Embed Size (px)
Citation preview

1
This article is protected by copyright. All rights reserved.
Thrombin as important factor for cutaneous wound healing - Comparison of fibrin
biomatrices in vitro and in a rat excisional wound healing model 1
Alfred Gugerell, PhD1,2,*
, Waltraud Pasteiner, PhD3, Sylvia Nürnberger, PhD
1, Johanna
Kober, M.Sc.2, Alexandra Meinl, PhD
1, Sabine Pfeifer
1, Joachim Hartinger
1, Susanne
Wolbank, PhD1, Andreas Goppelt, PhD
3, Heinz Redl, PhD
1, Rainer Mittermayr, MD
1
1Ludwig Boltzmann Institute for Experimental and Clinical Traumatology, Austrian Cluster
for Tissue Regeneration, Vienna, Austria
2Division of Plastic and Reconstructive Surgery, Department of Surgery, Medical University
of Vienna, Vienna, Austria
3Biosurgery, Baxter Innovations GmbH, Vienna, Austria
* corresponding author:
Dr. Alfred Gugerell, PhD
Medical University of Vienna, Department of Surgery, Division of Plastic and Reconstructive
Surgery
Waehringer Guertel 18-20, A-1090 Vienna, Austria
T: +43 1 40400 2165
Keywords: wound healing; thrombin; keratinocytes; rat excisional wound model; skin; fibrin
sealant; biomatrix
Running head: Thrombin influences cutaneous wound healing
This article has been accepted for publication and undergone full peer review but has not been through the
copyediting, typesetting, pagination and proofreading process, which may lead to differences between this
version and the Version of Record. Please cite this article as doi: 10.1111/wrr.12234 Acc
epte
d A
rticl
e
2
This article is protected by copyright. All rights reserved.
Manuscript received: 08 October 2013
Accepted in final form: 4 September 2014
Abstract
Fibrin biomatrices have been used for many years for hemostasis and sealing and are a well-
established surgical tool. The objective of the present study was to compare two commercially
available fibrin biomatrices regarding the effect of their thrombin concentration on
keratinocytes and wound healing in vitro and in vivo.
Keratinocytes showed significant differences in adhesion, viability and morphology in the
presence of the fibrin matrices in vitro. A high thrombin concentration (800-1200 IU/ml)
caused deteriorated cell compatibility. By using a thrombin inhibitor, those differences could
be reversed.
In a rat excisional wound healing model, we observed more rapid wound closure and
less wound severity in wounds treated with a fibrin matrix containing a lower concentration of
thrombin (4 IU/ml). Furthermore, fewer new functional vessels and a lower level of VEGF
were measured in wounds after seven days treated with the matrix with higher thrombin
concentration. These in vivo results may be partially explained by the in vitro
biocompatibility data. Additionally, Results show that low thrombin biomatrices were
degraded faster than the high thrombin material.
Hence we conclude that the composition of fibrin biomatrices influences keratinocytes
and therefore has an impact on wound healing.
Acc
epte
d A
rticl
e
3
This article is protected by copyright. All rights reserved.
Introduction
In the early phase of wound healing the clotting cascade builds an insoluble clot with fibrin,
platelets and cells to stop blood loss. (1). Furthermore, this provisional extracellular matrix is
required to support wound healing by providing a three-dimensional scaffold supporting
adhesion, proliferation, and migration of invading cells (2). Various growth factors (mainly
epidermal growth factor EGF, platelet derived growth factor PDGF, vascular endothelial
growth factor VEGF or members of the transforming growth factor (TGF)-family) and
cytokines are released by keratinocytes, fibroblasts, endothelial cells, macrophages, platelets
and other cells (3, 4) that attract and activate macrophages to induce phagocytosis of bacteria
and debris (5). It also causes the migration and division of cells (e.g. fibroblasts) into the clot.
Also fibrinopeptides FpA and FpB released by thrombin during clot formation are chemo-
attractants and activators of leukocytes. TGF-α and tumor necrosis factor (TNF- α) are
secreted from vascular endothelial cells, keratinocytes, and fibroblasts inducing the
inflammatory stage (6). Following the inflammatory stage, two or three days after injury,
vascular angiogenesis with capillary formation occurs to ensure the new tissue has sufficient
nutrients (7). Therefore, cells originated from uninjured blood vessels in the surrounding
tissue undergo epithelial-mesenchymal transition (EMT), activated through VEGFs.
Collagenases, plasminogen and plasmin (produced by the epidermal cells) decompose the
extracellular matrix to make way for the new vessels. Then, these cells start to migrate into
the matrix and to proliferate by forming new capillary-like tubes (8).
Some of the most important cells in reepithelialization are keratinocytes. In case of
injury, keratinocytes undergo a number of physical and biochemical changes in order to
migrate into the wound. The signal for migration is thought to be through the loss of contact
inhibition, signaling the cell to switch from a differentiation phenotype (expressing keratins 5
and 14 in the basal layer, or 1 and 10 in the suprabasal layers) to a migration phenotype Acc
epte
d A
rticl
e
4
This article is protected by copyright. All rights reserved.
(expressing keratins 6 and 16) (9). Keratinocytes then migrate across the wound bed through
interactions of their integrin receptors, binding to specific recognition sequences in the
granulation tissue (10).Among other integrins, migrating keratinocytes express integrin α3β1
to bind to the provisional matrix in the wound bed, rich in fibrin, fibronectin, vitronectin, and
laminin-5. Proliferating keratinocytes on the other hand bind via integrin αvβ5 and integrins
of type β4 and β1 (11). Proliferation and migration of keratinocytes are controlled by multiple
overlapping mechanisms, of which endothelial protein C receptor (EPCR) or protease-
activated receptor 1 (PAR-1) signaling may play an important role (12).
Adapted from the principles of the natural occurring final stage of hemostasis, fibrin
sealants were developed for surgery, mimicking the coagulation. They are widely used as
hemostats in various surgical indications and for soft tissue sealing(13, 14). In clinical studies
fibrin sealants have also been used as matrix to promote wound healing (15, 16) or as delivery
matrix for (stem) cells (17, 18).
Fibrin sealants are derived from human plasma and therefore do not only consist of
fibrinogen and thrombin, but also hundreds of constituents present in the plasma such as
ECM-molecules or growth factors (19, 20). Due to different purification and virus
inactivation procedures, variations in salt concentrations and diverse enrichments or
depletions, the products not only differ from brand to brand but also among lot numbers of the
same brand name. Therefore, we want to investigate the most important components of a
fibrin matrix and evaluate them for optimal interaction with cells.
The objective of this study was to compare two different commercially available fibrin
biomatrices regarding their effects on keratinocytes´ behavior and wound healing. We
characterized the two fibrin biomatrices regarding their cell compatibility with normal human
epithelial keratinocytes in several in vitro cell assays. Furthermore, the two materials were
tested in an excisional wound healing model in rats. Acc
epte
d A
rticl
e
5
This article is protected by copyright. All rights reserved.
Material and Methods
Fibrin Biomatrix
Fibrin sealants Artiss (FS A; Baxter AG, Vienna, Austria) and Evicel (FS E; Ethicon,
Sommerville, NJ, USA) comprise thrombin concentrations of 4 IU/ml (Artiss) and 800 - 1200
IU/ml (Evicel). Fibrinogen and thrombin were reconstituted according to the manufacturer´s
protocol. In brief, lyophilized sealer protein component of FS A was reconstituted in 3,000
KIE/ml aprotinin solution, the lyophilized thrombin component was reconstituted in 40 mM
CaCl2 solution. FS E (cryo kit) was warmed up to 37°C in a waterbath before use. For in
vitro clot formation, equal volumes of fibrinogen and thrombin components were mixed in a
tissue culture plate on a vortex mixer. Clots were incubated at 37°C for 1 hour for
polymerization.
Cell culture
Cryopreserved normal human epidermal keratinocytes (NHEK) were purchased from
PromoCell (Heidelberg, Germany). Cells were thawed and cultivated according to
manufacturer´s protocol at 37°C/5% CO2 and were cultivated until 70-80% confluence before
harvesting. Passages 3 to 6 were used for experiments.
