Embed Size (px)
Citation preview

Transformational
Leadership

Transformational Leadership
Strategic Planning TL1EO Nursing’s mission, vision, values and strategic plan align with the organization’s priorities to improve the organization’s performance.
Provide an example with supporting evidence of an initiative identified in the nursing strategic plan that resulted in an improvement in the nurse practice environment. Provide an example, with supporting evidence, of an initiative identified in the nursing strategic plan that resulted in an improvement due to a change in clinical practice.
Example #1 Improvement in Nurse Practice Environment: Implement Admit Discharge Team BACKGROUND/PROBLEM: Hospitals across the nation have been challenged with improving patient care and managing costs in an evolving healthcare industry that links care quality to reimbursement. For hospitals to be successful in this changing environment, they must work smarter and in a more cost-effective manner. The SJO Nursing Strategic Plan, under the nursing goal of Sacred Encounters, Objective #3 recognized these challenges and created a plan to “partner with other departments to improve the patient experience, patient flow and nursing workflow.” Objective #5 in the Nursing Strategic Plan under this same category of Sacred Encounters calls us to “support a Magnet environment while fostering change, innovation and stewardship.” Objective #1 under Sacred Encounters states “achieve top quartile rankings in nurse satisfaction.” All three of these objectives are critically important strategies in improving care and improving the nurse practice environment. In May 2012 CNO Katie Skelton, MBA, RN, NEA-BC, directed a team to come together to evaluate the complex components of the admission and discharge process to improve the nurse practice environment. In discussions at the Nursing Advisory Council meetings, Katie heard nurses talk about the challenges of providing “Perfect Care and Sacred Encounters,” particularly when they had a full assignment of patients and handled admissions and discharges as well. Staff shared that on days when they don’t have admits or discharges, they feel they can do a better job and manage their workload well; they feel in control over their practice. On those shifts when they have multiple admissions and discharges, the nurse can feel overwhelmed and does not see anyone available to help them. The charge nurses pitch in to help, but they are frequently busy with patient placement, rounding and staffing needs. Katie asked the Nursing Advisory Council members that if they had a team that could help them manage

Transformational Leadership
the admit and discharge process, do they think that this would improve the nurse practice environment. Unequivocally, they answered, “Yes!” GOAL STATEMENT: Smooth out the workflow and workload of the bedside RN by providing assistance from the Admit Discharge team to discharge at least 40% of patients from the five inpatient units identified. DESCRIPTION OF THE INTERVETIONS/INITATIVES/ACTIVITY(IES): In June 2012 a team assembled with the intent to evaluate all of the essential components required for a complete admission and discharge of the patient, seeking to support the clinical nurse at the bedside while maintaining safety and quality as the primary focus. Staff availability and bed availability were identified as two of the major barriers to patient flow, as there were patients waiting for admission in the Emergency Care Center (ECC) but no available staff or available bed on the receiving units. The team advocated for a pilot study of an Admit Discharge Team. Alex Wiggins, MSN, RN, NE-BC, Executive Director of Medical Surgical Nursing, was asked to lead this team. The team designed a four-week pilot, from July 9 through August 3, 2012 in which they would staff two full-time RNs in the roles of admit discharge nurses. These RNs would be based out of the ECC so they could actively “pull” patients out of the ECC. The goal initially in this pilot was to see if this new role could expedite patient flow, move patients out of the ECC more quickly, and help the receiving unit RN in managing the admission. Alex and Robert Garcia, MSN, RN, CMSRN, the manager of the ECC, met with staff daily to learn what was working and what wasn’t. The pilot proved successful at reducing the number of patients waiting in the ECC and provided the data Alex needed to advocate to the CNO for a permanent Admit Discharge Team. The pilot also identified that medication reconciliation was an important aspect of the admission process. Best practice in the literature recommended inclusion of a pharmacy tech onto the team, which was done after consultation with pharmacy leadership. Alex presented the pilot data to Katie in the fall of 2012. Alex had worked with a consultant, Sherry Cracroft, a specialist in workflow, staffing and productivity, who helped quantify the needed number of staff in this role in order to impact patient flow, nurse satisfaction, nurse workload and control over practice. Katie liked the innovative idea of smoothing out the nurse workload by providing frontline support to the staff. The team developed an outline of what duties the admit discharge nurse would be responsible for, and how we would measure our success. As the facilitator for the Nurse Advisory Council, Katie requested this be presented at Nurse Advisory Council for further discussion and buy-in regarding the proposed team and changes that would need to be made to support resources for a permanent team. Creation of the team would need to be budget-neutral with funding coming from several sources. To increase efficiency, nursing would need to keep the Medical Surgical units

