Embed Size (px)
Citation preview
TreatmentofType2Diabetes:WhatToDoWhenTreatmentwithMetformin
isInadequate?CanWeAchieveTherapeuticGoalsMore
Safely?MartinJ.Abrahamson,MDFACP
AssociateProfessorofMedicine,HarvardMedicalSchoolCOPYRIG
HT
WhatIwillcover
• Magnitudeoftheproblem• Pathophysiologyoftype2diabetes• The”guidelines”• Factorstoconsiderwhenchoosingamedication/stoaddtometformin
• Cardiovascularoutcomesstudies• Whichcombinationsmightbeappropriate?COP
YRIGHT
COPYRIG
HT
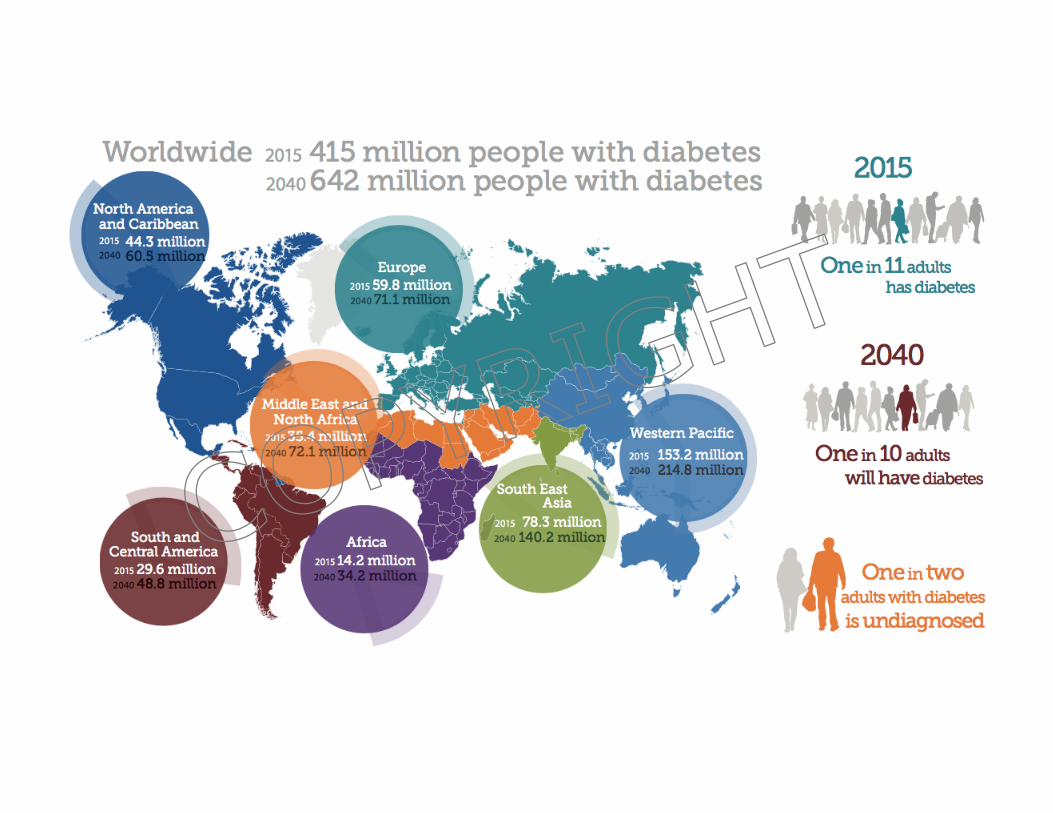
• Morethan29millionpeople– justover9%ofthepopulation
• 25%undiagnosed• Thenumberisgrowingby>1millionperyear• Amajorcauseofmortalityandmorbidity• Cost(directandindirect)$245billionperyear
• 1in10UShealthcaredollarsspentondiabetes• Almost86millionpeopleatriskfordiabetes• Goodnews– therateofnewcasesisdeclining(only1.4millionnewcasesperyearvs1.8million)
DiabetesintheUSAToday:AnEpidemic
Diabetes Care 2010
COPYRIG
HT
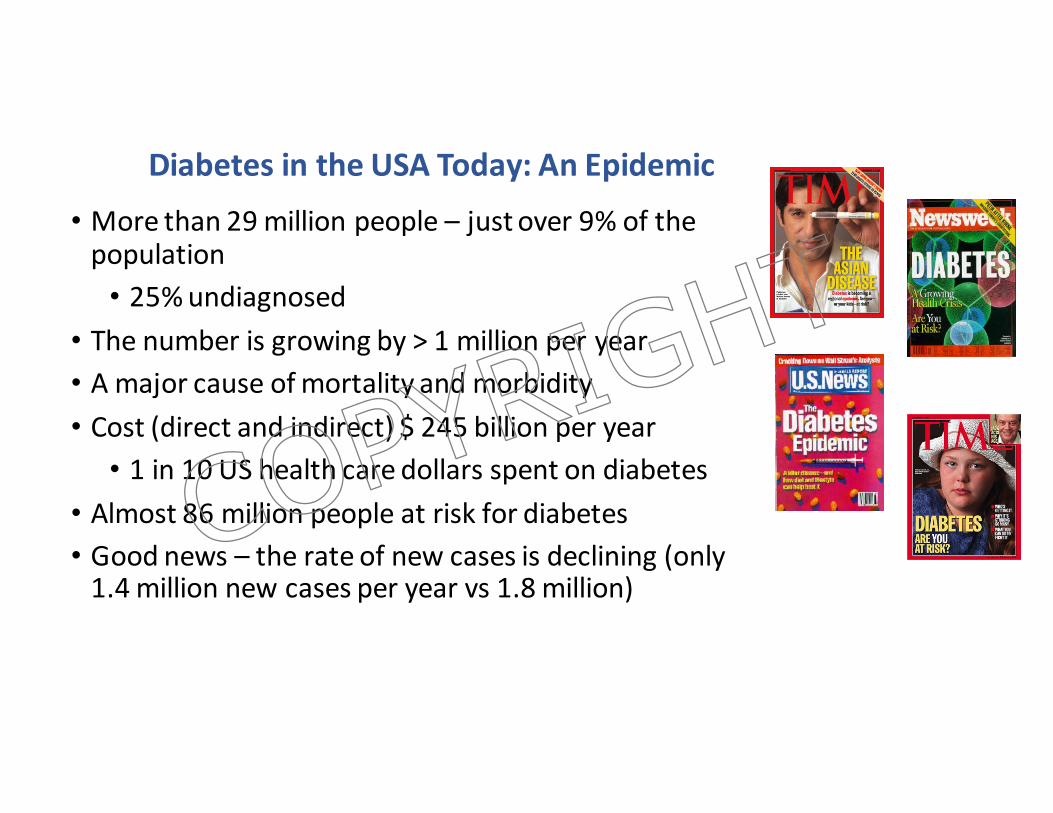
PathogenesisofType2DM:FromtheTriumvirate…
FromDeFronzoDiabetes2009;58:773-795
COPYRIG
HT
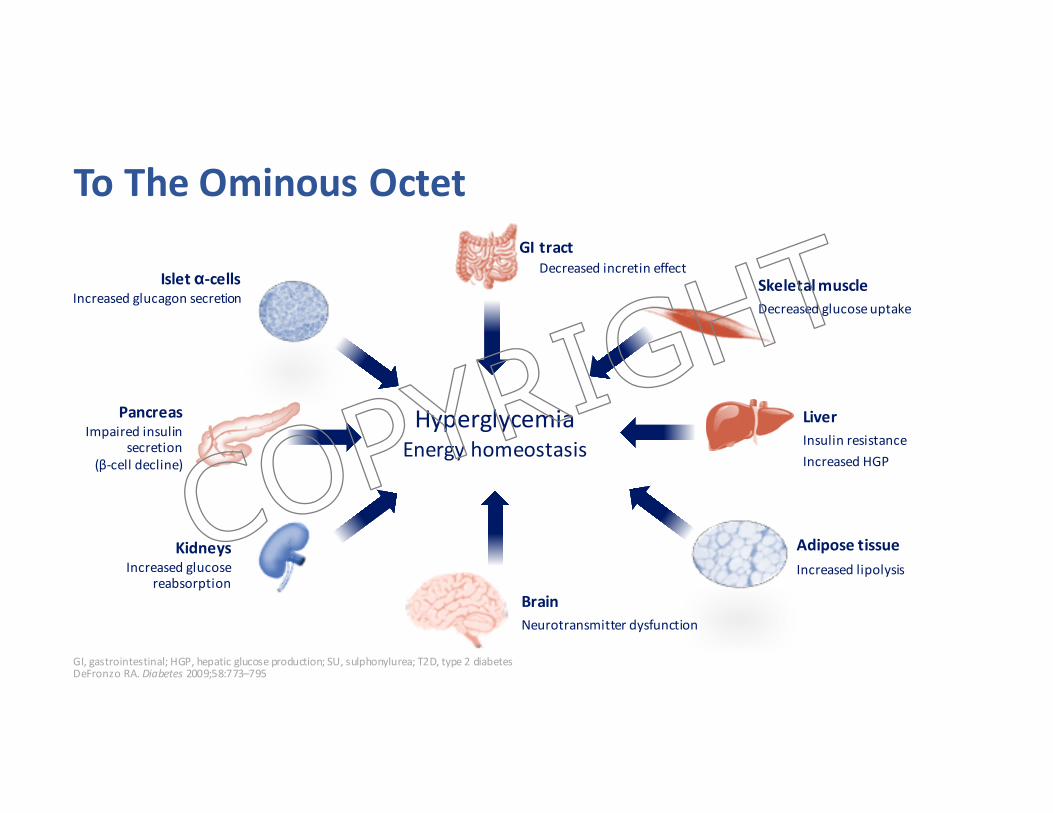
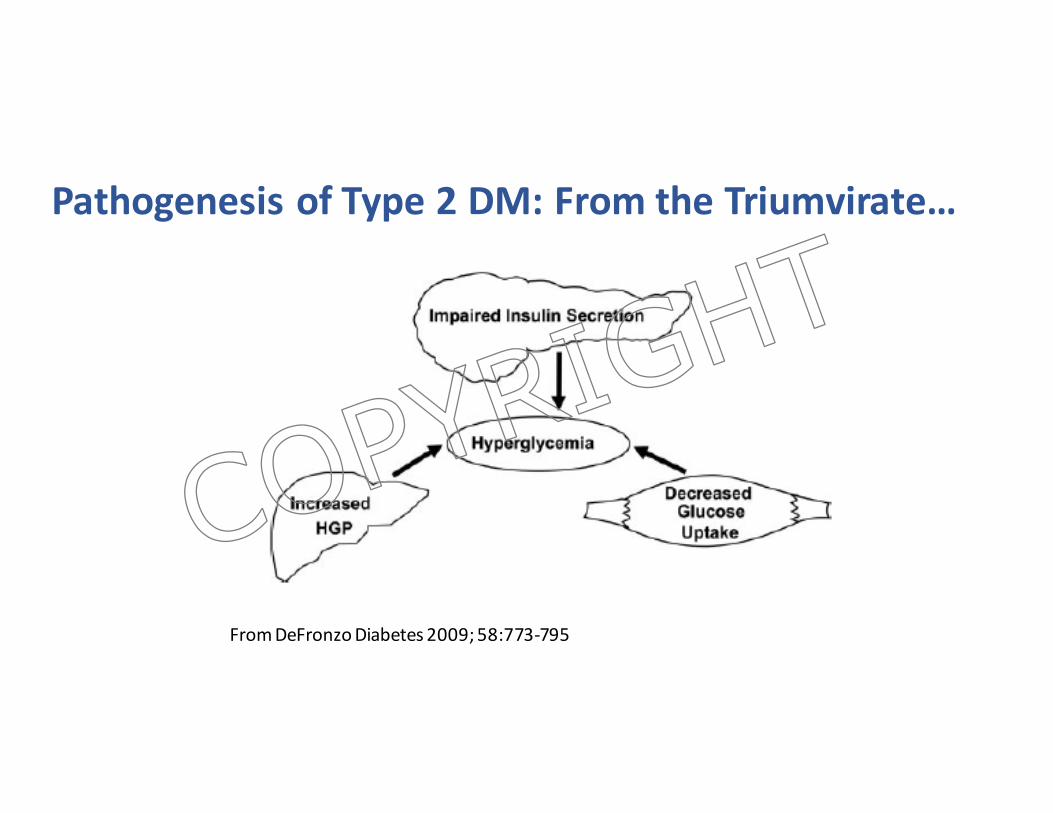
ToTheOminousOctet
GI,gastrointestinal;HGP,hepaticglucoseproduction;SU,sulphonylurea;T2D,type2diabetesDeFronzoRA.Diabetes 2009;58:773–795
