Embed Size (px)
Citation preview
478 BRITISH MEDICAL JOURNAL 1 JUNE 1974
induce vomiting, which could then cause acute dilatation fromhypokalaemia. Secondly, the hyperosmolar effect of introducinga relatively large amount of fluid and food into a stomach whichhas become used to less will cause dilatation.
Acute dilatation of the stomach is thus a recognized, if rare,complication of any patient suffering from anorexia nervosa whois beginning treatment. It seems that conservative managementalone is adequate in the acute phase provided the condition isdiscovered before perforation of the stomach occurs. Themortality of uncomplicated gastric dilatation is low, but afterperforation it is 80% (Evans, 1968).We considered whether any medication the patients received
before presentation might have caused the dilatation. Onepatient had been treated with diazepam and the other withchlorpromazine. We consulted Side Effects of Drugs (Meyler andHerxheimer, 1968) which made no reference to such effectsafter diazepam therapy. The phenothiazines have, however,
on rare occasions been noted to cause a depression of gastricsecretion leading to paralytic ileus in psychotic patients. Thiswas noted in four out of 720 people studied. Since only one ofour patients had received phenothiazines, however, we feel it isunlikely to have been a precipitating cause of presentation.
We thank Dr. N. C. Oswald and Mr. E. G. Tuckwell for per-mission to report these cases which were under their care andalso Mr. W. M. Castleden for his commnents and help.
ReferencesDragstedt, L. R., Montgomery, M. L., Ellis, J. C., and Matthews, W. R.
(1931). Surgery, Gynecology and Obstetrics, 52, 1075.Evans, D. S. (1968). British Journal of Surgery, 55, 940.Markowski, B. (1947). British Medical Journal, 2, 128.Meyler, L., and Herxheimer, A. (editors) (1968). Side Effects of Drugs, Vol. 6.
Amsterdam, Excerpta Medica.Russell, G. F. M. (1966). British_Journal of Psychiatry, 112, 203.
Titanium CranioplastyD. S. GORDON, G. A. S. BLAIR
British Medical Journal, 1974, 2, 478-481
Summary
The technique of repairing defects of the skull with titaniumis described. The skull contour can be accurately reproduced.The technique is simpler than wiring or suturing methods.The material is inert, radiolucent, and rigid.
Introduction
One of the most conspicuous after effects of a depressed frac-ture of the skull or a penetrating missile injury is a disfiguringskull defect. Repair by cranioplasty is often needed. Frontaldefects more than 2 cm in diameter are usually unsightly, andsome cause discomfort, especially when ithe patient stoops.Larger defects leave the brain vulnerable to trauma, givingthe patient a sense of insecuri;ty.A satisfactory cranioplasty should employ an onlay tech-
nique wvith a simple method of attaching the prosthesis to theskull. The material used should be inert in the tissues, radio-lucent, easily and accurately shaped, capable of being adjustedat the itime of insertion, and it should have sufficient mechani-cal strength to resist fracture or deformation under severeimpact loading.
After the 1914-18 war autogenous bone was the material ofchoice for cranioplasty. But repair of a large defect requires amajor operation to obtain the graft. Reproduction of thecorrect skull contour often proves difficult, and the patientoften has more postoperative pain from (the donor site thanfrom t.he grafted area.Some of the skull defects from the 1939-45 war were re-
paired with autopolymerized acrylic resin plates. At first theywere preformed from a template or impression made at thefirst operation. Spence (1954) descrilbed form-fining plastic
Department of Neurosurgery, Royal Victoria Hospital, Belfast BT126BA
D. S. GORDON, M.CH., F.R.C.S., Consultant
Department of Dental Prosthetics, Dental School, Belfast BT12 6BAG. A. S. BLAIR, M.D.S., F.F.D., Senior Lecturer and Consultant
cranioplasty in which the plastic was moulded into the defectduring the hardening process. When the defeot is large, how-ever, a smoothly contoured plate is difficul-t to shape and fitaccurately.Metals and alloys, including tantalum, titanium, stainless
steel, and chrome-cobalt are not widely used because of thedifficulty in forming the plate to the compound complex cur-vatures of the skull. Tantalum was used after -the 1939-45 war(Woodhall and Spurling, 1947). It was shaped by a die/counter die swaging technique or by hanmnering into a counterdie (Lewin et al., 1948). Lewin and Gibson (1956) used tan-talum to repair some of -the skull defeots in British soldiers in-jured in Korea. The higher thermal conductivity of metals ascompared with acrylic resin may limit their use for largeplates in very hot climates (Spence, 1954.) For treating smallskull defects plastic or metal plates or bone-grafting willusually prove satisfactory. The larger defect, however, posesspecial problems of contour and fixation which are difficult tosolve by any of the available techniques.
