Embed Size (px)
Citation preview

International Journal of Pediatric Otorhinolaryngology 74 (2010) 1432–1434
Case report
Tracheal foreign body after laser supraglottoplasty: A hidden but riskycomplication of an aluminum foil tape-wrapped endotracheal tube
Wen-Jue Soong a,b,*, Yu-Shen Lee a,b, Yen-Hui Soong c, Pei-Chen Tsao a,b, Chia-Feng Yang a,b,Mei-Ji Jeng a,b, Yu-Yun Peng a,b
a Department of Pediatrics, Children’s Medical Center, Taipei Veterans General Hospital, Taiwan, ROCb Department of Pediatrics, School of Medicine, Institute of Emergency and Critical Care Medicines, National Yang-Ming University, Taipei, Taiwan, ROCc School of Medicine, Michigan State University College of Human Medicine, Lansing, MI, USA
A R T I C L E I N F O
Article history:
Received 18 June 2010
Received in revised form 26 August 2010
Accepted 28 August 2010
Available online 8 October 2010
Keywords:
Laser
Airway fire
Aluminum foil tape
Foreign body
A B S T R A C T
Wrapping of the endotracheal tube with aluminum foil tape can prevent laser-beam-induced ignition of
the tube during laryngoplasty. However, this modified endotracheal tube may pose complications. Two
newborn infants had a portion of the foil tape trapped in their trachea after extubation from laser
supraglottoplasty. One infant was totally asymptomatic. The other infant‘s symptoms were masked by
the concurrent tracheomalacia. Both residual tapes were radiolucent on chest radiographs. Flexible
endoscopy was the suitable and safe modality for an accurate diagnosis and immediate retrieval of the
residual tapes in one session.
� 2010 Elsevier Ireland Ltd. All rights reserved.
Contents lists available at ScienceDirect
International Journal of Pediatric Otorhinolaryngology
journa l homepage: www.e lsev ier .com/ locate / i jpor l
1. Introduction
Carbon dioxide (CO2) laser surgery has been the most effectiveand appropriate treatment for severe laryngomalacia (LM) in thepast two decades [1–4]. However, despite continued improve-ments in CO2 laser technology and surgical techniques, laser-related complications still occur [5,6]. The traditional polyvinylchloride (PVC) endotracheal tube (ET) is susceptible to CO2 laserbeam and the most devastating complication during laser is anairway fire. That is the laser could pass through the ET lumen andignite the oxygen–anesthetic gas mixture, which, in turn, may burnand injure the infant’s delicate airway [7,8]. This has beenextensively studied, and alternatives have been developed toprotect the ET from laser energy [9–11].
The most effective and commonly used method in clinicalpractice involves wrapping the ET with a thin aluminum foil tape;its reflective surface can protect the ET from the laser beam [10–13]. However, this wrapped ET also poses potential risks [14]. Thisarticle describes, what to our knowledge are, the first two reportedcases of infants having a piece of aluminum tape retained in theirtracheas after extubation from laser supraglottoplasty. Theirclinical presentations were similar to underlying LM and
* Corresponding author at: Department of Pediatrics, Children’s Medical Center,
Taipei Veterans General Hospital, 201, Section 2, Shih-Pai Road, Taipei 112, Taiwan,
ROC. Tel.: +886 228725134; fax: +886 228739019.
E-mail address: [email protected] (W.-J. Soong).
0165-5876/$ – see front matter � 2010 Elsevier Ireland Ltd. All rights reserved.
doi:10.1016/j.ijporl.2010.08.019
tracheomalacia. Flexible endoscopy is the reliable modality foran accurate diagnosis and immediate retrieval of the residual tapesat bedside.
2. Case reports
2.1. Case 1
A 3-month-old male infant, with a body weight of 4.1 kg,received CO2 laser supraglottoplasty for treatment of severe LMand failure to thrive. General anesthesia was conducted with 100%oxygen and 1% sevoflurane administered via a T-piece circuit.Before surgery, an uncuffed PVC ET (ID 3.5 mm) was carefullywrapped with layers of thin aluminum tape spiraled around thetube. The wrapped ET was orally inserted to a depth of 10 cm. Aftersurgery, the ET was removed in the operation room and the infantwas sent back to the neonatal intensive care unit (NICU) with arespiratory support of nasal prong continuous positive airwaypressure. On the second day, the infant’s breathing pattern showeda little improvement; that is, with less noises and retractions thanbefore. Twenty hours after ET extubation, for suspicion ofaspiration after episodes of vomiting and choking, a chestradiogram was taken and revealed bilateral pulmonary infiltrationand a normal tracheal column with no visible foreign bodies(Fig. 1). It showed mild, but not significant, bilateral hyperinflationwith flattening of the diaphragms when compared to the pre-procedure film. The infant still breathed comfortably without any
[(Fig._1)TD$FIG]
Fig. 1. The chest film shows bilateral infiltrations and hyperinflation of lung with
flattening of the diaphragms. The tracheal column is clear with no visible foreign
body.
