Embed Size (px)
Citation preview
Tinea CapitisSuzy Tinker
CNS Paediatric Dermatology
Homerton NHS Foundation Trust
Making a diagnosis of scalp ringworm Suggested by presence of all or some of the following: Patches of scalp hair loss, thinning sometimes Scaling[minimal or thick scales may be present around hairs] Crusting or oozing Itching[of variable severity] Background erythema of scalp, or red scaly lesions, may
also occur on the body Post cervical lymphadenopathy
IMPORTANT TO BEGIN TREATMENT AS SOON AS CLINICAL DIAGNOSIS IS MADE
Laboratory Confirmation
Mycology samples should be taken of scalp scrapings, and in the case of Endothrix infections[within the hair shaft] a hair sample with the root.
Blunt forceps can be used to remove a hair and root, without any trauma
Samples should be transported in appropriate mycology pack or black paper securely sealed.
Majority of children in Hackney have Trichophyton Tonsurans as the organism, causing the endothrix infection.Endothrix are more difficult to treat, requiring oral anti fungals.
Infection are usually anthrophilic rather than zoophilic. More easily spread from person to person
Treatment clinical cases
BAD [British Association of Dermatologists] are changing guidelines at present, from oral Griseofulvin syrup 15mg-20mg/kg daily for 12 weeks., to Terbinafine tablets.
On web site they still have both treatments. Terbinafine orally which comes in a 250mg tablet, and is
divided into appropriate dose for weight ,and can then be crushed and given daily.
Under 20 kg [1/4 a tablet ]= 62.5 mg daily for 4 weeks 20kg to 40 kg [1/2 a tablet]=125mg daily for 4 weeks Over 40kg one tablet=250mg daily for 4 weeks
Family members Siblings or close relatives if they are children should wash
their hair twice a week with Nizoral [Ketaconazole shampoo] for 4 weeks, even if they have no sign of infection.
This may prevent them from catching the disease which is spread from fungal spores.
Many children are carriers of Tinea, a small proportion go on to develop the infection, others lose the fungus, whilst the rest remain carriers, thus spreading it in schools and nurseries.
Complications Kerion
A Kerion can develop on children's scalps. This is an abscess caused by a dramatic immune response to a
dermatophyte fungal infection, it is often misdiagnosed as a bacterialy infected boil. Attempts to lance the Kerion are usually unsuccesful, and cause scarring.
To confirm the diagnosis scrapings and hair samples can be taken from the affected area, bacterial swabs can also be taken, as there may well be a secondary infection .
Treatment is oral antifungals as before, oral antibiotics if needed, antifungal shampoo Ketaconazole to reduce the risk of spreading to others.
Parents often get Tinea Corporis, and siblings may well get Tinea capitis.
Id Reaction/ Autoeczematisation An Id reaction [autoeczematisation ]is an acute generalised
skin reaction to a variety of stimuli. The stimuli may be a pre-existing or new eczema or skin infection with fungi, bacteria viruses or parasites. The rash tends to occur at a site distant from the original infection.
If a child presents with a wide spread eczema to face , limbs and body, more severe than they have ever had eczema, or have never had eczema, look at the scalp.
Scalp may well show the signs of Tinea Capitis . Treat both theTinea and theEczema, skin soon settles.
