Embed Size (px)
Citation preview

ORIGINAL ARTICLE
Timing, prevalence, determinants and outcomes of homelessnessamong patients admitted to acute psychiatric wards
Alex D. Tulloch • Paul Fearon • Anthony S. David
Received: 14 December 2010 / Accepted: 30 June 2011 / Published online: 14 July 2011
� Springer-Verlag 2011
Abstract
Purpose To document the prevalence, timing, associa-
tions and short-term housing outcomes of homelessness
among acute psychiatric inpatients.
Methods Cross-sectional study of 4,386 acute psychiatric
admissions discharged from a single NHS Trust in
2008–2009.
Results Homelessness occurred in 16%. Most homeless-
ness (70%) was either recorded as present at admission or
started within 1 week. It was associated with younger age;
male gender; ethnicity other than White British or Black
African/Caribbean; being single, divorced, separated or
widowed; diagnosis of drug and alcohol disorder; detention
under a forensic section of the Mental Health Act; having
no previous admission or alternatively having a longer
previous admission; having a low score on the depressed
mood or hallucinations and delusions items of the Health of
the Nation Outcome Scales (HoNOS); and having a high
score on the HoNOS relationship difficulties and occupa-
tion and activities items. Of those who were followed-up
for 28 days after discharge, 53% had a new address
recorded; of those who were not, only 22% did.
Conclusions Homelessness affects a substantial minority
of psychiatric admissions in the UK. Housing outcomes are
uncertain, and it is possible that more than half continue to
be homeless or living in very transient situations. Demo-
graphic and diagnostic associations with homelessness
were consistent with US studies; associations with HoNOS
item scores and having had no admission in the preceding
2 years suggest that, in many cases, social adversity pre-
dominates over active psychopathology at the time of
admission.
Keywords Mental disorder � Homeless persons �Hospitals � Psychiatric � Residential mobility
Introduction
International and UK reports over many years have indi-
cated that psychiatric illness is common among homeless
individuals and that homelessness is common among psy-
chiatric patients [1]. Documenting the timing, prevalence
and associations of inpatient homelessness is important for
the planning of housing services and also for psychiatric
services, especially in view of reports that homelessness is
associated with increased length of stay (LOS) [2, 3].
In US, 35% of the patients present on Veterans’
Administration acute psychiatric units at the time of a
census were found to be homeless at admission, with 20%
of these ‘‘literally homeless’’ and 15% ‘‘doubled-up’’ [4].
In the Suffolk County Mental Health Project, 11% of the
patients with a first admission for psychosis had been lit-
erally homeless for at least one night in the preceding
period [5]. Among those admitted to state mental hospitals
reported prevalence has ranged from 9% in Michigan in
1984 [6], 5% in Illinois in 1980 [7], and 19% in the
A. D. Tulloch (&) � P. Fearon � A. S. David
Department of Psychosis Studies,
Institute of Psychiatry, Kings College London,
De Crespigny Park, London SE5 8AF, UK
e-mail: [email protected]
A. S. David
e-mail: [email protected]
P. Fearon
Trinity College Dublin and St Patrick’s University Hospital
Dublin, James’s Street, Dublin 8, Ireland
e-mail: [email protected]
123
Soc Psychiatry Psychiatr Epidemiol (2012) 47:1181–1191
DOI 10.1007/s00127-011-0414-4

3 months preceding admission in New York State [8]. In
Australia, 32% of a sample of patients admitted to a service
serving poor suburbs of Adelaide were homeless [9].
We are aware of four previous English studies of
homelessness among psychiatric inpatients. Whiteley [10]
examined the records of 1,536 men admitted to a psychi-
atric observation ward serving South London in 1953 and
1954, and found that 130 (8.4%) gave their last address as a
London County Council Reception Centre or common
lodging house. Herzberg [11] found all the homeless men
(N = 272) and women (N = 79) admitted to St Clement’s
Hospital, Whitechapel between 1971 and 1980 inclusive.
There was no control group. Of note, the author found that
half of the sample had been housed in at least part of the
7 days before admission, and commented that this ‘‘sub-
stantiates the clinical impression that NFA subjects often
present to emergency hospital services when their accom-
modation has been lost’’. Fisher et al [12] performed a
1-day census on the acute psychiatric wards of a single
inner London health district and found that 33 of 87
inpatients (33%) were homeless. The most sophisticated
and recent UK study is that of Koffman and Fulop [2] who
reported the results of a survey of all inpatients in adult
acute and low-level secure psychiatric beds in London on
the 15 June 1994. Of the 3,978 total patients, 817 (20.5%)
were identified by the ward manager as homeless (defined
here as not living in permanent accommodation), with a
slightly higher prevalence in inner as compared to outer
London.
Rosenheck and Seibyl [4] found that younger age, male
gender, being black and having a primary drug and alcohol
disorder were associated with homelessness, while being
married and having a diagnosis of schizophrenia were
inversely associated. Although based on much smaller
samples, Herman et al [5] found that homelessness was
more common among black participants, while Susser et al.
[8] found in a multivariable analysis that homelessness was
associated with urban location and having experienced
disruptive events in childhood. Koffman and Fulop [2]
found unadjusted associations between homelessness and
schizophrenia, male gender, admission under the Mental
Health Act and LOS [3 months. (All of these except
diagnosis of schizophrenia entered into a multivariable
analysis, together with not being registered with a GP and
having had a needs assessment by the local authority).
Short-term housing outcomes of homelessness among
psychiatric inpatients were described by some of these
studies. Appleby and Desai [7] noted that discharge to any
form of accommodation was relatively unusual among the
homeless patients they identified. Greenberg et al [13]
reported data from hospital discharge for the Veterans’
Administration sample described above [4]. The study was
complicated by a 30% rate of missing data, but for those
for whom data were collected, 13% were literally homeless
at the time of discharge, 40% were doubled-up, 33% were
transferred to institutional settings, such as halfway houses,
and 13% were living independently. Both continued literal
homelessness and transfer to other institutional living
arrangement were associated with literal homelessness at
admission, while continued doubling-up was more com-
mon among those doubled up at admission. Similarly, in
the case control studies comparing homeless and domiciled
individuals with schizophrenia in NY it was found that
50% of homeless men with schizophrenia had been dis-
charged to the streets or a shelter after the most recent
psychiatric hospitalization [14]. It is not known to what
extent such findings apply in the UK.
We aimed to estimate the prevalence, timing, associa-
tions and short-term housing outcomes of homelessness in
a large cohort of acute psychiatric admissions.
