Embed Size (px)
Citation preview

Translocation (2;3) in Hematologic Malignancies
Irma Slavutsky, Mabel Labal de Vinuesa, Irene Larripa, Juan Dupont, and Sonia Brieux de Salum
ABSTRACT: Cytogenetic studies have revealed nonrandom involvement of some chromesomes in specific structural abnurmalities in human neoplasias. In this report we present three patients with t(2:3) associated with hematologic malignancies, and review the pertinent literature. These findings lead us to regard the region between 3q26 and 3q29 as implicated in chromo- somal changes in these disorders, whereas, no vulnerable point has been observed in chro- mosome #2. We suggest that these translocatians may activate genes on chromosome #3 related to these neoplasius.
INTRODUCTION
The nonrandom involvement of certain chromosomes in human neoplasia has been well documented [1]. In hematologic condit ions, in particular, some specific struc- tural chromosomal abnormalit ies have been observed. Among these, different anomalies of chromosome #3 have been reported in cases of preleukemia, throm- bocythemia, acute nonlymphocyt ic leukemia (ANLL} [2-6], and malignant lym- phoma [7-11], whereas, chromosome #2 is less involved in rearrangements in these disorders.
We report herein the presence of t(2;3) in three patients: two with malignant lymphoma and one with ANLL M4 type; in addition, we summarize hematologic cases in the literature with this translocation.
METHODS
Chromosome analysis was performed on cells from biopsed lymph nodes [12] and bone marrow I"131. Chromosome preparations were stained with conventional Giemsa or banded with t rypsin-Giemsa [141. The International System of Human Cytogenetic Nomenclature [15] was used.
Cases were classified according to the Working Formulat ion [16] for non-Hodg- kin lymphomas and FAB criteria for leukemias [17]. The clinical stage of lymphoid malignancies was established using the Ann Arbor classification [18].
From the Cytogenetic Department of the Instituto de lnvestigaciones Hemtol6gicas Mariano R. Castex. Academia Na(:iomd de Medicina. Research Career of CONICET [I. S., M. L. de V.. I. 1..), the Department of Clinical Hematcdogy [1. I).). and Head. Department of Cytogenetics (S. B. de S.). Buenos Aires. Argentina.
Address requests for reprirlts to Dr. Irma Slavutsky, Departamento de Citogen~tica, /nsti- tufa de Investigaciones Hematol6gicas, Academia National tie Medicina, Pacheco de Melo 308]. 1425-Buenos Aires, Argentina.
Receiwrd November 13, 1984: accepted August 7, 1985.
335
~: 1986 Elsevier Science Publishing Cc~., Ira:. Cancer Genet Cytogenet 21:335-342(19861 52 Vanderbilt Ave.. New York, NY 10017 0165-4608,'86/$03.50
336 I. Slavutsky et al.
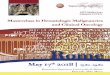
TABLE 1 Characterist ics of the patients s tudied
Clinic:al Disease Case Sex/age Sample Diagnosis stage stage
1 M/51 LN NHI,-FSCC IIIA Diagnosis 2 M/50 LN NHL-IB III B Diagnosis 3 t".'2 8 13M ANI .I,.M4 - - Diagnosis
I.N. lymph node; BM. bone marrow; NHI,. non- t tnd~kin lymphoma: FSCC. full icular small cleaved cell: lB. immunob- lasli¢.:: ANI,I,. acute imnly lnphablas t ic leukemia,
CASE R E P O R T S
Case 1
Case 2
S. L. is a 51-year-old white male (Tahle 1), who noticed a node in his left supracla- vicular area in March 1981. It was found to be a fol l icular small c leaved cell malig- nant lymphoma. After staging, liver and bone marrow biopsies were normal, the patient did but show abnormal lymphangiography in both left and right iliac and paraortic areas (stage Ill A). He received eight cycles of cytoxan, vincris t ine, and prednisone every 21 days. Restaging was normal and he cont inues in remission at the time of this writing.
