Embed Size (px)
Citation preview
Perspectives in Medicine (2012) 1, 357—361
Bartels E, Bartels S, Poppert H (Editors):New Trends in Neurosonology and Cerebral Hemodynamics — an Update.
Perspectives in Medicine (2012) 1, 357—361
j o u r n a l h o m e p a g e : w w w . e l s e v i e r . c o m / l o c a t e / p e r m e d
Transcranial sonography in psychiatric diseases
Milija D. Mijajlovic ∗
Neurology Clinic, Clinical Center of Serbia, School of Medicine University of Belgrade, Belgrade, Serbia
KEYWORDSTranscranialsonography;Basal ganglia;Brainstem raphe;Psychiatric diseases
Abstract Transcranial sonography (TCS) revealed reduced echogenicity of the brainstemraphe (BR) as a characteristic finding in unipolar depression and in depression associated withParkinson’s or Wilson’s disease, but not in healthy adults, schizophrenia, multiple sclerosiswith depression or Parkinson’s disease without concomitant depression. Similar findings wereshown also for adjustment disorder with depressed mood. In contrast to unipolar depression,sonographic findings of bipolar patients may generally indicate preserved structural integrityof mesencephalic raphe structures. If bipolar disorder is associated with hypoechogenic BR,depressive symptoms are more severe. BR hypoechogenicity could be caused by a modificationof tissue cell density, the interstitial matrix composition or an alteration of fiber tracts integrityrepresenting involvement of the basal limbic system in the pathogenesis of unipolar depressionand depression associated with certain neurodegenerative diseases.
Recently it was shown that nigrostriatal dopaminergic system is abnormal in children withattention-deficit hyperactivity disorder which was expressed by significantly larger echogenicityof substantia nigra.
The increasingly broad application of TCS in the early and differential diagnosis of neu-
rodegenerative and psychiatric disorders in many centers all over the world is probably thebest evidence for the value of the method. Main advantages include the easy applicability,the fact that it is quick and repeatedly performable with no limitations as known from otherneuroimaging techniques and that it is relatively cheap and side effect free.© 2012 Elsevier GmbH. All rights reserved.hdu
Transcranial sonography — historical overviewand method in psychiatric diseases
Transcranial sonography (TCS) is a relatively new neuroimag-
ing method which displays tissue echogenicity (intensity ofreflected ultrasound waves) of the brain through the intactskull.∗ Correspondence address: Neurology Clinic, Clinical Center ofSerbia, School of Medicine University of Belgrade, Dr Subotica 6,11000 Belgrade, Serbia. Tel.: +381 11 3064265;fax: +381 11 2684577.
E-mail address: [email protected]
srpirlpmbo
2211-968X/$ — see front matter © 2012 Elsevier GmbH. All rights reservdoi:10.1016/j.permed.2012.02.039
Besides the specific finding of the substantia nigra (SN)yperechogenicity in Parkinson’s disease (PD), first timeescribed in 1995 by Becker et al. [1], a series of studiessing TCS has reported another specific ultrasound feature:tructural abnormality of the midbrain raphe depicted aseduced echogenicity or invisible brainstem raphe (BR) inatients with unipolar depression compared with healthyndividuals [2,3]. The structural abnormality which waseported to occur in unipolar depressed patients, was unre-ated to severity of current illness, and was absent in
atients with schizophrenia [3]. The same structural abnor-ality has also been reported when depressed patients haveeen compared to non-depressed patients, having a varietyf neurological diseases, for example, PD [4,5], dystoniced.
