Embed Size (px)
Citation preview

Treatment of Acute Seizuresand Status Epilepticus
Daniel J. Costello, MD, MRCPIAndrew J. Cole, MD, FRCP(C)
Copyright © Sage Publications 1
Overt status epilepticus and persistent obtundation after awitnessed clinical seizure are neurologic emergencies.Early recognition and intervention in the electroclinicalsyndrome of status epilepticus reduces morbidity, althoughtreatment of the underlying etiology is also critical. Thisreview outlines key concepts related to status epilepticus,delineates an approach to the early management of statusepilepticus, and highlights novel but practical approachesin the evaluation and treatment of refractory status epilep-ticus, emphasizing the use of a treatment algorithm. Thisreview is written from the perspective of the intensive careunit clinician, and the approach and opinions expressedstem from clinical experience and review of the current lit-erature. Particular attention is given to an overall approachto the management of convulsive status epilepticus inadults and older children as well as exploring novelapproaches and diagnostic tools that may prove useful indifficult-to-control status epilepticus.
Key words: acute repetitive seizures; nonconvulsive status epilep-ticus; refractory status epilepticus; intensive care; infusion thera-pies; treatment algorithm; novel therapies
Status epilepticus (SE) is a heterogenous electro-clinical syndrome with diverse causes, inconsistentand dynamic clinical manifestations, and variableclinical course. Conventional teaching dictates thatthe outcome from SE is largely dependent on theunderlying etiology; however, some evidence suggeststhat SE carries its own morbidity and mortality,independent of the cause. The pathophysiologicchanges associated with ongoing seizure activityincreasingly point to SE being a dynamic rather thana static process. The clinical course of SE parallels
that of the underlying precipitating disease processbut occasionally may prove intractable even whenthe underlying disease improves, suggesting that SEcan “take on a life of its own” and come to domi-nate the clinical picture. Moreover, SE may arise inpatients with chronic epilepsy in the absence ofnewfound brain injury.
Although SE can be viewed and managed as anentity or disease in itself, somewhat separate fromassociated medical and surgical comorbidities, in mostcases, particularly in the intensive care unit (ICU) set-ting, SE should be more accurately thought of as astereotypical electroclinical response to a recent orremote cortical injury or irritation. One potential over-sight in the management of SE in the ICU is to equateSE with out-of-control epilepsy and give inadequateconsideration to the underlying cause. Ironically, SEoccurring in persons with established epilepsy may beeasier to control than SE in persons without preexist-ing epilepsy, possibly owing to earlier recognition ofSE and the presence of antiepileptic drugs (AEDs) inthese individuals. Furthermore, new onset SE is oftendue to an acute, active epileptogenic disease process,termed “acute symptomatic” SE, whereas SE in per-sons with preexisting epilepsy often arises owing to aremote but less acutely active disease process, termed“remote symptomatic.” When SE is viewed as an elec-troclinical response to brain injury, it follows that arigorous exploration for the underlying cause isalways warranted. This review will outline ourapproach when confronting SE in adults, paying par-ticular attention to the ICU environment.
Epidemiology
Status epilepticus has an incidence of approxi-mately 18.3 to 41 episodes per 100 000 populationper annum, amounting to 150 000 new cases peryear in the United States [1-5]. This figure largelyrefers to outpatient, population-based data and mayunderestimate the true incidence if one considersthose cases arising in persons in the hospital. The
From the Epilepsy Service, Department of Neurology, MassachusettsGeneral Hospital, Boston, Massachusetts.
Address correspondence to Daniel J. Costello, MD, MRCPI,Epilepsy Service, Department of Neurology, WACC 7, MassachusettsGeneral Hospital, 55 Fruit St, Boston, MA 02114; or e-mail:[email protected]
Received July 13, 2006, and in revised form December 1, 2006.Accepted for publication December 4, 2006.
DOI: 10.1177/0885066607307506

reported incidence varies substantially, dependingon the definition of SE being used. With recenttrends toward a more inclusive definition of SE, theincidence is likely to numerically increase. Further-more, the incidence refers to clinically apparentepisodes of SE, not incorporating the heretoforelargely underestimated incidence of nonconvulsiveSE. Suffice it to say that SE is quite common, per-haps the second most common acute neurologicemergency after acute vascular accidents.
Many cases of SE will be treated successfullywithout recourse to intubation and ICU admission.However, many patients admitted in SE needadmission to an ICU owing to persistent ictal activ-ity, obtundation secondary to seizures or treatment,or for treatment of the underlying neurologic dis-ease or injury. These patients are prone to seizurerecurrence, which may be clinically overt or subtle.Approximately 10% to 15% of patients with chronicepilepsy will experience an episode of SE at somepoint of their clinical course. Approximately 7% to10% of patients with chronic epilepsy initially pre-sent with an episode of SE. At a health economicslevel, SE costs approximately $4 billion per annumin the United States [6]. The annual number ofdeaths partly or fully attributable to SE has beenestimated to be 22 000 in the United States [7].
Definitions and Phenomenology
At first glance, the terms “epileptic seizure” and“epilepsy” ought to be easy to define, but there hasbeen considerable debate about their accuratedescription. The International League AgainstEpilepsy (ILAE) and the International Bureau forEpilepsy (IBE) recently proposed new definitions forboth of these clinical phenomena [8]. The proposeddefinition of an epileptic seizure is a “transient occur-rence of signs and/or symptoms due to abnormalexcessive or synchronous neuronal activity in thebrain.” This definition underscores the dual clinicaland electrographic nature of epileptic seizures.Following on from this, epilepsy is a “disorder of thebrain characterized by an enduring predisposition togenerate epileptic seizures and by the neurobiologic,cognitive, psychological, and social consequences ofthis condition.” The definition of epilepsy requiresthe occurrence of at least 1 epileptic seizure.
Epileptic seizures are either partial (also termed“focal” or “localization-related”) or generalized. Ageneralized seizure may be generalized at onset(primary generalized) or may have evolved from aninitial partial seizure (secondarily generalized). Partialseizures may (complex partial seizures) or may not (simple partial seizures) impair consciousness,
depending on the extent of cortical involvement,although the distinction of intact from altered con-sciousness is often difficult. The clinical manifesta-tions exhibited by patients during focal seizuresreflect both (1) loss of the normal function sub-served by the involved cortex, and (2) superaddedmanifestations inappropriately generated by theinvolved cortex, for example, unilateral involuntarymotor activity during seizures arising from themotor cortex.
Generalized seizures manifest clinically as tonic,atonic, clonic, tonic−clonic, myoclonic, or absenceseizures. Secondarily generalized seizures usuallyare tonic−clonic in nature. It is often difficult to dif-ferentiate primary generalized SE from secondarilygeneralized SE in the absence of a good account ofpreceding focal seizures before the episode of SE.Overall, most cases of generalized convulsive SE inadults that require ICU care are ultimately due tofocal cortical injury or irritation [1,9]. In general,epilepsy due to focal cortical injury (focal epilep-sies) is more difficult to control and manage thanidiopathic generalized epilepsy syndromes andhence predominate in the ICU setting.
More than 90% of generalized tonic−clonicseizures (either primary or secondarily general-ized) terminate within 2 minutes [10], probably dueto the overriding inhibitory cerebral activity thataccompanies the initial excitatory hypersynchro-nous cortical activity. This observation deservessome thought because it tells us something aboutthe nature of SE, where the ictal activity endures.Approximately 7% of seizures will progress into SE[11]. The factors that allow or promote persistentictal activity resulting in SE rather than self-limitingseizure activity are not well understood. What isevident is that the self-terminating nature of mostseizures is lost or overridden in SE. Defining SE hasproven more difficult than defining isolatedseizures, and any definition of SE needs to high-light this self-perpetuating tendency.
An intuitive approach to defining SE is to declareSE as any seizure activity sufficiently vigorous orprolonged enough to cause neuronal damage; how-ever, this definition is impractical because biomark-ers for brain injury are not easily available.Furthermore, similar electroclinical seizure activitywill have variable deleterious effects in differentpatients, depending on confounding clinical andgenetic factors such as age, fever, and medicationeffects. The threshold for induction of neuronalinjury can thus vary significantly from patient topatient; for example, classic absence SE is unlikelyto lead to significant morbidity, but nonconvulsiveseizures in medically ill patients are frequently asso-ciated with very significant morbidity and mortality.
Costello, Cole
2 Journal of Intensive Care Medicine XX(X); XXXX

The original definition by Gastaut and colleaguesin 1964 [12] described SE as “a seizure that persistsfor a sufficient length of time or is repeated fre-quently enough to produce a fixed or enduringepileptic condition.” This mechanistic definition hasmore recently been recast to read “generalizedconvulsive status epilepticus refers to a condition inwhich there is a failure of the ‘normal’ factors thatserve to terminate a typical generalized tonic-clonicseizure” [13]. Again, the difficulty lies in providing adefinition that is not just theoretically insightful andsound but is useful in an emergency department(ED) or ICU situation.
These mechanistic definitions have largely beensupplanted by more practical, operational, time-based definitions (particularly applied to convulsiveSE) referring to SE as “at least 5 minutes of persis-tent generalized, convulsive seizure activity or twoor more discrete seizures between which there isincomplete recovery of consciousness” [13]. Someexperts find the 5-minute definition arbitrary andfavor a working definition that SE is persistentseizure activity after sequential administration ofappropriate doses of appropriate first- and second-line AEDs. We believe that the 5-minute and 2-drugdefinitions both convey an appropriate sense ofurgency needed to proceed to the next stages ofclinical management.
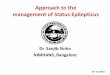
Following on from the distinction between partialand generalized seizures, SE can be either partial orgeneralized in nature. Partial SE can manifest withpreserved (simple partial SE) or impaired (complexpartial SE) consciousness. Generalized SE can man-ifest as generalized tonic-clonic SE (or convulsiveSE), absence SE or myoclonic SE, depending on thepredominant seizure type. A nonconvulsive form ofgeneralized SE with subtle or no clinical motor man-ifestations is increasingly being diagnosed. In fact,nonconvulsive SE may prove to be the most com-mon form of SE encountered in the ICU setting.Figure 1 illustrates the electrographic hallmarks offocal and generalized electrographic seizure activityand also illustrates the typical appearance of 3-Hzspike-and-wave activity.
Subtle Convulsive or NonconvulsiveStatus Epilepticus
Because of the dramatic nature of convulsive SE,prompt recognition by witnesses is universal andtreatment is generally initiated in a protocol-drivenfashion in most hospital settings; however, the samecannot be said for subtle convulsive SE or noncon-vulsive SE. Hereafter, we will use “nonconvulsive
status epilepticus” (NCSE) as a descriptive termdenoting cases of SE with little or no clinical signsof ongoing seizure activity apart from obtundationor subtle motor phenomena. Nonconvulsive SE islikely to represent a heterogenous collection ofelectroclinical states. Nonconvulsive SE is underrec-ognized, particularly in patients who have abnor-mal baseline cognitive abilities or multiorganmedical illnesses. In our experience, NCSE isapplicable to 3 broad categories of patients: post-convulsive NCSE, benign epileptic NCSE, and acutesymptomatic NCSE.
PostconvulsiveNonconvulsive Status Epilepticus
This category includes patients who have evolvedfrom overt convulsive SE into a state of electro-mechanical dissociation where the epileptiform dis-charges evident on the electroencephalogram(EEG) are not accompanied by clinical manifesta-tions, other than obtundation or coma [14-16].Patients with convulsive SE have a 10% to 20% riskof progression into subtle convulsive SE or NCSE,even after apparently successful treatment [16]. Thistruly epileptic form of NCSE represents the latterstages of convulsive generalized tonic−clonic SE.These patients need to be managed as if still in con-vulsive SE, using EEG rather than clinical observa-tions as the determinant of response to treatment.
Benign Epileptic Nonconvulsive StatusEpilepticus
The second broad category of NCSE includes thosepatients in focal or generalized SE where the clinicalmanifestations are either subtle or not incapacitating.This category encompasses partial SE (with motor,sensory, autonomic or psychic manifestations) andidiopathic absence SE (diagnosed most frequently inchildren and in the elderly). Essentially, these patientswarrant confirmatory EEG, benzodiazepine, andpossibly second-line agents but do not typically needICU care. These patients are otherwise systemicallywell but are at risk of developing convulsive seizuresand convulsive SE.
Patients with idiopathic generalized epilepsy(absence status, spike-wave stupor) that presentwith NCSE generally have a very good outcome[17,18]. Patients with partial SE typically fare lesswell because the outcome is etiology-dependentand the SE tends to recur and be more difficult toabolish [19,20].
Acute Seizures and Status Epilepticus
Journal of Intensive Care Medicine XX(X); XXXX 3

Cases of nondisabling focal SE should be dealt withon their own merits where the clinician gauges therisk of ongoing partial SE relative to the risks of coma-inducing therapies in an ICU setting. These cases aredifficult, because if one considers them as traditionalSE, one feels compelled to terminate the seizure activ-ity. However, despite the more benign appearance ofpartial SE, it often proves more difficult to terminateusing medical therapy than generalized convulsive orNCSE, resulting in significant iatrogenic morbidity.This is particularly true of prolonged focal motor SE,otherwise known as epilepsia partialis continua (EPC).An important determinant of the course of management
is consideration of the underlying etiology. As a rule,partial SE due to a solitary structural lesion is morelikely to subside with removal of the lesion (if possi-ble) than a course of pharmacologic coma in the ICU.
Acute SymptomaticNonconvulsive Status Epilepticus
The third category of NCSE is the least understood.This category encompasses patients who have hadfew if any recognized clinical seizures beforehandand who present with unexplained obtundation orcoma, often in an ICU and often in the setting of sig-nificant active comorbidities such as metabolic dis-array, hyperglycemia, hypoxia, or sepsis [15,21,22].The patients with focal cerebral injury are morelikely to have focal electrographic seizures on anEEG, whereas those with systemic illness are morelikely to have generalized electrographic seizures.Sometimes there is a clear history of significant braininjury, such as acute anoxia due to a cardiac or res-piratory arrest. Other patients are recognizedbecause of a highly abnormal EEG (often unex-pected) that demonstrates electrographic seizureactivity. This category of patient is becomingincreasingly recognized in ICUs that have access tocontinuous EEG monitoring facilities. This electro-clinical state is difficult to manage and it has not yetbeen shown that any intervention alters the clinicaloutcome. Although these patients typically do notexhibit clinical manifestations during the electro-graphic seizures or SE [23-25], they may occasionallyexhibit stimulus-induced clinical or electrographicseizures, or both [26].The EEG in acute symptomatic NCSE may reveal dis-crete, clearly defined electrographic seizures, whereit seems justifiable to treat by following the samealgorithm as that for convulsive SE until the electro-graphic seizures are abolished. However, manypatients will have equivocal EEG patterns withepochs of activity resembling electrographic seizures.These equivocal patterns overlap with periodic later-alized epileptiform discharges (PLEDs) and general-ized triphasic encephalopathic patterns. In thissituation, there is generally no “right answer” andeach case should be managed based on the clinicalsituation in conjunction with the EEG pattern. It maybe best to view these equivocal EEG patterns asepiphenomena, reflecting the diffuse cortical irritabilityor injury.
From a clinical perspective, identification ofNCSE on clinical grounds is undoubtedly unreliableand necessitates a high index of clinical suspicionto prompt the initiation of EEG monitoring. Another
Costello, Cole
4 Journal of Intensive Care Medicine XX(X); XXXX
Fig 1. Electroencephalographic (EEG) features of (A)focal electrographic seizure activity in a bipolar longitu-dinal “double banana” montage, (B) generalized electro-graphic seizure activity in a bipolar longitudinal “doublebanana” montage, and (C) classic generalized 3-Hz spike-and-wave EEG activity in a noncepalic (2nd cervicalvertebra) referential montage at a sensitivity of 15 uV/mm.

