Embed Size (px)
Citation preview

http://fai.sagepub.com/Foot & Ankle International
http://fai.sagepub.com/content/33/9/787The online version of this article can be found at:
DOI: 10.3113/FAI.2012.0787
2012 33: 787Foot Ankle IntAndrew R. Hsu
Topical Review: Barefoot Running
Published by:
http://www.sagepublications.com
On behalf of:
American Orthopaedic Foot & Ankle Society
can be found at:Foot & Ankle InternationalAdditional services and information for
http://fai.sagepub.com/cgi/alertsEmail Alerts:
http://fai.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
What is This?
- Sep 1, 2012Version of Record >>
at UNIVERSITAETBIBLIOTHEK on May 21, 2014fai.sagepub.comDownloaded from at UNIVERSITAETBIBLIOTHEK on May 21, 2014fai.sagepub.comDownloaded from

FOOT & ANKLE INTERNATIONAL
Copyright 2012 by the American Orthopaedic Foot & Ankle SocietyDOI: 10.3113/FAI.2012.0787
Topical Review: Barefoot Running
Andrew R. Hsu, MDChicago, IL
Key Words: Barefoot Running; Biomechanics; Gait
INTRODUCTION
Barefoot running has seen a resurgence of popularity inrecent years driven by claims of enhanced running efficiencyand injury prevention as individuals continue to explore alter-native training strategies to improve performance.19,62,65 Thisrising interest has sparked a significant growth of scientificresearch investigating the physiology, biomechanics, perfor-mance effects, and injury mechanisms of barefoot running.It has been established that footwear plays a significantrole in the pathophysiology of foot and ankle disordersby creating biomechanical changes in force transmission,lower extremity position, and gait kinematics.11,44,46,65
Since the invention of modern cushioned heel footwearin the 1970s, there has been a worldwide proliferation ofshoe manufacturers with claims of improved foot safetyand injury prevention that have gone unproven. Despiteprevious discussions in the scientific community in the1980s regarding the effects of barefoot running,6,16,28,59,60
there has been renewed mainstream media interest regardingbarefoot running as recreational and professional athletesexplore new training programs to increase strength andendurance.
Foot and ankle injuries associated with running includestress fractures, plantar fasciitis, and ligamentous injuries,among many others.1,2 Specific causative factors for theseinjuries such as anatomic and kinematic variables are notwell delineated or understood. Studies investigating therole of footwear in injury patterns report conflicting data
No benefits in any form have been received or will be received from a commercialparty related directly or indirectly to the subject of this article.
Corresponding Author:Andrew R. Hsu, MDDepartment of Orthopaedic SurgeryRush University Medical Center1611 West Harrison Street, Suite 200Chicago, IL 60612E-mail: [email protected]
For information on pricings and availability of reprints, e-mail [email protected] call 410-494-4994, x232.
as to whether the cushioned heel of modern shoes isbeneficial or detrimental to gait and foot force transmis-sion during running.7,20,34,65 There is considerable ongoingdebate regarding the proposed benefits and harms of bare-foot running with little consensus other than the needfor future well-designed studies.37 Proponents of barefootrunning argue that the development of modern footwearis detrimental from an evolutionary perspective as humansadapted a successful characteristic gait as a result of barefootstimulation.4,44 One of the central arguments in favor of bare-foot running is that the hindfoot strike induced by modernfootwear increases ground impact forces and decreases adap-tive foot proprioception, thus potentially increasing rates ofinjury.
A landmark study by Lieberman et al. showed that habit-ually barefoot endurance runners landed on the forefootor midfoot with a more plantarflexed ankle, whereas shod(footwear) runners landed on the hindfoot with significantlyhigher collision forces.44 The clinical implications of theseresults have not been investigated and remain theoretical.Those who oppose barefoot running contend that it is anexercise “fad” that is potentially harmful to individuals whoare not properly trained.43 Despite the increased recent atten-tion given to barefoot running as a potential performance-enhancing training strategy, the scientific evidence is lacking,without any clear conclusions for or against its use. Thereare also initial reports being published of injuries, such asmetatarsal stress fractures, induced by barefoot-simulatingfootwear that strongly caution against an abrupt transitionfrom shod to barefoot running.17
With the increased demand for minimalistic shoes, foot-wear manufacturers have released multiple lines of barefoot-simulating footwear to provide the flexibility and feel ofbarefoot running while also protecting the plantar foot fromenvironmental hazards. Currently, there are no clinical guide-lines that exist to help patients with and without estab-lished foot pathology transition to barefoot running in asafe and effective manner. Despite the lack of scientificevidence, the popularity of barefoot running among thepublic continues to steadily rise, and the growing numberof barefoot runners has significant potential implications for
787
at UNIVERSITAETBIBLIOTHEK on May 21, 2014fai.sagepub.comDownloaded from

788 HSU Foot & Ankle International/Vol. 33, No. 9/September 2012
the incidence rates of foot and ankle injuries in the generalpopulation. The purpose of this review is to present thephysiologic and biomechanical evidence in the literaturebehind barefoot running to help inform physicians caringfor patients interested or involved in this alternative formof training. A literature review of English-language arti-cles in medical publications that investigated barefoot and/orshod running was conducted in PubMed MEDLINE and theCochrane Database of Systemic Reviews from 1969 through2012. Primary studies, review articles, meta-analyses, andcase reports were included from the foot and ankle surgery,orthopaedic surgery, sports medicine, biomechanical, exer-cise physiology, and internal medicine literature.
