Embed Size (px)
Citation preview

TRAUMATIC ABDOMINAL SURGICAL EMERGENCIES
E. PAYNE PALMER, M.D.
PHOENIX, ARIZONA
T RAUMA of the abdomen constitutes an important group of injuries not only producing disability but also ending far too often in sudden death. Much of this is due either to entire
lack or to sIow application of proper emergency treatment. Far too often a patient arrives at the hospital with an abdominal trauma, having received no emergency care at the site of the accident. Irreparable damage is likewise done through improper handIing by well meaning but inexperienced persons. Many times the injured person is pIaced in the first available automobile; he is rushed over roads and streets at a high rate of speed, thereby damaging the traumatized abdomen stiIl more and increasing the shock with every jolt and turn.
The medical profession must realize the importance of prompt and proper first aid treatment for patients with abdominal trauma. Naturally physicians must be thoroughly trained in the funda-
mentals of first aid and in appreciating the importance of first aid for this class of patients. Every member of this organization needs to go forth and preach the gospel of first aid to physicians so they can direct the laity and can actively promote better emergency care to cases of abdominal traumas. Such first-aid service is possible through the training of those who are brought in contact with accident cases. This is especially important in modern warfare as abdominal trauma is exceedingly common in miIitary activity.
It is also necessary for interns to know the principle of first aid for abdominal trauma while serving on the ambulance or in the emer- gency room at the hospital. The general practitioner likewise renders emergency treatment to cases of abdominal trauma. He should be prepared to handIe those he is capable of treating, but he should not fair to recognize early those he is not equipped to treat. The physician who accepts a case of abdominal trauma for treatment beyond the emergency is responsible for the end results, not the surgeon who sees the case when failure is imminent. Likewise a surgeon who assumes the responsibility of treating these patients must be willing to accept
397

398 PALMER-ABDOMINAL EMERGENCIES
many patients for expIoration. He must be wilIing to give them much of his time, making painstaking examinations, performing extensive technica operations, giving that cJose postoperative attention which in itseIf wiI1 do much in reducing the mortaIity rate.
“Treat them where they Iie” is truIy the first principIe in the emergency treatment of abdomina1 traumas as we11 as of fractures. This treatment shouId begin immediateIy at the scene of the injury and should first combat shock, then check hemorrhage and reIieve pain. If shock is profound, no movement whatsoever shouId be aIIowed unti1 improvement has occurred. Many Iives have been sacrificed through subjecting patients in shock from abdomina1 traumas to the added traumas of transportation.
AbdominaI trauma may be parieta1, viscera1 or parietoviscera1; it may be closed or open. Any abdomina1 trauma caIIs for immediate
close attention; therefore, the patient shouId be carefuIIy examined to determine the diagnosis. In many cases a history, carefully taken and recorded, and a physica examination are sufficient for a correct diagnosis. Others require Iaboratory examinations before a diagnosis
can be determined. The trauma may be Iimited to the abdomina1 waI1, but one must
be certain of this fact. With a cIosed trauma of the parietes the pain and tenderness are usuaIIy Iocalized to the site of the trauma. Among the cIosed traumas are ruptures of the rectus muscIe and deep epigastric vesseIs. The commonest site is beIow the umbiIicus. Profuse hemorrhage foIIows rupture of the deep epigastric vesseIs; it is frequentIy diflicult to differentiate between hematoma of the
abdomina1 waI1, intraperitonea1, and retroperitonea1 hematoma. However, with the first the sweIIing in the abdomina1 waI1 protrudes prominentIy if the patient bIows with the nose heId tightIy, whiIe an intraperitonea1 or retroperitonea1 mass wiI1 disappear. If the intra- parieta1 hematoma is Iarge and increasing in size, it must be evacu- ated; bIeeding vessels must be cIamped and Iigated; any rupture of the muscIe shouId be carefuIIy sutured. There may be a great dea1 of damage to the parietes with the Ioss of much tissue. One shouId consider every incised, Iacerated, or puncture abdomina1 wound as potentiaIIy penetrating, unti1 it is proved otherwise.
Most open wounds of the abdomina1 parietes, regardIess of how dirty they are, if seen earIy, i.e., within four to six hours, can be cIeansed and prepared so that primary union occurs. NevertheIess, despite meticulous cleansing there are some wounds so heaviIy contaminated that infection occurs. Furthermore, there are some

