Embed Size (px)
Citation preview

Presented by: Ontario’s Geriatric Steering Committee
Thyroid disease Maria Wolfs MD MHSc FRCPC

Presented by: Ontario’s Geriatric Steering Committee 2
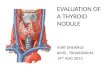
Thyroid nodules
Subclinical hypothyroidism
Subclinical hyperthyroidism
Outline

Presented by: Ontario’s Geriatric Steering Committee 3 Presented by: Ontario’s Geriatric Steering Committee
Thyroid Nodules

Presented by: Ontario’s Geriatric Steering Committee 4
Thyroid nodule - prevalence
Prevalence on palpation: – in iodine sufficient parts of the world
– 5% in women – 1% in men
Prevalence on ultrasound: – 19-67% of randomly selected patients
Risk of cancer in thyroid nodule: – 5-10 %
Cooper DS et al. Thyroid 2009;19(11)

Presented by: Ontario’s Geriatric Steering Committee 5
Investigating a thyroid nodule

Presented by: Ontario’s Geriatric Steering Committee 6
Investigating a thyroid nodule
LOW TSH N/HIGH TSH

Presented by: Ontario’s Geriatric Steering Committee 7
Investigating a nodule
LOW TSH
Hyperfunctioning
nodules = very low
risk for malignancy
Cooper DS et al. Thyroid 2009;19(11)

Presented by: Ontario’s Geriatric Steering Committee 8
Investigating a nodule
N/HIGH TSH
Thyroid Ultrasound

Presented by: Ontario’s Geriatric Steering Committee 9
Suspicious ultrasound features
Microcalcifications
Hypoechoic
Increased nodular vascularity
Infiltrative margins
Taller than wide on transverse view
Cooper DS et al. Thyroid 2009;19(11)

Presented by: Ontario’s Geriatric Steering Committee 10
Investigating a nodule
? Fine needle aspiration biopsy
N/HIGH TSH
Thyroid Ultrasound
Cooper DS et al. Thyroid 2009;19(11)

Presented by: Ontario’s Geriatric Steering Committee 11
Who needs a biopsy? > 0.7 cm nodule
High-risk history + nodule WITH suspicious sonographic features
Abnormal cervical lymph nodes
≥ 1 cm nodule
Solid nodule AND hypoechoic
Microcalcifications present in nodule
≥1-1.5 cm nodule
Solid nodule AND iso- or hyperechoic
≥1.5-2.0cm nodule
Mixed cystic–solid nodule WITH any suspicious ultrasound features
> 2.0cm nodule
Mixed cystic–solid nodule WITHOUT suspicious ultrasound features
Spongiform nodule
Cooper DS et al. Thyroid 2009;19(11)

Presented by: Ontario’s Geriatric Steering Committee 12
Who needs a biopsy?
> 0.7 cm nodule
High-risk history + nodule WITH suspicious sonographic features
Abnormal cervical lymph nodes
≥ 1 cm nodule
Solid nodule AND hypoechoic
Microcalcifications present in nodule
≥1-1.5 cm nodule
Solid nodule AND iso- or hyperechoic
≥1.5-2.0cm nodule
Mixed cystic–solid nodule WITH any suspicious ultrasound features
> 2.0cm nodule
Mixed cystic–solid nodule WITHOUT suspicious ultrasound features
Spongiform nodule
Cooper DS et al. Thyroid 2009;19(11)
•≥ 1 cm Solid
•≥ 2 cm Mixed solid-cystic

Presented by: Ontario’s Geriatric Steering Committee 13
Fine-needle biopsy
Benign
Non-diagnostic
Malignant
Suspicious (indeterminate) for neoplasm
Follicular lesion

Presented by: Ontario’s Geriatric Steering Committee 14
Fine-needle biopsy
Benign
–5% false-negative rate of FNA
–Higher in larger nodules (> 4cm)
Non-diagnostic
Malignant
Suspicious (indeterminate) for neoplasm
Follicular lesion

Presented by: Ontario’s Geriatric Steering Committee 15
Follow-up benign nodules
Yearly physical exam
Follow up ultrasound – in 6-18 months after initial FNA
If stable – next follow up 3-5 years later
If evidence of growth – 20% increase in two nodule dimensions with minimal increase of 2
mm in two dimensions on ultrasound – Repeat FNA – Refer to endocrine
LT4 suppression therapy is not recommended