BACKGROUND
The characteristic striding bipedal locomotion of man hasbeen one of the defining characteristics of humans and ourancestors for more than 2 million years.4 The specializedanatomy of the human foot represents the end product ofbarefoot bipedalism evolution with gait adaptations that haveremained largely unchanged until modern times.4 Devel-opmental adaptations, such as a robust and pliable mediallongitudinal arch, improved the mechanics of running in earlyman by storing and releasing elastic energy with increasedefficiency through mass-spring mechanics.30 Early permu-tations of footwear consisted of simple, thin coverings ofleather with string that had no arch or heel support andmainly served to protect against environmental hazards tothe skin of the sole.46,60 The advent of modern shoes withelevated and cushioned heels did not occur until the 1970s,when the prevailing thought was that human feet were fragileand unable to withstand the large impact stresses of runningwithout adequate support, elastic cushioning, and motioncontrol.
The counterargument supporting barefoot running is thatincreasingly padded and restrictive shoes cause disuseatrophy and stiffness of the intrinsic foot musculature, thusplacing larger demands on the surrounding joints and plantarfascia.60 In essence, if humans have evolved to run bare-foot over millions of years, it logically follows that naturalselection and evolution did not adapt the foot to runningin shoes. One of the main pieces of evidence in support ofbarefoot running is the unchanging prevalence and epidemi-ology of foot and ankle injuries in modern times. Despite thetechnological and research-driven design advances made infootwear over the past 30 years,50 the rates of running-relatedinjuries in the general population has remained relativelyconstant, with an incidence ranging from 35% to 79% instudies published between 1982 and 2010.25,35,45,51,68,69,71
In these studies, the most common site of injury reportedis the knee (7% to 50%) followed by the lower extremity(9% to 32%) and the foot (3% to 38%). However, injuryrates of the foot and ankle in competitive sports may becurrently increasing,23 and this has led many researchers to
the conclusion that footwear does not have adequate protec-tive effects or adaptive changes and may in fact exacerbaterunning injuries.
Despite persistently elevated injury rates, the use ofincreasingly cushioned and restrictive footwear has grownto become nearly ubiquitous in modern society, althoughthere is no supporting evidence of its clinical benefits. Someresearchers believe that among different types of footwear,cushioned heel running shoes have little to no benefit overless supportive footwear and may prove harmful in thelong term.9,49,50,52,55,56,58 One of the early supporters ofbarefoot running in the scientific literature was Robbins andHanna, who found significantly higher rates of foot injuryin individuals wearing shoes in Haiti compared with thosewho were habitually barefoot.60 Although injury rates werelikely multifactorial in this study, these findings provideda key springboard for subsequent research exploring thepotential benefits and risks of barefoot running. An analysisof the physiologic and biomechanical studies of barefootrunning in the literature reveals that its effects can be brokendown into five main categories: (1) anatomic adaptations,(2) metabolic demands, (3) proprioception, (4) impact forces,and (5) coordinative strategy.
PHYSIOLOGY
Anatomic adaptationsAnthropometric studies have provided valuable insight
into the effects of footwear on anatomic adaptations of thefoot, including intrinsic flexibility, muscular strength, andarch development.27,49 A guiding principle to foot adaptationis that the musculoskeletal system is responsive to loadingand requires stress in order to remodel and become stronger.Therefore, shoes with stiff soles and movement controlprevent bones and muscles from properly adapting to loadsincurred during impact activities such as running. Wolf etal. investigated foot pathology in children and cautioned thatyoung children should not wear restrictive footwear becauseof potential foot deformity and stiffness.73 Using foot modelanalyses, the authors demonstrated that footwear constrainsthe natural movements of the foot, particularly in regardsto forefoot to hindfoot motion. There was a 4% decreasein medial arch length when going from barefoot to shodconditions along with a 5◦ loss of range of motion in foottorsion along the longitudinal foot axis.73
The idea of avoiding restrictive footwear in childrenis supported by the American Academy of Pediatrics,which has stated that children should not wear shoes untilnecessitated by the surrounding environment because ofimpaired intrinsic musculature development caused by rigidfootwear.67 Sachithanandam and Joseph have shown that theearlier a child begins wearing footwear, the higher is thelikelihood of developing flatfoot deformity.63 Correlation ofthe static footprints of skeletally mature individuals with theage at which they began to use footwear showed a 1.8-fold
Copyright 2012 by the American Orthopaedic Foot & Ankle Society
at UNIVERSITAETBIBLIOTHEK on May 21, 2014fai.sagepub.comDownloaded from

Foot & Ankle International/Vol. 33, No. 9/September 2012 BAREFOOT RUNNING 789
increase in the incidence of flatfoot between subjects whofirst wore shoes before 6 years of age compared with thosewho started at the age of 16.63 Kadambande et al. comparedhabitually shod and barefoot individuals and found that footpliability was significantly decreased with similar intrinsicfoot musculature in the shod group.27 Rao and Joseph inves-tigated the effects of footwear on medial arch development inchildren and found that footwear had a 3-fold increase (9%versus 3%) in the incidence of flatfoot and was detrimental tothe development of the longitudinal arch and strength of theplantar intrinsic muscles.49 Further analysis showed that chil-dren wearing closed-toe shoes had a 2-fold higher incidence(13% versus 6%) of flatfoot compared with those wearingsandals without arch or heel support. Significant differencesin the development of foot musculature between barefoot andshod individuals have also been seen in adult populations.
