Embed Size (px)
DESCRIPTION
Tissue Renewal and Repair Regeneration , Healing & Fibrosis. Prof.Dr.Ferda ÖZKAN. The body's ability to replace injured or dead cells and to repair tissues after inflammation is critical to survival. - PowerPoint PPT Presentation
Citation preview
Tissue Renewal and Repair
Regeneration,Healing & Fibrosis
Prof.Dr.Ferda ÖZKAN
• The body's ability to replace injured or dead cells and to repair tissues after inflammation is critical to survival.
• The repair of tissue can be broadly separated into two processes, regeneration and healing .
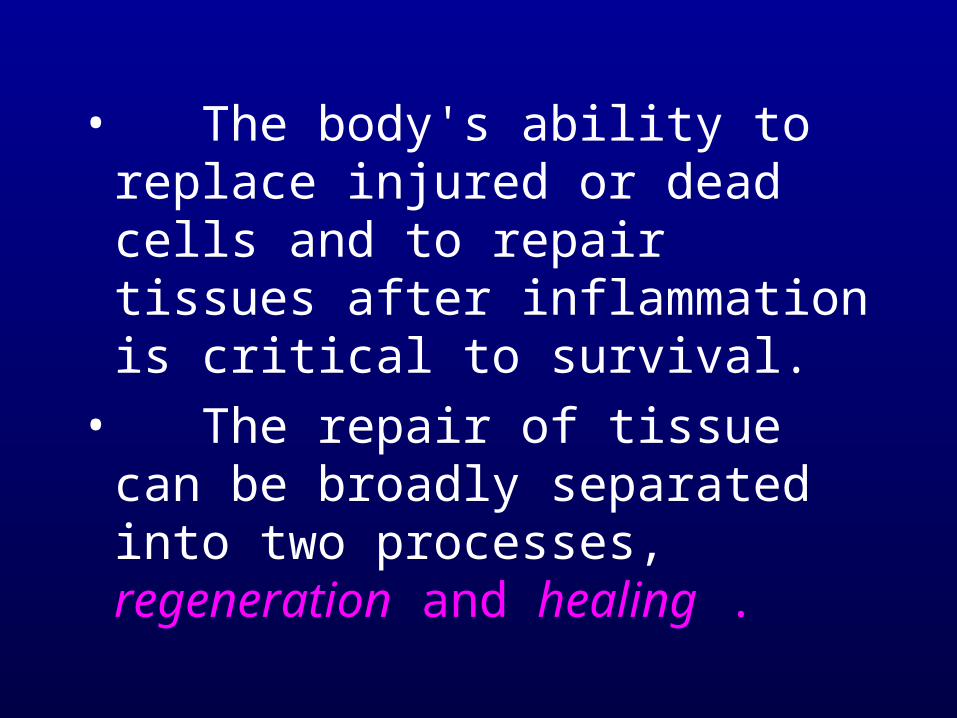
Tissue response to injury
• Regeneration refers to growth of cells and tissues to replace lost structures.
Regeneration requires an intact connective tissue scaffold.
Healing is a response to tissue injury, and represents an attempt to restore integrity to an injured tissue.
It is a tissue response:
(1) to a wound (commonly in the skin),
(2) to inflammatory processes in internal organs,
(3) to cell necrosis in organs incapable of regeneration.
• Healing consists of variable proportions of two distinct processes-regeneration, and the laying down of fibrous tissue, or scar formation.
• Healing with scar formation occurs if the extracellular matrix (ECM) framework is damaged, causing alterations of the tissue architecture.
Extracellular Matrix • Cells grow, move, and differentiate in
intimate contact with macromolecules outside the cell that constitute the ECM.
• The ECM is secreted locally and assembles into a network in the spaces surrounding cells
• Three groups of macromolecules, which are often physically associated, constitute the ECM:
• (1) fibrous structural proteins, such as the collagens and elastins;
• (2) a diverse group of adhesive glycoproteins;
• (3) proteoglycans and hyaluronic acid.
• These macromolecules are present in intercellular junctions and cell surfaces and form two general organizations:
• interstitial matrix The interstitial matrix is present in spaces between epithelial, endothelial, and smooth muscle cells and in connective tissue. It consists of fibrillar and nonfibrillar collagen, elastin, fibronectin, proteoglycans, hyaluronate, and other components.
• basement membrane (BM). BMs are produced by epithelial and mesenchymal cells and are closely associated with the cell surface. They consist of a network of amorphous nonfibrillar collagen (mostly type IV), laminin, heparan sulfate, proteoglycan, and other glycoproteins.
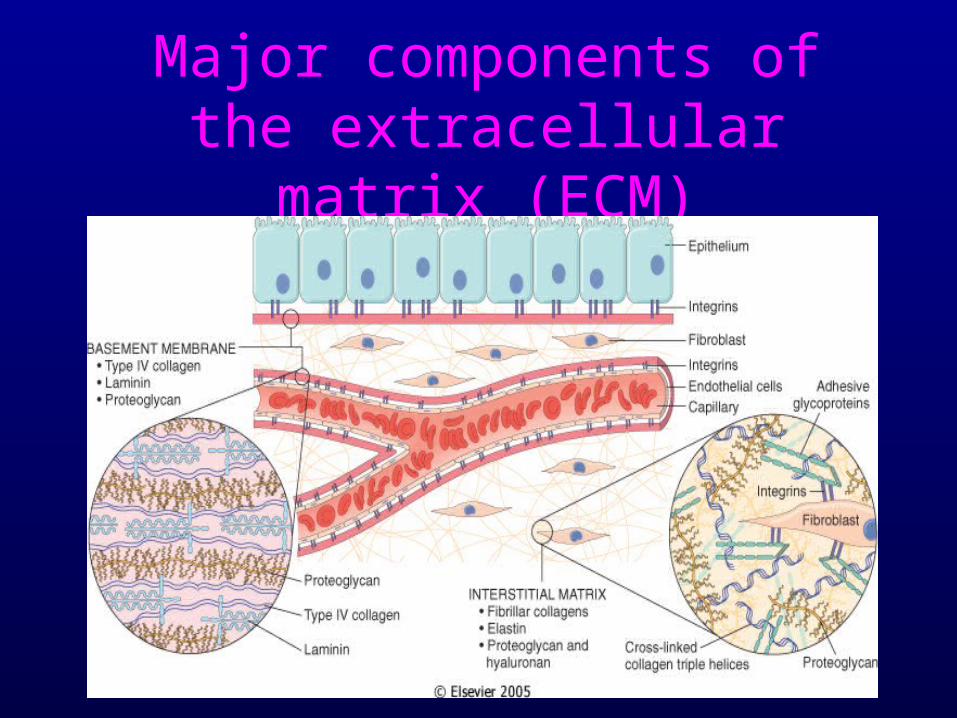
Major components of the extracellular matrix (ECM)
The Extracellular Matrix
• Major components– Collagens– Basement membranes– Elastic fibers– Fibronectin– Proteoglycans
• The Collagens– Type I: found in skin, bone, and mature scars– Type II: major component of cartilage– Type III: abundant in embryonic and pliable
tissues First collagen deposited in wound healing– Type IV: does not form fibers, but associates with
laminin and other matrix components, and is exclusively found in basement membranes
• Collagen catabolism and collagenase– Mature collagen is slowly remodeled via the
action of collagenases– Fibroblasts are the main source of collagenase,
although it is also produced by macrophages, epithelial, and endothelial cells
– The remodeling process is controlled by the binding of fibronectin and ubiquitous collagenase inhibitors
• Basement membranes– All epithelia are separated from the stroma by
basement membrane– All vascular endothelial cells are separated
from the underlying stroma by a basement membrane, except for the sinusoidal endothelium of the bone marrow, lymphoid organs, and liver
– Basement membranes are synthesized by the cells resting on them (epithelia, endothelium)
– Contain collagen type IV, laminin, entactin, and heparin sulfate proteoglycan (perlecan).
• Elastic fibers– Whereas tensile strength is provided by
collagen, elastic fibers provide recoil, and thus tend to be found in the aorta, smaller arteries, skin, lung, and uterus.
• Structural glycoproteins– Fibronectin (nectere, to bind)
• Binds to collagens, proteoglycans, fibrinogen, fibrin, cell surfaces, bacteria and DNA
• One of the first structural molecules deposited during embryonic development, and, by extension, in the early phases of wound healing
• Found in tissue and plasma
• Synthesized by hepatocytes
• Structural glycoproteins– Proteoglycans
• Used to be called mucopolysaccharides, but are now properly referred to as glycosaminoglycans
• Highly hydrophylic, and form hydrated gels, even at low concentration
• Deposited early in embryologic life, and by extension, early in wound healing.
