Embed Size (px)
DESCRIPTION
a detailed description of the bethesda system for reporting thyroid cytopathlogy by dr. wakely
Citation preview

Updating Thyroid Cytopathology: The Bethesda SystemThe Bethesda System
P.E. Wakely, Jr., M.D.Ohio State UniversityC l b OhiColumbus, OhioU.S.A.

Thyroid Nodules NEJM June 2007
• FNA: the most specific & sensitive method to select suspicious nodules for surgerynodules for surgery
• in 10-20% of thyroid FNA a precise diagnosis cannot be reached

NCI Thyroid FNA State of The S i C fScience Conference
Bethesda, MDOctober, 2007October, 2007

Classification Scheme Proposed by 2006ATA 2006
• Inadequate • Non-Diagnostic / UNSATInadequate
li
Non-Diagnostic / UNSAT• Benign
AC S / S• Malignant • ACUS / FLUS• Suspicious for Neoplasm
• Indeterminate – Follicular– Hürthle
• Benign• Suspicious for Malignancy• Malignantg

Classification Scheme Proposed by 2006ATA 2006
• Inadequate • Non-Diagnostic / UNSATInadequate
li
Non-Diagnostic / UNSAT• Benign
AC S / S• Malignant • ACUS / FLUS• Suspicious for Neoplasm
• Indeterminate – Follicular– Hürthle
• Benign• Suspicious for Malignancy• Malignantg

Clinical Management Algorithms
• Benign • FLUS–follow
• Suspicious– repeat FNAN di ti• Suspicious
–surgery• Non-diagnostic
(includes “cyst fluid • Malignant
surgery
only”)– repeat FNA–surgery repeat FNA
• usually after 3 monthsmonths

• This is not a• This is not a “standard of
i id lipractice” guideline nor is it endorsed as such by the NCI.

NCI/Bethesda Conference - Suggested Terminology for Reporting Thyroid FNA
• Nondiagnostic/ UnsatisfactoryNondiagnostic/ Unsatisfactory

Adequacy - according to the literatureAdequacy according to the literature
• 6 groups each ≥10 benign follicular cells6 groups, each ≥10 benign follicular cells Goellner et al Acta Cytol 1987; 31:587-90
h b i f lli l ll• 10 groups, each ≥20 benign follicular cells Nguyen et al. Pathol Annu 1991;23:63-80
• 6 groups on at least 2 of 6 aspirates Hamburger et
al. Diagn Cytopathol 1988;4:14-17
• 8 groups on at least 2 slides Kini SR. Guides to Clinical
Aspiration Biopsy: Thyroid, 2nd ed. 1996 p p y y

Adequacy in FNAAdequacy in FNA
• “The adequacy of FNA is highly dependent onThe adequacy of FNA is highly dependent on the skill and experience of the operator.” http://thyroidfna.cancer.gov
• “Why not accept the obvious? Training in proper technique is crucial for the success ofproper technique is crucial for the success of thyroid aspiration biopsy.” Waisman et al. AJCP 2008; 129:824.
• also dependent on the inherent quality of the lesion, e.g. cystic, solid, calcified, fibrotic, g y , , ,

Adequacy CriterionAdequacy Criterion• at least 6 groups of follicular cells
– each with at least 10 benign appearing, well-visualized follicular cellswell visualized follicular cells
• exceptions– thyroiditis–abundant colloidabundant colloid–any atypia

Non-Diagnostic

Thyroid CystsThyroid Cysts
• result of cystic degeneration of anresult of cystic degeneration of an adenomatous nodule
• risk of malignancy• risk of malignancy– 1- 4% in non-complex cysts
14% i i d lid/ i d l & l– 14% in mixed solid/cystic nodules & large cysts• diagnose as “Cyst Fluid Only” and categorized
as Non-Diagnostic / Unsatisfactory

NCI/Bethesda Conference - Suggested Terminology for Reporting Thyroid FNA
• Nondiagnostic / UnsatisfactoryNondiagnostic / Unsatisfactory• Benign
l i k f li ( 1%)– very low risk of malignancy (<1%)– benign follicular nodule [nodular goiter, colloid
d l d t id d l ]nodule, adenomatoid nodule]– lymphocytic (Hashimoto) thyroiditis
b / l h idi i– subacute/granulomatous thyroiditis– amyloid goiter




The recognition of abundant colloid shouldThe recognition of abundant colloid should override the requirement of a set number
f f lli l ll th f l tiof follicular cells as the false negative rate of such an aspirate approaches zero. As such, cytological interpretation should be reported as “negative or benign ” and p g g“consistent with a colloid nodule” , not "unsatisfactory" or "nondiagnostic”unsatisfactory or nondiagnostic .
htt //th idfhttp://thyroidfna.cancer.gov







NCI/Bethesda Conference - Suggested Terminology for Reporting Thyroid FNA
• Nondiagnostic / UnsatisfactoryNondiagnostic / Unsatisfactory• Benign
A i l C ll f d i d Si ifi /• Atypical Cells of Undetermined Significance / Follicular Lesion of Undetermined Si ifi [FLUS]Significance [FLUS]