Bruggemann and Potthast showed that running with bare-foot simulation footwear significantly increased the cross-sectional size and strength of intrinsic foot muscles in adultswith a 20% increase in metatarsophalangeal flexor strength inbarefoot simulation subjects compared with shod conditions.5
A proposed conclusion from these results was that strongerintrinsic musculature can elevate the arch of the foot to createa more effective shock absorber by deflecting the medial archof the foot on loading. Divert et al. have further shown thatbarefoot running causes elevated electromyographic activityin the preactivation of plantarflexion muscles, including thegastrocnemius and soleus, thus decreasing stress to the lowerextremity.13
Metabolic demands and proprioception
Studies have shown reduced oxygen consumption andlowered rate of perceived exertion in barefoot versus shodrunning groups with an overall decrease in energy expen-diture of roughly 5.7%.6,8,19 Divert et al. studied thesemetabolic differences and stated that the increased energyuse with shod running was likely attributable to effects offootwear mass along with shoe-related shock attenuationand a decreased net running efficiency.14 However, Perlet al. recently investigated differences in running economybetween minimal shoes and standard running shoes andfound a 3% improvement in oxygen transport in minimallyshod runners after controlling for shoe mass and stridefrequency.48 Webb et al. noted that the repetitive deformationof the shoe with each foot strike multiplied many times overduring a run removes elastic energy that could otherwise besaved and transferred if barefoot.72
Plantar proprioception during running activates reflexesand variable kinematic gait patterns to help maintain stability,avoid painful impacts, and modulate leg stiffness to avoidtraumatic and repetitive injuries.43 Robbins et al. inves-tigated proprioception while barefoot under static condi-tions to detect changes in ground slope and found thatthere was a loss of plantar tactile sensibility with shoe
wear and aging.56 The authors concluded that any protec-tive barrier between the plantar mechanoreceptors and theground surface, such as conventional footwear, significantlydecreases foot position awareness and the foot’s abilityto rapidly adapt to changing surfaces. The implications ofdecreased proprioception are worsened balance and footreaction time that may predispose patients to falls andother injuries.52,55 Fast-adapting plantar mechanoreceptorsplay a key role in postural control and balance duringambulation.22
Studies have shown that ankle injury is one of the mostcommon sports-related injuries, constituting 15% to 30% ofall sports injuries in athletes.1,16 Hootman et al. reported thatankle ligament sprains are the most common injury amongcollege athletes, constituting roughly 15% of all reportedinjuries.23 In younger high school athletes, foot and ankleinjury rates are even higher, at approximately 40% of allathletic injuries with sprains being the most prevalent.3 Crit-ical to the prevention and management of lateral ligamentouscomplex injuries of the ankle are the findings of Lephart etal., who have shown the importance of retraining propri-oception during rehabilitation to restore afferent feedbackfrom the joint.42 Robbins et al. found that barefoot condi-tions resulted in a 58% increase in foot position aware-ness compared with ankle taping.57 The authors stated thatankle sprains are attributable to reduced proprioception thatcauses an inability to utilize anticipatory muscle movementsin dynamic situations that may be improved with barefootambulation.54
The idea of injury prevention through enhanced proprio-ception was reinforced by Stacoff et al., who found increasedlateral ankle stability as measured by range of motion ininversion and angular velocity of the hindfoot during side-ward cutting movements in barefoot versus shod runninggroups.66 In this study, the greatest ankle stability wasfound in barefoot subjects, even when compared with shoesspecifically modified to improve lateral stability throughincreased stiffness and ankle constraint. Waddington andAdams found that elite soccer players had an enhancedability to discriminate ankle inversion movements when bare-foot compared with when wearing soccer footwear.70 Thesefindings together imply that increased proprioception duringbarefoot running may provide individuals with greater footadjustments to impact and decreased foot position error thatcan cause injury. However, it is important to note that thereare no studies to date that have shown a reduced rate ofrunning injuries between barefoot and shod runners resultingfrom changes in proprioception.
BIOMECHANICS
Impact forcesThe kinematics and biomechanics of barefoot and shod
running have been described in the literature but with
Copyright 2012 by the American Orthopaedic Foot & Ankle Society
at UNIVERSITAETBIBLIOTHEK on May 21, 2014fai.sagepub.comDownloaded from

790 HSU Foot & Ankle International/Vol. 33, No. 9/September 2012
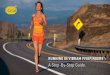
conflicting results and conclusions regarding their clinicalimplications.11,44,65 A key factor of shod running is thatthe cushioned heel of footwear positions the sole of thefoot in 5◦ less dorsiflexion than the sole of the shoe, thuspermitting runners to hindfoot strike more often and withgreater comfort. The most easily discernible gait adaptionassociated with barefoot running is a plantarflexed footposition leading to a predominantly forefoot and midfootstrike pattern (Figure 1). Despite various definitions used, ingeneral, hindfoot strike is a landing in which the heel landsbefore the ball of the foot (heel–toe run), a midfoot strikeis a simultaneous landing of the heel and ball of the foot,and a forefoot strike is a landing in which the ball of thefoot lands before the heel (toe–heel–toe).43 Hasegawa et al.analyzed the foot strike patterns of 415 runners during a half-marathon and found that roughly 75% of runners in standardshoes exhibited a hindfoot strike pattern.21 A midfoot orforefoot strike pattern was used by 25% of the shod runnersstudied, but this percentage was increased to 36% among eliterunners. It has been shown that hindfoot strike running cangenerate lower extremity forces 1.5 to 3 times body weightduring each foot impact.13
Shorter stride length and greater leg and ankle compliancecombined with quicker turnover rate act to lower the body’scenter of mass relative to the force of impact, so that thefoot lands more vertically aligned with the hip and knee.The combination of these adaptations has been shown byLieberman et al. to result in a 3-fold decrease in overallpeak ground forces as measured by impact force in bodyweights in barefoot versus shod running groups (0.58 versus1.74 body weights).44 Barefoot runners who forefoot strikehave also been shown to have a mean rate of loading (bodyweights per second) seven times lower than that of habituallyshod runners who hindfoot strike while barefoot.44 Thesefindings were discovered using a unique collisional modelof the foot and lower extremity as a double pendulum tocalculate how much energy was exchanged with the groundat different points of the foot with a stiff or flexible ankle.The authors found that forefoot strike patterns associatedwith barefoot running reduced the effective mass of the footand converted translational energy into rotational energy, thusallowing runners to maximize the recovery of elastic energystored in the Achilles tendon and longitudinal arch. In aforefoot strike, the arch of the foot acts as an elastic springstretching from foot strike until midstance, then recoilingduring the second phase of stance to transfer energy forforward propulsion.48
Several authors have suggested that the increased impactforces associated with shod running combined with over-training may exceed the tensile limits of soft tissue andbony structures in the lower extremity, thus causing running-related injuries.24,26 Edwards et al. showed that reducingstride length by 10% with an increased stride rate candecrease the strain magnitude experienced by bone duringrunning and lower the probability of stress fracture injury by
A
B
Fig. 1: Vertical ground impact forces and foot kinematics in shod andbarefoot running conditions. (A) A hindfoot strike pattern during shodrunning generates an early impact transient on heel contact with theground with the ankle dorsiflexed, whereas (B) a forefoot strike patternduring barefoot running produces no impact transient with a smoother forcetransmission through a more plantarflexed initial foot position. (Reproducedwith permission from Lieberman et al: Foot strike patterns and collisionforces in habitually barefoot versus shod runners. Nature 463:531–535,2010.)