R. F. was a 50-year-old white male (Table 1) who had a tumoral left testicle, fever, and malaise in Apri l 1981. An orch idec tomy was performed and a diagnosis of lymphoma was reached. A second biopsy in the cervical area confirmed the diag- nosis of immunoblas t ic mal ignant lymphoma. A left paraort ic mass was disclosed by palpat ion and on a computer tomography scan (stage IIIE B). He received eight cycles of BACOP (bleomycine, adr iamycin , cytoxan, vincris t ine, and prednisone) and achieved comple te cl inical remission. In May 1982 he compla ined of headache, d iplopia , and vomiting. Cerebrospinal fluid was analyzed and immunoblas t ic - l ike blasts were shown to be present in a concentra t ion of 200/mm a. He received several re induct ions of intrathecal methotrexate and radiat ion therapy, but d ied with per- sistent CNS involvement in December 1982.
Case 3
A. D. was a 28-year-old white female (Table 1}. In 1977 a thyroid node was excised and a diagnosis of Hodgkin 's disease, nodular sclerosis made. After staging, both iliac areas had involved nodes (stage IIIE A). She received nitrosourea, vinblast ine. prednisone, and procarbazine, monthly for 6 months. After achieving comple te re- mission she received a cycle of chemotherapy every 2 months for 1 year. In Apri l 1980, 2 years post therapy, a pancytopenia was recognized, with 3% of blasts in the per ipheral blood and 10% in the bone marrow. In addi t ion, the pat ient ' s bone mar- row smear showed myelo id hyperplas ia . She received 4 units of red cells. In De- cember 1980, remission of the Hodgkin 's disease cont inued. Her hematologic counts were hemoglobin 9.10 g/dl; WBC 5800; the differential counts revealed 25% polymorphonuclears , 55% lymphocytes , 14% monocytes , 6% blasts, and a platelet count of 80000/mm:'. She had a hypoplas t ic bone marrow with 50°/,, of myeloid blasts plus promyelocytes . A diagnosis of myelomonocyt ic leukemia was made. She refused intensive t reatment and was lost to follow up; she died 8 months later.
t(2;3) in H e m a t o l o g i c M a l i g n a n c i e s 337
T a b l e 2 Cy togene t i c s t u d i e s
Chromosome numbers Karyotyped ceils/
Case <45 45 46 47 48 Total cells analyzed Karyotypes
1 1 3 4 6 1 8 /15
2 4 5 15 1 - - 14,25
3 6 21 5/27
47,XY, - 2,-- 3, + der(3}t(2:31(q14:q271, ~- del(4](pl 3). - 6, + del (6J(q21 ). + 21/46,
XY. - 2, -- 3, + der(3)t(2;3)(q14:t1271, + del(4)[p13).- 6, + del(6)(q21 ).
46,XY,-- 3, ~ der{3)t(2:3)(q23;q271, - 6, -~11
45,XX.- 3, ~- der[3]t(2;3)(q12:q26]. - 7
R E S U L T S
C h r o m o s o m e c o u n t s , ma rke r s , a n d k a r y o t y p e s of the p a t i e n t s s t u d i e d are s h o w n in Table 2. L y m p h n o d e ce l l s f rom cases w i t h the m a l i g n a n t l y m p h o m a a n d b o n e m a r r o w cel ls f rom the ANLL p a t i e n t s we re a n a l y z e d .