AdiposetissueIncreasedlipolysis
SkeletalmuscleDecreasedglucoseuptake
LiverInsulinresistanceIncreasedHGP
BrainNeurotransmitterdysfunction
PancreasImpairedinsulin
secretion(β-celldecline)
GItractDecreasedincretineffect
KidneysIncreasedglucose
reabsorption
Isletα-cellsIncreasedglucagonsecretion
HyperglycemiaEnergyhomeostasis
COPYRIG
HT
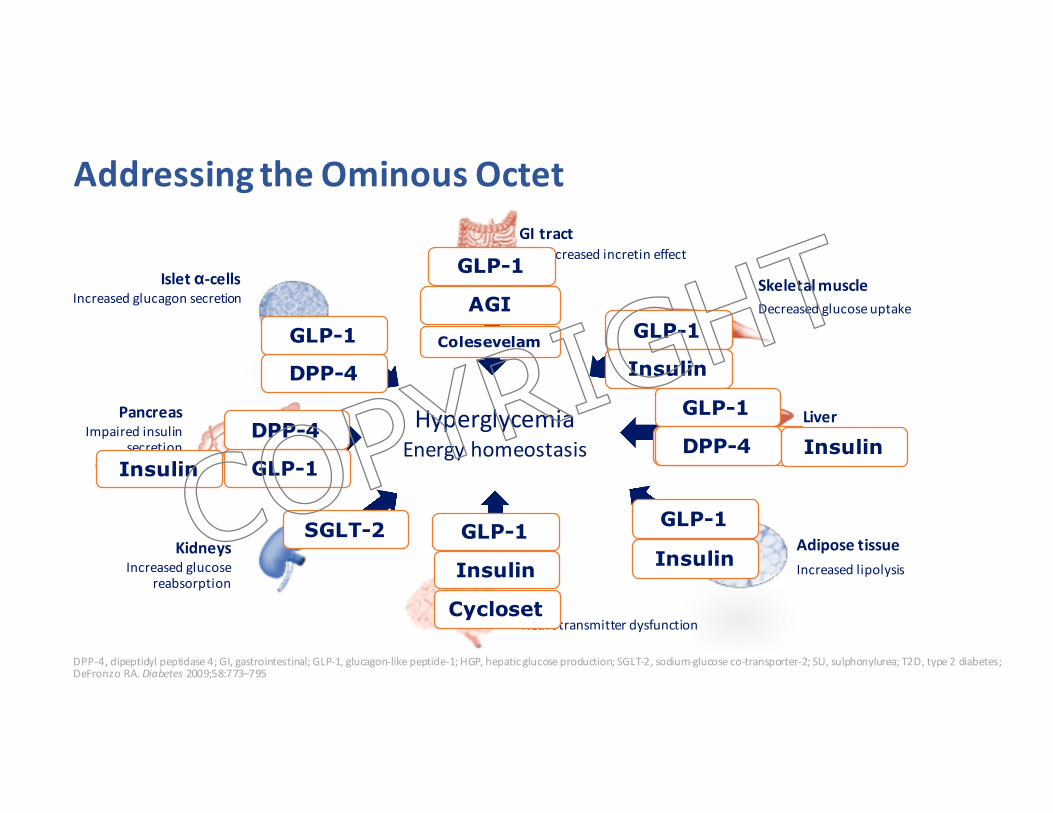
AddressingtheOminousOctet
DPP-4,dipeptidylpeptidase4;GI,gastrointestinal;GLP-1,glucagon-likepeptide-1;HGP,hepaticglucoseproduction;SGLT-2,sodium-glucoseco-transporter-2;SU,sulphonylurea;T2D,type2diabetes;DeFronzoRA.Diabetes 2009;58:773–795
AdiposetissueIncreasedlipolysis
SkeletalmuscleDecreasedglucoseuptake
LiverInsulinresistanceIncreasedHGP
BrainNeurotransmitterdysfunction
PancreasImpairedinsulin
secretion(β-celldecline)
GItractDecreasedincretineffect
KidneysIncreasedglucose
reabsorption
Isletα-cellsIncreasedglucagonsecretion
HyperglycemiaEnergyhomeostasisSUs Metformin
GLP-1
DPP-4
Insulin
DPP-4
GLP-1
GLP-1
GLP-1
Insulin
GLP-1
DPP-4 Insulin
GLP-1
InsulinGLP-1
Insulin
Cycloset
SGLT-2
Colesevelam
AGI
COPYRIG
HT
Type2DiabetesManagement2016• LoweringA1ctoaround7%especiallyearlyafterdiagnosiscanreducetheriskforthedevelopmentorprogressionofthelongtermcomplicationsofdiabetes
