Embed Size (px)
Citation preview

Trauma in the Older AdultEpidemiology and Evolving Geriatric Trauma
Principles
Stephanie Bonne, MD, Douglas J.E. Schuerer, MD*
KEYWORDS
� Geriatric � Trauma � Fractures � Falls
KEY POINTS
� From the initial time of injury, the overall experience of an elderly person who sustainsa traumatic injury can be very different from that of a younger patient with trauma, andspecial consideration should be made to properly triage and treat the geriatric patientwith trauma.
� Once a traumatic event occurs, there are several comorbidities that complicate recoveryfrom the trauma. Greater than 50% of the geriatric trauma population has underlyinghypertension, and greater than 30% have heart disease.
� The widespread use of medications and polypharmacy adds to the challenge of evaluatingand treating the elderly patient with trauma. Older patients may be using medications,such as b-blockers, that will mask abnormal vital signs, or may have pacemakers in place,which can further confound the primary survey.
There is little debate that the world’s population continues to age,1,2 and as such thereare increasing numbers of older patients presenting with traumatic injuries than in thepast. The current population of both the United States and the developed world isaging, creating a new subset of patients with trauma, the geriatric patient with trauma.If we are to study this population, we must quantitatively define it. In the case oftrauma, recent data suggest that mortality as adjusted for injury severity scale (ISS)increases at the age of 70 years, defining the population older than 70 as distinctfrom those younger than 70 years, and making the age of 70 the cutoff at which toconsider a patient with trauma elderly or geriatric.3 This notion is distinct fromAdvanced Trauma Life Support (ATLS) teaching, which recommends transport toa trauma center of any patient older than 55 years, or the Eastern Association forthe Surgery of Trauma (EAST) guidelines, which recommend considering any patient
Washington University in St Louis, 660 South Euclid Avenue, Campus Box 8109, St Louis, MO63110, USA* Corresponding author.E-mail address: [email protected]
Clin Geriatr Med 29 (2013) 137–150http://dx.doi.org/10.1016/j.cger.2012.10.008 geriatric.theclinics.com0749-0690/13/$ – see front matter � 2013 Elsevier Inc. All rights reserved.

Bonne & Schuerer138
older than 65 years as elderly.4,5 Although there is no consensus on an age cutoff fora patient with trauma to be considered elderly, the age of 65 is most often used whenconsidering a patient “elderly” or “geriatric” in the trauma literature. It is well recog-nized that the geriatric trauma population requires special consideration with regardto diagnosis and treatment, and it is important for the trauma clinician to be awareof the special needs of these patients.
EPIDEMIOLOGY
By 2050, it is expected that there will be nearly 90 million adults older than 65 yearsliving in the United States, representing more than one-fifth of the population.6 In addi-tion to the increase in the volume of the geriatric population, one can expect moreinjuries to occur in this population as they continue to live more independent andactive lifestyles. At present, patients older than 65 years account for 23% of all traumaadmissions, and trauma represents the fifth leading cause of death in this popula-tion.7,8 Because of the high prevalence of multiple comorbidities in the elderly, thereis an increased likelihood of death or severe disability following trauma.8 Up to one-third of all patients presenting with an ISS greater than 15 can be expected to diebefore leaving the hospital.9 In addition, the economic costs, as well as the societalcost and loss of life, are higher following trauma to an elderly patient. Falls are theleading cause of trauma in the elderly. There is approximately a one-third risk of fallfor geriatric adults each year.10 With an average hospital cost of $18,000 (UnitedStates, 2012) per fall, and further costs associated with long-term nursing carefollowing trauma, the economic implication of all trauma, but specifically of standinglevel falls, to the elderly is astonishing.11,12 Looking forward, the social and economicimplications of the expected increase in geriatric trauma cannot be overlooked, andclinicians must continue to strive toward a more standardized and evidence-basedapproach to the diagnosis and treatment of these patients.
MECHANISMS OF GERIATRIC TRAUMA
Several factors place the geriatric population at particular risk for traumatic events,and for subsequent delayed recovery from trauma. Conditions that predisposepatients to incurring trauma are seen in higher prevalence in the older population.Weakness or generalized deconditioning resulting from chronic illnesses can lead toan increased rate of falls or other accidents in these patients. Loss of visual acuity,balance and gait instability, slowed reaction times, and cognitive impairments arealso important disabilities that may lead to an increased incidence of traumatic eventsin the elderly. Often these issues are not recognized before trauma, and cognitivedysfunction can be seen up to 35% of the time in the geriatric visitor to the emergencydepartment, but is only recognized 6% of the time.13 Trauma itself is also an increasedrisk factor for future traumas, with elderly patients who have sustained trauma in thepast being 3 times more likely to have a future traumatic event.14 Because this partic-ular constellation of problems is seen in the elderly, prevention of geriatric traumashould be addressed by all clinicians caring for a geriatric patient. Trauma preventionin patients who are at high risk because of the aforementioned disabilities should beaddressed by the geriatric primary care physician (Fig. 1).The mechanisms of trauma are not unique to this particular population, but
because geriatric trauma presents at such a higher rate than in the younger popula-tion, they can be considered to be different mechanisms than those observedyounger patients with trauma. Unlike their younger counterparts, elderly patientswith trauma usually sustain blunt trauma rather than penetrating trauma. Falls

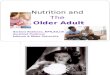
Fig. 1. Pie chart of injury mechanism in the elderly patient. MVC, motor vehicle accident.
