Embed Size (px)
Citation preview

Cas clinique
DOI of or
Departmenpital, Dublin,
CorrespondSurgery, SainIrlande, E-ma
Ann Vasc Surghttp://dx.doi.or� Annals of V�Edit�e par ELS
Thrombose veineuse superficielle et profondeli�ee �a une absence cong�enitale de veine caveinf�erieure sous-h�epatique chez un jeunehomme
Donal B. O’Connor, Noel O’Brien, Tahir Khani, Stephen Sheehan, Dublin, Irlande
Rationnelle : L’absence cong�enitale de veine cave inf�erieure (AIVC) est une anomalie vas-culaire rare qui peut etre associ�ee �a des thromboses veineuses profondes (DVT). Elle estsous-rapport�ee et peut etre pr�esente chez jusqu’�a 5% des sujets jeunes ayant une DVT.Nous rapportons un cas isol�e de thrombose simultan�ee des veines superficielles et profondeschez un patient avec AIVC.M�ethodes et R�esultats : Un homme de 20 ans s’est pr�esent�e avec une histoire de deux semai-nes de membre inf�erieur gauche gonfl�e, douloureux. �A l’examen, la jambe et la cuisse gauches�etaient gonfl�ees et des varicosit�es �etaient pr�esentes le long de la paroi abdominale inf�erieure.L’�echo-D€oppler montrait une thrombose veineuse superficielle et profonde �etendue du membreinf�erieur gauche. Le phl�ebo-scanner montrait une AIVC sous-h�epatique avec un drainage dumembre inf�erieur par les veines azygos et h�emi-azygos dilat�ees. Le patient �etait mis sous trai-tement anticoagulant oral et allait bien avec un suivi de six mois.Conclusion : L’hypoth�ese d’une DVT chez les patients avec une AIVC est que le drainage vei-neux des membres inf�erieurs est insatisfaisant, avec une stase et une thrombose veineuses.Tous les jeunes patients se pr�esentant avec une DVT idiopathique devraient etre �etudi�espour des anomalies de la veine cave inf�erieure par tomodensitom�etrie si l’examen duplex nevisualise pas la veine cave inf�erieure.
Congenital absence of the inferior vena cava (AIVC)
is an uncommon but well described vascular ano-
maly. It may present as deep vein thrombosis
(DVT) or be diagnosed as an incidental finding on
computed tomography (CT) or magnetic resonance
imaging (MRI). It is a rare risk factor for DVT but
may be underreported because ultrasound (US)
iginal article: 10.1016/j.avsg.2011.02.027.
t of Vascular Surgery, Saint Vincent’s University Hos-Irlande.
ence : Donal B O’Connor, MD, Department of Vasculart Vincent’s University Hospital, Elm Park, Dublin 4,il: [email protected]
2011; 25: 697.e1-697.e4g/10.1016/j.acvfr.2012.07.001ascular Surgery Inc.EVIER MASSON SAS
may not be sufficient for diagnosis in some patients.
We report a unique case of AIVC presenting with
concurrent superficial and DVT.
CASE REPORT
A 20-year-old male building laborer presented to the
emergency department with a 2-week history of pro-
gressive pain and swelling in his left lower limb. In parti-
cular, he complained of pain and tenderness in the left
groin. The patient had never had these symptoms before
and had no history of varicose veins or venous ulceration.