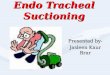
[(Fig._3)TD$FIG]
Fig. 3. A single layer of aluminum foil encircled over the inner mucosa of the trachea
and the central lumen is quite patent.
W.-J. Soong et al. / International Journal of Pediatric Otorhinolaryngology 74 (2010) 1432–1434 1433
difficulty. To evaluate the post-ablated condition of the laryngealtissue, a flexible endoscopy (OD 3.5 mm) was performed.
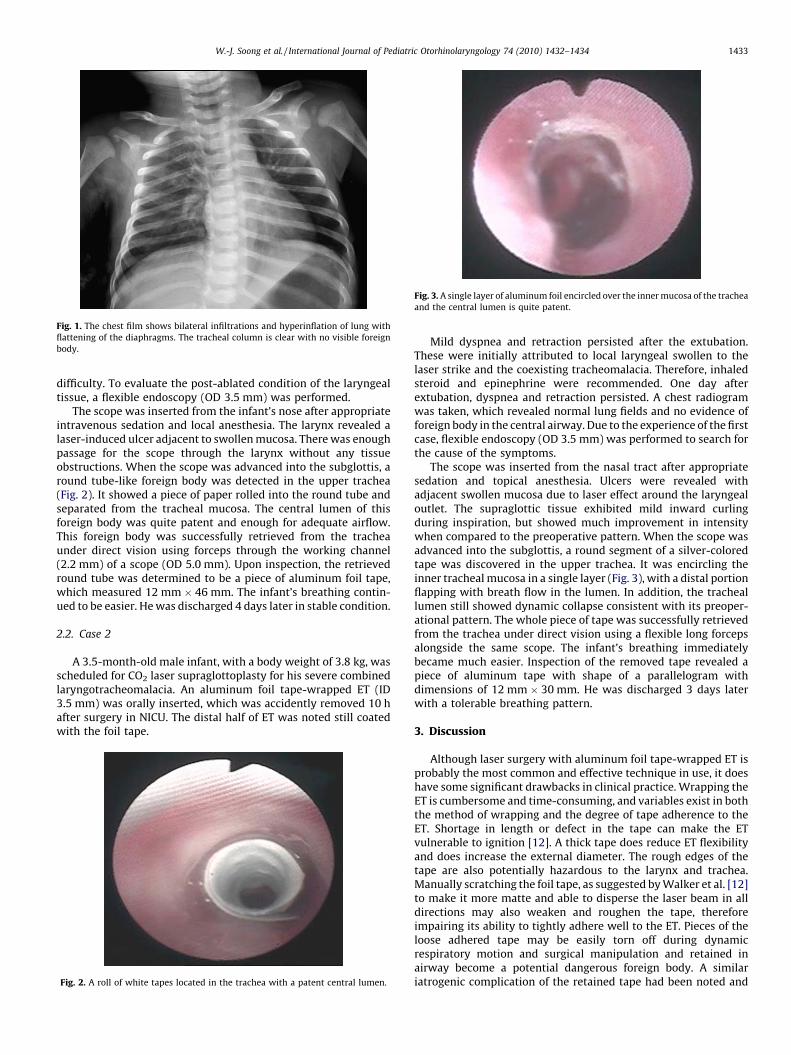
The scope was inserted from the infant’s nose after appropriateintravenous sedation and local anesthesia. The larynx revealed alaser-induced ulcer adjacent to swollen mucosa. There was enoughpassage for the scope through the larynx without any tissueobstructions. When the scope was advanced into the subglottis, around tube-like foreign body was detected in the upper trachea(Fig. 2). It showed a piece of paper rolled into the round tube andseparated from the tracheal mucosa. The central lumen of thisforeign body was quite patent and enough for adequate airflow.This foreign body was successfully retrieved from the tracheaunder direct vision using forceps through the working channel(2.2 mm) of a scope (OD 5.0 mm). Upon inspection, the retrievedround tube was determined to be a piece of aluminum foil tape,which measured 12 mm � 46 mm. The infant’s breathing contin-ued to be easier. He was discharged 4 days later in stable condition.