Trauma in the Older Adult 139
account for nearly three-quarters of all traumas in the geriatric population, with motorvehicle accidents accounting for nearly all of the remaining 25% of injuries. Pene-trating trauma and other mechanisms make up only 4% of total trauma in the geriatricpopulation.9 Among the elderly patients who fall, nearly 90% experience simple falls,such as falls from standing. Despite being simple mechanisms, the multiple comor-bidities in the elderly population, along with the need for rehabilitation, make fallsa significant medical and economic event in the life of these patients.15 Falls associ-ated with blunt cerebral injury and long bone fractures lead to the greatest morbidityand mortality.7,8 About one-quarter of all elderly victims of motor vehicle accidentssustain chest trauma, such as flail chest and rib fractures, which can complicatepreexisting cardiopulmonary disease and lead to pneumonia or respiratory failure,complications which are known to have particularly high morbidity and mortality.16
Car accidents also cause mortality at almost double the rate for the elderly as for theiryounger counterparts when adjusted for injury severity.16 Finally, although pene-trating trauma remains rare in the elderly population, it is associated with highermorbidity, longer stays in the intensive care unit (ICU), and longer overall hospitalstays when compared with younger patients.17 When caring for a geriatric patientwith trauma after a fall or motor vehicle accident, it is important to be aware of themost likely injuries and injury patterns, reviewed herein. These injury patterns mayvary from those seen to arise from the same mechanism in a younger patient, so itis important to be aware of the particular injury patterns seen in the elderly so thatoccult injuries are not missed.
TRIAGE AND EVALUATION OF THE GERIATRIC PATIENT WITH TRAUMA
From the initial time of injury, the overall experience of an elderly person who sustainsa traumatic injury can be very different from that of a younger patient with trauma, andspecial consideration should be given to proper triage and treatment of the geriatricpatient with trauma. Nursing homes or assisted care facilities, where elderly patientsoften reside, are a unique location, where health care workers are available and mayattempt to treat a traumatic event on site. However, this can actually delay the traumaevaluation of a patient who might otherwise be taken to an emergency departmentsooner if they reside in the community. Likewise, families or other laypersons may

Bonne & Schuerer140
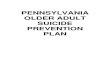
underestimate the severity of a traumatic event to their elderly family member,because the mechanism may seem trivial or their loved one may not initially showsigns and symptoms of having a major underlying injury. Once the emergency medicalservices (EMS) system is activated, it is critical for the emergency responder to appro-priately evaluate and triage the patient. For nearly 20 years it has been recognized thatelderly patients are consistently undertriaged to major trauma centers, possiblybecause emergency responders do not recognize potential major injuries or are notfully aware of all the potential comorbidities in the elderly patient, or because of poten-tial age bias on the part of the responders.18,19 Undertriage is particularly troublesomebecause trauma outcomes with regard to both morbidity and mortality have beenshown to be improved when the geriatric patient is taken immediately to a high-level trauma center.20 In addition to undertriage, it has been shown that geriatricpatients who are transferred to a trauma center but do not meet trauma activationcriteria on initial evaluation, will often have occult injuries, or their comorbid conditionswill act in synergy with their traumatic event to lead to higher morbidities for that partic-ular injury.21,22 When adjusted for injury severity, geriatric patients have consistentlyhigher levels of morbidity and mortality across all levels of injury.23 This fact has ledmany trauma surgeons to advocate for age alone to be a criterion for activation ofthe trauma system and transfer to a Level 1 trauma center, although the age thatshould be the threshold for such activation is debated.21,23 Level 1 trauma centerscan be identified at www.traumamaps.org. Current guidelines suggest that age alone,in the absence of any diagnosable injury, is insufficient for activation of the traumateam; however, the threshold for activation should be lower in patients who showhemodynamic instability or any potentially life-threatening injuries, such as severefractures, abdominal trauma, or chest trauma.3 In addition to improved outcomesfrom immediate evaluation at a higher-level trauma center, geriatric patients mayalso benefit from a dedicated geriatric trauma service, which may be increasinglyfound at higher-level trauma centers or academic centers (Fig. 2).24
Once an elderly patient arrives at a trauma center, the staff must be careful to eval-uate the geriatric patient as is appropriate for their advancing age. Vital signs andphysical examination can be deceptive in these patients, whomay exhibit examinationcharacteristics very different from those of younger patients. Although the ATLSprotocol should be followed for geriatric patients just as it is for younger patients, thereare some differences in the normal physiology of elderly patients that will make theirevaluation and treatment more challenging. Even among patients who are not taking
Fig. 2. Algorithm for field triage of the elderly patient with trauma. Current triage guide-lines suggest transfer to a trauma center provides optimal care. Those with obvious injuryor relative hypotension (low normal blood pressure but very low for patients with preexist-ing hypertension) should be triaged to a higher-level trauma center, depending on stateregulations.