Cell Proliferation
• In adult tissues, the size of cell populations is determined by the rates of cell proliferation, differentiation, and death by apoptosis.
Cell Proliferation
• Classification of cells by their proliferative potential
– Labile– Stable (quiescent)
– Permanent
Classification of CellsLabile cells
• This sub-population of cells is constantly turned over: – epithelium of skin
– mucous membranes (GIS)
– oviducts
– urothelium
– endometrium
– seminiferous tubules
– bone marrow
– lymphoid tissue.
• These cells have a short, finite life span, die via apoptosis, and are rapidly replaced.
Stable cells Stable cells are a sub-population of cells that are normally replaced very slowly, but are capable of rapid renewal after tissue loss.
• Hepatocytes and the proximal convoluted tubule cells of the kidney are good examples. – all glandular parenchymal cells
– fibroblasts,
– endothelial cells
– smooth muscle cells
– osteoblasts
– chondroblasts.
Permanent cells• contain cells that have left the cell cycle and
cannot undergo mitotic division in postnatal life
• Permanent cells are found in the central nervous system and heart.
• Once they are destroyed, they cannot regenerate. – neurons – cardiac muscle cells– skeletal muscle cells.
STEM CELLS
• Stem cell research is one of the most exciting topics in modern-day biomedical investigation and stands at the core of a new field called regenerative medicine
STEM CELLS
• Stem cells are characterized by their prolonged self-renewal capacity and by their asymmetric replication.
• Asymmetric replication describes a special property of stem cells; that is, in every cell division, one of the cells retains its self-renewing capacity while the other enters a differentiation pathway and is converted to a mature, nondividing population
Embryonic Stem Cells (ES)
• Embryos contain pluripotent ES cells, which can give rise to all the tissues of the human body.
• Such cells can be isolated from normal blastocysts, the structures formed at about the 32-cell stage during embryonic development
Adult Stem Cells
• Many tissues in adult animals have been shown to contain reservoirs of stem cells, which are called adult stem cells.
• Compared to ES cells, which are pluripotent, adult stem cells have a more restricted differentiation capacity and are usually lineage-specific.
• Stem cells are located in sites called niches, which differ among various tissues .
• in the gastrointestinal tract, they are located at the isthmus of stomach glands and at the base of the crypts of the colon (each colonic crypt is the clonal product of a single stem cell).
• Niches have been identified in other tissues, such as the bulge area of hair follicles and the limbus of the cornea.
• We first consider bone marrow stem cells and then discuss stem cells located in other tissues (tissue stem cells).
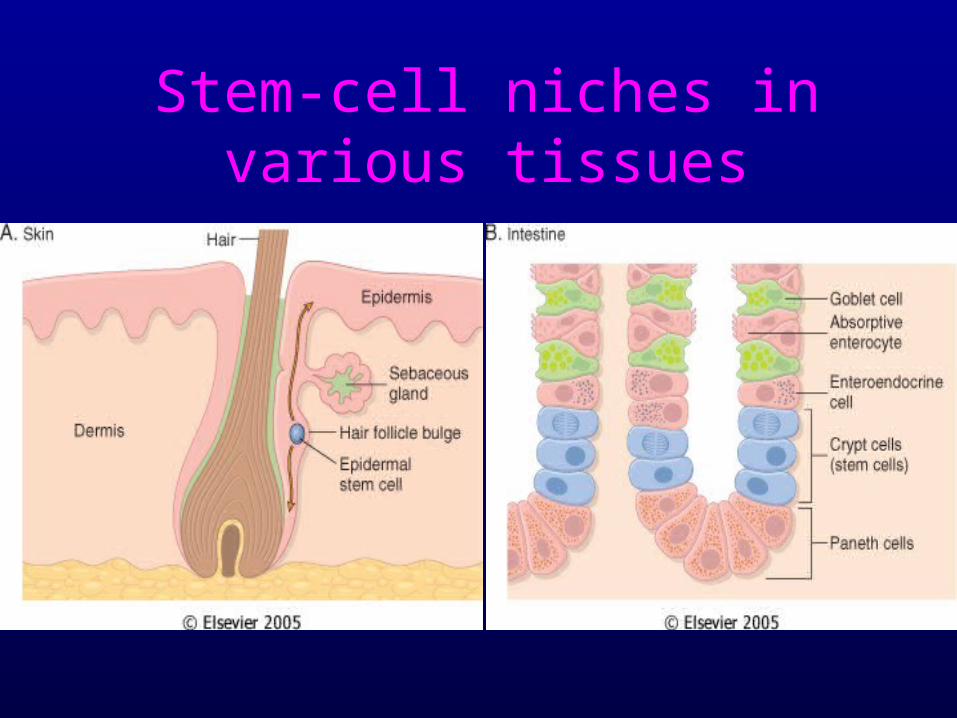
Stem-cell niches in various tissues
• In addition to bone marrow cells that may migrate to various tissues after injury, adult stem cells reside permanently in most organs.
• These cells (known as tissue stem cells) can generate the mature cells of the organs in which they reside.
• However, their differentiation commitment can change when they are transplanted into a different tissue.
Cell - Matrix Interactions• Margination and diapedesis:
– soluble factors attract cells to the wound site (chemotaxis),
– whereas the extracellular matrix helps align these cells for proper wound healing.
• Integrins: – Integrins are cell-surface receptors. – By interacting with integrins, the extracellular
matrix can directly modify cell behavior, via cytoskeletal proteins.
• Cytokines and Growth Factors– Macrophage-derived growth factor (MDGF)– Platelet-derived growth factor (PDGF)– Epidermal growth factor (EGF)– Fibroblast growth factor (FGF)– Transforming growth factor-beta (TGF-)
Cell- Cell Interactions
• Cytokines and Growth Factors– A single experimental dose of a cytokine at the
time of injury changed the rate of healing, the type of matrix deposited, and the cell types present in the wound.
• PDGF accelerates deposition of provisional matrix
• TGF- hastens deposition of collagen
• FGF induces a florid angiogenic response
Wound HealingWound Healing
• Induction of an acute inflammatory response• Regeneration of parenchymal cells• Migration and proliferation of both parenchymal
and connective tissue cells• Synthesis of extracellular matrix proteins• Remodeling• Collagenization and maturation of wound
Stages of Healing
• Inflammation
• Granulation tissue (soft callus)
• Scar – Fibrosis (hard callus)
• Remodeling
• Wound strength
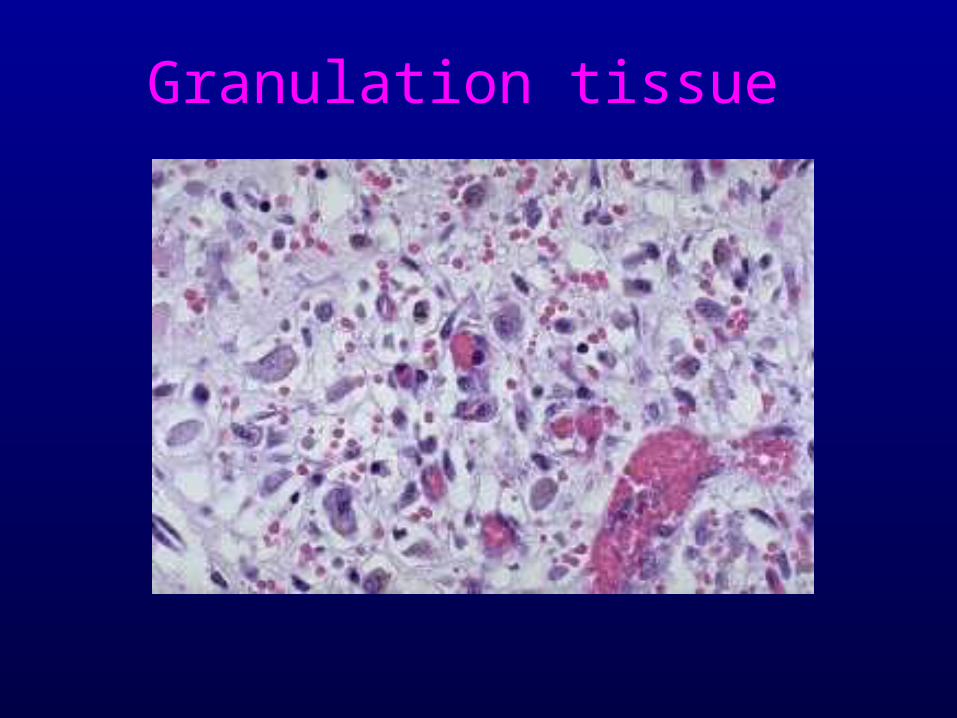
Granulation tissue

Healing Skin wound
Wound Healing by Primary Intention
• Contraction– Accounts for a reduction in size of the defect
primarily by the action of myofibroblasts– This process produces faster healing, – Myofibroblasts account for contraction, and
represent an intermediate type of cell, between a fibroblast and a myocyte
• Primary intention: the usual case with a surgical wound, in which there is a clean wound with well-apposed edges, and minimal clot formation.– No/minimal scar.