important clinical aspect of subtle convulsive SE andNCSE in general is that it responds less favorably totreatment than convulsive SE. This is underscored inthe study by Treiman et al [27], where among the134 patients with subtle generalized convulsive SE atpresentation, the successful termination of seizureactivity was much less likely (7.7%-24.2%) com-pared with the convulsive SE patients.
Clinical Management of NonconvulsiveStatus Epilepticus
Opinions vary on the correct management of NCSE[16,28,29]. As a rule, if NCSE has evolved in apatient with epilepsy or in the setting of an illnessknown to cause cortical irritation, then it should betreated in the same fashion as convulsive general-ized tonic−clonic SE. Hence, patients with primarygeneralized epilepsy syndromes, incapacitatingfocal SE, generalized tonic−clonic SE, and subtleconvulsive SE in the aftermath of generalized tonic−clonic SE should all be treated promptly using thestandard algorithm.
Management of acute symptomatic NCSE is moredifficult and less well studied. Frequently, thesecases do not have underlying epilepsy and the EEGpatterns reflect diffuse cortical network excitability.Clinicians vary in their approach from induction ofburst-suppression by infusion therapies to usingintermittent IV phenytoin boluses. The underlyingetiology often influences the approach—acutesymptomatic NCSE occurring in an otherwise-healthy post-operative patient may be treated moreaggressively than a patient after a 20-minute out-of-hospital cardiac arrest.
One approach in treating acute symptomaticNCSE manifesting as electrographic seizure activityrather than paroxysmal clinical ictal activity is toadminister a bolus of a benzodiazepine, but this ismuch less useful in the ICU because patients rarelyif ever “wake up” after the benzodiazepine trial dueto the altered mental state associated with theunderlying brain injury. Hence, treatment of ICUpatients with NCSE often involves administering anAED infusion using the EEG as a guide to dosingrather than the clinical state of the patient. Thisapproach, however, has not been proven toimprove morbidity and mortality in these patients.
Our approach is again to evaluate the case historyand EEG and then consider the underlying etiologybefore committing to a particular regimen. The prin-cipal criterion for starting an AED infusion (mida-zolam, pentobarbital, or propofol) is the presenceof definite, discrete, unequivocal electrographic seizures
of sufficient frequency and duration to impair thepatient over and above the underlying precipitatingcomorbidities. This criterion is deliberately nonspe-cific because each case will have unique character-istics that should govern decision making. Forexample, a patient whose EEG demonstrates gen-eralized slowing and lateralized rhythmic sharpwaves but is known to have underlying significantmetabolic dysfunction may be better served bytherapeutic-range phenytoin than by more aggres-sive coma-inducing therapies.
There is no definite evidence that NCSE causeslasting harm [28]; however, studies are confoundedby inconsistent definitions of NCSE. The morbidityassociated with NCSE was addressed by Shnekerand Fountain [30], where they carefully but retro-spectively appraised 100 consecutive ICU patientsin whom NCSE was detected. The authors reporteda mortality of 18% in the group in whom NCSEarose in the setting of significant medical comor-bidities and 3% mortality where NCSE was ascribedto preexisting epilepsy. The authors concluded thatthe mortality attributable to NCSE by itself is 3%,and, similar to convulsive SE, the underlying etiol-ogy largely determines the clinical outcome. Theauthors observed that the level of consciousnessevident during NCSE was a useful predictor of out-come. The mortality rate was 39% in patients withseverely impaired mental status and 7% in patientswho were mildly impaired. The principal messagefrom this study is that NCSE, like convulsive SE, isa heterogenous syndrome and that outcome isfavorable in the setting of a benign etiology butpoor in the setting of a malignant etiology.
All these clinical features suggest that NCSE (par-ticularly acute symptomatic) is a very different neu-robiologic phenomenon than overt convulsive SE.Presently our understanding of NCSE remains rudi-mentary, and much work is needed to elucidatewhich nonconvulsive electroclinical states aremerely epiphenomena and which warrant specificintervention with antiseizure medications.
Key Concepts
When managing seizures and SE in the ICU, a numberof overriding principles should be borne in mind:
• Clinical seizures may occur in any individual ifsufficient provocative factors are present.
• The physician needs to make a distinctionbetween SE arising in a person with preexistingepilepsy and SE arising de novo in a medicallyor surgically ill patient.
Acute Seizures and Status Epilepticus
Journal of Intensive Care Medicine XX(X); XXXX 5

• New-onset seizures or de novo SE in the settingof acute illness should be viewed as an electro-clinical expression of illness-related cortical irri-tability or injury.
• A relapse of seizures in the setting of subthera-peutic AED levels in a person with preexistingepilepsy often responds promptly to a bolusdose of the maintenance AED(s); however, SE(particularly convulsive SE) should be treated inthe standard fashion.
• Seizures and SE have 2 distinct but varyingcomponents⎯clinical and electrographic; oneneeds both clinical and EEG information to clas-sify patients.
• Both the clinical and electrographic manifesta-tions of SE have a natural history and evolutionwithin any given patient.
• Morbidity and mortality is high in untreated SE.• The chance of successful termination of SE with
use of a third-line AED after the first- and second-line agents have failed is only about 7%.
• The choice of first- and second-line AEDs is tosome extent arbitrary. Current protocols reflectease of use of specific AEDs rather than theirparticular therapeutic properties. A more impor-tant factor governing successful intervention isthe dose of AED given.
• Refractoriness is better predicted by theresponse to AEDs rather than the duration of SEbefore the patient received the first AED.
• In an obtunded patient, the EEG is more infor-mative than the clinical examination.
• When evaluating the patient once SE is con-firmed, one needs to consider the anatomic loca-tion of the seizures. Consideration of the merepresence or absence of seizures can overlookuseful lateralizing and localizing information.
• An information-gathering approach that usesmultimodal imaging and other diagnostic toolsincreases the likelihood of understanding thedisease process driving the SE.
• Persons in refractory focal status epilepticus arepotential candidates for surgical intervention.
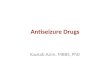
The acute occurrence of an epileptic seizure in apatient can lead to a number of potential clinicaloutcomes, each of which carries a particular mor-tality and morbidity (Figure 2). The spectrumranges from a self-limiting single seizure to highlyrefractory SE.
Causes of Status Epilepticus
Status epilepticus can be caused by a variety of dif-ferent underlying processes, the unifying aspect ofwhich is cortical irritation or injury. The clinical pre-sentation and semiology (clinical characteristics of
the seizures) typically do not convey accurate infor-mation about the underlying cause, although thetempo of the seizure activity often reflects theaggressiveness of the etiology.
Status epilepticus can be categorized as sympto-matic, idiopathic, or cryptogenic. The term “symp-tomatic” indicates that the seizure activity is asecondary phenomenon or a symptom of an under-lying disease process. “Idiopathic” denotes a con-stitutional or genetic predilection to seizure activityor SE, characteristic of idiopathic generalizedepilepsy syndromes. “Cryptogenic” refers to seizureactivity or SE for which a cause cannot be identi-fied. Most cases of cryptogenic SE are likely to besymptomatic, although the causative lesion cannotbe identified with existing technology. Most casesof refractory SE in adults are symptomatic. Theunderlying brain injury or dysfunction may haveoccurred temporally distant from the present SE(remote symptomatic) or may be recent (acutesymptomatic). Some authors describe SE associatedwith an underlying degenerative process such asAlzheimer dementia as progressive symptomatic.
The etiology of SE varies according to whethercase ascertainment occurs in the community or in ahospital setting and whether the epidemiologic dataare acquired retrospectively or prospectively. Themost informative prospective urban population-based epidemiologic study of SE was reported byDeLorenzo and colleagues [1,7]. Although there hasnot been a prospective ICU-based epidemiologicstudy on SE, the causes of new-found SE in the ICUsetting are likely to be similar but vary in propor-tion, with a greater number of cases due to trau-matic brain injury, central nervous system infection,and new vascular insults [31]. Table 1 gives anapproximate breakdown of the causes of SE inadults and older children that one could expectfrom all-comers in an urban ED, most of whom willnot need ICU care.
A recent retrospective ICU-based study high-lighted certain risk factors for the development ofSE [31]. Of 83 episodes of SE managed in an ICU,50 arose de novo from newly acquired cerebralinjury. Approximately 40% to 50% of SE arose inpatients without a history of epilepsy, which hasbeen noted in other studies [32]. Patients in refrac-tory SE, defined as SE which does not respond toappropriate doses of appropriate first- and second-line therapy, are more likely to have underlyingencephalitis, be associated with hyponatremia,exhibit cerebrospinal fluid (CSF) pleocytosis, andbe febrile [31].
Direct brain injury or irritation accounts for mostcauses of SE, but there are well-recognized systemic
Costello, Cole
6 Journal of Intensive Care Medicine XX(X); XXXX

causes, including hyponatremia [33], hypoxia/ischemia, narcotic withdrawal [34], alcohol anddrug toxicity [35], and ingestion of proconvulsantmedications including β-lactam antibiotics (peni-cillins and cephalosporins), certain antidepressants(bupropion), certain antipsychotics (clozapine),bronchodilators, and immunosuppressives. Precipitouswithdrawal from barbiturates, benzodiazepines,and opiates can lead to the development of orexacerbation of seizures, particularly in those withpreexisting epilepsy. Certain illicit drugs clearly areassociated with seizures and SE, both acutely and onwithdrawal, including cocaine and amphetamines.
Apparently mild or restricted electrolyte or meta-bolic disturbance, including hypophosphatemia,
hyponatremia, hypoglycemia, liver dysfunction, renalimpairment, hypo-osmolarity, hypomagnesemia, andhypocalcemia can be implicated in seizure provoca-tion, particularly in the inpatient population.
Overall, the causes of SE can be categorized asacute symptomatic (52%-72%), remote symptomatic(20%-31%), and idiopathic/cryptogenic (3%-15%) [5].
Detection of Status Epilepticus
When first observed, patients in convulsive SE are gen-erally found to be unresponsive, obtunded, and exhibitrepetitive truncal and limb movements, which maybe tonic or clonic. In those patients with prolonged
Acute Seizures and Status Epilepticus
Journal of Intensive Care Medicine XX(X); XXXX 7
DURATION STAGE % ALL-COMERS INTERVENTIONS MORTALITY
0-2 min Seizure 100% Supportive measures <1%
>2 min Prolonged seizure 10% Benzodiazepine <5%
>30 min Status Epilepticus 5-7% 1st line: Benzodiazepine 10-20%
2nd line: Fosphenytoin/Phenytoin
+- 3rd line: Phenobarbital/Valproate/LevetiracetamFailure of 1st
and 2nd +- 3rd
line therapies
2 hours Refractory SE 1-2% Continuous Infusion therapy 40%
Failure of initial trial of ContinuousInfusionTherapy
Midazolam/Propofol/Pentobarbital
>48 hours Highly refractory SE <1% Alternative Continuous Infusion Therapy >60%
Novel therapeutic options
Fig 2. Possible clinical outcomes from a single seizure.

clinical seizure activity, the movements gradually becomesubtle and eventually are restricted to brief facial,periorbital, and limb twitches [16,25]. Sometimes, noclinical movements are evident; hence, differentiationof subtle nonconvulsive SE from other causes ofobtundation based on clinical signs can be fraughtwith difficulty. Recognition of SE can be even moredifficult in the ICU, where patients frequently havecoexisting reasons for unresponsiveness. Furthermore,ICU patients are often paralyzed for ventilation anddo not exhibit motor signs of seizure activity. Finally,it must be remembered that motor manifestations ofseizure activity simply reflects involvement of themotor areas of cerebral cortex. Patients can haveseizure activity or SE arising from nonmotor areas,resulting in altered mental status without motor man-ifestations.
These factors conspire to make seizures and SEdifficult to detect by clinical assessment alone,although one can identify “at-risk” patients by thelikelihood of their underlying illness to cause cere-bral cortical injury with consequent seizures. Theunreliability of clinical detection of seizures in theICU is confirmed in recent studies where ICUpatients were screened for seizures by EEG moni-toring [23,29,36]. Towne et al [29] reported an 8%incidence of NCSE among 236 comatose patientswith no clinical evidence of seizure activity.
A larger study by Claassen et al [23] reported theEEG findings in 570 patients, 89% of whom were inan ICU, who underwent continuous EEG monitor-ing. Electrographic seizure activity was evident in110 patients, and only 9 exhibited convulsive motoractivity. The risk factors associated with detectionof electrographic seizure activity included coma(odds ratio [OR], 7.7; 95% confidence interval (CI),
4.2-14.2), age younger than 18 (OR 6.7; 95% CI,2.8-16.2), preexisting epilepsy (OR, 2.7; 95% CI,1.3-5.5), and witnessed convulsive seizures beforeEEG monitoring (OR 2.4; 95% CI, 1.4-4.3). Overall,77% of the patients who ultimately exhibited electro-graphic seizure activity did so within 6 hours of theonset of EEG monitoring, suggesting that EEG moni-toring can be an efficient and effective screeningmeasure. However, 5% of noncomatose and 20% ofcomatose patients needed more than 24 hours ofmonitoring to detect electrographic seizure activity.
These studies provide compelling evidence for agreater role for EEG monitoring in the detection ofseizures and SE in the ICU, although the impact oftreatment of heretofore-undetected electrographicseizures is unknown. Provision of a 24-hour EEGmonitoring service is logistically difficult, even forlarge urban centers. Training of ICU personnel in theinitiation of EEG recording may be the only effectivemeans of providing on-call EEG monitoring.
Certain scenarios should prompt initiation of on-site EEG monitoring or transfer to an institution wherecontinuous EEG monitoring is available. Broadlyspeaking, the principal indication for EEG monitoringin the ICU is the suspicion of NCSE, although otherindications are also important (see Table 2).
Pathophysiology of Status Epilepticus
It is important to appreciate that SE is not an all-or-nothing phenomenon with unvarying manifesta-tions. Many lines of evidence show that SE evolvesclinically, mechanistically, and electrographically.This dynamic quality mandates a dynamicapproach, the outcomes from which can be betterunderstood if one is aware of the maladaptive tis-sue responses to the seizure activity. The physio-logic effects can be arbitrarily divided intooverlapping early biochemical changes and lateranatomic and functional changes.
Within minutes of ictal onset, the persistent neu-ronal depolarization within the seizing corticalregion is associated with a gradual but profoundshift in local homeostasis and neuronal integritymanifesting as ionic fluxes, activation of secondmessenger systems, altered gene expression withconsequent altered protein production, nerve fiberarborization, synaptic reorganization, and ulti-mately, irreversible cell damage and loss [37-39]. Itis likely that self-terminating seizures have physio-logic effects that differ, both qualitatively and quan-titatively, from self-perpetuating seizure activity.With persisting ictal activity, these complex changesconspire to render the ictal region intrinsically more
Costello, Cole
8 Journal of Intensive Care Medicine XX(X); XXXX
Table 1. Etiology of Status Epilepticus
Approximate % Cause of Total
AED noncompliance/insufficient dosing 20Old brain injury 15Acute vascular injury 15Alcohol-related 10Metabolic/electrolyte disturbances 10Unknown/cryptogenic 10CNS infection 5Cerebral tumor 5Acute trauma 5Drug toxicity <5Global hypoxic injury <5Idiopathic epilepsy <5
AED = antiepileptic drug; CNS = central nervous system.