3 M.D. Mijajlovic
ssThhcsgiT
ructorptiietbobnBw[eeipgsfssli
imcaiisttiaPrrfi
T
Na
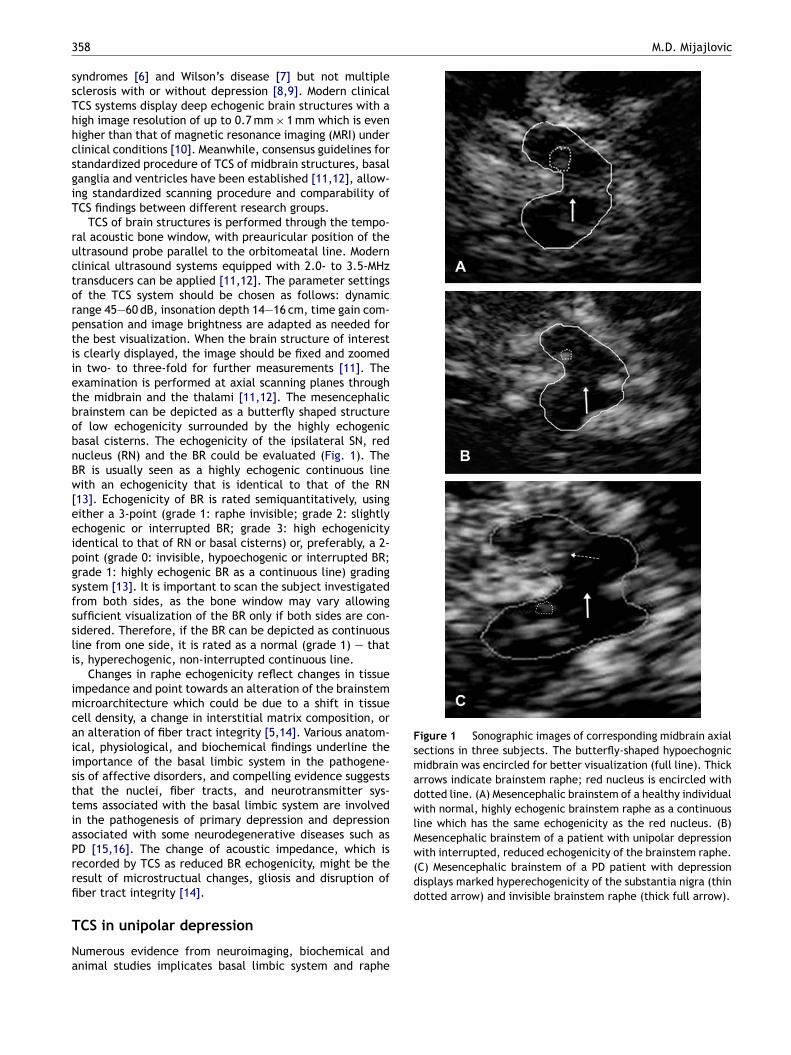
Figure 1 Sonographic images of corresponding midbrain axialsections in three subjects. The butterfly-shaped hypoechognicmidbrain was encircled for better visualization (full line). Thickarrows indicate brainstem raphe; red nucleus is encircled withdotted line. (A) Mesencephalic brainstem of a healthy individualwith normal, highly echogenic brainstem raphe as a continuousline which has the same echogenicity as the red nucleus. (B)Mesencephalic brainstem of a patient with unipolar depressionwith interrupted, reduced echogenicity of the brainstem raphe.(C) Mesencephalic brainstem of a PD patient with depressiondisplays marked hyperechogenicity of the substantia nigra (thindotted arrow) and invisible brainstem raphe (thick full arrow).
58
yndromes [6] and Wilson’s disease [7] but not multipleclerosis with or without depression [8,9]. Modern clinicalCS systems display deep echogenic brain structures with aigh image resolution of up to 0.7 mm × 1 mm which is evenigher than that of magnetic resonance imaging (MRI) underlinical conditions [10]. Meanwhile, consensus guidelines fortandardized procedure of TCS of midbrain structures, basalanglia and ventricles have been established [11,12], allow-ng standardized scanning procedure and comparability ofCS findings between different research groups.