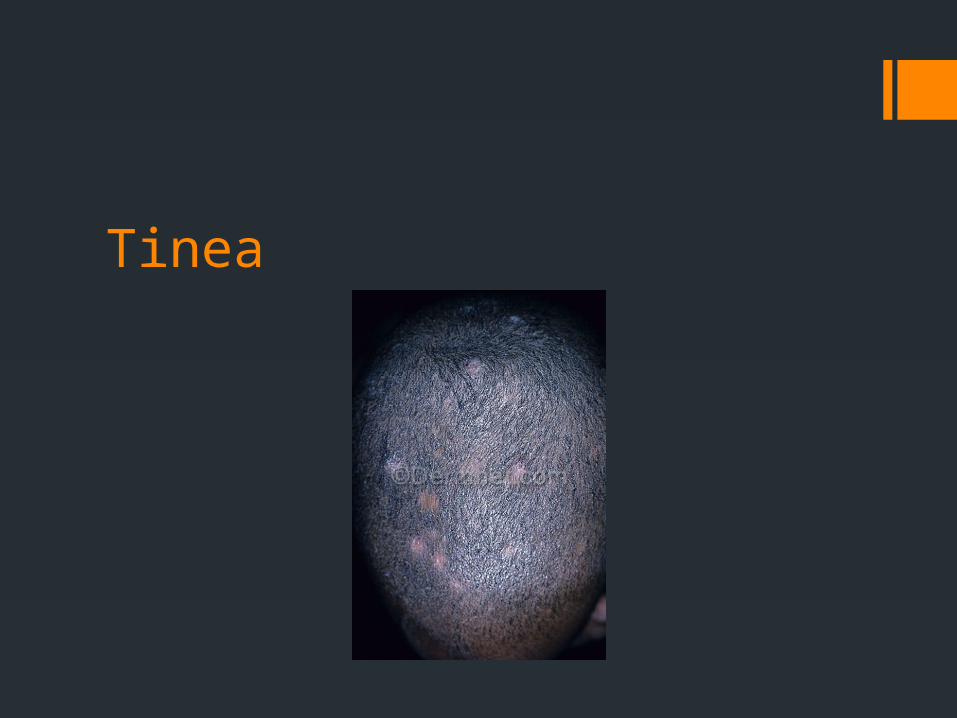
Tinea
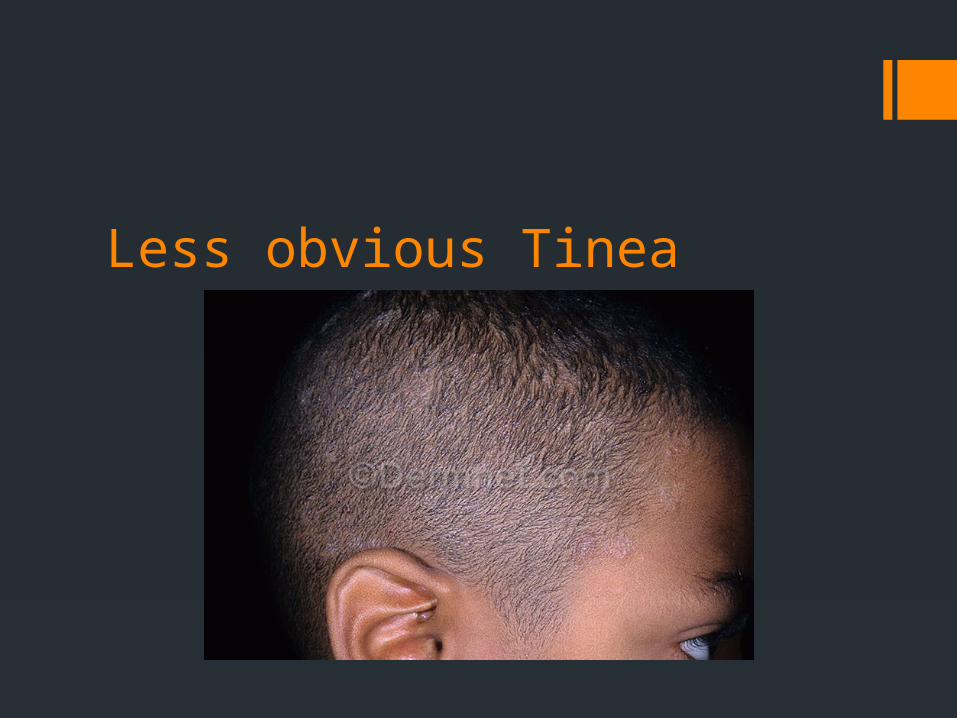
Less obvious Tinea
