Embed Size (px)
Citation preview

e u r o p e a n j o u r n a l o f p a e d i a t r i c n e u r o l o g y 1 6 ( 2 0 1 2 ) 1 7 5e1 7 8
Official Journal of the European Paediatric Neurology Society
Original article
Transcranial ultrasound in neurodegeneration with brain ironaccumulation (NBIA)
Jan Liman a,*, Andreas Wellmer b, Kevin Rostasy c, Mathias Bahr a, Pawel Kermer a
aDepartment of Neurology, University of Gottingen, Robert-Koch-Str. 40, 37075 Gottingen, GermanybDepartment of Neurology, Hospital Ludmillenstift, Ludmillenstraße 4-6, 49716 Meppen, GermanycDepartment of Paediatrics, Division of Paediatric Neurology, Medical University of Innsbruck, Anichstr. 35, 6020 Innsbruck, Austria
a r t i c l e i n f o
Article history:
Received 21 September 2010
Received in revised form
26 May 2011
Accepted 18 July 2011
Keywords:
NBIA
TCS
Sonography
Hallervorden-Spatz-Syndrome
* Corresponding author. Tel.: þ49 551 391413E-mail address: [email protected] (J. Lima
1090-3798/$ e see front matter ª 2011 Europdoi:10.1016/j.ejpn.2011.07.009
a b s t r a c t
NBIA/HSS is a neurodegenerative disorder associated with iron accumulation in specific
brain regions. To date, the diagnosis is obtained by typical MRI changes followed by genetic
mutation analysis. This procedure is laborious and limited to a few specially equipped
medical centres. Since transcranial sonography (TCS) is widely used for the early diagnosis
of PD in adults displaying parenchymal metal deposits, it is likely to be a reliable diagnostic
tool for the early diagnosis of NBIA.
In 7 patients with proven NBIA and 13 age-matched controls without record of neuro-
logical disease TCS was performed by an experienced ultrasound examiner. Data were
analysed by two blinded investigators regarding hyperechogenicity and size of the sub-
stantia nigra (SN). SN size and hyperechogenicity was significantly increased in patients
with NBIA compared to controls (students t-test: p < 0.001).
TCS appears to be a non-invasive and inexpensive screening technique in patients with
suspected NBIA. Performed by an experienced physician, it could enable an earlier diag-
nosis and pre-selection of patients for the MRI scan and genetic testing, which are still the
diagnostic gold standard.
ª 2011 European Paediatric Neurology Society. Published by Elsevier Ltd. All rights
reserved.
1. Introduction NBIA was designated pantothenate kinase-associated neuro-
Neurodegeneration with brain iron accumulation (NBIA),
formerly known as Hallervorden-Spatz-Syndrome is an
orphan disease with an estimated prevalence of 1e3 per
million. Neuropathological hallmarks are abnormal iron
accumulations especially in the globus pallidus and the sub-
stantia nigra pars reticulata.1 Recently, mutations in the
pantothenate kinase 2 (PANK2) gene were identified as caus-
ative for up to 70% of all NBIA cases. Hence, this subtype of
9; fax: þ49 551 3914302.n).ean Paediatric Neurology
degeneration (PKAN).2,3
Symptoms usually develop in childhood, but later mani-
festations occur and are associated with certain mutations in
PANK2 gene.3 Affected patients initially present with gait
abnormalities or an increased “clumsiness” before developing
the typical clinical signs consisting of dysarthria, dystonia and
visual problems.4
In the “pre-MRI”-era the diagnosis of NBIA could only be
suspected by clinical features and verified post mortem by
Society. Published by Elsevier Ltd. All rights reserved.

Table 1 e List of genetic background, age and sex of thepatients examined.
age geneticbackground
sex Right SNarea[cm2]
Left SNarea[cm2]
NBIA 1 8 years PKAN M 0.18 0.11
NBIA 2 5 years non-PKAN F 0.4 0.17
NBIA 3 14 years PKAN F 0.39 0.27
NBIA 4 26 years non-PKAN M 0.28 0.34
NBIA 5 10 years PKAN M 0.32 0.22
NBIA 6 21 years non-PKAN F 0.28 0.39
NBIA 7 34 years unknown F 0.3 0.34
e u r o p e a n j o u r n a l o f p a e d i a t r i c n e u r o l o g y 1 6 ( 2 0 1 2 ) 1 7 5e1 7 8176
a neuropathologist. To date, MR imaging is the gold standard
for diagnosing the disease by showing the pathognomonic
hypointensity within the globus pallidus along with high
signal intensity in the center of the globus pallidus internus
also known as “eye-of-the-tiger-sign” on T2-weighted
images.5 The diagnosis is then usually verified by PANK2
mutation screening in these patients. However, up to 30% of
cases who present with the clinical features do not have
a typical MRI and/or expected genetic findings.