PALMER-ABDOMINAL EMERGENCIES 399
virulent types of contamination which the body defenses seem impotent to combat. The abdominal wall should be shaved, then scrubbed with green soap and warm water until it is quite clean. The
FIG. I. FIG. 2.
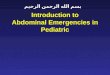
FIG. 1. Anteroposterior view of abdomen showing buIIet entering abdominal walI through left side, perforating the left lobe of of the Ever, diaphragm, pleura, Iung, again the pleura, and a compressed fracture of the body ofthe vertebra with compression of the cord. FIG. 2. LateraI view of location of buIIet in relation to the spine.
skin surface thereafter shouId be rinsed thoroughIy with sterile water, dried, and washed with ether. AI1 foreign materiaI visibIe in the wound must be removed; tissues which are obviousIy devitalized must be excised. Irrigate the wound thoroughly with normal saIine soIution, forcing this into a11 crevices of the wound. A chemica1 bacteriocide can be appIied to the normal skin of the abdominal wall. One shouId cautiously explore the depth of the wound to make certain that it is Iimited to the parietes or that it enters the abdomi- na1 cavity. There must, of course, be complete control of hemorrhage. This shouId be foIIowed by the pIacing of from 5 to IO Gm. of steriIe crystalIine sulfaniIamide in the depth of the wound. Wound cIosure with the Ieast number of anneaIed stee1 wire, cotton, or silk sutures, without tension, wiIl usuaIIy resuIt in primary wound healing. Wounds too extensive for satisfactory approximation of the edges, can have a pIastic repair if the patient’s condition permits; otherwise, pack with vaseIine gauze and protect with dressings or pack open and irrigate with Dakin’s soIution every two hours. Plastic repair can be done when the patient’s condition warrants it. Naturally, one would

400 PALMER-ABDOMINAL EMERGENCIES
give antitetanic serum after testing for sensitivity. The patient shouId be cIoseIy observed and given such treatment as indicated.
Notwithstanding the improved preoperative preparation and the
FIG. 3. Ruptured viscus (stomach) in supine pos-
ture, showing only eIevated diaphragm on right.
postoperative treatment of today, perforating abdomina1 wounds have approximateIy the same mortaIity as twenty-five years ago. The mortaIity rate increases in proportion to the age of the patient and the size of the missiIe. Incised, stab, or gunshot wounds may enter the peritoneal cavity, yet cause no damage to the viscera; however, they may, and probabIy wiI1, introduce contamination resuIting in a fata peritonitis. The majority of persons with penetrat- ing abdomina1 wounds die within twenty-four hours from hemor- rhage and shock. Those dying after this time succumb to peritonitis. Many incised and stab wounds appear to be Iimited to the parietes; yet as has been suggested, these must be considered potentially penetrating unti1 proved otherwise.
There are no reIiabIe symptoms suffrcientIy constant to indicate the absence or presence of viscera1 traumas. With the presence of genera1 muscIe rigidity and tenderness, pain and paIlor, one can be fairIy certain of an intra-abdomina1 trauma. Even in the absence of cIinica1 symptoms of an intra-abdomina1 trauma, indication for surgica1 intervention is aIways present. Patients arriving at the hospita1 in a serious state of shock shouId be treated for this condi-

PALMER-ABDOMINAL EMERGENCIES 401
tion before an examination is made. If after three or four hours the pulse rate continues rapid with a falling blood pressure and a reduc- tion in the hemoglobin and red ceIIs, or if air hunger deveIops, one
FIG. 4. Same as Figure I, in upright posture showing
free air or gas under diaphragm.
can be certain that hemorrhage exists. Therefore, an early operation is imperative, provided there is any reasonable prospect of the patient surviving the operation. Patients apparently in suitable condition shouId be sent to the operating room for examination. As
you know, many patients require very close study to determine the advisability of operation. The surgeon naturally wil1 use every means at his command to aid him in reaching a conclusion. The best surgical authority avaiIable should be called into consultation. Roentgeno- grams should show the presence of free air or fluid in the abdominal cavity. The peritoneoscope wiI1 also be a vaIuabIe aid in determining if there has been a penetration with blood or intestinal contents extravasated into the peritonea1 cavity. With every facility available to meet emergencies, enIarge and expIore the wound to its depths. If the incised or puncture wound has entered the abdominal cavity, an exploratory laparotomy must be performed as every perforating