epileptogenic and increasingly refractory to inter-ventions aimed at terminating the seizure activity.Later structural cortical consequences of SE includemossy fiber sprouting, synaptic reorganization, cellloss, gliosis, and eventually, increased susceptibilityto further seizures and loss of normal tissue func-tion. These enduring physical changes within thealready damaged cortical region may serve as asubstrate for the persistent epilepsy frequently seenafter episodes of SE.
At a physiologic level, Lothman [40] described 2phases of SE, termed phase I (compensated) orphase II (uncompensated) SE. Phase I is character-ized by increased cerebral metabolic demand com-pensated for by increased cerebral blood flow,increased anaerobic respiration, and increased car-diovascular parameters. Phase II evolves whencerebral autoregulation breaks down as cerebralblood flow falls in association with systemic hypoten-sion and autonomic dysfunction. Subsequent cere-bral edema, hypoxia, and cardiac dysfunctioncontribute to the high mortality associated withsevere, prolonged SE [41].
Seizure activity will ordinarily activate cortical inhi-bitory mechanisms, principally through γ-aminobutyricacid (GABA)-mediated mechanisms, with termina-tion of ictal activity. Benzodiazepines, the usualfirst-line intervention in SE, are GABA-agonists. InSE, there is evidence for failure of GABA-mediatedinhibition of ictal activity, which leads to a shifttoward excitatory glutamatergic activation of neu-rons through N-methyl-D-aspartate (NMDA) recep-tors [42,43]. This may explain the observation thatduration of seizure activity partially governs theresponse to the first-line AED [44].
Resistance to AEDs develops in parallel with ongo-ing seizure activity and partly explains why med-ications used to control chronic epilepsy are oftenineffective against SE. These dynamic changes intherapeutic responsiveness are complex and stemfrom pharmacokinetic, pharmacodynamic, and phar-macogenomic factors, which may be unique to theindividual person in SE. Other mechanisms for fail-ure of initial therapies include activation of putative
“drug-resistance” genes during SE by ill-understoodmechanisms [45]. Given the dynamic changeswithin the ictal cortical region, it is not surprisingthat therapeutic efficacy often wanes with increas-ing duration of ictal activity. Some authors proposea mechanistic approach to the management of thelatter stages of SE based on the predominant mech-anism of epileptogenesis, for example, use ofNMDA-antagonists [46-48].
In parallel with the clinical and neurobiologicevolution of SE, characteristic electrographic stageshave been described. Treiman et al [14] suggest thata number of identifiable EEG patterns evolve in apredictable sequence during the course of general-ized convulsive SE in humans. These include (1)discrete seizures, (2) merging seizures with waxingand waning amplitude and frequency of EEGrhythms, (3) continuous ictal activity, (4) continu-ous ictal activity punctuated by low-voltage flatperiods, and (5) periodic epileptiform dischargeson an attenuated background.
Initial Management of Status Epilepticus
The initial management of status epilepticus beginsin the community. Ideally, all caregivers and relativesof patients with epilepsy should be trained in deal-ing with their family member’s habitual seizures. Notinfrequently, patients (particularly children) withchronic epilepsy report a crescendo increase in thefrequency or severity of their habitual seizuresbefore the onset of SE itself. This premonitory phasepresents a critical window of opportunity for prevent-ing episodes of SE. A 1- to 3-day course of regularbenzodiazepine therapy, such as oral lorazepam,will often abort the impending SE.
In the community, brief seizures with quickrecovery generally do not warrant further immedi-ate treatment. However, more prolonged or repeti-tive seizures require intervention with AEDs. In thehome setting, where vascular access is not available,rectal, or enteral (eg, gastrostomy tube) diazepam[49] or buccal midazolam (in children) [50] can be
Acute Seizures and Status Epilepticus
Journal of Intensive Care Medicine XX(X); XXXX 9
Table 2. Indications for Continuous Electroencephalographic Monitoring in the Intensive Care Unit
• History of nonconvulsive status epilepticus• Unexplained persistent obtundation or coma in any setting• Unanticipated delay in recovery from anesthesia or surgery• Delayed recovery after witnessed convulsive seizure• Obtundation with subtle clinical signs: oculomotor abnormalities or subtle motor twitching (facial, limbs)• Suspected non-epileptic status (“pseudostatus”)• Monitoring of depth of anesthesia (burst−suppression interval)• Delayed recovery after initial treatment of seizure

used where convulsive seizure activity persistsbeyond what is typical for a patient or when con-vulsive seizure activity is sustained for more than 2minutes.
In the hospital setting, the early ED managementinvolves lateral positioning of the patient to avoidinjury and aspiration, maintaining a patent airway,oxygen supplementation, and correction of anyimmediately reversible precipitants, particularlyhypoglycemia. Parenteral thiamine (100 mg) should beadministered before a glucose bolus is given if alco-hol abuse or poor nutrition is suspected; pyridox-ine is a consideration in neonates. Where vascularaccess is available, the traditional initial manage-ment of prolonged convulsive seizures similarlybegins with administration of a benzodiazepine.
The rationale for the use of benzodiazepines asfirst-line AED therapy was consolidated by the mostinformative clinical trial performed to date examin-ing the optimal initial management of convulsive SE[27]. This trial was conducted in a hospital andcompared 4 different treatment arms: diazepam(0.15 mg/kg), followed by phenytoin (18 mg/kg),lorazepam alone (0.1 mg/kg), phenobarbital alone(15 mg/kg), and phenytoin alone (18 mg/kg). In384 patients with overt convulsive activity, lorazepamterminated the seizure activity in 64.9%, phenobar-bital in 58.2 %, diazepam plus phenytoin in 55.8%,and phenytoin in 43.6%. An intention-to-treat analy-sis found no significant difference among treatmentgroups in patients with overt convulsive SE (P =.12), except that lorazepam alone was significantlymore effective that phenytoin alone. Furthermore,the treatments did not differ with respect to seizurerecurrence during the initial 12-hour study period,the incidence of adverse reactions, or the clinicaloutcome at 30 days.
Thus, as a first-line treatment for convulsive SE,administration of lorazepam alone, phenobarbitalalone, or diazepam plus phenytoin were equallyeffective. In clinical practice, lorazepam alone iseasier and faster to use and hence has become wellestablished as a first agent given to patients in SEof any type. Lorazepam is thought to be morefavorable than diazepam because it has a longertherapeutic effect and a lower risk of venousthrombophlebitis and respiratory suppression, par-ticularly in children [51-53]. Alternative benzodi-azepines include diazepam (buccal, intramuscular,parenteral), midazolam (buccal, intranasal, par-enteral, intramuscular), and clonazepam (intravenous[IV]) although absorption from intramuscular injec-tion is probably too slow for emergency treatmentof seizures and SE.
Phenytoin, perhaps in part for traditional reasonsand relative ease of use, is widely used as the nextagent if lorazepam proves ineffective; however, thestrategy of lorazepam followed by phenytoin hasnever been compared with other treatments in awell-designed clinical trial. Approximately 40% to50% of patients who do not respond to initial ben-zodiazepine therapy will respond to a subsequent20-mg/kg loading dose of IV phenytoin [54].Fosphenytoin, a phenytoin pro-drug, is graduallyreplacing phenytoin owing to its improved safetyprofile with less risk of severe thrombophlebitisand local tissue necrosis, the possibility of fasteradministration (IV as well as intramuscular), andcompatibility with a wide range of infusion solu-tions. Other possible second-line AED interventionsinclude a second bolus of benzodiazepine, an IVbolus of sodium valproate, or an IV bolus of phe-nobarbital, although none of these agents havebeen studied in a rigorous fashion as an adjunct tolorazepam. Intravenous levetiracetam is a recentaddition to the armamentarium of parenteral anti-seizure medications, although it is less well studied.
Irrespective of which agent is chosen as a first- orsecond-line intervention, it is imperative that ade-quate doses are given. Fear of precipitatingunwanted adverse effects can be allayed by heartrate and blood pressure monitoring and appropriateadjustment of infusion rates. The infusions shouldbegin at 50% of the maximum infusion rate (eg, 25-mg/min phenytoin), followed by gradual titration ofinfusion rate upward according to the blood pres-sure response. If the loading dose of phenytoin isadministered during a 20-minute period, then themaximal brain concentration of phenytoin will beachieved toward the end of the infusion. Someauthors argue for an additional 5- to 10-mg/kg bolusof phenytoin if the levels do not exceed 20 μg/mLafter the initial bolus [55].
A critical juncture in the management of SEarrives when SE has not terminated after the admin-istration of both a benzodiazepine and phenytoin/fosphenytoin. The traditional approach is to pro-ceed to a third agent, usually a loading dose of IVphenobarbital. Alternatively, a loading dose of IVvalproate or IV levetiracetam may be administered.However, only 7% of patients who have notresponded to timely and appropriate doses of first-and second-line AED therapy will then respondto any third-line IV AED [27]. Use of a third-lineAED may be justifiable if one is trying to avoidintubation, although many authors favor proceed-ing directly to continuous infusion therapy atthis point.
Costello, Cole
10 Journal of Intensive Care Medicine XX(X); XXXX

Patients who are already taking AED therapyshould continue to take maintenance AEDs at thesame or higher doses. In patients admitted onphenytoin therapy, a phenytoin level should be drawnbefore they receive a loading dose of phenytoin;however, administration of a loading dose shouldnot be delayed while waiting for the phenytoinlevel. Overall, we believe that biochemical pheny-toin toxicity (ie, corrected level >20 μg/mL) is lessworrisome than ongoing seizure activity associatedwith inadequate phenytoin dosing. Biochemicaltherapeutic ranges for the older AEDs are applica-ble to the outpatient with chronic epilepsy ratherthan the ED/ICU patient, where the risk versus ben-efit favors higher AED serum concentrations.Duration of AED treatment in the ICU setting, par-ticularly with continuous infusion therapies, is morepredictive of treatment-related complications thanserum AED levels.
Specific protocols for the management of SE sug-gest the sequential administration of a benzodi-azepine and a loading dose of phenytoin orfosphenytoin. The critical point made by all authorsis that the treatment be instituted early, efficiently,and fully. In reality, all protocols are modified asclinical circumstances and institutional resourcesdictate. Table 3 outlines the current guidelines onthe management of generalized (convulsive andsubtle convulsive) SE used at our institution. Thisprotocol is idealized and difficult to implement effi-ciently in any busy hospital but serves as an algo-rithm for the initial management of SE. Each step is
open to discussion though the sequence is wellestablished.
Other aspects to the general management of SEinclude the following:
• Airway⎯If the clinical seizure activity termi-nates and it is safe to access the oropharynx, aGuedel (or nasopharyngeal) airway may beuseful to maintain oropharyngeal patency.
• Intubation⎯Intubation is generally neededduring infusion therapies, although patientsreceiving midazolam may not require intuba-tion. If intubation is necessary but difficult, usetemporary non-depolarizing neuromuscularjunction blockade for intubation (eg, vecuro-nium). Otherwise, muscle paralytics are typi-cally not used in the management of SE.
• Hypertension⎯Ensure volume replacement anduse vasopressors if needed. Do not treat hyper-tension unless critical.
• Hyperglycemia⎯Ensure glycemic control becausehyperglycemia may exacerbate neuronal injury.
• Cerebral edema⎯Treat hyperventilation withmannitol or steroids, depending on etiology, ifevident.
• Acidosis⎯Acidosis usually parallels the degreeof anaerobic metabolism and generally resolveswith seizure control or intubation with generalanesthesia. Boluses of sodium bicarbonate areused exceptionally.
• Hyperthermia⎯Hyperthermia, like hypertension,generally resolves with control of SE, but externalcooling, cool peritoneal lavage, or extracorporealblood cooling may be used if refractory.
Acute Seizures and Status Epilepticus
Journal of Intensive Care Medicine XX(X); XXXX 11
Table 3. Suggested Initial Management (First 30 Minutes) of Status Epilepticus
Stage, time Interventions Time, min
0 min Recognition of status epilepticus (clinical or EEG) 0 0-30 min Airway/breathing/circulation 0-1
Suctioning, supplemental oxygen, pulse oximetry 0-1Baseline vital signs; capillary glucose level 0-1ECG/cardiac telemetry 1-2Large bore proximal IV access, baseline labs, IV fluids 1-2Administer 100 mg IV thiamine and/or 50 mL bag of 50% dextrose (if needed) 1-3Administer 0.1 mg/kg bolus dose of IV lorazepam in equal volume of diluent 3-10
by slow IV push at ~2 mg/min or in divided stat dosesPrepare loading dose (20 mg/kg) of phenytoin or fosphenytoin Begin phenytoin infusion at 25 mg/min or fosphenytoin infusion at 75 mg/min 5-30
(begin 1 min after end of lorazepam bolus if seizure persists)Titrate phenytoin/fosphenytoin infusion rate up to maximum tolerated rate
(~50 mg/min for phenytoin and ~150 mg/min for fosphenytoin) according to BPRegular vital signs especially BP checks (every 2 min)Draw serum phenytoin level approximately 10 min after phenytoin load is
completed ± administer extra 5 mg/kg of phenytoin or fosphenytoin (if serum level available)
EEG = electroencephalogram; ECG = electrocardiogram; IV = intravenous; BP = blood pressure.

• Rhabdomyolysis⎯Rhabdomyolysis is an under-appreciated morbidity associated with convul-sive SE and should be detected and treatedearly with saline diuresis, urine alkalization, andif needed, muscle paralysis.
• Aspiration⎯Aspiration should be suspectedand screened for in all patients with SE.
• Maintenance AED therapy⎯All patients with denovo SE or epilepsy-related SE need mainte-nance AED therapy. Ideally, this should be ini-tiated within the first day of admission,irrespective of the clinical course. Once initi-ated, the maintenance AED regimen can bemodified toward the end of the hospital stay.
• Electroencephalographic monitoring⎯Ideally,begin EEG monitoring if patient is not wakingup 15 minutes after clinical movements havestopped.
Initial Diagnostic Evaluation
The treating clinician should recognize that the prog-nosis of SE is largely determined by the underlyingcause of the seizure activity and, from the outset,should initiate a diagnostic evaluation in parallel withtreating the SE itself. The collateral history fromfamily members or relevant witnesses is invaluable,as is determining the patient’s past neurologic history,compliance with AED therapy (if the patient has pre-existing epilepsy), medical history, medication andillicit drug ingestion, and recent ill health. The clini-cal findings are typically self-evident in convulsive SEwith generalized tonic−clonic activity, but the patientshould be closely examined for subtle motor andfacial/oculomotor signs in suspected NCSE. Theextent of the diagnostic evaluation should be depen-dent on a track record of prior episodes of SE.
Patients with SE in the setting of chronic epilepsyare less likely than patients with de novo SE to havean obscure underlying etiology. In general, patientswith new-onset SE should be investigated moreextensively than patients with previous episodes ofSE, although each case must be considered carefullyaccording to the specific clinical details.
Blood should be drawn from all patients tocheck values for routine laboratory indicators, glu-cose level, electrolyte levels (including magnesium,calcium, phosphate), creatine kinase level, anti-seizure medication levels, and toxicology screen inconjunction with urine sampling. Arterial bloodsampling is necessary for detection of systemicacidosis due to prolonged anaerobic metabolismassociated with vigorous convulsive seizures. Ifsystemic infection is suspected, a septic screen iswarranted with particular attention to a lumbar
puncture, preceded by a head computed tomogra-phy (CT) scan and careful funduscopy to excludeovertly raised intracranial pressure if the patient isobtunded. A follow-up diagnostic lumbar puncturemay be necessary if the SE developed precipitouslyin the early stages of a systemic or central nervoussystem illness, where the CSF fluid may initially benondiagnostic.
Emergency imaging by CT is overused but isimportant if one is to exclude “neurosurgical” causesfor SE, such as tumor and traumatic brain injury. Inour experience, the yield from semi-elective plannedmagnetic resonance imaging (MRI) of the brain ismuch higher than CT imaging in the ED. Computedtomography imaging should never delay the initiationof first- and second-line AED therapy or impede trans-fer to an ICU. If intracranial collections (particularlysubdural empyema) are suspected, then contrast-enhanced imaging may increase the sensitivity of theCT study. Another imaging tool that may be critical inspecial circumstances is MR venography where cen-tral venous sinus thrombosis is a clinical possibility.
Management of Refractory StatusEpilepticus
In practice, refractory SE (RSE) can be defined as SEthat does not respond to appropriate doses ofappropriate first- and second-line therapy such asIV benzodiazepine and phenytoin/fosphenytoin.The likelihood of progression to RSE in certainpatients is largely a reflection of the underlyingrefractory etiology, although other potential mech-anisms of therapeutic resistance include changes inGABA receptor composition [43] and increasedexpression of drug resistance genes [45].
To date, unfortunately, treatment algorithms in RSEhave not been compared in prospective, randomizedclinical trials, and the consequent empiricism has ledto significant variations in the management of thesecases [56-58]. Eriksson et al [59] provide some modestevidence that delay in the institution of first- or second-line therapy may also be a risk factor for developmentof RSE. Approximately 31% to 44% of all SE patientswill evolve into RSE [27,31,32,54]. De novo (firstepisode) SE has a moderate likelihood (40% to 50%)of becoming refractory [32]. Complex partial, focalmotor, and nonconvulsive forms of SE are relativelymore likely than convulsive or absence SE to becomerefractory to first- and second-line therapies, althoughall forms of SE may become refractory [54].
Although the initial management of SE is relativelywell established, the management of RSE is lesswell established and largely operator-dependent [58].
Costello, Cole
12 Journal of Intensive Care Medicine XX(X); XXXX