TCS of brain structures is performed through the tempo-al acoustic bone window, with preauricular position of theltrasound probe parallel to the orbitomeatal line. Modernlinical ultrasound systems equipped with 2.0- to 3.5-MHzransducers can be applied [11,12]. The parameter settingsf the TCS system should be chosen as follows: dynamicange 45—60 dB, insonation depth 14—16 cm, time gain com-ensation and image brightness are adapted as needed forhe best visualization. When the brain structure of interests clearly displayed, the image should be fixed and zoomedn two- to three-fold for further measurements [11]. Thexamination is performed at axial scanning planes throughhe midbrain and the thalami [11,12]. The mesencephalicrainstem can be depicted as a butterfly shaped structuref low echogenicity surrounded by the highly echogenicasal cisterns. The echogenicity of the ipsilateral SN, reducleus (RN) and the BR could be evaluated (Fig. 1). TheR is usually seen as a highly echogenic continuous lineith an echogenicity that is identical to that of the RN
13]. Echogenicity of BR is rated semiquantitatively, usingither a 3-point (grade 1: raphe invisible; grade 2: slightlychogenic or interrupted BR; grade 3: high echogenicitydentical to that of RN or basal cisterns) or, preferably, a 2-oint (grade 0: invisible, hypoechogenic or interrupted BR;rade 1: highly echogenic BR as a continuous line) gradingystem [13]. It is important to scan the subject investigatedrom both sides, as the bone window may vary allowingufficient visualization of the BR only if both sides are con-idered. Therefore, if the BR can be depicted as continuousine from one side, it is rated as a normal (grade 1) — thats, hyperechogenic, non-interrupted continuous line.
Changes in raphe echogenicity reflect changes in tissuempedance and point towards an alteration of the brainstemicroarchitecture which could be due to a shift in tissue
ell density, a change in interstitial matrix composition, orn alteration of fiber tract integrity [5,14]. Various anatom-cal, physiological, and biochemical findings underline themportance of the basal limbic system in the pathogene-is of affective disorders, and compelling evidence suggestshat the nuclei, fiber tracts, and neurotransmitter sys-ems associated with the basal limbic system are involvedn the pathogenesis of primary depression and depressionssociated with some neurodegenerative diseases such asD [15,16]. The change of acoustic impedance, which isecorded by TCS as reduced BR echogenicity, might be theesult of microstructual changes, gliosis and disruption ofber tract integrity [14].
CS in unipolar depression
umerous evidence from neuroimaging, biochemical andnimal studies implicates basal limbic system and raphe

eat
oo
Tmidc[sipdtisawfpesBs
efpucmicp
SPflsiefiis
Tm
Mwdb
Transcranial sonography in psychiatric diseases
nuclei involvement in the pathogenesis of the mood dis-orders, particularly depression. Typical ultrasound markerthat can be of value in the diagnosis and differential diag-nosis of depression is the low echogenicity or interruptedBR. Raphe hypoechogenicity is a common finding in 50—70%of patients with unipolar depression [2,17] and is asso-ciated with responsivity to serotonin-reuptake inhibitors(SSRI) [18]. In a pioneer study, echogenicity of the BR wasexamined by TCS in 20 patients with unipolar depressionand 20 healthy adult controls. A marked reduction of rapheechogenicity in depressed patients was found [2]. This find-ing was confirmed a year later on larger number of patientsin the study which compared echogenicity of the BR between40 patients with unipolar depression, 40 patients with bipo-lar disorder and 40 healthy controls. Raphe echogenicity inpatients with unipolar depression was found to be distinctlyreduced as compared with healthy adults and patients withbipolar affective disorder. BR echogenicity, on average, washalved in the unipolar depressed group. No correlation wasfound between BR echogenicity and age, sex or diseaseseverity [3]. Reduced brainstem midline echogenicity ofdepressed patients was interpreted as a structural alter-ation of the dorsal raphe nucleus or fiber tracts in this region[14]. Increased T2-relaxation time in a pontine brainstem inpatients with major depression could be in line with previousreports of brainstem pathology in these patients [14]. Theobservation might indicate a subtle tissue alteration, whichcannot be identified by visual inspection of the images. T2-relaxation time depends on physical tissue characteristicsand is influenced by hydration status or iron content. Differ-ences in T2-relaxation time of specific brain areas betweenpatients with major depression and healthy controls mayindicate different tissue composition caused by histologicalchanges.