4.02 PALMER-ABDOMINAL EMERGENCIES
wound of the abdomen means a probabIe perforating wound of the gastrointestina1 tract or some other viscus. Eviscerated omentum shouId be resected before the abdomen is opened or expIored.
FIG. 5. Intra-abdomina1 trauma with
peIvic fracture and rupture of bIadder
shown by extravasation of fluid in
cystogram.
FIG. 6. Same as Figure 5, after heaIing
of bIadder defect following open sur-
gical repair.
Eviscerated intestines shouId be cIeansed by irrigating with warm norma saIine soIution and Aushed with ether. Perforations shouId be cIosed before the intestines are returned to the abdomen.
Gunshot wounds of the abdomen frequentIy produce profuse hemorrhage and profound shock. Most of the fatal cases succumb within a few hours. They are so quickIy fata that no type of treat- ment offers hopes of benefit. Even apparentIy hopeless cases, how- ever, shouId be given every chance for recovery. The immediate intravenous administration of acacia, pIasma or serum and normal saline soIution may prove a Iifesaver. Patients in shock must be treated for this condition and observed frequentIy. When the patient faiIs to recover from shock in three or four hours, it is reasonabIe to suspect that the condition is due to actua1 bIood 10s~; therefore, prepare the patient for exploration as soon as the bIood pressure has been raised to a IeveI at which a Iaparotomy can be fairIy safeIy performed. Patients arriving at the hospital without much evidence of shock shouId be taken to the operating room immediateIy for examination and preoperative preparation. A carefu1 history shouId be taken and recorded. The physica examination must be thorough and the findings recorded. The buIIet’s wound of entrance and exit is particuIarIy important; an imaginary Iine connecting these two

PALMER-ABDOMINAL EMERGENCIES I.03
wounds wiI1 indicate the course of the buIIet through the body and the probable resulting trauma. If the bullet is still in the body, a flat x-ray film should be made and quickIy developed to provide informa-
FIG. 7. ExtracapsuIar rupture of left FIG. 8. Rupture of the right kidney; kidney; pyelogram showing diffused pyeIogram showing intracapsuIar ex- material in kidney area and Ioss of travasation of diotrast about kidney kidney outIine. pelvis.
tion regarding the location and size of the missile. It is often difficult to determine the optomal time for operation; yet the most important element aiding the recovery of patients with bullet wounds of the
abdomen is a short interval between the injury and the operation. The decision whether to operate immediately or not is usually based on the rate and character of the pulse and the blood pressure reading. Patients showing a reduction in the puIse rate with an increase in its voIume and a satisfactory blood pressure rise are probably good risks for operation. One with a feebIe p&e of 120 or over and a bIood pressure of 90 mm. or under is in a grave condition and could hardIy be expected to survive an operation; therefore, every effort shouId be made to improve the patient’s condition before an exploration is undertaken.
Regardless of the Iocation of an incised or punctured wound through the abdomina1 waII, intra-abdominal exploration requires a tong midline or a paramedian incision. As soon as the abdomen is