Current knowledge suggests that the optimal agentfor treatment of RSE should have both GABA-ergicand NMDA antagonistic properties, be fast acting,cross the blood−brain barrier, have a short half-life,neuroprotective properties, and a favorable riskprofile. In the future, the pharmacogenomic profileof the patient may be another factor in determiningthe choice of agent for use in SE. At present, nosuch agent exists. Three classes of medications arecurrently in use for treatment of RSE: barbiturates,propofol, and benzodiazepines (midazolam). Eachhas particular advantages and disadvantages.
All patients in whom there is a possibility ofrefractory, ongoing seizure activity (manifesting clin-ically or confirmed electrographically) need to be
cared for in an ICU by staff proficient in the man-agement of SE [23]. These patients need long-termEEG monitoring and typically need intubation.Although the management of early SE should befamiliar to all frontline medical personnel, the care ofpatients in RSE should ideally be undertaken bythose with experience in the ICU management of SEand with immediate access to expertise in EEG mon-itoring and interpretation. Hence, after recognition ofSE and subsequent treatment with IV benzodi-azepine and phenytoin or fosphenytoin, the clinicianin charge should seek transfer to an ICU, ideallywhere continuous EEG monitoring is available. Ouroverall approach to the management of difficult-to-terminate seizure activity is outlined in Table 4.
Acute Seizures and Status Epilepticus
Journal of Intensive Care Medicine XX(X); XXXX 13
Table 4. Suggested Management of Refractory Status Epilepticus
Time Interventions
0-30 min Initial management of status epilepticus (see Table 3)At ~30 min Contact EEG laboratory to initiate cEEG monitoring
Transfer to ICU (intubate if necessary)Decide on use of (a) 3rd-line IV agent or (b) initiating infusion therapy (see below)
30-60 min 3rd-line IV agentOnward Use a 3rd-line IV agent (particularly if reluctant to intubate)
• administer 20 mg/kg bolus of IV phenobarbital at rate of 75 mg/min, followed by initial maintenance dosing 60 mg TID
OR• administer 15-30 mg/kg bolus of sodium valproate at rate of up to 6 mg/kg/min, followed by
maintenance dosing 500 mg TIDOR• administer 20mg/kg bolus of levetiracetam over 15 minutes, followed by maintenance dosing
1500 mg BIDInitiate EEG monitoring in ICU settingIf electrographic seizure activity persists after 3rd-line agent, initiate infusion therapy
>60 min Infusion therapyAfter 60 min of clinical or electrographic seizure activity, options include:1. Midazolam infusionloading dose: 0.2 mg/kg by slow IV bolusmaintenance cIV dose: 0.1-0.4 mg/kg/h,maximum cIV dose: 2.0 mg/kg/h2. Pentobarbital infusionloading dose: 3 mg/kg at 0.2-0.4 mg/kg/minmaintenance cIV dose: 0.3-3.0 mg/kg/hmaximum cIV dose: 3.0 mg/kg/h3. Propofol infusionloading dose: 1-2 mg/kg at 10 mg/minmaintenance cIV dose: 2-10 mg/kg/hmaximum cIV dose: 15 mg/kg/h (varies according to institution)Titrate infusion rate to abolish all clinical and electrographic seizure activity, irrespective of presence
or absence of burst−suppression pattern on EEG.Taper (in 25%-50% decrements every 12-24 hours) the midazolam, pentobarbital, or propofol cIV after
12-24 hours, once the therapeutic level of maintenance AED is achieved (ie, corrected phenytoinlevel, 20-30 μg/mL; phenobarbital level, 35-50 μg/mL; valproate level, 80-120 μg/mL) or thetherapeutic dose range is reached (topiramate, 800-1600 mg/d; levetiracetam, 1500-3000 mg/d).
EEG = electroencephalograph; cEEG = continuous electroencephalographic monitoring; ICU = intensive care unit; IV = intravenous; cIV = continuous intravenous infusion; AED = antiepileptic drug.

All patients receiving continuous infusions forthe management of SE should be in an ICU andshould have continuous EEG monitoring. Intermittent“snapshot” EEGs may be satisfactory once the patientreaches a status quo where a given infusion rateleads to seizure abolition; however, titration of infu-sion rates is best done using continuous EEG guid-ance. It is important for the clinicians to regularlyreview the EEG (3 times per day) and, ideally, befamiliar with the original ictal EEG pattern charac-teristic of that patient, particularly when faced withdeciding the significance of equivocal or difficultEEG findings. Staff members should highlight andcommunicate the recent EEG findings to other rele-vant carers. Repeated interaction with an epileptologistor neurophysiologist will aid in the interpretation ofthe video-EEG when difficulties arise.
The traditional end point for dosing continuousinfusion therapy with propofol, midazolam, andpentobarbital is induction of a burst−suppressionpattern where bursts of activity are separated by 10-to 15-second periods of EEG attenuation or flatten-ing. It is likely that seizure-suppression (ie, sup-pression of electrographic seizures, irrespective ofwhether the EEG enters a burst−suppression pat-tern) is a better end point than burst−suppressionwhere coma-inducing infusions are used. Althoughoften strived for, burst−suppression on continuousEEG monitoring has not been shown to improveclinical outcome [32,60]. Moreover, a patient whoseEEG reveals a burst−suppression pattern may stillexhibit electrographic seizure activity, and it mustbe remembered that suppression of the EEG doesnot necessarily equate with termination of seizures.However, until more sensitive means of neuro-physiologic or biomonitoring (ie, microdialysis),become available, scalp-derived EEG remains themost reliable and practical method for the monitor-ing of patients in SE.
The choice of coma-inducing agent(s) for contin-uous infusion therapy is often determined by physi-cian preferences and the particular aspects of aclinical case, particularly the presence of hypoten-sion. Barbiturates generally lead to a longer hospi-tal stay because the prolonged clearance leads to alonger recovery from iatrogenic coma. Someauthors avoid propofol in children because of anincreased risk of the propofol infusion syndrome.
The clinician should view the use of IV infusionsas temporary respite from seizure activity. It is crit-ical to ensure that the patient is placed and main-tained on appropriate doses of maintenance AEDsgiven enterally or as intermittent IV boluses thatwill, hopefully, prevent a return to SE when theinfusion(s) have been withdrawn. Intravenous admin-istration of AEDs should be used rather than enteral
administration if gastrointestinal motility andabsorption is impaired. In general, high-normal orsupra-therapeutic concentrations of maintenanceAEDs should be maintained; for example, correctedphenytoin level, 20 to 30 μg/mL; phenobarbitallevel, 35 to 50 μg/mL; and valproate level, 80 to 120μg/mL. In the absence of established therapeuticconcentration ranges, newer oral agents should bemaintained on full adult doses of these agents; forexample, topiramate, 800 to 1600 mg/d, and leve-tiracetam, 3000 to 4000 mg/d.
There are currently no prospectively acquireddata to support the use of one particular infusionregimen over another. What is clear, however, isthat each of these agents can be associated withparticular morbidities and thus should be used in agoal-oriented fashion rather than indefinitely. Theinfusions should be tapered gradually at fixed timepoints, usually every 12 to 24 hours. This can bedone in a staged manner where the dose is reducedby 25% to 50%, followed by a period of observation,followed by further tapering of the infusion, and soon. If one particular infusion regimen fails, as evi-denced by a return of clinical or electrographicseizures on discontinuation or reduction of the infu-sion, then that particular regimen should be aban-doned, although the agent may be used in acombination regimen thereafter.
Another useful strategy in managing a case ofRSE is to taper and temporarily discontinue the infu-sion therapy. This allows a fresh look at the EEGwithout the confounding effects of the IV infusionsand allows differentiation between the persistenceof sustained electroclinical SE and intermittent non-sustained electroclinical or electrographic seizures,which may not necessarily need treatment with con-tinuous IV AED therapy.
In conjunction with ongoing treatment of the SE,the clinician should be satisfied that he or she recog-nizes the underlying etiology. An unclear etiologyshould prompt systematic investigations includingMRI, CSF analysis, screening for infections (particu-larly if the patient is immunocompromised), parane-oplastic markers, antithyroid antibodies, porphyriascreen, and screens for toxins and illicit drugs.Particular effort should go into planning good qualityneuroimaging studies, including consideration of par-ticular sequences and techniques, for example,gadolinium administration, coronal views, MR venog-raphy, diffusion maps, and gradient-echo sequences.Careful planning with an experienced neuroradiolo-gist will greatly enhance the information gleanedfrom imaging, which may clarify the underlying eti-ology. If an etiology remains obscure, considerationshould be given to rare or unusual causes of RSE orrecurrent SE, which are listed in Table 5.
Costello, Cole
14 Journal of Intensive Care Medicine XX(X); XXXX

Antiseizure MedicationsUsed in Status Epilepticus
A limited number of AEDs are used in the manage-ment of SE. These medications overlap with theAEDs used in chronic epilepsy, although the doseescalation is more rapid and the desired serum con-centrations are higher when patients are in SE. Thetreating clinician should be familiar with dosing reg-imens and potential adverse effects associated witheach of the commonly used AEDs. The key aspectsof the commonly used AEDs are outlined here.
Benzodiazepines
The benzodiazepines are a family of medicationswhose mode of action is primarily agonistic atGABA receptors, which exert inhibitory effects onneurons. At high concentrations, benzodiazepineslimit sustained repetitive neuronal firing in a man-ner similar to that of carbamazepine and phenytoin.These agents are generally easy to administer byoral and parenteral routes, although new formula-tions administrable by the rectal, intranasal, andbuccal routes are being developed and used, par-ticularly diazepam and midazolam. Owing to theirrelative ease of use, the agents have become thefirst-line treatment for SE of any type. The principaladverse effects are sedation and respiratory sup-pression. When persistently administered, tachy-phylaxis becomes a significant problem.
Within the family of benzodiazepines, variousagents differ from each other, mainly by pharmaco-kinetic properties. In the hospital setting, the most
commonly used benzodiazepines are diazepam,lorazepam, and midazolam.
DiazepamDiazepam is highly protein-bound (99%). Although thehalf-life of the metabolite of diazepam is 20 to 40 hours,when administered IV, diazepam is rapidly redistrib-uted into body fat away from the brain, leading to ashort therapeutic effect of 15 to 20 minutes. Diazepammay be associated with a higher risk of ventilatory sup-pression requiring intubation among children.
LorazepamLorazepam has a slower onset of action of about 5minutes but a longer duration of action (4-14 hours)primarily due to retention in brain tissue. Hence,although diazepam has a quicker mode of onset, itseffect is curtailed by rapid redistribution, whereaslorazepam has a slower onset of action but moredurable clinical effect. This has led to replacementof diazepam with lorazepam as a first-line agent intreatment of seizures and SE.
MidazolamEffective parenteral benzodiazepine therapy can beimplemented by administering serial boluses orinfusions of diazepam or lorazepam, but in the ICU setting, midazolam has gained popularity as thebenzodiazepine of choice owing to its relativelyshort elimination half-life of 1.8 to 6.4 hours, rela-tively benign side-effect profile, and reported effec-tiveness [61]. Elimination takes place via hepaticmetabolism of midazolam to hydroxylated metabo-lites that are conjugated and excreted in the urine.Midazolam is very effective for suppression of
Acute Seizures and Status Epilepticus
Journal of Intensive Care Medicine XX(X); XXXX 15
Table 5. Rare or Under-recognized Causes of Status Epilepticus
Structural Occult cortical dysplasias and malformations of cortical developmentGenetic Mitochondrial disorders, porphyriaSystemic inflammatory disease Neurosarcoidosis, systemic lupus erythematosusCNS inflammatory disease Rasmussen encephalitis, primary angiitis of the CNS, Hashimoto encephalopathy,
ADEM, multiple sclerosis Infections Neurosyphilis, prion diseases, Bartonella, rabies, emerging forms of viral encephalitisIllicit drugs Cocaine, amphetamine derivatives, heroin, PCP, Ecstasy (MDMA)Oncologic causes Paraneoplastic limbic encephalitisToxic causes Domoic acid and marine toxins, other causes of toxic leukoencephalopathyIatrogenic causes Lithium toxicity, theophyllines, isoniazid (consider giving vitamin B6), insulin,
lidocaine, certain psychotropic agents, beta-lactam antibiotics, meperidine,cyclosporine, tiagabine, baclofen
Metabolic Hypocalcemia, hypomagnesemia, hypoglycemia from insulinoma, nonketotichyperglycemia
Vascular Central venous sinus thrombosis, antiphospholipid syndrome
CNS = central nervous system; ADEM = acute disseminated encephalomyelitis; PCP = phencyclidine; MDMA = 3,4-methylenedioxy-N-methylamphetamine.

seizure activity and is generally very well tolerated.However, the main difficulty with use of midazolamis tachyphylaxis, which becomes a problem within48 hours of initiation.
Phenytoin
Phenytoin remains the traditional second-lineAED, after the benzodiazepines. Phenytoin has theadvantages of relative ease of use, familiarity amongclinicians, cheap cost, long duration of action, andthe ability to rapidly load the patient in the EDor ICU. The disadvantages of phenytoin includehypotension, drug rashes, eosinophilia, irritativethrombophlebitis, purple-hand syndrome if extrava-sation occurs, and unstable serum concentrationscaused by zero-order kinetics, which may be par-ticularly problematic in the setting of renal dys-function or illness-associated hypoalbuminemia.
Phenytoin is a potent inducer of the P450 system,leading to increased metabolism of some concurrentlyprescribed medications. The half-life of phenytoinvaries according to the serum concentration, typi-cally about 24 hours at therapeutic concentrations.Phenytoin is extensively bound to albumin and theconcentration of free, unbound phenytoin (the activeagent) varies with albumin levels. The true “corrected”concentration (C) of phenytoin (in μg/mL) can be cal-culated by the Sheiner-Tozer equation as follows:
CCORRECTED = CMEASURED /[(0.2 × serum albumin) + 0.1]
In the setting of renal impairment with creati-nine clearance of less than 10 mL/min, the adjustedlevel is:
CCORRECTED = CMEASURED/[(0.1 × serum albumin) + 0.1]
In the setting of SE, clinicians should aim tomaintain the patient’s phenytoin concentration at15 to 25 μg/mL. A 20-mg/kg loading dose will typ-ically lead to a plasma concentration of more than20 μg/mL for the next 24 hours. Obtaining the levelof free phenytoin is the best way to assay pheny-toin concentrations, although this is not rapidlyavailable in many institutions.
Fosphenytoin
Fosphenytoin is a dose-equivalent pro-drug ofphenytoin used IV as an alternative to phenytoin.Its advantages are that it can be given more rapidlythan phenytoin (up to 150 mg/min IV) because it iswater soluble and less likely to cause problematic
hypotension, has a neutral pH in solution, and con-sequently leads to fewer injection site reactions.Like phenytoin, IV administration requires electro-cardiographic monitoring. Fosphenytoin can alsobe given intramuscularly, but absorption is too slowby this route for treatment of SE. The use of fos-phenytoin has been hampered by its expense,although it is generally safer than phenytoin to use.
Barbiturates
Barbiturates bind to specific sites on GABA-regulatedion channels. This leads to increased channel opentimes resulting in an increased influx of chloride ionsinto neurons with resultant enhanced hyperpolar-ization of the postsynaptic neuron. Barbiturates areclassified according to duration of action. Long-actingagents include phenobarbital, short-acting agentsinclude pentobarbital, and ultra−short-acting agentsinclude thiopental and methohexital.
PhenobarbitalPhenobarbital, also known as phenobarbitone, isthe traditional agent of choice after phenytoin hasproven ineffective in the setting of SE. However,the role of IV phenobarbital in SE is diminishingbecause of the recognition that a third-line AEDrarely terminates SE. Phenobarbital requires lessdilution, can be given as a slow IV push over 10minutes, and can be quick to control seizures [62].Phenobarbital is sedating although not sufficient toinduce a burst−suppression EEG pattern when a 20 mg/kg loading dose is administered. Many patientsneed intubation after a loading dose.
Phenobarbital has a very long half-life of 3 to 7days and accumulates in tissues; hence, patientsoften require a long waking-up period after signifi-cant doses are administered. Many clinicians nowfavor directly proceeding to continuous infusiontherapy rather than using a third-line AED such asphenobarbital. However, phenobarbital is still usefulin SE treatment where rapid access to an ICU is notavailable and when weaning a patient off continuousinfusion therapy. Phenobarbital rarely causes idio-syncratic reactions, but rashes, hepatic dysfunction,and aplastic anaemia have been reported.
Thiopental/PentobarbitalThe commonly used barbiturates for coma inrefractory SE are thiopental (used in Europe), or itsmetabolite pentobarbital (used in North America).These agents are very potent antiseizure medica-tions but are hampered by cardiovascular depres-sion and hypotension. Pentobarbital has a veryprotracted clearance, with a half-life of 144 hours,
Costello, Cole
16 Journal of Intensive Care Medicine XX(X); XXXX