He had no other medical or surgical history and was not
taking any medications. On examination, the left leg and
thigh were found to be swollen. There were prominent
tortuous palpable veins over the lower abdomen and both
left and right groins. There was bruising and tenderness
overlying the groin veins. DVT was diagnosed clinically
and duplex ultrasonography demonstrated extensive
743.e17
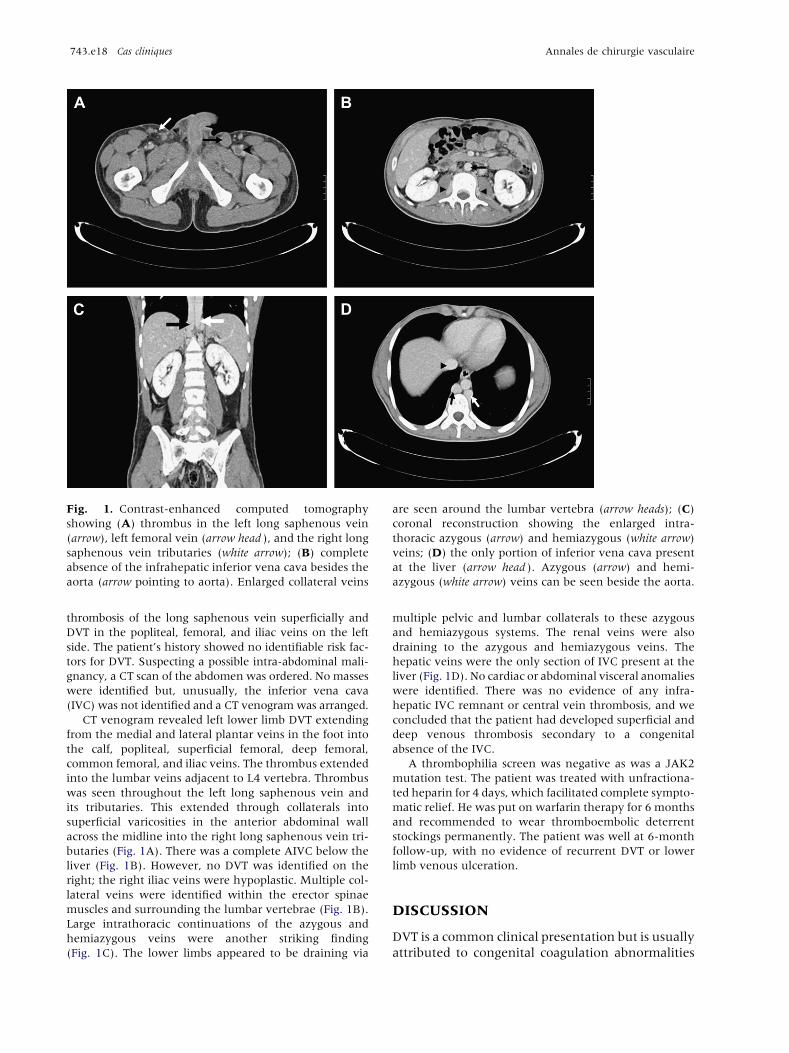
Fig. 1. Contrast-enhanced computed tomography
showing (A) thrombus in the left long saphenous vein
(arrow), left femoral vein (arrow head ), and the right long
saphenous vein tributaries (white arrow); (B) complete
absence of the infrahepatic inferior vena cava besides the
aorta (arrow pointing to aorta). Enlarged collateral veins
are seen around the lumbar vertebra (arrow heads); (C)
coronal reconstruction showing the enlarged intra-
thoracic azygous (arrow) and hemiazygous (white arrow)
veins; (D) the only portion of inferior vena cava present
at the liver (arrow head ). Azygous (arrow) and hemi-
azygous (white arrow) veins can be seen beside the aorta.
743.e18 Cas cliniques Annales de chirurgie vasculaire
thrombosis of the long saphenous vein superficially and
DVT in the popliteal, femoral, and iliac veins on the left
side. The patient’s history showed no identifiable risk fac-
tors for DVT. Suspecting a possible intra-abdominal mali-
gnancy, a CT scan of the abdomen was ordered. No masses
were identified but, unusually, the inferior vena cava
(IVC) was not identified and a CT venogram was arranged.
CT venogram revealed left lower limb DVT extending
from the medial and lateral plantar veins in the foot into
the calf, popliteal, superficial femoral, deep femoral,
common femoral, and iliac veins. The thrombus extended
into the lumbar veins adjacent to L4 vertebra. Thrombus
was seen throughout the left long saphenous vein and
its tributaries. This extended through collaterals into
superficial varicosities in the anterior abdominal wall
across the midline into the right long saphenous vein tri-
butaries (Fig. 1A). There was a complete AIVC below the
liver (Fig. 1B). However, no DVT was identified on the
right; the right iliac veins were hypoplastic. Multiple col-
lateral veins were identified within the erector spinae
muscles and surrounding the lumbar vertebrae (Fig. 1B).
Large intrathoracic continuations of the azygous and
hemiazygous veins were another striking finding
(Fig. 1C). The lower limbs appeared to be draining via
multiple pelvic and lumbar collaterals to these azygous
and hemiazygous systems. The renal veins were also
draining to the azygous and hemiazygous veins. The
hepatic veins were the only section of IVC present at the
liver (Fig. 1D). No cardiac or abdominal visceral anomalies
were identified. There was no evidence of any infra-
hepatic IVC remnant or central vein thrombosis, and we
concluded that the patient had developed superficial and
deep venous thrombosis secondary to a congenital
absence of the IVC.
A thrombophilia screen was negative as was a JAK2
mutation test. The patient was treated with unfractiona-
ted heparin for 4 days, which facilitated complete sympto-
matic relief. He was put on warfarin therapy for 6 months
and recommended to wear thromboembolic deterrent
stockings permanently. The patient was well at 6-month
follow-up, with no evidence of recurrent DVT or lower
limb venous ulceration.
