Embed Size (px)
DESCRIPTION
TOP 12 ISSUES WEBINAR SERIES Health: Medicaid and Health Reform
Citation preview
TOP 12 ISSUES WEBINAR SERIES Health: Medicaid and Health Reform
Health
Today’s webinar will cover:
Medicaid
Health Reform
– Health Insurance Exchanges
– Essential Health Benefits
– Opposition Actions

Martha King
NCSL Health Program Group Director
Melissa Hansen
NCSL Senior Policy Specialist
Presenters
Martha Salazar
NCSL Policy Associate
Dick Cauchi
NCSL Health Program Director
Medicaid
Medicaid overview
Why Medicaid is a top issue for
states in 2012
4 things for states to consider as
they address Medicaid issues
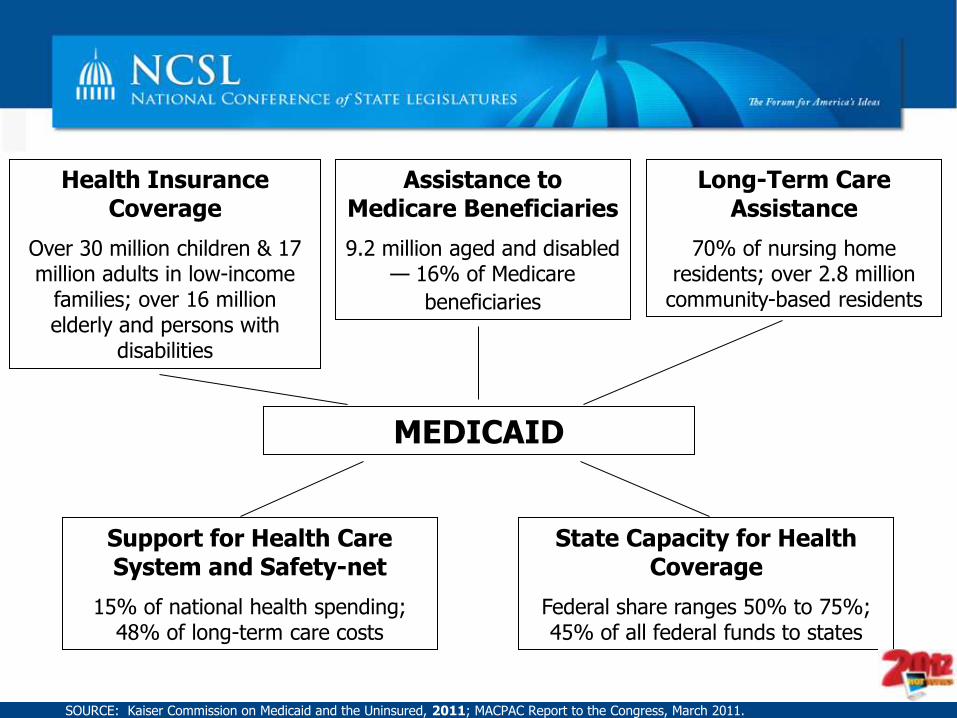
Health Insurance Coverage
Over 30 million children & 17 million adults in low-income
families; over 16 million elderly and persons with
disabilities
State Capacity for Health Coverage
Federal share ranges 50% to 75%; 45% of all federal funds to states
MEDICAID
Support for Health Care System and Safety-net
15% of national health spending; 48% of long-term care costs
Assistance to Medicare Beneficiaries
9.2 million aged and disabled — 16% of Medicare
beneficiaries
Long-Term Care Assistance
70% of nursing home residents; over 2.8 million
community-based residents
SOURCE: Kaiser Commission on Medicaid and the Uninsured, 2011; MACPAC Report to the Congress, March 2011.
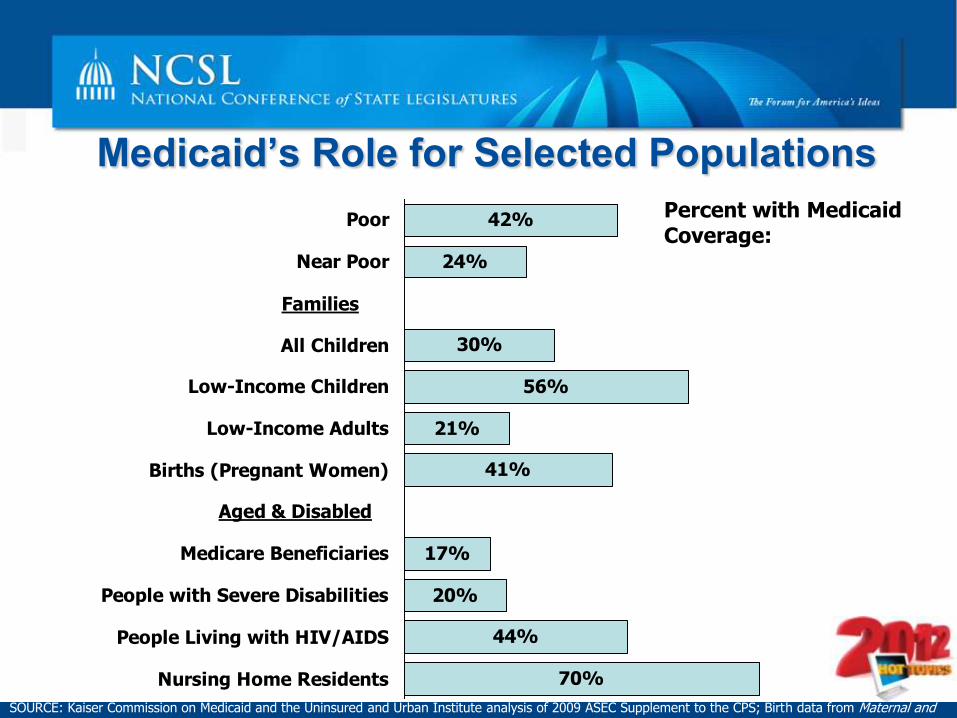
Medicaid’s Role for Selected Populations
SOURCE: Kaiser Commission on Medicaid and the Uninsured and Urban Institute analysis of 2009 ASEC Supplement to the CPS; Birth data from Maternal and Child Health Update: States Increase Eligibility for Children's Health in 2007, National Governors Association, 2008; Medicare data from USDHHS.