leading to accumulation in tissues. The use of bar-biturate infusion therapies has become less popularamong clinicians with the advent of the shorter-acting agents propofol and midazolam. That said,there is a perception that barbiturate therapy is themost potent and effective of the infusion therapies[23]. Their main action is also agonistic at GABAA
receptors, with possible action also on Ca2+ chan-nels. Both thiopental and pentobarbital are NMDAantagonists in vitro. Barbiturates are known to causepoikilothermia and there is also some evidence thatbarbiturates exert immunologic effects [63].
Sodium Valproate
Sodium valproate is a very effective, traditionalbroad-spectrum antiseizure medication in whichthere has been a resurgence of interest owing tothe availability of an IV formulation. This role ofsodium valproate in SE has yet to be determined.It is frequently used when there is a contraindica-tion to the use of phenytoin/fosphenytoin or if thetreating clinician is hoping to avoid the use ofpharmacologic coma in the ICU. There is some evi-dence that intravenous valproate may be as effec-tive as phenytoin in the initial management of SE[64]. Sodium valproate is reported to be safe whenadministered rapidly as an infusion in medicallyunstable patients [65,66]. A loading dose of sodiumvalproate of 20 to 30 mg/kg yields an averageserum concentration of 132.6 μg/mL (range, 64-204μg/mL). One report of the use of sodium valproateinvolved administration of loading doses of up to78 mg/kg [67] at rates of up to 500 mg/min.
In the context of SE, recognized adverse effectsinclude hyperammonemia pancreatitis, (1:250patients treated), hepatic dysfunction and thrombo-cytopenia. A significant obstacle to the use of val-proate in medically complex patients or RSE is thedrug−drug interactions (sodium valproate is a P450enzyme system inhibitor) associated with valproate,particularly with other AEDs.
Preexisting thrombocytopenia precludes useof sodium valproate, particularly in patients withintracranial hemorrhages and collections. Hyper-ammonemia is a common and under-recognizedadverse effect of sodium valproate. Sodium valproateis contraindicated in patients with urea cycle disor-ders, such as ornithine transcarbamylase deficiency,and mitochondrial disorders. Ideally, all patients start-ing sodium valproate in the setting of SE should havean arterial ammonia level checked before therapy isinitiated, but certainly within 24 hours and at regularintervals thereafter. This is especially true in patientswith underlying hepatic dysfunction.
Sodium valproate has a half-life of 12 to 20 hoursand is 80% to 90% protein bound. Serum valproateconcentrations are notoriously variable in patientstaking valproate, often for unclear reasons. Thequoted therapeutic range is 50 to 120 mg/L. In thesetting of SE, the clinician should strive for a con-centration of at least 80 mg/L, usually requiring adaily maintenance dose of 500 mg (or more) by IVroute every 8 hours for the average 70-kg patient.
Propofol
Propofol is an ultra−short-acting, nondissociative IVanesthetic agent that was first used for proceduralsedation. The principal antiseizure mechanism ofaction is as an agonist on GABAA receptors, butmodulation of Ca2+ and Na+ channels has also beendescribed [68]. Its effect on NMDA glutamate recep-tors is unclear. Propofol is hydrophobic and is pre-pared as a milky white emulsion containing soybeanoil, egg lecithin, and glycerol. It is highly lipophilic,with a physiologic volume of distribution of 600 L.
Because of its short half-life of 3 minutes, it mustbe used in a continuous IV infusion for long-durationsedation. Propofol is only available in an IV formu-lation. An IV injection of a therapeutic dose ofpropofol produces hypnosis rapidly, with minimalexcitation, usually within 40 seconds. As with otherrapidly acting IV anesthetic agents, the half-time ofthe blood−brain equilibration is approximately 1 to3 minutes, and this accounts for the rapid inductionof anesthesia.
The pharmacodynamic properties of propofol aredependent on the therapeutic blood propofol con-centrations. Steady-state propofol blood concentra-tions are generally proportional to infusion rates,especially within an individual patient. Undesirableside effects such as cardiorespiratory depression arelikely to occur at higher blood concentrations thatresult from bolus dosing or a rapid increase in infu-sion rate. After an IV bolus dose, there is rapid equi-libration between the plasma and the highlyperfused tissue of the brain, thus accounting for therapid onset of anesthesia. Plasma levels initiallydecline rapidly as a result of rapid distribution andhigh metabolic clearance. Distribution accounts forabout half of this decline after a bolus of propofol.
The principal concern associated with use ofpropofol is that of the development of the propofolinfusion syndrome, a rare but often fatal syndromefirst described in critically ill children. The main fea-tures of the syndrome consist of cardiac failure, rhab-domyolysis, severe metabolic acidosis, and renalfailure. Propofol infusion syndrome typically occurs inthe setting of high infusion doses over long periods of
Acute Seizures and Status Epilepticus
Journal of Intensive Care Medicine XX(X); XXXX 17

time in patients who are otherwise very ill. A recentcomprehensive evaluation of use of propofol in abusy adult ICU suggested that this syndrome isdetectable by monitoring plasma triglyceride levelsand serum creatinine kinase concentrations. VigilantICU clinicians can thus be alerted early in the devel-opment of this preventable syndrome [69].
Some evidence suggests that propofol may notbe as safe as midazolam in very ill patients [70,71].One study found that propofol was associated with a56% mortality rate in patients with Acute Physiologyand Chronic Health Evaluation (APACHE) scoresexceeding 20, whereas patients treated with mida-zolam had a 17% mortality rate [70].
Carbamazepine, Oxcarbazepine,Topiramate, and Levetiracetam
These antiseizure medications are often added tothe acute AED regimen with the intention of pro-viding adequate maintenance AED coverage to pre-vent SE recurrence when infusion therapy iswithdrawn. In the setting of SE, these medicationsare generally titrated quickly up to dose rangesconsidered high in the outpatient setting.
• Carbamazepine is a traditional AED used in themanagement of chronic epilepsy. The use of car-bamazepine in SE is primarily as a maintenanceantiseizure medication, important when coma-inducing infusions are withdrawn. A parenteralformulation is not yet available. Typical dailydoses in the setting of SE are up to 1600 mg/d.
• Oxcarbazepine is used in the same way as carba-mazepine. A parenteral formulation is not yetavailable. Typical daily doses are up to 2400 mg/d.
• Topiramate is a new AED that has beenreported to be effective when administeredenterally in the setting of SE [72]. Topiramatecan be administered by nasogastric tube or rec-tally, is generally well tolerated except for mildsedation, and can be quickly titrated to doseranges of up to 1600 mg/d.
• Levetiracetam is a new AED that has gainedpopularity in the setting of ICU care.Levetiracetam can now be administered par-enterally as well as by nasogastric tube. Typicaldaily doses of levetiracetam in the setting of SEare up to 5000 mg/d. There are some prelimi-nary reports on the use of levetiracetam in thesetting of SE both as an IV agent and as a main-tenance AED given by nasogastric tube [73-75].The main advantage of levetiracetam in the set-ting of acute seizures and SE is the ease ofadministration, rapid titration, easy transition touse as a maintenance AED, and few drug−druginteractions. However, although this AED is
increasing in popularity, there are limited dataon its efficacy in SE in humans.
Other AEDs
The list of other maintenance AEDs is growing andincludes lamotrigine, gabapentin, zonisamide, pre-gabalin, felbamate, methsuximide, ethosuximide,acetazolamide, primidone, tiagabine, and vigabatrin.Although used in chronic epilepsy, these agents arerarely used in SE owing to slow titration or lack ofevidence for clinical efficacy in the setting of SE.Felbamate had promise as a maintenance AED buthas been associated with development of aplasticanemia in adults.
Novel Therapeutic Approaches in HighlyRefractory Status Epilepticus
Given that the best predictor of clinical outcomefrom SE is the underlying etiology, then it seemslikely that the most effective way to terminate RSEis to successfully treat the underlying cause. Hence,it is important to treat any active underlying diseaseprocesses in conjunction with treatment of the SEitself. However, many causes of SE are actually sta-tic or remote from the active episode of SE, such asan old stroke. Treatment of the SE should be thefocus of one’s efforts in these cases.
So what does a clinician do when a patient remainsin SE despite pharmacologic suppression of seizuresby coma-inducing agents? When confronted with apatient with persistent, highly refractory SE despiteapparently appropriate management, we recom-mend the following steps:
• Reevaluate the case and be satisfied that theunderlying cause has been identified, particu-larly metabolic, inflammatory, infectious, oriatrogenic causes.
• Ensure that imaging studies, using MRI, positronemission tomography (PET), and single-photonemission computed tomography (SPECT), ifavailable, have been conducted appropriatelyand studied adequately. These frequently reveala causal structural lesion.
• Be certain that the electrographic seizure activityis abolished while the patient is receiving infusiontherapy. The presence of a burst−suppressionpattern on EEG does not equate to abolition ofall seizure activity: the bursts may in fact be elec-trographic seizures. Study the bursts carefullyand compare them with the characteristic elec-trographic seizures evident at the onset of EEGrecording, before infusion therapy.
Costello, Cole
18 Journal of Intensive Care Medicine XX(X); XXXX

• Ensure that adequate levels of maintenanceAEDs are being used to increase the success ofan elective wean from infusion therapy.
• If an infusion therapy does not work, thenanother should be tried. There is little prospec-tive evidence that one agent (from midazolam,propofol, or pentobarbital) is more effective orsafer than another, although some retrospectivedata suggest that pentobarbital is more effective(but more likely to induce hypotension) thaneither propofol or midazolam [76]. If a giveninfusion therapy regimen does not terminate SEafter the initial 12- to 24-hour period, then it isunlikely to be successful after a 48- or 72-hourperiod. The regimen should be changed, andthe underlying etiology should be identifiedand treated.
If the patient continues to seize despite appropri-ate trials of appropriate regimens and the underlyingetiology has been managed appropriately, then othernovel therapeutic measures can be considered. Itmust be noted that use of these novel treatmentstrategies is based on anecdotal cases or small caseseries rather than prospective clinical trials.
Lastly, at times, when EEG activity is equivocalor difficult to interpret, it is not unreasonable totemporarily discontinue infusion therapies to allowclarification of the current clinical and EEG status.This is sometimes the only way to be sure that thepatient is still in SE. This is likely to be less riskythan prolonged trials of unnecessary treatment.
Surgical Intervention
Although rarely undertaken, surgery is a plausibleoption where electrographic SE remains focal, par-ticularly if there is evidence of a candidate causalstructural lesion. The very high morbidity and mor-tality rates associated with RSE argue for a role forsurgical intervention where that SE is focal and par-ticularly where the SE is related to a clearly delin-eated focal cortical lesion or region. Evidencesuggests that patients are unlikely to respond to are-trial of any particular medical intervention if theintervention failed on the initial trial [55,70,77,78].Hence, by working through a therapeutic algorithmon a day-by-day basis, one can identify possiblesurgical candidates.
Surgical resection of epileptogenic foci hasgained widespread acceptance as a valid therapeu-tic intervention in chronic epilepsy. The general cri-teria for surgery in patients with epilepsy are (1) theepilepsy is medically refractory, (2) the epilepsy isdisabling, (3) the focal epileptogenic region can
be identified, (4) the focal epileptogenic region canbe removed without risk of a cognitive, motor, orsensory deficit, and (5) removal of the epilepto-genic region has a reasonable expectation of com-plete or nearly complete abolition of further seizures.
The same criteria can be extended to the acutesetting of refractory focal SE. In the acute setting,however, consideration of postoperative deficitsand the prospect of long-term seizure freedomshould be weighed against the risks associated withongoing focal SE. The likelihood of successful inter-vention is related to identification of a causativecandidate structural lesion or functional epilepto-genic region and the timing of surgical resection.Identification of a structural lesion or functionalregion requires correlation of EEG findings withstructural (usually MR) and functional (usually PETor SPECT) imaging. This often requires an aggres-sive approach to imaging, with repeated studiesduring the course of SE and use of optimal imagingtechniques.
The timing of surgical intervention is critical to thelikelihood of success for a number of reasons.Historically, surgical intervention for refractory SE isundertaken as a last-ditch effort to terminate the SE,typically after at least a month in the ICU. Thesepatients are more likely to have suboptimal out-comes because they usually have undergone pro-longed medical therapy and their SE may haveevolved into a broader secondarily generalized elec-troclinical form of SE where the chance of success ofsurgical removal of a focal cortical region decreases.
There have been a number of reports of suc-cessful treatment of refractory focal SE by surgicalremoval of an underlying structural lesion, particu-larly in the pediatric population [79]. Surgery gen-erally involves removal of the structural lesion(lesionectomy) or brain region in which the lesionis embedded (partial or complete lobectomy) [80].
Multiple Continuous Infusion Therapy
In general, if a single-agent infusion therapy is noteffective on the first trial, it generally remains inef-fective thereafter. It is not known whether combina-tions of these infusions are more effective or safer. Ifhypotension is a major problem, then the infusionrate of pentobarbital can be lessened if midazolam iscommenced. Moreover, the different modes of actionmay enhance the chance of terminating SE. It isworth re-emphasizing that continuous infusion ther-apy simply provides temporary abolition of SE.Optimization of maintenance AED therapy is at leastas important as the choice of infusion therapy.
Acute Seizures and Status Epilepticus
Journal of Intensive Care Medicine XX(X); XXXX 19