• Therearemanymedicationsavailabletodaytotreattype2diabetes– ifusedappropriatelythiscouldtranslatetoimprovedcontrolandlessriskforcomplications
• ThechallengeforthepracticingphysicianistoknowwhichmedicationstouseandwhenbesttousethemCOPYRIG
HT
Type2DiabetesManagement2016• ThereIS consenus thatmetforminshouldbefirstlinetherapy
• ThereisNO clearconsensuswhattoaddtometforminwhenA1cgoalsarenotmet
• Fewheadtoheadcomparatortrials• Evenfewerlongtermstudiesevaluatingdurabilityofmedicationsonglycemiccontrol,especiallywhenaddedtometforminCOP
YRIGHT

more stringent
less stringent
Patient attitude and expected treatment efforts highly motivated, adherent,
excellent self-care capacities less motivated, non-adherent,
poor self-care capacities
Risks potentially associated with hypoglycemia and other drug adverse effects
low high
Disease duration newly diagnosed long-standing
Life expectancy long short
Important comorbidities absent severe few / mild
Established vascular complications absent severe few / mild
Readily available limited
Usually not modifiable
Potentially modifiable
HbA1c'7%('
PATIENT / DISEASE FEATURES
Approach to the management of hyperglycemia
Resources and support system
Figure'1.'Modula$on'of'the'intensiveness'of'glucose'lowering'therapy'in'T2DM'
Diabetes Care 2015;38:140-149; Diabetologia 2015;10.1077/s00125-014-3460-0
COPYRIG
HT
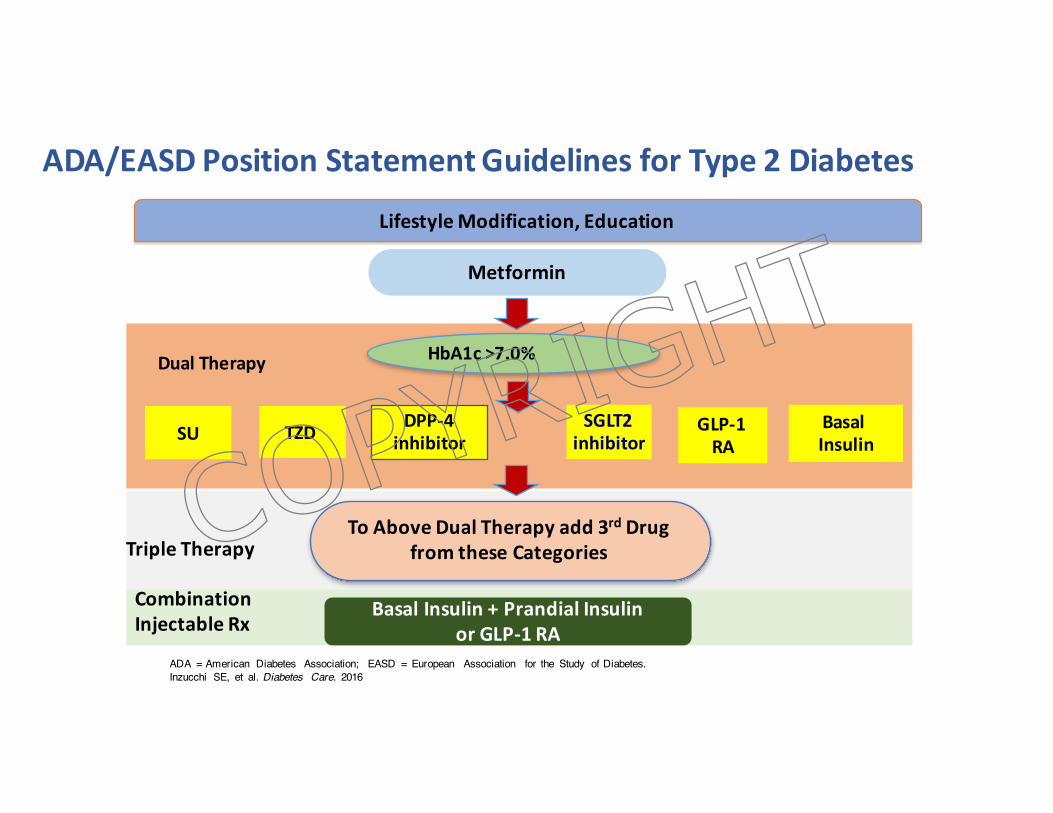
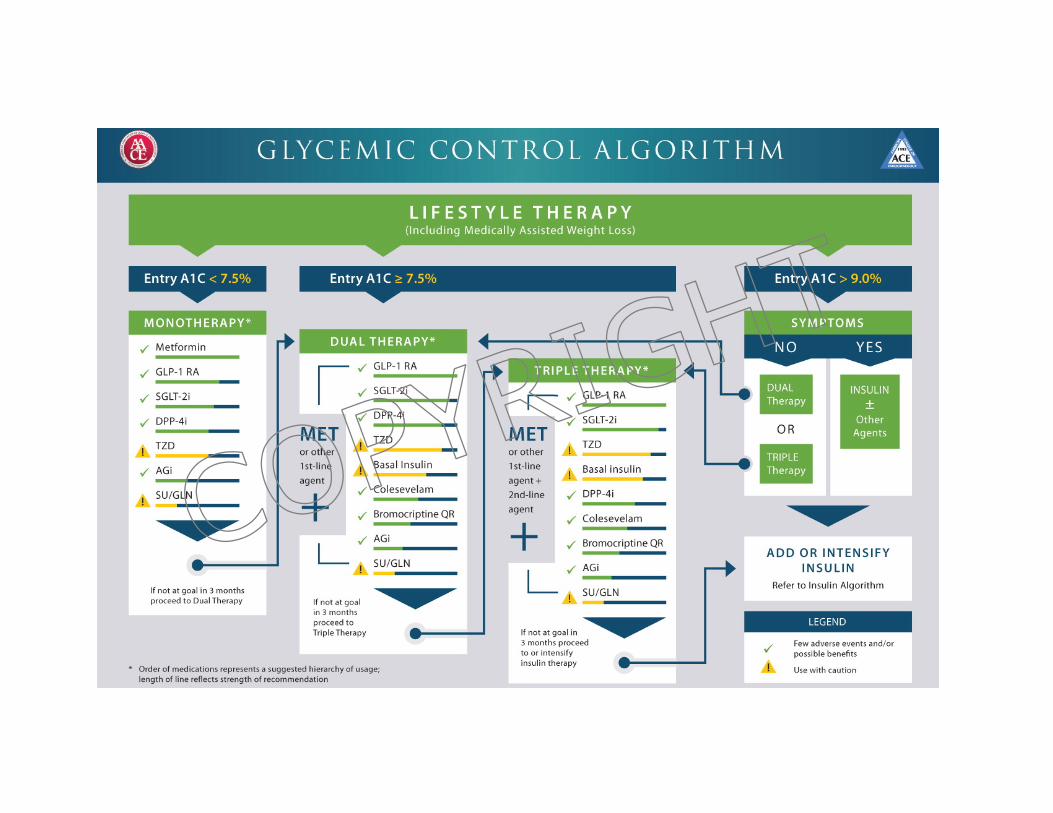
ADA/EASDPositionStatementGuidelinesforType2Diabetes
ADA = American Diabetes Association; EASD = European Association for the Study of Diabetes.Inzucchi SE, et al. Diabetes Care. 2016
ToAboveDualTherapyadd3rd DrugfromtheseCategoriesTripleTherapy
GLP-1RA
BasalInsulin
BasalInsulin+PrandialInsulinorGLP-1RA
CombinationInjectableRx
LifestyleModification,Education
Metformin
DualTherapy
SU
HbA1c>7.0%
DPP-4inhibitorTZD SGLT2
inhibitor
COPYRIG
HT
COPYRIG
HT
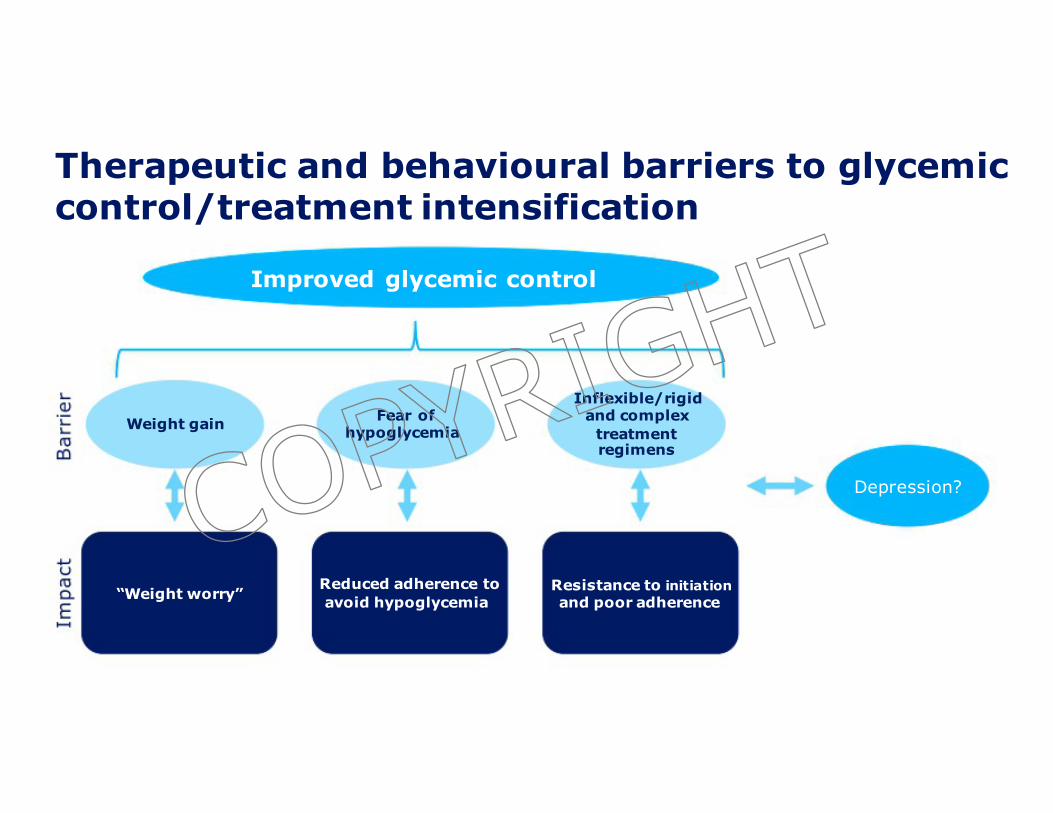
Therapeutic and behavioural barriers to glycemiccontrol/treatment intensification
Improved glycemic control
Inflexible/rigid
Weight gain
“Weight worry”
Fear ofhypoglycemia
Reduced adherence toavoid hypoglycemia
and complextreatmentregimens
Depression?
Resistance to initiationand poor adherence
COPYRIG
HT
Howshouldwechoosewhichdrug/stoaddtometformin?
• Safety• Efficacy• Tolerability/acceptability• Cost
• PhenotypicandgenotypicapproachestodeterminemosteffectivetherapyarelackingCOP
