-
8/3/2019 TRALI - TUCSON
1/46
TRANSFUSION RELATED ACUTE
LUNG INJURY
TRANSFUSION RELATED ACUTE
LUNG INJURYA. Sergio Torloni MD
Assistant Medical Director
United Blood Services
Scottsdale AZ
A. Sergio Torloni MD
Assistant Medical Director
United Blood Services
Scottsdale AZ
Medical Director
Transfusion Services / Stem Cell Collection
Therapeutic Apheresis
Mayo Clinic Hospital
Phoenix AZ
[email protected]
-
8/3/2019 TRALI - TUCSON
2/46
What is T.R.A.L.I ?What is T.R.A.L.I ?
Severe respiratory compromise during transfusion.
- severe hypoxemia + non-cardiogenic pulmonary edema
Usually within 2 hours of tx (may be upto 4-6 hours)
TRALI IS A DIAGNOSIS OF EXCLUSION !
Severe respiratory compromise during transfusion.
- severe hypoxemia + non-cardiogenic pulmonary edema
Usually within 2 hours of tx (may be upto 4-6 hours)
TRALI IS A DIAGNOSIS OF EXCLUSION !
A SEVERE REACTION TO TRANSFUSION OF BLOOD PRODUCTSA SEVERE
REACTION TO TRANSFUSION OF BLOOD PRODUCTS
-
8/3/2019 TRALI - TUCSON
3/46
-
8/3/2019 TRALI - TUCSON
4/46
-
8/3/2019 TRALI - TUCSON
5/46
TRALI: What is it ?TRALI: What is it ?Acute respiratory distress
occurring 1 2 hours after transfusion
of plasma containing blood products
Acute respiratory distress occurring 1 2 hours after
transfusion
of plasma containing blood products
Symptoms %
Respiratory Distress 76
Hypotension 15
Hypertension 15
Symptoms %
Respiratory Distress 76
Hypotension 15
Hypertension 15
N=46*
*Popovsky & Haley, Immunohematology, 2000; 16** Popovsky
& Moore, Transfusion, 1985
Incidence : 1 in 5000 tx (Mayo Clinic Study)**
Grossly Under diagnosed !
-
8/3/2019 TRALI - TUCSON
6/46
TRANSFUSION RELATED ACUTE LUNG INJURY
(T.R.A.L.I)
TRANSFUSION RELATED ACUTE LUNG INJURY
(T.R.A.L.I)
Male / Female ratio = 1:1
Age : No age preference
Male / Female ratio = 1:1
Age : No age preference
Incidence: 0.02% of all units or 0.16% of all transfused
patients*Incidence: 0.02% of all units or 0.16% of all transfused
patients*
Very Likely Under diagnosedVery Likely Under diagnosed
AKA : Allergic Pulmonary Edema
Pulmonary Hypersensitivity reaction
AKA : Allergic Pulmonary Edema
Pulmonary Hypersensitivity reaction
Popovsky & Moore, Transfusion 25:573-7, 1985
-
8/3/2019 TRALI - TUCSON
7/46
TRALI: Common SymptomsTRALI: Common Symptoms
Acute respiratory distress
Hypoxemia
Acute pulmonary edema
Fever ( 1 - 2 C elevation)
Pulmonary edema usually resolves within 96 hours
6 10% of cases result in death
Acute respiratory distress
Hypoxemia
Acute pulmonary edema
Fever ( 1 - 2 C elevation)
Pulmonary edema usually resolves within 96 hours
6 10% of cases result in death
Likely Mechanism is Immune mediated
Other mechanisms may exist (Lipid Mediator PAF like substance
that primes leukocytes)
Second Hit Theory (Leukocytes already primed by previous injury
i.e. hypoxia, sepsis, cytokine tx
Likely Mechanism is Immune mediated
Other mechanisms may exist (Lipid Mediator PAF like substance
that primes leukocytes)
Second Hit Theory (Leukocytes already primed by previous injury
i.e. hypoxia, sepsis, cytokine tx
-
8/3/2019 TRALI - TUCSON
8/46
TRANSFUSION RELATED ACUTE LUNG INJURY
(T.R.A.L.I)
TRANSFUSION RELATED ACUTE LUNG INJURY
(T.R.A.L.I)
Differential DxDifferential Dx
Pulmonary embolism
Circulatory overload Shock
Bacterial Contamination (Sepsis)
Hemolytic Transfusion Reaction Anaphylaxis
Pulmonary embolism
Circulatory overload Shock
Bacterial Contamination (Sepsis)
Hemolytic Transfusion Reaction Anaphylaxis
Incidence : 1 in 5000 tx (Mayo Clinic Study)*
Grossly Under diagnosed !