Transformational Leadership
at least 80% occupancy. This would mean a consolidation of nursing units in order to decrease overhead costs and half- filled nursing units. The savings from these efforts would help fund the Admit Discharge Team. Creation of a Definitive Step-Down Unit was also identified as a strategy to help fund this team. Consolidating all patients requiring 1:3 level of care in one unit, rather than have them spread out over many units, would help manage that resource more closely. An additional funding source would come from the units that would be served by the Admit Discharge Team. Alex advocated with the nurse managers of these units to provide clinical hours to help fund the needed FTEs for the team. This planning work continued through budget preparation for the hospital fiscal year 2013, as it was complex with many moving parts. In July 2013 the Admit Discharge Team members were selected from internal candidates who exhibited strong service and educational expertise. Based on the varied clinical backgrounds of the nurses there was a readily available mentoring network within the team from the beginning. The pharmacy techs were hired from within the organization so they knew systems and processes already. To prepare for their new roles, the new clinical nurses on the Admit Discharge Team were orientated August 5 to 16, 2013 that included an introduction to the concept and the vision for team, role and responsibilities. The group reviewed a checklist of admission and discharge processes and met with representatives from Quality, Patient Safety and Home Health. Documentation and procedures were reviewed along with developing a standard of care for the discharge and admit process. The orientation also included meeting with the managers and charge nurses on the units to fully understand the specific needs of each individual patient population and understand specific physician preferences and needs. The Admit Discharge Team launched on August 19, 2013. Its focus was the five inpatient nursing units of General Surgery, Oncology, Orthopedics, Medical Telemetry and Pulmonary Renal.
TL1EO PARTICIPANTS:
PARTICIPANTS:
Name Discipline Title Department
Alex Wiggins MSN, RN, NE-BC Executive Director
Medical Surgical
Sherry Craycroft External Expert
Kathleen Penzes DNP, RN-C, NEA-BC Executive Director
Women’s Services
Cheryl Welp MHA, BSN, RN, CNM
Nurse Manager Pulmonary Renal and Observation
Robert Garcia MSN, RN, CMSRN Nurse Manager Emergency Care Center
Pat Brydges NBA, BSN, RN, ACM Executive Director
Case Management
Kathy Yezarski BSN, RN, ACM Nurse Manager Case Management
Jessica Koegel Facilitator St. Joseph Way

Transformational Leadership
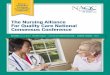
OUTCOME(S): We have learned a great deal during the past two years as we planned and implemented this Admit Discharge Team. Originally, we thought the best location for the team would be in the ECC. What we discovered is that locating the majority of the team on the nursing units is optimal, as they can begin assisting with patient discharges in the mornings in order to help the unit nurses prepare patients for home. This gives the nurses in all roles a chance to do their job well, and it makes help available for nurses when their workload increases. As seen in the graph below, we have been successful in achieving our goal of evening out the nurses’ workload by providing support for greater than 40% of the discharges for the nurses in the five inpatient units. Our data shows that we are well above the 40% goal at 64%. This innovative support for the bedside nurses has helped improve their work environment. TL1EO Figure 1 Discharges by Admit Discharge Team
Cathy Leong BSN, RN, CMSRN Nurse Manger Pulmonary Renal
Dana Madi AD, RN CN II Emergency Care Center
Sonomi Kawasaki DIP, RN CN II Emergency Care Center

Transformational Leadership
Example #2 Improvement in Clinical Practice: Fall Prevention - Behavioral Health Unit BACKGROUND/PROBLEM: The Nursing Strategic Plan supports the hospital’s strategic outcome goal of Perfect Care. One strategy identified under Perfect Care includes efforts to “reduce harm to patients by utilizing evidence-based practice.” Fall prevention is an initiative that supports the goal of mitigating and eliminating harm due to patient falls. Factors that predispose behavioral health patients to falls are significantly different than those in the general medical population. However, the severity and repercussions of a fall are equally as serious. Evidence demonstrates that falls among psychiatric patients are related to the severity of their psychiatric and psychotic symptoms, the presence of extrapyramidal symptoms, and psychiatric medication adjustment or use (Chan et al., 2013; Lee et al., 2010). Lee and colleagues (2010) reported a 78% increase in falls in patients receiving antipsychotic medications; the highest correlation occurred with typical antipsychotics. Although other psychiatric medications such as Selective Serotonin Reuptake Inhibitors and benzodiazepines have been associated with falls, drugs prescribed for co-occurring medical conditions including class 1 antidysrhythmics, antihypertensives, diabetic medications, and anticonvulsant drugs can also increase the risk of falling (Allen, Nesnera, & Robinson, 2012; Malik & Patterson, 2012). Fall risk is greatest in those more than 70 years of age when combined with the other identified predictors (Blair & Szarek). Among psychiatric patients, falls are associated with potential physical injury, pain and long-term disability. Falls often increase length of stay and hospital costs. The financial implications are compounded by Centers for Medicare and Medicaid Services regulations that disallow reimbursement for medical expenses incurred as a result of falls in the hospital setting. A review of SJO Behavioral Health Services (BHS) cases identified that patient falls increased at the end of calendar year 2013. More concerning was the increase of falls with injuries. During the last two months of 2013 falls with injuries increased to 6.24 and 2.50 per 1,000 patient days respectively. This was an increase from a mean of 1.365 per 1,000 patient days in the four prior months. This issue was recognized by hospital and the BHS department management as well as clinical nurses within the department. The Nursing Strategic Plan addressed falls throughout the organization, specifically identifying “the need to utilize the Falls Work Group to review fall incidents and hardwire processes to eliminate falls with harm.” The following goal was developed for this high risk population. GOAL STATEMENT: Reduce falls with injuries in BHS by improving identification of high risk patients and implementing population-specific strategies to reduce falls with injuries.