2.2. Case 2
A 3.5-month-old male infant, with a body weight of 3.8 kg, wasscheduled for CO2 laser supraglottoplasty for his severe combinedlaryngotracheomalacia. An aluminum foil tape-wrapped ET (ID3.5 mm) was orally inserted, which was accidently removed 10 hafter surgery in NICU. The distal half of ET was noted still coatedwith the foil tape.[(Fig._2)TD$FIG]
Fig. 2. A roll of white tapes located in the trachea with a patent central lumen.
Mild dyspnea and retraction persisted after the extubation.These were initially attributed to local laryngeal swollen to thelaser strike and the coexisting tracheomalacia. Therefore, inhaledsteroid and epinephrine were recommended. One day afterextubation, dyspnea and retraction persisted. A chest radiogramwas taken, which revealed normal lung fields and no evidence offoreign body in the central airway. Due to the experience of the firstcase, flexible endoscopy (OD 3.5 mm) was performed to search forthe cause of the symptoms.
The scope was inserted from the nasal tract after appropriatesedation and topical anesthesia. Ulcers were revealed withadjacent swollen mucosa due to laser effect around the laryngealoutlet. The supraglottic tissue exhibited mild inward curlingduring inspiration, but showed much improvement in intensitywhen compared to the preoperative pattern. When the scope wasadvanced into the subglottis, a round segment of a silver-coloredtape was discovered in the upper trachea. It was encircling theinner tracheal mucosa in a single layer (Fig. 3), with a distal portionflapping with breath flow in the lumen. In addition, the tracheallumen still showed dynamic collapse consistent with its preoper-ational pattern. The whole piece of tape was successfully retrievedfrom the trachea under direct vision using a flexible long forcepsalongside the same scope. The infant’s breathing immediatelybecame much easier. Inspection of the removed tape revealed apiece of aluminum tape with shape of a parallelogram withdimensions of 12 mm � 30 mm. He was discharged 3 days laterwith a tolerable breathing pattern.
3. Discussion
Although laser surgery with aluminum foil tape-wrapped ET isprobably the most common and effective technique in use, it doeshave some significant drawbacks in clinical practice. Wrapping theET is cumbersome and time-consuming, and variables exist in boththe method of wrapping and the degree of tape adherence to theET. Shortage in length or defect in the tape can make the ETvulnerable to ignition [12]. A thick tape does reduce ET flexibilityand does increase the external diameter. The rough edges of thetape are also potentially hazardous to the larynx and trachea.Manually scratching the foil tape, as suggested by Walker et al. [12]to make it more matte and able to disperse the laser beam in alldirections may also weaken and roughen the tape, thereforeimpairing its ability to tightly adhere well to the ET. Pieces of theloose adhered tape may be easily torn off during dynamicrespiratory motion and surgical manipulation and retained inairway become a potential dangerous foreign body. A similariatrogenic complication of the retained tape had been noted and

W.-J. Soong et al. / International Journal of Pediatric Otorhinolaryngology 74 (2010) 1432–14341434
removed from the tracheal stoma in a 12-year-old boy during laserlaryngeal surgery. [14]
Normally, after laser supraglottoplasty and ET extubation, noisybreathing and dyspnea may still last for a few days [1–5]. However,the iatrogenic complications, such as retained tape in our twocases, should need to be kept in mind before considering the otherdifferential diagnosis of laryngeal swelling to the ET or the laser,residual LM, or coexisting lesions, etc. Once a piece of tape isdislodged in the trachea, it may not cause respiratory symptomsinitially, as exemplified in our two cases. Case 1 was totallyasymptomatic because the retained foil tube was well alignedlongitudinally in the tracheal lumen without impeding thebreathing flow. Although in chest film, the infiltrations, hyperin-flation, and flattening diaphragms may suggest a presence ofairway foreign body, however, the effect of partial airwayobstruction of the swollen larynx or residual LM may also showsame picture. Case 2 even had demonstrated some symptoms butboth clinical presentation and chest film might easily mask by thealready known underlying tracheomalacia. Fortunately, bothretained tapes were incidentally discovered and successfullyretrieved in time by bedside flexible endoscopy.