In individuals with suspected NBIA MRI remains the diag-
nostic tool of choice, butpatientshave tobeanesthetized for this
procedure because of potential movement artefacts due to the
severe movement disorder and young age. Therefore MRI units
with an experienced anaesthesiologist, which is mostly
restrictedto largemedicalcentresinmajorcities,aremandatory.
According to our experience, these difficulties often prolong the
time from disease onset to definite diagnosis for years.
Since its first description by Becker et al. (1995), trans-
cranial sonography (TCS) has become a widely accepted
diagnostic tool in early and differential diagnosis of Parkin-
son’s disease (PD).6 More than 90% of PD patients exhibit an
increased area of hyperechogenicity of the substantia nigra
(SN), which in combination with clinical features is highly
characteristic for this disease.6,7 As there is some evidence
that the structural correlate of this hyperechogenicity in PD is
related to increased SN iron levels and since iron accumula-
tion in the SN also is one of the key features in NBIA, we
intended to test TCS as diagnostic tool for early and differ-
ential diagnosis of NBIA.8 In our opinion, TCS could become
a screening method for NBIA, as it is easy to use, even in non
anesthetised patients, widely available, cheap and is not
associated with any side effects.
In this study, we performed TCS in 6 patients with genet-
ically proven NBIA, one patient without genetic analysis, but
typical MRI findings and 13 age-matched controls without any
record of neurological disease or brain damage.
2. Materials and methods
2.1. Participants
Patients were recruited during the annual meeting of the
German NBIA Association “Hoffnungsbaum” in 2008. Six
patients had a diagnosis of NBIA with (3 patients) or without
PKANmutation (3 patients) prior to the study, one patient had
the diagnosis NBIA without any genetically testing, but with
typical MRI changes (eye- of ethe-tiger-sign). The age ranged
from 5 to 34 years (for overview see Table 1).
13 agematched individuals recruited from the Department
of Paediatric Cardiology, (age range 7e28 years), without any
neurological symptoms, served as controls.
This study was approved by the local ethical committee
(No. 1/1/08), all participants or their legal guardians gave
written informed consent to this study.
2.2. Procedure
Transcranial ultrasound was performed by an experienced
sonographer through the temporal bone window with
a 2.5Mhz phased-array transducer (Siemens, Acuson Sequoia
Erlangen Germany), as described previously.9 The ultrasound
parameters chosen were: penetration depth 14e16 cm,
dynamic range 50 dB, high persistence, gray scale and focus
were adjusted individually. The obtained data were recorded,
saved and analysed further without marking of any sono-
graphic structures.
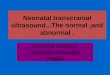
In the mesencephalic plane the brainstem was visualized
as a hypoechogenic “butterfly shaped” structure (Fig. 1A).
Afterwards the data obtained were analysed a second time by
two independent examiners. Both examiners were blinded to
the subgroup (patient or control), and to the results of each
other. Planimetric measurements were performed automati-
cally, after manually encircling the outer circumference of
SN’s echogenic area. Measurement was only performed ipsi-
lateral to the ultrasound probe. Statistical analysis was per-
formed using two tailed students t-test.
3. Results
Size measurements of SN hyperechogenicity in the NBIA
group yielded a mean area of hyperechogenicity of 0,39 cm2
þ/� 0,04 cm2 on the right and 0,35 cm2 þ/� 0,04 cm2.on the
left side. Compared to age-matched controls with a mean
size of 0,12 cm2 þ/� 0,01 cm2 for the right and 0,1 cm2 þ/�0.006 cm2 for the left side, there was a highly significant
difference (t-test p < 0.001; Fig. 1B). Most NBIA patients also
showed hyperechogenicity of the Nucleus ruber (data not
shown), however we were not able to detect this feature
consistently which may be due to technical difficulties,
because of heavy dystonic movement in some patients. A
correlation between age or sex and size of the hyper-
echogenic SN could be documented neither for the NBIA nor
the control group, as the absolute number of subjects in this
study is too low to provide solid statistical data in this regard.
In our study all examined patients displayed a hyper-
echogenicity of the SN. But total numbers of examined
patients were too low to calculate a solid Positive Predictive
Value (PPV).