404 PALMER-ABDOMINAL EMERGENCIES
opened, bIood cIots and semisohd feca1 material shouId be removed
with the hands; then the cleansing process may be continued with suction until finaIIy a compIete toiIet of the abdomen and its contents may be made with sponges wrung out of warm norma saIine soIution. Next check a11 hemorrhage by seeking out the bIeeding vesseIs and ligating individuaIIy, avoiding mass Iigation and devitaIization of tissue. Thereafter systematicaIIy examine for trauma to the viscus. This may revea1 many injuries.
Percutaneous abdomina1 traumas usuaIIy resuIt from direct force appIied to the abdomina1 waI1; they rareIy occur from indirect force due to muscIe effort. Trauma caused by bIunt vioIence are of two
types; the widespread traumas caused by a severe crush, and the Iimited Iesion foIIowing a sudden IocaI trauma. Crushing injuries are usuaIIy muItipIe, often producing death within a short time. The
Iimited trauma is the most dangerous. FrequentIy there are no externa1 signs of trauma and symptoms of viscera1 trauma may be absent soon after the accident. Circumscribed bIows more commonIy
injure the stomach and intestine when distended, also the bIadder; on the other hand, diffuse force is apt to resuIt in trauma to the more fixed and soIid organs, such as the retroperitonea1 colon and duode- num and the Iiver and spIeen. Percutaneous injuries produce many types of traumas. Among these are, contusion and rupture of the free Iarge and smaI1 intestine, retroperitonea1 rupture of the coIon and duodenum, tearing of the mesentery from the intestine, tearing of the mesenteric vesseIs, tearing of the omentum, trauma of the
mesenteric, omenta1, and spIenic vesseIs with resuIting infarcts, rupture of the Iiver and spIeen, together with an associated rupture
of the bIadder, kidney, and diaphragm, postperitonea1 hemorrhage or a combination of any of these. These injuries are frequentIy fatal because their seriousness is not recognized earIy; accordingIy, emergency treatment is negIected, hospitaIization is Iate and since diagnosis is frequentIy d&cuIt, appropriate treatment is deIayed. Patients arriving at the hospita1 after an accident, apparentIy in good condition, shouId be carefuIIy examined for trauma. Even with Iack of symptoms and no evidence of a trauma, they shouId be put to bed and observed frequentIy. BIood pressure readings and puIse rate shouId be taken every haIf hour. Often in the presence of a ruptured viscus, definite symptoms may deveIop sIowIy. The presence of an acute abdomina1 pain, of muscIe ribidity, and tenderness with an anxious expression, of paIIor, of an increasing puIse rate and a faIIing bIood pressure shouId make one suspicious of a serious abdominal

PALMER-ABDOMINAL EMERGENCIES
trauma. Therefore, a carefuI examination shouId be made to deter- mine the cause of the patient’s condition. In many cases a carefully taken and recorded history and a painstaking physica examination are sufficient for the diagnosis. Though under some conditions a
definite diagnosis can not be made, time spent in attempting such a diagnosis, and in preparing the patient for an operative procedure, wiII stiI1 reward one for the effort, for this time wiIl give a decreased morbidity and a Iower mortality.
Associated traumas to the bIadder, kidney and diaphragm are common in both penetrating and percutaneous intra-abdominal traumas, therefore, they should be looked for in al1 such cases.
Recent advances in surgery have taught us to be more careful in evaIuating the patient’s fitness for surgery. Preoperative preparation of the patient, pre-anesthetic sedation, and the postoperative care are frequentIy of more importance than the operation.
Contamination of the peritonea1 cavity by penetrating wounds or percutaneous rupture of hohow viscus does not invariabIy require drainage; many cases do well without drainage. One should, however, make an effort to remove contaminating foreign materia1 from the peritonea1 cavity at the time of the operation. Patients frequentIy die of spreading peritonitis because absorbed toxins have not been adequately neutralized. The Iocal and genera1 immunity are the processes which actuaIIy protect. We have used CoIi-Bactragen in a considerabIe number of perforated and ruptured wounds of the intestine, and we beIieve that the resuIts obtained justify continuing the procedures. Also, the prophyIactic use of suIfaniIamide in these cases has apparentIy resuIted in a marked reduction in the morbidit!- and mortaIity. Though it is true that peritonitis of traumatic origin is a polymicrobic infection and that SulfaniIamide is not fuIIy effec- tive against a11 the bacteria present, stil1 other conditions appear to be favorabIe for the therapeutic action of the drug.
A Iarge number of patients surviving an operation performed within the first six hours after such traumas wiI1 recover if given cIose attention and proper postoperative treatment. CompIete rest and good nursing are essential.
CONCLUSIONS
The reduction of the high mortality due to traumas of the abdo- men Iies first and foremost in the dissemination of much of the information embodied in this paper. There is IittIe here that has not previousIy been said. Many are as famiIiar with this subject as the