C a s e 1
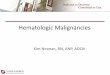
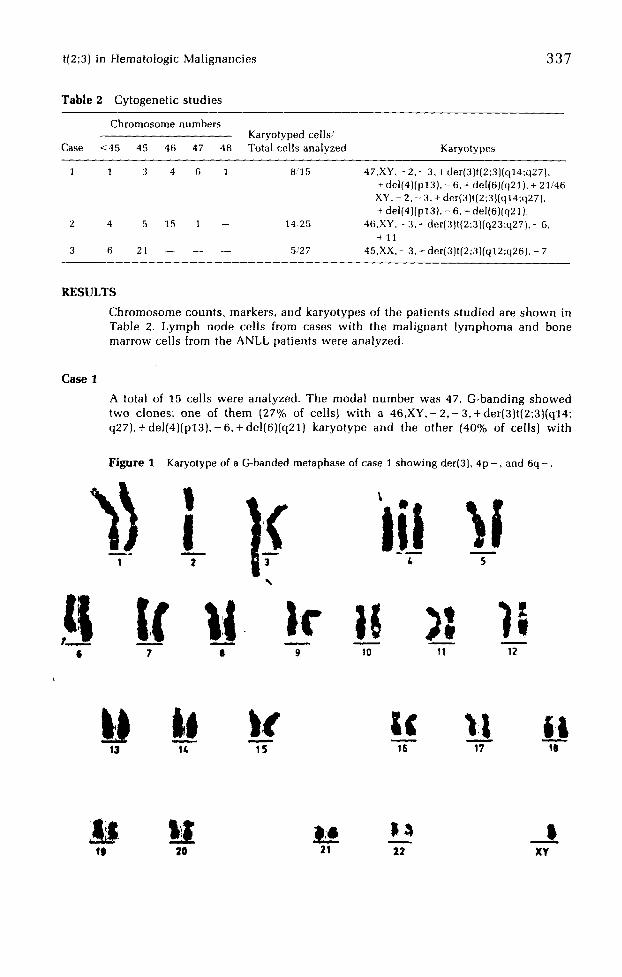
A total of 15 ce l l s were a n a l y z e d . T h e m o d a l n u m b e r was 47. G - b a n d i n g s h o w e d two c lones : o n e of t h e m (27% of cel ls) w i t h a 4 6 , X Y , - 2 , - 3 , + d e r ( 3 ) t ( 2 ; 3 ) ( q 1 4 " q 2 7 ) , + d e l ( 4 ) ( p 1 3 ) , - 6 , + d e l ( 6 } I q 2 1 ) k a r y o t y p e a n d the o t h e r [40% of cells} w i t h
F i g u r e 1 Karyotype of a G-banded metaphase of case 1 showing der(3}, 4p - , and 6q - .
Ill "+I /. 5
,ll li' I,-I+ ): , ~, i 9 ,o ,t 12
1~ ~o 2i 22 !
XY
338 I. Slavutsky et al.
a 47,XY,- 2 , - 3, + der(3)t(2:3)(q14;q27), + del(4)(p13),- 6, + del(6)(q21), + 21 karyo- type (Figs. 1 and 3). Examination revealed random gain and loss of chromosomes in the remaining aneuploid cells. No normal cells were found.
Case 2
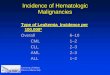
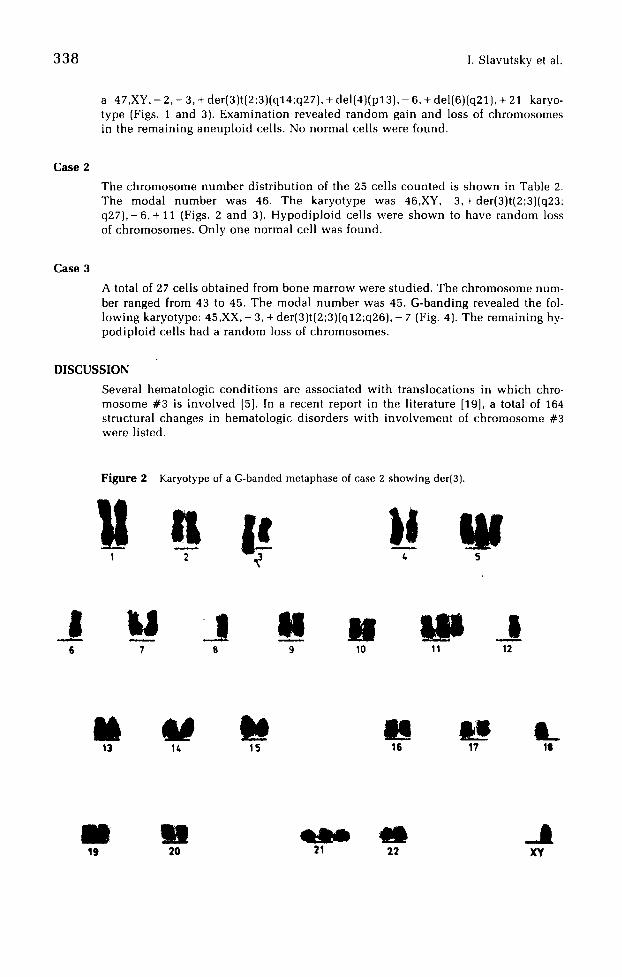