• Secondary intention: when wound edges cannot be apposed, (e.g., following wound infection), then the wound slowly fills with granulation tissue from the bottom up. – A large scar usually results.
Stages of Wound Healing
• Immediate : Blood clot• 2-3hours : Early Inflammation• 2-3 days : Macrophages, clearing• 10-14 days : Soft Granulation tissue• Weeks : Fibrous hard scar• M’nths -Yrs : Remodeling, minimal scar
Skin Wound HealingBy First intention• Clean cut wound• Less injury• Less dead tissue• Less infection• Faster healing• Minimal scar• Minimal
complications
By Second intention
• Large rough wound
• More injury
• More dead tissue
• More infection
• Delayed healing
• More scar
• More complications
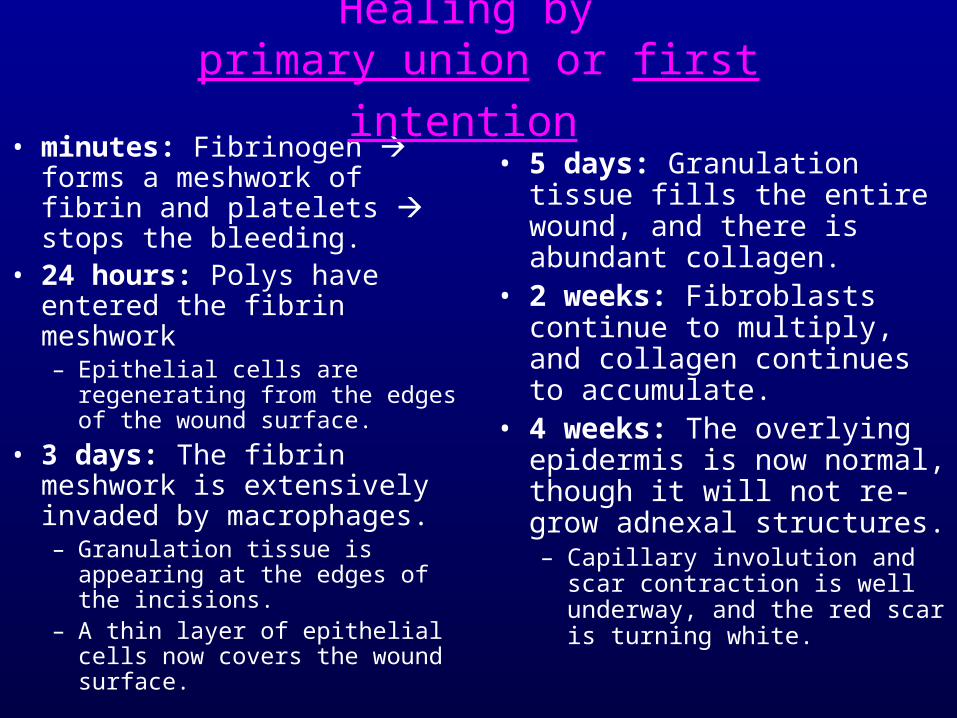
• minutes: Fibrinogen forms a meshwork of fibrin and platelets stops the bleeding.
• 24 hours: Polys have entered the fibrin meshwork – Epithelial cells are regenerating
from the edges of the wound surface.
• 3 days: The fibrin meshwork is extensively invaded by macrophages.– Granulation tissue is appearing
at the edges of the incisions. – A thin layer of epithelial cells
now covers the wound surface.
• 5 days: Granulation tissue fills the entire wound, and there is abundant collagen.
• 2 weeks: Fibroblasts continue to multiply, and collagen continues to accumulate.
• 4 weeks: The overlying epidermis is now normal, though it will not re-grow adnexal structures. – Capillary involution and scar
contraction is well underway, and the red scar is turning white.
Healing by
primary union or first intention
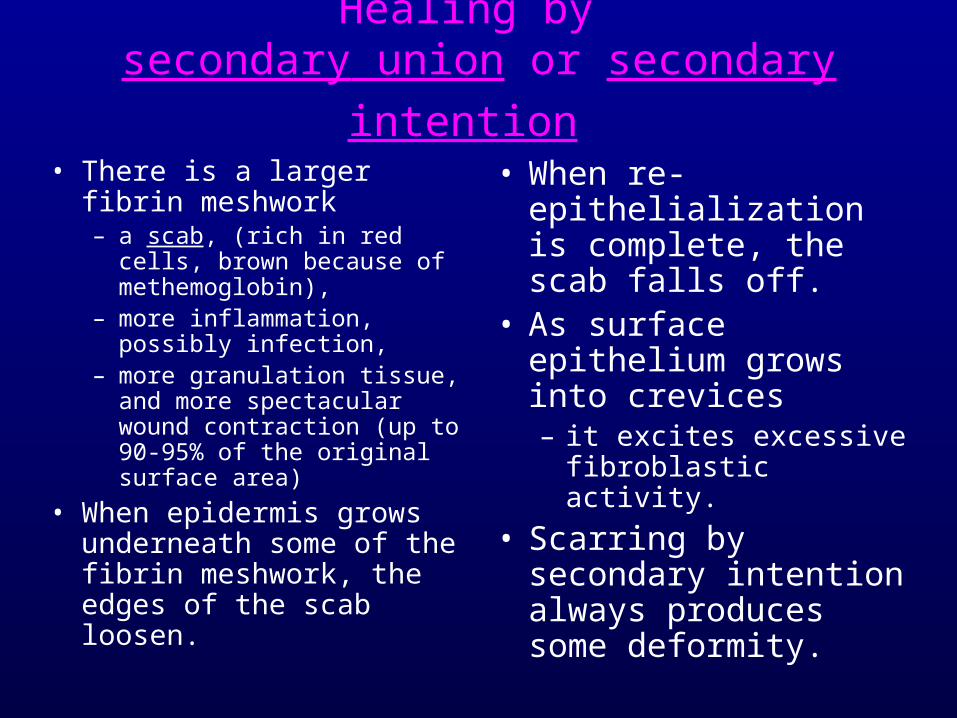
• There is a larger fibrin meshwork– a scab, (rich in red cells,
brown because of methemoglobin),
– more inflammation, possibly infection,
– more granulation tissue, and more spectacular wound contraction (up to 90-95% of the original surface area)
• When epidermis grows underneath some of the fibrin meshwork, the edges of the scab loosen.
• When re-epithelialization is complete, the scab falls off.
• As surface epithelium grows into crevices – it excites excessive
fibroblastic activity.
• Scarring by secondary intention always produces some deformity.
Healing by
secondary union or secondary intention
• Repair– The orderly process by which a wound is
eventually replaced by a scar– Destruction of epithelium only is termed an
erosion, and heals exclusively by regeneration– If destruction of the basement membrane occurs
(extracellular matrix), then a scar will form
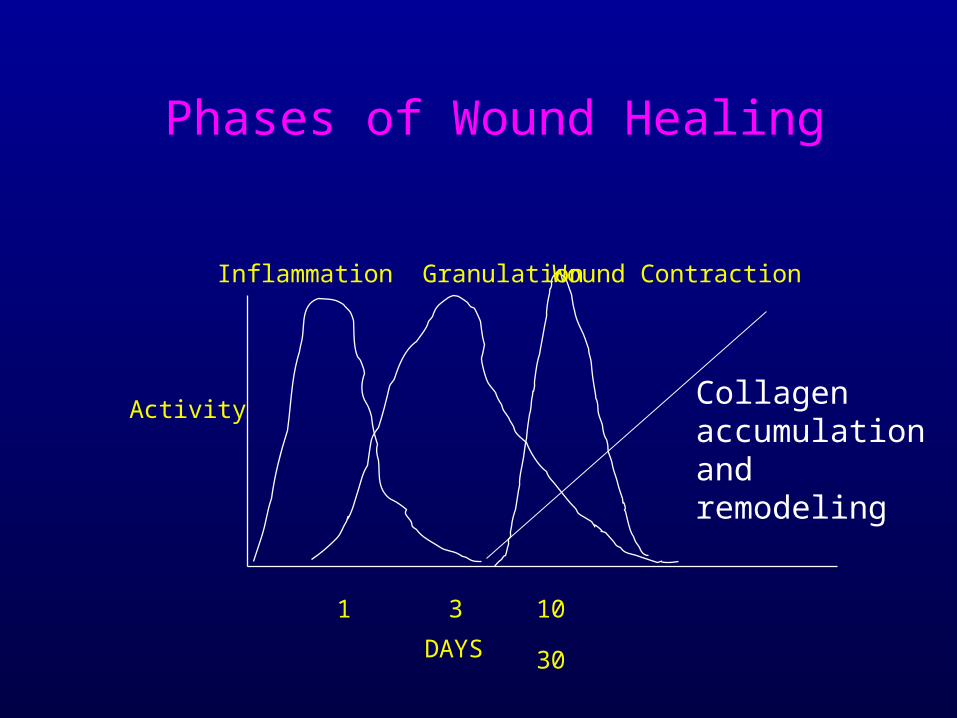
Phases of Wound Healing
Wound ContractionInflammation Granulation
DAYS
Activity
1 3 10 30
Collagen accumulation and remodeling

• Repair – Granulation tissue is the initial event in the repair of
an injury, and consists of • richly vascular connective tissue which contains
capillaries,
• young fibroblasts,
• a variable infiltrate of inflammatory cells.