Several further studies confirmed the finding of reducedechogenicity of the BR in unipolar depression. In the studyof Walter [17] the frequency of patients with reducedechogenicity of BR was higher in unipolar depression com-pared with healthy individuals and in depressed PD patientscompared with non-depressed. The frequency of reducedechogenicity of BR was the highest in patients with unipolardepression. In this study, reduced echogenicity of the BR wasmore frequent in depressed than in non-depressed patients,irrespective of presence of PD.
TCS findings of another study [19], showed that reducedechogenicity of pontomesencephalic BR is frequent indepressive states, irrespective of diagnostic category ofdepression, but only rare in healthy subjects withoutany history of psychiatric disorder. BR echogenicity couldnot discriminate between major depressive disorder andadjustment disorder with depressed mood. BR echogenicityscores showed in this study were significantly lower in SSRIresponders compared with SSRI non-responders. Reduced BRechogenicity indicated SSRI responsivity with a positive pre-dictive value of 88%.
Recently, reduced raphe echogenicity was found in 47%of the patients with major depressive disorder but only in15% of healthy controls. In patients with suicidal ideations
that finding was even more pronounced (86%) with the high-est frequency of completely not visible TCS raphe finding(72%). Data showed that altered echogenicity of the BR isfrequent in patients with suicidal ideation. Normal raphebcpe
359
chogenicity in patients with major depression was associ-ted with less severe depressive symptoms and rarely withhe presence of suicidal ideations [20].
Although there are several reports of MRI signal alterationf BR in depression, a characteristic neuroimaging patternf BR abnormality has not yet been found [21].
Ultrasound investigations have been supplemented by2-weighted MRI studies in order to investigate patho-orphological pattern of the BR in depression. Increased
ntensity of the midline has been reported for unipolarepressed patients when compared to bipolar patients andontrols in a retrospective study using T2-weighted MRI22]. A difference between patients with major depres-ion and control subjects for T2-relaxation times was foundn a region of interest located along the midline of theons. No difference was found between patients with bipolarisorder and control subjects. Alterations of T2-relaxationimes might indicate subtle tissue changes [23]. These find-ngs are in line with the results of pathoanatomic and PETtudies demonstrating morphological and functional alter-tion of the dorsal raphe nucleus in major depression,ith decreased serotonin type 1A receptor binding and
ewer neurons expressing serotonin transporter mRNA com-ared with findings in controls [24]. The relationship of BRchogenicity and SSRI responsivity which was found in thetudy of Walter [19] further supports the idea that reducedR echogenicity reflects an alteration of the serotonergicystem.
In contrast with previous reports, no difference inchogenicity of the BR of unipolar depressed patients wasound in the study of Steele, the only one which investigatedossible structural changes of the BR in unipolar depressionsing diffusion tensor imaging, did not confirm structuralhanges of the BR in unipolar depressive patients using thisethod [25]. One of the important advantages of TCS is that
t could also detect a subgroup of patients with depressionharacterized by mild clinical signs of parkinsonism who areossibly at an elevated risk of developing definite PD.
TCS data in a recent study showed that the finding ofN hyperechogenicity, which is characteristic for idiopathicD, was related to motor asymmetry and reduced verbaluency in patients with depressive disorders. This relation-hip was even stronger in younger patients (<50 years) andndependent from age, in patients who had reduced BRchogenicity [21]. Since, both liability for developing PD andrequency of PD-like TCS findings were found to be increasedn depression, patients with depressive disorders might be anmportant population to screen for sonographic and clinicaligns of early PD.
CS in adjustment disorder with depressedood (ADDM)
ajor depressive disorder (MDD) and adjustment disorderith depressed mood (ADDM) are currently regarded asistinct disease entities [26]. Especially, DSM axis-II comor-idity and suicidal behavior have been reported to differ
etween MDD and ADDM. Following the Structured Clini-al Interview for DSM-IV Axis-I Disorders [27], in the studyerformed by Walter et al. [18], 15 patients with singlepisode of MDD (MDDs), 22 with recurrent MDD (MDDr)
3
aifdabrtfctaeanl
T
BeIsndpoivBgpetto(bt
pbnSS
fw(mctp
ishiet
T
AqmHrimtssspewtAtddotIiomid
C
Tddbttroifr
adr
R
60
nd 15 with ADDM. Reduced BR echogenicity was foundn 54% of the patients with MDD and ADDM, but only inour (8%) of the healthy subjects. BR echogenicity scoresid not differ among patients with MDDs, MDDr, or ADDM,nd pair-wise group comparisons failed to show differencesetween diagnostic groups with respect to frequency ofeduced BR echogenicity. TCS findings of this study showedhat reduced echogenicity of pontomesencephalic BR isrequent in depressive states, irrespective of diagnosticategory. As a result of the present study, the hypothesishat BR echogenicity might distinguish patients with MDDnd patients with ADDM had to be rejected. Reduced BRchogenicity is found with similar frequency in MDDs, MDDr,nd ADDM. This is in agreement with results of clinical andeurophysiological studies suggesting common pathophysio-ogical mechanisms in MDD and ADDM [28].