The chromosome number distr ibution of the 25 cells counted is shown in Table 2. The modal number was 46. The karyotype was 46,XY,-3,+der(3)t(2:3)(q23: q 2 7 ) , - 6 , + 11 (Figs. 2 and 3). Hypodiploid cells were shown to have random loss of chromosomes. Only one normal cell was found.
Case 3
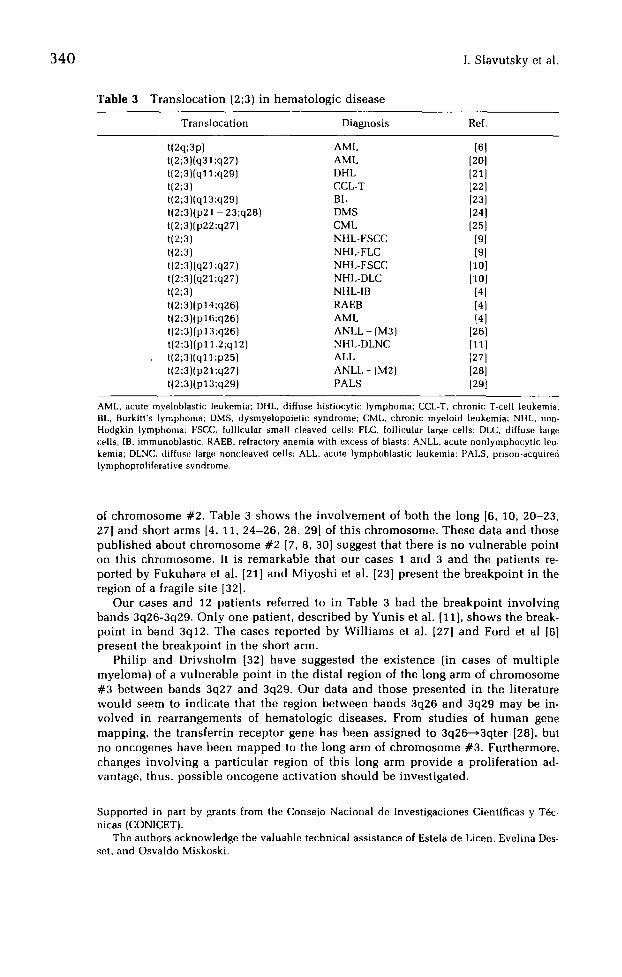
A total of 27 cells obtained from bone marrow were studied. The chromosome num- ber ranged from 43 to 45. The modal number was 45. G-banding revealed the fol- lowing karyotype: 45,XX, - 3, + der(3)t(2;3)(q12;q26), - 7 (Fig. 4). The remaining hy- podiploid cells had a random loss of chromosomes.
DISCUSSION
Several hematologic condit ions are associated with translocations in which chro- mosome #3 is involved [5]. In a recent report in the literature [19], a total of 164 structural changes in hematologic disorders with involvement of chromosome #3 were listed.
Figure 2
U Karyotype of a G-banded metaphase of case 2 showing der(3).