70%
44%
21%
56%
17%
20%
30%
42%
41%
24%
Nursing Home Residents
People Living with HIV/AIDS
People with Severe Disabilities
Medicare Beneficiaries
Births (Pregnant Women)
Low-Income Adults
Low-Income Children
All Children
Near Poor
Poor Percent with Medicaid Coverage:
Families
Aged & Disabled
Why Medicaid is a top
issue for states in 2012
Fiscal situation in states
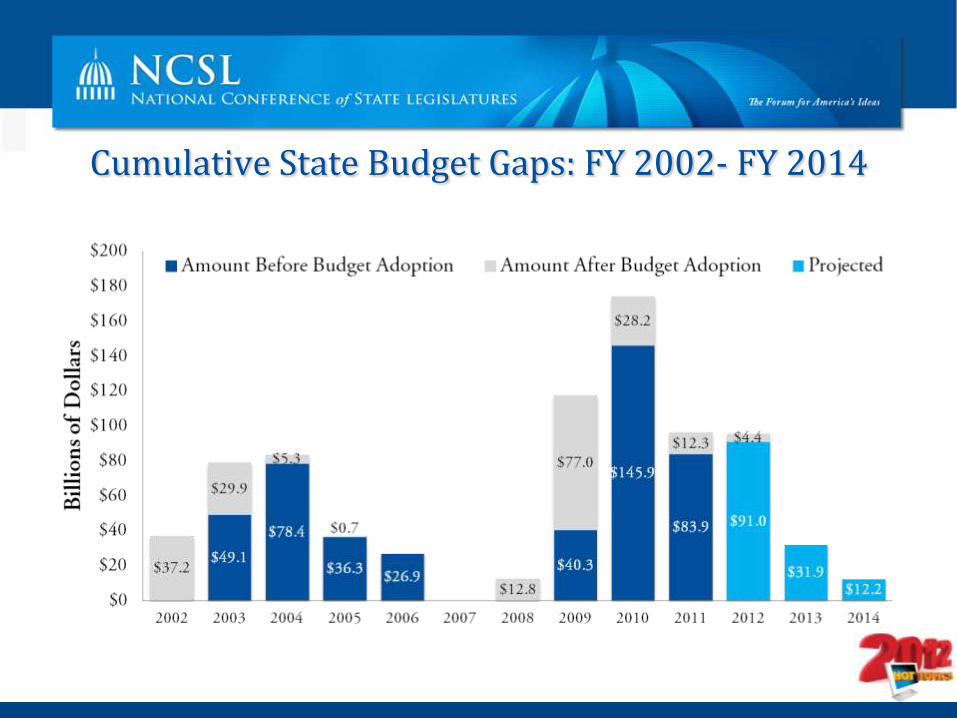
Cumulative State Budget Gaps: FY 2002- FY 2014
Source: NCSL survey of state legislative fiscal offices, various years.
Why Medicaid is a top
issue for states in 2012
Fiscal situation in states
Enrollment increase associated with the Great
Recession
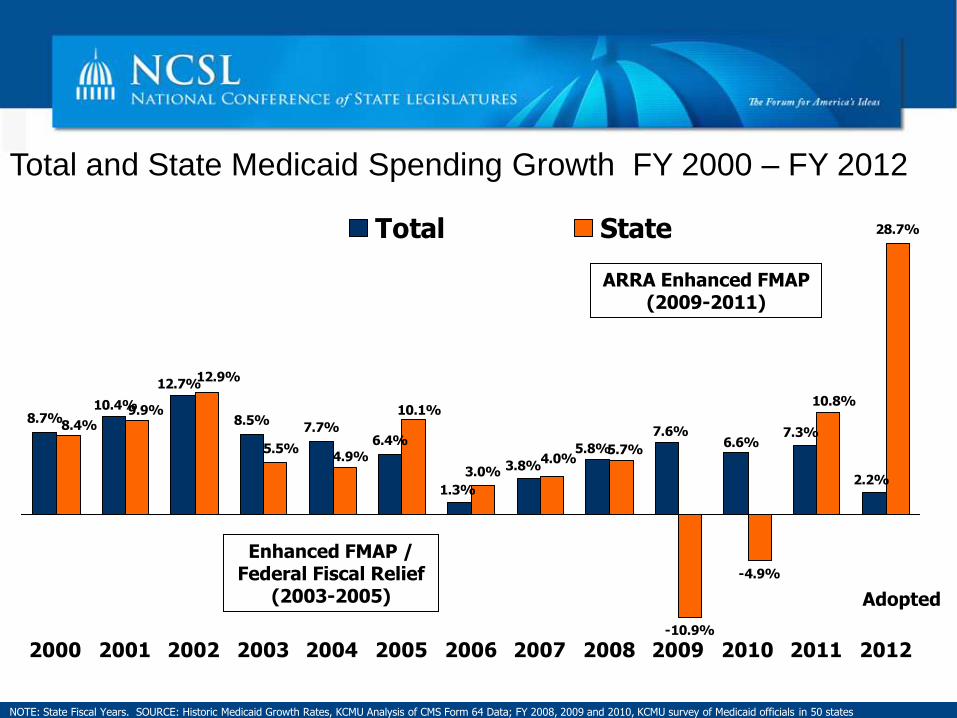
Total and State Medicaid Spending Growth FY 2000 – FY 2012
8.7% 8.5%7.7%
6.4%
3.0%
-10.9%
-4.9%
28.7%
6.6%7.6%
10.4%
12.7%
1.3%
3.8%
5.8%
7.3%
2.2%
10.8%10.1%
8.4%9.9%
12.9%
5.5%4.9% 4.0%
5.7%
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012
Total State
Enhanced FMAP / Federal Fiscal Relief
(2003-2005)
NOTE: State Fiscal Years. SOURCE: Historic Medicaid Growth Rates, KCMU Analysis of CMS Form 64 Data; FY 2008, 2009 and 2010, KCMU survey of Medicaid officials in 50 states and DC conducted by Health Management Associates, 2011 .
ARRA Enhanced FMAP (2009-2011)
Adopted

Why Medicaid is a top
issue for states in 2012
Fiscal situation in states
Enrollment increase associated with the Great
Recession
Affordable Care Act expansion in 2014
Affordable Care Act expansion in 2014
2014 expansion will qualify all Americans
under age 65 with family incomes at or below
133 percent of federal poverty guidelines.