– Do not confuse with GRANULOMA
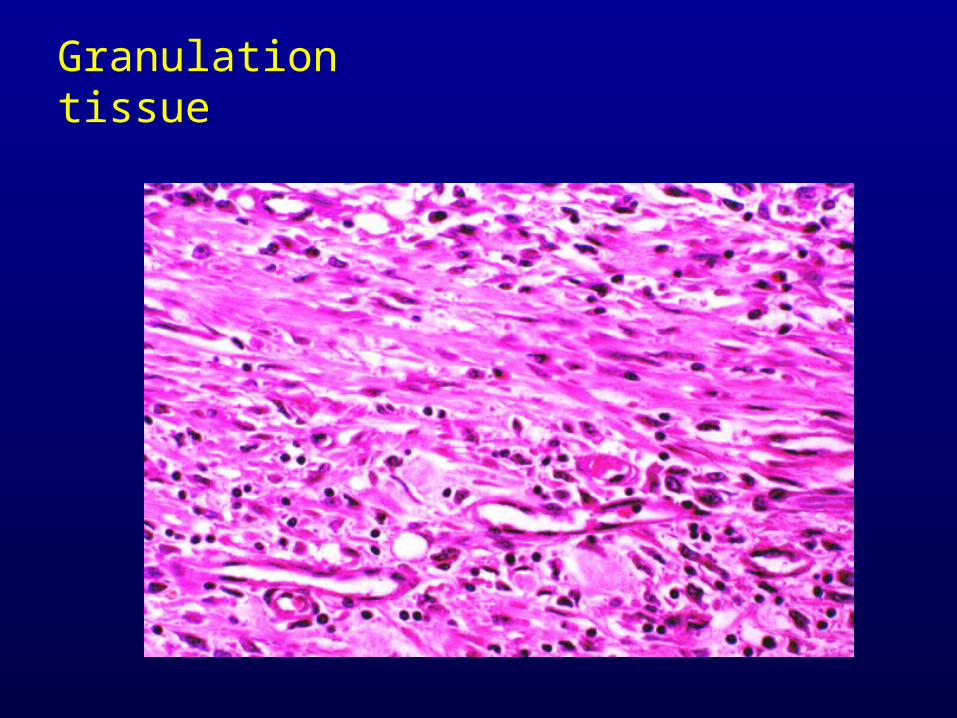
Granulation tissue
• Repair – As the repair of the wound progresses, collagen
synthesis exceeds degradation and remodeling, and a scar is formed.
– The tensile strength of the wound continues to increase over many months, becoming maximal at about a year.
• Regeneration– In skin, cytokine and growth factor signals for
regeneration are probably related to the loss of contact inhibition.
– Proliferation of epithelia continues, until contact is re-established.
Factors affecting Healing
Systemic
• Age
• Nutrition
• Vitamin def.
• Immune status
• Chronic diseases– DM, TB, etc.
Local
• Necrosis
• Infection
• Apposition
• Blood supply
• Mobility
• Foreign body
Factors that influence wound healing
• Type, size, and location of the wound• Vascular supply
– diabetics heal poorly
• Infection – delays wound healing and leads to more granulation tissue
and scarring
• Movement – wounds over joints do not heal well due to traction
• Radiation – ionizing radiation is bad, UV is good.
• Overall nutrition– vitamin and protein deficiencies lead to poor wound
healing,
– especially vitamin C, which is involved in collagen synthesis
• Age: – younger is definitely better
• Hormones– corticosteroids drastically impair wound healing, because
of their profound effect on inflammatory cells.
Complications :• Non Healing / delayed healing
• Scar contractures (burns, ulcers)
• Defective scar formation
• Keloid
• Adhesions (peritoneum, pleura, pericardium)
• Defective scar formation
– Dehiscence or ulceration is usually due to:• Wound infection (common)• Malnutrition (scurvy)• Hypoxia with ulceration,
– usually due to inadequate vascularity in a skin flap (common).
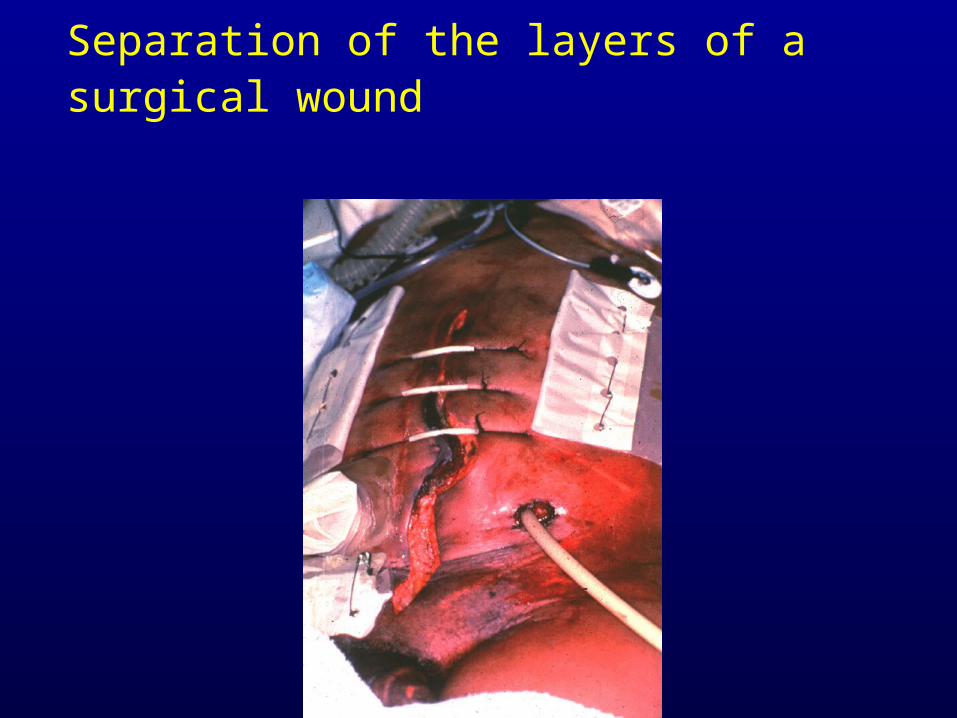
Separation of the layers of a surgical wound
• Excessive Scar Formation– Keloids (hypertrophic scars) are the result of
over-exuberant production of scar tissue, which is primarily composed of type III collagen
• The cause is thought to be due to genetic factors, perhaps due to lack of the proper collagenases to degrade type III collagen.

Keloid

Peritoneum Adhesions
Healing in specific tissues
Heart• Cardiac myocytes are permanent cells.
• They do not divide, and the heart thus heals by resolution (dead myocytes are phagocytized by macrophages) and collagenous scar formation.