Trauma in the Older Adult 141
confounding medications, vital signs can be falsely reassuring. Increased mortalityhas been shown among elderly patients with heart rates greater than 90 beats/minand systolic blood pressure less than 110 mm Hg, whereas the same increase inmortality is not seen until 130 beats/min and 95 mm Hg in younger patients.25 Elderlypatients also subjectively report less pain for the same severity of injury than do theiryounger counterparts, potentially masking injuries or falsely reassuring staff that aninjury is less severe than it actually is.26 Mental status examinations and GlasgowComa Scale (GCS) scoring can be particularly difficult in the geriatric patient, whomay have preexisting cognitive deficits, hearing impairment, or other factors thatcan confound these examinations.27 Clinical neurologic examination has also beenshown to be unreliable in detecting significant hemorrhage in patients with minorhead trauma.28 The difficulty in using normal clinical judgment and assessment inelderly patients has led many emergency medicine and trauma surgeons to advocatefor a low threshold of reliability in ancillary studies on the geriatric patient withtrauma.27
COMORBIDITIES IN GERIATRIC TRAUMA
Once a traumatic event occurs, several comorbidities complicate recovery from thetrauma. Greater than 50% of the geriatric trauma population has underlying hyperten-sion, and greater than 30% has heart disease.7 Other conditions that can complicateevaluation and management of the patient with trauma include diabetes, previouscerebrovascular events, chronic obstructive pulmonary disease (COPD), dementia,arrhythmias, and endocrine disorders; all of which are present in greater than 10%of the geriatric trauma population.7 Other common diseases in the elderly, such ascommunity-acquired infections, cancers, and chronic renal failure, also lead toincreased risk of poor outcomes following trauma.9,29 The comorbid conditions thatconfer the highest risk of mortality in the geriatric population are hepatic disease, renalinsufficiency, and cancer.30 The presence of congestive heart failure, particularly inpatients who take b-blockers or are anticoagulated, can confer a 5- to 10-foldincreased risk of death following trauma.31 Because the geriatric population is gener-ally less healthy at baseline, they are at increased risk of certain types of trauma and atincreased risk of in-hospital complications once a trauma has occurred. Comorbidconditions, therefore, become a major factor in the evaluation and treatment of theelderly patient with trauma. Closely related to this are the medications a patient withtrauma may be taking for the aforementioned comorbidities.The widespread use of medications and polypharmacy adds to the challenge of
evaluating and treating the elderly patient with trauma. Older patients may be usingmedications, such as b-blockers, that will mask abnormal vital signs, or may havepacemakers in place, which can further confound the primary survey. Preinjuryb-blocker use does confer an increased risk of mortality, particularly when con-founded with warfarin or other cardiac medications.27 This risk may be due to under-recognition of tachycardia owing to b-blocker use, conferring a falsely reassuringclinical picture. In the secondary survey, geriatric patients may bleed more rapidlyfrom seemingly minor wounds because of widespread use of anticoagulants and anti-platelet agents. Because falls and head trauma comprise such a large percentage oftotal trauma in the elderly, anticoagulation becomes a significant problem that theemergency or trauma clinician can expect to encounter often.In addition to cardiac medications and anticoagulation, other medications can
confound the treatment of trauma. Steroids, often prescribed for COPD in theelderly, can cause reduced wound healing or can lead to clinical adrenal

Bonne & Schuerer142
insufficiency in the critically ill patient, and have been shown independently to leadto a 1.6- to 5-fold increased incidence of death in the geriatric trauma population.26
Antipsychotics may render neurologic examinations unreliable, and antidopaminer-gic agents used for Parkinson disease may change the neurologic examination ofthe extremities. Eye drops or systemic medications taken for glaucoma may alterthe pupillary examination, as may corneal or other eye implants. It is crucial to docu-ment the pupillary examination on arrival, and document any ophthalmologic historyto avoid confusion among care providers during the patient’s hospitalization. Inaddition to taking into account the patient’s home medications when evaluatingthe patient, it is important to consider which home medications are necessary tocontinue during the stay in hospital. Patients may exhibit adverse effects to thesudden discontinuation of antidepressants, antipsychotic agents, and in particularto antidopaminergic agents. In short, the polypharmacy seen more often in theelderly must be carefully considered, from the point of initial evaluation throughthe entire treatment course of the geriatric patient, so as not to miss occult injuriesor to cause additional clinical problems by discontinuing a chronic medication(Table 1).
PATTERNS OF INJURY AND SPECIFIC INJURIES
In addition to global considerations of geriatric patients, there are special consider-ations for each injury. In the case of head-injured patients, there is a linear relationship
Table 1Physiologic and functional preexisting differences in the older adult
Organ System NormalPotential Differences in the OlderPatient
Vital signs Increased mortality if HR >130beats/min or SBP <95 mm Hg
Increased mortality if HR >90 beats/minor SBP <110 mm Hg
Neurologic No baseline deficits Baseline deficits (dementia, stroke,hearing loss)
Report less pain for equivalent injuries,potentially limiting injury discovery
Cardiovascular No baseline deficits, nohypertension
No cardiac medications
Baseline hypertensionMedications that affect blood pressure
and heart rate (b-blocker, calcium-channel blocker, amiodarone)
History of heart failure
Pulmonary Normal functional residualcapacity
Potential smoker
Decreased functional residual capacityChronic obstructive pulmonary disease
Renal Normal renal function Decreased glomerular filtration rate
Coagulation Normal coagulation status On blood-thinning medicationsincluding ASA, warfarin, and plateletinhibitors
Skeletal Normal bone density Osteoporosis, leading to easier fracturerate
Medications Minimal medications Polypharmacy that can change mental,hemodynamic, renal, andcoagulation status
Abbreviations: ASA, acetylsalicylic acid; HR, heart rate; SBP, systolic blood pressure.