Cell quantification by measurement of lactate dehydrogenase
NHEK were seeded on top of fibrin clots. Hirudin, a direct thrombin inhibitor, was used to
determine the effect of thrombin activity on cell proliferation. For cell quantitation on (fibrin-
bound) thrombin blocked matrices, clots were incubated with hirudin one hour prior cell
seeding as described in previous works (21).For PAR-1 blocking, NHEK were incubated with
75 nM SCH797979 (Santa Cruz Biotechnology, Inc., Santa Cruz, CA, USA), a selective
PAR-1 antagonist, for 30 minutes at 37°C before seeding. At selected time points, cells were
lysed with 9% TritonX-100. Lysate aliquots from each well were transferred into a 96 well Acc
epte
d A
rticl
e
6
This article is protected by copyright. All rights reserved.
plate and lactate dehydrogenase (LDH) was measured (CytoTox96 assay substrate mix,
Invitrogen, Carlsbad, CA, USA). Clots without cells served as controls.
Cell Viability
Cells were grown on top of fibrin biomatrix for 48 hours. For viability examination, cells
were incubated with calcein AM and ethidium homodimer-1 fluorescent dye solution
according to the manufacturer´s protocol (Live/Dead® viability/cytotoxicity kit for
mammalian cells; Invitrogen, Carlsbad, CA, USA). Microscopy was done on an
AxioObserver Z1 invert microscope (Zeiss, Jena, Germany). Red and green fluorescent
signals were quantified with a Plate Reader Synergy MX (Bio-Tek, Winooski, VT, USA) at
485 nm and 528 nm.
Apoptosis
Cells were seeded onto fibrin clots and activity of caspases 3 and 7 was measured after 4
hours by using a one-step fluorometric assay with caspase-labeling DEVD-Rhodamine110
substrate according to the manufacturer´s protocol (Homogeneous Caspases Assay®
, Roche
Applied Sciences, Basel, Switzerland). LDH assay was used to normalize the results to the
cell number.
Morphology of cells
Cells were grown on fibrin clots for 48 hours. After fixation (4% formaldehyde in PBS) and
permeabilization (0.9% TritonX-100), cells were stained with 10 µg/ml TRITC-
phalloidin/PBS and 5 µg/ml 4´,6-diamidino-2-phenylinol (DAPI) under light protection.
Microscopic analysis was done on an AxioObserver Z1 invert microscope (Zeiss, Jena,
Germany).
For ultrastructure analysis, fibrin clots were fixed in fixing solution containing 0.1 M
sodium cacodylate and 2.5% glutaraldehyde. Subsequently, clots were washed (0.1 M sodium
cacodylate without glutaraldehyde), dehydrated with an increasing series of alcohol and dried Acc
epte
d A
rticl
e
7
This article is protected by copyright. All rights reserved.
with hexamethyldisilazane. Clots were sputter coated with palladium gold in an Emitech
(Molfetta, Italy) sputter coater SC7620 and analyzed in a scanning electron microscopy
(SEM) Jeol 6510 (Jeol Ltd, Tokyo, Japan).
Ethics Statement
The in vivo experimental protocol was approved by the Animal Protocol Review Board of
Vienna, Austria (Approval Nr. M58/004157/2010/9). All surgery was performed under
anesthesia, and all efforts were made to minimize suffering (22).
Surgical procedure and animal treatment
Male Sprague Dawley rats (350 – 450 g) were purchased from Charles Rivers Laboratories.
After initial inhalation narcosis with 2.5% isoflurane, anesthesia was maintained by 110
mg/kg ketaminhydrochloride and 12 mg/kg xylazin intraperitoneal. Rats were shaved,
depilated and disinfected on the back. Two circular full-thickness excisions with a diameter of
1.3 cm were set paravertebral. One excision was treated, the other one on the contra-lateral
side remained untreated as internal control. Both wounds were covered by a transparent
wound film (Opsite, Smith and Nephew) and a Fixomull® stretch dressing (BSN Medical,
Hamburg, Deutschland) which was changed on day three and when necessary. As analgesic
treatment, all animals received 1.25 mg/kg Butorphanol s.c. and 0.15 mg/kg Meloxicam 5
mg/ml s.c. after operation and 0.15 mg/kg Meloxicam 5 mg/ml s.c. for three days post-
operative. Animals were housed in pairs, maintained at 22–24°C with a 12-hours light/dark
cycle and allowed food and water ad libitum.
Rats were divided into two groups (n=10), one treated with FS A (Artiss, Baxter; 4
IU/ml thrombin) one treated with FS E (Evicel, Omrix, 820 IU/ml thrombin). For clot
formation in vivo, fibrinogen and thrombin were filled into 1 ml syringes each and put into a
syringe holder with a mixing piece to get a homogeneously mixed fibrin-thrombin-compound.
150 µl of fibrin matrix was applied to the wound and let polymerize for two minutes. Acc
epte
d A
rticl
e
8
This article is protected by copyright. All rights reserved.
After seven days, rats were sacrificed by an intra-cardial injection of an overdose barbiturate.
For histological analysis, tissue was fixed in 3% phosphate-buffered formalin for 48 hours,
dehydrated and embedded in paraffin. Tissue from the wound area was stored in liquid N2 for
protein analysis.
Planimetry
To measure wound closure, excisional wounds were traced on a transparent acrylic sheet after
surgery and on day 3 and 7 post-OP. Sheets were digitalized and initial as well as residual
open wound areas were further analyzed with a ChemiDoc XRS (BioRad) with QuantityOne
4.6.3.
Histomorphometry
Excisional wounds were fixed in 3% neutrally buffered formalin for 24-48 hours. Then,
samples were cut with a microtome blade exactly in the middle of the wound (paramedian).
After embedding in paraffin, 3 µm tissue sections were cut, de-paraffinized and stained. After
hematoxylin and eosin (HE) staining, slides were scanned with an Olympus BX51 scanning
microscope, photographed with an Olympus XC10 camera and manually measured with the
program dotSlide2.3. Parameters for histomorphometry were used and calculated as described
in Lemo et al. (108). S: distance between the borders of the wound (last keratinocyte); L:
length of re-epithelialization zone; D: depth of the wound from S to deepest point of the
wound; T: thickness of the connective tissue (residual dermis or new dermis); N: thickness of
the natural dermis N=D+T; Superficial Contraction Index SCI = (L-S)/L: Deep Contraction
Index DCI = (N-D)/N; Wound Severity Index WSI = (N-T)/N; Wound Contraction Index
WCI: SCI+DCI; Global Healing Index GHI: SCI+DCI-WSI.
Immuno-histochemistry for angiogenesis
Endogenous peroxidase was blocked by incubation with H2O2 and epitope retrieval was
performed by proteinase K treatment or steaming using a conventional vegetable steaming Acc
epte
d A
rticl
e
9
This article is protected by copyright. All rights reserved.
device (Braun GmbH, Kronberg/Taunus, Germany). Then, tissue sections were stained with a
mouse anti-α smooth muscle actin (SMA, Sigma-Aldrich, St. Louis, MO) or a rabbit anti-
human von Willebrand factor (vWF, DakoCytomation, Glostrup, Denmark) followed by a
nucleus counter staining with Mayer’s Hemalaun, dehydration and permanent mounting.
Microscopy was done on an Olympus BX51, photographed with an Olympus XC10 and
measured with the program dotSlide2.3 or on a Zeiss Observer.Z1 invert microscope and
evaluated with the program AxioVision 4.8.0.
Angiogenic potential and inflammation
For measuring the level of inflammation, additional animals were treated as described above
with FS A and FS E and sacrificed on day two. Five rats per group were randomly treated
either with FS A or FS E. In three rats both wounds remained untreated as control. On day 2,
biopsies were taken from the wound area and from healthy tissue of the back 4 cm caudal of
the FS A and FS E treated wounds. The tissue was lysed in 2% Triton X-100 containing
phosphatase and protease inhibitors at 4°C for 4 hours and was periodically homogenized
during this time. Protein concentration of the lysates was measured by a DC-protein assay
(BD Biosciences, San Jose, CA, USA).