YRIGHT
Safety
• Hypoglycemia
• Cardiacsafety
COPYRIG
HT
Hypoglycemia
• Insulin
• Sulfonylureas(SUs)• NOT (whenusedalone/without insulinorSUs)
• Metformin• DPP-IVInhibitors• GLP-1agonists• TZD• SGLT-2inhbitors• Dopaminereceptoragonist• Colesevalam• Alphaglucosidase inhibitorsCOPYRIG
HT
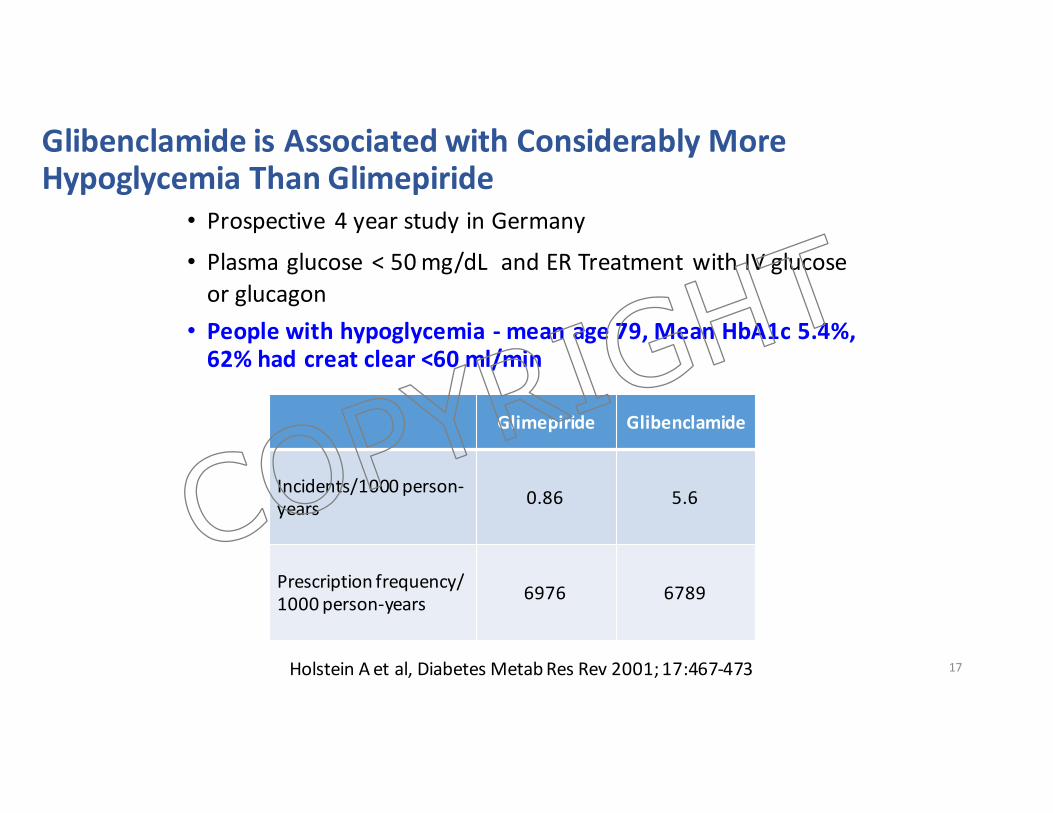
Glibenclamide isAssociatedwithConsiderablyMoreHypoglycemiaThanGlimepiride
• Prospective 4yearstudyinGermany
• Plasmaglucose <50mg/dL andERTreatmentwithIVglucoseorglucagon
• Peoplewithhypoglycemia- meanage79,MeanHbA1c5.4%,62%hadcreat clear<60ml/min
17
Glimepiride Glibenclamide
Incidents/1000person-years 0.86 5.6
Prescriptionfrequency/1000person-years 6976 6789
HolsteinAetal,DiabetesMetabResRev2001;17:467-473
COPYRIG
HT

CardiovascularsafetyCOPYRIG
HT
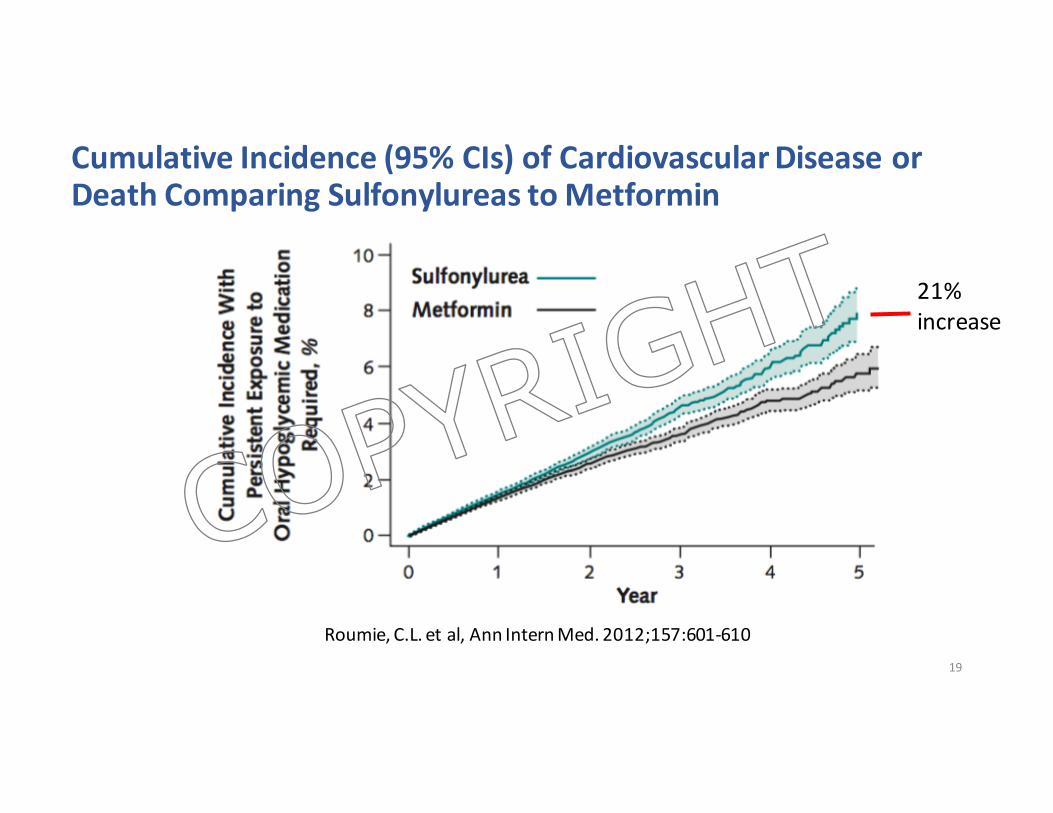
CumulativeIncidence(95%CIs)ofCardiovascularDiseaseorDeathComparingSulfonylureastoMetformin
19
Roumie,C.L.etal,AnnInternMed.2012;157:601-610
21%increase
COPYRIG
HT
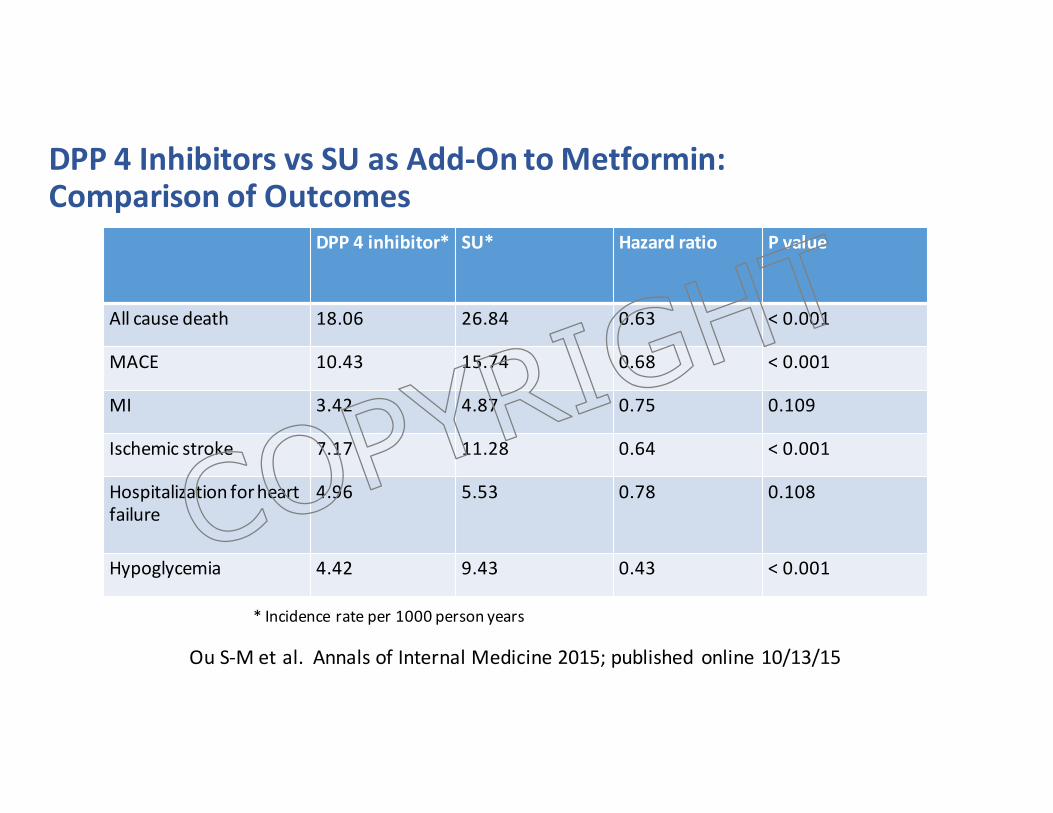
DPP4InhibitorsvsSUasAdd-OntoMetformin:ComparisonofOutcomes
DPP4inhibitor* SU* Hazard ratio Pvalue
Allcausedeath 18.06 26.84 0.63 < 0.001
MACE 10.43 15.74 0.68 <0.001