Presented by: Ontario’s Geriatric Steering Committee 16
Follow-up benign nodules
Yearly physical exam
Follow up ultrasound – in 6-18 months after initial FNA
If stable – next follow up 3-5 years later
If evidence of growth – 20% increase in two nodule dimensions with minimal
increase of 2 mm in two dimensions on ultrasound
– Repeat FNA
– Refer to endocrine
LT4 suppression therapy is not recommended

Presented by: Ontario’s Geriatric Steering Committee 17
Follow-up benign nodules
Yearly physical exam
Follow up ultrasound
– in 6-18 months after initial FNA
If stable
– next follow up 3-5 years later
If evidence of growth
– 20% increase in two nodule dimensions with minimal increase of 2 mm in two dimensions on ultrasound
– Repeat FNA
– Refer to endocrine
LT4 suppression therapy is not recommended

Presented by: Ontario’s Geriatric Steering Committee 18
Fine-needle biopsy
Benign
Non-diagnostic
–Repeat FNA
Malignant
Suspicious (indeterminate) for neoplasm
Follicular lesion

Presented by: Ontario’s Geriatric Steering Committee 19
Fine-needle biopsy
Benign
Non-diagnostic
Malignant – 95% risk of malignancy
Suspicious (indeterminate) for neoplasm – 50-75% risk of malignancy
Follicular lesion – 5-15% risk of malignancy
Refer to endocrine or ENT

Presented by: Ontario’s Geriatric Steering Committee 20
Indications for thyroid surgery
Malignant or suspicious pathology
Family history of familial medullary thyroid cancer Recurrent cystic nodule with benign FNA
Compressive symptoms
Increasing in size
Size > 4 cm
Patient preference

Presented by: Ontario’s Geriatric Steering Committee 21 Presented by: Ontario’s Geriatric Steering Committee
Thyroid Nodules
Take home message

Presented by: Ontario’s Geriatric Steering Committee 22
Thyroid nodule - summary
N/HIGH TSH
Thyroid Ultrasound
LOW TSH
Thyroid Uptake and Scan

Presented by: Ontario’s Geriatric Steering Committee 23
Thyroid nodule - summary
Fine needle aspiration biopsy if:
• ≥ 1 cm Solid
• ≥ 2 cm Mixed solid-cystic
N/HIGH TSH
Thyroid Ultrasound

Presented by: Ontario’s Geriatric Steering Committee 24
Thyroid nodule - summary
Fine needle aspiration biopsy if:
• ≥ 1 cm Solid
• ≥ 2 cm Mixed solid-cystic
N/HIGH TSH
Thyroid Ultrasound
Yearly physical exam
Ultrasound in 6-18 months after initial FNA
If stable Next follow up 3-5 years

Presented by: Ontario’s Geriatric Steering Committee 25
Biopsy: – Malignant
– Suspicious (indeterminate) for neoplasm
– Follicular lesion
Follow-up US shows significant growth
Indications for surgery: – Family/personal history of familial thyroid cancer (MEN2,
FMTC)
– Recurrent cystic nodule with benign FNA (cosmetic concerns)
– Compressive symptoms
– > 4 cm
Refer to endocrine or ENT

Presented by: Ontario’s Geriatric Steering Committee 26
Thyroid nodules
Subclinical hypothyroidism
Subclinical hyperthyroidism
Outline

Presented by: Ontario’s Geriatric Steering Committee 27 Presented by: Ontario’s Geriatric Steering Committee
Subclinical
Hypothyroidism

Presented by: Ontario’s Geriatric Steering Committee 28
TSH
log/linear inverse relationship
between serum TSH and FT4

Presented by: Ontario’s Geriatric Steering Committee 29 Surks M I , Hollowell J G JCEM 2007;92:4575-4582
TSH distribution by age groups

Presented by: Ontario’s Geriatric Steering Committee 30
% TSH >4.5 mIU/L

Presented by: Ontario’s Geriatric Steering Committee 31
Subclinical hypothyroidism
prevalence 4 to 15% – USA NHANES III 4.3 %
– Europe • 4.2 % iodine-deficient areas
• 23.9 % abundant iodine intake
↑ with age
females > males whites > blacks
75% have TSH <10
Endocrine Reviews 29: 76–131, 2008