Methods
Sample
Data were taken from the Case Register maintained by the
NIHR Specialist Biomedical Research Centre for Mental
Health. This repository is a copy of the South London and
Maudsley NHS Foundation Trust’s paperless electronic
patient record database, anonymised and optimised for data
extraction [15]. All activity since 2006 is covered, with
largely complete coverage for administrative data for
several years preceding that date. All analysis was per-
formed using Stata 10.
We extracted all admissions for which the first ward was
one of the acute psychiatric wards serving the London
Boroughs of Croydon, Lambeth, Lewisham and South-
wark, and which culminated in a discharge between 31
December 2007 and 31 December 2009. In those cases
where the same individual had more than one discharge
over this period, the last period was selected. (The use of a
multi-level dataset with multiple admissions per person
would have invalidated the approach used for missing
data.) Contiguous periods on different wards were con-
catenated, but periods separated by 1 day or more were
treated as separate admissions. Periods of ward leave were
disregarded.
Non-housing variables
Non-housing data merged with these were: age, sex, eth-
nicity, current marital status (that is, at the time of data
extraction), current employment status, primary diagnosis
recorded nearest to the date of discharge, lifetime drug and
alcohol misuse, Mental Health Act status, longest
1182 Soc Psychiatry Psychiatr Epidemiol (2012) 47:1181–1191
123

admission leading to a discharge in the preceding 2 years
and the set of Health of the Nation Rating Scales (HoNOS)
ratings [16] recorded nearest to the date of admission,
excluding scores made more than 3 days before or 21 days
after admission and post-discharge scores. In order to
reduce computing time for multiple imputation, HONOS
item scores were recoded as dichotomous variables (0–1
‘‘no or minor’’ vs. 2–4 ‘‘mild to very severe’’).
Address data
The complete set of address records for each subject was
extracted from the Case Register. In the source clinical
database, each address record consists of an address, a
postcode, a start date and—if the period resident at the
address has ended—an end date. Individuals who are of
no fixed abode are represented by a mock postcode. Each
individual should have at least one address record, and
new records may be added when an individual moves
home, becomes homeless, or re-enters the clinical service
after a period outside secondary mental health care. (End
dates are generated automatically at the time of entry of a
new permanent address or at the time of discharge from
all services provided by the NHS Trust.) As an anony-
mised data repository, the BRC Case Register removes
the address itself and replaces valid postcodes with the
corresponding Office of National Statistics (ONS) Output
Area code; the mock postcode for homelessness is
replaced with a marker for homelessness. Output areas
contain approximately 100 households, so their use will
only fail to detect changes of address if these are within a
very small area.
As detection of homeless periods using the method
above depends on the entry of a specific mock postcode, we
also extracted and reviewed those free-text progress notes
entered during the relevant admission which contained the
character strings ‘‘NFA’’, ‘‘no fixed abode’’, and ‘‘home-
less’’. We corrected records as necessary and created a
variable recording whether homelessness was recorded
only in the address records, only in free-text, or in both.
Residential variables
These address records were used in three ways. First, we
extracted all homeless periods with a recorded start date
that was either (a) 28 days or less before an admission,
(b) during an admission or (c) 28 days or less after a dis-
charge. To these, we added (d) all homeless periods that
had a recorded start date more than 28 days before an
admission, but which continued into the period from
28 days before admission to 28 days after discharge. The
start dates of all these periods were used in the graphical
analyses (see below), truncating periods that began more
than 28 days before admission so that they appeared to
start 28 days before admission.
Second, we defined those individuals who were recorded
as currently homeless at the time of admission, or who
were first recorded as homeless during the admission. This
variable was used in the single variable analyses and the
multivariable analysis of the associations of homelessness.
Third, we defined a variable that recorded moves from
homelessness or from a residential address into a second
residential address over the period from admission to
28 days after discharge. This variable was used in the
multiple imputation process and was also used to calculate
the proportion of homeless individuals who acquired a new
address during or after the period of admission.
Missing data
Multiple imputation of missing data was performed using
chained equations [17]. The imputed datasets were also
used for analyses of LOS after acute psychiatric admission
and residential mobility related to acute psychiatric
admission [18]. All exposure variables were included in the
imputation model. We also added the Nelson-Aalen
cumulative hazard estimator for discharge from hospital
derived from a Cox regression of LOS without covariates
performed on the same dataset, the HoNOS problems with
living conditions item, the measure of homelessness, a
measure of residential mobility and additional predictors of
missing HoNOS data (the calendar period of the admission
and the ward to which the subject was first admitted). We
created 50 imputed datasets; this is a higher number than
required in order to provide unbiased estimates, but reduces
the Monte Carlo error attributable to the imputation process
itself [19]. Multiple imputation is known to produce
unbiased parameter estimates under the assumption of
missing completely at random (MCAR) or missing at
random (MAR). In the case of the HoNOS data, which
accounted for most missing data, the MAR model seems
intuitively likely. At the time of the study, HoNOS had
little clinical and no financial importance, and whether it
was measured or not was related primarily to LOS, the
calendar period and the ward to which the patient was
admitted, suggesting that staff enthusiasm, Trust policy and
whether or not the patient was admitted for long enough
were primary determinants of missingness.
Descriptive and graphical analyses
The initial stages of analysis were graphical, and aimed to
demonstrate when homelessness was first recorded in
relation to admission and discharge; these graphical anal-
yses and the single variable analyses used the original
(unimputed) data. A series of histograms of starting times
Soc Psychiatry Psychiatr Epidemiol (2012) 47:1181–1191 1183
123
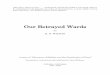
of recorded homeless periods was constructed (Fig. 1). As
noted above, homeless periods ending more than 28 days
before admission or beginning more than 28 days after
discharge were not shown, and homeless periods beginning
more than 28 days before admission but not ending before
that point were truncated and, therefore, appear to start at
28 days before admission. Each histogram represents the
date at which homelessness was first recorded relative to
admission and to discharge. On the X-axis of these graphs,
‘‘A’’ denotes the day of admission, ‘‘D’’ denotes the day of
discharge, ‘‘A-28’’ denotes 28 days before admission, and
‘‘D?28’’ denotes 28 days after discharge. Therefore,
periods of recorded homelessness starting before admission
or after discharge were scaled in order to appear at the
appropriate point relative to the 28 days before admission
or after discharge, and periods of recorded homelessness
starting during the admission were scaled in order to appear
at the appropriate point relative to the LOS. This process
allowed stays to be overlapped and the timing of
homelessness to be compared across multiple admissions
with differing LOS. We graphed start dates of recorded
homeless periods separately within deciles of LOS—this
was in order to minimise the extent to which the apparent
timing of homelessness during the admission was distorted
by scaling. Single variable analyses were used to further
describe the prevalence and timing of homelessness and
also to describe unadjusted associations with homelessness.