Proteins were examined on 10% Bis-Tris SDS PAGE gels (Invitrogen, Carlsbad, CA,
USA). Primary antibodies VEGF-A, IL-1α, and ERK1/2 (all Santa Cruz Biotechnology, Inc.,
Santa Cruz, CA, USA) were diluted and the blots were incubated at 4°C overnight. Secondary
antibodies used: IRDye® goat-α-rabbit 800 nm, IRDye
® goat-α-mouse 680 nm (LI-COR,
Lincoln, NE, USA). Signal detection was monitored with an Odyssey imaging system from
LI-COR (Lincoln, NE, USA). VEGF and IL-1α signals were normalized with total ERK1/2
signal.
Fibrin degradation in vivo Acc
epte
d A
rticl
e
10
This article is protected by copyright. All rights reserved.
For fibrin degradation studies FS A and FS E were mixed with 150 µg/ml human fibrinogen
conjugates Alexafluor 546 (Molecular Probes, Eugene, OR, USA). Matrix application was
done as described above. In one wound FS A was applied and FS E on the contra-lateral side
of the same rat. Fluorescence was measured on days 0, 1, 2, 3, 4, 6, 8, 9, 10 and 13 in a
Maestro Multispectral Imaging Device (PerkinElmer, Waltham, MA, USA).
Statistics
Data are presented as mean ± SEM of at least three independent experiments. Statistical
analysis was performed with software MiniTab 15. Statistical comparison for all experimental
settings was based on two sample t-test, ANOVA or General Linear Model using Tukey’s test
with p < 0.05 considered as significant.
Results
Fibrin biomatrices FS A and FS E were tested for cell compatibility with primary human
epithelial keratinocytes (NHEK). Cells were seeded on these fibrin sealant clots. After 4
hours, 24 hours and 48 hours cell proliferation was measured, after 48 hours, morphology and
viability staining was performed.
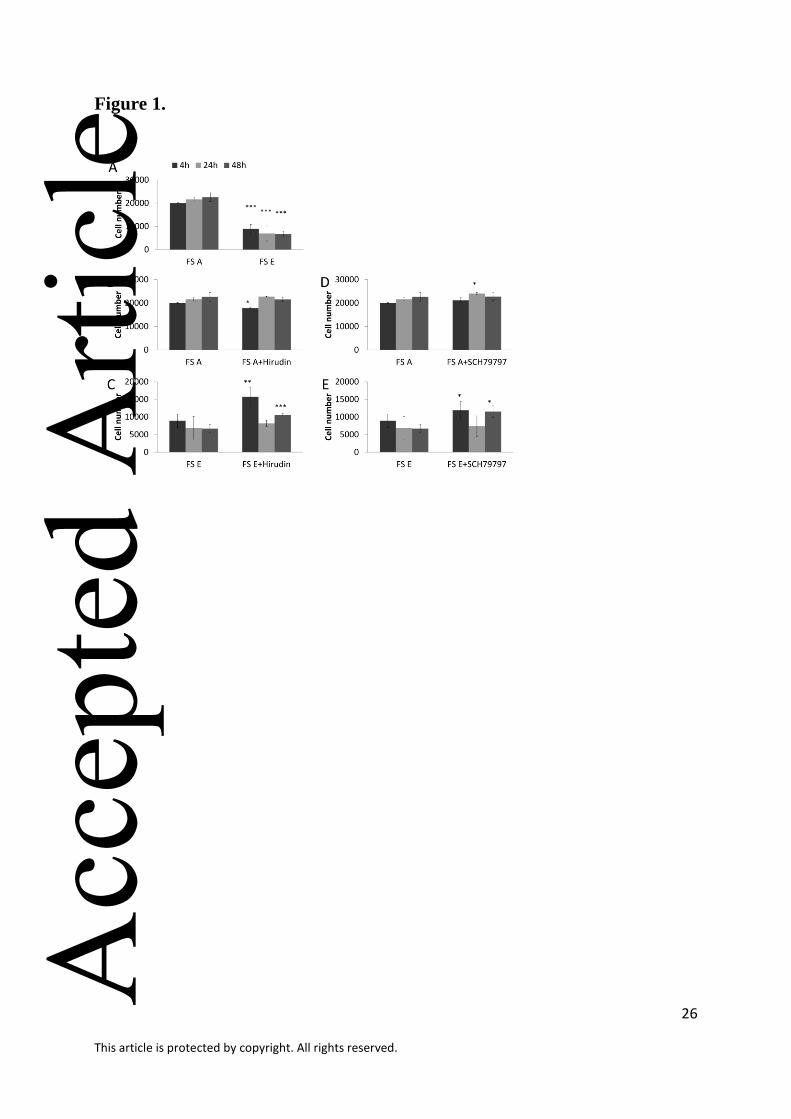
Proliferation of cells was evauluated using an LDH assay. On FS E clots, significant lower
cell numbers were measured at all three time points (-66.48% after 48 hours; p<0.000 for 4,
24 and 48 h) compared to FS A, indicating a higher proliferation rate of NHEK on FS A clots
(Figure 1 A).
To block fibrin bound thrombin, clots were incubated with hirudin before cell seeding.
By this thrombin blocking a recovery of cell proliferation could be observed in FS E clots
whencompared to untreated FS E clots.After 4 hours 33.9% more cells were counted than on Acc
epte
d A
rticl
e
11
This article is protected by copyright. All rights reserved.
FS E clots with intact thrombin activity (p=0.001) and therefore 78.5% compared to FS A.
After 24 hours, no significant better proliferation was measured (p=0.309) but after 48 hours
19.5% (p<0.000) more cells were counted on blocked FS E clots (Figure 1 C). Cell numbers
on FS A clots treated with hirudin varied between 10.7% less compared to clots without
hirudin treatment (time point 4 hours; p=0.033) and 5.2% more cells (24 hours; p=0.161)
(Figure 1 B). To confirm this diminishing effect of thrombin on keratinocyte proliferation, the
thrombin receptor PAR-1 was blocked with with SCH79797, a specific PAR-1 antagonist. FS
A and FS E clots (not blocked with hirudin) were seeded with keratinocytes with and without
SCH79797 treatment. Significantly more cells with blocked PAR-1 were measured after 4
(p=0,041) and 48 hours (p=0,024) on FS E clots compared to untreated cells (Figure 1 E). On
FS A a higher number of PAR-1 blocked cells attached after 24 hours (p=0,038) while there
were no differences at the other time points (Figure 1 D).
To show cell viability, live/dead staining of NHEK on clots was performed. After 48
hours, 2.9% (± 1.2) dead cells were found on FS A clots compared to 17.5% (± 8.3) on FS E
clots. To assess whether these dead cells were caused by apoptotic events, caspase 3/7 activity
was examined 4 hours after cell seeding. The caspase 3/7 activity level was nearly three-fold
higher (292% ± 79%) in cells grown on FS E clots (set to 100 %) indicating an induction of
apoptosis by high level of thrombin in the FW E fibrin matrix.