Presented by: Ontario’s Geriatric Steering Committee 32
Causes of SHypo
Inadequate replacement therapy for overt hypothyroidism – inadequate dosage
– non-adherence
– drug interactions • iron, calcium carbonate, cholestyramine, dietary soy, fiber,
etc.
– increased T4 clearance • phenytoin, carbamazepine, phenobarbital, etc.
– malabsorption
CMAJ 2012;184:205

Presented by: Ontario’s Geriatric Steering Committee 33
Causes of SHypo
Chronic autoimmune thyroiditis
Recovery from thyroiditis
Central hypothyroidism
TSH receptor gene mutations
CMAJ 2012;184:205

Presented by: Ontario’s Geriatric Steering Committee 34
Causes of SHypo
Drugs impairing thyroid function: – iodine and iodine-containing medications
• amiodarone, radiographic contrast agents
– lithium carbonate
– cytokines (especially interferon α)
– aminoglutetimide
– ethionamide
– sulfonamides
– sulfonylureas
CMAJ 2012;184:205

Presented by: Ontario’s Geriatric Steering Committee 35
Progression to overt hypothyroidism
% /year TSH
↑ N
TPO + 4.3% 2.0%
- 2.6% 0.5%

Presented by: Ontario’s Geriatric Steering Committee 36
Vascular effects of SHypo
↑ systemic vascular resistance
↑ arterial stiffness
Altered endothelial function
↑ atherosclerosis
Altered coagulability
Rodondi N. et al. JAMA. 2010;304(12):1365-1374

Presented by: Ontario’s Geriatric Steering Committee Biondi B , Cooper D S Endocrine Reviews 2008;29:76-131

Presented by: Ontario’s Geriatric Steering Committee 38
Increased CHD events and mortality
Rodondi N. et al. JAMA. 2010;304(12):1365-1374

Presented by: Ontario’s Geriatric Steering Committee 39
Lipid effects of hypothyroidism
Pearce E N JCEM 2012;97:326-333

Presented by: Ontario’s Geriatric Steering Committee 40
Effect of LT4 on dyslipidemia
Biondi B , Cooper D S Endocrine Reviews 2008;29:76-131 Cochrane Database Syst Rev 2007 Jul 18;(3):CD003419
Overall - no effect on cholesterol levels, HDL-C, LDL-C, triglycerides, ApoA, ApoB, or Lp(a)

Presented by: Ontario’s Geriatric Steering Committee 41
Hypothyroid symptoms score
Cochrane Database Syst Rev 2007 Jul 18;(3):CD003419

Presented by: Ontario’s Geriatric Steering Committee 42
Emotional Function tests
Jul 18;(3):CD003419

Presented by: Ontario’s Geriatric Steering Committee 43
Health Related Quality of Life Cochrane Database Syst Rev 2007 Jul 18;(3):CD003419

Presented by: Ontario’s Geriatric Steering Committee 44
Cognitive function
Cochrane Database Syst Rev 2007 Jul 18;(3):CD003419

Presented by: Ontario’s Geriatric Steering Committee 45
Consider LT4 treatment
High background CV risk
– Diastolic dysfunction
– Diastolic hypertension
– Atherosclerotic risk factors
– Dyslipidemia
– Diabetes

Presented by: Ontario’s Geriatric Steering Committee 46
Consider LT4 treatment

Presented by: Ontario’s Geriatric Steering Committee 47
Ongoing trials of SHypo in the elderly
IEMO 80-plus Thyroid Trial Collaboration
– www.iemo.nl
Thyroid Hormone Replacement for
Subclinical Hypo-Thyroidism Trial (TRUST)
– www.trustthyroidtrial.com

Presented by: Ontario’s Geriatric Steering Committee 48 Presented by: Ontario’s Geriatric Steering Committee
Subclinical
Hypothyroidism Take home message

Presented by: Ontario’s Geriatric Steering Committee 49
Repeat TSH, FT4, Thyroid antibodies in 3-6
months
No evidence of benefit for Rx with LT4
Consider treatment if:
– TSH > 10 mU/L
– Cardiac disease
– Symptoms
Subclinical hypothyroidism

Presented by: Ontario’s Geriatric Steering Committee 50
Thyroid nodules
Subclinical hypothyroidism
Subclinical hyperthyroidism
Outline

