELINES IN MANAGING SPINAL PROBLEMSSPINAL PROBLEMS
3. Demonstrate safe postures3. Demonstrate safe postures Teach awareness of safe postures and effects of Teach awareness of safe postures and effects of
movementmovement Passive Positioning/ supportPassive Positioning/ support
4. Initiate neuromuscular control of stabilizing mm4. Initiate neuromuscular control of stabilizing mm Drawing in ManeuverDrawing in Maneuver Teach Basic StabilizationTeach Basic Stabilization
5. Teach basic functional movements5. Teach basic functional movements
6. Review Precautions6. Review Precautions

GENERAL GUIDELINES IN GENERAL GUIDELINES IN MANAGING SPINAL PROBLEMSMANAGING SPINAL PROBLEMS
SubacuteSubacute
1.1. Learn self-management and decrease episodes Learn self-management and decrease episodes of painof pain
Ergonomics and safe act and posturesErgonomics and safe act and postures
2.2. Progress awareness and control of spinal Progress awareness and control of spinal segmentsegment
Practice spinal control in all positions and exercisesPractice spinal control in all positions and exercises
3.3. Increase mobilityIncrease mobility Joint mob/ manipulation, inhibitionJoint mob/ manipulation, inhibition Stretching exercisesStretching exercises

GENERAL GUIDELINES IN MANAGING GENERAL GUIDELINES IN MANAGING SPINAL PROBLEMSSPINAL PROBLEMS
4. Develop neuromuscular control, strength 4. Develop neuromuscular control, strength and endurance in stabilizing mmand endurance in stabilizing mm
Progress stabilization ex, increase reps and Progress stabilization ex, increase reps and challengechallenge
5. Increase dynamic trunk and extremity 5. Increase dynamic trunk and extremity strengthstrength
6. Develop general aerobic endurance6. Develop general aerobic endurance
7. Learn technique of stress and relaxation7. Learn technique of stress and relaxation
8. Learn safe body mechanics8. Learn safe body mechanics
9. Develop functional skills9. Develop functional skills

GENERAL GUIDELINES IN GENERAL GUIDELINES IN MANAGING SPINAL PROBLEMSMANAGING SPINAL PROBLEMS
ChronicChronic progress exercises progress exercises Habitually use techniques of stress Habitually use techniques of stress
relief/relaxationrelief/relaxation return to high level/ high intensity activitiesreturn to high level/ high intensity activitiesDevelop healthy exercise habits Develop healthy exercise habits

Guidelines for Management of Guidelines for Management of Impairments with an Extension Impairments with an Extension
BiasBias
Principles of Mx:Principles of Mx:1.1. Effects of Postural changes on IV discEffects of Postural changes on IV disc2.2. Effects of Bed restEffects of Bed rest3.3. Effects of TractionEffects of Traction4.4. Effects of flexion and extension on IV and Effects of flexion and extension on IV and
Fluid stasisFluid stasis5.5. Effects of Isometric and Dynamic ExerciseEffects of Isometric and Dynamic Exercise6.6. Effects of MM guardingEffects of MM guarding

Guidelines for Management of Guidelines for Management of Impairments with an Extension Impairments with an Extension BiasBias Indication for Extension Ex.Indication for Extension Ex. Precaution and CI to Extension Ex.Precaution and CI to Extension Ex.
1. acute pain not influenced by changing the 1. acute pain not influenced by changing the patient’s position or movementpatient’s position or movement2. peripheralization of sy2. peripheralization of sy3. CI:3. CI:
No movement or position decrease the syNo movement or position decrease the sySaddle anesthesia and bladder weaknessSaddle anesthesia and bladder weaknessExtreme painExtreme pain
4. Any activity or exercises that increases 4. Any activity or exercises that increases intradiskal pressure , such as valsalva intradiskal pressure , such as valsalva maneuver, active pelvic tilt or trunk raising maneuver, active pelvic tilt or trunk raising exercise exercise

Guidelines for Management of Guidelines for Management of Impairments with an Extension Impairments with an Extension BiasBiasTechniques of Intervention Using an Extension Techniques of Intervention Using an Extension
Approach in the Acute StageApproach in the Acute Stage Lumbar SpineLumbar Spine
Passive ExtensionPassive Extension Lateral ShiftLateral Shift TractionTraction Patient EducationPatient Education
• Position and motions increase and decrease pain Position and motions increase and decrease pain or other symptomsor other symptoms
• Self-correction of lateral shiftSelf-correction of lateral shift• Respect painRespect pain• Passive support during healingPassive support during healing• Avoid flexion activitiesAvoid flexion activities

Guidelines for Management of Guidelines for Management of Impairments with an Extension Impairments with an Extension BiasBias
Techniques of Intervention Using an Techniques of Intervention Using an Extension Approach in the Acute StageExtension Approach in the Acute Stage
Cervical spineCervical spinePassive Axial ExtensionPassive Axial ExtensionPatient EducationPatient EducationTractionTractionKinesthetic Training for PostureKinesthetic Training for Posture