Acute MI
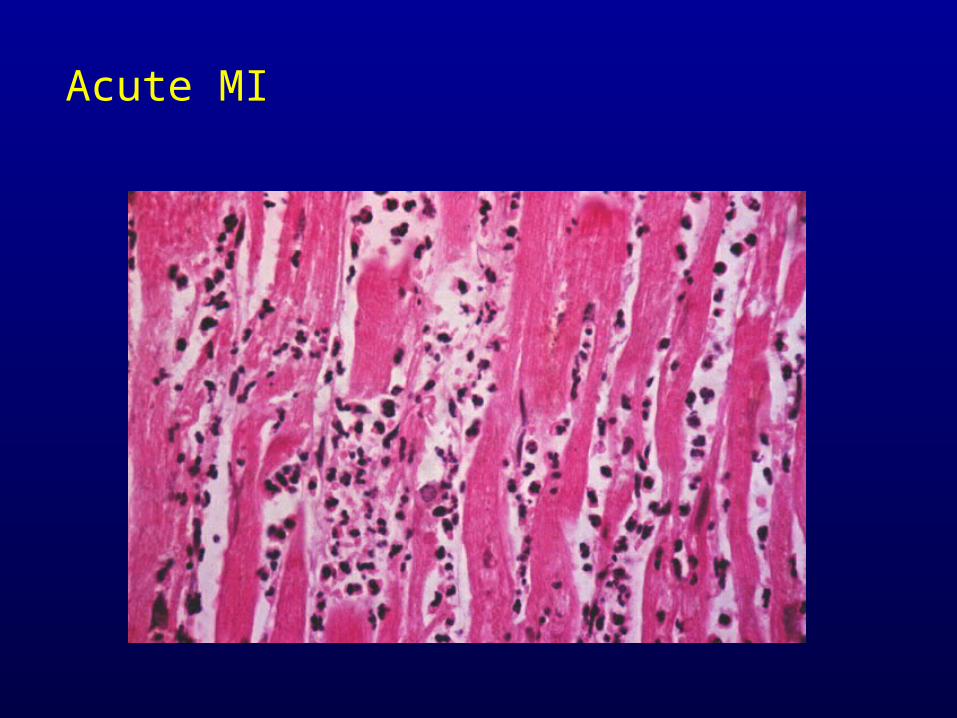
Acute MI
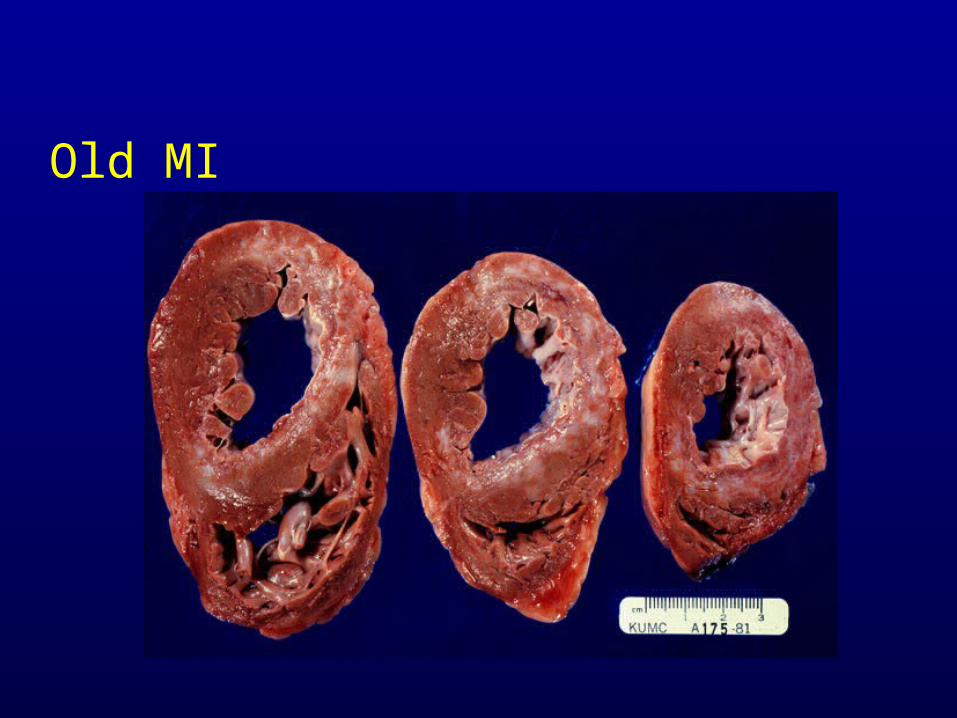
Old MI
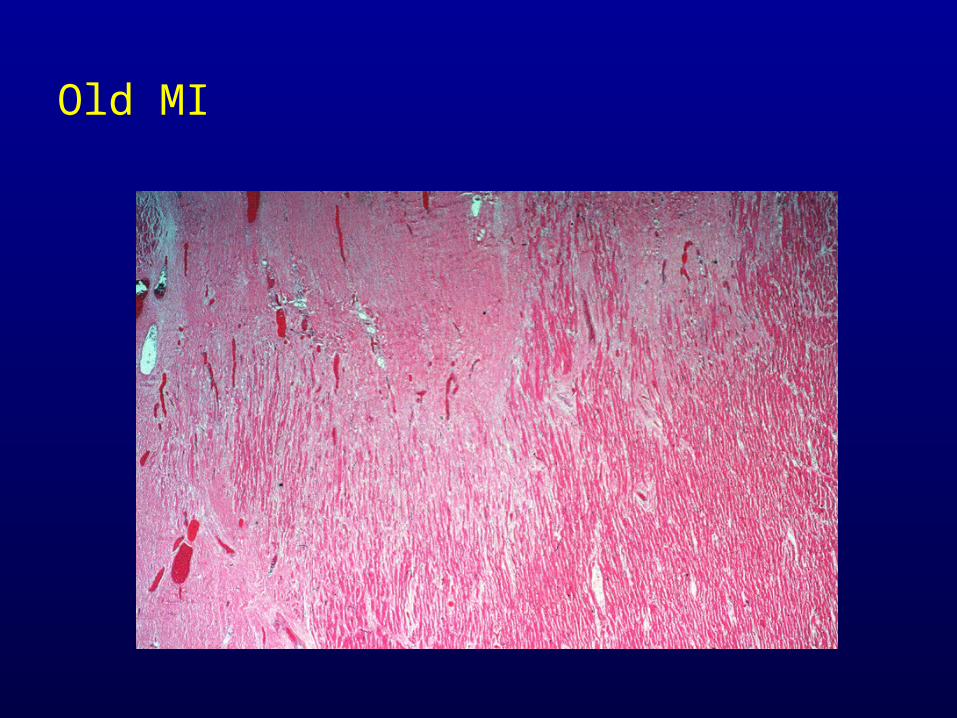
Old MI
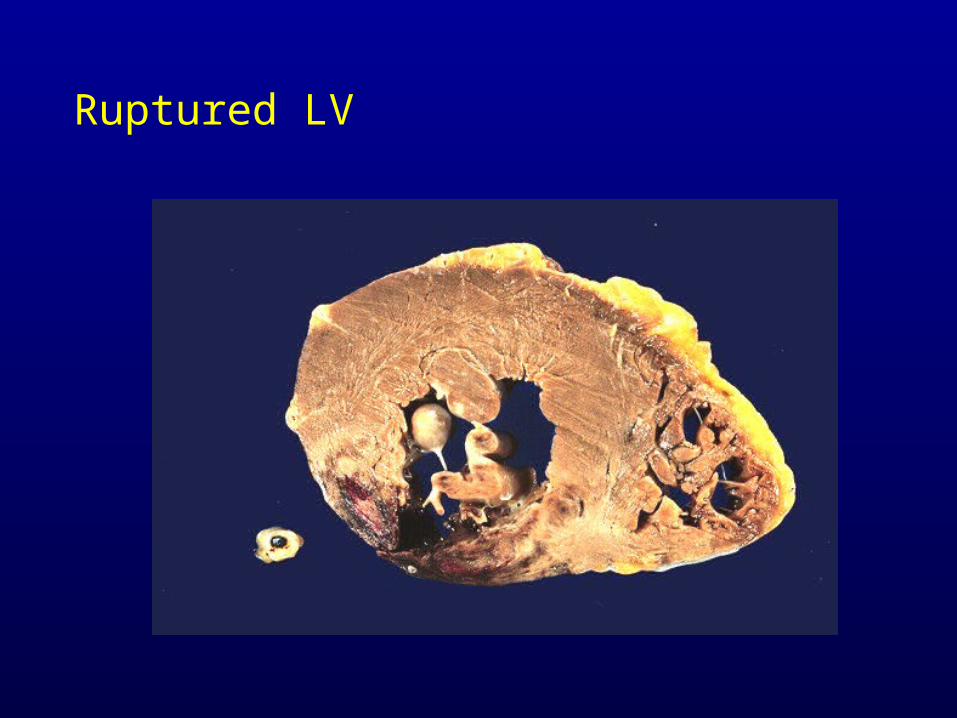
Ruptured LV
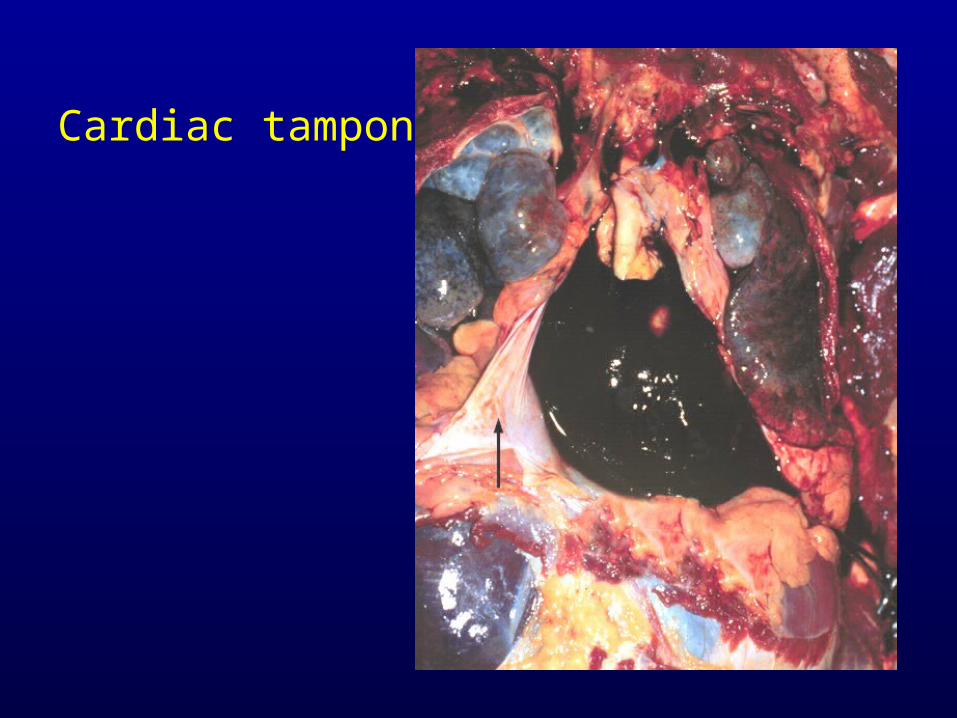
Cardiac tamponade
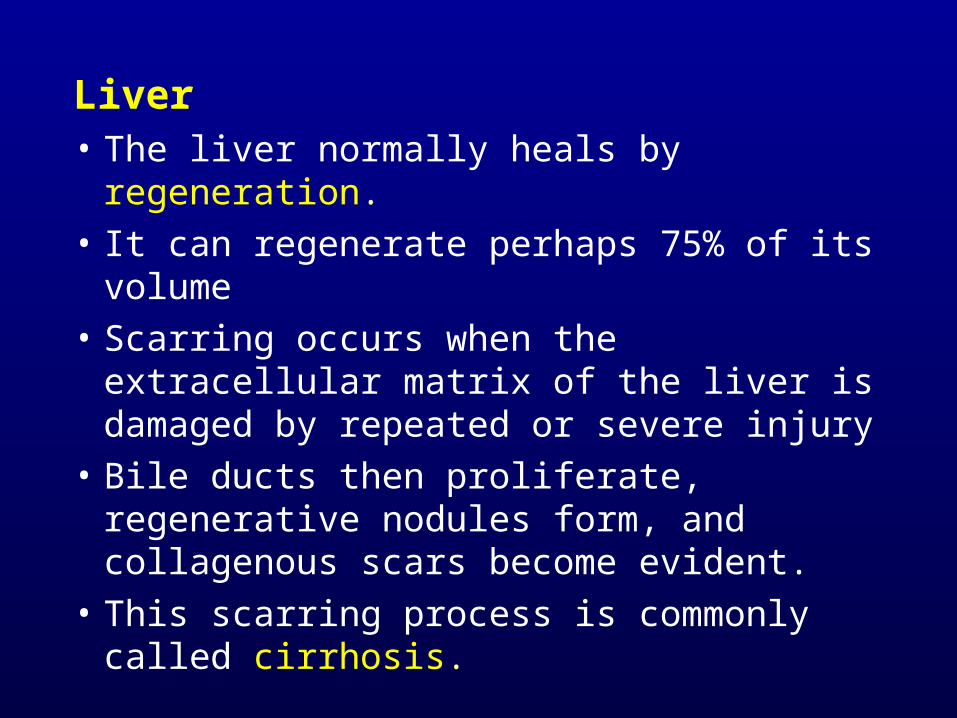
Liver• The liver normally heals by regeneration.
• It can regenerate perhaps 75% of its volume
• Scarring occurs when the extracellular matrix of the liver is damaged by repeated or severe injury
• Bile ducts then proliferate, regenerative nodules form, and collagenous scars become evident.
• This scarring process is commonly called cirrhosis.

Fatty Liver
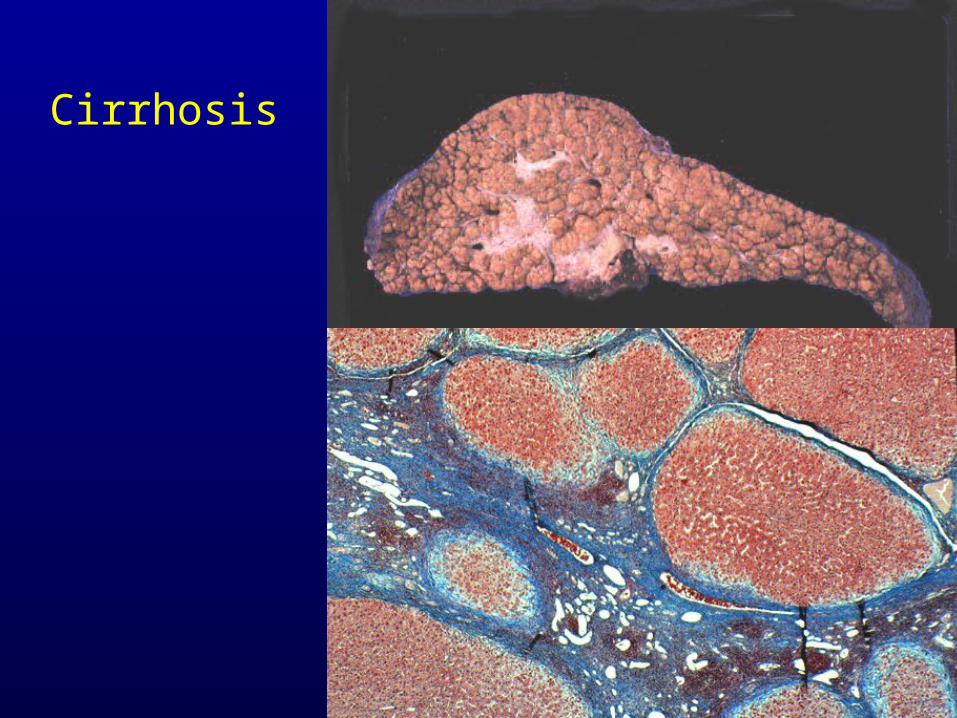
Cirrhosis
Brain • The brain heals by a process known as
gliosis. • Astrocytes proliferate and form what is