– This includes childless adults
New eligibility calculation called “modified
adjusted gross income,” (MAGI) will effectively
raise the eligibility level to 138 percent of the
poverty level for most applicants.
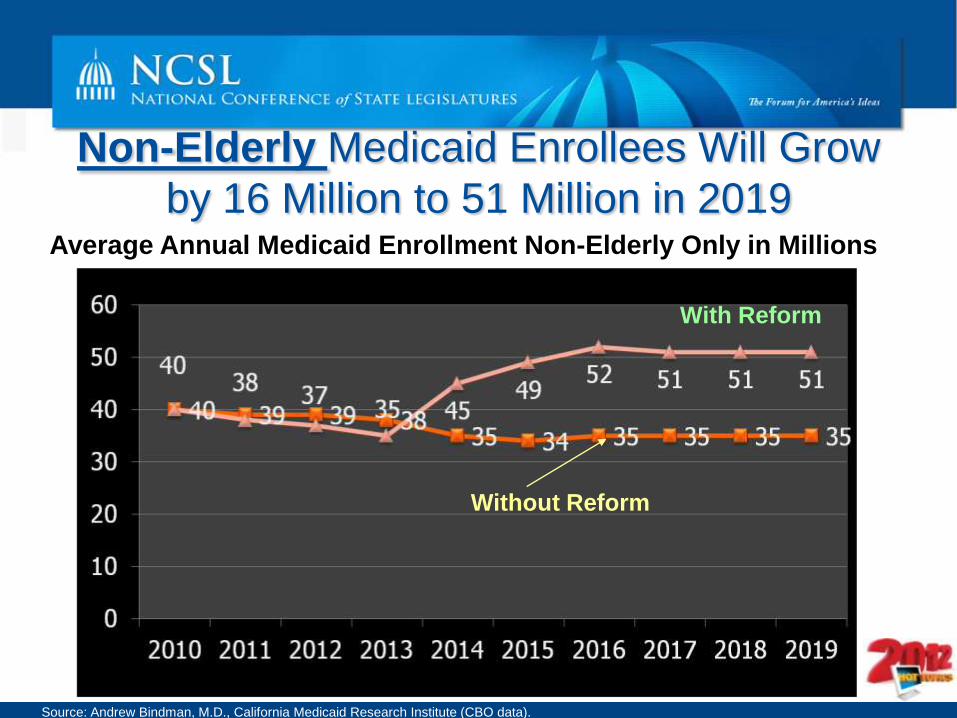
Non-Elderly Medicaid Enrollees Will Grow
by 16 Million to 51 Million in 2019 Average Annual Medicaid Enrollment Non-Elderly Only in Millions
With Reform
Without Reform
Source: Andrew Bindman, M.D., California Medicaid Research Institute (CBO data).
Other ACA-related Medicaid changes
Requires maintenance of effort (MOE) for state Medicaid and
Children’s Health Insurance Program (CHIP) eligibility levels.
Includes new mandatory and optional benefits in Medicaid.
Requires states to improve outreach and enrollment for
Medicaid and to coordinate Medicaid eligibility with the new
health benefit exchanges, which must be operational by
2014.
For a list of Medicaid changes, please visit:
http://www.ncsl.org/issues-research/health/medicaid-home-page.aspx

Why Medicaid is a top
issue for states in 2012
Fiscal situation in states
Enrollment increase associated with the Great
Recession
Affordable Care Act expansion in 2014
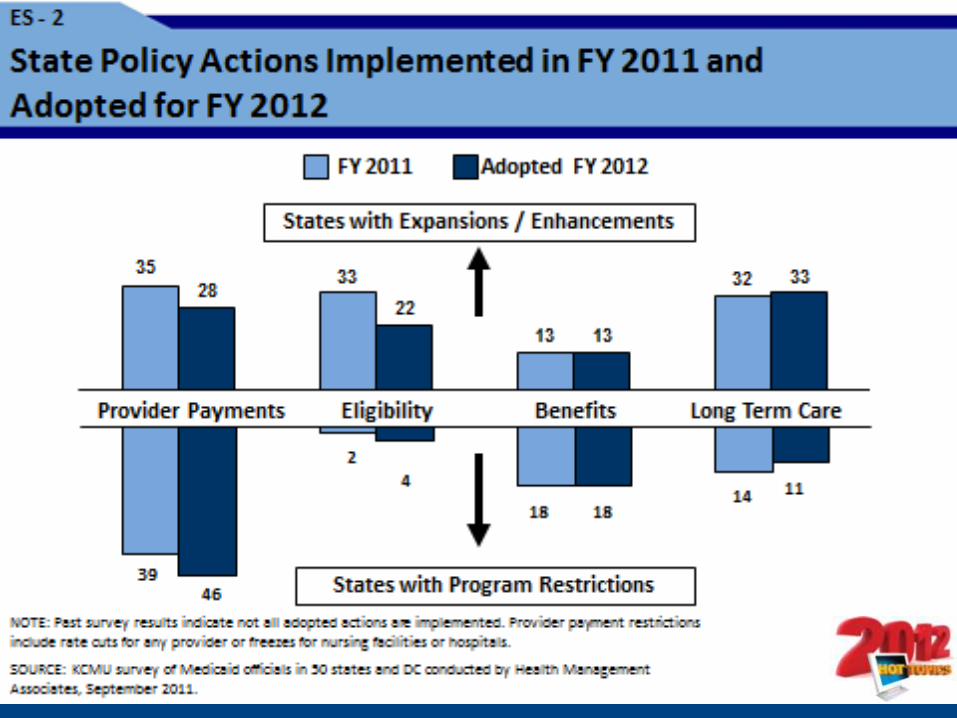
State actions to improve efficiency and
effectiveness within Medicaid programs
Why Medicaid is a top issue for states in 2012:
State Actions …
More than 200 Medicaid-related bills
have been filed this session in at least 34
states.
– More than 150 of these bills are
related to ACA implementation.
Many of these bills attempt to contain
costs within the program.
4 things for states to consider as they
address Medicaid issues
Know what the cost drivers are in your
state's Medicaid program.