ACUS/FLUS• set of lesions with architectural/cytologic atypia
but insufficient for a dx of FN• some examples:
– sparsely cellular - but seem to have a predominance of– sparsely cellular - but seem to have a predominance of microfollicles
– atypical cyst lining cellsatypical cyst lining cells– hypocellular aspirate, but nearly all cells are Hürthle
rare cells with features suggesting PTC– rare cells with features suggesting PTC• Bethesda committee: no more 7% of diagnoses
t (80% ) l i t b i t• most (80% or more) resolve into benign category


Implications of proposed …category of “Follicular lesion of undetermined significance”Follicular lesion of undetermined significance .
Diagn Cytopathol 2009; 37:710.
• 5-year study; 3 medical centers5 year study; 3 medical centers• 6,872 thyroid aspirates; 664=FLUS; 28 pathologists• Range of FLUS diagnosis: 2 5 – 28 6%• Range of FLUS diagnosis: 2.5 28.6%
C l i “FLUS t i• Conclusion: “FLUS category requires more rigorously defined morphologic criteria for it to become a useful guide in clinical management.”g

NCI/Bethesda Conference - Suggested Terminology for Reporting Thyroid FNA
• Nondiagnostic / UnsatisfactoryNondiagnostic / Unsatisfactory• Benign
A i l C ll f d i d Si ifi• Atypical Cells of Undetermined Significance• Suspicious for Follicular Neoplasm / Follicular
Neoplasm

Suspicious for Follicular NSuspicious for Follicular N
• used for cases where a predominance of• used for cases where a predominance of microfollicles is present [“architectural t i ”]atypia”]
• raises the possibility of Follicular CAp y• distinction between Follicular Adenoma
& Follicular CA not possible with FNA& Follicular CA not possible with FNA cytomorphology


“ h i b ll bl“The ‘magic bullet’ to enable cytopathologists to segregate follicular y p g g gpatterned neoplasms into benign and
malignant categories, and thus, guide themalignant categories, and thus, guide the therapeutic approach to any individual
thyroid nodule remains to be discovered ”thyroid nodule, remains to be discovered.
• LiVolsi VA, Baloch ZW. Determining the diagnosis and prognosis of thyroid neoplasms: do special studies help? Hum Pathol 1999; 30: 885-6.


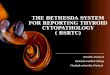
Microfollicular Pattern• monotonous population of follicular cells with
i i l b ll idminimal - absent colloid• nuclear overlapping and crowding are common• cells are usually arranged in three dimensional
groups and µfolliclesg p µ• µfollicle: <15 cells arranged in circle that is at
least two-thirds complete Arch Pathol Lab Med. 2006;130:148.least two thirds complete • nuclear atypia is not required


NCI/Bethesda Conference - Suggested Terminology for Reporting Thyroid FNA
• Nondiagnostic / UnsatisfactoryNondiagnostic / Unsatisfactory• Benign
A i l C ll f d i d Si ifi• Atypical Cells of Undetermined Significance• Suspicious for Follicular Neoplasm/ Follicular
Neoplasm– Hürthle Cell Neoplasm– “refers to a cellular aspirate that consists
exclusively (or almost exclusively) of y ( y)Hürthle cells”


Helpful Ancillary Techniques toHelpful Ancillary Techniques to Distinguish Adenoma From
Carcinoma
NONENONE

NCI/Bethesda Conference - Suggested Terminology for Reporting Thyroid FNA
• Nondiagnostic / UnsatisfactoryNondiagnostic / Unsatisfactory• Benign• Atypical Cells of Undetermined Significance• Atypical Cells of Undetermined Significance• Suspicious for Neoplasm
– FollicularFollicular– Hürthle
• Suspicious for MalignancySuspicious for Malignancy– quantitatively/qualitatively insufficient
“aim is to preserve the very high PPV of the– aim . . . is to preserve the very high PPV of the malignant category. . . ”

Suspicious for MalignancySuspicious for Malignancy
• suspicious for PTCsuspicious for PTC– subtle nuclear features, paucity of cells, unusual
variantvariant • e.g. FVPTC often lacks exhibit classic PTC features
• suspicious for MTC• suspicious for MTC– e.g. insufficient cells to perform IHC for calcitonin
i i f th f f• suspicious for other forms of cancer– e.g. complete necrosis of cellular material


NCI/Bethesda Conference - Suggested Terminology for Reporting Thyroid FNA
• Nondiagnostic / UnsatisfactoryNondiagnostic / Unsatisfactory• Benign
A i l C ll f d i d Si ifi• Atypical Cells of Undetermined Significance • Suspicious for Neoplasm
– Follicular– Hürthle
• Suspicious for Malignancy• Malignant• Malignant

Papillary Thyroid CarcinomaPapillary Thyroid Carcinoma

PTC – typical featuresPTC typical features
• syncytial monolayer • intranuclearsyncytial monolayer• papillary architecture
ll l i l
intranuclear pseudoinclusions
• dense cytoplasm• cellular swirls• enlarged, oval
• dense cytoplasm• marginal μnucleoli
nucleus• fine, pale chromatin
• MG cells• psammoma bodies, p
• longitudinal nucleargrooves
p• “bubble-gum”
colloidgrooves colloid







Clinical Management Algorithms
• Benign • FLUS–follow
• Suspicious– repeat FNAN di ti• Suspicious
–surgery• Non-diagnostic
(includes “cyst fluid • Malignant
surgery
only”)– repeat FNA–surgery repeat FNA
• usually after 3 monthsmonths

Goitered GazelleGoitered GazelleGazella subgutturosa