*Popovsky & Moore, Transfusion 1985
-
8/3/2019 TRALI - TUCSON
9/46
TRANSFUSION RELATED ACUTE LUNG INJURY
(T.R.A.L.I)
TRANSFUSION RELATED ACUTE LUNG INJURY
(T.R.A.L.I)
Causes:Causes:
Pre-formed anti white cell antibodies in donor plasma
Donor is usually a multiparous female
Pre-formed anti white cell antibodies in donor plasma
Donor is usually a multiparous female
Anti-HLA ( A, B, DR)
Anti Neutrophil (NA-1, NA-2, NB, 5b)
Sometimes, no antibody is demonstrated
Anti-HLA ( A, B, DR)
Anti Neutrophil (NA-1, NA-2, NB, 5b)
Sometimes, no antibody is demonstrated
2) Two Strikes theory
1)
-
8/3/2019 TRALI - TUCSON
10/46
Anti Neutrophil antibodies: **
3% during pregnancy
7.7% female donors
78% of granulocyte recipients
Anti Neutrophil antibodies: **
3% during pregnancy
7.7% female donors
78% of granulocyte recipients
TRALI Mechanisms: Maternal Sensitization to Fetal AntigensTRALI
Mechanisms: Maternal Sensitization to Fetal Antigens
Anti HLA antibodies*
1st pregnancy : 7.8%
2nd pregnancy: 14.6%
3rd pregnancy: 28.3%
Anti HLA antibodies*
1st pregnancy : 7.8%
2nd pregnancy: 14.6%
3rd pregnancy: 28.3%
* Densmore et al. Transfusion 1999;39:103-6
** Stroncek et al. Transfusion 1996;36: 1009-15
-
8/3/2019 TRALI - TUCSON
11/46
When Transfusing Blood ,What else are we transfusing ?When
Transfusing Blood ,What else are we transfusing ?
RBC
-
8/3/2019 TRALI - TUCSON
12/46
Preformed anti HLA or Anti Neutrophil Antibodies Bind to
Recipients WBCPreformed anti HLA or Anti Neutrophil Antibodies Bind
to Recipients WBC
1) Donor has Antibodies to Recipients WBC1) Donor has Antibodies
to Recipients WBC
-
8/3/2019 TRALI - TUCSON
13/46
Preformed anti HLA or Anti Neutrophil Antibodies Bind to Donors
WBCPreformed anti HLA or Anti Neutrophil Antibodies Bind to Donors
WBC
2) Recipient has Antibodies to Donors WBC2) Recipient has
Antibodies to Donors WBC
Recipient WBCRecipient WBC
Donor WBCDonor WBC
-
8/3/2019 TRALI - TUCSON
14/46
IL1
IL6
TNF IL8
Leukocyte ActivationLeukocyte Activation
Vascular permeability
-
8/3/2019 TRALI - TUCSON
15/46
CytokinesCytokines
IL 1IL 1FF:: Causes fever by production of PG ECauses fever by
production of PG E22IL 1IL 1FF:: Causes fever by production of PG
ECauses fever by production of PG E22
TNFTNF
IL6IL6
IL1IL1
TNFTNF
IL6IL6
IL1IL1
mediators of inflammationmediators of inflammationmediators of
inflammationmediators of inflammation
-
8/3/2019 TRALI - TUCSON
16/46
Antibody Binds to GranulocytesAntibody Binds to Granulocytes
-
8/3/2019 TRALI - TUCSON
17/46
Alveoloar Space
Alveolar Capillary
Alveolar Capillary
Terminal Bronchiole
Activated Neutrophils Adhere to Pulmonary Endothelium
-
8/3/2019 TRALI - TUCSON
18/46
Alveolar Space
Alveolar membrane
Endothelium
Activated Neutrophils Release ProteasesActivated Neutrophils
Release Proteases
-
8/3/2019 TRALI - TUCSON
19/46
Endothelium
Increased Vascular PermeabilityIncreased Vascular
Permeability
-
8/3/2019 TRALI - TUCSON
20/46
Sequence of Events in TRALISequence of Events in TRALIWBC Anti
WBC interaction
WBC are trapped in the pulmonary vasculature
WBCs Release Cytokines and Enzymes
Pulmonary Vascular Injury
Increased Vascular permeability
Pulmonary Edema
WBC Anti WBC interaction
WBC are trapped in the pulmonary vasculature
WBCs Release Cytokines and Enzymes
Pulmonary Vascular Injury
Increased Vascular permeability
Pulmonary Edema
-
8/3/2019 TRALI - TUCSON
21/46
TRANSFUSION RELATED ACUTE LUNG INJURY
(T.R.A.L.I)
-
8/3/2019 TRALI - TUCSON
22/46
TRALI : Origin of AntibodiesTRALI : Origin of Antibodies
Most Common:
Donor has antibody against target antigen in donor WBC
Less Common:
Recipient has antibody to target antigen in donor WBC
Most Common:
Donor has antibody against target antigen in donor WBC
Less Common:
Recipient has antibody to target antigen in donor WBC
Who has antibodies to whom ?Who has antibodies to whom ?