2 L, 5
l U 7
!1 I t 141 i l l 8 9 ' 10 11 12
il
13 U N M
14 15 16 17 t
111
M M w ~ _ t 19 20 71 ?.2 XY
t(2;3) in Hematologic Malignancies 339
,.+.... I P " . •
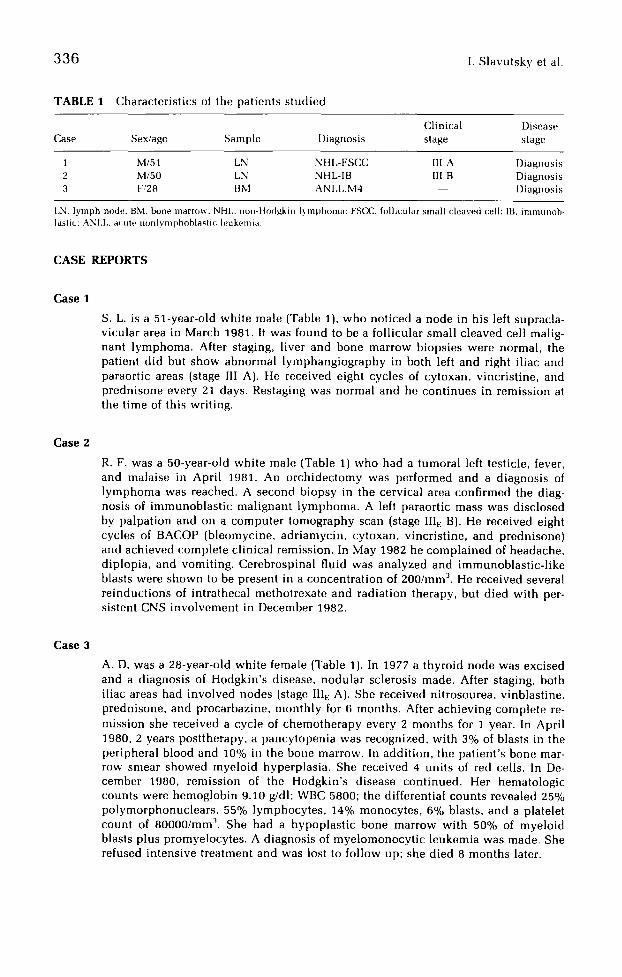
~ 2 tla el a 2 dl~"(3) 3 2 dl,r(3) 3
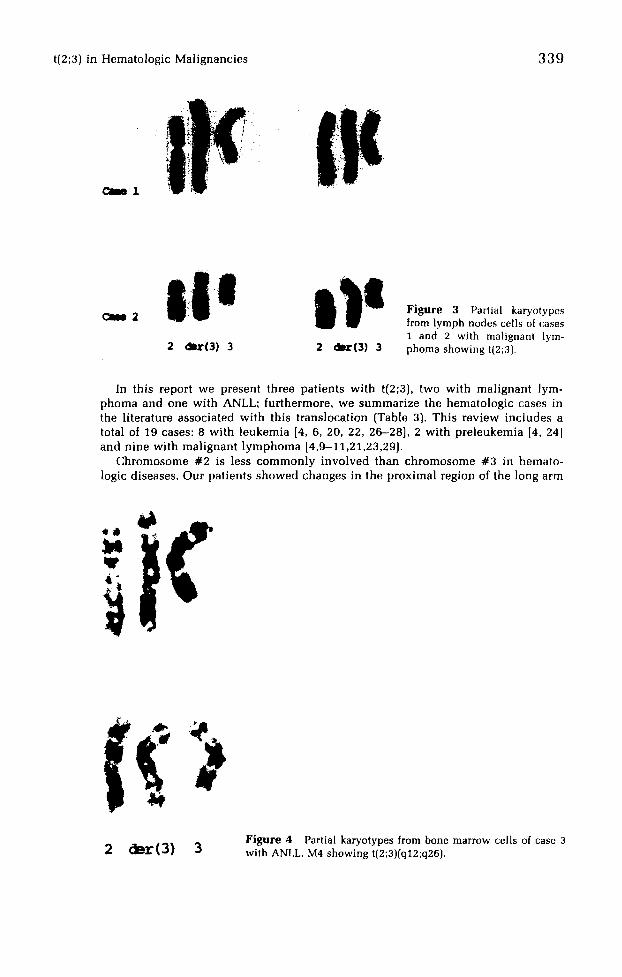
Figure 3 Partial karyotypes from lymph nodes cells of cases 1 and 2 with malignant lym- phoma showing t(2;31.