Ketamine
Ketamine is a potent NMDA antagonist that hasbeen used in some institutions in the setting ofRSE. It is administered as a loading dose of2 mg/kg, followed by an infusion of 10 to 50μg/kg/min. Limited data are available on the useof this infusion therapy in humans, although itsuse in RSE has theoretic advantages. In establishedSE, there is evidence that excessive NMDA excita-tory receptor-mediated transmission is an impor-tant mechanism of persistent neuronal firing. Thismay explain the ineffectiveness of GABA agonistsin the latter stages of SE. Ketamine is used in thesame fashion as other coma-inducing agents; thatis, IV bolus, followed by maintenance infusion.The evidence for efficacy of ketamine is largelyanecdotal [47,81].
The reported adverse effects relate to its use asan analgesic, where hallucinations and other tran-sient psychotic sequelae are reported. Ketamine isassociated with cardiovascular stimulation and arise in arterial pressure and heart rate and shouldbe used with caution in patients with systemic orintracranial hypertension. Cerebellar damage hasalso been reported after longer-term use [82].
Lidocaine Infusion
There are a number of reports of successful use oflidocaine in the setting of RSE [83]. This agentshould not be used in patients with coexistingsinoatrial disorders, all grades of atrioventricularblock, or severe myocardial depression.
Inhalation Anesthetics
Inhalational anesthetics are used for the inductionand maintenance of anesthesia. There have beenseveral case reports of successful use of inhalationanesthetics in the setting of RSE [84]. These includeisoflurane and desflurane [85]. These agents havenot been rigorously tested in a clinical trial.
Paraldehyde
Paraldehyde was an important therapy in the pastbut is now rarely used because of difficulties inadministration and associated unwanted adverseeffects.
Direct Brain Stimulation
Although surface and deep brain stimulationdevices are being developed for use in focal andgeneralized epilepsies, their use has not beenreported in humans in the setting of SE.
Transcranial Magnetic Stimulation
Transcranial magnetic stimulation has similarly beenevaluated in animal models of focal SE but has notyet been reported to be helpful in human SE.
Electroconvulsive Therapy
Owing to its potent anticonvulsant actions, electro-convulsive therapy has been proposed as an inter-vention for SE [86]. It may seem illogical to administera proconvulsive stimulus in SE, but the after-cominginhibitory state after a convulsion induced by elec-troconvulsive therapy may, in theory, be beneficial topatients in SE. Electroconvulsive therapy has notbeen evaluated in a rigorous fashion by clinical trial.In our experience, it has not been helpful in the man-agement of refractory SE.
Diagnostic Toolsin Refractory Status Epilepticus
The principle advances in diagnostic techniques inthe setting of difficult-to-control SE have been digi-tal EEG recording and novel imaging approaches.These diagnostic modalities in conjunction withestablished investigations (CSF analysis, AED levels)allow greater insight into the etiology and progres-sion of SE in patients, particularly those who havebecome refractory.
Digital EEG has made continuous EEG monitor-ing with video much less cumbersome comparedwith paper EEG. Continuous digital EEG monitoringallows for easier data acquisition, reformatting, stor-age, and application of seizure-screening softwaretools such as event detection and spectral analysis.Continuous video recording in conjunction withEEG facilitates interpretation, principally by facilitat-ing artifact rejection and assessing the clinical corre-lation of paroxysmal EEG activity or events.
Imaging plays a role in the management of SE at2 levels. Most patients initially undergo imaging,typically with CT, in the ED or en route to an ICU.
Costello, Cole
20 Journal of Intensive Care Medicine XX(X); XXXX

This initial imaging is generally done to excludeneurosurgical causes for seizures, such as masslesions and traumatic injury, and to gauge the safetyof a planned lumbar puncture. Overall, CT imaginghas a limited further role in the specific manage-ment of SE.
In RSE, careful planning of appropriate structuraland functional imaging can maximize the informa-tion obtained with respect to the cause of the SEand the degree of progression. Before cliniciansinterpret such imaging, however, they need to befamiliar with potential peri-ictal changes frequentlyseen in patients with prolonged seizure activity thatare related to the ictal activity itself. These peri-ictalchanges should not be interpreted as structurallesions, although they often correlate neuroanatom-ically with an underlying structural lesion. Table 6lists recognized peri-ictal changes evident on imag-ing studies in some patients with SE or vigorouselectroclinical seizures.
These peri-ictal structural changes are best seenon MRI. Peri-ictal findings can be categorized aslocal or remote according to their proximity to thesite of maximal ictal EEG activity. Many of the find-ings described are reversible and do not necessar-ily equate with neuronal loss, although the factorsthat determine their occurrence and persistence areincompletely understood. It is likely that the remotediencephalic, corpus callosal (splenium), and con-tralateral cerebellar changes arise as a consequenceof abnormal reverberating para-ictal activity in cir-cuits involving these structures [87].
Local peri-ictal findings that may be presentinclude a swollen cortical ribbon with loss of grey−white matter differentiation. Increased T2 signalintensity due to edema occurs in areas of cortexand adjacent subcortical white matter. The local T2-weighted changes may be associated with MRI evi-dence of restricted diffusion, which are bright ondiffusion-weighted imaging and dark on apparentdiffusion coefficient maps, suggesting that they rep-resent cytotoxic rather than vasogenic edema.Whereas in acute ischemia, diffusion-weightedimages reveal restricted diffusion before any abnor-mality of the T2 signal becomes apparent, in ongo-ing SE, diffusion-weighted images and T2 signalchanges appear to occur roughly synchronously.Restricted diffusion has commonly been identifiedas a marker of irreversible ischemic injury, but recentstudies suggest that in some situations, decreaseddiffusion associated with seizures is reversible with-out the subsequent appearance of tissue injury.
Another important finding to recognize is theoccasional occurrence of migratory T2 and lesions
on diffusion-weighted imaging, appearing in remotecortical areas, distant from the original or principalseizure focus (in focal SE). It is important to recog-nize that these local findings, at times quite dramatic,are often reversible, at least in the early stages of SE.
Perhaps even more informative are the variousperi-ictal findings evident on functional neuroimag-ing techniques. Both ictal SPECT, which uses tech-netium Tc 99-hexamethyl-propyleneamine-oximeas a marker of local cerebral perfusion, and fluo-rodeoxyglucose (FDG)-PET, which uses fluo-rodeoxyglucose-18 as a marker for cortical glucoseutilization, can provide valuable data in focalseizures. Ictal SPECT may be used to localize theseizure focus in focal epilepsy. Imaging with FDG-PET often demonstrates peri-ictal focal hyperme-tabolism in SE of focal origin.
In our view, the most informative use of EEG struc-tural and function imaging modalities involves co-reg-istration of data sets from each of these diagnosticmodalities. This is critical if any surgical interventionis planned, but we have also found this approachinvaluable in the assessment of nonlesional SE wherea structural focus for the seizures is not evident.
Outcomes
Factors that are thought to contribute to the morbid-ity and mortality associated with SE are underlyingetiology, the age of the patient, and possibly, theduration of the SE. Secondary factors that likely con-tribute to the outcome from SE include sepsis, anoxia,duration of infusion therapy, and comorbid ICU-related medical complications. Data from 2 recentICU-based studies of SE [31,32], along with previousdata [1,4,9,54,88-92], can be used to summarize theclinical sequelae of a bout of SE (see Table 7).
Acute Seizures and Status Epilepticus
Journal of Intensive Care Medicine XX(X); XXXX 21
Table 6. Peri-ictal Imaging Findings
Local Remote
Mass effect Posterior leukoencephalopathyHippocampal swelling Unilateral/bilateral diencephalic
lesionsFocal cortical lesions Splenium abnormalitiesMigratory lesions Cerebellar diaschisisBlood−brain barrier
breakdownLocal increased
vascularityRestricted diffusion

Inpatient mortality is linked to potentially fataletiologies, increasing age, and severely impairedconsciousness when first evaluated [32]. Not sur-prisingly, the list of potentially fatal etiologies isidentical to the list of causes of RSE. As expected,patients with underlying anoxic brain injury, vascu-lar lesions, tumors, and infections fare worse thanpatients whose SE was provoked by alcohol, drugwithdrawal, or noncompliance with AED therapy.Although intuitively one would expect that abun-dance of data that SE results in neuronal injury, ithas been difficult to separate the morbidity associ-ated with the underlying cause of the SE frominjury due to the SE itself. Despite these constraints,there is some evidence that SE per se carries a 3%mortality rate [93]. Animal studies suggest that SE isassociated with significant neuronal injury [94,95].
There are numerous reports of progressive imag-ing findings in patients who have experienced anepisode of SE [96-98]. These reports typicallydescribe progressive hippocampal damage manifest-ing as atrophy, gliosis, and destruction of corticalarchitecture. Rare neuropathologic case reports havedescribed neuropathologic changes associated withSE in humans [97,99]. This correlates with neuronalloss within the hippocampus, especially in the CA1and CA4 regions, as well as neuronal loss in morediffuse brain regions [99,100].
One consistent long-term adverse outcome relatedto SE is progression to chronic epilepsy, seen in upto 90% [2,3,9,31,32]. The risk that enduring epilepsywill develop is approximately 4 times greater aftera bout of SE than after a single seizure. Althoughone would expect significant cognitive decline afteran episode of SE, this has been a less consistentfinding in the few and largely retrospective studiesthat have examined this question [101-103].
The mortality rates for SE, which are not uniformacross age groups, are about 40% for patients aged
older than 60 years and exceed 60% for those agedolder than 80 [104,105]. Patients with short-durationSE, lasting less than 1 hour, have a lower mortalityof 2.7% compared with the 32% mortality rate inthose with longer-duration SE that lasts more than1 hour [106]. This 1-hour demarcation may be acrude temporal dividing line between responsiveand refractory SE. Increased complications are evi-dent where SE persists for longer than 4 hours[105]. It must be noted that any study that includespatients with postanoxic SE skews mortality ratestoward the high end. Finally, NCSE was associatedin 1 study with an overall 18% mortality rate,although the patients who died had a greater bur-den of medical comorbidities [30]. As with convul-sive SE, the attributable morbidity and mortalityassociated with NCSE are difficult to quantify, but itseems clear that NCSE is not a favorable prognosticfactor in the ICU.
Despite the high morbidity associated with RSE,there are numerous reports of survival even aftervery prolonged hospital courses for SE, particularlyin children. As a rule, however, many patients willhave persistent refractory epilepsy and functionaldeficits [107,108]. Particularly alarming but less wellrecognized is that approximately 40% of patientswho survive the first 30 days after a first episode ofSE die within the next 10 years [109]. The combinedshort- and long-term mortality associated with SEaccounts for the estimated 22 000 deaths associatedwith SE per annum in the United States [7].
Problem Areas in Intensive Care UnitManagement of Status Epilepticus
The management of SE is frequently difficult. “Statusepilepticus” is not a single entity but is a heterogenouscollection of electroclinical syndromes with wide
Costello, Cole
22 Journal of Intensive Care Medicine XX(X); XXXX
Table 7. Morbidity and Mortality of Status Epilepticus
Variable Nonrefractory SE Refractory SE
Duration of seizure activity, h 2.4 92Seizure recurrence,a% 6.5 45.4Duration of stay, d
Intensive care unit 2.0 16.5Hospital 10-11.1 25.3-30
Mortality, %Inpatient 8.0-8.6 16.7-23.030-day 7.0-44
Discharge home without assistance, % 50 31Development of epilepsy, % 22.2-42.0 87.5
SE = status epilepticus.aWithin 24 hours of apparent termination of SE.

ranging etiologies, some benign and some malignant,and with varied clinical outcomes. Despite the vari-able manifestations and evolution, SE is often treatedby the same management algorithm within the sameinstitution. This one-size-fits-all approach is based onsolid evidence, particularly in the early stages of SE.However, a number of specific management prob-lems arise in patients with SE, particularly whenrefractory, that are not easily dealt with in an algo-rithmic fashion and can be difficult to resolve.
Significance of Periodic LateralizedEpileptiform Discharges
With the advent of continuous EEG monitoring, theclinician will frequently encounter rhythmic orrepetitive EEG patterns that do not have a parox-ysmal clinical correlate. These most common pat-terns include periodic lateralized epileptiformdischarges (PLEDs) and stimulus-related dischargessuch as stimulus-induced rhythmic, periodic, or ictaldischarges (SIRPIDS). When the EEGs in thesepatients are reviewed, it is important to recognizethat although sensitive to summated cortical activ-ity, the EEG is still a relatively crude 2-dimensionalmode of demonstrating complex cortical activities.Thus, benign and malignant neurophysiologicprocesses may be similarly represented without eti-ologic or prognostic distinction. Like seizures andSE, PLEDs are neurophysiologic markers of corticalinjury and disturbance.
The definition of PLEDs remains critical when try-ing to ascribe significance to this electrographicentity. Irrespective of the definition used, lateralizedepileptiform discharges are typically evident in thesetting of focal, acute brain injury or insult. The tra-ditional definition [110] of PLEDs highlighted the reg-ular, constant periodicity of the discharges occurringevery 0.5-2.0 seconds. Periodic lateralized epilepti-form discharges do not wax and wane in frequency,but remain relatively constant (see Figure 3). In ourview, epileptiform discharges that wax and wane(ie, are not periodic) should be thought of as inter-ictal epileptiform discharges, and that traditionalPLEDs are less epileptogenic than frequent, waxingand waning epileptiform discharges.
These are relative distinctions, however, becauseboth electrographic patterns are symptomatic ofunderlying cortical injury, from which substrateseizures can arise. These distinctions are often notvery helpful when one is at the bedside determiningif a particular EEG pattern represents seizure activ-ity. Generally speaking, we will not treat the EEGpattern per se after a single viewing. Recognition ofPLEDs will prompt us to continue EEG monitoringto make a determination of whether the PLEDs areinterictal or ictal in a given patient. Our overallapproach is to make a judgment based on the evo-lution of the EEG⎯comparing with EEGs done inthe past, if available⎯in conjunction with the clin-ical details. Comparison of the current EEG activitywith any previous unequivocal ictal EEG activity isoften the most useful way of ascribing significance to
Acute Seizures and Status Epilepticus
Journal of Intensive Care Medicine XX(X); XXXX 23
Fig 3. The electroencephalographic characteristics of periodic lateralized epileptiform discharges⎯regular, constantperiodicity of the discharges occurring at once per second or less.

PLEDs or repetitive epileptiform discharges. It oftenrequires review of at least an hour of EEG to deter-mine if a particular pattern is likely to be truly ictal.
Unwavering constant PLEDs persisting for hoursare less likely to represent true seizure activity.Electrographic seizure activity typically tends towax and wane in a crescendo-decrescendo mannerbecause the cerebral cortex is generally not capableof generating energy-expending hypersynchronousictal activity indefinitely but rather tends to gener-ate seizures in a stop-and-start fashion. The excep-tion to this rule may be electrographic SE of sleep(ESES) and epilepsia partialis continua, where ictalactivity can persist for long periods of time.
If available, functional imaging using SPECT orPET can be helpful to assess the significance ofPLEDs. A hotspot (focus of increased blood flow orincreased glucose uptake) on a SPECT or PET studyduring active PLED activity is suggestive of signifi-cant ongoing seizure activity, particularly if thehotspot is not evident on a repeat study when thePLEDs are suppressed by infusion therapy.
A number of studies have examined the out-comes of patients with EEGs exhibiting (presum-ably) new-onset PLEDs in the setting of acuteneurologic illness. Snodgrass et al [111] reportedthat 90% of such patients had 1 or more seizuresduring hospitalization and 60% to 70% had anepisode of SE. Walsh and Brenner [112] reportedthat 41% of patients whose EEGs demonstratedPLEDs died within 2 months. The limitations ofthese studies of PLEDs are that they were largely
retrospective and used varied definitions of PLEDs.Furthermore, it is likely that the true incidence ofPLEDs is underestimated, but only those patientswho had EEGs as a result of the development ofacute symptomatic seizures or altered mental statuswere discovered to have PLEDs.
Nonconvulsive status epilepticus versus encephalopa-thy. When trying to decide if a generalized peri-odic or rhythmic EEG pattern is due to NCSE or toa metabolic encephalopathy, it is important tofactor in the clinical aspects and evolution of thepatient, particularly changes in metabolic parame-ters. As such, there is no reliable method of distin-guishing NCSE from an encephalopathic EEG. Ourbelief is that the triphasic EEG pattern that arises inthe setting of metabolic disarray is neurophysiolog-ically similar to NCSE that arises in very ill ICUpatients (see Figure 4), and both of these patternsreflect diffuse cortical excitability.
Electroencephalographic artifact. The use of con-current video recording will help to determine ifthe EEG abnormalities are artifactual or have anassociated clinical correlate. This is particularlyimportant with the wide array of artifacts seen inthe ICU environment.
Paroxysmal clinical behaviors. Many ICU patientswill exhibit episodic behaviors of unclear significance.This should prompt the performance of an EEG, toexclude seizures, though other causes should be
Costello, Cole
24 Journal of Intensive Care Medicine XX(X); XXXX
Fig 4. Metabolic encephalopathy with characteristic “triphasic” morphology, in a longitudinal bipolar “double banana”montage. Examples of triphasic waves are highlighted.