Trauma in the Older Adult 143
between age and mortality following head injury, such that even within the populationolder than 65 there is increased risk of death with increasing age.32 Among thosepatients who do not die from their head trauma, poor outcomes are common andalso increase with increasing age.33 These patients may present with a very mildmechanism for head injury or may have few hard neurologic signs, such as neurologicdeficits, weakness, or altered mental status, on initial evaluation, but may still havevery significant underlying subdural or epidural hematomas.34 The widespread useof anticoagulation in the elderly population has led to a large body of literature evalu-ating the effects of anticoagulation on the patient with trauma. Some studies haveshown an increased risk of mortality with warfarin use in all patients with trauma,whereas other students show that in the absence of head trauma, warfarin usedoes not lead to increased mortality in the patient with trauma.31,35 However, if theelderly patient with head trauma is taking warfarin, there is a significantly increasedrisk of fatal intracranial hemorrhage.31 Patients who are anticoagulated on arrival,particularly those with head trauma, should be rapidly corrected, and there shouldbe a low threshold to repeat brain imaging with any clinical neurologic change.36
The GCS is an unreliable clinical tool in this scenario, and rapid and repeated use ofcomputed tomography (CT) of the head becomes the essential means of identifyingincreased intracranial pressure in this scenario.37 In the case where medical historyis unavailable or unreliable, there should be a low threshold for the use of head CTin the elderly population, because of both the high prevalence of occult injuries andthe rising prevalence of anticoagulant use.34 Common rules such as the NEXUS-IIspecifically rule out patients older than 65 when determining who does not needa CT.38 Even with use of intracranial pressure (ICP) monitoring and careful pharmaco-logic management of ICP, elderly patients have poorer autoregulatory mechanisms,which subsequently lead to a 30% decrease in the Glasgow Outcome Score afterhead injury in comparison with their younger counterparts.39
In the case of cervical spine injuries, elderly patients have mechanisms and risks forspine injury similar to those of their younger counterparts; however, the prevalence ofcervical stenosis or degenerative spine disease is more common in this population.Also, there is little need to consider future cancer risk from radiation in the elderlypatient. Common predictors of cervical spine injury include focal neurologic deficits,concomitant head injury, and high energy mechanism. Although similar predictorsare seen in the younger population, the older population requires its own risk stratifi-cation to guide clinicians to suspect cervical spine fractures, because an apparentlylesser injury can be so much more devastating in the older population.40 One canexpect a lower energy mechanism, such as a fall from standing, to cause greater injuryto an elderly patient, because of the higher likelihood that the patient has preexistingdegenerative spine disease or cervical stenosis. Also, because the elderly patient ismost likely a victim of blunt trauma, most will require cervical spine evaluation. Earlyspine evaluation, a low threshold for involvement of a spine service, and the carefuluse of cervical spine immobilization are all essential in ensuring that a low energymechanism does not become a devastating neurologic injury.Thoracic trauma in the elderly is most likely to be blunt, and most likely to be from
amotor vehicle accident. Fractures that might seem clinically insignificant in a youngerpatient, such as isolated rib fractures or clavicle fractures, may represent significantforce and be associated with significantly higher morbidity in elderly patients.8 Ribfractures in the elderly can be particularly worrisome, because of the increasedmorbidity and mortality associated with as few as 3 or fewer nondisplaced rib frac-tures. In addition, the increase in number of rib fractures increases the rate of compli-cations.41 Elderly patients are likely to develop pulmonary contusions or pneumonia

Bonne & Schuerer144
from rib fractures, even isolated rib fractures.42 Pneumonia following a rib fracture canbe a devastating complication for an elderly patient who, at baseline, does not havethe pulmonary reserve and ability to generate a forceful cough that a younger patientmay have. It is essential to aggressively manage rib fractures in elderly patients,including, when indicated, epidural anesthesia and rib fixation. Pain control will helpwith pulmonary toilet and use of incentive spirometry (IS). Admission should bestrongly considered if more than 2 rib fractures and/or IS use is found to be poordespite analgesia.Abdominal trauma in the geriatric patient does not differ significantly from abdom-
inal trauma in the younger patient. The same mechanisms and grades of solid organinjury apply to the older adult. Early experience with operative management for bluntabdominal trauma in the geriatric population showed poor outcomes; however, morerecent studies have shown that operative management is possible and, in fact, pref-erable to nonoperative management based on age criteria alone, likely attributablein part to improved perioperative care and improved surgical optimization.43,44 Infact, a patient older than 55 years will be more likely than their younger counterpartsto fail nonoperative management of blunt splenic trauma.45 Of course, in cases ofpenetrating abdominal trauma or bowel injury, operative exploration must be per-formed regardless of age criteria.Much like the other injuries discussed, pelvic fractures in the elderly have a higher
incidence of complications and mortality than in the younger population. The injurypattern of pelvic fractures in the geriatric population tends to be different to that inthe younger population, specifically with a higher incidence of lateral compressionfractures.46 These fractures are more likely to cause hemorrhage that requires inter-vention, such as angiography.47 The trauma surgeon should be aware that the elderlypatient with a pelvic fracture may have pelvic bleeding that often otherwise goesunrecognized both clinically and radiographically on simple radiographic or CT exam-inations.48 In addition, older age and concomitant long bone fracture, often seen in theelderly, impart a higher likelihood of finding occult bleeding with angiography.49 Someinvestigators therefore advocate the liberal use of angiography in the geriatric popu-lation, regardless of hemodynamic stability, because of the very high incidence ofoccult bleeding.The treatment of extremity orthopedic injuries among the elderly does not vary sig-
nificantly from treatment of the younger population. The evaluation of concomitantneurovascular injury and the treatments of surgery, splinting, and reduction arelargely the same as for the younger population. The exception is the long bone femurfracture, or hip fracture. This fracture was formerly considered a fatal event for theelderly osteoporotic patient, but with advances in pinning and plating, this is nolonger true. The incidence of this injury remains high, however, as more womenlive well past menopause and experience osteoporosis, among other risk factors.50
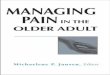
Low bone density imparts an increased risk for all types of long bone fractures, butparticularly for hip fractures. It is also important to consider the surgical risk ofa patient in whom operative fixation may be indicated. Should the elderly patienthave multiple surgical risk factors, it may be more prudent for the orthopedic surgeonto simply splint or cast a fracture rather than expose the patient to the risk of anes-thesia. This approach needs to be carefully considered in juxtaposition to thepatient’s functional goals and outcomes, and the potential risks of deep vein throm-bosis or occupational deconditioning if the patient is unable to use the extremity fora period of time. Although orthopedic management may not be drastically differentfor the elderly patient with trauma, careful medical management must be consideredfor the geriatric patient (Fig. 3).