The aluminum foil tape that we used, the most commerciallyavailable type, is radiolucent. It is potentially dangerous whenparts of it are accidentally lost in the trachea. Plain radiographalone cannot detect its presence. Flexible airway endoscopy isprobably the only convenient bedside modality that allowsclinicians to make correct diagnosis and commit immediatetreatment in one session. Otherwise, this ‘‘hidden’’ and riskyiatrogenic complication may be overlooked or lead to a misdiag-nosis, causing the use of more unnecessary medical managementsuch as inhalation therapy, ET reintubation, positive pressuresupport, or even tracheostomy, which may further develop anintractable respiratory course and hazardous events.
Therefore, in light of these two cases, we now stronglyrecommend that in circumstances where foreign bodies, such asET, instrument and materials, are put into the airway duringanesthesia or intervention that should be radiopaque and carefully
examined after removal at the end of the procedure; ensuring thatit has been removed in entirety. The wrapping tape should also besmooth surface, good adherence and durability, measure andrecord the length before and after used. Upon any suspicion ofmissing parts, a complete airway endoscopy is mandatory.
References
[1] K.S. Lee, B.N. Chen, C.C. Yang, Y.C. Chen, CO2 laser supraglottoplasty for severelaryngomalacia: a study of symptomatic improvement, Int. J. Pediatr. Otorhinolar-yngol. 71 (2007) 889–895.
[2] A.D. Whymark, W.A. Clement, H. Kubba, N.K. Geddes, Laser epiglottopexy forlaryngomalacia—10 years’ experience in the West of Scotland, Arch. Otolaryngol.Head Neck Surg. 132 (2006) 978–982.
[3] S.C. Toynton, M.W. Saunders, C.M. Bailey, Aryepiglottoplasty for laryngomalacia:100 consecutive cases, J. Laryngol. Otol. 115 (2001) 35–38.
[4] O. Merrot, P. Fayoux, F. Vachin, D. Chevalier, A. Desaulty, Severe laryngomalacia:surgical indication and results in 33 patients, Ann. Otolaryngol. Chir. Cervicofac.121 (2004) 14–21.
[5] F. Denoyelle, M. Mondain, N. Gresillon, G. Roger, F. Franck Chaudre, E.N. Gar-abedian, Failures and complications of supraglottoplasty in children, Arch. Oto-laryngol. Head Neck Surg. 129 (2003) 1077–1080.
[6] M.P. Fried, A survey of the complications of laser laryngoscopy, Arch. Otolaryngol.110 (1984) 31–34.
[7] J.C. Snow, M.L. Norton, T.S. Saluja, A.E. Estanislao, Fire hazard during CO2 lasermicrosurgery on the larynx and trachea, Anesth. Analg. 55 (1976) 146–147.
[8] H.C. Lai, S.E. Juang, T.J. Liu, W.M. Ho, Fires of endotracheal tubes of three differentmaterials during carbon dioxides laser surgery, Acta Anaesthesiol. Sin. China 40(2002) 47–51.
[9] R.H. Ossoff, Laser safety in otolaryngology—head and neck surgery: anesthetic andeducational considerations for laryngeal surgery, Laryngoscope 99 (Suppl.) (1989)1–26.
[10] K.F. Patel, J.N. Hicks, Prevention of fire hazards associated with the use of carbondioxide lasers, Anesth. Analg. 60 (1981) 885–888.
[11] C.A. Hirshman, J. Smith, Indirect ignition of the endotracheal tube during carbondioxide laser surgery, Arch. Otolaryngol. Head Neck Surg. 118 (1980) 722–724.
[12] P. Walker, A. Temperley, S. Thelfo, A. Hazelgrove, Avoidance of laser ignition ofendotracheal tubes by wrapping in aluminium foil tape, Anaesth. Intensive Care32 (2004) 108–112.
[13] C.H. Kuo, P.H. Tan, J.J. Chen, C.H. Peng, C.C. Lee, H.C. Chung, et al., Endotrachealtube fires during carbon dioxide laser surgery on the larynx—a case report, ActaAnaesthesiol. Sin. 39 (2001) 53–56.
[14] C.S. Kaeder, C.A. Hirshman, Acute airway obstruction: a complication of alumi-num tape wrapping of tracheal tubes in laser surgery, Can. Anesth. Soc. J. 26(1979) 138–139.