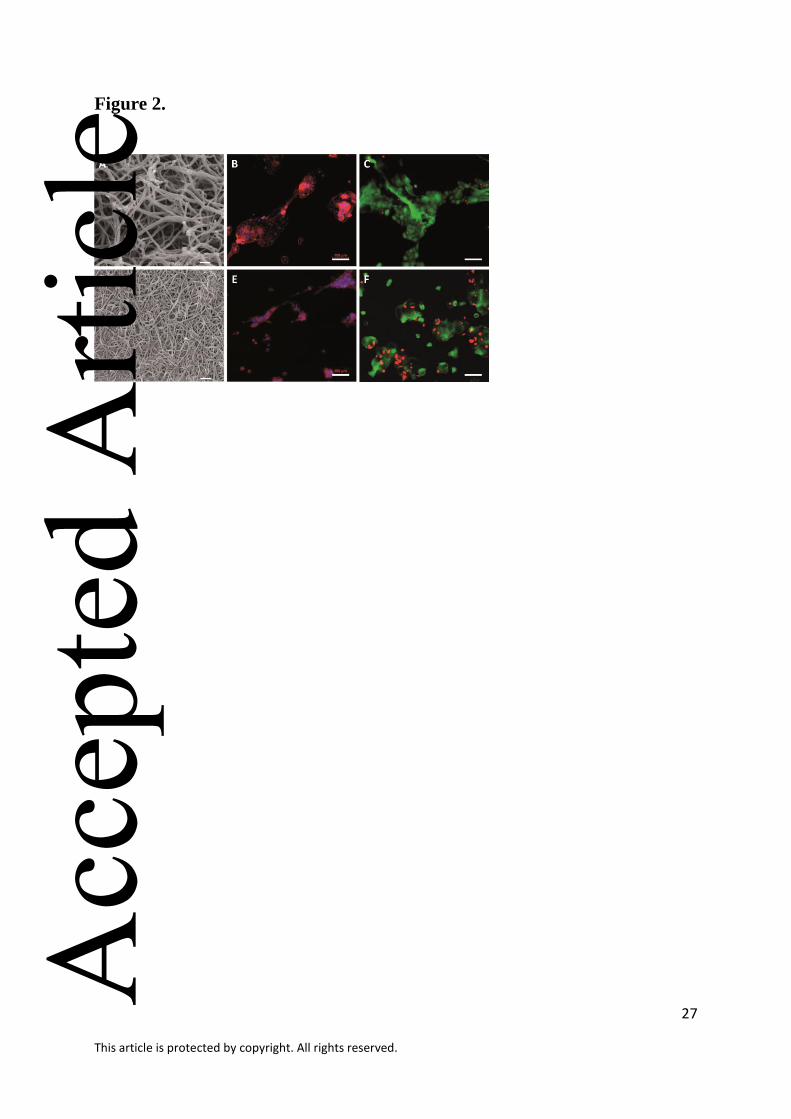
The ultrastructure of the fibrin biomatrices showed large differences in fiber density
between FS A and FS E (Figure 2). The material with higher thrombin content (FS E) formed
a tighter network than the loose mesh of FS A. Phalloidin/DAPI staining showed deteriorated
cell morphology and minimal spreading of NHEK when grown 48 hours on FS E clots.
Live/dead staining of cells show more dead cells (red stained) in FS E clots.
To analyze the impact of different fibrin matrices on wound healing, FS A and FS E
biomatrices were applied to excisional wounds (13 mm in diameter) on the back of rats. To Acc
epte
d A
rticl
e
12
This article is protected by copyright. All rights reserved.
estimate wound closure, wound area was measured via planimetry. A decrease of wound area
of 77% was observed in the FS A treated group after 7 days (significant wound closure
between day 0 and day 3). Rats treated with FS E had a decrease of wound area of 24% after 7
days (Figure 3).
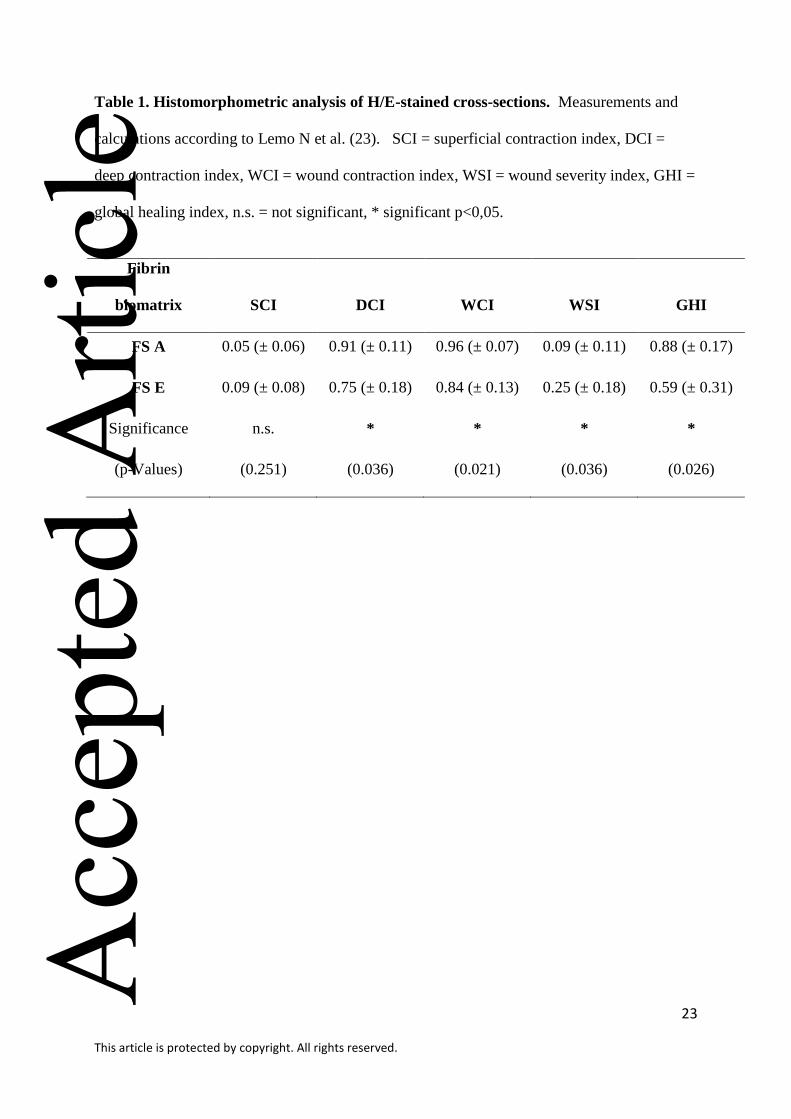
Advances in wound healing (wound contraction, wound severity, granulation and
global healing in general) were measured on day 7 by histomorphometric analysis according
to Lemo et al. (23). The Global Healing Index considers wound contraction as well as the
depth and is therefore a better index to evaluate the severity of the wound. A high GHI
indicates a better wound healing. The results showed a significantly lower GHI in the FS E
treated group compared to the FS A group and therefore indicate a less advanced wound
healing (Table 1). The superficial contraction index SCI showed no significant differences
between the groups, whereas FS A treated wounds had a significantlygreater deep contraction
compared to FS E treated wounds. Also the wound contraction index, which considers both
kinds of contractions, is significantly higher with FS A treatment, presumably as a result of
more contracted wounds. Concerning the wound severity index which regards the depth of the
wound and the new formed granulation tissue in relation to the thickness of the natural
healthy dermis, FS E treated wounds were calculated as significantly more severe compared
to FS A treated wounds.
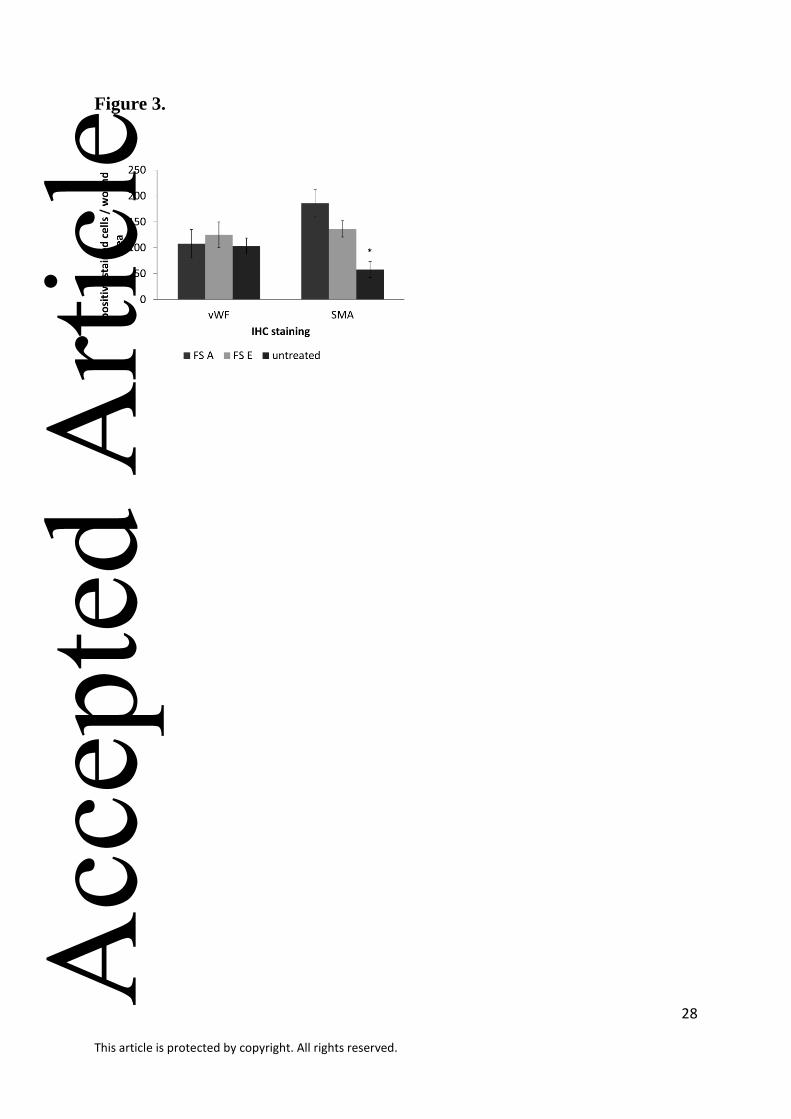
Immunohistochemcial staining against the endothelial marker smooth muscle actin
showed a higher number of positive vessels in the wound area of groups treated with fibrin
matrix compared to the untreated control (Figure 4 and 5). Treatment with FS A leaded to a
higher number of newly formed functional vessels in the wound area compared to FS E.