3% to 6%.15 In addition to decreases in foot–ground impactforces in barefoot conditions, Shakoor and Block found thatwalking barefoot decreased peak joint loads at the hips andknees and reduced knee adduction moment by 11.9% inpatients with osteoarthritis.64 The authors stated that alteredgait mechanics with barefoot ambulation, in particular, stride,cadence, and range of motion, were the likely contributingfactors.
Changes in lower extremity joint torque with barefootrunning have been investigated by Kerrigan et al. usingthree-dimensional motion analysis.32 The authors found a54%, 36%, and 38% increase in hip internal rotation torque,knee flexion torque, and knee varus torque, respectively, withshod compared with barefoot running. In theory, decreasedjoint forces and torques may potentially decrease muscleand tendon strain and therefore reduce rates of injurywith barefoot running. However, while multiple studieshave confirmed reductions in impact forces during barefoot
Copyright 2012 by the American Orthopaedic Foot & Ankle Society
at UNIVERSITAETBIBLIOTHEK on May 21, 2014fai.sagepub.comDownloaded from

Foot & Ankle International/Vol. 33, No. 9/September 2012 BAREFOOT RUNNING 791
running,12,13,44,65 no studies have shown the clinical corre-lations of this finding.46
Coordinative strategy
The main principle behind ankle coordinative strategy isthat a runner will continually modify ankle and foot posi-tion to optimize efficiency and avoid undesirable positionsbased off of sensory feedback to the limb. Kurz and Ster-giou investigated the effects of footwear style and stiffnesson ankle coordinative strategy during the running stancephase to determine whether there are unconscious modifi-cations in subtalar joint positioning during barefoot runningto maximize gait efficiency.38 The authors found increasedinversion of the subtalar joint with a plantarflexed ankleposition and forefoot strike pattern in barefoot versus shodrunning. The inverted subtalar position was thought to becaused by a reduced need for shock attenuation throughsubtalar pronation, because increased surrounding muscula-ture activation could provide the necessary shock dampening.Followup studies by Kurz et al. showed that kinematic gaitvariability was increased in barefoot compared with shodrunners, suggesting that there is an increased ability of footmechanoreceptors to adjust the joint pattern and avoid repet-itive impact forces.39,40 Robbins and Hanna reported thatbarefoot running improved sensory feedback and changedfoot strike position to be centered around the metatarsal headsrather than the heel.60 These improved coordination strate-gies are thought to be largely attributable to the enhancedfoot proprioception seen in barefoot running.56
Divert et al. found lower contact and flight times, increasedbraking and pushing impulses, and increased preactivationof the triceps surae muscles during barefoot running.13
The authors explained that because of improved sensoryfeedback and muscle coordination, the triceps surae canbetter anticipate impact during foot contact with the groundand therefore reduce the force at foot strike. An importantpoint raised by the authors was that earlier findings byKomi et al., which showed significantly increased verticalimpact forces during barefoot running, did not give subjectsenough time to acclimate to the new forefoot strike pattern.33
Therefore, subjects tested in that study were continuing to runin a hindfoot strike pattern while under barefoot conditions.
Forefoot striking creates a smoother impact force profilethat more evenly distributes total forces across each stride.44
From a mechanical standpoint, a disadvantage of footwearis that its geometry elevates foot position and increases thelever arm length between the ground reaction force andthe subtalar joint axis. This altered position decreases anklecoordination and magnifies supination forces and stresses onthe lateral ankle ligaments during shod running.28,66 Findingsby Kerr et al. support this concept by demonstrating increasedperoneus longus muscle contraction in shod versus barefootpatients when given an unanticipated, sudden inversionforce.31 This increased muscle contraction thus indicates that
a larger compensatory mechanism is needed to counteract theinherent inversion of the shod condition.