406 PALMER-ABDOMINAL EMERGENCIES
author; and yet at the same time there are many physicians engaged
in genera1 practice who have not had the opportunity to inform themselves on much herein outhned.
But equalIy, and perhaps of greater importance, is the need for instructing the Iaity in proper procedure when an accident occurs. It is indeed rare for a physician to be first at the scene of an accident; and in those first precious moments there are a few simpIe procedures the Iayman couId do-or abstain from doing-that wouId expedite
the surgeon’s task enormousIy and wouId save many Iives that are
now needIessIy being sacrificed.
DISCUSSION
HENRY C. MARBLE (Boston, Mass.): I think at the moment there is littIe to add. Perforating wounds of the abdomen, as Dr. PaImer has pointed out, are important and require organization once they are in the hospital.
There is across the river from Boston a IittIe hospital in an underprivi- Ieged community, in which we occasionaIIy have cases of perforating wounds of the abdomen, often with stilettoes, sometimes with buIIets. The ruIes for the junior staff in that hospital are that a11 perforated wounds of the abdomen shaI1 be expIored with no delay.
The advent of bIood banks has made it possibIe to proceed boIdIy to the operation, and to rescue the patient from the shock or from the increasing shock with bIood or blood pIasma or saIine.
RecentIy at a staff meeting, a young surgeon presented his case. He told about the patient having been impaIed upon a stiIetto, and as he presented his case he stated that the white count was 10,000. The onIy criticism of the presentation (he had a nice operation and repair to the wound) was that one gentIeman inquired why they bothered with the white count.
Now, the other group of cases are, as we see them, mostly chiIdren. In CheIsea, apparentIy, it is the favorite diversion of the chiId in the street to throw himseIf under the passing automobiIe, and the history as they arrive in the hospita1 definitely states that the whee1 of the automobiIe went right across the chiId’s abdomen. That presents a11 of the picture.
Here, again, the only thing I can say is that the bIood bank is of vaIue. But as far as I am concerned, the junior surgeon or the resident in charge can cancel a11 appointments for the next twenty-four hours, and if he canceIs a11 appointments and sets himself down beside the patient and does nothing eIse, I think mortaIity wiI1 be on the decrease. He, and he aIone, is the onIy person equipped to evaIuate the changing conditions, and the more cIoseIy he sticks to that patient the better able he is to evaIuate the neces- sity for expIoration or for operation.
D. C. PATTERSON (Bridgeport, Conn.): The subject assigned to Dr. PaImer is so big, that it is very diffrcuIt to cover it in a short time. I want to

PALMER-ABDOMINAL EMERGENCIES -VT
compliment him on the field he has taken in. The treatment of these injuries, as he says, requires the best surgical skill, with all that implies,
nameIy, preoperative study and preparation, meticulous and competent operative care and very conscientious after-treatment.
There is not a great deal that can be done at the scene of the accident.
These patients, you might say, have automatically splinted the abdomen.
They can be kept warm, shock can be reduced and morphine administered,
but they should be gotten to the hospital as soon as possible.
The most important thing in the early stages is the careful observation and study of the patient himself, and it is well to bear in mind the truism
of Gorrel, that “where one mistake is made by not knowing, ten mistakes
are made by not Iooking.”
The externaI wound on the patient may give littIe indication of the seriousness of the internal injury. We had one patient come in-a street
sweeper-and the onIy accident that he could report was that in pulling his
brush toward him he struck the handle of his brush against the lower left
flank. He later comprained of pain and was sent to the hospital. We found
that he had a rupture of the sigmoid. Fortunately, he made a good recovery.
We had, two winters ago, as the result of coasting accidents, three cases
on the service at one time; a ruptured kidney, a ruptured spleen and a
ruptured liver. To put it briefly, we Ieft the kidney alone, removed the spleen, and packed the liver, this was in a girl of nineteen, with a huge crack
across the dome. They all made very good recoveries.
In the matter of kidney injuries, before one should ever think of remov-
ing the damaged kidney, he should be sure that the other kidney is properly functioning. I know of a case in which a damaged kidney was removed three
or four days after an accident, so it hardly seems as if it were necessary,
without the other kidney having been investigated. Unfortunately, the only kidney that he had was the one that was removed.
In injuries of the spleen, the matter of delayed hemorrhage has been
brought to our attention. We had a patient that developed hemorrhage
seven days after a basebalI bIow in the region of the spleen. Fortunately, he had remained in the hospita1 a11 the time. I think if we had been reaI smart,
we would have known the state of the spIeen and removed it before it
ruptured.
There is one thing the doctor spoke of that I cannot quite agree with, that is, the drawing of the straight line between the wound of entrance and
the wound of exit of the buIIet. It has been our experience that the course
of a bullet in the human body is about as erratic as a downhill putt; you never know what is going to happen after a buIIet enters the body.
Just one thing further which I should like to mention. They have strange
ways, probabIy, in Bridgeport, but we have had several cases of compressed air rupture of the intestine. Three of these I have had personal experience
with, only one of which came to the hospital in time for operation. The