BRAIN
Baseline defects Dementia StrokeLess pain reportingSDH more likely due to cerebral atrophyVision changes
Figure of specific concerns for the older trauma patient
EAR
Hearing loss
LUNGS
Emphysema (potentially creating pneumothorax)Decreased functional residual capacity COPD
KIDNEY/BLADDER
Decreased glomerularfiltration rateIncreased UTI
CARDIOVASCULAR
Baseline hypertensionBaseline heart failureCardiac medications Heart rate control Blood pressure control Anticoagulation
GLOBAL
PolypharmacyDiabetes mellitusPsychiatric medicationsBeta-BlockersCa Channel BlockersAnticoagulation Platelet inhibitors Blood thinners
NECK
OsteophytesArthritisMore difficult intubationEasier to fracturespinal column
SKELETAL
OsteoporosisMore frequent fractureFractures with minimal energy injury
Fig. 3. Specific concerns for the older trauma patient.
Trauma in the Older Adult 145
INTENSIVE CARE MANAGEMENT OF GERIATRIC PATIENTS WITH TRAUMA
Once a patient’s management course has been set, or their injuries have been defini-tively managed, the patient may require a course of treatment in the ICU. Intensivecare medicine for the elderly patient, and specifically the elderly patient with trauma,differs from that for younger patients. Patients older than 65 years have a significantlygreatermortality ratewhenmatched for injury severity and comorbidities. This situationactually leads to decreased use of ICU resources, as many elderly patients will diebefore reaching the ICU and thus use little or no ICU resources.51 Once resuscitationhas begun, it is clear that the geriatric population has less physiologic reserve andtherefore requires more rapid, yet judicious, treatment.52 In addition, patients who

Bonne & Schuerer146
are stable on initial evaluation will often have measureable hemodynamic compromisewhen invasive monitoring has been performed.53 This occult hemodynamic compro-mise can present a unique challenge to the clinician who does not retain a high indexof suspicion. Renal function in the elderly patient will differ from that in the youngerpatient owing to decreased renal blood flow and declining renal mass, therefore urineoutput alone is a poor clinical indicator of resuscitation. Creatinine clearance alsobecomes a much more important marker of renal function because creatinine alonecan be deceptive in the elderly patient with lower muscle mass.54 Although there hasbeen insufficient evidence to suggest the routine use of pulmonary artery catheters inthis population, the judicious use of invasive monitoring is warranted in the patientwith an unclear clinical picture. Newer studies have shown a benefit to elderly patientswho receive pulmonary artery catheter monitoring, and this monitoring has beenshown to be low risk.55,56 Even though there are no specific end points for resuscitationin these patients, the optimization of cardiac index and the use of base deficit as amea-sure of the status of resuscitation may be useful to the clinician.57 It remains the clini-cian’s choice to place an invasive line in a patient who is thought to warrant one;however, it canbebeneficial in guiding the resuscitationof theolderpatientwith trauma.In addition to the hemodynamic changes seen in the elderly, the pulmonary
mechanics of the elderly individual vary significantly from those of younger patients,leading to challenges in ventilator management in the older population. Elderlypatients with trauma have a distinct increase in the vulnerability to pulmonary compli-cations after trauma, owing to the decrease in their pulmonary reserve.58 The ability ofa nonventilated older patient to compensate for metabolic disturbances is decreased,which may cloud the clinical picture for the clinician because the patient may havea normal respiratory rate while becoming progressively hypoxic and hypercarbic.59
In addition, when matched for injury severity, elderly patients are more likely todevelop nosocomial infections, such as pneumonia, which in turn lead to longer lengthof stay in the ICU and hospital, and a higher mortality.60 To reduce these complica-tions, early and aggressive treatment of injuries, pulmonary toilet, pain control, andearly mobilization must be implemented to give such fragile patients the best oppor-tunity for a good outcome.It is known that elderly patients have a higher morbidity and mortality following
trauma than younger patients, which may lead to different recommendations regard-ing continuing care and withdrawal of care by clinicians. Elderly patients may not havethe reserve to survive a long hospitalization following trauma, nor may they be able toparticipate in intensive rehabilitation following neurologic or orthopedic injuries. Thesepatients may be intubated, sedated, confused, or delirious following their injuries, andtherefore may be unable to participate in conversations regarding their goals of care.The discussion a clinician has with the patient’s family must therefore take into consid-eration the increased length of stay, increased complications, and long recovery timeassociated with an elderly patient following trauma.61 Because the majority of thesepatients will survive their injuries, a frank discussion of rehabilitation expectations,disposition, and other outcomes besides mortality is key to patient and family under-standing of the severity of injury.62
THE TRAUMA TEAM FOR GERIATRIC PATIENTS
The unique difficulties of caring for the patient with trauma have led to the develop-ment of trauma teams for geriatric patients at many institutions. While still awaitinggood data, the concept is to treat this population as a distinct specialty. In the pastsuch patients may have end up with the orthopedic, medicine, or trauma service.