considered. In general, if clinical movements arenonpatterned or nonspecific, then one should per-form an EEG rather than assume that the move-ments are seizures. Other behaviors that mimicseizures in the ICU include agitation due to pain orpartial awareness, transient ischemic attacks, delir-ium, nonepileptic myoclonus, hemiballism, brainstem-mediated posturing, motor manifestations of brainherniation, nonepileptic seizures or pseudostatus,and transient neurologic symptoms associated withcerebral amyloid angiopathy.
Nonepileptic seizures. It is not unheard of forpatients with nonepileptic seizures to present sorealistically that intubation and anesthesia are initi-ated. This is a very forgivable mistake, and gener-ally speaking, clinicians should err on the side ofcaution when dealing with atypical clinical presen-tations. It is important to obtain video EEG moni-toring early in the course of management to avoidinappropriate and potentially harmful management.
Nonconvulsive status epilepticus. There will be anincreasing awareness of NCSE because of moreproactive use of continuous EEG monitoring. Asmentioned above, although NCSE is clearly not agood prognostic sign in an ICU patient, it is not clearwhether the NCSE is an epiphenomenon in thesepatients or whether it carries attributable morbidityand mortality. It is not clear whether intervention forthe NCSE itself confers benefit to the patient.
Partial (focal) status epilepticus. Generally speak-ing, most cases of SE should be treated promptlyand aggressively. The most common cause of focalSE is stroke: seizures develop in 5% to 9% of acutestroke patients and SE develops in 20% of these[113]. However, caution should be taken whenmanaging some patients in focal SE, particularlywhen consciousness is preserved. The textbookexample is that of simple focal motor SE or epilepsia partialis continua. Epilepsia partialis con-tinua and other forms of focal SE where con-sciousness is preserved are often tolerated by thepatient and are sometimes very refractory to AEDtherapy, including infusion therapies. Epilepsiapartialis continua often persists for weeks but isless likely to lead to widespread cerebral damage.The appropriate approach to the management ofthese cases is often dictated by the underlying etiology and often does not involve pharmaco-logic coma in an ICU. Epilepsia partialis con-tinua may respond to correcting reversible causesof encephalopathy, for example, hyperosmolar nonketotic hyperglycemia.
When to stop treating highly refractive status epilep-ticus. In our estimation, the prognosis of theunderlying etiology determines the duration andintensity of extended (weeks to months) highlyrefractory SE. There are reports of good clinical out-comes from very prolonged (>1 month) episodes ofhighly refractory SE. However, if the underlying eti-ology causing the SE carries a grave prognosis (eg,glioblastoma multiforme), then a less aggressiveapproach of clearly defined duration, agreed on byfamily members, is appropriate.
Postanoxic Status Epilepticus
Postanoxic SE is a specific electroclinical state result-ing from diffuse cortical damage. Electrographically,the postanoxic state varies in severity from electro-cerebral silence to diffuse nonreactive alpha andtheta-range activity (“alpha coma” and “thetacoma”) to an intrinsic burst−suppression pattern tofrequent generalized epileptiform discharges. TheEEG findings may reflect the activity of the residualislands of viable cerebral cortex, which are some-times capable of generating background activity orepileptiform discharges.
Irrespective of the EEG findings, the patient mayor may not exhibit myoclonus. Such myoclonic sta-tus that arises in patients after an anoxic insult isusually transient (evolving into motionless coma)and invariably has a dismal outcome [114-117]. Thepresence of myoclonus may confer a worse prog-nosis than electrographic SE without clinical mani-festations. The myoclonus is often very dramaticand distressing for caregivers and family membersand in association with an “active” EEG, one feelscompelled to institute treatment.
We view such measures as being palliative,although it is critical to establish that the originalbrain injury was anoxic rather than due to a poten-tially reversible cause such as a lithium overdose. Areasonable course of action is to institute a clearlydefined course (24-48 hours) of IV propofol ormidazolam sufficient to abolish the myoclonus andto suppress the EEG. This can be performed in con-junction with other interventions such as head-cooling and administering neuroprotective agents.
During this period, useful prognostic informationcan be obtained by ancillary tests and serial clinicalevaluations such as MRI brain imaging, SPECTimaging, and somatosensory evoked potentials[117]. This prognostic information along with theclinical state of the patient after the infusion ther-apy, in consultation with family members, will dic-tate subsequent clinical management. It is critically
Acute Seizures and Status Epilepticus
Journal of Intensive Care Medicine XX(X); XXXX 25

important to determine that the cause of the comawas due to an anoxic event, because some causesof myoclonic SE carry a favorable prognosis, suchas myoclonic SE seen in primary generalizedepilepsy and lithium toxicity or after respiratoryarrest. Overall, we rely on the clinical history (cir-cumstances of cardiorespiratory arrest) and prog-nostic markers to a much greater extent than theEEG or the presence or absence of myoclonus toguide what we relay to the family and our clinicalmanagement of the case.
Potential Mistakes in the Management ofStatus Epilepticus
Potential errors in the management of SE do notrevolve around the nuances of choosing fifth- orsixth-line agents in RSE but relate to the early recog-nition and prompt use of appropriate doses ofappropriate first- and second-line AEDs. Potentialmistakes that can occur in the ED setting includeassuming that the seizure activity has terminatedwhen overt convulsive activity has stopped but thepatient remains obtunded, failure to administerappropriate loading doses of AEDs in proportion to thepatient’s weight, and failure to recognize nonepilepticseizures or pseudostatus. In general, one cannotovertreat SE in the acute setting. A more problematicerror is undertreatment of SE, because delay in treat-ment will lead to an increasingly refractory situation.
Potential errors in an ICU setting include the mis-labeling of paroxysmal clinical behaviors as seizures,underutilization of diagnostic EEG monitoring, lackof recognition of NCSE or metabolic encephalopa-thy, failure to initiate adequate amounts of mainte-nance AED therapy, and inappropriate delay inswitching from an ineffective treatment regimen(manifesting as ongoing seizure activity on EEGmonitoring) to another regimen. Overall, once atreatment regimen at appropriate doses is deemed tobe ineffective then another regimen should be insti-tuted promptly. Reinstituting a regimen that hasalready failed delays potentially successful interven-tions. Finally, potential mistakes in the diagnosticevaluation of patients with SE include misinterpret-ing perictal imaging findings as structural lesions andan inadequate search for an underlying etiology.
Future
In the future, as our understanding of the biologicevolution of SE increases, novel agents willundoubtedly emerge. To rigorously evaluate these
interventions in SE, the nomenclature used todescribe the various forms of SE and electrographicpatterns needs to be unified and clearly defined.This is particularly important when studying a het-erogenous syndrome. However, given the dynamicand protean nature of SE, it is unlikely that a single“magic bullet” will prove effective. Just as ourapproach to acute stroke has changed in the lastdecade, a similar shift in attitude and emphasistoward early recognition and intervention in SE isneeded.
In overt convulsive SE, treatment in the fieldby paramedical personnel may be effective at ter-minating SE at the potential expense of overtreatingsome seizures that would have self-terminated. Inthe ED setting, use of prefilled syringes with weight-appropriate doses of lorazepam (akin to prefilledsyringes used in cardiac resuscitation) may reduce thetime to first-line treatment. Another advance in theearly management of SE is the recent development ofEEG caps that allow easier initiation and recording ofEEG, critical in the early recognition of nonconvulsiveSE and pseudostatus. In the ICU setting, the principaladvance is the advent of continuous digital formatEEG monitoring allied to surveillance software tech-nology that will allow automatic detection of seizures.Other forms of monitoring, such as microdialysis, mayoffer very useful diagnostic information in the ICU set-ting, particularly when faced with equivocal EEG pat-terns such as PLEDs and NCSE.
The diagnostic workup of patients in SE is likelyto include functional and metabolic imaging suchas PET, SPECT, and MR spectroscopy as well asnovel structural imaging modalities and applica-tions. The therapeutic role of the newer AEDs andnewer parenteral formulations of existing AEDsremains to be determined. The use of other treat-ment modalities such as surgery and neurostimula-tion devices may increase with the increasingrecognition of heretofore poorly recognized struc-tural lesions such as dysplasias increasinglydetected by high resolution MRI in the setting of SE.
Conclusions
The initial management of SE is now well established,but the management of advanced or refractory SEremains a difficult proposition. However, advancesin our understanding of SE as well as both diagnos-tic and monitoring tools offer the prospect of betterclinical outcomes in the future. Early recognitionand intervention in SE is far more likely to succeedthan any delayed intervention. Ensuring an appro-priate dose of a first- and second-line antiseizure
Costello, Cole
26 Journal of Intensive Care Medicine XX(X); XXXX

medication is more important than which specificagent is chosen. The morbidity of administeringexcessive amounts of first- or second-line antiseizuremedications is far less than the morbidity of endur-ing seizure activity or the adverse effects associatedwith prolonged treatment of SE in an ICU setting.
The ICU management of refractory SE is stilllargely operator-dependent. There is a pressingneed for a prospective multicenter trial to deter-mine the best of the currently available strategiesfor the management of refractory SE. All ED, neu-rology, and ICU personnel should be well versed inthe initial management of SE. It behooves para-medic personnel, neurologists, and clinicians in theED and ICU to collectively develop and implementa practical treatment algorithm applicable to theirinstitution for the comprehensive management ofSE, beginning in the community and ending in theICU. Neurologists are ideally placed to manage SE,particularly those with a knowledge of EEG, andshould be consulted early.
Because of the high morbidity and mortalityassociated with SE, physicians and staff must beaggressive in the management of SE. It is impera-tive to follow a designated therapeutic algorithmand progress to the next step in the algorithm if thecurrent intervention is proving ineffective. Finally,surgery should be considered a potential therapeu-tic option in refractory focal SE.
References
1. DeLorenzo RJ, Hauser WA, Towne AR, et al. A prospectivepopulation-based epidemiological study of status epilepti-cus in Richmond, Virginia. Neurology. 1996;46:1029-1035.
2. Hesdorffer DC, Logroscino G, Cascino G, Annegers JF,Hauser WA. Incidence of status epilepticus in Rochester,Minnesota, 1965-1985. Neurology. 1998;50:735-741.
3. Hauser WA. Status epilepticus: epidemiologic considera-tions. Neurology. 1990;40:S9-S13.
4. Coeytaux A, Jallon P, Galobardes B, Morabia A. Incidence ofstatus epilepticus in French-speaking Switzerland (EPISTAR).Neurology. 2000;55:693-697.
5. Chin RF, Neville BG, Scott RC. A systematic review of theepidemiology of status epilepticus. Eur J Neurol. 2004;11:800-810.
6. Penberthy L, Towne A, Garnett L, et al. Costs of statusepilepticus [Abstract]. Epilepsia. 1997;38:s225.
7. DeLorenzo RJ, Pellock JM, Towne AR, Boggs JG.Epidemiology of status epilepticus. J Clin Neurophysiol.1995;12:316-325.
8. Fisher RS, van Emde Boas W, Blume W, et al. Epilepticseizures and epilepsy: definitions proposed by the Interna-tional League Against Epilepsy (ILAE) and the InternationalBureau for Epilepsy (IBE). Epilepsia. 2005;46:470-472.
9. Aminoff MJ, Simon RP. Status epilepticus. Causes, clinicalfeatures and consequences in 98 patients. Am J Med.1980;69:657-666.
10. Theodore WH, Porter RJ, Albert P, et al. The secondarilygeneralized tonic-clonic seizure: a videotape analysis.Neurology. 1994;44:1403-1407.
11. Shorvon S. Status Epilepticus: Its Clinical Features andTreatment in Children and Adults. Cambridge UK:Cambridge University Press; 1994.
12. Commission on Terminology of the International Leagueagainst Epilepsy. A proposed international classification ofepileptic seizures. Epilepsia. 1964;5:297-306.
13. Lowenstein DH, Bleck T, Macdonald RL. It’s time to revise thedefinition of status epilepticus. Epilepsia. 1999;40:120-122.
14. Treiman DM, Walton NY, Kendrick C. A progressivesequence of electroencephalographic changes during gen-eralized convulsive status epilepticus. Epilepsy Res. 1990;5:49-60.
15. Drislane FW, Schomer DL. Clinical implications of general-ized electrographic status epilepticus. Epilepsy Res. 1994;19:111-121.
16. DeLorenzo RJ, Waterhouse EJ, Towne AR, et al. Persistentnonconvulsive status epilepticus after the control of con-vulsive status epilepticus. Epilepsia. 1998;39:833-840.
17. Thomas P, Beaumanoir A, Genton P, et al. “De novo”absence status of late onset: report of 11 cases. Neurology.1992;42:104-110.
18. Scholtes FB, Renier WO, Meinardi H. Non-convulsive statusepilepticus: causes, treatment, and outcome in 65 patients.J Neurol Neurosurg Psychiatry. 1996;61:93-95.
19. Cockerell OC, Walker MC, Sander JW, et al. Complex par-tial status epilepticus: a recurrent problem. J NeurolNeurosurg Psychiatry. 1994;57:835-837.
20. Scholtes FB, Renier WO, Meinardi H. Simple partial statusepilepticus: causes, treatment, and outcome in 47 patients.J Neurol Neurosurg Psychiatry. 1996;61:90-92.
21. Privitera M, Hoffman M, Moore JL, Jester D. EEG detectionof non tonic-clonic status epilepticus in patients withaltered consciousness. Epilepsy Res. 1994;18:155-166.
22. Lowenstein DH, Aminoff MJ. Clinical and EEG features ofstatus epilepticus in comatose patients. Neurology.1992;42:100-104.
23. Claassen J, Mayer SA, Kowalski RG, et al. Detection of elec-trographic seizures with continuous EEG monitoring in crit-ically ill patients. Neurology. 2004;62:1743-1748.
24. Haffey S, McKernan A, Pang K. Non-convulsive statusepilepticus: a profile of patients diagnosed within a tertiaryreferral centre. J Neurol Neurosurg Psychiatry. 2004;75:1043-1044.
25. Husain AM, Horn GJ, Jacobson MP. Non-convulsive statusepilepticus: usefulness of clinical features in selectingpatients for urgent EEG. J Neurol Neurosurg Psychiatry.2003;74:189-191.
26. Hirsch LJ, Claassen J, Mayer SA, et al. Stimulus-inducedrhythmic, periodic, or ictal discharges (SIRPIDs): a commonEEG phenomenon in the critically ill. Epilepsia. 2004;45:109-123.
27. Treiman DM, Meyers PD, Walton NY, et al. A comparisonof four treatments for Generalized convulsive status epilep-ticus. Veterans Affairs Status Epilepticus Cooperative StudyGroup. N Engl J Med. 1998;339:792-798.
28. Kaplan PW. Assessing the outcomes in patients with non-convulsive status epilepticus: nonconvulsive status epilep-ticus is underdiagnosed, potentially overtreated, andconfounded by comorbidity. J Clin Neurophysiol.1999;16:341-352.
29. Towne AR, Waterhouse EJ, Boggs JG, et al. Prevalence ofnonconvulsive status epilepticus in comatose patients.Neurology. 2000;54:340-345.
30. Shneker BF, Fountain NB. Assessment of acute morbidityand mortality in nonconvulsive status epilepticus. Neurology.2003;61:1066-1073.
31. Holtkamp M, Othman J, Buchhheim K, et al. Predictors andprognosis of refractory status epilepticus treated in a neu-rological intensive care unit. J Neurol Neurosurg Psychiatry.2005;76:534-539.
32. Rossetti AO, Logroscino G, Bromfield EB. Refractory statusepilepticus: effect of treatment aggressiveness on progno-sis. Arch Neurol. 2005;62:1698-1702.
Acute Seizures and Status Epilepticus
Journal of Intensive Care Medicine XX(X); XXXX 27