In this report we present three patients with t(2;3), two with malignant lym- phoma and one with ANLL; furthermore, we summarize the hematologic cases in the literature associated with this translocation (Table 3). This review includes a total of 19 cases: 8 with leukemia [4, 6, 20, 22, 26-28], 2 with preleukemia [4, 24] and nine with malignant lymphoma [4,9-11,21,23,29].
Chromosome #2 is less commonly involved than chromosome #3 in hemato- logic diseases. Our patients showed changes in the proximal region of the long arm
( ) Figure 4 Partial karyotypes from hone marrow cells of case 3
2 glint ( 3 ) 3 with ANLL, M4 showing t(2;3)(q12;q26).
340 I. Slavutsky et al.
Table 3 Translocation (2;3) in hematologic disease
Translocation Diagnosis Ref.
t(2q;3p) AML [6] t(2;3)(q31 ;q27) AML [20l t(2;3)(ql 1 ;q29) I)HL [21l t(2;3) CCL-T [22] t(2;3)(q13;q29] BL [23] t(2;3)(p21 - 23;q28) DMS [24] t(2;3)(p22;q27) CML [251 t(2;3) NHL-FSCC [9] t(2;3] NHL-FLC [9] t[2;3)(q21 ;q27) NHL-FSCC [10] t(2;3)(q21;q27) NHI,-DLC [101 t(2;3) NHL-IB [41 t[2;3)[p14;q26) RAEB [4] t(2;3)(p16;q26) AML [4] t(2;3)(pl 3;q26) ANLL - (M3) [26] t(2;3](p 11.2;ql 2) NHI,-I)LN(~ [11 ] t(2;3)(q11 ;p25) AI,L [27] t(2;3)(p21 ;q27) ANLL - (M2) [281 t(2;3)(p13;q29) PALS 129 t
AML, acute myeloblastic leukemia: Dill., diffuse histiocyti¢: lymphoma; CCL-T. chronic T-cell leukemia; BL, Burkitt's lymphoma; DMS. dysmy,alopoietic syndrome; CMI., chronic myeloid leukemia; NIIL, non- Hodgkin lymphoma; FSCC, follicular small cleaw,~d cells: FLC, follicular large cells: DLC, diffuse large cells; IB, immunoblastic; RAEB, refractory anemia with excess of blasts: ANLL, acute uonlymphocytic leu- kemia; DLNC, diffuse large noncleaved cells; ALL. acute lymphoblastic leukemia; PALS. pristm-acquired lymphoproliferative syndrome.
of chromosome #2. Table 3 shows the involvement of both the long [6, 10, 20-23, 27] and short arms [4, 11, 24-26, 28, 29] of this chromosome. These data and those published about chromosome #2 [7, 8, 30] suggest that there is no vulnerable point on this chromosome. It is remarkable that our cases 1 and 3 and the patients re- ported by Fukuhara et al. [21] and Miyoshi et el. [23] present the breakpoint in the region of a fragile site [32].
Our cases and 12 patients referred to in Table 3 had the breakpoint involving bands 3q26-3q29. Only one patient, described by Yunis et al. [11], shows the break- point in band 3q12. The cases reported by Williams et al. [27] and Ford et al [6] present the breakpoint in the short arm.