Trauma in the Older Adult 147
Although each specialty does its part well, often it may not as accurately address theother medical issues. For instance, the medical practitioner will likely address thecardiac problems, but may not as aggressively treat a few rib fractures. In such a situ-ation the patient would benefit from a traumatologist as well.To improve on the old system, a trauma team for geriatric patients should be staffed
with interested individuals from each of the disciplines, along with mid-level providersto bring the consistency needed in treating these individuals. Protocols to addresswell-proven strategies should be written, created, and followed. Early involvementwith anesthesia and prevetted anesthesia workups should take place, limiting delaysto the operating room for unnecessarily thorough medical clearance. These teamsshould be led by geriatric traumatologists, who have experience in leading a multidis-ciplinary team, and should include orthopedic surgeons and neurosurgeons, geriatri-cians, dedicated therapists, social workers, dieticians, and others, all experienced intreating and appropriately dispositioning such patients. While an inpatient, homehealth could also perform evaluation of fall hazards to help prevent future injuries.In short, the team approach used in the ICU should be used to improve patientoutcomes.
OUTCOMES IN GERIATRIC TRAUMA
As geriatric patients are studied, improvement in care of their trauma can be expected.Although geriatric patients have a higher mortality owing to multiple factors alreadydiscussed, the patients who do survive will eventually achieve some level of functionaloutcome following trauma. Their comorbidities, while playing a role in their survivaland recovery, do not appear to affect their overall outcome.63 For example, althoughgeriatric brain-injured patients have a longer recovery time and require more inpatientcare, they will generally improve in functional status and eventually reach the samerehabilitation goals as their younger counterparts.64 These results, however, are agedependent, with geriatric patients older than 80 years having poorer functionaloutcomes than those aged 65 to 80.65 There are also promising results regardinglong-term survival following trauma, with long-term survival of several years aftertrauma for geriatric patients who are discharged from hospital.66 Such lead datashould inspire optimism in the clinician caring for the geriatric patient with trauma,who can be confident that in most patients, survival and functional outcomes will begood should the patient survive hospitalization. The effort spent, therefore, in caringfor and rehabilitating the older patient with trauma is not in vain, and provides goodquality of life and longer quality time for these patients.Future research that will likely yield improvement for the elderly patient must focus
on early recognition of instability and on falls, which make up approximately 75% oftrauma in elderly patients. Efforts in early recognition have included triaging the elderlyto trauma centers, but proof that this prospectively improves survival is not yet avail-able. Also, research that helps EMS recognition of relative hypotension, and thustriages the patient appropriately, may improve survival. However, research that workstoward reducing the incidence of falls, especially recurrent falls, and determining riskof falls of this population, will begin to address the single largest reason for injury in thispopulation.In conclusion, elderly patients with trauma must be triaged, evaluated, and treated
differently to their younger counterparts. We must learn, as we did with children, thatolder adults have unique physiologic and structural differences that leave them at anincreased risk of mortality from even minor trauma. Early recognition of these differ-ences can lead to a better mortality rate and a more productive recovery after trauma.

Bonne & Schuerer148
REFERENCES
1. O’Neill S, BradyRR,KerssensJJ, et al.Mortality associatedwith traumatic injuries inthe elderly: a population based study. Arch Gerontol Geriatr 2012;54(3):e426–30.
2. Lustenberger T, Talving P, Schnuriger B, et al. Impact of advanced age on out-comes following damage control interventions for trauma. World J Surg 2012;36(1):208–15.
3. Caterino JM, Valasek T, Werman HA. Identification of an age cutoff for increasedmortality in patients with elderly trauma. Am J Emerg Med 2010;28:151–8.
4. American College of Surgeons Committee on Trauma. Geriatric trauma. In: ATLS:student course manual. 8th edition. Chicago: ACLS; 2008. p. 247–57.
5. The Eastern Association for the Surgery of Trauma. Geriatric trauma (update).Available at: http://www.east.org/resources/treatment-guidelines/geriatric-trauma-(update). Accessed July 20, 2012.
6. The Department of Health and Human Services, Administration on Ageing. Pro-jected future growth of the older population. Available at: http://www.aoa.gov/aoaroot/aging_statistics/future_growth/future_growth.aspx#age. Accessed July20, 2012.