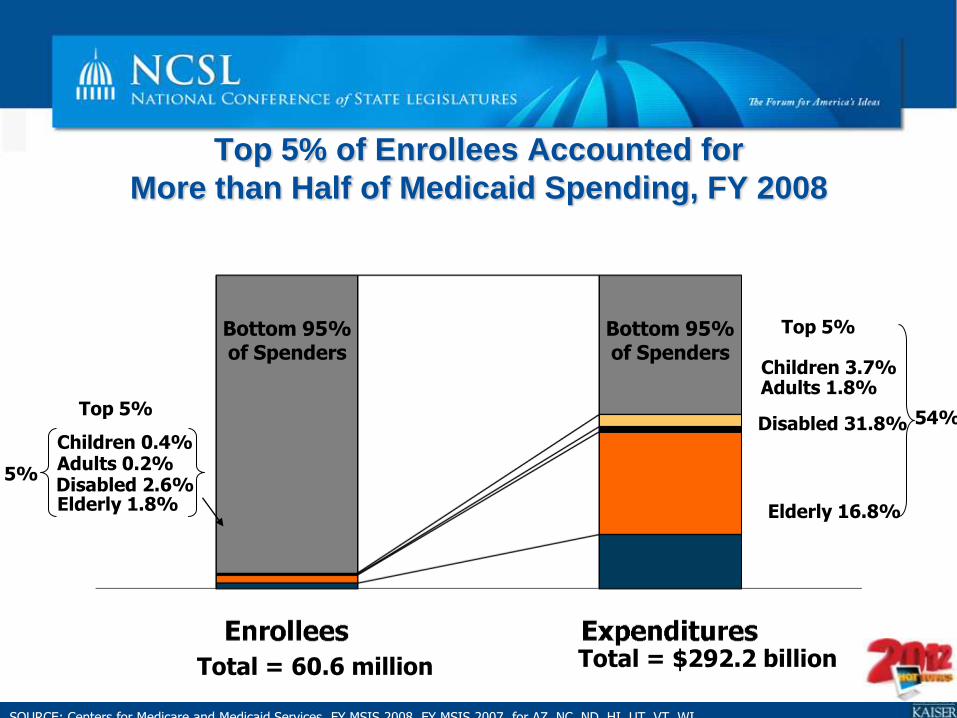
Children 3.7% Adults 1.8%
Children 0.4%
Top 5% of Enrollees Accounted for
More than Half of Medicaid Spending, FY 2008
SOURCE: Centers for Medicare and Medicaid Services, FY MSIS 2008, FY MSIS 2007 for AZ, NC, ND, HI, UT, VT, WI.
Disabled 31.8%
Total = 60.6 million Total = $292.2 billion
Elderly 16.8%
Bottom 95% of Spenders
Top 5%
Adults 0.2% Disabled 2.6% Elderly 1.8%
Top 5%
5%
54%
Bottom 95% of Spenders
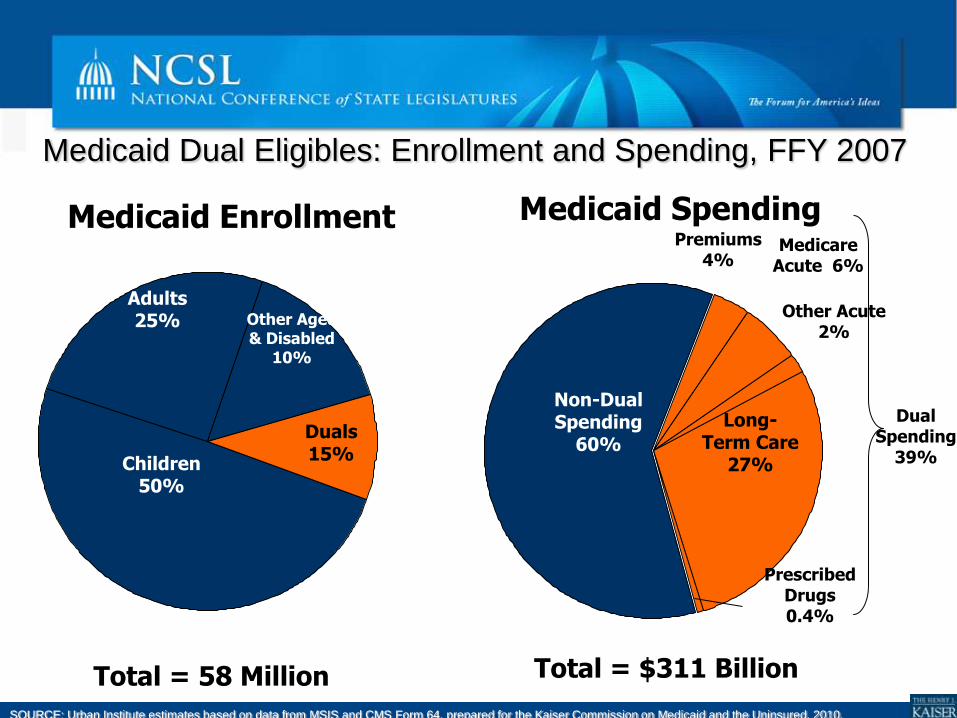
Medicaid Dual Eligibles: Enrollment and Spending, FFY 2007
SOURCE: Urban Institute estimates based on data from MSIS and CMS Form 64, prepared for the Kaiser Commission on Medicaid and the Uninsured, 2010.
Total = 58 Million
Medicaid Enrollment Medicaid Spending
Total = $311 Billion
Duals 15%
Children 50%
Other Aged & Disabled
10%
Adults 25%
Non-Dual Spending
60%
Long-Term Care
27%
Prescribed Drugs 0.4%
Premiums 4%
Medicare Acute 6%
Other Acute 2%
Dual Spending
39%
4 things for states to consider as they
address Medicaid issues
Know what the cost drivers are in your state's
Medicaid program.
Understand your state's Medicaid managed
care program's challenges and
opportunities.