called a glial scar. • The only exception to this is in the process
of abscess formation, where fibroblasts from cerebral blood vessels form a collagenous scar.
• This scar may later serve as a focus for epileptic seizures.
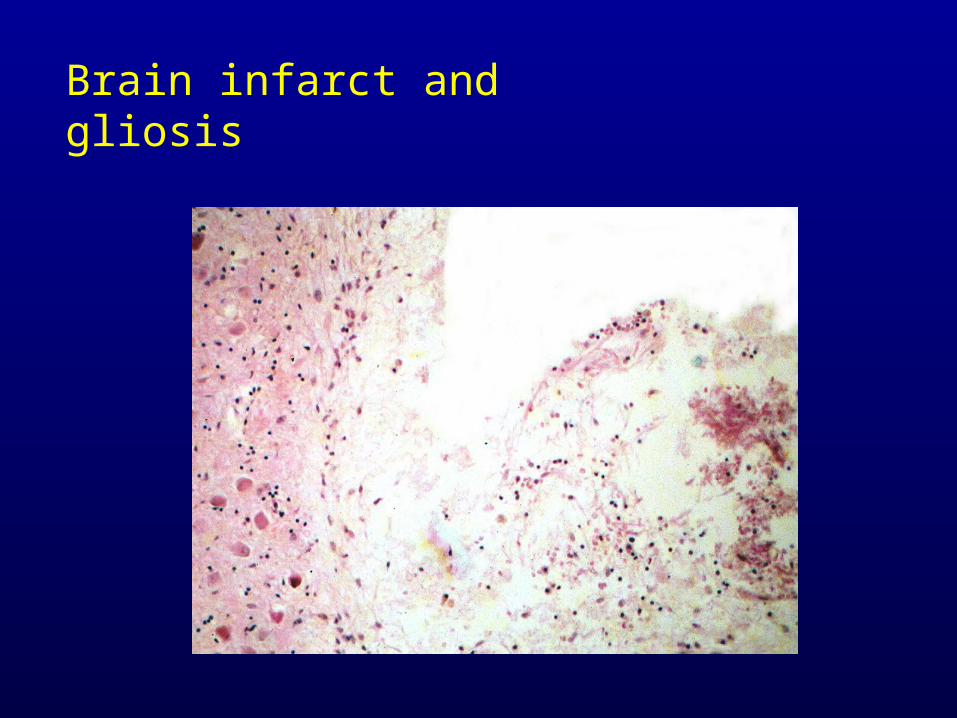
Brain infarct and gliosis
Healing of the Bone FractureHealing of the Bone Fracture
Inflammatory response
Time of injury to 24-72 hours • Injured tissues and platelets release vasoactive
mediators, growth factors and other cytokines. • These cytokines influence cell migration,
proliferation, differentiation and matrix synthesis. • Growth factors recruit fibroblasts, mesenchymal
cells & osteoprogenitor cells to the fracture site. • Macrophages, PMNs & mast cells (48hr) arrive at
the fracture site to begin the process of removing the tissue debris.