Definition of functional form for continuous covariates
Before performing the main analysis, we defined an
appropriate functional form for the two continuous vari-
ables using fractional polynomials [20, 21]. This allows the
selection of an appropriate polynomial form to represent
continuous variables, where such a form fits the data better
than the untransformed (linear) form of the variable. The
method avoids both the loss of information and the
anomalies related to choice of boundaries resulting from
010
2030
Fre
quen
cyF
requ
ency
Fre
quen
cy
Fre
quen
cyF
requ
ency
Fre
quen
cyF
requ
ency
Fre
quen
cyF
requ
ency
Fre
quen
cy
A -28 A D D +28
LOS 1 day
LOS 15-21 days
LOS 72-129 days LOS 130+ days
LOS 22-31days LOS 32-46 days LOS 47-71 days
LOS 5-8 daysLOS 2-4 days LOS 9-14 days
010
2030
40
50
A -28 A D D +28
010
2030
A -28 A D D +28
01
020
30
A -28 A D D +28
010
203
0
A -28 A D D +28
010
203
0
A -28 A D D +28
05
1015
202
5
A -28 A D D +28
05
1015
2025
A -28 A D D +28
05
1015
20
A -28 A D D +28
010
2030
40
A -28 A D D +28
Fig. 1 Starting dates of recorded homeless periods relative to
admission and discharge. Note: See text for full description. Starting
dates of recorded homeless periods are depicted relative to admission
and discharge. An uncertain number of recorded periods of home-
lessness may have been truncated relative to the true date at which
homelessness commenced. Periods of recorded homelessness starting
more than 28 days before admission are truncated at 28 days before
admission. Periods ending more than 28 days before admission or
starting more than 28 days after discharge are not shown. ‘‘A-
28’’denotes the date 28 days before admission, ‘‘A’’ denotes the day
of admission, ‘‘D’’ denotes the day of discharge and ‘‘D?28’’ denotes
28 days after discharge. Each histogram is constructed for a decile of
length of stay (LOS) and homeless periods beginning during
admission are shown at the appropriate point relative to the eventual
LOS for that admission
1184 Soc Psychiatry Psychiatr Epidemiol (2012) 47:1181–1191
123

categorical transformation. For this preliminary step, we
used a subsample of 3,700 cases that had complete data for
age, sex, ethnicity, marital status, diagnosis, service use
and Mental Health Act status, and from which we removed
a small number of observations with outlying values for
longest admission in the preceding 2 years; all the afore-
mentioned variables were included as covariates. (We
aimed to select functional forms that would be as close as
possible to those that would have been selected for the full
model using the complete sample had we had no missing
data. The inclusion of other variables with more missing
data would have further reduced the size and representa-
tiveness of this sample, which represented 82% of the total
sample of admissions.) A danger of the fractional polyno-
mial approach is overfitting due to small numbers of
influential values [22]. We dealt with this by removing
outlying values as above, by constructing diagnostic plots
of covariate values against the partial linear predictor and
deviance residuals [23], and by assessing the stability of the
selected functional form using 1,000 bootstrap samples
(Stata mfpboot; [24]).
Multivariable analysis
A multivariable logistic regression model for the odds of
homelessness was fitted. As we aimed to obtain the esti-
mates of the effects of all of the demographic, clinical and
service use variables, and in order to avoid the potential for
bias due to over-fitting [25], we fitted a full model
including all exposure variables listed above. We analysed
each of the 50 imputed datasets and automatically com-
bined the results according to Rubin’s rules [26]. As in the
derivation of functional form for age and longest previous
admission, we omitted seven observations with outlying
values for longest admission in the preceding 2 years,
giving a sample size of 4,378 for the main analysis. We
used the parameters for the two continuous covariates to
generate category-based estimates representing the average
estimated effect for a given band of values for the two
continuous covariates [23]. Age was presented by deciles,
taking the midpoint of each decile as the reference value.
Longest previous admission was presented by quartiles of
its distribution among those who had an admission, taking
the mid-centile value within each quartile as the reference
value.
Results
Descriptive and graphical analyses
A total of 735 patients were recorded as homeless at some
point during the period from 28 days before admission to
28 days after discharge. A small number of these only had
a recorded period of homelessness ending before admission
(N = 4) or were only recorded as becoming homeless in
the 28 days after discharge (N = 12). The graphical plots
included these latter values. Of the total 4,386 patients with
address data, 719 patients (16%) were, therefore, defined as
homeless at hospital admission or during the admission—
these were the subjects used in the single variable and
multivariable analyses.
Of the 719 subjects, 392 (55%) were recorded as
homeless on the day of admission and 327 (45%) were first
recorded as homeless during the admission. A total of 505
(70%) were either recorded as homeless at admission or
within 7 days of admission. A total of 393 patients were
recorded as homeless only in the free-text (54.7%), while
233 patients had a structured record indicating homeless-
ness but did not have a free text record containing the string
‘‘homeless’’, ‘‘no fixed abode’’ or ‘‘NFA’’. Only 93 patients
had both a free text record of the above type and a struc-
tured record indicating homelessness.
Figure 1 indicates that homelessness tends to be first
recorded at or around the time of admission, but continues
to occur throughout admission, but with reduced frequency,
especially among those with greatest LOS. There were very
few homeless periods which began more than 28 days
before admission.