Presented by: Ontario’s Geriatric Steering Committee 51 Presented by: Ontario’s Geriatric Steering Committee
Subclinical
Hyperthyroidism

Presented by: Ontario’s Geriatric Steering Committee 52
Subclinical hyperthyroidism
Prevalence (NHANES III)
– TSH < 0.4 mU/L: 2%
– TSH < 0.1 mU/L: 0.7%
Latrogenic
– 14 - 21% of those on LT4 therapy
Most patients are asymptomatic
– Elderly can present with hypothyroid symptoms
Biondi B , Cooper D S Endocrine Reviews 2008;29:76-131

Presented by: Ontario’s Geriatric Steering Committee 53
Causes of SHyper
Endogenous causes
– Graves’ disease
– Autonomously functioning thyroid adenoma
– Multinodular goiter
Exogenous causes
– Excessive thyroid hormone replacement
– Intentional thyroid hormone suppression
Biondi B , Cooper D S Endocrine Reviews 2008;29:76-131

Presented by: Ontario’s Geriatric Steering Committee 54
Non-thyroid causes of SHyper
1st trimester pregnancy
Non-thyroidal illness
Psychiatric illness
Administration of drugs – dopamine, glucocorticoids
Pituitary or hypothalamic insufficiency
Decreased age-related thyroid hormone clearance or pituitary set point
Biondi B , Cooper D S Endocrine Reviews 2008;29:76-131

Presented by: Ontario’s Geriatric Steering Committee 55
SHyper Mood and cognition
Conflicting data – reduced feeling of well-being
– feelings of fear, anxiety, hostility
– inability to concentrate
– ↑ risk of dementia and Alzheimer’s Disease
Confounding factors – autoimmunity
– depression itself
Screening bias
Biondi B , Cooper D S Endocrine Reviews 2008;29:76-131

Presented by: Ontario’s Geriatric Steering Committee 56
SHyper Cardiovascular effects
Impaired quality of life
– increased heart rate
– reduced exercise capacity
Atrial fibrillation - elderly
↑ Left ventricular mass
– negative prognostic cardiovascular factor in the
general population
Biondi B , Cooper D S Endocrine Reviews 2008;29:76-131

Presented by: Ontario’s Geriatric Steering Committee 57
SHyper Skeletal effects
Accelerated bone turnover
– In postmenopausal patients
Increased fracture risk
– TSH ≤ 0.1 mU/L vs. N TSH
– 3-fold increased risk of hip fracture
– 4-fold increased risk of vertebral fracture
Biondi B , Cooper D S Endocrine Reviews 2008;29:76-131

Presented by: Ontario’s Geriatric Steering Committee 58
Fracture risk and LT4 dose
BMJ 2011;342:d2238

Presented by: Ontario’s Geriatric Steering Committee 59
SHyper management algorithm
Physical exam
↓TSH and N FT4 + N FT3

Presented by: Ontario’s Geriatric Steering Committee 60
SHyper management algorithm
Large goitre
Surgical intervention
if significant airway
compression
Physical exam
↓TSH and N FT4 + N FT3

Presented by: Ontario’s Geriatric Steering Committee 61
SHyper management algorithm
Physical exam
↓TSH and N FT4 + N FT3
Large goitre
Surgical intervention
if significant airway
compression
No goitre
Depends on
degree of TSH
suppression

Presented by: Ontario’s Geriatric Steering Committee 62
SHyper management algorithm
Repeat TSH FT4 FT3 in 3-6 months
TSH 0.1 - 0.4 mU/L

Presented by: Ontario’s Geriatric Steering Committee 63
SHyper management algorithm
Age >65 years
Post-menopausal women
Cardiac risk factors
Cardiac disease
Osteoporosis
Repeat TSH FT4 FT3 in 3-6 months
TSH 0.1 - 0.4 mU/L

Presented by: Ontario’s Geriatric Steering Committee 64
SHyper management algorithm
Repeat TSH FT4 FT3 in 6 weeks
(sooner if CVS problems)
TSH < 0.1 mU/L

Presented by: Ontario’s Geriatric Steering Committee 65
SHyper management algorithm
Repeat TSH FT4 FT3 in 6 weeks
(sooner if CVS problems)
TSH < 0.1 mU/L
Work-up for overt
hyperthyroidism