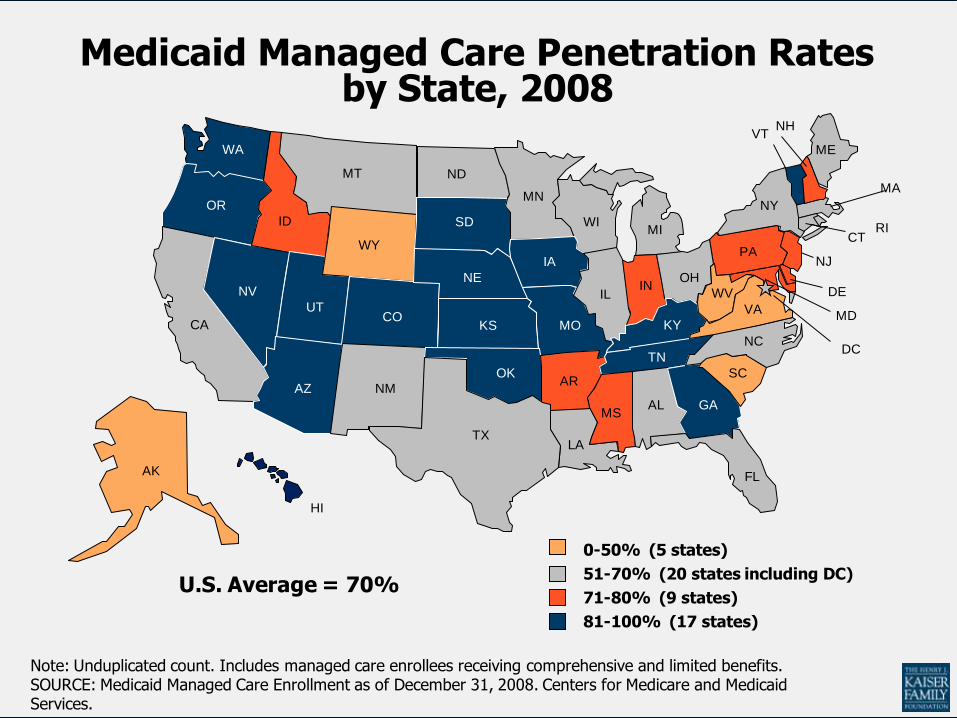
Figure 23
Medicaid Managed Care Penetration Rates by State, 2008
IL
CT
ME
NY
NH
MA
VT
PANJ
RI
AZ
WA
WY
ID
UTCO
OR
NV
CA
MT
HI
AK
NM
MN
ND
IA
WIMI
NE
SD
MOKS
OHIN
IL
AR
MS
LA
KY
TN
NC
VA
WV DE
MD
DC
SCOK
GA
TX
FL
AL
Note: Unduplicated count. Includes managed care enrollees receiving comprehensive and limited benefits.SOURCE: Medicaid Managed Care Enrollment as of December 31, 2008. Centers for Medicare and Medicaid Services.
U.S. Average = 70%51-70% (20 states including DC)
71-80% (9 states)
0-50% (5 states)
81-100% (17 states)
4 things for states to consider as they
address Medicaid issues
Know what the cost drivers are in your state's
Medicaid program.
Understand your state's managed care
contracts.
Fraud and abuse prevention and recovery
4 things for states to consider as they
address Medicaid issues
Know what the cost drivers are in your state's
Medicaid program.
Understand your state's managed care
contracts.
Fraud and abuse prevention and recovery
Health information systems
– Medicaid Electronic Health Records (EHR) Incentive
Program
Health Insurance Exchanges
Marketplace for health insurance.
Provide coverage options for individuals and small
businesses with more transparency than currently
exists today.
Vehicle for administering the new federal tax
credits for certain people who don’t have coverage
through their employer.
Enrollment "facilitator" for public programs.
What is Required?
Every state must have Exchange(s) for
individuals and small businesses (up to 100
employees), effective Jan. 1, 2014.
Will it be a state-based exchange, federally
facilitated exchange or a partnership?
Exchange health plans must offer a
minimum level of coverage.
Upcoming Deadlines and
Decisions
State-based exchanges must demonstrate
process is underway to establish an exchange
that will be operational by January 2014 via a
State Plan before January 1, 2013.
Options for States If a state decides to establish an exchange, it has the
following options:
A state agency
– Existing agency
– Independent public agency
A non-profit entity
Who will serve on the governing board?
Contract with other eligible entities to carry out various
functions of the exchange.
How will the state regulate insurers in the exchange?
Concerns and Challenges
Timeframe
Guidance
– First regulations published in July
– Medicaid coordination, subsidies, quality, and other
regulations still to come
Building/Upgrading Health Information
Technology Systems
Medicaid/Exchange Eligibility
Systems
Simpler eligibility rules
Efficient and easy to use seamless enrollment
"No Wrong Door" Approach
MD
AK*
HI
WA
OR
CA
ID
NV
MT
WY
UT CO
AZ NM
ND
SD
NE
KS
OK*
TX
MN*
IA*
MO
AR
LA
WI*
IL
MI*
IN
KY
TN
MS AL GA
FL
OH
WV VA
NC
SC*
DC
DE
PA* NJ
NY
CT
RI*
MA
VT
NH*
ME*
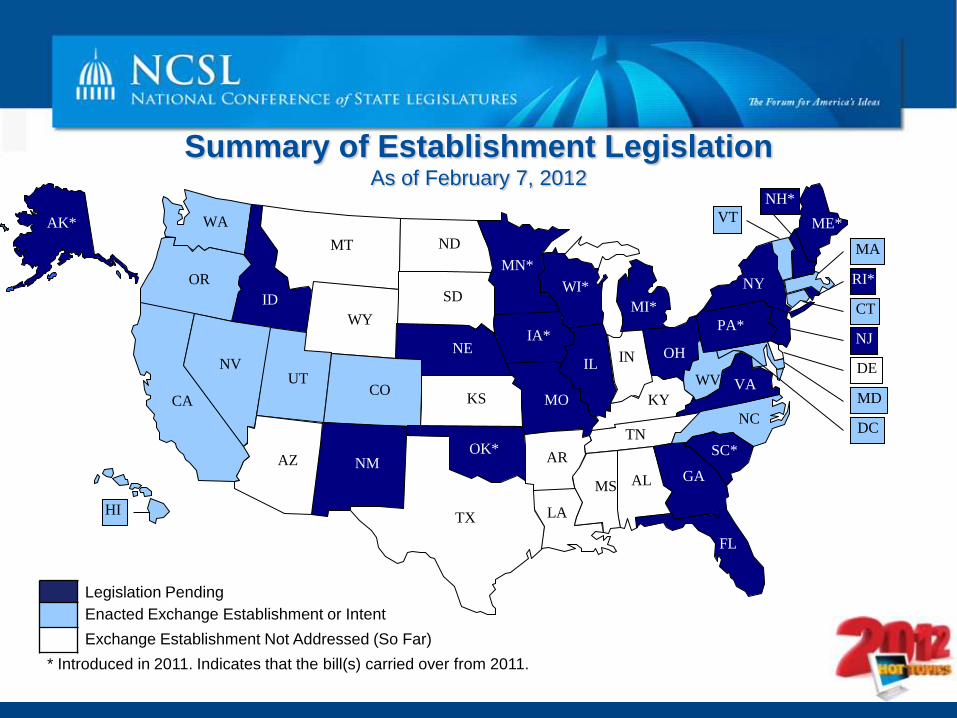
Summary of Establishment Legislation As of February 7, 2012
Legislation Pending
Enacted Exchange Establishment or Intent
Exchange Establishment Not Addressed (So Far)
* Introduced in 2011. Indicates that the bill(s) carried over from 2011.