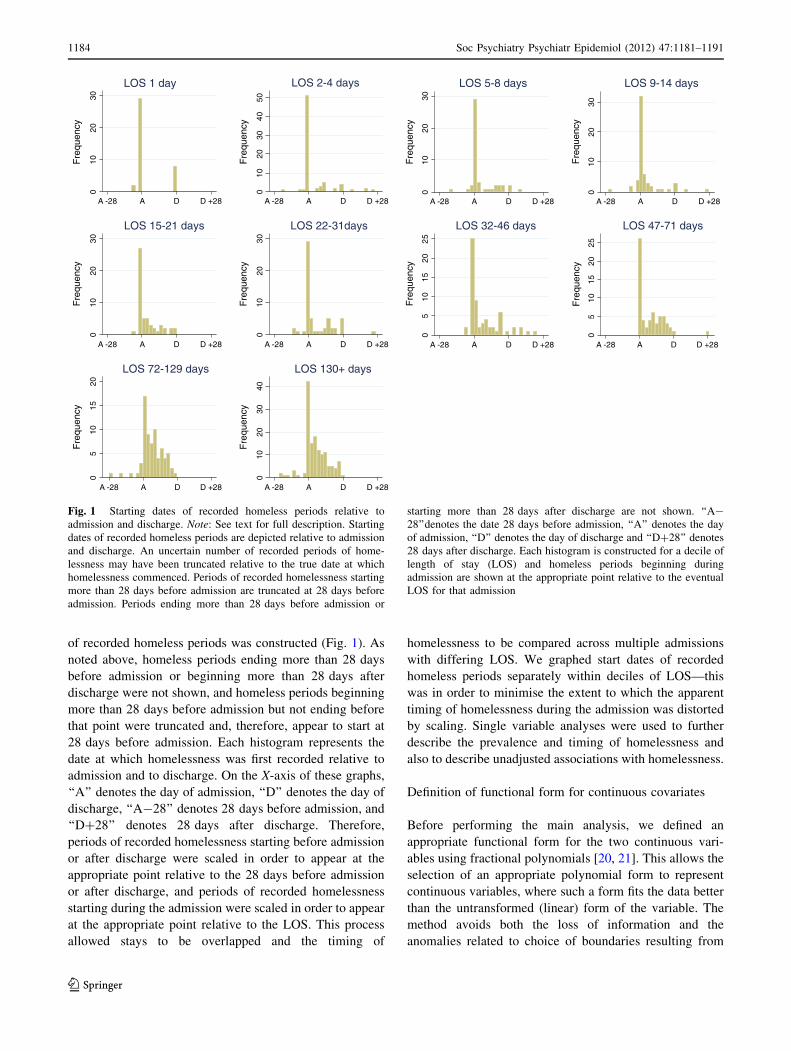
Single variable associations with homelessness
Variables with an unadjusted association with homeless-
ness with p \ 0.05 were: age, sex, ethnicity, marital status,
employment, primary diagnosis, lifetime diagnosis of drug
and alcohol disorder, Mental Health Act status, length of
the longest admission in the preceding 2 years, and the
HoNOS drug and alcohol item, physical illness item, hal-
lucinations and delusions item, depressed mood item,
relationship difficulties item and occupational difficulties
item. (See Table 1).
Multivariable analysis of associations
with homelessness
Both age and longest admission in the preceding 2 years
were best fitted by linear terms. Graphical plots demon-
strated no evidence of overfitting and these functional
forms were selected by 686/1,000 and 943/1,000 bootstrap
replications, respectively. Full results of the final multi-
variable analysis are displayed in Table 2. Odds of
homelessness declined steeply with advancing age
(p \ 0.0001). There were also significant associations with
marital status (p = 0.0002; lower in married, higher among
divorced and single), and ethnicity (p \ 0.0001; higher
among patients who were neither White British nor Black
Soc Psychiatry Psychiatr Epidemiol (2012) 47:1181–1191 1185
123
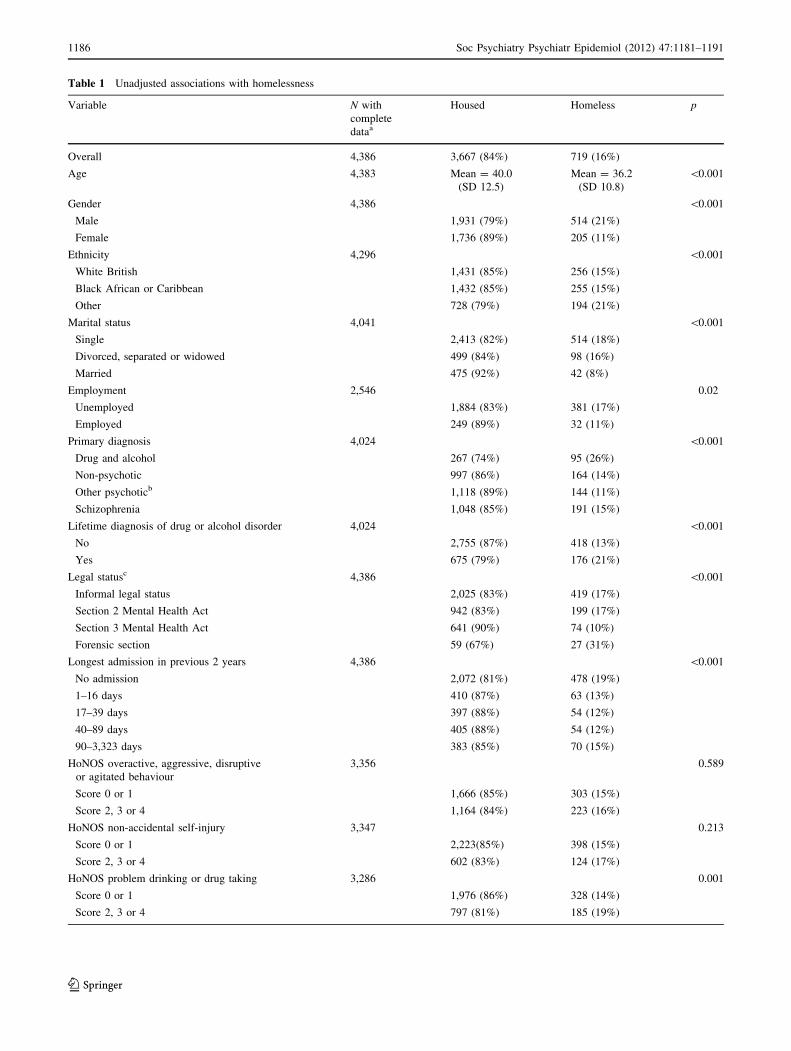
Table 1 Unadjusted associations with homelessness
Variable N with
complete
dataa
Housed Homeless p
Overall 4,386 3,667 (84%) 719 (16%)
Age 4,383 Mean = 40.0
(SD 12.5)
Mean = 36.2
(SD 10.8)
\0.001
Gender 4,386 \0.001
Male 1,931 (79%) 514 (21%)
Female 1,736 (89%) 205 (11%)
Ethnicity 4,296 \0.001
White British 1,431 (85%) 256 (15%)
Black African or Caribbean 1,432 (85%) 255 (15%)
Other 728 (79%) 194 (21%)
Marital status 4,041 \0.001
Single 2,413 (82%) 514 (18%)
Divorced, separated or widowed 499 (84%) 98 (16%)
Married 475 (92%) 42 (8%)
Employment 2,546 0.02
Unemployed 1,884 (83%) 381 (17%)
Employed 249 (89%) 32 (11%)
Primary diagnosis 4,024 \0.001
Drug and alcohol 267 (74%) 95 (26%)
Non-psychotic 997 (86%) 164 (14%)
Other psychoticb 1,118 (89%) 144 (11%)
Schizophrenia 1,048 (85%) 191 (15%)
Lifetime diagnosis of drug or alcohol disorder 4,024 \0.001
No 2,755 (87%) 418 (13%)
Yes 675 (79%) 176 (21%)
Legal statusc 4,386 \0.001
Informal legal status 2,025 (83%) 419 (17%)
Section 2 Mental Health Act 942 (83%) 199 (17%)
Section 3 Mental Health Act 641 (90%) 74 (10%)
Forensic section 59 (67%) 27 (31%)
Longest admission in previous 2 years 4,386 \0.001
No admission 2,072 (81%) 478 (19%)
1–16 days 410 (87%) 63 (13%)
17–39 days 397 (88%) 54 (12%)
40–89 days 405 (88%) 54 (12%)
90–3,323 days 383 (85%) 70 (15%)
HoNOS overactive, aggressive, disruptive
or agitated behaviour
3,356 0.589
Score 0 or 1 1,666 (85%) 303 (15%)
Score 2, 3 or 4 1,164 (84%) 223 (16%)
HoNOS non-accidental self-injury 3,347 0.213
Score 0 or 1 2,223(85%) 398 (15%)
Score 2, 3 or 4 602 (83%) 124 (17%)
HoNOS problem drinking or drug taking 3,286 0.001
Score 0 or 1 1,976 (86%) 328 (14%)
Score 2, 3 or 4 797 (81%) 185 (19%)
1186 Soc Psychiatry Psychiatr Epidemiol (2012) 47:1181–1191
123
African or Caribbean). Odds of homelessness were lowest
in the group with non-schizophrenic psychotic illness, with
higher odds among those with schizophrenia and non-
psychotic illness, but the highest odds were seen in the