Mc Kenzie RegimenMc Kenzie Regimen Method of diagnosis and treatment based on Method of diagnosis and treatment based on
movement patterns of the spinemovement patterns of the spine advocates position and movement patterns that advocates position and movement patterns that
best relieve patient’s symptomsbest relieve patient’s symptoms Classified LBP based on spinal movement pattern, Classified LBP based on spinal movement pattern,
each classification has a specific treatment that each classification has a specific treatment that includes postural correction and educationincludes postural correction and education
Approach:Approach:Technique is a more passive form of spinal manipulation Technique is a more passive form of spinal manipulation
which patient produces the motion , position and forceswhich patient produces the motion , position and forcesCyclic ROM to endrange- centralizes painCyclic ROM to endrange- centralizes painLumbar flexion ex maybe added later when patient has Lumbar flexion ex maybe added later when patient has
full spinal ROMfull spinal ROM

McKenzie RegimenMcKenzie Regimen
1.1. Lying prone – 5 minsLying prone – 5 mins
2.2. Lying in extension ( prone on elbows)Lying in extension ( prone on elbows)
3.3. Extension in lying ( prone on hands)Extension in lying ( prone on hands)
4.4. Extension in standingExtension in standing
5.5. Flexion in supine (knee to chest)Flexion in supine (knee to chest)
6.6. Flexion in sittingFlexion in sitting
7.7. Flexion in standingFlexion in standing

McKenzie Regimen (New)McKenzie Regimen (New)1.1. Lying ProneLying Prone2.2. Lying Prone in ExtensionLying Prone in Extension3.3. Extension in LyingExtension in Lying4.4. Extension in Lying with Belt FixationExtension in Lying with Belt Fixation5.5. Sustained ExtensionSustained Extension6.6. Extension in StandingExtension in Standing7.7. Extension MobilizationExtension Mobilization8.8. Extension ManipulationExtension Manipulation9.9. Rotation Mobilization in ExtensionRotation Mobilization in Extension

McKenzie Regimen (New)McKenzie Regimen (New)
10. Rotation Manipulation in Extension10. Rotation Manipulation in Extension11. Sustained Rotation / Mobilization in 11. Sustained Rotation / Mobilization in
FlexionFlexion12. Rotation Manipulation in Flexion12. Rotation Manipulation in Flexion13. Flexion in Lying13. Flexion in Lying14. Flexion in Standing14. Flexion in Standing15. Flexion in Standing15. Flexion in Standing16. Correction of Lateral Shift16. Correction of Lateral Shift17. Self Correction of Lateral Shift17. Self Correction of Lateral Shift

Guidelines for Management of Guidelines for Management of Impairments with an Flexion BiasImpairments with an Flexion Bias
Principles of Mx:Principles of Mx:
1.1. Effects of positionEffects of position
2.2. Effects of tractionEffects of traction
3.3. Effects of Trauma and repetitive irritationEffects of Trauma and repetitive irritation
4.4. Effects of meniscoid tissueEffects of meniscoid tissue

Guidelines for Management of Guidelines for Management of Impairments with an Flexion BiasImpairments with an Flexion Bias
Techniques of Intervention Using an Flexion Techniques of Intervention Using an Flexion Approach in the Acute StageApproach in the Acute Stage rest and Supportrest and SupportFunctional position for comfortFunctional position for comfortTractionTractionCorrection of lateral shiftCorrection of lateral shiftCorrection of meniscoid Impingement Correction of meniscoid Impingement
1. Traction1. Traction
2. Spinal mobilization and manipulation2. Spinal mobilization and manipulation

William’s ExerciseWilliam’s Exercise

Guidelines for Management of Guidelines for Management of Impairments with a NonWB BiasImpairments with a NonWB Bias
Techniques of Intervention Using a NonWB Techniques of Intervention Using a NonWB Approach in the Acute StageApproach in the Acute Stage Traction Traction
separate vertebraseparate vertebra mechanical sliding of facetsmechanical sliding of facets reduce circulation congestionreduce circulation congestion relieve pressure on the dura, blood vessels and relieve pressure on the dura, blood vessels and
nerve rootnerve root stimulation of mechanoreceptorsstimulation of mechanoreceptors
HarnessHarness PoolPool

NEURAL TENSION IMPAIRMENTSNEURAL TENSION IMPAIRMENTSNervous System Mobility CharacteristicsNervous System Mobility Characteristics
arrangement allows for mobilityarrangement allows for mobility Nerves are wavyNerves are wavy Connective tissue absorb tensile and compressive Connective tissue absorb tensile and compressive
forcesforces
Positive Signs: Tension SignsPositive Signs: Tension Signs Causes of SyCauses of Sy MxMx CICI
Acute or unstable neurologic signsAcute or unstable neurologic signs cauda equina symptomscauda equina symptoms SCI or sySCI or sy