DISCUSSION
DVT is a common clinical presentation but is usually
attributed to congenital coagulation abnormalities
Vol. 25, No. 5, 2011 Cas cliniques 743.e19
or acquired risk factors such as surgery or mali-
gnancy.1 The incidence is 1 per 1,000 patient-
years, but this is believed to be even less in those
aged <40 years.2 As a risk factor for DVT, AIVC is
believed to be very rare. A Medline search of
reports published between 1960 and 2009 found
only 23 cases. This may be an underestimation
because conventional compression scanning ultra-
sonography may not always detect intra-abdominal
venous anomalies. Three studies have reported the
incidence of AIVC to be as high as 5% in patients of
age <40 years presenting with ‘‘idiopathic’’ DVT.3-5
The IVC develops between weeks 6 and 8 of ges-
tation. The suprarenal portion is formed by the sub-
cardinal veins and the infrarenal portion by the
supracardinal veins. Aberrant development during
this period may result in IVC anomalies, including
AIVC. Absence of the suprarenal IVC is the more
common abnormality, whereas absence of the infra-
renal or entire infrahepatic, as in the case of this
patient, accounts for only 6% of all cases of AIVC.6
AIVC may remain asymptomatic and undetected
because a collateral deep venous system may be
sufficiently developed through the azygous and
hemiazygous systems to compensate for such ano-
malies. The hypothesis for DVT in patients with
AIVC is that despite these collaterals, venous drai-
nage of the lower limbs is inadequate leading to
venous stasis and thrombosis.
Some common features of the clinical presenta-
tion of AIVC have been identified from reviewing
previously published cases. The majority of cases
presented clinically as proximal DVT involving the
iliac and femoral veins. In two cases, venous ulcera-
tion secondary to chronic stasis without DVT deve-
loped.7,8 Patients with DVT associated with AIVC
are significantly younger than those without ana-
tomical anomalies. The mean age in the previously
published data is 30 years, as compared with 60
years in a large study of DVT in medical patients.9
More than half of the cases involved bilateral DVT,
which is higher than expected, particularly because
no case of AIVC to date has been associated with
underlying malignancy. As in the case of the patient
presented in this study, in cases of AIVC, lumbar and
spinal collaterals draining the iliac veins, usually, to
prominent azygous and hemiazygous veins, are
often seen on abdominal imaging. There have been
three reports of pulmonary embolus associated with
AIVC. It is hypothesized that enlarged azygous or
hemiazygous veins could act as conduits for emboli
to the pulmonary circulation.10-12
Thrombophilic disorders have been diagnosed in
approximately one-third of cases.13,14 It has been
suggested that AIVC is not because of a congenital
anomaly but instead occurs secondary to a perinatal
thrombosis causing regression of a previously nor-
mal IVC.15 There was no evidence for this in our
patient’s history or radiology. The absence of any
clotting defects or other predisposing history in both
our patient and in other cases3 supports the theory
that AIVC can be a true congenital agenesis rather
than an acquired defect. AIVC alone may be a suf-
ficient risk factor for DVT if collaterals are not suf-
ficiently developed to facilitate adequate blood
return leading to increased pressure and venous
stasis. Physical exertion has been identified as a risk
factor for DVT in patients with AIVC and pre-
cipitated the clinical presentation in five cases.13-16
Additional congenital anomalies have been diag-
nosed in five patients with AIVC and involved
aplasia or hypoplasia of the right kidney.17 This
association can be explained by embryogenesis
because the IVC drains the right metanephros and
therefore, complete or partial IVC absence could
affect renal development.
To our knowledge, this is the first reported case
of simultaneous superficial and DVT associated
with AIVC. It is possible that the initial thrombosis
occurred in the deep veins with secondary exten-
sion to the superficial system. The patient had signi-
ficant thrombus in the common femoral vein.
Occlusion of the saphenofemoral junction likely
precipitated the extension of thrombus into the
long saphenous vein and tributaries. This superficial
thrombosis was particularly symptomatic. The
patient developed anterior abdominal wall collate-
rals as a consequence of AIVC, and these facilitated
the extension of thrombus to the right limb super-
ficial veins.
US is the investigation of choice for any patient
with suspected DVT and can help visualize the iliacs
and intra-abdominal IVC. However, it may not
always permit examination of the retroperitoneal
veins, especially in obese patients, andwill therefore
miss some cases of AIVC. CT or magnetic resonance
imaging can readily diagnose AIVC.12,18 We would
like to propose that all patients with proximal DVT
without obvious risk factors should undergo abdo-
minal CT venogram to exclude AIVC if US has not
adequately demonstrated the IVC. Patients should
also be screened for thrombophilic disorders.