group with drug and alcohol disorders (overall test of
significance p = 0.0040). Individuals with no previous
admission had the greatest odds of homelessness and
individuals with a one-day previous admission had the
lowest odds, with a small linear increase in the log odds of
homelessness with increasing length of the longest
admission in the previous 2 years (overall test of signifi-
cance p \ 0.0001). Mental Health Act status was also
highly significant (p = 0.0011); odds were highest among
those detained under forensic sections of the Mental Health
Act and lowest among those detained under Section 3 of
the Act. Among the HoNOS items, homelessness was
positively associated with high scores on the difficulties in
relationships item (item 9; p = 0.0006) and the difficulties
in occupation item (item 12; p\0.0001) and negatively
associated with high scores on the hallucinations and
delusions item (item 6; p = 0.0022) and depressed mood
item (item 7; p = 0.0033).
Analysis of housing subsequent to homelessness was
complicated by truncation of address records when dis-
charge from all secondary mental health care occurred at
the time of hospital discharge or shortly afterwards. Of
the 485 homeless individuals who remained in contact
with mental health services for at least 28 days after
hospital discharge, 245 (50.3%) gained an address during
the admission or within 28 days of discharge. Of the 234
homeless individuals who were discharged from services
within 28 days of discharge, 52 (22.2%) gained an
address during the admission or within 28 days of dis-
charge. The median time at which these address spells
began relative to the day of discharge was on the day of
discharge itself.
Table 1 continued
Variable N with
complete
dataa
Housed Homeless p
HoNOS cognitive problems 3,330 0.873
Score 0 or 1 2,175 (85%) 399 (16%)
Score 2, 3 or 4 637 (84%) 119 (16%)
HoNOS physical illness or disability problems 3,331 0.042
Score 0 or 1 2,272 (84%) 438 (16%)
Score 2, 3 or 4 541 (87%) 80 (13%)
HoNOS hallucinations and delusions 3,327 0.037
Score 0 or 1 1,168 (83%) 242 (17%)
Score 2, 3 or 4 1,639 (86%) 278 (15%)
HoNOS depressed mood 3,337 0.043
Score 0 or 1 1,580 (83%) 320 (17%)
Score 2, 3 or 4 1,232 (86%) 205 (14%)
HoNOS other mental and behavioural problems 3,352 0.118
Score 0 or 1 1,199 (83%) 242 (17%)
Score 2, 3 or 4 1,628 (85%) 282 (15%)
HoNOS problems with relationships 3,267 \0.001
Score 0 or 1 1,531 (86%) 241 (14%)
Score 2, 3 or 4 1,226 (82%) 269 (18%)
HoNOS problems with activities of daily living 3,294 0.359
Score 0 or 1 1,819 (85%) 324 (15%)
Score 2, 3 or 4 963 (84%) 188 (16%)
HoNOS problems with occupation and activities 3,155 \0.001
Score 0 or 1 1,662 (87%) 242 (13%)
Score 2, 3 or 4 1,007 (81%) 244 (20%)
a 4,386 of 4,485 admissions had complete address data (97.2%)b ‘Other psychotic’ comprised ICD-10 codes F21 to F31 inclusivec Legal status was defined as the most restrictive section of the Mental Health Act in force during the first week of the admission. Detention only
under Section 136, Section 5(2) or Section 5(4) was treated as informal legal status
Soc Psychiatry Psychiatr Epidemiol (2012) 47:1181–1191 1187
123
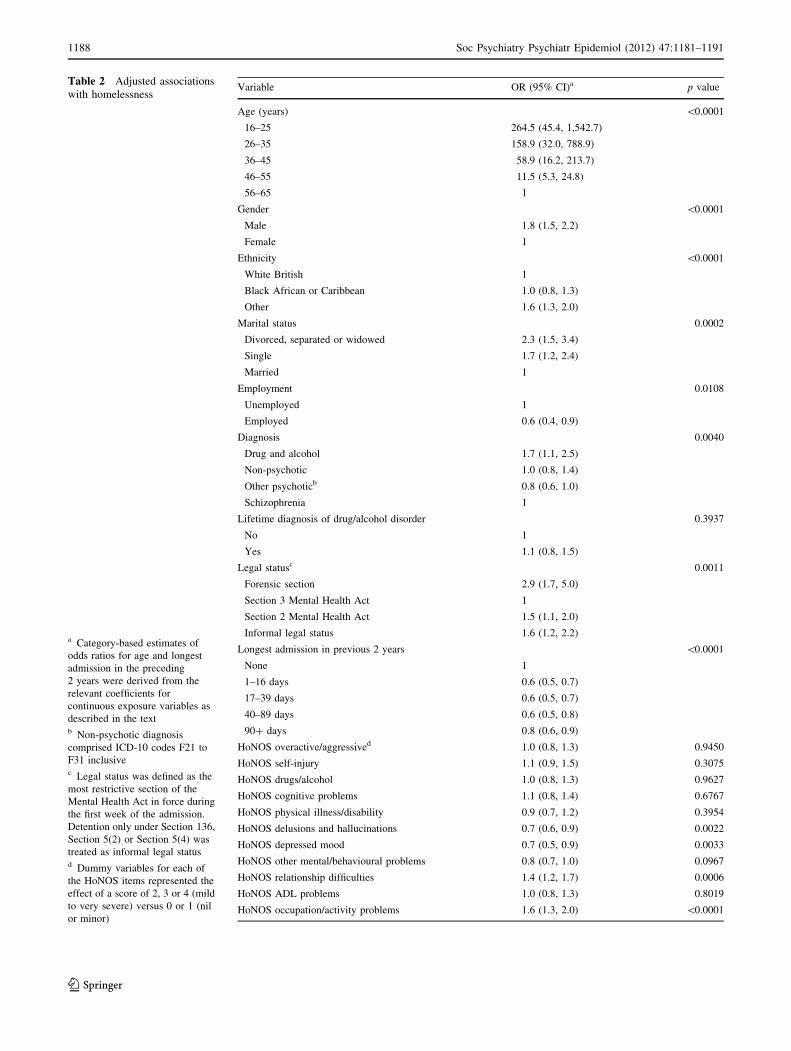
Table 2 Adjusted associations
with homelessness
a Category-based estimates of
odds ratios for age and longest