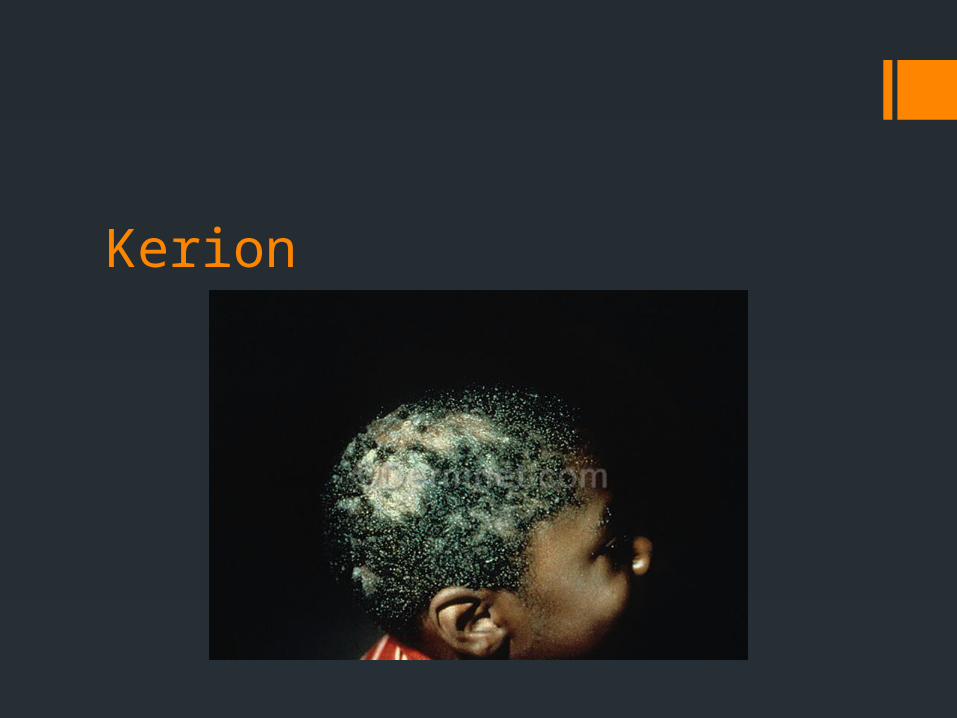
Kerion
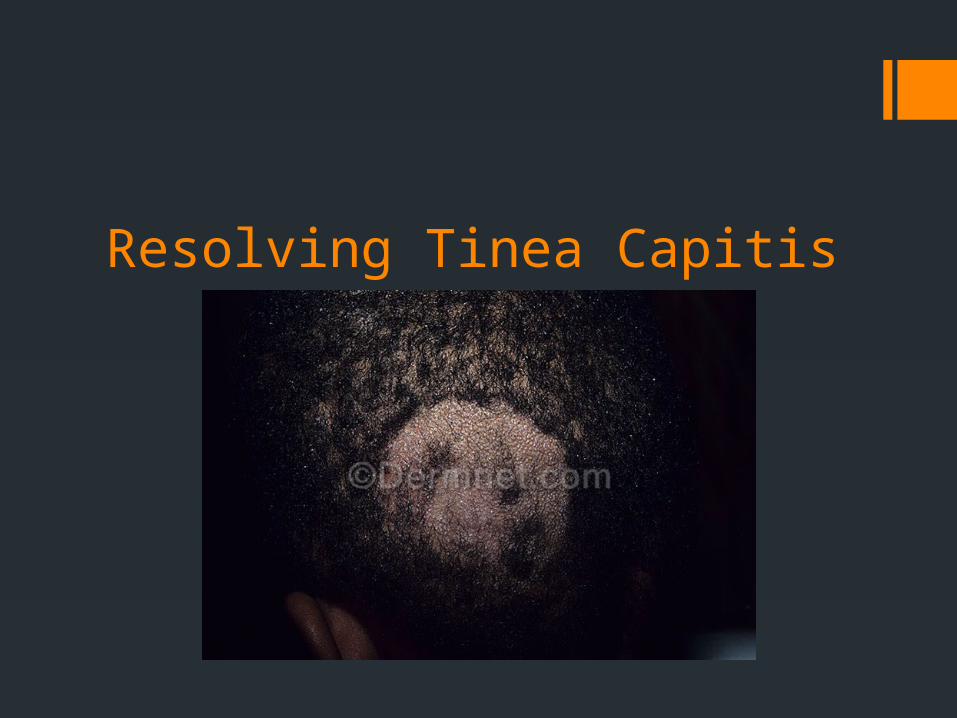
Resolving Tinea Capitis

Severe Tinea Capitis