MUSCLE RELAXATION TECHNIQUEMUSCLE RELAXATION TECHNIQUE
1.1. AROMEAROME
2.2. Conscious Relaxation Training in the Conscious Relaxation Training in the Cervical RegionCervical Region
3.3. Modalities and MassageModalities and Massage

BODY MECHANICSBODY MECHANICS

BODY MECHANICSBODY MECHANICS
1.1. Lifting with a flexed spineLifting with a flexed spine Support is from inert structuresSupport is from inert structures Mm is elongated and relaxedMm is elongated and relaxed
2.2. Lifting with an extended spineLifting with an extended spine Mm in the lumbar spine is active Mm in the lumbar spine is active
3.3. Lifting with a neutral spineLifting with a neutral spine

PROPER LIFTING TECHNIQUESPROPER LIFTING TECHNIQUES
DIAGONAL DIAGONAL LIFTLIFT

DIAGONAL LIFT….DIAGONAL LIFT….

PROPER LIFTING TECHNIQUESPROPER LIFTING TECHNIQUES
SQUAT LIFTSQUAT LIFT

SQUAT LIFTSQUAT LIFT

PROPER LIFTING TECHNIQUESPROPER LIFTING TECHNIQUES Plan ahead before lifting.Plan ahead before lifting.
Knowing what you're doing and where you're going will Knowing what you're doing and where you're going will prevent you from making awkward movements while prevent you from making awkward movements while holding something heavy. Clear a path, and if lifting holding something heavy. Clear a path, and if lifting something with another person, make sure both of you something with another person, make sure both of you agree on the plan. agree on the plan.
Lift close to your body.Lift close to your body.You will be a stronger, and more stable lifter if the object You will be a stronger, and more stable lifter if the object is held close to your body rather than at the end of your is held close to your body rather than at the end of your reach. Make sure you have a firm hold on the object you reach. Make sure you have a firm hold on the object you are lifting, and keep it balanced close to your body. are lifting, and keep it balanced close to your body.
Feet shoulder width apart.Feet shoulder width apart.A solid base of support is important while lifting. Holding A solid base of support is important while lifting. Holding your feet too close together will be unstable, too far your feet too close together will be unstable, too far apart will hinder movement. Keep the feet about apart will hinder movement. Keep the feet about shoulder width apart and take short steps. shoulder width apart and take short steps.

PROPER LIFTING TECHNIQUESPROPER LIFTING TECHNIQUES
Bend your knees and keep your back straight.Bend your knees and keep your back straight.Practice the lifting motion before you lift the object, and think about Practice the lifting motion before you lift the object, and think about your motion before you lift. Focus on keeping you spine straight--your motion before you lift. Focus on keeping you spine straight--raise and lower to the ground by bending your knees. raise and lower to the ground by bending your knees.
Tighten your stomach muscles.Tighten your stomach muscles.Tightening your abdominal muscles will hold your back in a good Tightening your abdominal muscles will hold your back in a good lifting position and will help prevent excessive force on the spine. lifting position and will help prevent excessive force on the spine.
Lift with your legs.Lift with your legs.Your legs are many times stronger than your back muscles--let your Your legs are many times stronger than your back muscles--let your strength work in your favor. Again, lower to the ground by bending strength work in your favor. Again, lower to the ground by bending your knees, not your back. Keeping your eyes focused upwards your knees, not your back. Keeping your eyes focused upwards helps to keep your back straight. helps to keep your back straight.
If you're straining, get help.If you're straining, get help.If an object is too heavy, or awkward in shape, make sure you have If an object is too heavy, or awkward in shape, make sure you have someone around who can help you lift. someone around who can help you lift.
Wear a belt or back support.

PROPER LIFTING TECHNIQUESPROPER LIFTING TECHNIQUESTips:Tips: Never bend your back to pick something up.Never bend your back to pick something up.
It's just not worth the damage that improper It's just not worth the damage that improper lifting technique can cause. lifting technique can cause.
Hold the object close to your body.Hold the object close to your body.You are a much more stable lifter if you're not You are a much more stable lifter if you're not reaching for an object. reaching for an object.
Don't twist or bend.Don't twist or bend.Face in the direction you are walking. If you Face in the direction you are walking. If you need to turn, stop, turn in small steps, and need to turn, stop, turn in small steps, and then continue walking. then continue walking.
Keep your eyes up.Keep your eyes up.Looking slightly upwards will help you Looking slightly upwards will help you maintain a better position of the spine.maintain a better position of the spine.

ERGONOMICSERGONOMICS1.1. Lumbar supportLumbar support
2.2. Chair heightChair height
3.3. Desk height or table heightDesk height or table height
4.4. Mattress and pillowsMattress and pillows
5.5. PositionPosition
6.6. Reaching overheadReaching overhead