State Exchanges State Structure Governance Carrier Selection
CA Independent State Agency 5 Member Board Active Purchaser
CO Non-Profit 12 Member Board All Plans Allowed
CT Quasi-Public 14 Member Board Active Purchaser
HI Non-Profit 15 Member Interim Board Commissioner will decide
MD Independent State Agency 9 Member Board Board will decide
MA Independent State Agency 11 Member Board Active Purchaser
NV Independent State Agency 10 Member Board TBD
OR Quasi-Governmental 9 Member Board Active Purchaser
UT Existing Agency Up to 9 Members All Plans Allowed
VT Existing Agency Deputy Commissioner All Plans Allowed
WA Public/Private Partnership 11 Member Board TBD
WV New Agency with Office of
Insurance
10 Member Board All Plans Allowed
Federal Funding Awarded 49 states and DC received up to $1 million in exchange planning
grants. Four territories received similar grants on March 21,
2011.
– FL, LA and NH returned grants, AK did not apply.
6 states and a multi-state consortium led by the University of
Massachusetts Medical School received over $241 million in
Early Innovator grants to develop model Medicaid/Exchange IT
systems.
– KS, OK and WI returned grants.
29 states and the District of Columbia were awarded $1-$39
million in level one exchange Establishment grants.
– More expected to come…
Essential Health Benefits Defining what services will be covered
The ACA requires HHS to define "essential health benefits"
for exchanges + small group + individual plans
nationwide.
– 10 uniform categories listed in the law.
– Additional details & definitions must be resolved in 2012.
ACA does not directly change or preempt state mandates.
Starting in 2014, states must cover extra cost of mandated
benefits that go beyond essential benefits package.
State Mandate Laws: a Major
Factor? Every state has a substantial but varied number
of state laws (about 1,600 nationwide) that
"mandate" commercial market health insurance
to cover specific benefits/providers.
Actual coverage mandates vary widely
– Autism = 29 states Home health = 20 states
– Diabetes = 47 states Acupuncturist= 11 states
Timeline: Latest developments
Oct 6, 2011 Institute of Medicine Report -
Dec. 16, 2011: Major change; HHS proposes to allow
each state to pick among its health plans. – 1 of largest state "small group" plans or
– 1 of largest state employee plans
– Largest state HMO in commercial market
– 1 of largest Federal Employee plans (FEHBP)
Jan. 25 - HHS list of 50-states' small group plans
Jan. 31, 2012 - Comments filed with HHS (including NCSL)
By May 1, 2012 - HHS final rules expected.
Expected state action for 2012-13
Most states will choose a single state-based or
FEBHP “essential benefit plan” in 2012.
Will legislatures weigh in or make decisions?
Legislatures may address existing state law
mandates in 2012 and 2013.
States could Expand? Repeal? Review?

Opposition to Health Reform:
States and the U.S. Supreme Court
State Attorneys General in the lead with court suits
25 federal court cases filed, divided rulings
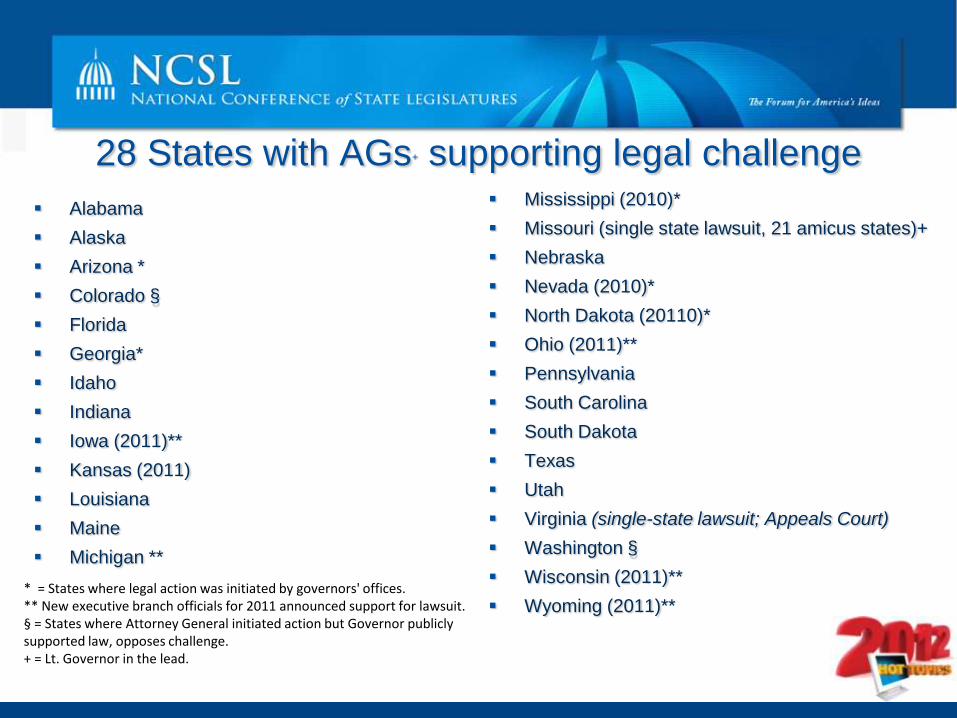
28 States with AGs+ supporting legal challenge
Alabama
Alaska
Arizona *
Colorado §
Florida
Georgia*
Idaho
Indiana
Iowa (2011)**
Kansas (2011)
Louisiana
Maine
Michigan **
Mississippi (2010)*
Missouri (single state lawsuit, 21 amicus states)+
Nebraska
Nevada (2010)*
North Dakota (20110)*
Ohio (2011)**
Pennsylvania
South Carolina
South Dakota
Texas
Utah
Virginia (single-state lawsuit; Appeals Court)
Washington §
Wisconsin (2011)**
Wyoming (2011)** * = States where legal action was initiated by governors' offices. ** New executive branch officials for 2011 announced support for lawsuit. § = States where Attorney General initiated action but Governor publicly supported law, opposes challenge. + = Lt. Governor in the lead.