POTENTIAL RISKS
Opponents of barefoot running point to potential associ-ated risks as one of the primary reasons to continue shodrunning. The proposed dangers of barefoot running rangefrom superficial skin injury to repetitive stress overload andfoot deformity.17,33,47 In healthy individuals, the skin alongthe plantar surface of the foot, especially the thickened heelpad, is resilient and requires a 6-fold higher abrading loadin order to reach pain threshold compared with other skinsurfaces.53,59 Although there is a generalized increased riskof skin abrasions, thermal injury, puncture wounds, and local-ized infection with barefoot running depending on the localenvironment, no studies to date have investigated the inci-dence of superficial injuries from barefoot running specifi-cally. Immunocompromised patients, diabetics, and patientswith peripheral neuropathy or wound healing dysfunction inparticular are cautioned against barefoot running despite thedecreases in foot impact forces because of their elevated riskof foot ulceration and infection.41
Nearly all of the studies that have shown increased forcesat foot impact and shock transmission to back musculaturewith barefoot running have been refuted because of flawedmethodology.33,47 These studies tested habitually shod, hind-foot striking runners under barefoot conditions but did notaccommodate for changing gait patterns that are the maincomponent of barefoot running. Improper implementation ofbarefoot running is a potential risk that can have seriousclinical consequences. Forefoot striking requires more calfmuscle strength than hindfoot striking and places increaseddemands on intrinsic foot musculature. Inadequate transi-tion to barefoot running may induce calf muscle strainsand Achilles injury, both of which reflect increased plan-tarflexion moments.43 Giuliani et al. recently reported twocases of metatarsal stress fractures in experienced runnerswhose only training change was the transition from shodrunning to barefoot-simulating footwear (Figure 2).17 Oneof the main risk factors discussed was the lack of a properbarefoot gait implementation program to transition from ahindfoot to forefoot strike pattern. Therefore, even thoughthese patients were running barefoot, they were continuingto hindfoot strike, thus subjecting their feet to repetitiveincreased peak forces at the metatarsals. A critical elementof barefoot running is the progressive, sustained implementa-tion of shock-reducing forefoot strike patterns over a periodof weeks to months.58
There are no studies that have examined the most effec-tive implementation program for barefoot running as themajority of training programs thus far have been anec-dotal and unproven. Robbins and Gouw suggested a 6-weekadaptation period for plantar skin and musculature along
Copyright 2012 by the American Orthopaedic Foot & Ankle Society
at UNIVERSITAETBIBLIOTHEK on May 21, 2014fai.sagepub.comDownloaded from

792 HSU Foot & Ankle International/Vol. 33, No. 9/September 2012
Fig. 2: Axial T1-weighted, fat-suppressed, magnetic resonance imaging(MRI) showing marrow edema and stress reaction of the entire left secondmetatarsal with soft tissue edema in a 19-year-old runner who newly adoptedbarefoot-simulating footwear for 3 to 4 weeks. Patient was successfullytreated with protected weight bearing and modified activity. (Reproducedwith permission from Giuliani et al: Barefoot-simulating footwear associatedwith metatarsal stress injury in 2 runners. Orthopedics 34:e320–323, 2011.)
with short periods of daily barefoot running when transi-tioning from shod to barefoot conditions.58 However, thebasis for this length of time was not tested or substanti-ated by any scientific evidence. Therefore, with the growingpopularity of barefoot running and lack of formal imple-mentation programs, it is possible that additional negativeclinical sequelae may arise in the future with broad publichealth implications. Although studies have demonstrated thatbarefoot running decreases ground reaction forces at footstrike,44,65 this does not mean that the overall load placedon the lower extremity is reduced. Increasing activation ofankle plantarflexors and the gastrocnemius-soleus complexduring foot strike reduces impact forces but may subse-quently increase surrounding joint and tendon strain. Thepotential effects and clinical consequences of these additionalmuscular forces remain to be clarified.
CURRENT LIMITATIONS
Although there is evidence in the literature to supportthe physiologic and biomechanical advantages of barefootrunning, many of the studies are significantly limited inmethodology and level of evidence. In investigations of bare-foot running, it is critical to control for strike type, shoeweight, shoe type, and the baseline strike patterns of subjects
because all of these factors can have a major influence onstudy results. Several studies by Robbins et al. that investi-gated differences between barefoot and shod running wereperformed under static conditions and not during the actionof running itself.58,60 Similarly, many referenced barefootrunning studies were performed in a controlled laboratorysimulation that likely altered gait and running conditionscompared with a more realistic outside environment. Themain limitation in barefoot running research is that no clin-ical studies are available to support or reject any performanceor injury prevention benefits.46 In addition, there are also nostudies that directly compare footwear-based orthotics withbarefoot running to investigate ankle overuse injuries stem-ming from impaired mechanical control.10,18,61
Another limitation of the literature is that barefootrunning has not been tested in individuals with estab-lished foot pathology, deformity, or running-related injuries,such as plantar fasciitis, tibial stress syndrome, Achillestendinopathy, and iliotibial band syndrome.1 Alterations infoot alignment play a major role in the incidence of stressfractures and have been shown to be more prevalent inpatients with forefoot and hindfoot varus.29,36 It is unknownwhat effect that increased intrinsic musculature and plan-tarflexion activation during barefoot running will have onpatients susceptible to overuse injuries.
CONCLUSIONS
Changes in gait pattern from hindfoot to forefoot strikewith a reduction in peak ground forces with barefootrunning are the main findings that can be supported onthe basis of a review of the literature. Secondary claimsof increased proprioception and coordinative strategy alongwith improved intrinsic foot muscle strength have supportingevidence that is less strong and limited by study design andmethodology. Although there are promising results showingpotential benefits of barefoot running, many of the claimssupporting its use are anecdotal and individual opinionswithout scientific support. There are numerous questions thatmust be investigated before any conclusions can be made foror against established footwear running.
Analysis of barefoot running from an evolutionary perspec-tive has provided key insights into the biomechanicalbasis of running. However, this research has also raised amyriad of questions regarding running anatomy, gait, biome-chanics, performance, and injury pathogenesis that needto be addressed in the future. It is important to instructpatients interested in barefoot running that a proper adap-tation program is necessary and that barefoot running cannotcorrect preexisting pathology, biomechanical abnormalities,or other medical issues. The potential risks and benefits ofbarefoot running should be explained to patients, taking intoaccount their individual medical history, functional needs,and goals. Prospective, randomized, controlled short- and
Copyright 2012 by the American Orthopaedic Foot & Ankle Society
at UNIVERSITAETBIBLIOTHEK on May 21, 2014fai.sagepub.comDownloaded from

Foot & Ankle International/Vol. 33, No. 9/September 2012 BAREFOOT RUNNING 793
long-term studies are needed to elucidate the proposed clin-ical benefits and risks of barefoot running. Whether provenbeneficial or harmful to overall foot and ankle health, itis important for physicians to be aware of the scientificevidence behind barefoot running in order to better educateand guide patients regarding running exercise activity andimplementation.