Reparative response 2 days to 2 weeks • Vasoactive substances (Nitric Oxide & Endothelial Stimulating
Angiogenesis Factor) cause neovascularisation & local vasodilation
• Undifferentiated mesenchymal cells migrate to the fracture site and have the ability to form cells which in turn form cartilage, bone or fibrous tissue (callus formation).
• The fracture hematoma is organised and fibroblasts and chondroblasts appear between the bone ends and cartilage is formed (Type II collagen).
• The amount of callus formed is inversely proportional to the amount of immobilisation of the fracture.
• In fractures that are fixed with rigid compression plates there can be primary bone healing with little or no visible callus formation.
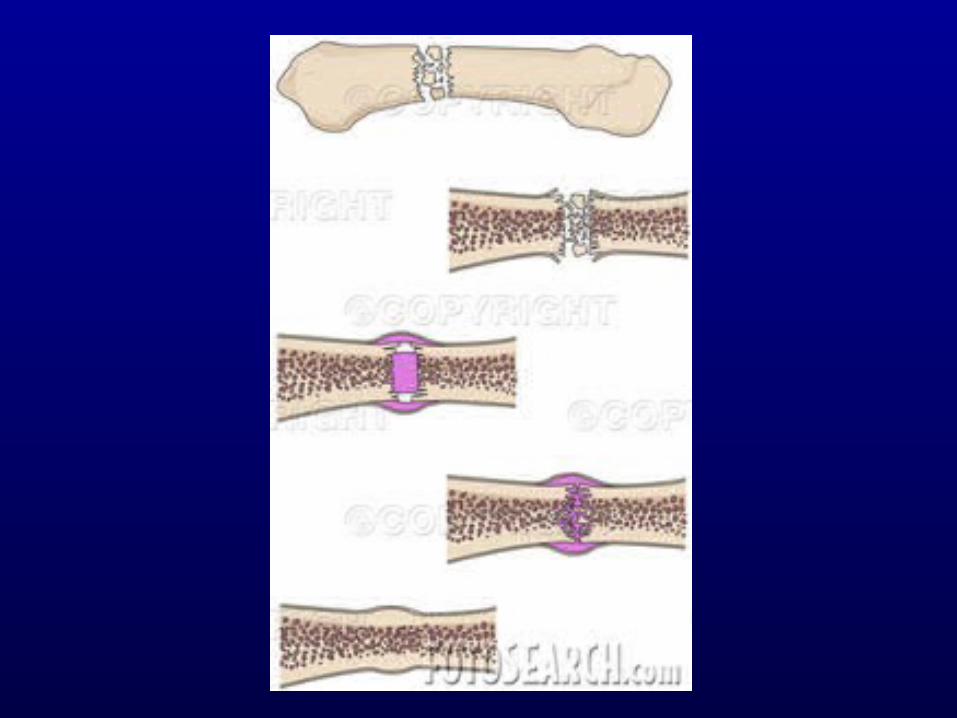
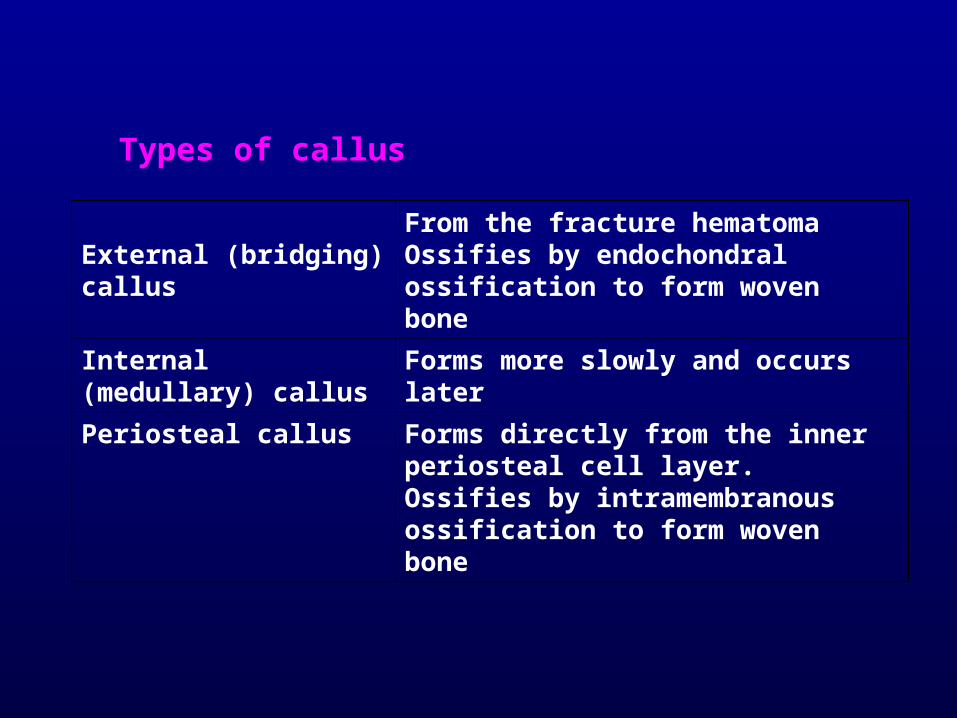
Types of callus
External (bridging) callus
From the fracture hematoma Ossifies by endochondral ossification to form woven bone
Internal (medullary) callus
Forms more slowly and occurs later
Periosteal callus Forms directly from the inner periosteal cell layer. Ossifies by intramembranous ossification to form woven bone
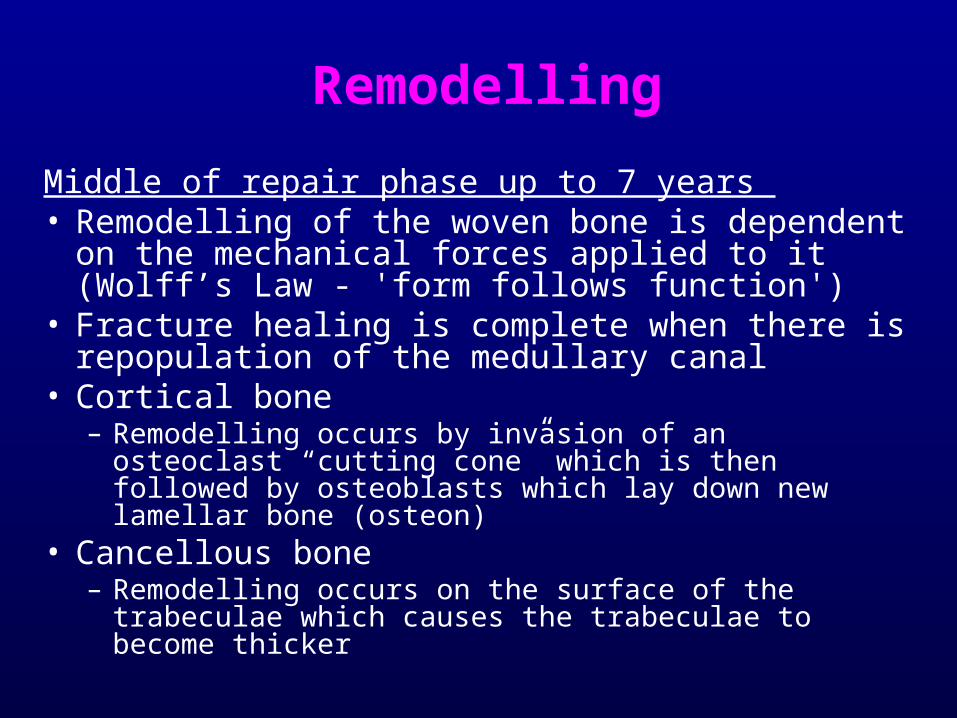
Remodelling
Middle of repair phase up to 7 years • Remodelling of the woven bone is dependent on the
mechanical forces applied to it (Wolff’s Law - 'form follows function')
• Fracture healing is complete when there is repopulation of the medullary canal
• Cortical bone – Remodelling occurs by invasion of an osteoclast “cutting
cone” which is then followed by osteoblasts which lay down new lamellar bone (osteon)
• Cancellous bone – Remodelling occurs on the surface of the trabeculae which
causes the trabeculae to become thicker
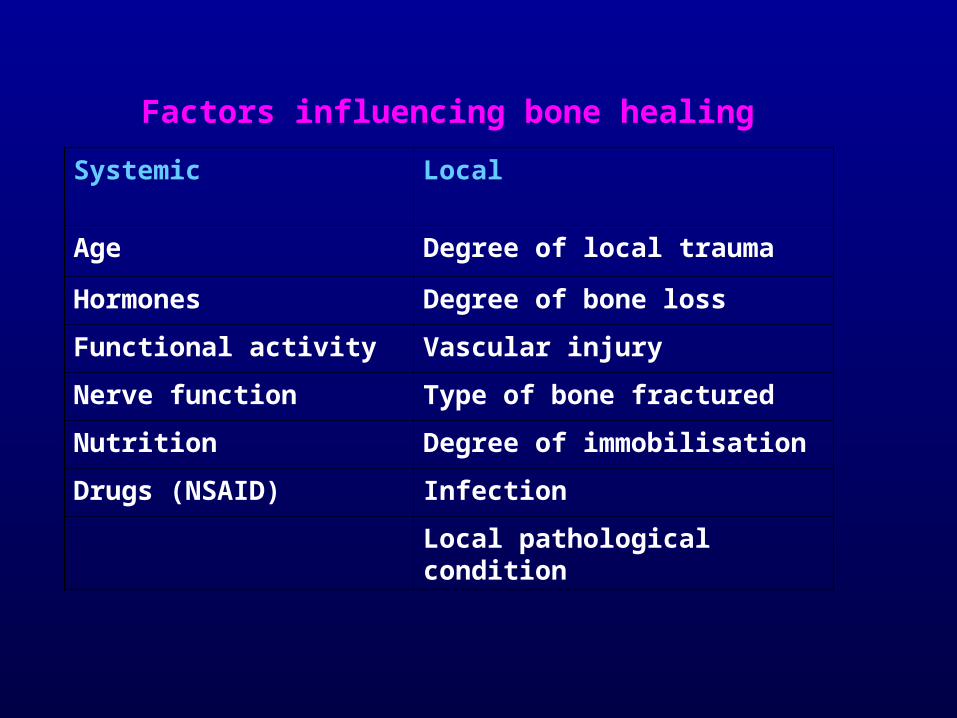