-
8/3/2019 TRALI - TUCSON
23/46
TRALI Mechanisms: Two ModelsTRALI Mechanisms: Two Models
Donor AntibodiesDonor Antibodies
Antibody activates WBC
Complement is Activated
C5 causes WBC aggregation
Pulmonary Leukostasis
Leukocyte degranulation
Antibody activates WBC
Complement is Activated
C5 causes WBC aggregation
Pulmonary Leukostasis
Leukocyte degranulation
Two HitTwo Hit
WBCs Primed by Cytokines or LPS
Lipid Mediators present in transfused plasma
WBC are activated in Pulmonary Vasculature
Respiratory Burst & Protease Release
WBCs Primed by Cytokines or LPS
Lipid Mediators present in transfused plasma
WBC are activated in Pulmonary Vasculature
Respiratory Burst & Protease Release
PULMONARY EDEMA
-
8/3/2019 TRALI - TUCSON
24/46
TRALI : Mechanisms Involved
1. WBC, Lipids , Protein mediators
2. HLA activation of WBC
3. Activated WBC produce Cytokines
4. PAF production (loss of cell to cell contact)
5. Endothelial cells metabolize LTA4 to LTC4 ( Vascular
permeability)
6. Inflammation WBC dwell time in lungs
7. TNF endothelial cell expression of ICAM
-
8/3/2019 TRALI - TUCSON
25/46
TRANSFUSION RELATED ACUTE LUNG INJURY
(T.R.A.L.I)
TRANSFUSION RELATED ACUTE LUNG INJURY
(T.R.A.L.I)
Clinical Outcome*
Oxygen Support 36 100%
Mechanical Ventilation 26 72%
Pulmonary infiltrates 35 97%
Deaths 2 5%
Long time sequalae 0
*Popovsky & Moore, Transfusion 1985
Popovsky & Haley , Transfusion 2000
SHOT** study: 18 cases (6 deaths!)
**Serious Hazards of Transfusion reporting system
-
8/3/2019 TRALI - TUCSON
26/46
How Important is TRALI ?How Important is TRALI ?
CBER : Fatality rate is greater than 10 %CBER : Fatality rate is
greater than 10 %
SHOT*: 70 confirmed cases of TRALI have resulted in 18 deaths
&SHOT*: 70 confirmed cases of TRALI have resulted in 18 deaths
&
49 cases of major morbidity49 cases of major morbidity
CBER : Fatality rate is greater than 10 %CBER : Fatality rate is
greater than 10 %
SHOT*: 70 confirmed cases of TRALI have resulted in 18 deaths
&SHOT*: 70 confirmed cases of TRALI have resulted in 18 deaths
&
49 cases of major morbidity49 cases of major morbidity
*Serious Hazards of Transfusion
-
8/3/2019 TRALI - TUCSON
27/46
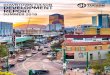
TRALI cases by diagnosis (n = 139)
35%
38%
4%5%
9%
9%
Haem-onc
Surgery
Acute h'age
Correctn coag
Sepsis
Plasma exchange
SHOT Experience and UK Initiatives on TRALI preventionSHOT
Experience and UK Initiatives on TRALI prevention
Lorna MWilliamson
University ofCambridge/National Blood Service
Lorna MWilliamson
University ofCambridge/National Blood Service
http://www.shotuk.org/presentations04.htmhttp://www.shotuk.org/presentations04.htm
-
8/3/2019 TRALI - TUCSON
28/46
Timing of onset of symptoms (n = 108)
63%
25%
7%
5%
D/
-
8/3/2019 TRALI - TUCSON
29/46
Components implicated
(n = 139)
Components implicated
(n = 139)
FFP/cryosupernate 45
Red cells 34
Platelets 27
Whole blood 2
Cryoprecipitate 2 Other 4 (SDFFP, I/V IgG,MBFFP, buffy coat)
Unassignable 25
FFP/cryosupernate 45
Red cells 34
Platelets 27
Whole blood 2
Cryoprecipitate 2 Other 4 (SDFFP, I/V IgG,MBFFP, buffy coat)
Unassignable 25
SHOT Experience and UK Initiatives on TRALI preventionSHOT
Experience and UK Initiatives on TRALI prevention
Lorna MWilliamson
University ofCambridge/National Blood Service
Lorna MWilliamson
University ofCambridge/National Blood Service
http://www.shotuk.org/presentations04.htmhttp://www.shotuk.org/presentations04.htm
-
8/3/2019 TRALI - TUCSON
30/46
Components implicated/total issues
(n = 139)
Components implicated/total issues
(n = 139)
Risk from high plasma components was 5-8 times
higher than from low plasma components.