4 Legal Issues in 3 Days of Oral Argument
Individual mandate - "Whether Congress had the power under
Article I of the Constitution to enact the minimum coverage provision."
Medicaid expansion - "Does Congress exceed its enumerated
powers ... when it coerces States into accepting onerous conditions that
it could not impose directly by threatening to withhold all federal funding"
for non-compliance?
Severability - "To what extent (if any) can the mandate be struck
down but) severed from the remainder of the Act?"
Delay decision due to Anti-Injunction Act- whether the penalty
provision in the ACA is a tax, which could prevent a court challenge until
it is in effect, 2014.
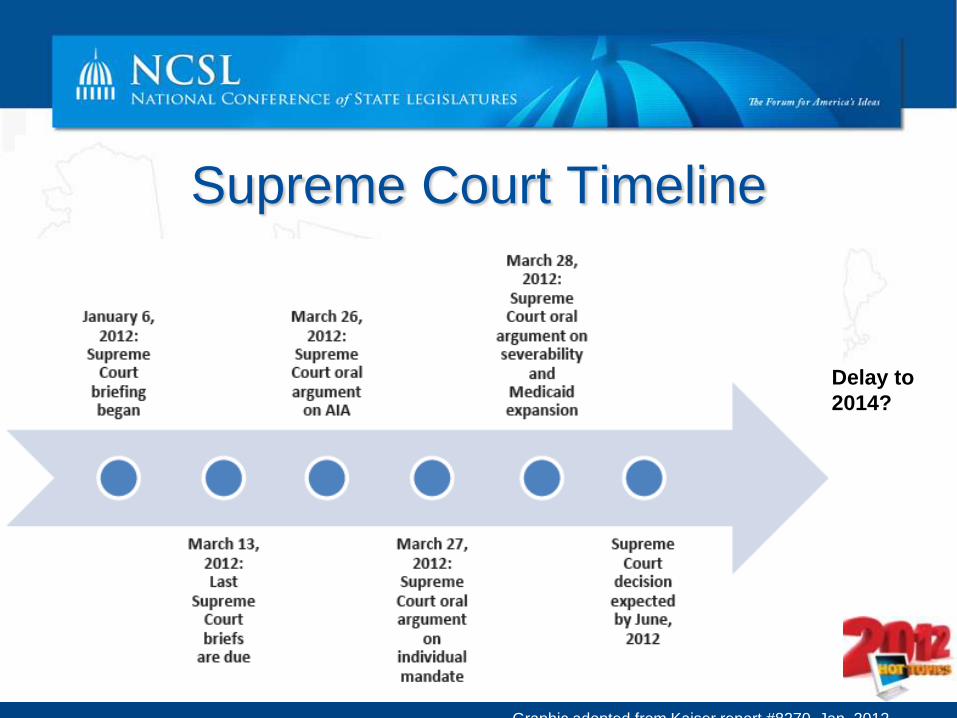
Supreme Court Timeline
Delay to
2014?
Graphic adopted from Kaiser report #8270, Jan. 2012
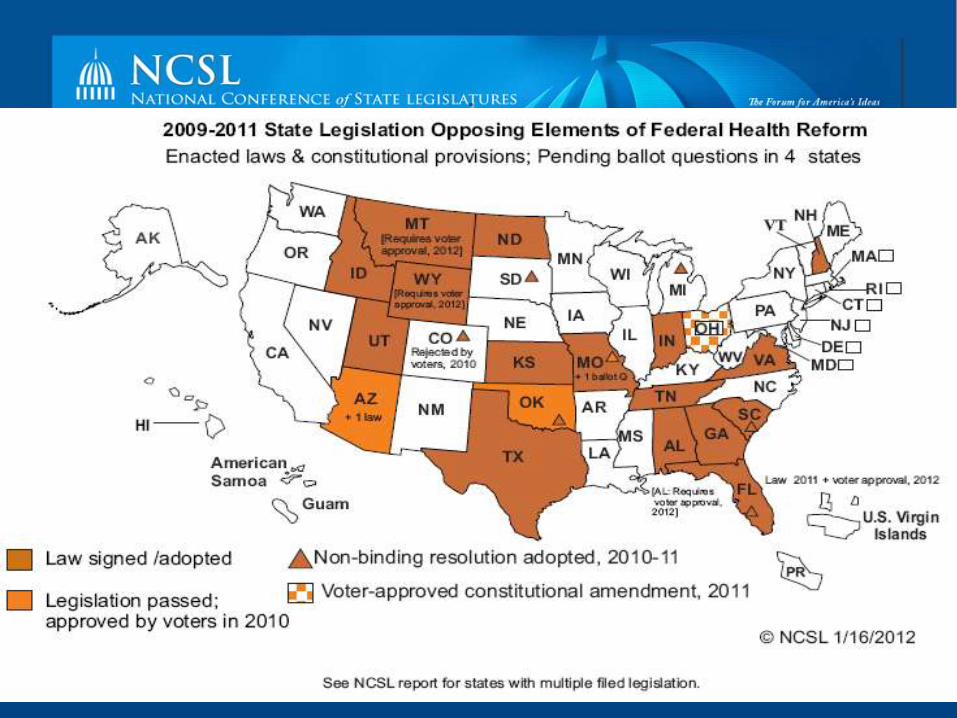
State Legislation Opposing, Opting Out or Avoiding Certain Reforms
• In 2011: 45 states considered 210 proposals.