REFERENCES
1. Anderson, RB; Hunt, KJ; McCormick, JJ: Management of commonsports-related injuries about the foot and ankle. J Am Acad Orthop Surg.18(9):546–556, 2010. http://dx.doi.org/10.1053/j.otsm.2009.12.001
2. Baxter, DE; Zingas, C: The foot in running. J Am Acad Orthop Surg.3(3):136–145, 1995.
3. Borowski, LA; Yard, EE; Fields, SK; Comstock, RD: The epidemi-ology of US high school basketball injuries, 2005–2007. Am J SportsMed. 36(12):2328–2335, 2008. http://dx.doi.org/10.1177/0363546508322893
4. Bramble, DM; Lieberman, DE: Endurance running and the evolutionof Homo. Nature. 432(7015):345–352, 2004. http://dx.doi.org/10.1038/nature03052
5. Bruggemann, GP; Potthast, W: Effect of increased mechanical stimulion foot muscles functional capacity. ASB 29th Annual Meeting,Cleveland, OH, 2005.
6. Burkett, LN; Kohrt, WM; Buchbinder, R: Effects of shoes and footorthotics on VO2 and selected frontal plane knee kinematics. Med SciSports Exerc. 17(1):158–163, 1985.
7. Butler, RJ; Davis, IS; Hamill, J: Interaction of arch type and footwearon running mechanics. Am J Sports Med. 34(12):1998–2005, 2006.http://dx.doi.org/10.1177/0363546506290401
8. Catlin, MJ; Dressendorfer, RH: Effect of shoe weight on the energycost of running. Med Sci Sports Exerc. 11:80, 1979.
9. Clinghan, R; Arnold, GP; Drew, TS; Cochrane, LA; Abboud, RJ:Do you get value for money when you buy an expensive pair of runningshoes? Br J Sports Med. 42(3):189–193, 2008. http://dx.doi.org/10.1136/bjsm.2007.038844
10. Collins, N; Bisset, L; McPoil, T; Vicenzino, B: Foot orthoses in lowerlimb overuse conditions: a systematic review and meta-analysis. FootAnkle Int. 28(3):396–412, 2007. http://dx.doi.org/10.3113/FAI.2007.0396
11. De Wit, B; De Clercq, D; Aerts, P: Biomechanical analysis of thestance phase during barefoot and shod running. J Biomech. 33(3):269–278, 2000. http://dx.doi.org/10.1016/S0021-9290(99)00192-X
12. Divert, C; Baur, H; Mornieux, G; Mayer, F; Belli, A: Stiffnessadaptations in shod running. J Appl Biomech. 21(4):311–321, 2005.
13. Divert, C; Mornieux, G; Baur, H; Mayer, F; Belli, A: Mechanicalcomparison of barefoot and shod running. Int J Sports Med. 26(7):593–598, 2005. http://dx.doi.org/10.1055/s-2004-821327
14. Divert, C; Mornieux, G; Freychat, P, et al.: Barefoot-shod runningdifferences: shoe or mass effect? Int J Sports Med. 29(6):512–518,2008. http://dx.doi.org/10.1055/s-2007-989233
15. Edwards, WB; Taylor, D; Rudolphi, TJ; Gillette, JC; Derrick,TR: Effects of stride length and running mileage on a probabilisticstress fracture model. Med Sci Sports Exerc. 41(12):2177–2184, 2009.http://dx.doi.org/10.1249/MSS.0b013e3181a984c4
16. Garrick, JG; Requa, RK: The epidemiology of foot and ankle injuriesin sports. Clin Sports Med. 7(1):29–36, 1988.
17. Giuliani, J; Masini, B; Alitz, C; Owens, BD: Barefoot-simulatingfootwear associated with metatarsal stress injury in 2 runners.Orthopedics. 34(7):e320–323, 2011.
18. Gross, MT; Byers, JM; Krafft, JL; Lackey, EJ; Melton, KM:The impact of custom semirigid foot orthotics on pain and disability
for individuals with plantar fasciitis. J Orthop Sports Phys Ther.32(4):149–157, 2002.
19. Hanson, NJ; Berg, K; Deka, P; Meendering, JR; Ryan, C:Oxygen cost of running barefoot vs. running shod. Int J Sports Med.32(6):401–406, 2011. http://dx.doi.org/10.1055/s-0030-1265203
20. Hardin, EC; van den Bogert, AJ; Hamill, J: Kinematic adaptationsduring running: effects of footwear, surface, and duration. Med SciSports Exerc. 36(5):838–844, 2004.
21. Hasegawa, H; Yamauchi, T; Kraemer, WJ: Foot strike patterns ofrunners at the 15-km point during an elite-level half marathon. J StrengthCond Res. 21(3):888–893, 2007. http://dx.doi.org/10.1519/R-22096.1
22. Hennig, EM; Sterzing, T: Sensitivity mapping of the human foot:thresholds at 30 skin locations. Foot Ankle Int. 30(10):986–991, 2009.http://dx.doi.org/10.3113/FAI.2009.0986
23. Hootman, JM; Dick, R; Agel, J: Epidemiology of collegiate injuriesfor 15 sports: summary and recommendations for injury preventioninitiatives. J Athl Train. 42(2):311–319, 2007.