In the civil disturbances in Northem Ireland over 900people died between 1969 and 1973. In this type of urbanguerilla warfare over 95% of penetrating injuries are gunshotwounds, many of them caused by high velocity bullets. Thesurvivors usually have large skull defects, some with an areagreater than 20 in2 (129 cm2).We describe here how titanium has been used to repair
these defeats. The method combines accuracy with ease ofinsertion and is now used for skull defects of any size.
Methods
INITIAL OPERATION
Beause of the risk of infection immediate cranioplasty is sel-dom advisable in patients with compound depressed skullfractures with brain laceration. The overlying skin is oftenseverely lacerated and many wounds are heavily contamin-ated. Certain steps taken at the initial operation, however, willfacilitate subsequent cranioplasty. A full-thickness skin coverfor the defeat and later for the prosthesis is essential. Inmissile wounds and depressed fractures caused by sharp objectsthe scalp laceration is often small and can be excised andstured. A generous scalp flap is then cut about 2-3 cm be-yond the limits of the skull fracture. This flap can be reflected
8RITISH MEDICAL JOURNAL 1 JUNE 1974
again for the cranioplasty procedure. For frontal wounds acoronal flap may be preferable. When the scalp laceration ismore extensive retraction of the wound edges gives sufficientexposure. Patients who have lost an area of scalp usually needskin advancement or a rotation scalp flap.Apart from neurological damage the chief complication of a
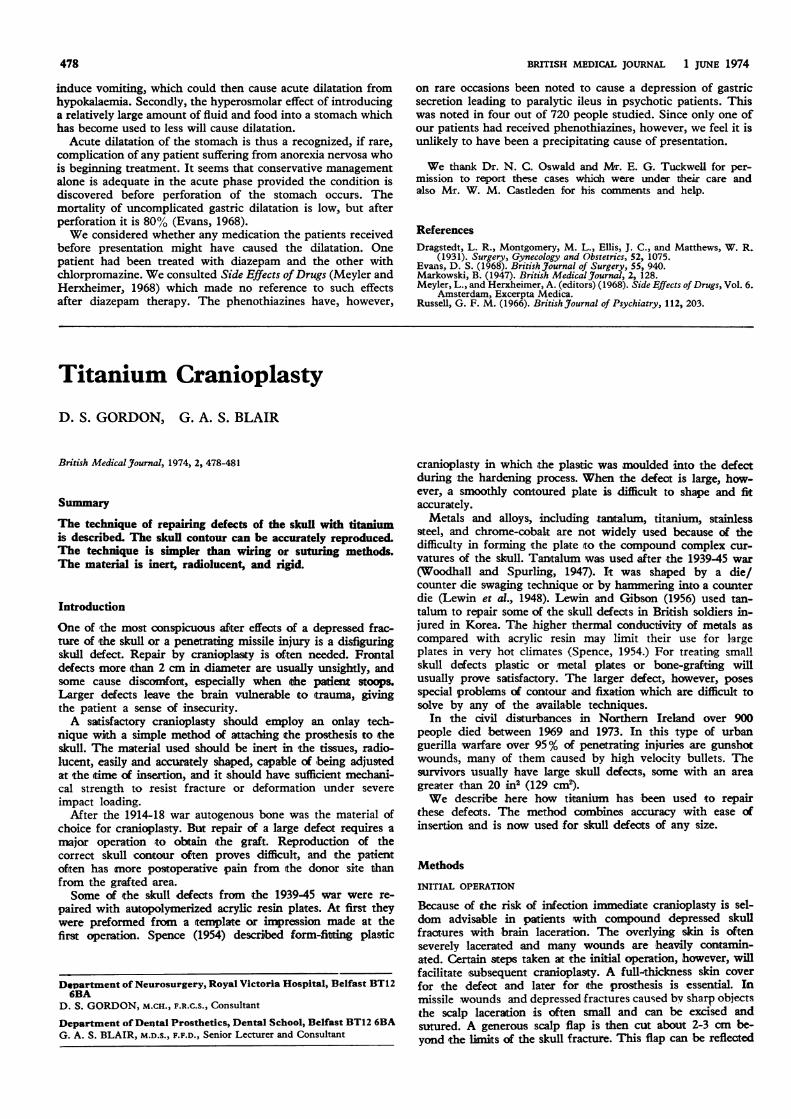
compound cranial wound is infeotion, leading to meningitis orbrain abscess (Jefferson, 1919). Initial surgery is thereforedirected towards the removal of foreign material and bonefragments. Intact skull is removed by rongeurs until normaldura mater is exposed around the brain wound; the resultingdefect becomes considerably larger than seen on the initialx-ray pictures (figs. 1 and 2).
FIG. 1-Tangential high velocity buUet wound in parietal bone producing"gutter" fracture and widespread shattering of surrounding skull. Pressure-recording transducer has been inserted between skull and dura mater.
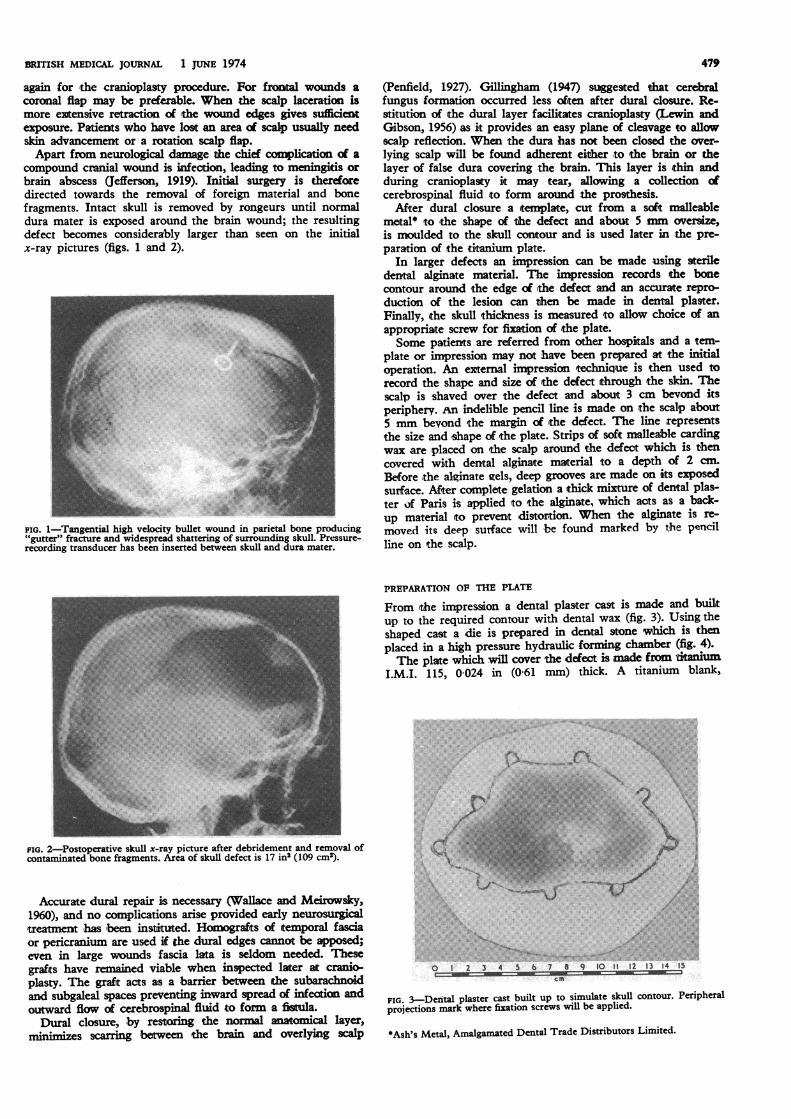
FIG. 2-Postoperative skull x-ray picture after debridement and removal ofcontaminated bone fragments. Area of skull defect is 17 ins (109 cm2).