HIGH PLASMA (300 MLS)
FFP /CSP 45/ 2.6 million = 1: 58,000
Platelets 27/ 1.7 million = 1: 63,000
LOW PLASMA (30 MLS)
Cryoppt 2/ 0.6 million = 1: 300,000
Red cells 34/17.8 million = 1: 523,000
SHOT Experience and UK Initiatives on TRALI prevention
Lorna MWilliamson
University ofCambridge/National Blood Service
http://www.shotuk.org/presentations04.htmhttp://www.shotuk.org/presentations04.htm
-
8/3/2019 TRALI - TUCSON
31/46
Probability of TRALI according
to component implicated
Probability of TRALI according
to component implicated
0
2
4
6
8
10
12
14
1618
FFP Platelets Red
cells
High
Low
SHOT Experience and UK Initiatives on TRALI preventionSHOT
Experience and UK Initiatives on TRALI prevention
Lorna MWilliamson
University ofCambridge/National Blood Service
Lorna MWilliamson
University ofCambridge/National Blood Service
http://www.shotuk.org/presentations04.htmhttp://www.shotuk.org/presentations04.htm
-
8/3/2019 TRALI - TUCSON
32/46
-
8/3/2019 TRALI - TUCSON
33/46
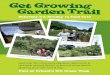
Positive serological investigations in
donors 1998-2003 (n = 71)
Positive serological investigations in
donors 1998-2003 (n = 71)
PositiveXmatch
18
Cognateantigen
18
Antibodiesonly
14
HLA antibodies (cIass I orII)
50
Both HLA and
granulocyte reactive5
PositiveXmatch
6
Cognateantigen
2
Antibodiesonly
8
Granulocyte
reactive16
71 cases
SHOT Experience and UK Initiatives on TRALI preventionSHOT
Experience and UK Initiatives on TRALI prevention
Lorna MWilliamson
University ofCambridge/National Blood Service
Lorna MWilliamson
University ofCambridge/National Blood Service
http://www.shotuk.org/presentations04.htmhttp://www.shotuk.org/presentations04.htm
http://www.shotuk.org/presentations04.htmhttp://www.shotuk.org/presentations04.htm
-
8/3/2019 TRALI - TUCSON
34/46
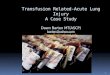
TRALI cases reported to SHOT
(n = 155)
0
10
20
30
40
50
1996 1997 1998 1999 2000 2001 2003
12
months
15
months
SHOT Experience and UK Initiatives on TRALI preventionSHOT
Experience and UK Initiatives on TRALI prevention
Lorna MWilliamson
University ofCambridge/National Blood Service
Lorna MWilliamson
University ofCambridge/National Blood Service
http://www.shotuk.org/presentations04.htmhttp://www.shotuk.org/presentations04.htm
-
8/3/2019 TRALI - TUCSON
35/46
TRALI :What CanWe Do to Prevent it ?TRALI :What CanWe Do to
Prevent it ?
Leukocyte antibody screen of all donors ?
Collect plasma only from low risk donors
Collect plasma only from male donors ?
SERIOUS IMPACT ON PLASMA SUPPLY !
Leukocyte antibody screen of all donors ?
Collect plasma only from low risk donors
Collect plasma only from male donors ?
SERIOUS IMPACT ON PLASMA SUPPLY !