Regarding vWF positive vessels, no significant differences could be detected.
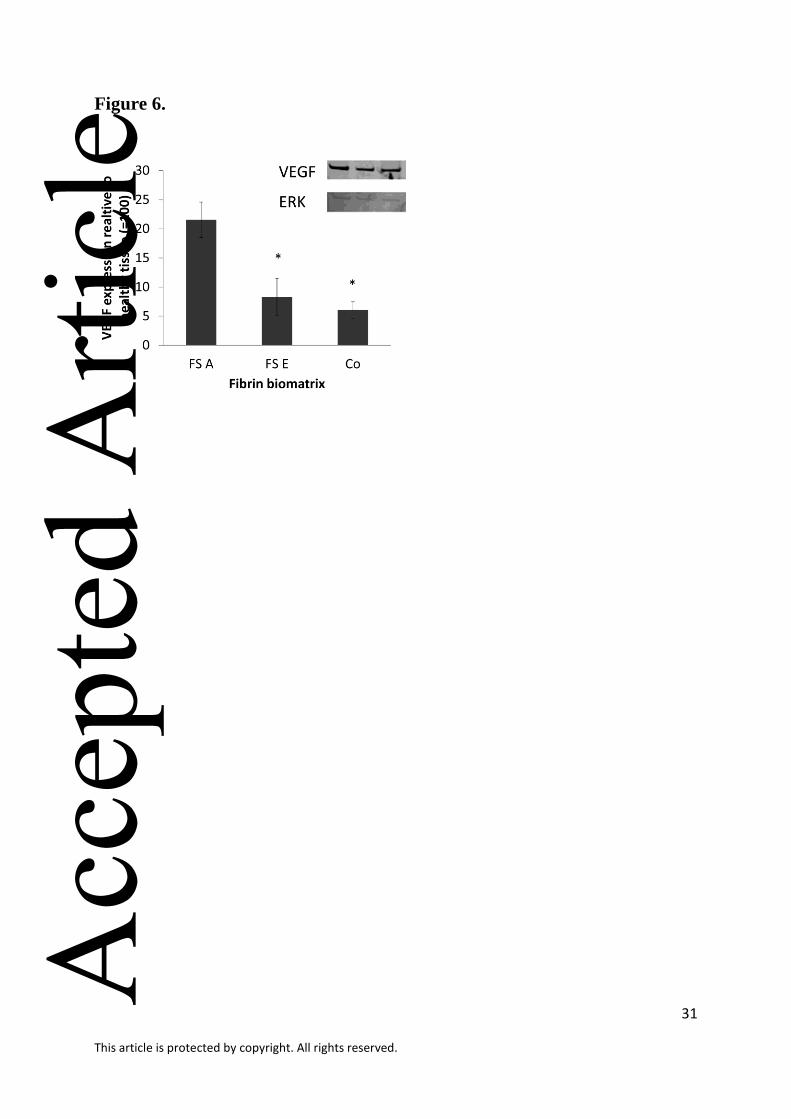
For VEGF-expression analysis, biopsies of FS A and FS E treated wounds as well as
untreated wounds and healthy tissues were taken on day two. Compared to healthy tissue, all Acc
epte
d A
rticl
e
13
This article is protected by copyright. All rights reserved.
samples showed a lower level of VEGF expression in wounds (Figure 6). Furthermore, in
wounds treated with FS A, the level of VEGF was significantly higher than in FS E or
untreated wounds (p = 0.04 to FS E, 0.01 to control). These results indicate that FS A leads to
more vessel formation compared to the other groups but far less than in healthy tissue.
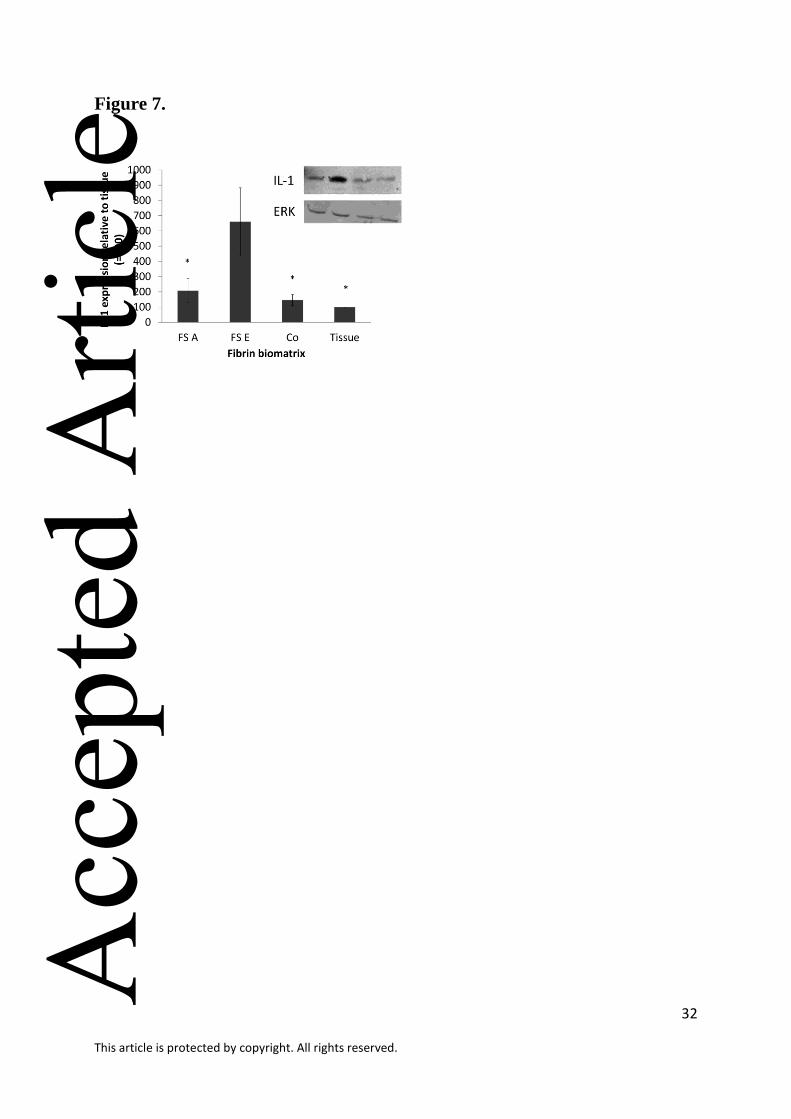
To detect the level of inflammation in the wounds, biopsies were taken from the
wound area of FS A and FS E treated wounds as well as untreated wounds and healthy tissue
on day 2. Wounds treated with FS E showed a 6.5-fold higher IL-1α expression on day 2 than
healthy tissue (p = 0.46). FS A and untreated wounds had a two-fold higher expression
compared to healthy tissue (p = 0.23) (Figure 7).