Accurate dural repair is necessary (Wallace and Meirowsky,1960), and no complications arise provided early neurosurgical-treatment has ibeen instiuted. Homografts of temporal fasciaor pericranium are used if the dural edges cannot be apposed;even in large wounds fascia lata is seldom needed. Thesegrafts have rmained viable when inspected later at cranio-plasty. The graft acts as a barrier between the subarachnoidand subgaleal spaces preventing irnward spread of infection andoutward flow of cerebrospinal fluid to form a fistula.Dural closure, by restoring the normal atcal layer,
minimizes scarring between the brain and overlying scalp
479
(Penfield, 1927). Gillingham (1947) suggested that cerebralfungus formation occurred less ofiten after dural closure. Re-stitution of the dural layer facili,tates cranioplasty (Lewin andGibson, 1956) as it provides an easy plane of cleavage to allowscalp reflection. When the dura has not been closed the over-lying scalp will be found adherent either to the brain or thelayer of false dura covering the brain. This layer is thin andduring cranioplasty it may tear, allowing a collection ofcerebrospinal fluid to form around the prosthesis.
After dural closure a template, cut from a soft malleablemetal* to 'the shape of the defect and about 5 nmn oversize,is moulded to the skull contour and is used later in the pre-paration of the ititanium plate.
In larger defects an impression can be made using steriledental alginate material. The impression records the bonecontour around the edge of ¢the defect and an accurate repro-duction of the lesion can -then be made in dental plaster.Finally, the skull tthickness is measured to allow choice of anappropriate screw for fixation of the plate.Some patients are referred from other hospitals and a tem-
plate or impression may not have been prepared at the initialoperation. An external impression technique is then used torecord the shape and size of the defect through the skin. Thescalp is shaved over the defect and about 3 cm bevond i;tsperiphery. An indelible pencil line is made on the scalp about5 mm bevond the margin of the defect. The line representsthe size and shape of the plate. Strips of softnmalleable cardingwax are placed on the scalp around the defect which is thencovered wi,th dental alginate material to a depth of 2 cm.
BIefore the alginate eels, deep grooves are made on its exposedsurface. After complete gelation a thick mixture of dental plas-ter of Paris is applied to the alginate, which acts as a back-up material to prevent distortion. When the alginate is re-
moved its deep surface will be found marked by the pencilline on the scalp.