24. Hreljac, A: Impact and overuse injuries in runners. Med Sci SportsExerc. 36(5):845–849, 2004.
25. Jacobs, SJ; Berson, BL: Injuries to runners: a study of entrants to a10,000 meter race. Am J Sports Med. 14(2):151–155, 1986. http://dx.doi.org/10.1177/036354658601400211
26. James, SL: Running injuries to the knee. J Am Acad Orthop Surg.3(6):309–318, 1995.
27. Kadambande, S; Khurana, A; Debnath, U: Comparative anthropo-metric analysis of shod and unshod feet. Foot. 16(4):188–191, 2006.http://dx.doi.org/10.1016/j.foot.2006.06.001
28. Kalin, VX; Denoth, J; Stacoff, A; Stussi, E: [Running injuries andrunning shoe construction: demonstration of possible correlations].Sportverletz Sportschaden. 2(2):80–85, 1988.
29. Kaufman, KR; Brodine, SK; Shaffer, RA; Johnson, CW; Cullison,TR: The effect of foot structure and range of motion on musculoskeletaloveruse injuries. Am J Sports Med. 27(5):585–593, 1999.
30. Ker, RF; Bennett, MB; Bibby, SR; Kester, RC; Alexander, RM:The spring in the arch of the human foot. Nature. 325(7000):147–149,1987. http://dx.doi.org/10.1038/325147a0
31. Kerr, R; Arnold, GP; Drew, TS; Cochrane, LA; Abboud, RJ: Shoesinfluence lower limb muscle activity and may predispose the wearerto lateral ankle ligament injury. J Orthop Res. 27(3):318–324, 2009.http://dx.doi.org/10.1002/jor.20744
32. Kerrigan, DC; Franz, JR; Keenan, GS; Dicharry, J; DellaCroce, U; Wilder, RP: The effect of running shoes on lowerextremity joint torques. PM R. 1(12):1058–1063, 2009. http://dx.doi.org/10.1016/j.pmrj.2009.09.011
33. Komi, PV; Gollhofer, A; Schmidtbleicher, D; Frick, U: Interactionbetween man and shoe in running: considerations for a morecomprehensive measurement approach. Int J Sports Med. 8(3):196–202,1987. http://dx.doi.org/10.1055/s-2008-1025655
34. Kong, PW; Candelaria, NG; Smith, DR: Running in new and wornshoes: a comparison of three types of cushioning footwear. Br JSports Med. 43(10):745–749, 2009. http://dx.doi.org/10.1136/bjsm.2008.047761
35. Koplan, JP; Powell, KE; Sikes, RK; Shirley, RW; Campbell,CC: An epidemiologic study of the benefits and risks of running.JAMA. 248(23):3118–3121, 1982. http://dx.doi.org/10.1001/jama.248.23.3118
36. Korpelainen, R; Orava, S; Karpakka, J; Siira, P; Hulkko, A: Riskfactors for recurrent stress fractures in athletes. Am J Sports Med.29(3):304–310, 2001.
37. Krabak, BJ; Hoffman, MD; Millet, GY; Chimes, GP: Barefootrunning. PM R. 3(12): 1142–1149, 2011.
38. Kurz, MJ; Stergiou, N: Does footwear affect ankle coordinationstrategies? J Am Podiatr Med Assoc. 94(1):53–58, 2004.
39. Kurz, MJ; Stergiou, N: The spanning set indicates that variabilityduring the stance period of running is affected by footwear. Gait
Copyright 2012 by the American Orthopaedic Foot & Ankle Society
at UNIVERSITAETBIBLIOTHEK on May 21, 2014fai.sagepub.comDownloaded from

794 HSU Foot & Ankle International/Vol. 33, No. 9/September 2012
Posture. 17(2):132–135, 2003. http://dx.doi.org/10.1016/S0966-6362(02)00064-4
40. Kurz, MJ; Stergiou, N; Blanke, D: Spanning set defines variabilityin locomotive patterns. Med Biol Eng Comput. 41(2):211–214, 2003.http://dx.doi.org/10.1007/BF02344891
41. Lavery, LA; Walker, SC; Harkless, LB; Felder-Johnson, K: Infectedpuncture wounds in diabetic and nondiabetic adults. Diabetes Care.18(12):1588–1591, 1995. http://dx.doi.org/10.2337/diacare.18.12.1588
42. Lephart, SM; Pincivero, DM; Giraldo, JL; Fu, FH: The roleof proprioception in the management and rehabilitation of athleticinjuries. Am J Sports Med. 25(1):130–137, 1997. http://dx.doi.org/10.1177/036354659702500126
43. Liebeman, DE: What we can learn about running from barefootrunning: an evolutionary medical perspective. Exerc Sport Sci Rev.Epub ahead of print, 2012. http://dx.doi.org/10.1097/JES.0b013e31824ab210
44. Lieberman, DE; Venkadesan, M; Werbel, WA, et al.: Foot strikepatterns and collision forces in habitually barefoot versus shod runners.Nature. 463(7280):531–535, 2010. http://dx.doi.org/10.1038/nature08723
45. Macera, CA; Pate, RR; Powell, KE, et al.: Predicting lower-extremityinjuries among habitual runners. Arch Intern Med. 149(11):2565–2568,1989. http://dx.doi.org/10.1001/archinte.149.11.2565
46. Nigg, B: Biomechanical considerations on barefoot movement andbarefoot shoe concepts. Footwear Sci. 1(2):73–79, 2009. http://dx.doi.org/10.1080/19424280903204036
47. Ogon, M; Aleksiev, AR; Spratt, KF; Pope, MH; Saltzman, CL:Footwear affects the behavior of low back muscles when jogging. IntJ Sports Med. 22(6):414–419, 2001. http://dx.doi.org/10.1055/s-2001-16240
48. Perl, DP; Daoud, AI; Lieberman, DE: Effects of footwear and striketype on running economy. Med Sci Sports Exerc. Epub ahead of print,2012. http://dx.doi.org/10.1249/MSS.0b013e318247989e
49. Rao, UB; Joseph, B: The influence of footwear on the prevalence of flatfoot. A survey of 2300 children. J Bone Joint Surg Br. 74(4):525–527,1992.
