Embed Size (px)
Citation preview
Transition to Clerkship – Radiology
Marc Gosselin, MD
What Penguins Fell Off The Iceberg Since We Last Meet?
Introduction:‘Medicine is the Science of Uncertainty and
the Art of Probability’ – Sir William Osler
• Goals• ·Become familiar with and practice using the webPACS
system• ·Gain a basic approach to interpreting chest images• ·Gain a basic approach to interpreting bone images• ·Understand the use of the abdominal film • ·Understand the use of contrast• ·Understand practical issues with MRI
Key Points
• · Understand the need for clinical information when ordering and interpreting radiological studies
• · Understand how consultation with a radiologist before you order a study can help get the proper study
• · Try to learn about the tests that you are ordering your patient to experience during your rotations. You may never have another chance!
BEWARE:
The ‘Diamond Algorithm’
is Very Common!
Do NOT Be Fooled!
Basics for Radiology
• Contrast• MRI• Web sites• Images into a
presentation
Contrast
Contrast for x-ray related images is either:
Iodinated
Barium or Omni for Gastrointestinal tract
Contrast for MRI is gadolinium based
Some newer experimental agents are iron based.
Contrast
What it’s used for• Vessels• Tumor detection• Infection detection• Better anatomic detail
Contrast- When to order
• Brain (1st ? to ask - CT or just order MRI)– Looking for tumor– Infection
• Spine– Rarely need– Canal infection (epidural abscess, MRI better
choice)– Minimal use in “bone” tumors/mets
• Chest, Neck, Abd, pelvis– Very helpful and usually used (except Chest)
• Musculoskeletal system– Ask Radiologist– Mainly if need to know about vessels
Contrast - Risks
• Risk of death, at worst 1 in 130,000
• Renal failure, stroke, other severe reaction is low as well
• Contrast Induced Nephropathy may be more common than previously thought
Contrast – Risks – Allergy?
• Reaction to iodinated contrast agents are not true allergies– too small of agent to act as antigen– no antibodies ever detected
• Even if the patient has had a previous reaction, unlikely to have a reaction the next time– Although a prior reaction remains the best predictor
of a future adverse event, the likelihood is in the range of 8 – 25%
– If it were a true allergy the risk should approach 100%
• Other allergies or asthma– Only minimally predicts an increase risk– Not a reason to avoid injection– Asthma only predicts bronchospasm and then
only in active asthma cases– Allergy to shellfish is not a predictor (organic
iodine)
Contrast – Risks – Allergy?
Contrast-Induced Nephropathy
• Mainly a risk if there is some underlying compromise of renal function
• BUN as a guide to state of hydration• Creatinine as a guide to whether there is true
dysfunction• Better test is creatinine clearance (calculated)
Alice Mitchell, MD et al: ACADEMIC EMERGENCY MEDICINE 2012; 19:618–625
Nephropathy – Risk Factors• Diabetes• Recurrent renal stones• Recurrent UTI• Hx of bladder outlet obstruction• Recent events
– Major surgery– Dehydration!! (Adequate hydration prior and after
administration is 1st step to prevent nephrotoxicity)– Cardiogenic shock
• Other nephrotoxic agents– Gentamycin etc.– High-dose nonsteroidals– Certain chemotherapy agents
• Prior contrast reactions– Urticaria to anaphylactoid process– Use different agent (low osmolality, nonionic
isotonic dimmer (iodixanol))– Have equipment and expertise available to
treat– Pre-medicate with corticosteroids and/or
antihistamines• Prevents minor reactions• Not enough data to know if it prevents life-
threatening reactions
Contrast – Risks – Allergy?