• In 2012: 34 states are considering 125 proposals (so far)
• Most bills seek to block state government involvement; creating a policy
of no implementation or enforcement of mandates (federal or state) to
require:
– purchase of insurance by individuals,
– or contribution to premiums by employers,
– or imposing fines or penalties for those who fail to do so.
90% of state bills do not discuss federal constitutionality.
Missouri ballot question, election day , 8/3/10
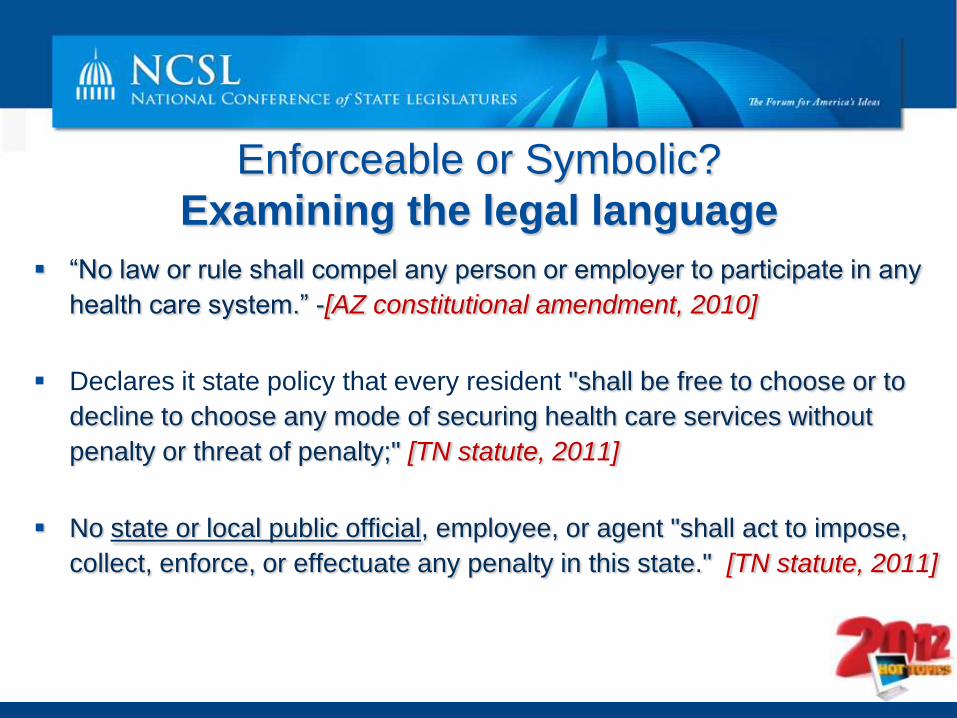
Enforceable or Symbolic?
Examining the legal language
“No law or rule shall compel any person or employer to participate in any
health care system.” -[AZ constitutional amendment, 2010]
Declares it state policy that every resident "shall be free to choose or to
decline to choose any mode of securing health care services without
penalty or threat of penalty;" [TN statute, 2011]
No state or local public official, employee, or agent "shall act to impose,
collect, enforce, or effectuate any penalty in this state." [TN statute, 2011]
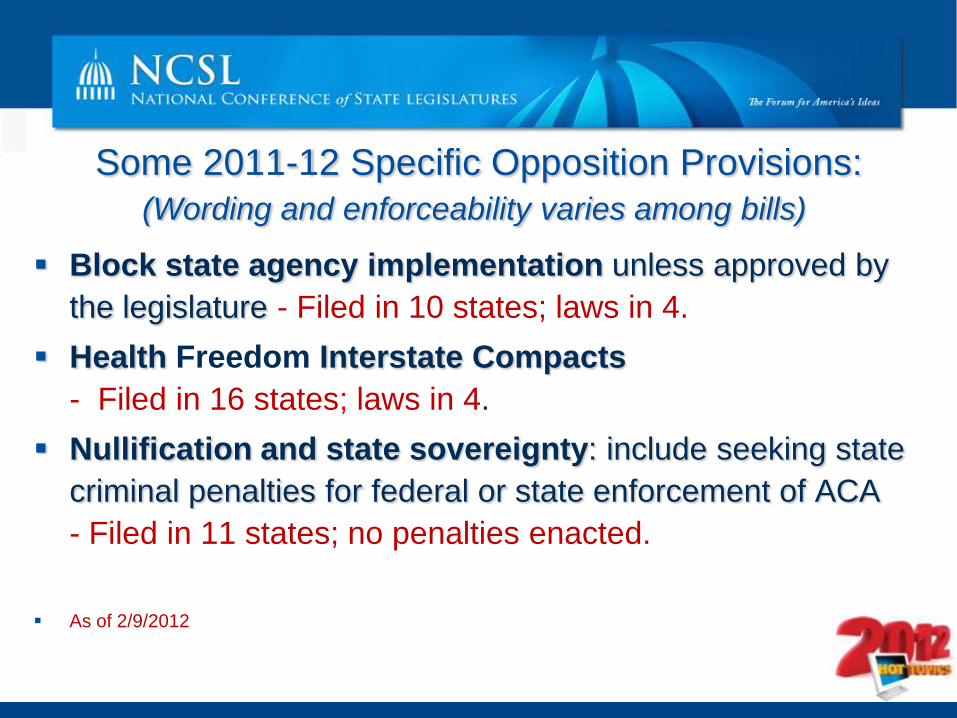
Some 2011-12 Specific Opposition Provisions:
(Wording and enforceability varies among bills)
Block state agency implementation unless approved by
the legislature - Filed in 10 states; laws in 4.
Health Freedom Interstate Compacts
- Filed in 16 states; laws in 4.
Nullification and state sovereignty: include seeking state
criminal penalties for federal or state enforcement of ACA
- Filed in 11 states; no penalties enacted.
As of 2/9/2012
.
Upcoming Webinars:
Feb.13 Putting Election Laws to the Test
Feb. 17 Corrections, Juvenile Justice and Drugged Driving
Feb. 20 Transportation Funding, Natural Gas and
Environmental Regulations
Feb. 24 Funding Education in a Climate of Cutting
Questions & Contact Information
•The webinar archive and power points will be
emailed to you next week.
•Contact
•For more information: •www.ncsl.org/healthreform
•www.ncsl.org/issues-research/health/medicaid-home-page.aspx