408 PALMER-ABDOMINAL EMERGENCIES
others were admitted in a moribund state. One of them was mahcious, one
was a joke and the other was pureIy accidental.
In regard to the way those things can happen, the men in the foundries
had a habit, at the end of the day’s work, of dusting each other off with a
compressed air hose. It is not necessary for the nozzIe to be inserted in the
anal opening, or even in the buttocks; if it comes within six inches, the
conformation of the buttocks produces a funne1 through which air can enter the intestinal cana1.
It is we11 to warn a11 safety men in factories against this very pernicious practice of dusting off the clothing with compressed air.
CHARLES JOHNSTON (Detroit, Mich.): Dr. Palmer has painted a
rather bright and pretty picture of how to handIe these surgica1 emergen-
cies. In the case of a stab wound or gunshot wound, I think I can agree
with him that we can outline fairIy we11 what to do. The problem is
not one, as Dr. MarbIe suggests, for a resident to watch; it is one for the
entire staff. The more experienced person must be perfectly wiIIing to get
up in the middIe of the night and wrestIe with this problem. Too fre-
quentIy, these patients are brought into the emergency room, a diagnosis
is hoped to be obtained there, and a decision made on whether or not to
operate. Usually these patients are much better off if taken to their beds and aIIowed to get some rest and then studied. During this interim, of
course, bIood transfusions shouId be given to combat hemorrhage or shock
and any other probIem which they present shouId be met. The diffrcuIty in diagnosis is extreme. Many of these patients may show
very IittIe in the beginning after very severe intraperitonea1 trauma; others
may show signs of tremendous shock and have nothing wrong with their
viscera at aI1. Two compIicating features have caused us diffrcuIty in diagnosis in the
cases which have not had rea1 trauma to the intra-abdomina1 structures but
which simuIated it. These are acute diIatation of the stomach, and rigidity
of the abdomen associated with fractured ribs. Frequently, patients with
minor trauma wiI1 have an acute dilatation of the stomach and wiI1 appear practicahy moribund when brought into the hospita1. These will respond
quite rapidIy to reIief of the distention. Chest injuries, especiaIIy fractured
ribs, may cause enough rigidity to suspect that the patient has a fuIIbIown peritonitis.
Dr. CharIes Henry, of our staff, has carried out studies on perforations, especiaIIy ruptured uIcers in which the acid is aIIegedIy high, and his data indicate IittIe harm from chemica1 effects. The same things hoId for the
iIeum aIso, i.e., that the chemica1 aspects of the peritonitis are of very minor importance. It is the bacteria that are present, and the fact that many individuals have not found bacteria means that the organisms have been so diffused by the inffow of ffuid that a decent cuIture is not obtained.

PALMER-ABDOMINAL EMERGENCIES 3.09
Dr. Henry found that if he takes a large enough quantity of material,
the bacteria will usuaIly be found. Furthermore, he has found that the chemica1 composition of the intraperitonea1 fluid after ruptured uIcers is
practically that of blood serum. In other words, the ill effects of the chemical
(the acid or the aIkaIi) are pretty well neutralized. We have not studied
enzymes, however, and it is possible that the enzyme may he a dangerous
factor.
The greatest complications that we have seen are, of course, bleeding
and peritonitis. Frequently we have seen, without other injury, mesenteric injury, i.e., bruise to the mesentery and subsequent thrombosis of the
mesenteric vessels. It is practically impossible to diagnose the situation
before death. The patient gets a marked ileus which is assumed to be the
ileus based on trauma, which we of course see quite commonIy in these cases
and which, if intubated and allowed to right themselves, wiII recover. If
marked vascular occlusion is present, death ensues.
I think this has been a very interesting subject. I want to point out that
you cannot differentiate trauma to the abdomen from trauma generally, and attempts to farm out the care of these patients on an anatomical basis
are absurd. Segregation of head injuries on the neurosurgical service, or
chest cases on the chest service is not so good for the patient as it might
seem. The patient must be looked at as a sick individual who has been
traumatized, and must be cared for as a whole; he cannot be divided among
various services. Someone has to take the responsibility for the patient.