7. Thompson HJ, McCormick WC, Kagan SH. Traumatic brain injury in older adults:epidemiology, outcomes, and future implications. J Am Geriatr Soc 2006;54:1590–5.
8. Keller JM, Sciadini MF, Sincalir E, et al. Geriatric trauma: demographics, injuriesand mortality. J Orthop Trauma 2012;26(9):e161–5.
9. Labib N, Nouh T, Winocour S, et al. Severely injured geriatric population:morbidity, mortality and risk factors. J Trauma 2011;71:1908–14.
10. Ganz DA, Bao Y, Shekelle PE, et al. Will my patient fall? JAMA 2007;297:77–86.11. Roudsari BS, Ebel BE, Corso PS, et al. The acute medical care costs of fall-
related injuries among the US older adults. Injury 2005;36:1316–22.12. Hartholt KA, Polinder S, Van der Cammen TJ, et al. Costs of falls in an ageing
population: a nationwide study from the Netherlands (2007-2009). Injury 2012;43:1199–203.
13. Carpenter CR, DesPain B, Keeling TN, et al. The Six-Item Screener and AD8for the detection of cognitive impairment in geriatric emergency departmentpatients. Ann Emerg Med 2011;57(6):653–61.
14. McGwin G, May AK, Melton SM, et al. Recurrent trauma in elderly patients. ArchSurg 2001;136:197–203.
15. Siracuse JJ, Odell DD, Gondek SP, et al. Health care and socioeconomic impactof falls in the elderly. Am J Surg 2012;203:335–8.
16. Lee WY, Cameron PA, Bailey MJ. Road traffic injuries in the elderly. Emerg Med J2005;23:42–6.
17. Nagy KK, Smith RF, Roberts RR, et al. Prognosis of penetrating trauma in elderlypatients: a comparison with younger patients. J Trauma 2000;49:190–3.
18. Phillips S, Rond PC 3rd, Kelly SM, et al. The failure of triage criteria to identifygeriatric patients with trauma: results from the Florida trauma triage study.J Trauma 1996;40:278–83.
19. Chang DC, Bass RR, Cornwell EE, et al. Undertriage of elderly trauma patients tostate-designated trauma centers. Arch Surg 2008;8:776–81.
20. Meldon SW, Reilly M, Drew BL, et al. Trauma in the very elderly: a community-based study of outcomes at trauma and nontrauma centers. J Trauma 2002;52:79–84.
21. Demetriades D, Sava J, Alo K, et al. Old age as a criterion for trauma team acti-vation. J Trauma 2001;51:754–7.

Trauma in the Older Adult 149
22. Lehmann R, Beekley A, Casey L, et al. The impact of advanced age on traumatriage decisions and outcomes: a statewide analysis. Am J Surg 2009;197:571–4.
23. Shifflette VK, Lorenzo M, Mangram AJ, et al. Should age be a factor to changefrom a Level II to a Level I trauma activation? J Trauma 2010;69:88–92.
24. Mangram AJ, Mitchell CD, Shifflette VK, et al. Geriatric trauma service: a one-yearexperience. J Trauma Acute Care Surg 2012;72(1):119–22.
25. Hefferman DS, Thakkar RK, Monahan SF, et al. Normal presenting vital signs areunreliable in geriatric blunt trauma victims. J Trauma 2010;69:813–20.
26. Gibson SJ, Helme RD. Age-related differences in pain perception and report. ClinGeriatr Med 2001;17:433–56.
27. Zuercher M, Ummenhofer W, Baltussen A, et al. The use of Glasgow Coma Scalein injury assessment: a critical review. Brain Inj 2009;23(5):371–84.
28. Mack LR, Chan SB, Silva JC, et al. The use of head computed tomography inelderly patients sustaining minor head trauma. J Emerg Med 2003;24:157–62.
29. Bochicchio GV, Joshi M, Scalea T. Community-acquired infections in the geriatrictrauma population. Shock 2000;14:338–42.
30. Grossman MD, Miller D, Scaff DW, et al. When is an elder old? Effect of preexist-ing conditions on mortality in geriatric trauma. J Trauma 2002;52:242–6.
31. Ferraris VA, Ferraris SP, Saha SP. The relationship between mortality and preex-isting cardiac disease in 5,971 trauma patients. J Trauma 2010;69(3):645–52.
32. Hukkelhoven CW, Steyerberg EW, Rampen AJ, et al. Patient age and outcome fol-lowing severe traumatic brain injury: an analysis of 5600 patients. J Neurosurg2003;99:666–73.
33. Mosenthal AC, Lavery RF, Addis M, et al. Isolated traumatic brain injury: age is anindependent predictor of mortality and early outcome. J Trauma 2002;52:907–11.
34. Rathlev N, Medzon R, Lowery D, et al. Intracranial pathology in the elderly withmild head injury. Acad Emerg Med 2006;13:302–7.
35. Mina AA, Knipfer JF, Park DY, et al. Intracranial complications of preinjury antico-agulation in trauma patients with head injury. J Trauma 2002;53:668–72.
36. Cohen DB, Rinker C, Wilberger JE. Traumatic brain injury in anticoagulatedpatients. J Trauma 2006;60:553–7.
37. Ivascu FA, Howells FA, Junn FS, et al. Rapid warfarin reversal in anticoagulatedpatients with traumatic intracranial hemorrhage reduces hemorrhage progressionand mortality. J Trauma 2005;59:1131–7.