Tinea capitis
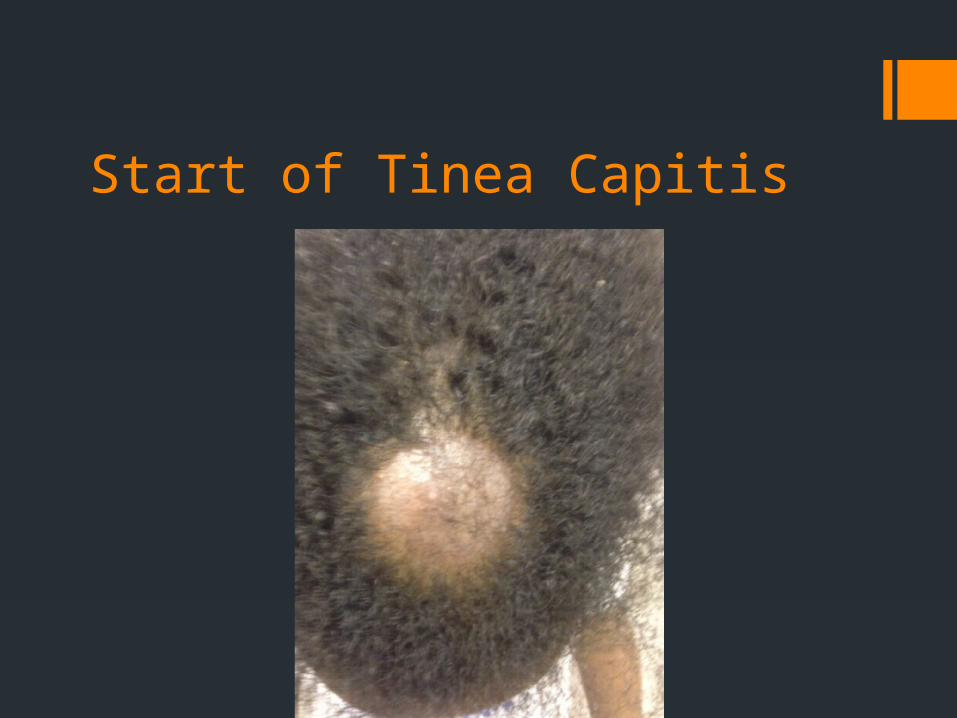
Start of Tinea Capitis
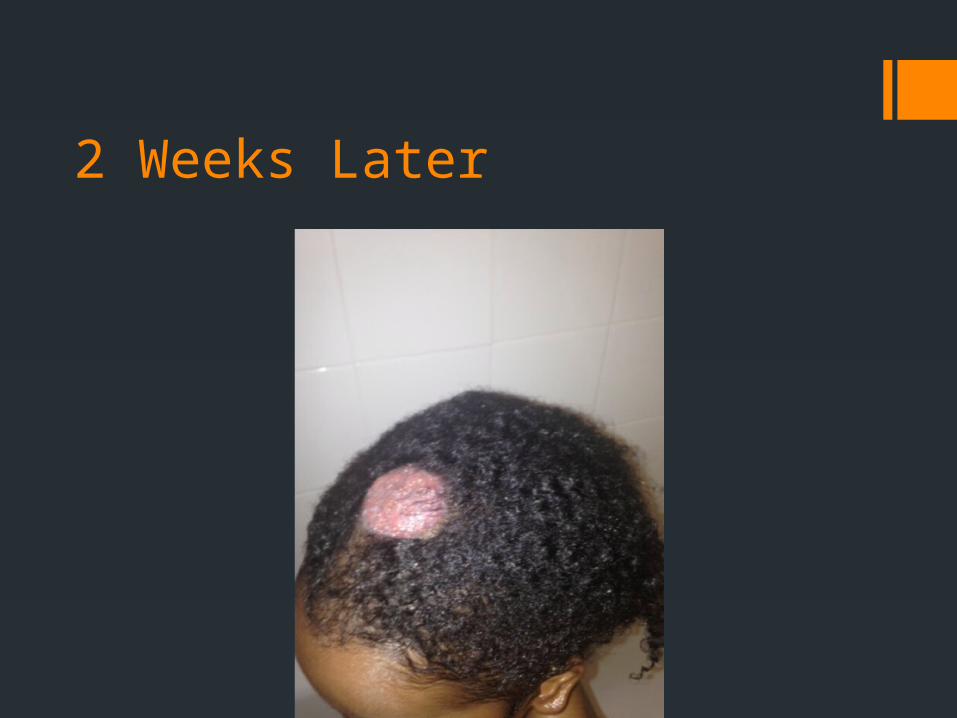