MRI Safety
• Who can and can’t get scanned• What are the risks• What is the cost• What things to think/worry about
• Bottom line – risk vs. benefit vs. cost
MRI Safety Issues
• Metal– Ferromagnetic– Non-ferromagnetic– Location
• Orbit• Vessels/heart• Bones• Brain• Other
• Implantable devices– Pacemakers, ICDs– Pumps, stimulators– Wires, lines– Heart Valves– Aneurysm clips– Intravascular coils,
filters, & stents
MRI – other considerations
• Claustrophobia• Noise• Heating (SAR – specific absorption rate)• Tattoos & permanent cosmetics• Pregnancy and Breast feeding• Magnetic Field Strength
Web Sites
• American College of Radiology Appropriateness Criteria – www.acr.org/dyna/?doc=departments/appropria
teness_criteria/text.html• UpToDate (I Call it ‘FOX NEWS’)
– www.uptodate.com• The Number Needed to Treat
– www.nnt.com• OHSU Medical Student page
– http://sunweb1.ohsu.edu/radiology/med/
Web Sites• Virginia Web Site (sections on head CT,
Cervical spine, ICU chest film, ER body CT, Skeletal Trauma)
• http://www.med-ed.virginia.edu/courses/rad/• Virtual Hospital, Introduction to Abdominal
Radiology.http://www.vh.org/Providers/Lectures/icmrad/abdominal/Abdominal.html
• University of Washington, Radiology Review:http://uwcme.org/site/courses/legacy/threehourtour/
3rd Year Tips• Always try to helpful, in any way• Search for evidence on the disease or treatment
regarding your patients each day• Give presentations with literature from
different specialties…good career habit!• Try to refer back to your basic science classes as
much as possible! (Don’t throw your books away)
• Don’t rock the boat…at least not yet! (There are serious “land mines” out there for students…watch your step, watch what you say!)
3rd Year Tips• Generate Questions (to Yourself) Every day!
• Generate Options for Work up or Therapy Every day (to Yourself)
• Do NOT ‘Marry’ ANY Medical ‘Fact’ (Dogma) or ‘Standard of Care’! Watch out for ‘They say…’ or ‘Everybody knows…’
• Be Outraged (Quietly) When You see any of this: (I’ll likely get Vocal - you don’t…yet)
White Zinfandel is NOT a wine!
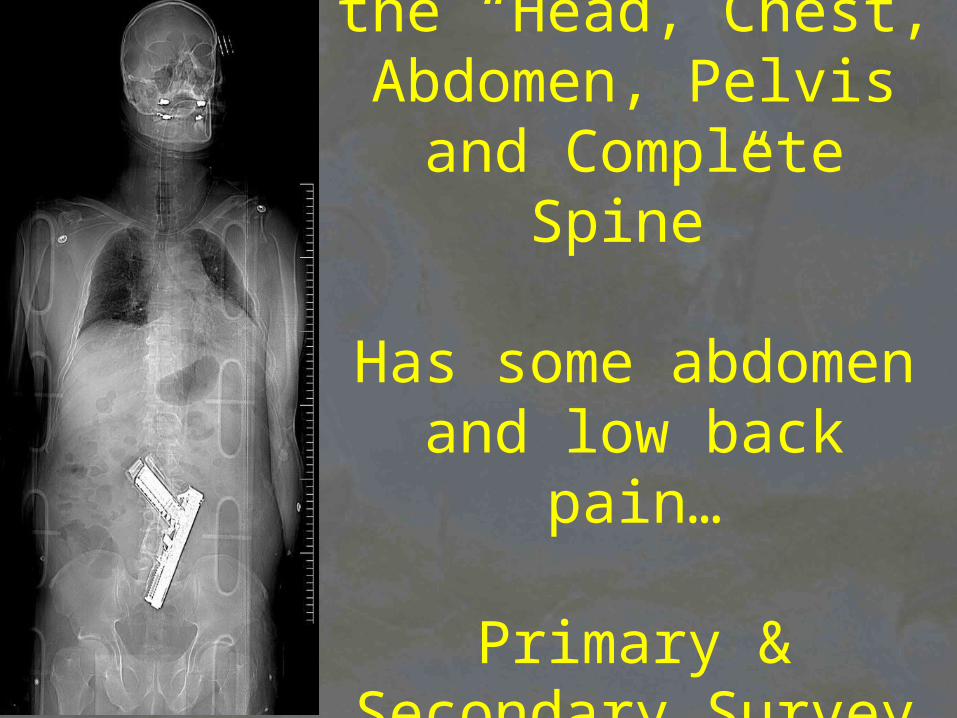
Scout for a CT of the “Head, Chest, Abdomen,
Pelvis and Complete Spine”
Has some abdomen and low back pain…
Primary & Secondary Survey were ‘Done’