Oral anticoagulation is recommended for all
patients, but there is no evidence regarding optimal
duration of treatment. Patients have been treated
for 6-24 months without recurrence after 2 years
of follow-up.3,5 However, there have been two
reports of DVT recurrence after 1 and 2 years of
therapy.12 There are no studies with long-term fol-
low-up of patients, on or off treatment. Patients

743.e20 Cas cliniques Annales de chirurgie vasculaire
with extensive DVT should also be followed up cli-
nically in case they develop stasis ulcers.
To date, surgical management has been reserved
for the treatment of nonhealing ulcers. The two
successfully managed cases involved prosthetic
reconstruction of an absent infrarenal IVC7 and a
prosthetic graft bypass from the iliac to intrathoracic
azygous vein.8
Although rare, AIVC should be considered in all
younger patients with DVT in the absence of predis-
posing risk factors. Such patients require investiga-
tion with abdominal CT if the IVC is not visualized
with US.
REFERENCES
1. Rosendall FR. Venous thrombosis: a multicausal disease.
Lancet 1999;353:1167-1173.
2. Anderson FA, Wheeler HB, Goldberg RJ, et coll. A popula-
tion based perspective of the hospital incidence and case-
fatality rates of deep vein thrombosis and pulmonary
embolism, the Worcester DVT study. Arch Intern Med
1991;151:933-938.
3. Ruggeri M, Tosetto A, Castaman G, et coll. Congenital
absence of the inferior vena cava: a rare risk factor for
idiopathic deep-vein thrombosis. Lancet 2001;357:441.
4. Siragusa S, Anastasio R, Falaschi F, et coll. Congenital
absence of the inferior vena cava. Lancet 2001;357:1711.
5. Chee YL, Dominic J, Watson CG, et coll. Inferior vena cava
malformation as a risk factor for deep venous thrombosis in
the young. Br J Haematol 2001;114:878-880.
6. Shah NL, Shanley CJ, Prince MR, et coll. Deep venous
thrombosis complicating a congenital absence of the inferior
vena cava. Surgery 1996;120:891-896.
7. Tofigh AM, Coscas R, Koskas F, et coll. Surgical manage-
ment of deep venous insufficiency caused by congenital
absence of the inferior vena cava. Vasc Endovascular Surg
2008;42:58-61.
8. Dougherty MJ, Calligaro KD, DeLaurentis DA. Congenitally
absent inferior vena cava presenting in adulthood with
venous stasis and ulceration: a surgically treated case. J Vasc
Surg 1996;23:141-146.
9. Samama MM. An epidemiological study of risk factors for
deep vein thrombosis in medical outpatients: the Sirius
study. Arch Intern Med 2000;160:3415-3420.
10. D’Aloia, Faggiano P, Fiorina C, et coll. Absence of inferior
vena cava as a rare cause of deep vein thrombosis compli-
cated by liver and lung embolism. Int J Cardiol 2003;88:
327-329.
11. Cho BC, Choi HJ, Kang SM, et coll. Congenital absence of
the inferior vena cava as a rare cause of pulmonary
thromboembolism. Yonsei Med J 2004;45:947-951.
12. Takehara N, Hasebe N, Enomoto S, et coll. Multiple and
recurrent systemic thrombotic events associated with con-
genital anomaly of inferior vena cava. J Thromb Thrombo-
lysis 2005;19:101-103.
13. Gayer G, Luboshitz J, Hertz M, et coll. Congenital ano-
malies of the inferior vena cava revealed on CT in patients
with deep vein thrombosis. Am J Roentgenol 2003;180:
729-732.
14. Obernosterer A, Aschauer M, Schnedl W, et coll. Anomalies
of the inferior vena cava in patients with iliac venous
thrombosis. Ann Intern Med 2002;136:37-41.
15. Ramanathan T, Hughes TM, Richardson AJ. Perinatal infe-
rior vena cava thrombosis and absence of the infrarenal
inferior vena cava. J Vasc Surg 2001;33:1097-1099.
16. Dean SM, Tytle TL. Acute right lower extremity iliofemoral
deep venous thrombosis secondary to an anomalous vena
cava: a report of two cases. Vasc Med 2006;11:165-169.
17. Gayer G, Zissin R, Strauss S, et coll. IVC anomalies and right
renal aplasia detected on CT: a possible link? Abdom
Imaging 2003;28:395-399.
18. Ueda J, Hara K, Kobayashi Y, Ohue S, Udrida H. Anomaly of
the inferior vena cava observed by CT. Comput Radiol
1983;7:145-154.





