Presented by: Ontario’s Geriatric Steering Committee 66
SHyper management algorithm
Repeat TSH FT4 FT3 in 6 weeks
(sooner if CVS problems)
TSH < 0.1 mU/L
Work-up for overt
hyperthyroidism
Referral to endocrinology

Presented by: Ontario’s Geriatric Steering Committee
Low TSH + high FT4
Increased uptake:
Graves disease
Toxic nodule
Toxic multi-nodular goitre
Thyroid gland stimulation by HCG
Decreased uptake: Thyroiditis
Extra-thyroidal sources Exogenous
Endogenous
Thyroid scan
Thyroid uptake

Presented by: Ontario’s Geriatric Steering Committee
Increased uptake:
Graves disease
Toxic nodule
Toxic multi-nodular goitre
Thyroid gland stimulation
by HCG
Low TSH + high FT4
Thyroid uptake

Presented by: Ontario’s Geriatric Steering Committee Thyroid scan
Increased uptake:
Graves disease
Toxic nodule
Toxic multi-nodular goitre
Thyroid gland stimulation
by HCG
Low TSH + high FT4
Thyroid uptake

Presented by: Ontario’s Geriatric Steering Committee
Decreased uptake:
Thyroiditis
Extra-thyroidal sources Exogenous
Endogenous
Thyroid scan
Increased uptake:
Graves disease
Toxic nodule
Toxic multi-nodular goitre
Thyroid gland stimulation
by HCG
Low TSH + high FT4
Thyroid uptake

Presented by: Ontario’s Geriatric Steering Committee 71
Investigating a nodule
LOW TSH

Presented by: Ontario’s Geriatric Steering Committee 72
Thyroid scan – toxic nodule(s)
Normal scan Abnormal scan
uptake on R side with
suppression on L side

Presented by: Ontario’s Geriatric Steering Committee 73
Toxic nodule
Management
– Radioactive I131
– Surgery
– Consider pre-treatment with anti-thyroid drugs
if symptomatic or poor surgical candidate
Referral to endocrinology

Presented by: Ontario’s Geriatric Steering Committee 74
Thyroid scan – Grave’s disease
Normal uptake (<15%) Increased uptake in Graves disease (30-50%)

Presented by: Ontario’s Geriatric Steering Committee
Thyroid Receptor Ab - TRAb (Thyroid Stimulating
Immunoglobulin - TSI) in 85-
90% of Grave’s disease

Presented by: Ontario’s Geriatric Steering Committee
Thyroid Receptor Ab -
TRAb (Thyroid
Stimulating
Immunoglobulin - TSI) in
85-90% of Grave’s
disease
NB TRAb (TSI)
NOT covered
by MOH labs

Presented by: Ontario’s Geriatric Steering Committee 77
Graves’ disease
Management
– Consider beta-blocker
– Anti-thyroid drugs
• Propylthiouracil (ODB coverage)
• Methimazole
– Consider bone health
Referral to endocrinology

Presented by: Ontario’s Geriatric Steering Committee 78 Presented by: Ontario’s Geriatric Steering Committee
Subclinical
Hyperthyroidism Take home message

Presented by: Ontario’s Geriatric Steering Committee 79
SHyper
Clinical effects in the elderly
– Mood and cognition
– Atrial fibrillation
– Increased fracture risk

Presented by: Ontario’s Geriatric Steering Committee 80
Take home message - SHyper
Repeat TSH FT4 FT3
in 3-6 months
TSH 0.1 - 0.4 mU/L
Repeat TSH FT4 FT3 in 6 weeks
(sooner if CVS problems)
TSH < 0.1 mU/L

Presented by: Ontario’s Geriatric Steering Committee 81
Take home message - SHyper
Thyroid uptake and scan
Referral to endocrinology
Repeat TSH FT4 FT3
in 3-6 months
TSH 0.1 - 0.4 mU/L
Repeat TSH FT4 FT3 in 6 weeks
(sooner if CVS problems)
TSH < 0.1 mU/L

Presented by: Ontario’s Geriatric Steering Committee 82
Thyroid nodules
Subclinical hypothyroidism
Subclinical hyperthyroidism
Outline

Presented by: Ontario’s Geriatric Steering Committee
Thank you!









![Approach to Thyroid Nodule[1]](https://img.pdfslide.net/doc/110x75/55286aea55034670588b47b5/approach-to-thyroid-nodule1.jpg)