Factors influencing bone healing
Systemic Local
Age Degree of local trauma
Hormones Degree of bone loss
Functional activity Vascular injury
Nerve function Type of bone fractured
Nutrition Degree of immobilisation
Drugs (NSAID) Infection
Local pathological condition
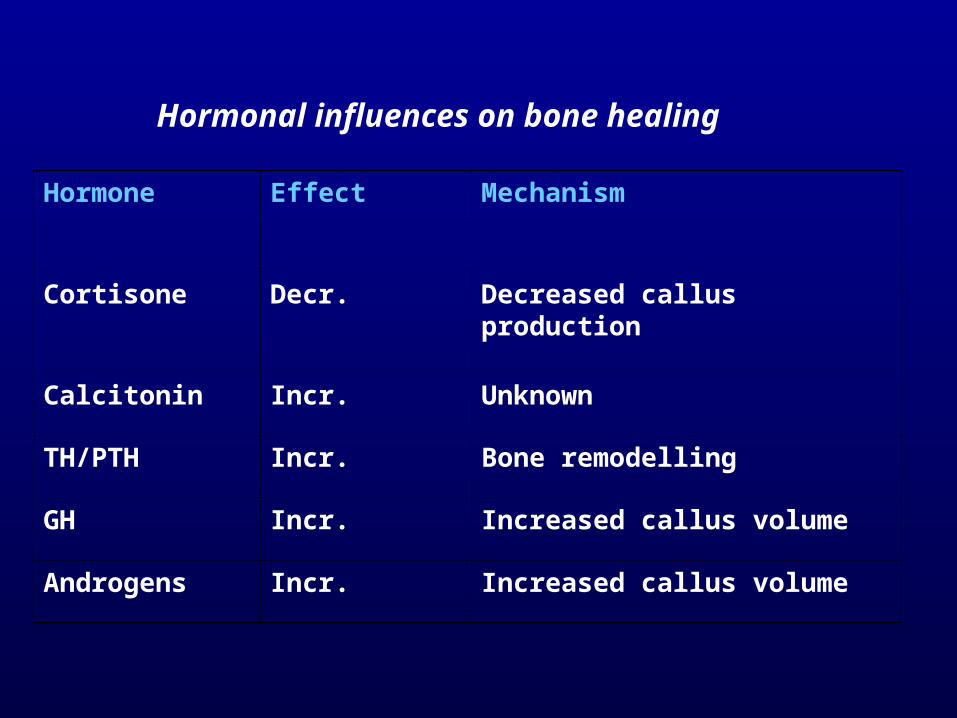
Hormonal influences on bone healing
Hormone Effect Mechanism
Cortisone Decr. Decreased callus production
Calcitonin Incr. Unknown
TH/PTH Incr. Bone remodelling
GH Incr. Increased callus volume
Androgens Incr. Increased callus volume
Problems That Can Occur During Fracture Healing
• Neurovascular injury: Some fractures are so severe that the arteries and nerves around the injury site are damaged.
• Infection: Open fractures can become infected when the jagged bone ends are exposed to the air where they have torn through the skin.
• Post-traumatic arthritis: Fractures that extend into the joints (intra-articular fractures) or fractures that cause the bones to meet at an abnormal angle in the joint can cause premature arthritis of a joint.
• Growth abnormalities: A fracture in the open epiphysis, or growth plate, in a child, can cause many problems. Two of these problems are premature partial or complete closure of the physis. If the whole bone, such as a thigh bone, stops growing prematurely, it will be shorter than the other thigh bone, making one leg shorter than the other.
• Delayed union: A fracture that takes longer to heal than expected is a delayed union.
• Nonunion: A fracture that fails to heal in a reasonable amount of time is called a nonunion.
• Malunion: A fracture that does not heal in a normal alignment is called a malunion.
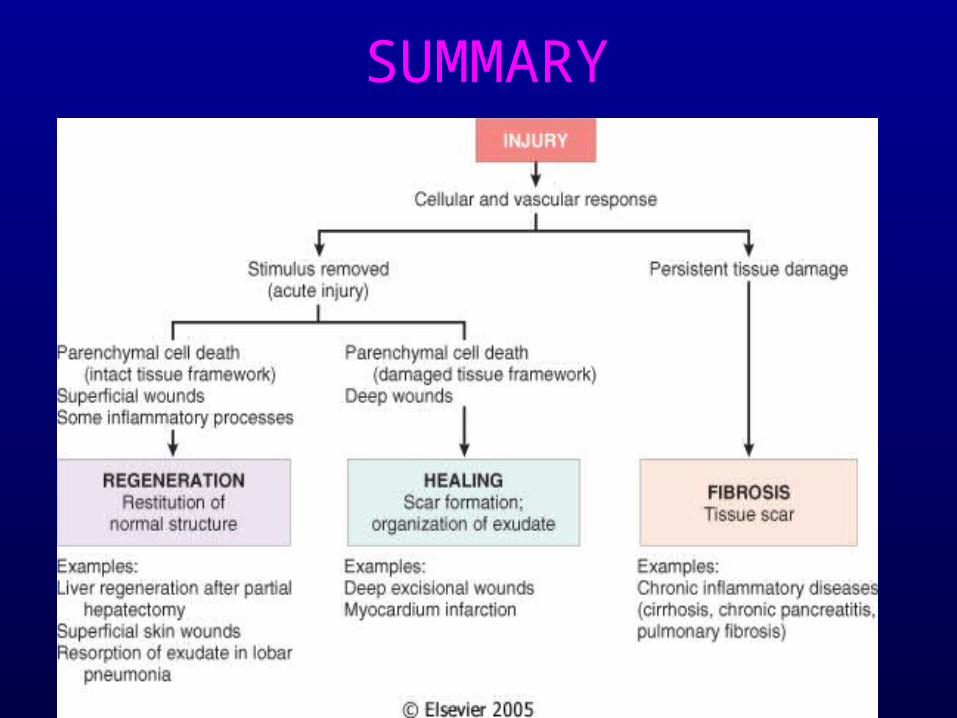
SUMMARY

THANK YOU