Philip and Drivsholm [32] have suggested the existence (in cases of multiple myeloma) of a vulnerable point in the distal region of the long arm of chromosome #3 between bands 3q27 and 3q29. Our data and those presented in the literature would seem to indicate that the region between bands 3q26 and 3q29 may be in- volved in rearrangements of hematologic diseases. From studies of human gene mapping, the transferrin receptor gene has been assigned to 3q26-~3qter [28], but no oncogenes have been mapped to the long arm of chromosome #3. Furthermore, changes involving a particular region of this long arm provide a proliferation ad- vantage, thus, possible oncogene activation should be investigated.
Supported in part by grants from the (]onsejo Nacional de Investigaciones Cientlficas y T6c- nicas (CONICET).
The authors acknowledge the valuable technical assistance of Estela de Licen, Evelina Des- set, and Osvaldo Misknski.
t(2;3) in H e m a t o l o g i c M a l i g n a n c i e s 341
REFERENCES
1. Sandberg AA (1980): Chromosomes in Human Cancer and Leukemia. Elsevier North-Hol land, New York
2. Norrby A, Ridel B, Swolin B, Westin J (1982): Rearrangement of chromosome n°3 in a cas~ of preleukemia with thrombocytosis. Cancer Genet Cytogenet 5:257-263.
3. Sweet DL, Golomb tIM, Rowley JD, Vardiman JM (1979): Acute myelogenous leukemi~ and thrombocythemia associated with an abnormality of chromosome n°3. Cancer Gene Cytogenet 1:33-37.
4. Mecucci C, Vermaelen K, Tricot G, Louwagie A, Michaux JL, Bosly A, Thomas J, Barbier D, Van Den Berghe H (1983): 3 q - , 3q+ anomaly in malignant proliferations in humans Cancer Genet Cytogenet 7:1-18.
5. Sandberg AA, Hecht BK, Ondreyco SM, Prieto F, Hecht F (1982): Translocations involving chromosomes #3 and #12: Hematologic diseases associated with abnormalit ies of thes~ chromosomes. Cancer Genet Cytogenet 7:1-18.
6. Ford JH, Pittman SM, Singh S, Wass EJ, Vincent PC, Gunz FW (1975): Cytogenetic basi., of acute myeloid leukemia. J Natl Cancer Inst 55:761-765.
7. Mark J, Ekedhal C, Dahlenfars R (1978): Characteristics of the banding patterns in non. Hodgkin and non-Burkitt lymphomas. Hereditas 88:229-242.
8. Mark J, Dahlenfors R, Ekedhal C (1979): Recurrent chromosomal aberrations in non-Hodg. kin and non-Burkitt lymphomas. Cancer Genet Cytogenet 1:39-56.
9. Yunis JJ, Oken MM, Kaplan ME, Ensrud KM, Howe RR,Theologides A (1982): Distinctive chromosomal abnormalities in histologic subtypes od non-Hodgkin's lymphoma. New En- gland J Med 307:1231--1236.
10. Bloomfield CD, Arthur DC, Frizzera G, Levine EG, Petersen BA, Gajl-Peczalska KJ (1983) Nonrandom chromosome abnormalit ies in lymphorna. Cancer Res 43:2975-2984.
11. Yunis JJ, Oke MM, Theologides A, Howe RB, Kaplan ME, (1984): Recurrent chromosomal defects are found in most patients with non-Hodgkin's lymphoma. Cancer Genet Cytoge- net 13:17-28.
12. Slavutsky [, Vinuesa MI, de, Dupont J, Mondini N, Salum SB de (1981): Abnormalit ies oJ chromosome n°l: Two cases with lymphocytic [ymphomas. Cancer Genet Cytogenel 3:341-346.
13. Vinuesa ML de, Slavutsky I, Dupont J, Di Risio CB de, Salum SB de (1981): Phi-negative chronic myelocytic leukemia (CMI,) with an unusual karyotype. Cancer Genet Cytogenel 3:347-351.