2 Weeks Later
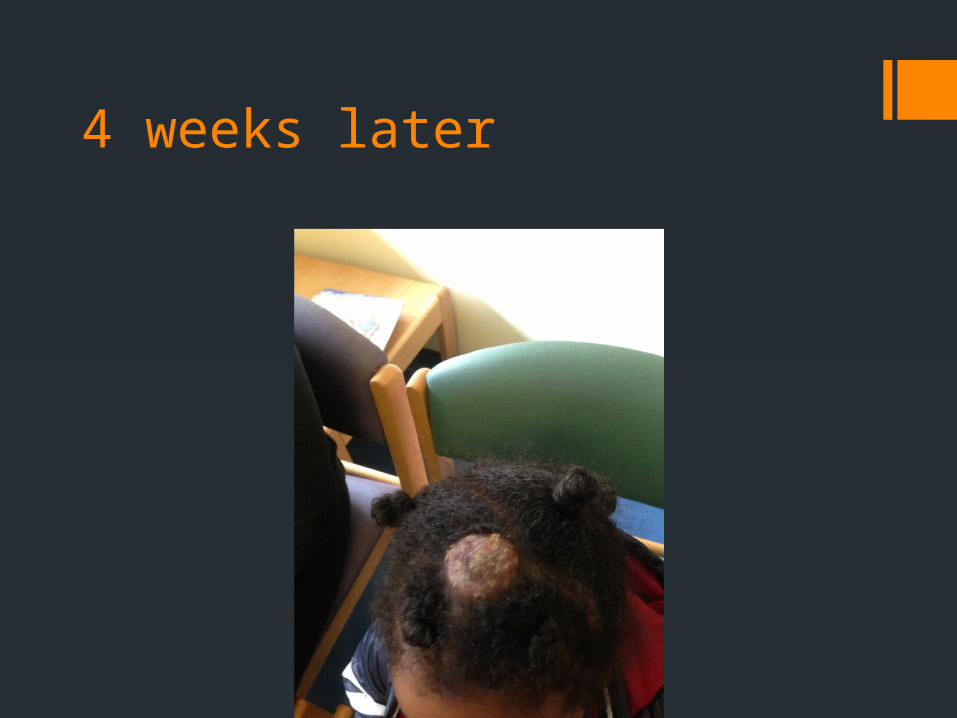
4 weeks later

9 days post treatment



