admission in the preceding
2 years were derived from the
relevant coefficients for
continuous exposure variables as
described in the textb Non-psychotic diagnosis
comprised ICD-10 codes F21 to
F31 inclusivec Legal status was defined as the
most restrictive section of the
Mental Health Act in force during
the first week of the admission.
Detention only under Section 136,
Section 5(2) or Section 5(4) was
treated as informal legal statusd Dummy variables for each of
the HoNOS items represented the
effect of a score of 2, 3 or 4 (mild
to very severe) versus 0 or 1 (nil
or minor)
Variable OR (95% CI)a p value
Age (years) \0.0001
16–25 264.5 (45.4, 1,542.7)
26–35 158.9 (32.0, 788.9)
36–45 58.9 (16.2, 213.7)
46–55 11.5 (5.3, 24.8)
56–65 1
Gender \0.0001
Male 1.8 (1.5, 2.2)
Female 1
Ethnicity \0.0001
White British 1
Black African or Caribbean 1.0 (0.8, 1.3)
Other 1.6 (1.3, 2.0)
Marital status 0.0002
Divorced, separated or widowed 2.3 (1.5, 3.4)
Single 1.7 (1.2, 2.4)
Married 1
Employment 0.0108
Unemployed 1
Employed 0.6 (0.4, 0.9)
Diagnosis 0.0040
Drug and alcohol 1.7 (1.1, 2.5)
Non-psychotic 1.0 (0.8, 1.4)
Other psychoticb 0.8 (0.6, 1.0)
Schizophrenia 1
Lifetime diagnosis of drug/alcohol disorder 0.3937
No 1
Yes 1.1 (0.8, 1.5)
Legal statusc 0.0011
Forensic section 2.9 (1.7, 5.0)
Section 3 Mental Health Act 1
Section 2 Mental Health Act 1.5 (1.1, 2.0)
Informal legal status 1.6 (1.2, 2.2)
Longest admission in previous 2 years \0.0001
None 1
1–16 days 0.6 (0.5, 0.7)
17–39 days 0.6 (0.5, 0.7)
40–89 days 0.6 (0.5, 0.8)
90? days 0.8 (0.6, 0.9)
HoNOS overactive/aggressived 1.0 (0.8, 1.3) 0.9450
HoNOS self-injury 1.1 (0.9, 1.5) 0.3075
HoNOS drugs/alcohol 1.0 (0.8, 1.3) 0.9627
HoNOS cognitive problems 1.1 (0.8, 1.4) 0.6767
HoNOS physical illness/disability 0.9 (0.7, 1.2) 0.3954
HoNOS delusions and hallucinations 0.7 (0.6, 0.9) 0.0022
HoNOS depressed mood 0.7 (0.5, 0.9) 0.0033
HoNOS other mental/behavioural problems 0.8 (0.7, 1.0) 0.0967
HoNOS relationship difficulties 1.4 (1.2, 1.7) 0.0006
HoNOS ADL problems 1.0 (0.8, 1.3) 0.8019
HoNOS occupation/activity problems 1.6 (1.3, 2.0) \0.0001
1188 Soc Psychiatry Psychiatr Epidemiol (2012) 47:1181–1191
123

Discussion
Based on a modified consecutive sample of hospital dis-
charges, we performed a cross-sectional study of the
prevalence, timing and associations of homelessness
among patients admitted to acute psychiatric wards. This
study is similar in size to the previous London-based study
of Koffman and Fulop [2], but is based on a sample of
hospital discharges rather than on a survey of cases present
on a ward, the latter being a method which invariably
creates a sample biased towards those with the greatest
LOS. Probably because housing status has never been
reported as part of Hospital Episode Statistics, previous
studies have relied on manual collection of data, whereas
we were able to make use of a large repository of anony-
mised electronic patient records which were enriched by
the inclusion of a multi-item routine outcome measure
(HoNOS) and longitudinal data on addresses. We were able
to distinguish between homelessness recorded at the point
of admission and homelessness first recorded during the
admission and found that nearly half of all homelessness
was in the second category, although most of this occurred
early in admission.