Analysis of the globus pallidus via TCS in patients who had
a typical “Eye-of-the-tiger-sign” inMRI scans did not show any
valid abnormalities compared to controls. As there is evidence
that the lenticular nucleus is also altered on TCS in diseases
with heavy metal accumulation in the brain, we also paid
special attention to this particular brain region.10 However, we
were not able to demonstrate any valid changes in this region.

Fig. 1 e A: Sonographic measurement of SN in NBIA patients and controls Butterfly-shaped hypoechogenic mesencephalic
brainstem. The hyperechogenic area at the anatomical site of the SN in two NBIA patients of different ages (upper row),
compared to age-matched controls (lower row). B: Planimetric measurement values in NBIA patients compared to controls
Comparison between both groups illustrated for each side separately show a highly significant difference between NBIA
patients and controls (t-test<0.001).
e u r o p e a n j o u r n a l o f p a e d i a t r i c n e u r o l o g y 1 6 ( 2 0 1 2 ) 1 7 5e1 7 8 177
4. Discussion
Our findings demonstrate a highly significant increase of SN
hyperechogenicity in patients suffering from NBIA compared
to age-matched controls (Fig. 1B). Taking into account that
abnormal iron accumulation in the SN is a key feature in NBIA
andmore severe than in PD, our results suggest that TCS could
serve as an easy to use and valid tool for the early and
differential diagnosis in patients with movement abnormali-
ties with regards to the diagnosis of NBIA. New neuropatho-
logical studies showed differences in iron accumulation with
regard to the genetic subtype of NBIA.11 Especially in PKAN
there was no hard evidence for iron deposits in the SN.
However, recent MRI studies identifiedmetal accumulation as
causative for signal changes in the SN of PKAN patients.12 This
highlights the controversy of neuropthological findings on one
hand and technical information gained e.g. by MRI on the
other hand. In our cohort, all patients regardless of their
genetic background displayed a hyperechogenictiy in the SN.
Though it is intriguing to speculate that iron accumulation
leads to the demonstrated changes in midbrain TCS, even in
Parkinson’s disease, where TCS is widely accepted as
a method for early and differential diagnosis, the patholgical
correlate of the hyperechogenicity is still matter of debate.13
Unfortunately, TCS is not able to provide diagnostic discrim-
ination between the genetic subtypes of NBIA in our study due
to the limited number of patients. To examine this issue,
a large, internationalstudy would be needed to achieve a crit-
ical number of individuals presenting with different
genotypes.
In contrast to previous reports14 where it was shown that
SN echogenicity is slightly increased within the first 6 years of
age we did not observe hyperechogenicity of the SN our
control group. However, onset of NBIA is usually found
beyond the fifth year of age andmean age in our control group
was 13,9 years, a time-point where SN hyperechogenicity is
almost decreased to adult ratios.14 Moreover, the increase of
SN hyperechogenicity in NBIA patients is much more
pronounced compared to the reported mildly increased SN
ratios of healthy patients below the age of 10 and therefore
represents a robust finding. This fact also explains our diffi-
culties in discriminating the red nucleus in the patients group
consistently. Due to the markedly enlarged area of the sub-
stantia nigra it was easy to detect even in patients with dys-
tonic movements. Another limitation of TCS in general is the
absence of a proper bone window in 10e20% of adult patients.
In our experience this limitation appears especially with
increasing age. In case of NBIA, probably due to the young age
of patients, we did not observe any restrictions regarding this
shortcoming of TCS. Surprisingly, we did not find consistent
abnormalities in the basal ganglia, namely the globus pallidus,
which in NBIA with PKAN is known to display the pathogno-
monic “Eye-of-the-tiger-sign”. This may partly be due to the
heavy dystonic movements of the patients. In those cases
where we were able to detect signal abnormalities the degree
was substantially less intense compared to the reported cases
by Walter et al. in Wilson’s disease.15 However, as the total
number of patients examined in this study is quite low, this,
as well as the possible differences between subtypes of NBIA
should be addressed in a larger study. Still, we conclude that
TCS in NBIA could serve as a screening method ahead of the
gold standard examinations. One main shortcoming of
sonography in general is the mandatory experience of the
examiner. But as midbrain sonography also has become
widely used and accepted in the early and differential diag-
nosis of Parkinson’s disease since its first description in 1995,
we do not rate this as a permanent drawback.6
The clinical importance of our observations is underlined
by the fact, that the MRI as the gold standard does not always

e u r o p e a n j o u r n a l o f p a e d i a t r i c n e u r o l o g y 1 6 ( 2 0 1 2 ) 1 7 5e1 7 8178
show the “eye- of- the-tiger-sign”, as it may only appear
during disease progression or may even disappear during
course of the disease.3,16 Especially in light of at least one
report about an absent “eye-of-the-tiger-sign” in a patient
with a genetically proven PANK2 mutation,16 we think that
TCS is an interesting diagnostic tool, which could be used as
a screening method before MR-imaging and gene mutation
screens.