50. Richards, CE; Magin, PJ; Callister, R: Is your prescription of distancerunning shoes evidence-based? Br J Sports Med. 43(3):159–162, 2009.http://dx.doi.org/10.1136/bjsm.2008.046680
51. Ristolainen, L; Heinonen, A; Turunen, H, et al.: Type of sport isrelated to injury profile: a study on cross country skiers, swimmers,long-distance runners and soccer players. A retrospective 12-monthstudy. Scand J Med Sci Sports. 20(3):384–393, 2010. http://dx.doi.org/10.1111/j.1600-0838.2009.00955.x
52. Robbins, S; Gouw, GJ; McClaran, J: Shoe sole thickness andhardness influence balance in older men. J Am Geriatr Soc. 40(11):1089–1094, 1992.
53. Robbins, S; Gouw, GJ; McClaran, J; Waked, E: Protective sensationof the plantar aspect of the foot. Foot Ankle. 14(6):347–352, 1993.
54. Robbins, S; Waked, E: Factors associated with ankle injuries.Preventive measures. Sports Med. 25(1):63–72, 1998.
55. Robbins, S; Waked, E; Gouw, GJ; McClaran, J: Athletic footwearaffects balance in men. Br J Sports Med. 28(2):117–122, 1994. http://dx.doi.org/10.1136/bjsm.28.2.117
56. Robbins, S; Waked, E; McClaran, J: Proprioception and stability:foot position awareness as a function of age and footwear. Age Ageing.24(1):67–72, 1995. http://dx.doi.org/10.1093/ageing/24.1.67
57. Robbins, S; Waked, E; Rappel, R: Ankle taping improvesproprioception before and after exercise in young men. Br J SportsMed. 29(4):242–247, 1995. http://dx.doi.org/10.1136/bjsm.29.4.242
58. Robbins, SE; Gouw, GJ: Athletic footwear and chronic overloading.A brief review. Sports Med. 9(2):76–85, 1990.
59. Robbins, SE; Gouw, GJ; Hanna, AM: Running-related injuryprevention through innate impact-moderating behavior. Med Sci SportsExerc. 21(2):130–139, 1989. http://dx.doi.org/10.1249/00005768-198904000-00004
60. Robbins, SE; Hanna, AM: Running-related injury prevention throughbarefoot adaptations. Med Sci Sports Exerc. 19(2):148–156, 1987.http://dx.doi.org/10.1249/00005768-198704000-00014
61. Roos, E; Engstrom, M; Soderberg, B: Foot orthoses for the treatmentof plantar fasciitis. Foot Ankle Int. 27(8):606–611, 2006.
62. Rothschild, CE: Primitive running: a survey analysis of runners’interest, participation, and implementation. J Strength Cond Res. Epubahead of print, 2011.
63. Sachithanandam, V; Joseph, B: The influence of footwear on theprevalence of flat foot. A survey of 1846 skeletally mature persons. JBone Joint Surg Br. 77(2):254–257, 1995.
64. Shakoor, N; Block, JA: Walking barefoot decreases loading onthe lower extremity joints in knee osteoarthritis. Arthritis Rheum.54(9):2923–2927, 2006. http://dx.doi.org/10.1002/art.22123
65. Squadrone, R; Gallozzi, C: Biomechanical and physiologicalcomparison of barefoot and two shod conditions in experienced barefootrunners. J Sports Med Phys Fitness. 49(1):6–13, 2009.
66. Stacoff, A; Steger, J; Stussi, E; Reinschmidt, C: Lateral stability insideward cutting movements. Med Sci Sports Exerc. 28(3):350–358,1996. http://dx.doi.org/10.1097/00005768-199603000-00010
67. Staheli, LT: Shoes for children: a review. Pediatrics. 88(2):371–375,1991.
68. van Mechelen, W: Running injuries. A review of the epidemiologicalliterature. Sports Med. 14(5):320–335, 1992.
69. Van Middelkoop, M; Kolkman, J; Van Ochten, J; Bierma-Zeinstra,SM; Koes, B: Prevalence and incidence of lower extremity injuries inmale marathon runners. Scand J Med Sci Sports. 18(2):140-144, 2008.http://dx.doi.org/10.1111/j.1600-0838.2007.00683.x
70. Waddington, G; Adams, R: Football boot insoles and sensitivity toextent of ankle inversion movement. Br J Sports Med. 37(2):170–174,2003. http://dx.doi.org/10.1136/bjsm.37.2.170
71. Walter, SD; Hart, LE; McIntosh, JM; Sutton, JR: The Ontario cohortstudy of running-related injuries. Arch Intern Med. 149(11):2561–2564,1989. http://dx.doi.org/10.1001/archinte.149.11.2561
72. Webb, P; Saris, WH; Schoffelen, PF; Van Ingen Schenau, GJ; TenHoor, F: The work of walking: a calorimetric study. Med Sci SportsExerc. 20(4):331–337, 1988. http://dx.doi.org/10.1249/00005768-198808000-00002
73. Wolf, S; Simon, J; Patikas, D, et al.: Foot motion in children shoes:a comparison of barefoot walking with shod walking in conventionaland flexible shoes. Gait Posture. 27(1):51–59, 2008. http://dx.doi.org/10.1016/j.gaitpost.2007.01.005
Copyright 2012 by the American Orthopaedic Foot & Ankle Society
at UNIVERSITAETBIBLIOTHEK on May 21, 2014fai.sagepub.comDownloaded from