Transformational Leadership
DESCRIPTION OF THE INTERVETIONS/INITATIVES/ACTIVITY(IES): Laura Conley-Prince, MSN, RN-BC, CN IV, volunteered to lead efforts to address the increase in falls beginning in January 2014. She formed a Fall Prevention Sub-Committee within BHS comprised of day and night clinical nurses. They identified the following questions to inform the committee’s purpose and actions:
1) What factors contribute to patient falls in BHS? 2) What evidence-based interventions and protocols have demonstrated reduction
of falls among the behavioral health population? A multi-faceted approach was undertaken by the sub-committee. In an attempt to involve all stakeholders and increase buy-in for the project, the goals and processes were shared with the Unit-Based Council (UBC). The UBC approved the project and incorporated the goals into the department’s overarching annual goals and added the new sub-committee as a standing agenda item. Further support was sought and obtained from Beverly Hatch, MS, BSN, RN-BC, department manager; Tina Retrosi, BSN, RN, Patient Safety Officer; and Elizabeth Winokur, PhD, RN, CEN, clinical educator. Current evidence-based literature was obtained through internal and external searches. All evidence was appraised, summarized and synthesized using the Johns Hopkins research appraisal process. The Behavioral Health Unit Fall Prevention Sub-Committee utilized the BHS Fall Summary Reports and the incident reporting system to perform a comprehensive review of the falls occurring during the past six months of 2013. Additionally, Laura attended the hospital-wide Falls Work Group and Hospital Safety Committee for additional input and strategies. From January to March 2014 the sub-committee planned a broad-based approach to addressing falls:
Staff education regarding fall prevention and reduction including the dynamic nature of the behavioral health patient’s fall risk related to medication changes while hospitalized.
Improve incident reporting with detailed delineation of factors related to falls. Monthly, instead of quarterly, reporting of falls to determine trends and be able to
initiate timely corrective action. Changes in clinical practice included the development of the following processes:
A Centralized Falls Station was established in March 2014. This area within the nursing station contains fall reports, on-going staff education, patient fall risk identification items (yellow socks and arm bands) and documentation reminders.
A “Culture of Safety” was adopted to identify system failures that contributed to falls. This process was specifically undertaken to increase reporting of fall-related factors while decreasing the “assignment of blame,” a factor that the literature correlates with decreased or insufficient reporting of incidents.
Improved communication of fall risk status to the attending physician during daily rounds.

Transformational Leadership
Intensive staff education occurred between January and March 2014. Education included factors associated with falls, a standardized fall risk staff communication process utilizing SBAR, and expanded reporting in the incident reporting system.
In addition the team recognized that a new hospital-based fall assessment tool that was standardized across the health system was not sufficient for identifying fall risk among the behavioral health patient population. Laura sought support from department management and the patient safety officer to reinstate the Edmondson Psychiatric Fall Assessment Tool.
TL1EO PARTICIPANTS:
Name Discipline Title Department
Laura Conley MSN, RN-BC CN IV Behavioral Health Services
Shelly Aguilar MSN, RN-BC, Clinical Coordinator Behavioral Health Services
Vera Trone AD, RN-BC CN II; Unit Based Council Chair
Behavioral Health Services
Jimmy Salazar AD, RN CN II Behavioral Health Services
Diane Akullian AD, RN, CN II Behavioral Health Services
Marion Castello AD, RN-BC, CN II Behavioral Health Services
Mark Libonati BSN, RN CN II Behavioral Health Services
Donna Hume LCSW Social Worker Behavioral Health Services
Beverly Hatch MS,BSN, RN-BC
Department Manager
Behavioral Health Services
Tina Retrosi BSN, RN Patient Safety Officer
Quality Management
Elizabeth Winokur PhD, RN, CEN Clinical Educator Clinical Education
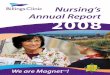
OUTCOME(S): The implementation of evidence-based practice fall prevention strategies had the desired effect on the clinical practice of nurses in BHS. Falls with injuries demonstrated significant decreases during the period following the interventions to a mean of 0.39 per 1,000 patient days, significantly less than before. The BHS falls sub-committee and the hospital-wide falls committee continues with monthly monitoring.

Transformational Leadership
TL1EO Figure 2 BHS Falls with Injuries
Return to TL home page