PREPARATION OF THE PLATE
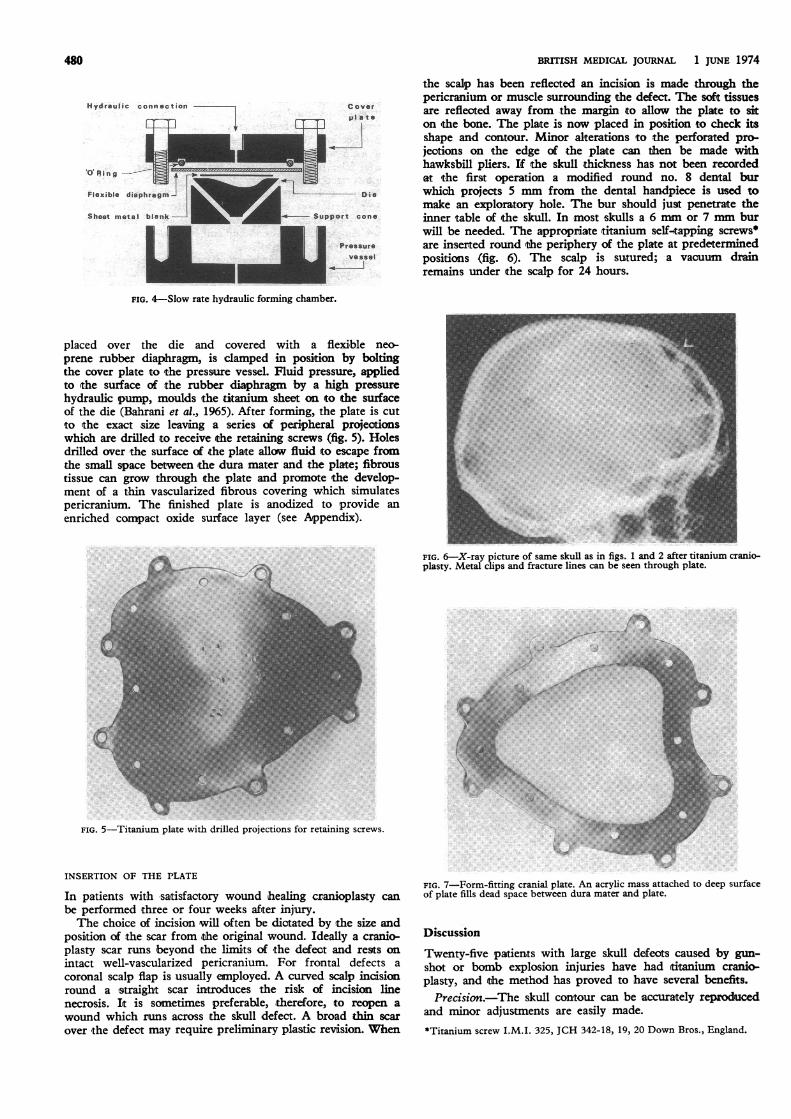
From the impression a dental plaster cast is made and builtup to the required contour with dental wax (fig. 3). Using theshaped cast a die is prepared in dental one which is thenplaced in a high pressure hydraulic forming chamber (fig. 4).The plate which will cover the defect is made from titium
I.M.I. 115, 0 024 in (0-61 mm) thick. A titanium blank,
v I A i .* a1-co
FIG. 3Derial plaster cast built up to simulate skull contour. Peripheralprojections mark where fixation screws will be applied.
*Ash's Metal, Amalgamated Dental Trade Distributors Limited.
480
Hydraulic connection Coverpl ate
Flexible diaphragm Die
Sheet metal blaenk Support cone
Pressurev ssel
I-
BRITISH MEDICAL JOURNAL 1 JUNE 1974
the scalp has been reflected an incision is made through thepericranium or muscle surrounding -the defect. The soft tissuesare reflected away from the margin to allow the plate to siton 'the bone. The plate is now placed in posi-tion to check itsshape and contour. Minor alterations to the perforated pro-jeotions on the edge of -the plate can then be made withhawksbill pliers. If the skull thickness has not been recordedat the first operation a modified round no. 8 dental burwhich projects 5 mm from the dental handpiece is used tomake an exploratory hole. The bur should just penetrate theinner table of the skull. In most skulls a 6 mm or 7 mm burwill be needed. The appropriate titanium self-tapping screwsare inserted round the periphery of the plate at predeterminedpositions (fig. 6). The scalp is sutured; a vacuum drainremains under the scalp for 24 hours.
FIG. 4-Slow rate hydraulic forming chamber.
placed over the die and covered with a flexible neo-prene rubber diaphragm, is clamped in position by boltingthe cover plate rto the pressure vessel. Fluid pressure, appliedto ithe surface of the rubber diaphragm by a high pressurehydraulic pump, moulds the titanium sheet on to the surfaceof the die (Bahrani et al., 1965). After forming, the plate is cutto the exact size leaving a series of peripheral projectionswhich are drilled to receive the retaining screws (fig. 5). Holesdrilled over the surface of the pla-te allow fluild to escape fromthe small space between the dura mater and the plate; fibroustissue can grow through ithe plate and promote the develop-ment of a thin vascularized fibrous covering which simulatespericranium. The finished plate is anodized to provide anenriched compact oxide surface layer (see Appendix).