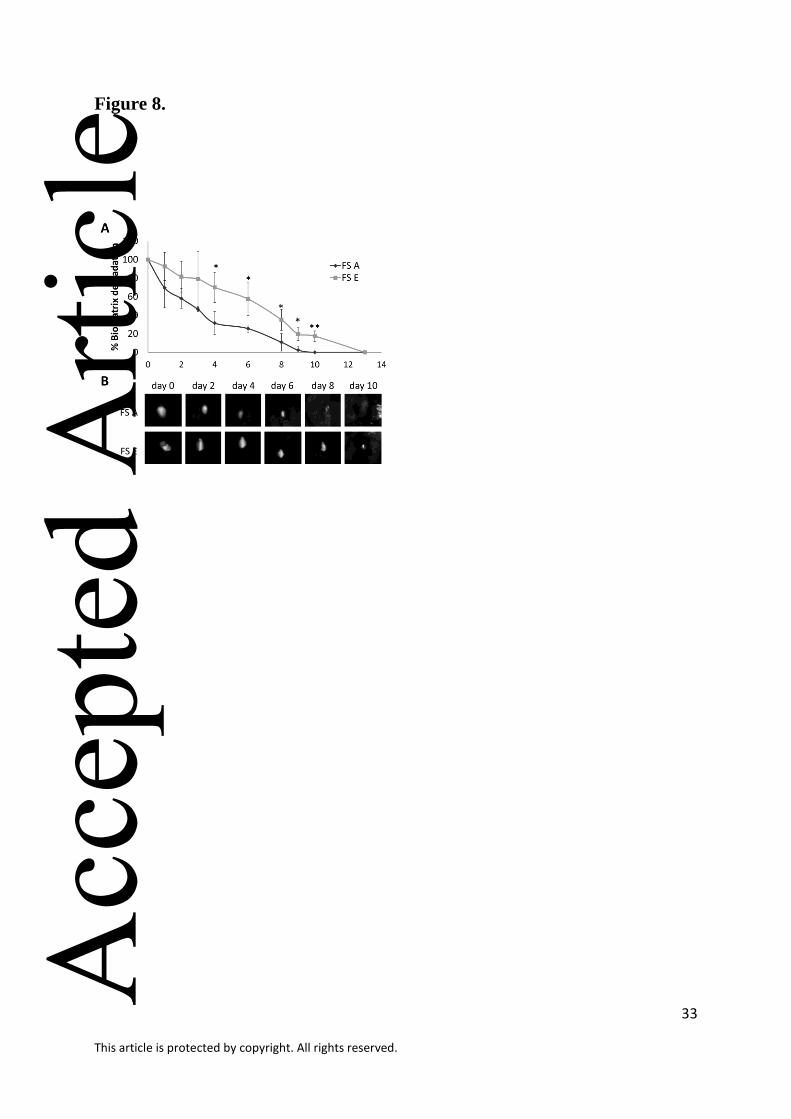
In vivo imaging of fibrin degradation of the biomatrices FS A and FS E was done by
using fluorochrome labeled fibrinogen (both matrices in one rat). The decrease of
fluorescence over time is directly associated with fibrin degradation. Four days post-surgery,
significant differences could be observed: FS A showed faster fibrin degradation compared to
FS E (Figure 8).
Discussion
The aim of this work was to compare the compatibility of two commercially available fibrin
biomatrices with cells involved in skin tissue repair: keratinocytes, fibroblasts and endothelial
cells (5). For tissue regeneration, the compatibility of fibrin with relevant cell types will be of
crucial importance for their application and performance in vivo.
There are several fibrin sealant products available in the market and often have been
used in surgery for years. They differ in their composition and every fibrin sealant product is
approved for its own indications, e.g. Tisseel and Evicel (FS E) in the US for hemostasis in
surgeries (see IFUs) or Artiss (FS A) in adhesion of autologous skin grafts especially in burn Acc
epte
d A
rticl
e
14
This article is protected by copyright. All rights reserved.
wounds or facelifts. Due to components like fibrinogen, thrombin, fibronectin, vitronectin,
and other growth factors, fibrin gels provide a bio-functional environment with beneficial
effects on the cell activities and tissue regeneration (20). Therefore, it has already been used
for various tissue engineering approaches and as matrix for cell or drug delivery (24, 25).
In this study, we compared the fibrin biomatrices FS A (with a low thrombin content
of 4 IU/ml) and FS E (with a high thrombin content of 800-1200 IU/ml) concerning their
effect on keratinocytes. Normal human epidermal keratinocytes (NHEK) on FS E showed less
adhesion and a deteriorated morphology. These results match with other published data
(26).Since concentrations of thrombin differ strongly between these two matrices,we
hypothesizethrombin could be the reason for deteriorated biocompatibility. The observed
effects could partly be reversed with the use of hirudin since significantly more cells were
detected on FS E clots after 4 and 48 hours. In this work we used hirudin, a direct thrombin
inhibitor, to block thrombin which may get in contact with the cells. Because of the blocking
efficiency of hirudin of about 80% (described by Weitz et al. (27) and affirmed by own
experiments (21)) matrix-bound thrombin partly remains active and therefore no full recovery
could be expected. Thrombin mainly acts as signaling molecule by direct binding to PAR-1 or
PAR-3 expressed on the surface of keratinocytes(28). Therefore, PAR-1 was blocked by
SCH79797 and also in this case, cell adhesion after four hours and viability of NHEK after 48
hours on FS E were significantly better compared to cells without SCH79797 treatment. This
also indicates – as the experiments with hirudin – that thrombin has an important influence on
cell compatibility with the fibrin sealant clot.
Thrombin directly binds to PAR-1 or PAR-3 expressed on the surface of keratinocytes
or other cell types (28).Fibrin bound thrombin activates PAR-1 and can induce cell
proliferation (29) but also can increase cell apoptosis (30) which often is accompanied by pro-Acc
epte
d A
rticl
e
15
This article is protected by copyright. All rights reserved.
inflammatory events (31). The threshold concentration of thrombin which results in negative
effects depends on the concentration and cell type (32, 33).
We were able to show that higher thrombin levels trigger apoptosis in keratinocytes. A
live/dead stain showed more dead cells after 48 hours in FS E compared with cells on FS A
and activity of caspase 3 and 7 – key proteins in apoptosis pathway (34) – was nearly three
times higher in cells grown on FS E. Our results impressively show clear differences in cell
behavior and cell compatibility with low and high thrombin concentrations. But as fibrin
sealant products do not only differ in thrombin concentration but also in fibrinogen
composition with its various constituents effects cannot be solely attributed to thrombin
because of the interaction and interplay of many factors.
Fibrin materials serve as temporal scaffolds for cells involved in wound healing and
are often used as matrix for cell or drug delivery (24), especially in research. Therefore, the
next step after our in vitro experiments was to evaluate our data in an in vivo wound healing
model. We chose the rat excisional wound healing model because rats provide an excellent
model for skin wound healing by allowing the standardization of the type, size, shape, and
depth of the wound injury (35).
To measure wound closure, the wound area was sized on day 0 (baseline), day 3 and
day 7. Wound area of FS E on day 3 seemed to be smaller by trend than on day 7, possibly be
due to initial stronger contraction of wounds of the subcutaneous panniculus carnosus muscle
in rats. For histomorphometric analyses, cross sections of the wounds were stained and
measured, and indices for wound characterization were calculated (23). Contraction was
distinguished in superficial (SCI) and deep contraction (DCI) because of the above mentioned
wound closure via panniculus carnosus. Results were not significant but by trend, FS A
showed more contraction compared to the FS E group. This correlates with the reduction of
wound area. The planimetric analyses also showed less wound closure at FS E. This could be Acc
epte
d A
rticl
e
16
This article is protected by copyright. All rights reserved.
a result of higher clot stiffness that spreads the wound open and could be due to lower
plasminogen-driven fibrin degradation. Also the denser alignment of fibers in the matrix of
FS E could be a reason for the slow wound closure preventing cells to migrate into the clot
and therefore retarded fibrinolysis. The indices of severity and wound healing did not differ
significantly. Only by trend FS A had a faster wound healing compared to the FS E group.
An important step in wound healing is vascularization of the newly formed tissue to
ensure its supply of nutrition and oxygen. To analyze new vessel formation, cross sections of
the wounds were stained immuno-histochemically for vWF to look at the endothelium of
vessels in general and for SMA to show more differentiated, functional vessels. vWF was
used for vessel staining although this staining allows only limited predication as it is too
unspecific. Also other tissue components can be vWF-positive: vWF is present in plasma, in
the subendothelial matrix of the vessel wall, and in the alpha-granule in megakaryocytes and
platelets derived from them (36). This could be the reason for the observation of no
significant differences in vWF-staining between the groups. Concerning the SMA-staining,
the fibrin treated groups had more vessel formation compared to the untreated group without
matrix. Within the biomatrix treated groups, FS A formed a higher number of functional
vessels within the wound area, FS E showed a less initiated SMA-positive vessel formation.