CS in bipolar disorder
ipolar affective disorders are characterized by recurrentpisodes of depression as well as mania or hypomania [26].n histological studies, subtle structural deficits in the dor-al raphe with a regional reduction in the synthesis oforadrenalin have been described in patients with bipolarisorder. The first TCS study evaluated BR alterations inatients with bipolar affective disorders, revealed normalr even increased echogenicity of BR in bipolar disorder,rrespective of the existing disease conditions. This obser-ation led to the assumption that reduced echogenicity ofR may be specific to unipolar depression [3]. Recently, Kro-ias et al. found the BR hypoechogenicity in 36.1% of the 36atients with bipolar I disorder (14 depressed, 8 manic, 14uthymic) and in 20% of the 35 healthy controls. Comparedo the control group, frequency of altered BR echogenici-ies did not reach statistical significance. Hypoechogenicityf BR was depicted in six (42.9%) of the depressed, in three37.5%) of the manic and in four (28.6%) of the euthymicipolar patients, with no significant difference between thehree subgroups [29].
The width of third ventricle was significantly larger in theatient group (3.8 ± 2.1 mm vs. 2.7 ± 1.2 mm). Depressedipolar patients with reduced BR echogenicity showed sig-ificantly higher scores on the Hamilton Depression Ratingcale as well as the Montgomery-Åsberg Depression Ratingcale [29].
Relating to echogenicity of SN, a strong trend of morerequent SN hyperechogenicities in the depressed subgroupas identified. Hyperechogenic SN was seen in six patients
16.7%): five (35.7%) of the depressed, in none (0%) of theanic and in one (7.1%) of the euthymic patients, indi-
ating cyclical dysregulation in quantitative dopaminergicransmission as one of the underlying pathologies in theathogenesis of bipolar disorder.
One of the main conclusions to be drawn from the studys that sonographic findings do not differ in different moodtates of bipolar I disorder. Regarding the brainstem raphe,
ypoechogenicity is correlated to the severity of symptomsn bipolar depression. Furthermore, bipolar patients in gen-ral showed significantly larger widths of the third ventriclehan the control group in this study [29].M.D. Mijajlovic
CS in attention-deficit hyperactivity disorder
ttention-deficit hyperactivity disorder (ADHD) is fre-uent neuropsychiatric disorder characterized by excessiveotor activity, increased impulsivity and attention deficits.ypotheses about its pathophysiology implicate various neu-otransmitters including dopamine [30]. One recent studynvestigated echogenicity of the SN as a potential structuralarker for dysfunction of the nigrostriatal dopaminergic sys-
em in children with ADHD. Echogenicity of the SN in thistudy was determined in 22 children with DSM-IV diagno-is of ADHD and 22 healthy controls matched for age andex. The echogeniciity of SN was significantly larger in ADHDatients than in healthy controls (F1,42 = 9.298, p = 0.004,ffect size = 0.92, specificity was 0.73 and sensitivity 0.82)ithout effects of age or sex. The study showed that nigros-
riatal dopaminergic system is abnormal in children withDHD. Increased SN echogenicity in ADHD patients relativeo healthy controls might be explained by a developmentalelay. Although most findings with regard to a presumptiveevelopmental delay in ADHD relate to diminished growthf cortical thickness, recent studies have reported struc-ural alterations in the basal ganglia of patients with ADHD.t remains unclear whether an enlarged echogenic SN arean ADHD patients can be attributed to a primary disturbancef nigral iron metabolism, whether it is related to a pri-ary developmental delay of brain structure, or whether it
ndicates a general structural marker for dysfunction of theopaminergic system [31].