14. Seabright M (1971): Rapid banding technique for human chromosomes. Lancet ii:971-972.
15. ISCN (1978): An international system for human cytogenetic nomenclature. Cytogenet Cell Genet 21:309--404.
16. Pathologic Classification Project, National Cancer Institute (1982): The non-Hodgkin's lymphomas. Sponsored study of classifications of non-Hodgkin's lymphomas: Summary and description of a working formulation for clinical usage Cancer 49:2112-2135.
17. Bennet JM, Cah~vsky 13, Daniel MT, Flandrin G, Galton DAG, Gralnick HR, Sultan C (1982): The French-Amer ican-Br i t i sh (FAB) Co-operative Group: Proposals for the clas- sification of the myelodysplastic syndromes. Br J Hematol 51:189-199.
18. Carbone PP, Kaplan HS, Musshoff K, Smithers DW, Zuliana M (1971): Report of the com- mittee on Hodgkin's disease staging classification. Cancer Res 31:1860-1861.
19. Mitelmau F (1983): Catalogue of chromosome aberrations in cancer. Cytogenet Cell Genet 36:1-515.
20. Oshimura M, Hayata I. Kakati S, Sandberg AA (1976): Chromosomes and causation of human cancer and leukemia XVII. Banding studies on acute myeloblastic leukemia (AML). Cancer 38:748-761.
21, Fukuhara S, Rowley JD, Variakojis D, Sweet DL (1978): Banding studies on chromosomes in diffuse "hist iocytic" lymphomas: Correlation of 14q + marker chromosome with cytol- ogy. Blood 52:989-1002.
22. Finan J. Daniele R, RowIands Jr D, Nowell P (1978): Cytogenetics of chronic T cell leuke- mia, including two patients with a 14q+ translocation. Virchows Arch B Cell Pathol 29:121-127.
342 I. S l a v u t s k y et al.
23. Miyoshi I, Hamasaki K, Miyamoto K, Nagase K, Narahara K, Kitajima K, Kimura I, Sato J (1981): Chromosome translocations in Burkitt 's lymphoma. N Engl ] Med 304:734.
24. Rowley JD, Golomb HM, Vardiman JW (1981): Nonrandom chromosome abnormalit ies in acute leukemia and dysmyelopoietic syndromes in patients with previously treated malig- nant disease. Blood 58:759-767.
25. Fleischman EW, Prigogina EL, Volkova MA, Frenkel MA, Zakhartchenko NA, Konstanti- nova LN, Puchkova GP, Balakirev SA (1981): Correlations between the clinical course, characteristics of blasts cells and karyotype patterns in chronic myeloid leukemia. Hum Genet 58:285-293.
26. Fort International Workshop on Chromosomes in Leukemia, 1982 (1984): Chromosomes in acute promyelocytic leukemia. Cancer Genet Cytogenet 11:288-293.
27. Williams DL, Look AT, Melvin SL, Roberson PK, Dahl G, Flake T, Stass S (1984): New chromosomal translocations correlate with specific immunophenotypes of childhood acute lymphoblastic leukemia. Cell 36:101-109.
28. Barbieri D, Vermaelen K, Van Den Berghe H (1984): Preliminary data on the in vitro pro- liferation pattern and karyotypic characteristics in cells of patients with ANLL. Cancer Genet Cytogenet 11:1-10.
29. Takeuchi J, Ochi H, Han T, Ozer H, Henderson ES, Sandberg AA (1985): Clonal chromo- some abnormalities in prison-acquirect lymphoproliferative syndrome. Cancer Genet Cy- togenet 15:7-16.
30. Reeves I~R, Pickup VL (1980): The chromosome changes in non-Burkitt lymphomas. Hum Genet 53:349-355.
31. Human Gene Mapping Workshop 7 (1984): Cytogenet Cell Genet 37:1-398.
32. Philip P, Drivsholm A (1976): G-banding analysis of complex aneuploidy in multiple my- eloma bone marrow cells. Blood 36:729-735.