33. Barolomei F, Gastaut JL. Complex partial status epilepticusprovoked by hyponatraemia. Eur Neurol. 1998;40:53-54.
34. Wijdicks EF, Sharbrough FW. New-onset seizures in criti-cally ill patients. Neurology. 1993;43:1042-1044.
35. Varelas PN, Mirski MA. Seizures in the adult intensive careunit. J Neurosurg Anesthesiol. 2001;13:163-175.
36. Jordan KG. Present status of critical care research. Crit CareMed. 1992;20:716.
37. Cole AJ. Is epilepsy a progressive disease? The neurobiolog-ical consequences of epilepsy. Epilepsia. 2000;41:S13-S22.
38. Coulter DA, DeLorenzo RJ. Basic mechanisms of statusepilepticus. Adv Neurol. 1999;79:725-733.
39. Wasterlain CG, Fujikawa DG, Penix L, et al.Pathophysiological mechanisms of brain damage from sta-tus epilepticus. Epilepsia. 1993;34(suppl 1):37-53.
40. Lothman E. The biochemical basis and pathophysiology ofstatus epilepticus. Neurology. 1990;40(suppl 2):13-23.
41. Manno EM, Pfeifer EA, Cascino GD, et al. Cardiac pathol-ogy in status epilepticus. Ann Neurol. 2005;58:954-957.
42. Walton NY, Treiman DM. Motor and electroencephalo-graphic response of refractory experimental status epilepti-cus in rats to treatment with MK-801, diazepam, or MK-801plus diazepam. Brain Res. 1991;553:97-104.
43. Kapur J. Hippocampal Neurons Express GABA-A ReceptorInsensitive to Diazepam in Hyperexcitable Conditions.Epilepsia 2000;41:S86-S89.
44. Lowenstein DH, Alldredge BK. Status epilepticus at an urbanpublic hospital in the. 1980s. Neurology. 1993;43:483-488.
45. Sisodiya SM, Thom M. Widespread upregulation of drug-resistance proteins in fatal human status epilepticus. Epilepsia.2003;44:261-264.
46. Bleck TP. Refractory status epilepticus in. 2001. ArchNeurol. 2002;59:188-189.
47. Borris DJ, Bertram EH, Kapur J. Ketamine controls pro-longed status epilepticus. Epilepsy Res. 2000;42:117-122.
48. Jevtovic-Todorovic V, Wozniak DF, et al. Propofol andsodium thiopental protect against MK-801-induced neu-ronal necrosis in the posterior cingulated/retrosplenial cor-tex. Brain Res. 2001;913:185-189.
49. Dreifuss FE, Rosman NP, Cloyd JC, et al. A comparison ofrectal diazepam gel and placebo for acute repetitiveseizures. N Engl J Med. 1998;338:1869-1875.
50. McIntyre J, Robertson S, Norris E, et al. Safety and efficacyof buccal midazolam versus rectal diazepam for emergencytreatment of seizures in children: a randomized controlledtrial. Lancet. 2005;366:205-210.
51. Alldredge BK, Gelb AM, Isaacs SM, et al. A comparison oflorazepam, diazepam, and placebo for the treatment of out-of-hospital status epilepticus. N Engl J Med. 2001;345:631-637.
52. Appleton R, Sweeney A, Choonara I, et al. Lorazepam ver-sus diazepam in the acute treatment of epileptic seizures andstatus epilepticus. Dev Med Child Neurol. 1995;37:682-688.
53. Cock HR, Schapira AH. A comparison of lorazepam anddiazepam as initial therapy in convulsive status epilepticus.Quart J Med. 2002;95:225-231.
54. Mayer SA, Claassen J, Lokin J, et al. Refractory status epilep-ticus: frequency, risk factors, and impact on outcome. ArchNeurol. 2002;59:205-210.
55. Osorio I, Reed RC. Treatment of refractory generalizedtonic-clonic status epilepticus with pentobarbital anesthesiaafter high-dose phenytoin. Epilepsia. 1989;30:464-471.
56. Walker MC, Smith SJ, Shorvon SD. The intensive care treat-ment of convulsive status epilepticus in the UK. Results ofa national survey and recommendations. Anaesthesia.1995;50:130-135.
57. Holtkamp M, Masuhr F, Harms L, et al. The management ofrefractory generalized convulsive and complex partial statusepilepticus in three European countries: a survey amongepileptologists and critical care neurologists. J NeurolNeurosurg Psychiatry. 2003;74:1095-1099.
58. Claassen J, Hirsch LJ, Mayer SA. Treatment of status epilep-ticus: a survey of neurologists. J Neurol Sci. 2003;211:37-41.
59. Eriksson K, Metsaranta P, Huhtala H, Auvinen A, KuuselaAL, Koivikko M. Treatment delay and the risk of prolongedstatus epilepticus. Neurology. 2005;65:1316-1318.
60. Krishnamurthy KB, Drislane FW. Depth of EEG suppressionand outcome in barbiturate anesthetic treatment for refrac-tory status epilepticus. Epilepsia. 1999;40:759-762.
61. Claassen J, Hirsch LJ, Emerson RG, et al. Continuous EEGmonitoring and midazolam infusion for refractory noncon-vulsive status epilepticus. Neurology. 2001;57:1036-1042.
62. Shaner DM, McCurdy SA, Herring MO, Gabor AJ. Treatmentof status epilepticus: a prospective comparison ofdiazepam and phenytoin versus phenobarbital andoptional phenytoin. Neurology. 1988;38:202-207.
63. Kress HG, Eberlein T, Horber B. Suppression of neutrophilmigration and chemiluminescence is due to the sulphuratom in the thiobarbiturate molecule. Acta AnaesthesiolScand. 1989;33:122-128.
64. Venkataraman V, Wheless JW. Safety of rapid intravenousinfusion of valproate loading doses in epilepsy patients.Epilepsy Res. 1999;35:147-153.
65. Sinha S, Naritoku DK. Intravenous valproate is well toler-ated in unstable patients with status epilepticus. Neurology.2000;55:722-724.
66. Yu KT, Mills S, Thompson N, Cunanan C. Safety and effi-cacy of intravenous valproate in pediatric status epilepticusand acute repetitive seizures. Epilepsia. 2003;44: 724-726.
67. Limdi NA, Shimpi AV, Faught E, et al. Efficacy of rapid IVadministration of valproic acid for status epilepticus.Neurology. 2005;64:353-355.
68. Marik PE. Propofol: therapeutic indications and side-effects.Curr Pharm Des. 2004;10:3639-3649.
69. Rossetti AO, Reichhart MD, Schaller MD, Despland PA,Bogousslavsky J. Propofol treatment of refractory statusepilepticus: a study of 31 episodes. Epilepsia. 2004;45:757-763.
70. Prasad A, Worrall BB, Bertram EH, et al. Propofol andmidazolam in the treatment of refractory status epilepticus.Epilepsia. 2001;42:380-386.
71. Stecker MM, Kramer TH, Raps EC O’Meeghan R, DulaneyE, Skaar DJ. Treatment of refractory status epilepticus withpropofol: clinical and pharmacokinetic findings. Epilepsia.1998;39:18-26.
72. Towne AR, Garnett LK, Waterhouse EJ, Morton LD,DeLorenzo RJ. The use of topiramate in refractory statusepilepticus. Neurology. 2003;60:332-334.
73. Rossetti AO, Bromfield EB. Levetiracetam in the treatmentof status epilepticus in adults: a study of 13 episodes. EurNeurol. 2005;54:34-8.
74. Baulac M, Brodie MJ, Elger CE, et al. Levetiracetam intra-venous infusion as an alternative to oral dosing in patientswith partial-onset seizures. Epilepsia. 2007;48:589-92.
75. Rupprecht S, Franke K, Fitzek S, Witte OW, Hagemann G.Levetiracetam as a treatment option in non-convulsive sta-tus epilepticus. Epilepsy Res. 2007;73:238-44.
76. Claassen J, Hirsch LJ, Emerson RG, Mayer SA. Treatment ofrefractory status epilepticus with pentobarbital, propofol,or midazolam: a systematic review. Epilepsia. 2002;43:146-153.
77. Krishnamurthy KB, Drislane FW. Relapse and survival afterbarbiturate anesthetic treatment of refractory status epilep-ticus. Epilepsia. 1996;37:863-867.
78. Yaffe K, Lowenstein DH. Prognostic factors of pentobarbi-tal therapy for refractory generalized status epilepticus.Neurology. 1993;43:895-900.
79. Alexopoulos A, Lachhwani DK, Gupta A, et al. Resectivesurgery to treat refractory status epilepticus in children withfocal epileptogenesis. Neurology. 2005;64:567-570.
80. Costello DJ, Simon MV, Eskandar EN, et al. Efficacy of sur-gical treatment of de novo adult-onset cryptogenic refrac-tory focal status epilepticus Arch Neurol. 2006;63:895-901.
81. Yen W, Williamson J, Bertram EH, Kapur J. A comparisonof three NMDA receptor antagonists in the treatment ofprolonged status epilepticus. Epilepsy Res. 2004;59:43-50.
Costello, Cole
28 Journal of Intensive Care Medicine XX(X); XXXX

82. Ubogu EE, Sagar SM, Lerner AJ, et al. Ketamine for refrac-tory status epilepticus: a case of possible ketamine-inducedneurotoxicity. Epilepsy Behav. 2003;4:70-75.
83. Walker IA, Slovis CM. Lidocaine in the treatment of statusepilepticus. Acad Emerg Med. 1997;4:918-922.
84. Kofke WA, Bloom MJ, Van Cott A, Brenner RP.Electrographic tachyphylaxis to etomidate and ketamineused for refractory status epilepticus controlled with isoflu-rane. J Neurosurg Anesthesiol. 1997;9:269-272.
85. Mirsattari SM, Sharpe MD, Young GB. Treatment of refrac-tory status epilepticus with inhalational anesthetic agentsisoflurane and desflurane. Arch Neurol. 2004;61:1254-1259.
86. Carrasco Gonzalez MD, Palomar M, Rovira R. Electrocon-vulsive therapy for status epilepticus. Ann Intern Med.1997;127:247-248.
87. Lothman EW, Bertram EH, Stringer JL. Functional anatomyof hippocampal seizures. Prog Neurobiol. 1991;37:1-82.
88. Hesdorffer DC, Logroscino G, Cascino G, Annegers JF,Hauser WA. Risk of unprovoked seizure after acute symp-tomatic seizure: effect of status epilepticus. Ann Neurol.1998;44:908-912.
89. Logroscino G, Hesdorffer DC, Cascino G, Annegers JF,Hauser WA. Short-term mortality after a first episode of sta-tus epilepticus. Epilepsia. 1997;38:1344-1349.
90. Knake S, Rosenow F, Vescovi M, et al. Incidence of statusepilepticus in adults in Germany: a prospective, population-based study. Epilepsia. 2001;42:714-718.
91. Vignatelli L, Tonon C, D’Alessandro R; Bologna Group forthe Study of Status Epilepticus. Incidence and short-termprognosis of status epilepticus in adults in Bologna, Italy.Epilepsia. 2003;44:964-968.
92. Logroscino G, Hesdorffer DC, Cascino GD, et al. Mortalityafter a first episode of status epilepticus in the United Statesand Europe. Epilepsia. 2005;46(suppl 11):46-58
93. Waterhouse EJ, Vaughan JK, Barnes TY, et al. Synergisticeffect of status epilepticus and ischemic brain injury onmortality. Epilepsy Res. 1998;29:175-183.
94. Holmes, GL. Seizure-induced neuronal injury: animal data.Neurology. 2002;59(suppl 5):3-6.
95. Meldrum BS, Vigouroux RA, Rage P, Brierley JB.Hippocampal lesions produced by prolonged seizures inparalyzed artificially ventilated baboons. Experientia.1973;29:561-563.
96. Wieshmann UC, Woermann FG, Lemieux L, et al.Development of hippocampal atrophy: a serial magneticresonance imaging study in a patient who developedepilepsy after generalized status epilepticus. Epilepsia.1997;38:1238-1241.
97. Pohlmann-Eden B, Gass A, Peters CN, Wennberg R,Blumcke I. Evolution of MRI changes and development ofbilateral hippocampal sclerosis during long lasting general-ized status epilepticus. J Neurol Neurosurg Psychiatry.2004;75:898-900.
98. Doherty CP, Cole AJ, Grant PE, et al. Multi-modal longitu-dinal imaging in focal status epilepticus. Can J Neurol Sci.2004;31:276-281.
99. Nixon J, Bateman D, Moss T. An MRI and neuropathologi-cal study of a case of fatal status epilepticus. Seizure.2001;10:588-591.
100. Fujikawa DG, Itabashi HH, Wu A, Shinmei SS. Statusepilepticus-induced neuronal loss in humans without sys-temic complications or epilepsy. Epilepsia. 2000;41:981-991.
101. Maytal J, Shinnar S, Moshe SL, Alvarez LA. Low morbidityand mortality of status epilepticus in children. Pediatrics.1989;83:323-331.
102. Dodrill CB, Wilensky AJ. Intellectual impairment as an out-come of status epilepticus. Neurology. 1990;40(suppl 2):23-27.
103. Adachi N, Kanemoto K, Muramatsu R, et al. Intellectualprognosis of status epilepticus in adult epilepsy patients:analysis with Wechsler Adult Intelligence Scale revised.Epilepsia. 2005;46:1502-1509.
104. DeLorenzo RJ, Towne AR, Pellock JM, Ko D. Statusepilepticus in children, adults, and the elderly. Epilepsia.1992;33(suppl 4): 15-25.
105. Scholtes FB, Renier WO, Meinardi H. Generalized convul-sive status epilepticus: causes, therapy, and outcome in 346patients. Epilepsia. 1994;35:1104-1012.
106. Towne AR, Pellock JM, Ko D, DeLorenzo RJ. Determinantsof mortality in status epilepticus. Epilepsia. 1994;35:27-34.
107. Sahin M, Menache CC, Holmes GL, Riviello JJ. Outcome ofsevere refractory status epilepticus in children. Epilepsia.2001;42:1461-1467.
108. Sahin M, Menache CC, Holmes GL, Riviello JJ Jr. Prolongedtreatment for acute symptomatic refractory status epilepti-cus: outcome in children. Neurology. 2003;61:398-401.
109. Logroscino G, Hesdorffer DC, Cascino GD, Annegers JF,Bagiella E, Hauser WA. Long-term mortality after a firstepisode of status epilepticus. Neurology. 2002;58:537-541.
110. Chatrian GE, Shaw CM, Leffman H. The significance ofperiodic lateralized epileptiform discharges in EEG: anelectrographic, clinical and pathological study.Electroencephalogr Clin Neurophysiol. 1964;17:177-193.
111. Snodgrass SM, Tsuburaya K, Ajmone-Marsan C. Clinical sig-nificance of periodic lateralized epileptiform discharges:relationship with status epilepticus. J Clin Neurophysiol.1989;6:159-172.
112. Walsh JM, Brenner RP. Periodic lateralized epileptiformdischarges—long-term outcome in adults. Epilepsia. 1987;28:533-536.
113. Rumbach L, Sablot D, Berger E, Tatu L, Vuillier F, Moulin T.Status epilepticus in stroke: report on a hospital-basedstroke cohort. Neurology. 2000;54:350-354.
114. Wijdicks EF, Parisi JE, Sharbrough FW. Prognostic value ofmyoclonus status in comatose survivors of cardiac arrest.Ann Neurol. 1994;35:239-243.
115. Celesia GG, Grigg MM, Ross E. Generalized status myocloni-cus in acute anoxic and toxic-metabolic encephalopathies.Arch Neurol. 1988;45:781-784.
116. Young GB, Gilbert JJ, Zochodne DW. The significance ofmyoclonic status epilepticus in postanoxic coma.Neurology. 1990;40:1843-1848.
117. Zandbergen EG, Hijdra A, Koelman JH, et al. Prediction ofpoor outcome within the first 3 days of postanoxic coma.Neurology. 2006;66:62-68.
Acute Seizures and Status Epilepticus
Journal of Intensive Care Medicine XX(X); XXXX 29