The limitations of the study are closely related to its
strengths: the data are administrative, and the coding of
homelessness and housing was subject to multiple institu-
tional contingencies. Exactly what determined the record-
ing of homelessness or having no fixed abode in free-text or
structured records is unknown. It is not known, for example,
to what extent those ‘‘doubling up’’ (also known as ‘‘sofa-
surfing’’), but who were not literally homeless, were
recorded as homeless or of no fixed abode. We found a
substantial number of dates of onset of homelessness only in
the free text notes, suggesting a lack of rigour about
recording homelessness. Another factor may have been the
existence of addresses that were entered without valid
postcodes or without the mock postcode for homeless-
ness—it is conceivable that some of these were homeless
addresses. There were also a large number of structured
records of homelessness without a corresponding free text
record containing the strings for which we searched. The
amount of data was too large for an exhaustive search, but it
is conceivable that we missed some free text records indi-
cating homelessness but which described this in other ways.
Another limitation was the extent of missing data: although,
as we suggested above, missingness at random is a plausible
mechanism for the missingness of HoNOS, it is not possible
to test this assumption and our results are inevitably less
secure than those that would have been achieved with
complete data. However, most of the strong effects that we
observed were for variables which were essentially com-
plete, and an analysis using multiple imputation is likely to
be less biased than one restricted to complete cases.
Homelessness has been observed in a significant
minority of psychiatric inpatients in our catchment area for
over 50 years [10]. More recent prevalence estimates from
London and elsewhere vary, but homelessness among
patients admitted to psychiatric wards is plainly neither
restricted to London nor to the UK. Our findings were
consistent with previous reports among mental health ser-
vice users of associations between homelessness and
younger age [4, 8, 27, 28], male gender [28, 29], being
unmarried [28], drug and alcohol misuse [4, 27–29] and
ethnicity [4, 27, 29]. These associations were also consis-
tent with the findings of general population studies in the
US [30, 31]. Novel findings were that homelessness was
most common among people who had not been admitted to
a psychiatric hospital in the preceding 2 years, but also
slightly more common among high as compared to mod-
erate users of inpatient services, and that homelessness was
associated with lower ratings on the two key psychopa-
thology items contained within the HoNOS (hallucinations
and delusions and depressed mood) but higher ratings on
two HoNOS scores reflecting social dysfunction (problems
with relationships and problems with occupation and
activities). Previous research has found that relationship
difficulties and financial difficulties are frequently cited as
an explanation for homelessness [32–34] and this may
perhaps explain this pattern of ratings. Both Canadian and
Australian research [35, 36] suggest that a higher score on
the relationships item is associated with a diagnosis of
personality disorder, while Danish research [37] found
patients with schizophrenia to score higher on this item as
compared to those with depression or mania. Highest mean
score in the occupational difficulties item has similarly
been found to be associated with a diagnosis of schizo-
phrenia [35, 37] or personality disorder [36]. However, the
HoNOS problems with occupation and activities item has
been found to have lower interrater reliability than other
HoNOS items [36].
Because our data on housing spells were often left
truncated, we were unable to ascertain the duration of
homelessness for many of our subjects. Only a small
minority had been recorded as homeless earlier than the
day of admission itself, and it is possible but by no means
certain that much inpatient homelessness occurred shortly
before admission. We also demonstrated that many recor-
ded periods of homelessness begin shortly after admission.
Some proportion of this was presumably an artefact of data
entry, but we suggest that these cases are also likely to
include: (1) individuals for whom exclusion from housing
is bound up with the process of admission but occurs
subsequent to it and (2) individuals who become homeless
because of institutional action at some later point sub-
sequent to admission. This might include people who are
evicted during hospital admission because of rent arrears
Soc Psychiatry Psychiatr Epidemiol (2012) 47:1181–1191 1189
123

but is also likely to include individuals who voluntarily
relinquish tenancies at the instigation of housing and health
services in order to expedite housing [38].
We believe that one of our most striking findings is the
high proportion of homeless individuals for whom no
subsequent address was recorded, even among those fol-
lowed-up for a month after discharge and for whom,
therefore, there was least chance that a change of address
would fail to be recorded (new addresses could only be
entered if a patient was under active follow-up). As the UK
is unusual in homelessness conferring statutory duties on
local authorities, and the UK is considered to have well-
integrated care services, the consistency of these findings
with US studies [7, 13, 14] was surprising. Without the use
of additional data sources, we are unable to comment on
the fate of these individuals. We would hope that our fig-
ures over-estimate literal homelessness but they suggest at
the very least that a large number of homeless individuals
are discharged to very transient accommodation that may
not warrant the recording of an address. What accounts for
the difference in the rate of recorded mobility between
those who were and were not followed-up is not clear. The
lower rate among those who were not followed-up could
simply reflect lack of information in this group. It is,
however, conceivable that fewer efforts to assist rehousing
were made among those who were discharged from follow-
up. We suggest that the short-term housing outcomes of
homeless psychiatric inpatients are not only an important
topic for further research but also should be monitored as
an indicator of the quality of care received in inpatient
settings. This would require that greater care should be
taken to ensure that homeless patients recently discharged
from hospital are followed-up if only in order to record
their housing outcomes.
References
1. Bhugra D (1996) Homelessness and mental health. Cambridge
University Press
2. Koffman J, Fulop N (1999) Homelessness and the use of acute
psychiatric beds: findings from a one-day survey of adult acute
and low-level secure psychiatric patients in North and South
Thames regions. Health Soc Care Commun 7:140–147. doi:
10.1046/j.1365-2524.1999.00156.x
3. Salit SA, Kuhn EM, Hartz AJ, Vu JM, Mosso AL (1998) Hos-
pitalization costs associated with homelessness in New York
City. N Engl J Med 338:1734–1740
4. Rosenheck R, Seibyl C (1998) Homelessness: health service use
and related costs. Med Care 36:1256–1264
5. Herman DB, Susser ES, Jandorf L, Lavelle J, Bromet EJ (1998)
Homelessness among individuals with psychotic disorders hos-
pitalized for the first time: findings from the Suffolk County
Mental Health Project. Am J Psychiatry 155:109–113 Retrieved
May 27, 2010
6. Mowbray CT, Johnson VS, Solarz A (1987) Homelessness in a
state hospital population. Hosp Commun Psychiatry 38:880–882
Retrieved June 6, 2010
7. Appleby L, Desai PN (1985) Documenting the relationship
between homelessness and psychiatric hospitalization. Hosp
Commun Psychiatry 36:732–737 Retrieved May 27, 2010
8. Susser ES, Lin SP, Conover SA (1991) Risk factors for home-
lessness among patients admitted to a state mental hospital. Am J
Psychiatry 148:1659–1664 Retrieved June 6, 2010
9. Ash D, Haynes J, Braben P, Galletly C (2003) Violence, self-
harm, victimisation and homelessness in patients admitted to an
acute inpatient unit in South Australia. Int J Soc Psychiatry
49:112–118. doi:10.1177/0020764003049002004
10. Whiteley JS (1955) Down and out in London; mental illness in
the lower social groups. Lancet 269:609–610 Retrieved June 14,
2010
11. Herzberg JL (1987) No fixed abode. A comparison of men and
women admitted to an East London psychiatric hospital. Br J
Psychiatry 150:621–627 Retrieved June 13, 2010
12. Fisher N, Turner S, Pugh R (1990) Homeless and mentally ill.
Lancet 335:916–917. doi:10.1016/0140-6736(90)90516-8
13. Greenberg GA, Hoblyn J, Seibyl C, Rosenheck R (2006) Housing
outcomes for hospitalized homeless veterans. J Health Care Poor
Underserved 17:425–440 Retrieved June 6, 2010
14. Caton CL, Shrout PE, Eagle PF, Opler LA, Felix A, Dominguez
B (1994) Risk factors for homelessness among schizophrenic
men: a case-control study. Am J Public Health 84:265–270. doi:
10.2105/AJPH.84.2.265
15. Stewart R, Soremekun M, Perera G, Broadbent M, Callard F,
Denis M et al (2009) The South London and Maudsley NHS
Foundation Trust Biomedical Research Centre (SLAM BRC)
case register: development and descriptive data. BMC Psychiatry
9:51. doi:10.1186/1471-244X-9-51
16. Wing JK, Beevor A, Curtis R, Park S, Hadden S, Burns A (1998)
Health of the Nation Outcome Scales (HoNOS). Research and
development. Br J Psychiatry 172:11–18. doi:10.1192/bjp.
172.1.11
17. Royston P (2005) Multiple imputation of missing values: update
of ice. Stata J 5:188–201
18. Tulloch AD, Fearon P, David AS (2011) Residential mobility
among patients admitted to acute psychiatric wards. Health Place
17:859–866
19. Bodner TE (2008) What improves with increased missing data
imputations? Struct Equ Model: Multidiscip J 15:651. doi:
10.1080/10705510802339072
20. Royston P, Ambler G, Sauerbrei W (1999) The use of fractional
polynomials to model continuous risk variables in epidemiology.
Int J Epidemiol 28:964–974 Retrieved March 26, 2010
21. Royston P, Sauerbrei W, Becher H (2010) Modelling continuous
exposures with a ‘‘spike’’ at zero: a new procedure based on
fractional polynomials. Stat Med Adv online publ. doi:
10.1002/sim.3864
22. Hosmer DW, Lemeshow S, May S (2008) Applied survival
analysis: regression modeling of time-to-event data. Wiley
23. Royston P, Sauerbrei W (2008) Multivariable model-building: a
pragmatic approach to regression analysis based on fractional
polynomials for modelling continuous variables. Wiley
24. Royston P, Sauerbrei W (2003) Stability of multivariable frac-
tional polynomial models with selection of variables and trans-
formations: a bootstrap investigation. Stat Med 22:639–659. doi:
10.1002/sim.1310
25. Harrell FE (2001) Regression modeling strategies: with applica-
tions to linear models, logistic regression and survival analysis.
Springer, New York
26. Rubin DB (1987) Multiple imputation for nonresponse in sur-
veys. John Wiley & Sons, Inc, New York
1190 Soc Psychiatry Psychiatr Epidemiol (2012) 47:1181–1191
123

27. Adams J, Rosenheck R, Gee L, Seibyl CL, Kushel M (2007)
Hospitalized younger: a comparison of a national sample of
homeless and housed inpatient veterans. J Health Care Poor
Underserved 18:173–184. doi:10.1353/hpu.2007.0000
28. Nordentoft M, Knudsen HC, Jessen-Petersen B, Krasnik A, Sa-
elan H, Brodersen AM et al (1997) Copenhagen Community
Psychiatric Project (CCPP): characteristics and treatment of
homeless patients in the psychiatric services after introduction of
community mental health centres. Soc Psychiatry Psychiatr Epi-
demiol 32:369–378. doi:10.1007/BF00788176
29. Folsom DP, Hawthorne W, Lindamer L, Gilmer T, Bailey A,
Golshan S et al (2005) Prevalence and risk factors for home-
lessness and utilization of mental health services among 10, 340
patients with serious mental illness in a large public mental health
system. Am J Psychiatry 162:370–376. doi:10.1176/appi.ajp.162.
2.370
30. Greenberg GA, Rosenheck RA (2010) Mental health correlates of
past homelessness in the National Comorbidity Study Replica-
tion. J Health Care Poor Underserved 21:1234–1249. doi:
10.1353/hpu.2010.0926
31. Greenberg GA, Rosenheck RA (2010) Correlates of past home-
lessness in the National Epidemiological Survey on Alcohol and
Related Conditions. Adm Policy Ment Health 37:357–366. doi:
10.1007/s10488-009-0243-x
32. Caton CL (1995) Mental health service use among homeless and
never-homeless men with schizophrenia. Psychiatr Serv
46:1139–1143 Retrieved June 6, 2010
33. Martijn C, Sharpe L (2006) Pathways to youth homelessness. Soc
Sci Med 62:1–12
34. Mojtabai R (2005) Perceived reasons for loss of housing and
continued homelessness among homeless persons with mental
illness. Psychiatr Serv 56:172–178. doi:10.1176/appi.ps.56.2.172
35. Kisely S, Campbell L, Crossman D, Gleich S, Campbell J (2007)
Are the Health of the Nation Outcome Scales a valid and practical
instrument to measure outcomes in North America? A three-site
evaluation across Nova Scotia. Commun Ment Health J
43:91–107. doi:10.1007/s10597-006-9067-2
36. Trauer T, Callaly T, Hantz P, Little J, Shields R, Smith J (1999)
Health of the Nation Outcome Scales. Results of the Victorian
field trial. Br J Psychiatry 174:380–388. doi:10.1192/bjp.174.
5.380
37. Bech P, Bille J, Schutze T, Søndergaard S, Wiese M, Waarst S
(2003) Health of the Nation Outcome Scales (HoNOS): imple-
mentability, subscale structure and responsiveness in the daily
psychiatric hospital routine over the first 18 months. Nord J
Psychiatry 57:285–290. doi:10.1080/08039480310002156
38. Social Exclusion Unit (2004) Mental health and housing: fact-
sheet 6. Office of the Deputy Prime Minister, London
Soc Psychiatry Psychiatr Epidemiol (2012) 47:1181–1191 1191
123