FIG. 6-X-ray picture of same skull as in figs. 1 and 2 after titanium cranio-plasty. Metal clips and fracture lines can be seen through plate.
FIG. 5-Titanium plate with drilled projections for retaining screws.
INSERTION OF THE PLATE
In patients with satisfactory wound healing cranioplas,ty canbe performed three or four weeks after injury.The choice of incision will often be dictated by the size and
position of the scar from the original wound. Ideally a cranio-plasty scar runs 'beyond -the limits of the defect and rests onintact well-vascularized pericranium. For frontal defects acoronal scalp flap is usually employed. A curved scalp incisionround a !straight scar introduces the risk of incision linenecrosis. Ift is sometimes preferable, therefore, to reopen awound which runs across ithe skull defect. A broad thin scarover the defect may require preliminary plastic revision. When
FIG. 7-Form-fitting cranial plate. An acrylic mass attached to deep surfaceof plate fills dead space between dura mater and plate.
Discussion
Twenty-five patients with large skull defects caused by gun-shot or bomb explosion injuries have had titanium cranio-plasty, and the method has proved to have several benefits.Precision.-The skull contour can be accurately reproduced
and minor adjustments are easily made.
*Titanium screw I.M.I. 325, JCH 342-18, 19, 20 Down Bros., England.

BRITISH MEDICAL JOURNAL 1 JUNE 1974 481
Ease of Fixation.-Drilling the skull and inserting screws istechnically simple and much easier than wiring or suturingmethods, which involve dissection of the bone edge and theextradural space. The use of an onlay technique considerablyreduces the operating time.Good Tissue Acceptance.-Anodized titanium is an inert
implant material. There is no reactive oedema of the scalp andno postoperative subgaleal effusion.Dead Space.-Previous metal onlay techniques did not in-
clude provision for obliterating the dead space between theplate and the dura. When there is a large space a heat-curedacrylic resin mass can be processed to the tissue fitting sur-face of the plate (fig. 7).Radiolucency.-An objection to most metallic plates is that
they are radio-opaque. Titanium, however, is sufficiently radio-lucent to allow radiological studies (see fig. 6).Strength.-When titanium sheet is shaped to a formed con-
tour it becomes rigid and will withstand considerable externalforce. As -the plate is 05-1 cm "oversize," only an exceptionalforce would displace it inwards.Lightness.-The density of titanium is low compared with
that of other metals and alloys.
Sterilization.-Titanium plates and screws can be auto-claved. As most plastic materials need protection to preventdeformation due to stress relief on heating their sterilitycannot be guaranteed.
Appendix
The anodizing solution is made up of 80% phosphoric acid, 10%suphuric acid, and 10% water. The anode is titanium, voltagecomes from a single phase rectified supply 0-120 V, and thecurrent is about 10 A/ft2.
References
Bahrani, A. S., Blair, G. A. S., and Crossland, B. (1965). British Dental3Jour-nal, 118, 425.
Gillingham, F. J. (1947). British J3ournal of Surgery, War Surgery Supple-ment no. 1, p. 80.
Jefferson, G. (1919). British Journal of Surgery, 7, 262.Lewin, W., and Gibson, R. M. (1956). British Journal of Surgery, 43, 628.Lewin, W., Graham, M. P., and Northcroft, G. B. (1948). British
Journal of Surgery, 36, 26.Penfield, W. (1927). Brain, 50, 409.Spence, W. T. (1954). Jfournal of Neurosurgery, 11, 219.Wallace, P. B., and Meirowsky, A. M. (1960). Annals of Surgery, 151, 174.Woodhall, B., and Spurling, R. G. (1945). Annals of Surgery, 121, 649.