MI 3.42 4.87 0.75 0.109
Ischemic stroke 7.17 11.28 0.64 <0.001
Hospitalizationforheartfailure
4.96 5.53 0.78 0.108
Hypoglycemia 4.42 9.43 0.43 <0.001
*Incidencerateper1000personyears
Ou S-Metal.AnnalsofInternalMedicine2015;published online10/13/15
COPYRIG
HT
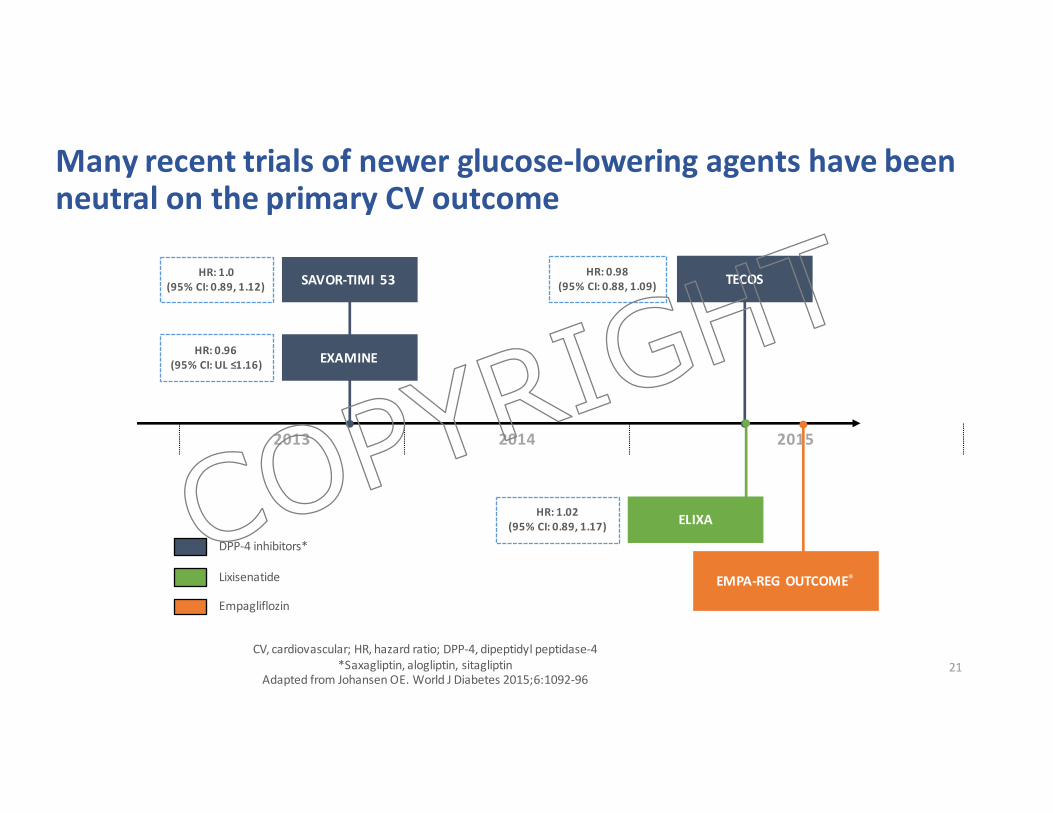
Manyrecenttrialsofnewerglucose-loweringagentshavebeenneutralontheprimaryCVoutcome
21
SAVOR-TIMI 53
EXAMINE
HR:1.0(95%CI:0.89,1.12)
HR:0.96(95%CI:UL≤1.16)
TECOSHR:0.98(95%CI:0.88,1.09)
EMPA-REGOUTCOME®
ELIXAHR:1.02(95%CI:0.89,1.17)
Empagliflozin
DPP-4inhibitors*
Lixisenatide
CV,cardiovascular;HR,hazardratio; DPP-4,dipeptidylpeptidase-4*Saxagliptin,alogliptin,sitagliptin
AdaptedfromJohansenOE.WorldJDiabetes2015;6:1092-96
2013 2014 2015
COPYRIG
HT
NEngl JMed2015;373:2117-2128
COPYRIG
HT
EMPA-REGOUTCOME®• Randomised, double-blind, placebo-controlled CVoutcomestrial
• ObjectiveToexamine the long-termeffectsofempagliflozin versusplacebo,inaddition tostandardofcare,onCVmorbidityandmortality inpatientswithtype2diabetes andhighriskofCVevents
CV,cardiovascular
COPYRIG
HT
Pre-specifiedprimaryandkeysecondaryoutcomes
• Primaryoutcome• 3-pointMACE:Time tofirstoccurrenceofCVdeath,non-fatalMIornon-fatalstroke