onclusion
he increasingly broad application of TCS in the early andifferential diagnosis of psychiatric and neurodegenerativeiseases in many centers all over the world is probably theest evidence for the value of the method. The main advan-ages include the easy applicability, even in moving (e.g.remulous or agitated) patients, the fact that it is quick andepeatedly performable with no limitations as known fromther neuroimaging techniques (metal in the body as a lim-tation for MRI imaging, specific medication as a limitationor many forms of functional neuroimaging), and that it iselatively cheap and side effect free.
It is a reliable method to investigate, diagnosend follow-up patients with unipolar depression, bipolarisorder, ADHD and depression associated with some neu-odegenerative diseases.
eferences
[1] Becker G, Seufert J, Bogdahn U, Reichmann H, Reiners K.Degeneration of substantia nigra in chronic Parkinson’s diseasevisualized by transcranial color-coded real-time sonography.Neurology 1995;45:182—4.
[2] Becker G, Struck M, Bogdahn U, Becker T. Echogenicity of thebrainstem raphe in patients with major depression. PsychiatryRes 1994;55:75—84.
[3] Becker G, Becker T, Struck M, Lindner A, Burzer K, Retz W, et al.Reduced echogenicity of brainstem raphe specific to unipolardepression: a transcranial color-coded real-time sonographystudy. Biol Psychiatry 1995;38:180—4.
[
[
[
[
[
[
[
[
[
[
[
[
Transcranial sonography in psychiatric diseases
[4] Becker T, Becker G, Seufert J, Hofmann E, Lange KW, NaumannM, et al. Parkinson’s disease and depression: evidence for analteration of the basal limbic system detected by transcranialsonography. J Neurol Neurosurg Psychiatry 1997;63:590—6.
[5] Berg D, Supprian T, Hofmann E, Zeiler B, Jager A, Lange KW,et al. Depression in Parkinson’s disease: brainstem midlinealteration on transcranial sonography and magnetic resonanceimaging. J Neurol 1999;246:1186—93.
[6] Naumann M, Becker G, Toyka KV, Supprian T, Reiners K.Lenticular nucleus lesion in idiopathic dystonia detected bytranscranial sonography. Neurology 1996;47:1284—90.
[7] Walter U, Krolikowski K, Tarnacka B, Benecke R, CzlonkowskaA, Dressler D. Sonographic detection of basal ganglia lesionsin asymptomatic and symptomatic Wilson disease. Neurology2005;64:1726—32.
[8] Berg D, Supprian T, Thomae J, Warmuth-Metz M, Horowski A,Zeiler B, et al. Lesion pattern in patients with multiple sclerosisand depression. Mult Scler 2000;6:156—62.
[9] Berg D, Mäurer M, Warmuth-Metz M, Rieckmann P, Becker G.The correlation between ventricular diameter measured bytranscranial sonography and clinical disability and cognitivedysfunction in patients with multiple sclerosis. Arch Neurol2000;57:1289—92.
[10] Walter U, Kanowski M, Kaufmann J, Grossmann A, BeneckeR, Niehaus L. Contemporary ultrasound systems allow high-resolution transcranial imaging of small echogenic deepintracranial structures similarly as MRI: a phantom study. Neu-roimage 2008;40:551—8.
[11] Walter U, Behnke S, Eyding J, Niehaus L, Postert T, Seidel G,et al. Transcranial brain parenchyma sonography in movementdisorders: state of the art. Ultrasound Med Biol 2007;33:15—25.
[12] Berg D, Godau J, Walter U. Transcranial sonography in move-ment disorders. Lancet Neurol 2008;7:1044—55.
[13] Mijajlovic MD. Transcranial sonography in depression. Int RevNeurobiol 2010;90:259—72.