NBIA is not the only paediatric disease in which metal
deposition in the brain occurs e.g, copper accumulation in the
SN of subjects withWilson’s disease or metal accumulation in
early beginning spinocerebellar ataxias such as SCA 7 or 13.17
Taken together, our data suggest that TCS may be an
inexpensive and safe tool for the diagnosis of NBIA disorders
which could be used ahead of MR imaging and gene mutation
analysis in patients with an unexplained progressive move-
ment disorder.
Acknowledgements
We thank the German NBIA association “Hoffungsbaum e.V.”,
the patients and their families as well as the Department of
Paediatric Cardiology in Goettingen (Dr. Schill) for their
support. JL received assistance with travel expenses from
the German NBIA association. AW, KR, MB and PK have no
conflicts of interest.
Appendix. Supplementary data
Supplementary data related to this article can be found online
at doi:10.1016/j.ejpn.2011.07.009.
r e f e r e n c e s
1. Koeppen AH, Dickson AC. Iron in the Hallervorden-Spatzsyndrome. Pedriatic Neurol 2001;25(2):148e55.
2. Zhou B, Westaway SK, Levinson B, et al. A novel pantothenatekinase gene (PANK2) is defective in Hallervorden-Spatzsyndrome. Nat Genet 2001;28:345e9.
3. Hayflick SJ, Westaway SK, Levinson B, et al. Genetic, clinicaland radiographic delineation of Hallervorden- Spatzsyndrome. N Engl J Med 2003;348:33e40.
4. Gordon N. Pantothenate kinase-associatedneurodegeneration (Hallervorden-Spatz syndrome). Eur JPaediatr Neurol 2002;6(5):243e7.
5. Sethi KD, Adams RJ, Loring DW, el Gammal T. Hallervorden-Spatz syndrome: clinical and magnetic resonance imagingcorrelations. Ann Neurol 1988;24:692e4.
6. Becker G, Seufert J, Bogdahn U, Reichmann H, Reiners K.Degeneration of substantia nigra in chronic Parkinson’sdisease visualized by transcranial color-coded real timesonography. Neurology 1995;45:182e4.
7. Berg D, Godau J, Walter U. Transcranial sonography inmovement disorders. Lancet Neurol 2008;7:1044e55.
8. Berg D, Roggendorf W, Schroeder U, et al. Echogenicity of thesubstantia nigra-association with increased iron content andmarker for suceptibility to nigrostriatal injury. Arch Neurol2002;59:999e1005.
9. Becker G, Berg D. Neuroimaging in basal ganglia disorders:perspectives for transcranial ultrasound. Mov Disord 2001;16:23e32.
10. Walter U, Dressler D, Lindemann C, Slachevsky A, Miranda M.Transcranial sonography findings in Welding-relatedParkinsonism in comparison to Parkinson’s disease. MoveDisord 2008;23(1):141e5.
11. Kruer MC, Hiken M, Gregory A, et al. Novel histopathologicfindings in molecularly-confirmed pantothenate kinase-associated neurodegeneration. Brain 2011;134:947e58.
12. McNeill A, Birchall D, Hayflick SJ, et al. T2* and FSE, MRIdistinguishes four subtypes of neurodegeneration with brainiron accumulation. Neurology 2008;70:1614e9.
13. Stern MB. Transcranial Ultrasound in Parkinson’s Disease LancetNeurology 2008;7:376e7.
14. Iova A, Garmashov A, Androuchtenko N, et al. Postnataldecrease in substantia nigra echogenicity. J Neurol 2004;251:1451e4.
15. Walter U, Krolikowski K, Tarnacka b, Benecke R,Czlonkowska A, Dressler D. Sonogrgaphic detection of basalganglia lesions in asymptomatic and symptomatic Wilsondisease. Neurology 2005;64:1726e32.
16. Baumeister FA, Auer DP, Hortnagel K, Freisinger P,Meitinger T. The eye-of-the-tiger sign is not a reliable markerfor Hallervorden-Spatz syndrome. Neuropaedriatrics 2005;36:221e2.
17. Suedmeyer M, Saleh A, Wojtecki L, et al. Wilson’s diseasetremor is associated with magnetic resonance imaginglesions in basal ganglia structures. Mov Disord 2006;21(12):2134e9.