• Keysecondaryoutcome• 4-pointMACE:Time tofirstoccurrenceofCVdeath,non-fatalMI,non-fatalstrokeorhospitalisation forunstableangina
24CV,cardiovascular;MI,myocardialinfarction;MACE,MajorAdverseCardiovascularEvent
COPYRIG
HT
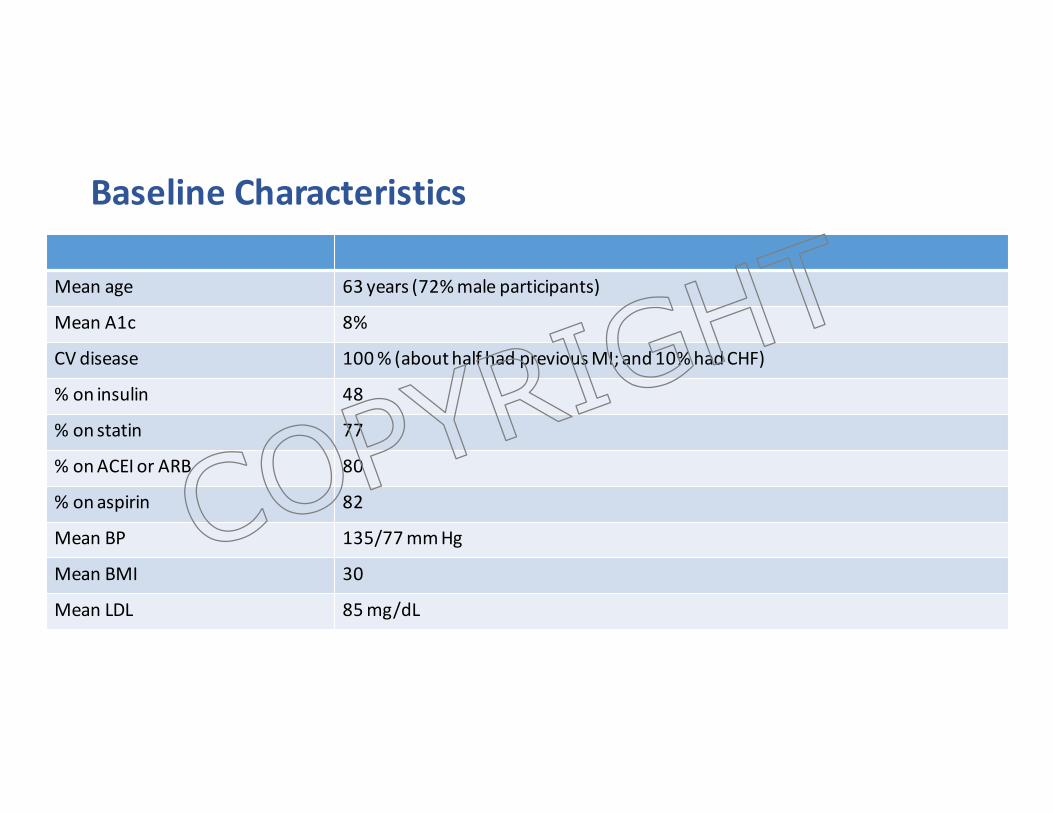
BaselineCharacteristics
Meanage 63years(72%maleparticipants)
MeanA1c 8%
CVdisease 100%(abouthalf hadpreviousMI;and10%hadCHF)
%oninsulin 48
%onstatin 77
%onACEIorARB 80
%onaspirin 82
Mean BP 135/77mmHg
MeanBMI 30
Mean LDL 85mg/dL
COPYRIG
HT
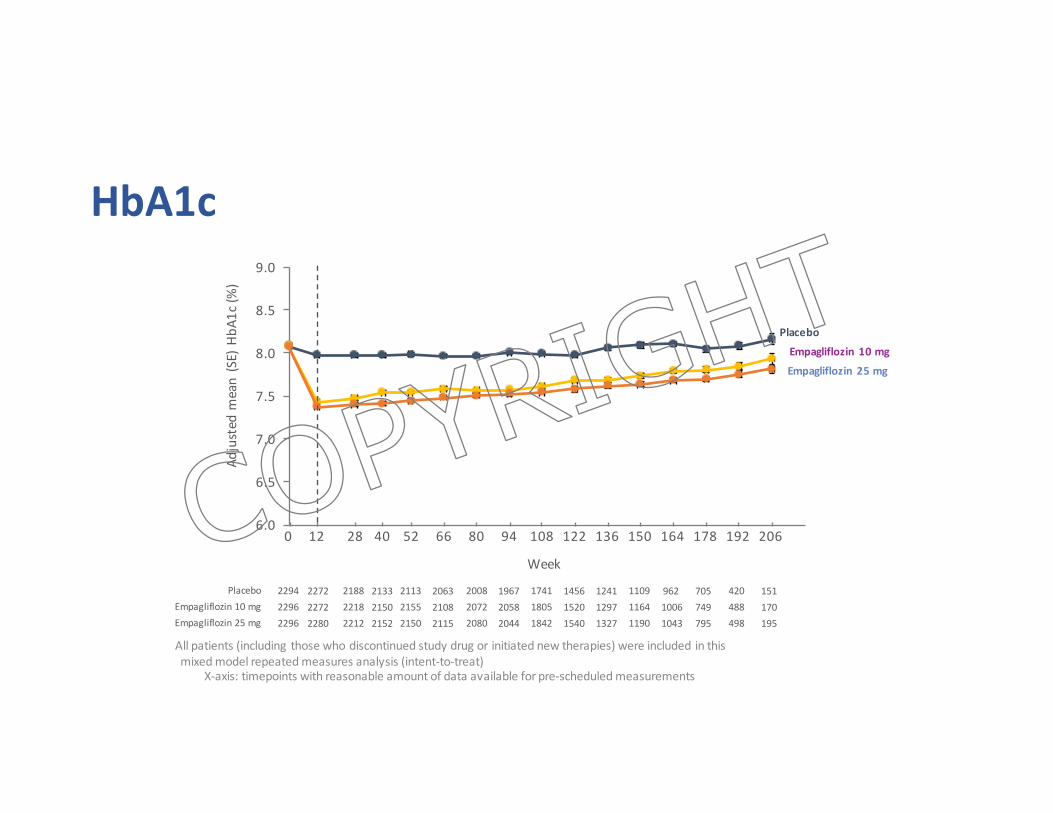
HbA1c
6.0
6.5
7.0
7.5
8.0
8.5
9.0
Adjustedm
ean(SE)HbA
1c(%
)
Week
Placebo
Empagliflozin10mg
Empagliflozin25mg
229422962296
PlaceboEmpagliflozin10mgEmpagliflozin25mg
227222722280
218822182212
213321502152
211321552150
206321082115
200820722080
196720582044
174118051842
145615201540
124112971327
110911641190
96210061043
705749795
420488498
151170195
12 28 52 94 10880 12266 1360 150 164 178 192 20640
Allpatients(includingthosewhodiscontinuedstudydrugorinitiatednewtherapies)wereincludedinthismixedmodelrepeatedmeasuresanalysis(intent-to-treat)
X-axis:timepointswithreasonableamountofdataavailableforpre-scheduledmeasurements
COPYRIG
HT
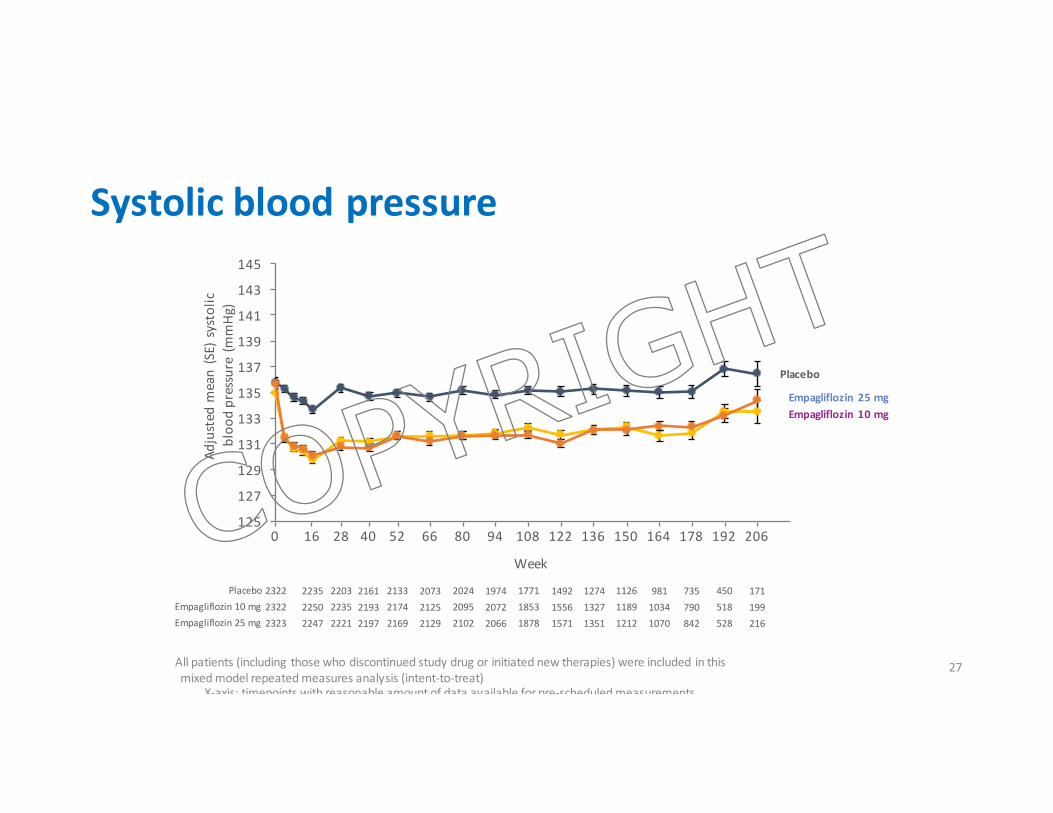
Systolicbloodpressure
27
125
127
129
131