MEDICAL MEMORANDA
Hepatorenal Failure with Self-initiated Intermittent RifampicinTherapy
D. L. ROTHWELL, D. E. RICHMOND
British Medical Journal, 1974, 2, 481-482
Continuous rifampicin therapy is considered to be relativelynon-toxic. Nevertheless, complications associated with itsintermittent administration have been reported (Campese et al.,1973; Kleinknecht, 1972; Poole et al., 1971; Girling et al.,1971; Aquinas et al., 1972). The symptoms include pyrexia,chills, arthralgia, jaundice, and acute renal failure. We reporta case of combined hepatorenal failure in a patient who tookrifampicin from time to time of her own accord.
Case Report
A 62-year-old European woman was admitted to hospital in Septem-ber 1973 complaining of acute abdominal pain, nausea, vomiting,and chills. She was confused, but her history was later confirmed byher husband.
In April 1972 she was diagnosed as having active pulmonarytuberculosis. Three cachets of sodium aminosalicylate twice a dayand rifampicin 450 mg daily were prescribed. She took these regu-larly until August 1973 when she developed severe heartburn andstopped both. Six days later she took three tablets of rifampicin.After two hours she developed chills, nausea, and vomiting, whichresolved after 24 hours but left her lethargic for two weeks, duringwhich she took no rifampicin. A fortnight after her first intermittentdose she took three tablets of rifampicin and some hours later she
Department of Medicine, Auckland Hospital, New ZealandD. L. ROTHWELL, M.B., CH.B., RegistrarD. E. RICHMOND, M.B., M.R.C.P., Senior Lecturer
developed nausea amd malaise. Three days later she again took threetablets of rifampicin. This was rapidly followed by acute pain in theright loin, nausea, and vomiting. She had had severe dermatitis 39years previously after a course of sulpha drugs. There was no pre-existing renal or liver disease.On admission she was jaundiced and had a temperature of 38°C.
No obvious abnormality was detected in the cardiovascular or res-piratory system; the blood pressure was 140/80 mg Hg. She wasalmost anuric and was confused. Blood values were: bilirubin 4.3mg/100 ml; Prothrombin time 60%; alkaline phosphatase 165 IU;SGOT 1,450 IU/ml; urea 106 mg/100 ml; creatinine 2.2 mg/100 ml;Hb 12.3 g/100 ml; E.S.R. 15 mm in 1 hour (Westergren). Reticu-locyte counts were 1.4%, 1.5%, and 1.3% during the two weeks afteradmission. Urine microscopy showed white cells 13/high-powerfield, red blood cells 15/high-power field, no casts, and no protein.Nothing abnormal was seen on chest x-ray examination. Anti-streptolysin-O antistreptokinase, antihyaluronidase titres, and serumcomplement were all normal. Tests for L.E. cells and antinuclearfactor gave negative results. These findings indicated hepatocellulardamage and early acute renal failure with an absence cf haemolysis.Liver function returned to normal after five days but the patientremained anuric and became progressively uraemic. The pain dis-appeared rapidly and its cause was never explained. Peritoneal dia-lysis was performed on the seventh day. Renal biopsy was not per-formed because glomerulonephritis seemed an unlikely diagnosisand she was'treated as a case of acute tubular necrosis. Three dayslater she began a brisk diuresis and her renal function soon returnedto normal.
Comment
Side effects of intermittent rifampicin therapy are well re-cognized (Aquinas et al., 1972). One of the more well-definedsyndromes is an influenza-like illness with pain and shocksimilar to that described by the patient. It is not widely knownthat intermittent rifampicin therapy can cause acute renal andhepatic failure, though workers in Scandinavia and Hong Konghave described transient minor abnormalities of liver functionnear the start of treatment (Aquinas et al., 1972). The fewreported cases of acute renal failure have occurred when anintermittent high dose of rifampicin has been deliberatelyprescribed. Acute tubular necrosis has been found on renalbiopsy in two such patients (Aquinas et al., 1972; Campese,





