[14] Becker G, Berg D, Lesch KP, Becker T. Basal limbic systemalteration in major depression: a hypothesis supported bytranscranial sonography and MRI findings. Int J Neuropsy-chopharmacol 2001;4:21—31.
[15] Ball WA, Whybrow PC. Biology of depression and mania. CurrOpin Psychiatry 1993;6:27—34.
[16] Mayberg HS, Solomon D. Depression in Parkinson’s dis-ease: a biochemical and organic viewpoint. Adv Neurol1995;65:49—60.
[17] Walter U, Hoeppner J, Prudente-Morrissey L, Horowski S,Herpertz SC, Benecke R. Parkinson’s disease-like midbrainsonography abnormalities are frequent in depressive disorders.Brain 2007;130:1799—807.
[18] Walter U, Prudente-Morrissey L, Herpertz SC, Benecke R,Hoeppner J. Relationship of brainstem raphe echogenicityand clinical findings in depressive states. Psychiatry Res2007;155:67—73.
[
361
19] Walter U, Horowski S, Benecke R, Zettl U. Transcranial brainsonography findings related to neuropsychological impair-ment in multiple sclerosis. J Neurol 2007;254(Suppl. 2):49—52.
20] Budisic M, Karlovic D, Trkanjec Z, Lovrencic-Huzjan A, VukovicV, Bosnjak J, et al. Brainstem raphe lesion in patients withmajor depressive disorder and in patients with suicidal ideationrecorded on transcranial sonography. Eur Arch Psychiatry ClinNeurosci 2010;260(3):203—8.
21] Hoeppner J, Prudente-Morrissey L, Herpertz SC, BeneckeR, Walter U. Substantia nigra hyperechogenicity in depres-sive subjects relates to motor asymmetry and impairedword fluency. Eur Arch Psychiatry Clin Neurosci 2009;259:92—7.
22] Becker T, Becker D, Berg D, Hofmann E, Lange K, Struck M.Pathological findings in neuropsychiatric diseases. In: BogdahnU, Becker G, Schlachetzki F, editors. Echoenhancers and tran-scranial color duplex sonography. London: Blackwell Science;1998. p. 359—73.
23] Supprian T, Reiche W, Schmitz B, Grunwald I, Backens M, Hof-mann E, et al. MRI of the brainstem in patients with majordepression, bipolar affective disorder and normal controls. Psy-chiatry Res 2004;131:269—76.
24] Meltzer C, Price J, Mathis C, Butters MA, Ziolko S, Moses-Kolko E, et al. Serotonin 1A receptor binding and treatmentresponse in late-life depression. Neuropsychopharmacology2004;29:2258—65.
25] Steele JD, Bastin ME, Wardlaw JM, Ebmeier KP. Possible struc-tural abnormality of the brainstem in unipolar depressiveillness: a transcranial ultrasound and diffusion tensor mag-netic resonance imaging study. J Neurol Neurosurg Psychiatry2005;76:1510—5.
26] American Psychiatric Association. Diagnostic and statisticalmanual of mental disorders. 4th ed. Washington, DC: AmericanPsychiatric Press; 1994.
27] First MB, Spitzer RL, Gibbon M, Williams JBW. StructuredClinical Interview for DSM-IV Axis I Disorders Clinician Ver-sion (SCID-CV). Washington, DC: American Psychiatric Press;1996.
28] Bar KJ, Brehm S, Boettger MK, Wagner G, Boettger S, SauerH. Decreased sensitivity to experimental pain in adjustmentdisorder. Eur J Pain 2005;10:467—71.
29] Krogias C, Hoffmann K, Eyding J, Scheele D, Norra C, Gold R,et al. Evaluation of basal ganglia, brainstem raphe and ventri-cles in bipolar disorder by transcranial sonography. PsychiatryRes 2011;194(November (2)):190—7.
30] Biederman J, Faraone SV. Attention-deficit hyperactivity disor-der. Lancet 2005;366:237—48.
31] Romanos M, Weise D, Schliesser M, Schecklmann M, Löffler J,Warnke A, et al. Structural abnormality of the substantia nigrain children with attention-deficit hyperactivity disorder. J Psy-chiatry Neurosci 2010;35(1):55—8.