Further, also the vascularization marker VEGF was analyzed by Western blot analysis. In
wounds proteins like VEGF are secreted by cells in phase two of wound healing in order to
trigger angiogenesis (37). In the present study, wounds treated with FS A contained a
significant higher amount of VEGF compared to FS E or untreated wounds.
As inflammation is the first phase of wound healing (37) biopsies were taken on day
two because the main effectors of inflammation are expressed between day one and four after
injury (38). One of the most important effectors in this phase is the interleukin family,
especially interleukin-1 (37). Western blot analyses showed a significant higher expression of Acc
epte
d A
rticl
e
17
This article is protected by copyright. All rights reserved.
IL-1 in the wound edge in FS E treated wounds compared to FS A or untreated wounds or to
healthy tissue. Comparing FS A and FS E, pathological observations of HE-stained cross-
sections of the wound found a higher number of polymorphonuclear leukocytes and foreign-
body giant cells, cells typical for inflammation (data not shown). This could be a reason for
higher inflammation marker IL-1 (or vice versa).
To analyze fibrinolysis in vivo, fluorescent dye labeled fibrin matrices FS A and FS E
were applied on excisional wounds in rats. Degradation was measured over time and after
four days FS A clots were significantly smaller than FS E clots and completely degraded after
about ten days whereas FS E clots could be detected until day 15. As shown in the
ultrastructure results (Figure 2) the FS E matrix is denser than the FS A matrix. This denser
fiber arrangement could retard cell migration into the matrix and therefore decelerate the
release of enzymes produced by several cells. Furthermore, tPA/plasminogen is the main
player in fibrinolysis in vivo. In the FS E product, the plasminogen amount is reduced to
decelerate fibrin degradation which prolongs the shelf life of the product. As a consequence
also natural fibrinolysis is prolonged. In FS A products the protease aprotinin is added to
achieve this but can diffuse out of the clot in the first hours or days, so fibrin degradation in
the wound is possible. Here we raise the question if faster – more physiological? –
degradation is desirable to afford faster development of granulation and scar tissue.
In this study we compared two different fibrin biomatrices regarding their effects on
keratinocyte´s behavior and wound healing in an excisional wound healing model in rats. We
could show the effect of two different fibrin matrices on keratinocytes in vitro and found that
high thrombin concentrations have a negative effect on proliferation and viability of normal
human epidermal keratinocytes. In vivo we found faster wound closure, increased
vascularisation and faster degradation in FS A (low thrombin concentration)compared to FS E
(high thrombin concentration). However, since analyses were done with two different Acc
epte
d A
rticl
e
18
This article is protected by copyright. All rights reserved.
commercially available materials it cannot be excluded that other unknown factors influenced
the results. Nevertheless, our findings show that fibrin formulations influence cellular reaction
and wound healing and suggest that the choice of a certain fibrin matrices should be
dependent on the specific application.
ACKNOWLEDGMENTS
The authors would like to thank Dr. Wolfgang Öhlinger for the histological and pathological
expertise, Anna Hofmann for excellent technical skills and the Karl Donath Laboratory for
Hard Tissue and Biomaterial Research at the Bernhard Gottlieb University Clinic of Dentistry
for providing access to their Olympus dotSlide scanning microscope.
The research leading to these results has received funding from the FFG (Austrian
Research Promotion Agency) through the grant Eurostars project 5650 UGEN. The funding
source had no involvement in study design, in the collection, analysis and interpretation of
data, in the writing of the report and in the decision to submit the article for publication.Prof.
Dr. Heinz Redl served as consultant to Baxter Bioscience, Dr. Waltraud Pasteiner and Dr.
Andreas Goppelt were employed at Baxter Bioscience. All other authors do not have any
conflict of interest.
Acc
epte
d A
rticl
e
19
This article is protected by copyright. All rights reserved.
REFERENCES
1. Davie EW, Ratnoff OD. Waterfall Sequence for Intrinsic Blood Clotting. Science
1964;145(3638):1310-2.
2. Clark RA. Fibrin sealant in wound repair: A systematic survey of the literature. Expert
Opin Investig Drugs 2000;9(10):2371-92.
3. Laurens N, Koolwijk P, de Maat MP. Fibrin structure and wound healing. J Thromb
Haemost 2006;4(5):932-9.
4. Nurden AT. Platelets, inflammation and tissue regeneration. Thromb Haemost 2011;105
Suppl 1:S13-33.
5. Martin P. Wound healing--aiming for perfect skin regeneration. Science
1997;276(5309):75-81.
6. Brissett AE, Hom DB. The effects of tissue sealants, platelet gels, and growth factors on
wound healing. Curr Opin Otolaryngol Head Neck Surg 2003;11(4):245-50.
7. Eming SA, Brachvogel B, Odorisio T, Koch M. Regulation of angiogenesis: wound
healing as a model. Prog Histochem Cytochem 2007;42(3):115-70.
8. Staton CA, Brown NJ, Lewis CE. The role of fibrinogen and related fragments in tumour
angiogenesis and metastasis. Expert Opin Biol Ther 2003;3(7):1105-20.
9. Werner S, Grose R. Regulation of wound healing by growth factors and cytokines.
Physiol Rev2003;83(3):835-70.
10. Grose R, Hutter C, Bloch W, Thorey I, Watt FM, Fassler R, et al. A crucial role of beta 1
integrins for keratinocyte migration in vitro and during cutaneous wound repair.
Development 2002;129(9):2303-15.
11. Santoro MM, Gaudino G. Cellular and molecular facets of keratinocyte reepithelization
during wound healing. Exp Cell Res 2005;304(1):274-86. Acc
epte
d A
rticl
e

20
This article is protected by copyright. All rights reserved.
12. Telgenhoff D, Shroot B. Further evidence of multifunctionality in the keratinocyte: The
endothelial protein C receptor. J Invest Dermatol 2005;125(6):xviii-xix.
13. Mankad PS, Codispoti M. The role of fibrin sealants in hemostasis. Am J Surg
2001;182(2 Suppl):21S-8S.
14. Currie LJ, Sharpe JR, Martin R. The use of fibrin glue in skin grafts and tissue-engineered
skin replacements: A review. Plast Reconstr Surg 2001;108(6):1713-26.
15. Michlits W, Mittermayr R, Schafer R, Redl H, Aharinejad S. Fibrin-embedded
administration of VEGF plasmid enhances skin flap survival. Wound Repair Regen
2007;15(3):360-7.
16. Roy S, Driggs J, Elgharably H, Biswas S, Findley M, Khanna S, et al. Platelet-rich fibrin
matrix improves wound angiogenesis via inducing endothelial cell proliferation. Wound
Repair Regen 2011;19(6):753-66.
17. Falanga V, Iwamoto S, Chartier M, Yufit T, Butmarc J, Kouttab N, et al. Autologous bone
marrow-derived cultured mesenchymal stem cells delivered in a fibrin spray accelerate
healing in murine and human cutaneous wounds. Tissue Eng 2007;13(6):1299-312.
18. Zimmerlin L, Rubin JP, Pfeifer ME, Moore LR, Donnenberg VS, Donnenberg AD.
Human adipose stromal vascular cell delivery in a fibrin spray. Cytotherapy
2013;15(1):102-8.
19. Wozniak G. Fibrin sealants in supporting surgical techniques: The importance of
individual components. Cardiovasc Surg 2003;11 (Suppl 1):17-21.
20. Buchta C, Hedrich HC, Macher M, Hocker P, Redl H. Biochemical characterization of
autologous fibrin sealants produced by CryoSeal and Vivostat in comparison to the
homologous fibrin sealant product Tissucol/Tisseel. Biomaterials 2005;26(31):6233-41.
Acc
epte
d A
rticl
e
21
This article is protected by copyright. All rights reserved.
21. Gugerell A, Schossleitner K, Wolbank S, Nurnberger S, Redl H, Gulle H, et al. High
thrombin concentrations in fibrin sealants induce apoptosis in human keratinocytes. J
Biomed Mater Res A 2012;100(5):1239-47.