38. Mower WR, Hoffman JR, Herbert M, et al. NEXUS II Investigators. Developinga decision instrument to guide computed tomographic imaging of blunt headinjury patients. J Trauma 2005;59(4):954–9.
39. Czosnyka M, Balestreri M, Steiner L, et al. Age, intracranial pressure, autoregu-lation, and outcome after brain trauma. J Neurosurg 2005;102:450–4.
40. BubLD,BlackmoreCC,MannFA, et al. Cervical spine fractures in patients 65 yearsand older: a clinical prediction rule for blunt trauma. Radiology 2005;234(1):143–9.
41. Battle CE, Hutchings H, Evans PA. Risk factors that predict mortality in patientswith blunt chest wall trauma: a systematic review and meta-analysis. Injury2012;43(1):8–17.
42. Elmistekawy EM, Hammad AA. Isolated rib fractures in geriatric patients. AnnThorac Med 2007;2(4):166–8.
43. Falimirski ME, Provost D. Nonsurgical management of solid abdominal organinjury in patients over 55 years of age. Am Surg 2000;66:631–5.
44. Myers JG, Dent DL, Stewart RM, et al. Blunt splenic injuries: dedicated traumasurgeons can achieve a high rate of nonoperative success in patients of allages. J Trauma 2000;48:801–5.

Bonne & Schuerer150
45. Harbrecht BG, Peitzman AB, Rivera L, et al. Contribution of age and gender tooutcome of blunt splenic injury in adults: multicenter study of the eastern associ-ation for the surgery of trauma. J Trauma 2001;51:887–95.
46. O’Brien DP, Luchette FA, Pereira SJ, et al. Pelvic fracture in the elderly is associ-ated with increased mortality. Surgery 2002;132:710–4.
47. Henry SM, Pollack AN, Jones AL, et al. Pelvic fracture in geriatric patients:a distinct clinical entity. J Trauma 2002;53:15–20.
48. Kimbrell BJ, Velmahos GC, Chan LS, et al. Angiographic embolization for pelvicfractures in older patients. Arch Surg 2004;139:728–32.
49. Velmahos GC, Toutouzas KG, Vassiliu P, et al. A prospective study on thesafety and efficacy of angiographic embolization for pelvic and visceral injuries.J Trauma 2002;53:303–8.
50. Cummings SR, Melton LJ. Epidemiology and outcomes of osteoporotic fractures.Lancet 2002;359:1761–7.
51. Taylor MD, Tracy JK, Meyer W, et al. Trauma in the elderly: intensive care unitresource use and outcome. J Trauma 2002;53:407–14.
52. Schulman AM, Claridge JA, Young JS. Young vs old: factors affecting mortalityafter blunt traumatic injury. Am Surg 2002;68:942–7.
53. Scalea TM, Simon HM, Duncan AO, et al. Geriatric blunt multiple trauma:improved survival with invasive monitoring. J Trauma 1990;30:129–36.
54. Fairman R, Rombeau JL. Physiologic problems in the elderly surgical patient. In:Miller TA, Rowlands BJ, editors. Physiologic basis of modern surgical care. StLouis (MO): CV Mosby; 1988. p. 1108–17.
55. Friese RS, Shafi S, Gentilello LM. Pulmonary artery catheter use is associatedwith reduced mortality in severely injured patients: a national trauma data bankanalysis of 53,312 patients. Crit Care Med 2006;34(6):1597–601.
56. Brown CV, Shoemaker WC, Wo CC, et al. Is noninvasive hemodynamic moni-toring appropriate for the elderly critically injured patient? J Trauma 2005;58:102–7.
57. Jacons DG, Plaisier BR, Barie PS, et al. Practice management guidelines for geri-atric trauma: the EAST practice management guidelines work group. J Trauma2003;54:391–416.
58. Epstein CD, Peerless J, Martin J, et al. Oxygen transport and organ dysfunction inthe older trauma patient. Heart Lung 2002;31:315–26.
59. Sharma G, Goodwin J. Effect of aging on respiratory system physiology andimmunology. Clin Interv Aging 2006;1:253–60.
60. Bochicchio GV, Joshi M, Knorr KM, et al. Impact of nosocomial infection intrauma: does age make a difference? J Trauma 2001;50:612–7.
61. Schecter WP. Withdrawing and withholding life support in geriatric surgicalpatients. Ethical considerations. Surg Clin North Am 1994;74:245–59.
62. Richmond TS, Kauder D, Strumpf N, et al. Characteristics and outcomes ofserious traumatic injury in older adults. J Am Geriatr Soc 2002;50:215–22.
63. Ferrera PC, Bartfield JM, D’Andrea CC. Outcomes of admitted geriatric traumavictims. Am J Emerg Med 2000;18:575–80.
64. Mosenthal AC, Livingston DH, Lavery RF, et al. The effect of age on functionaloutcome in mild traumatic brain injury: 6-month report of a prospective multi-center trial. J Trauma 2004;56:1042–8.
65. Grossman M, Scaff DW, Miller D, et al. Functional outcomes in octogenariantrauma. J Trauma 2003;55:26–32.
66. Grossman MD, Ofurum U, Stehly CD, et al. Long-term survival after major traumain geriatric patients: the glass is half-full. J Trauma Acute Care Surg 2012;72:1181–5.