-
8/3/2019 TRALI - TUCSON
36/46
Incidence US & European DataIncidence US & European
Data
European Data (SHOT* study)
70 cases per 17 million blood components
European Data (SHOT* study)
70 cases per 17 million blood components
US Data (Popovsky et al)
- 0.02% of all blood components transfused
- 0.16% of all patients transfused (1 in 625)
US Data (Popovsky et al)
- 0.02% of all blood components transfused
- 0.16% of all patients transfused (1 in 625)
*Serious Hazards of Transfusion
-
8/3/2019 TRALI - TUCSON
37/46
Products Containing PlasmaProducts Containing Plasma
PRBC or WB FFP Platelets Cryoprecipitate
Can Cause TRALIBone Marrow Granulocytes
-
8/3/2019 TRALI - TUCSON
38/46
TRALITRALI
Transfusion Related DeathsTransfusion Related Deaths
1) Hemolytic Transfusion Reaction
2) Long time sequellae of Hepatitis C
3) TRALI
1) Hemolytic Transfusion Reaction
2) Long time sequellae of Hepatitis C
3) TRALI
Sazama K,. Reports of 355 Transfusion Associated Deaths
Transfusion 30: 583-590 (1990)
Sazama K,. Reports of 355 Transfusion Associated Deaths
Transfusion 30: 583-590 (1990)
-
8/3/2019 TRALI - TUCSON
39/46
-
8/3/2019 TRALI - TUCSON
40/46
My First Case of TRALI 58 yr old dwarf
Pneumectomy for TB in late 40s
Transfusion for refractory anemia
Sudden SOB, Hypotention
Transferred to ICU Intubated
CXR complete pulmonary white out 4 days on the respirator
Recovered fully !
58 yr old dwarf
Pneumectomy for TB in late 40s
Transfusion for refractory anemia
Sudden SOB, Hypotention
Transferred to ICU Intubated
CXR complete pulmonary white out 4 days on the respirator
Recovered fully !
-
8/3/2019 TRALI - TUCSON
41/46
What to do when TRALI is suspectedWhat to do when TRALI is
suspected
Blood Bank is notified
Medical Director evaluates case
UBS form needs to be filled out
Samples are drawn for lab work
Blood Bank is notified
Medical Director evaluates case
UBS form needs to be filled out
Samples are drawn for lab work
What happens at the lab ?
EDTA/Citrate; + ClotSerological Workup for HLA class I & II
antibodies
Serological Workup for Anti Neutrophil antibodies
What happens at the lab ?
EDTA/Citrate; + ClotSerological Workup for HLA class I & II
antibodies
Serological Workup for Anti Neutrophil antibodies
-
8/3/2019 TRALI - TUCSON
42/46
Serological InvestigationSerological Investigation Indirect:
GCLT: Granulocyte Chemoluminescent Test
GIFT: Granulocyte Immunoflulorescence Test LIFT: Lymphocyte
Immunofluorescense Test
Indirect:
GCLT: Granulocyte Chemoluminescent Test
GIFT: Granulocyte Immunoflulorescence Test LIFT: Lymphocyte
Immunofluorescense Test
MAIGA: Monoclonal antibody immobilization of Granulocyte
AntigenMAIPA: Monoclonal Antibody immobilization of Platelet
Antigens
ELISA: Enzyme Lynked Immunosorbent Assay
MAIGA: Monoclonal antibody immobilization of Granulocyte
AntigenMAIPA: Monoclonal Antibody immobilization of Platelet
Antigens
ELISA: Enzyme Lynked Immunosorbent Assay
-
8/3/2019 TRALI - TUCSON
43/46
TRALI: Role of the Medical DirectorTRALI: Role of the Medical
Director
Educate Clinicians
Evaluate patients who have respiratory distress during Tx.
Go through the list of differential diagnosis
Discuss the case with the clinicians
Initiate TRALI work-up when appropriate.
Educate Clinicians
Evaluate patients who have respiratory distress during Tx.
Go through the list of differential diagnosis
Discuss the case with the clinicians
Initiate TRALI work-up when appropriate.
-
8/3/2019 TRALI - TUCSON
44/46
Are Clinicians Aware of TRALI ?Are Clinicians Aware of TRALI
?
1 Donor linked to a TRALI fatality
Chart review of recipients of previous donations
- 50 patients had received components from same donor- 13
patients had reactions related to tx
- 7 reactions were reported to Blood Bank (46.7%)
1 Donor linked to a TRALI fatality
Chart review of recipients of previous donations
- 50 patients had received components from same donor- 13
patients had reactions related to tx
- 7 reactions were reported to Blood Bank (46.7%)
-
8/3/2019 TRALI - TUCSON
45/46
TRALI : When in Doubt Dont despairTRALI : When in Doubt Dont
despair
Call one of the UBS Medical Directors for Assistance !
-
8/3/2019 TRALI - TUCSON
46/46
THE
END
THE
END