22. Kilkenny C, Browne WJ, Cuthill IC, Emerson M, Altman DG. Improving bioscience
research reporting: the ARRIVE guidelines for reporting animal research. PLoS Biol
2010;8(6):e1000412.
23. Lemo N, Marignac G, Reyes-Gomez E, Lilin T, Crosaz O, Ehrenfest DM. Cutaneous
reepithelialization and wound contraction after skin biopsies in rabbits: A mathematical
model for healing and remodelling index. Veterinarski Arhiv 2010;80(5):637-52.
24. Nürnberger S, Wolbank S, Peterbauer-Scherb A, Morton TJ, Feichtinger GA, Gugerell A,
et al. Properties and Potential Alternative Applications of Fibrin Glue Biological Adhesive
Systems. In: Byern J, Grunwald I, editors.: Springer Vienna; 2010. p. 237-59.
25. Mann BK. Biologic gels in tissue engineering. Clin Plast Surg 2003;30(4):601-9.
26. Macasev D, Diorio JP, Gugerell A, Goppelt A, Gulle H, Bittner M. Cell compatibility of
fibrin sealants: In vitro study with cells involved in soft tissue repair. J Biomater Appl
2011;26(2):129-49.
27. Weitz JI, Hudoba M, Massel D, Maraganore J, Hirsh J. Clot-bound thrombin is protected
from inhibition by heparin-antithrombin III but is susceptible to inactivation by
antithrombin III-independent inhibitors. J Clin Invest 1990;86(2):385-91.
28. Artuc M, Hermes B, Algermissen B, Henz BM. Expression of prothrombin, thrombin and
its receptors in human scars. Exp Dermatol 2006;15(7):523-9.
29. Smadja DM, Basire A, Amelot A, Conte A, Bieche I, Le Bonniec BF, et al. Thrombin
bound to a fibrin clot confers angiogenic and haemostatic properties on endothelial
progenitor cells. J Cell Mol Med 2008 Jun;12(3):975-86. Acc
epte
d A
rticl
e
22
This article is protected by copyright. All rights reserved.
30. Chin AC, Vergnolle N, MacNaughton WK, Wallace JL, Hollenberg MD, Buret AG.
Proteinase-activated receptor 1 activation induces epithelial apoptosis and increases
intestinal permeability. Proc Natl Acad Sci U S A 2003;100(19):11104-9.
31. Bae JS, Kim YU, Park MK, Rezaie AR. Concentration dependent dual effect of thrombin
in endothelial cells via Par-1 and Pi3 Kinase. J Cell Physiol 2009;219(3):744-51.
32. Striggow F, Riek M, Breder J, Henrich-Noack P, Reymann KG, Reiser G. The protease
thrombin is an endogenous mediator of hippocampal neuroprotection against ischemia at
low concentrations but causes degeneration at high concentrations. Proc Natl Acad Sci U
S A 2000;97(5):2264-9.
33. Furuhashi I, Abe K, Sato T, Inoue H. Thrombin-stimulated proliferation of cultured
human synovial fibroblasts through proteolytic activation of proteinase-activated receptor-
1. J Pharmacol Sci 2008;108(1):104-11.
34. Li P, Nijhawan D, Budihardjo I, Srinivasula SM, Ahmad M, Alnemri ES, et al.
Cytochrome c and dATP-dependent formation of Apaf-1/caspase-9 complex initiates an
apoptotic protease cascade. Cell 1997;91(4):479-89.
35. Dorsett-Martin WA. Rat models of skin wound healing: a review. Wound Repair Regen
2004;12(6):591-9.
36. Franchini M, Lippi G. Von Willebrand factor and thrombosis. Ann Hematol
2006;85(7):415-23.
37. Singer AJ, Clark RA. Cutaneous wound healing. N Engl J Med 1999;341(10):738-46.
38. Enoch S, Grey JE, Harding KG. Recent advances and emerging treatments. BMJ
2006;332(7547):962-5.
Acc
epte
d A
rticl
e
23
This article is protected by copyright. All rights reserved.
Table 1. Histomorphometric analysis of H/E-stained cross-sections. Measurements and
calculations according to Lemo N et al. (23). SCI = superficial contraction index, DCI =
deep contraction index, WCI = wound contraction index, WSI = wound severity index, GHI =
global healing index, n.s. = not significant, * significant p<0,05.
Fibrin
biomatrix SCI DCI WCI WSI GHI
FS A 0.05 (± 0.06) 0.91 (± 0.11) 0.96 (± 0.07) 0.09 (± 0.11) 0.88 (± 0.17)
FS E 0.09 (± 0.08) 0.75 (± 0.18) 0.84 (± 0.13) 0.25 (± 0.18) 0.59 (± 0.31)
Significance n.s. * * * *
(p-Values) (0.251) (0.036) (0.021) (0.036) (0.026)
Acc
epte
d A
rticl
e
24
This article is protected by copyright. All rights reserved.
FIGURE LEGENDS
Figure 1: Cell proliferation: cell numbers of attached NHEK on FS A and FS E fibrin clots
(A) +/- treated with hirudin (B, C) and +/- SCH79797 treatment (D, E). Cell number was
evaluated after 4, 24 and 48 hours of incubation by LDH assay. Significances are relative to
FS A (A) and to untreated samples (B-E). * p<0,05; ** p<0,01; *** p<0,001
Figure 2: SEM analysis of FS A and FS E fibrin clots (A, D). Morphology of NHEK after 48
hours (B, E), red stain indicates cytoskeleton, blue stain represents cell nuclei. Live/dead
staining of NHEK on FS A and FS E fibrin clots after 48 hours cultivation (C, F), green stain
(Calcein AM) indicates living cells and red stain (Ethidium Homodimer 1) indicates dead
cells. FS A: A, B, C; FS E: D, E, F. Size bars: 1 µm (A, D), 100 µm (B, E), 200 µm (C, F).
Figure 3: Wound closure: planimetry of wounds treated with FS A and FS E. Day 0 was set
as 100%, standard error is shown. Significances are relative to day 0. * p<0,05
Figure 4: Immuno-histochemical analysis: von Willebrand factor and smooth muscle actin
staining (vascularization) on day 7. Significances are relative to FS A. * p<0,05
Figure 5: Immuno-histochemical staining: smooth muscle actin (A,B) and von Willebrand
factor (C, D) on day 7 in FS A (A, C) and FS E (B, D) treated wounds.
Figure 6: Western blot analysis of VEGF-A expression in biopsies taken from excisional
wounds treated with FS A or FS E on day 2. As control, untreated wounds wereinvestigated.
The graph shows the mean of five independent Western blots, one representative blot is
shown. Significances are relative to FS A. * p<0,05
Acc
epte
d A
rticl
e
25
This article is protected by copyright. All rights reserved.
Figure 7: Western blot analyses of IL-1 expression in biopsies taken from excisional wounds
treated with FS A or FS E on day 2. As controls, untreated wounds and healthy tissue was
observed. The graph shows the mean of four independent Western blots, one representative
blot is shown. Significances are relative to FS E. * p<0,05
Figure 8: Fibrin clot degradation of FS A and FS Ein vivo: fluorescence in excisional rat
wounds measured by placing rats in a Maestro Multispectral Imaging Device of representative
clots (B) and given in percent relative to day 0 (A). * p<0,05; ** p<0,01
Acc
epte
d A
rticl
e
26
This article is protected by copyright. All rights reserved.
Figure 1.
Acc
epte
d A
rticl
e
27
This article is protected by copyright. All rights reserved.
Figure 2.
Acc
epte
d A
rticl
e
28
This article is protected by copyright. All rights reserved.
Figure 3.
Acc
epte
d A
rticl
e

29
This article is protected by copyright. All rights reserved.
Figure 4.
Acc
epte
d A
rticl
e
30
This article is protected by copyright. All rights reserved.
Figure 5.
Acc
epte
d A
rticl
e
31
This article is protected by copyright. All rights reserved.
Figure 6.
Acc
epte
d A
rticl
e
32
This article is protected by copyright. All rights reserved.
Figure 7.
Acc
epte
d A
rticl
e
33
This article is protected by copyright. All rights reserved.
Figure 8.
Acc
epte
d A
rticl
e