133
135
137
139
141
143
145
Adjustedm
ean(SE)systolic
bloo
dpressure(m
mHg
)
Week
232223222323
PlaceboEmpagliflozin10mgEmpagliflozin25mg
223522502247
220322352221
216121932197
213321742169
207321252129
202420952102
197420722066
177118531878
149215561571
127413271351
112611891212
98110341070
735790842
450518528
171199216
Placebo
Empagliflozin10mgEmpagliflozin25mg
16 28 52 94 10880 12266 1360 150 164 178 192 20640
Allpatients(includingthosewhodiscontinuedstudydrugorinitiatednewtherapies)wereincludedinthismixedmodelrepeatedmeasuresanalysis(intent-to-treat)
X-axis:timepointswithreasonableamountofdataavailableforpre-scheduledmeasurements
COPYRIG
HT
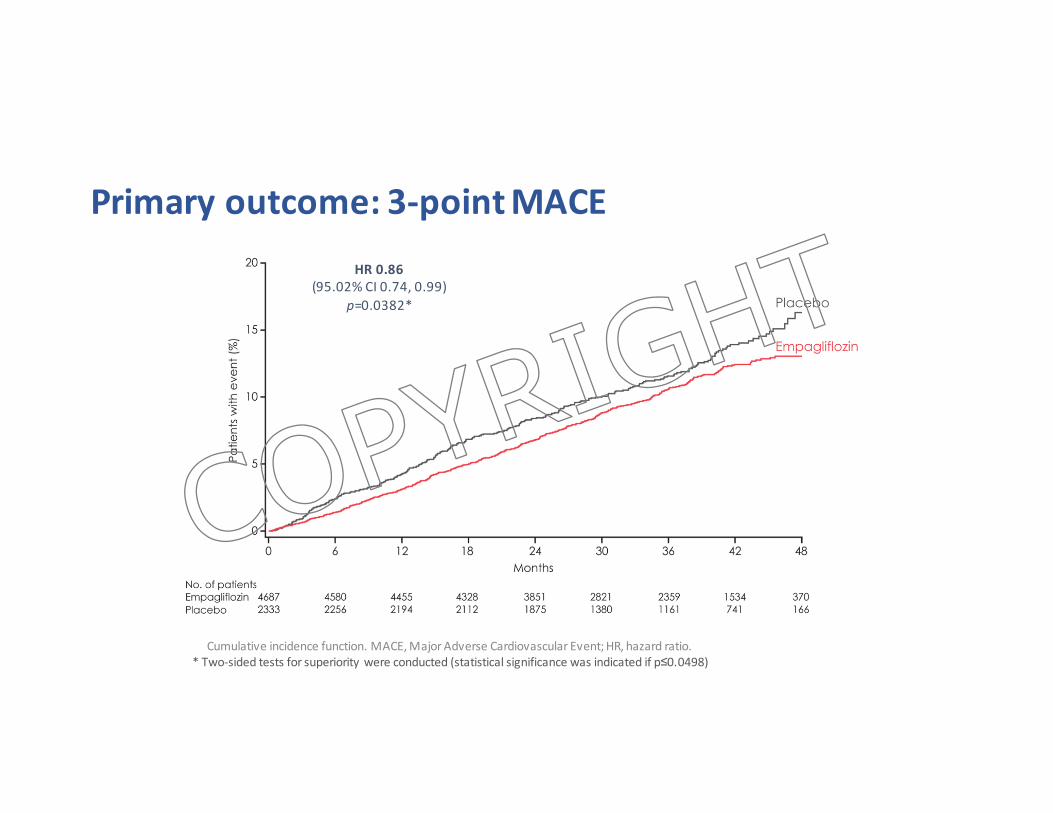
Primaryoutcome:3-pointMACEHR0.86
(95.02%CI0.74,0.99)p=0.0382*
Cumulativeincidencefunction.MACE,MajorAdverseCardiovascularEvent;HR,hazardratio.*Two-sidedtestsforsuperioritywereconducted(statisticalsignificancewasindicatedifp≤0.0498)
COPYRIG
HT
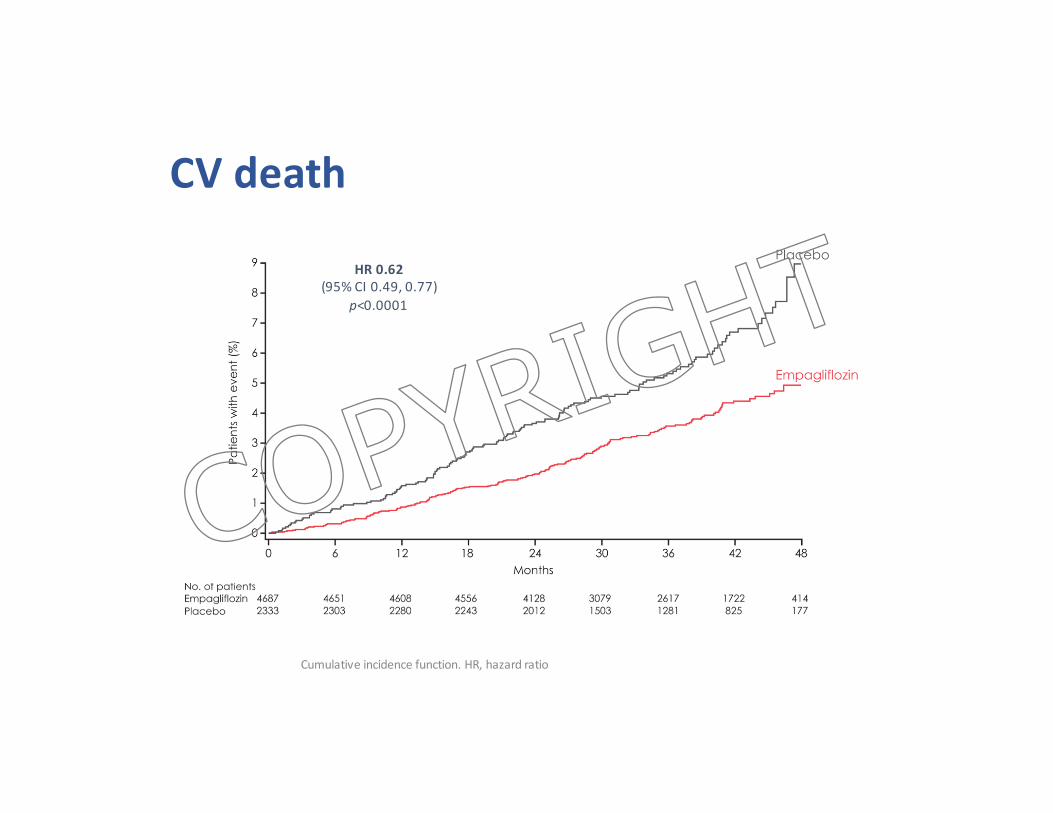
CVdeath
HR0.62(95%CI0.49,0.77)
p<0.0001
Cumulativeincidencefunction.HR,hazardratio
COPYRIG
HT
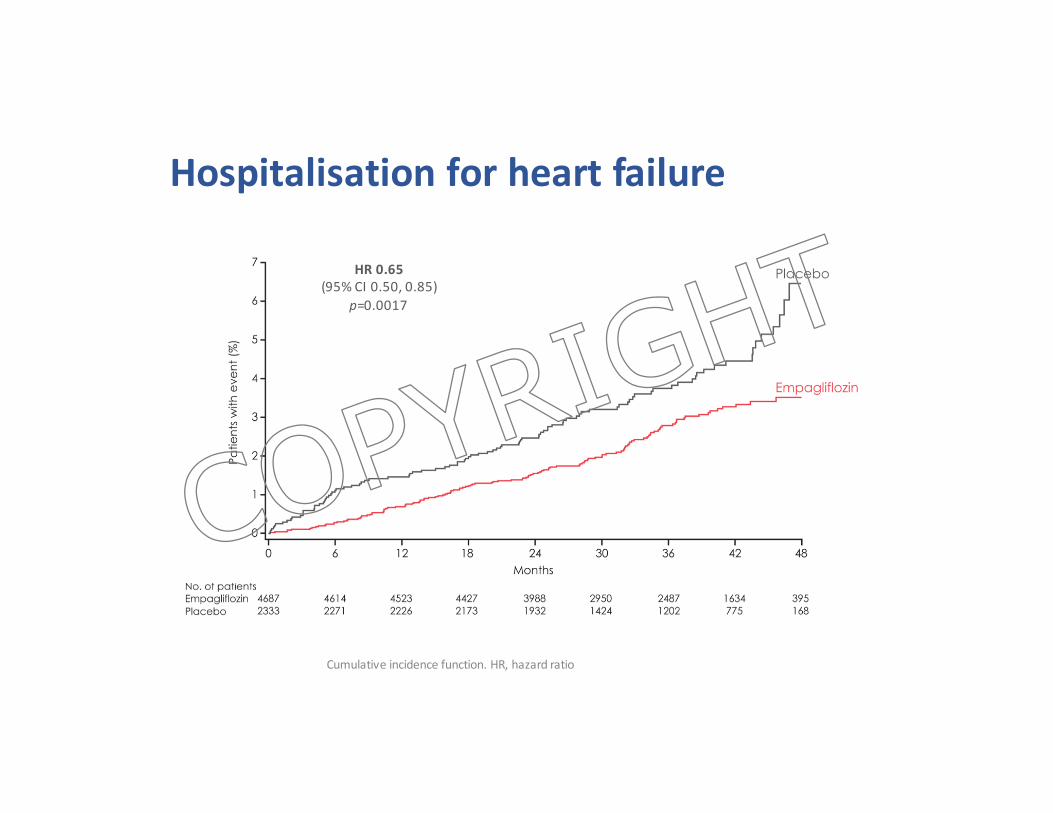
Hospitalisationforheartfailure
HR0.65(95%CI0.50,0.85)
p=0.0017
Cumulativeincidencefunction.HR,hazardratio
COPYRIG
HT
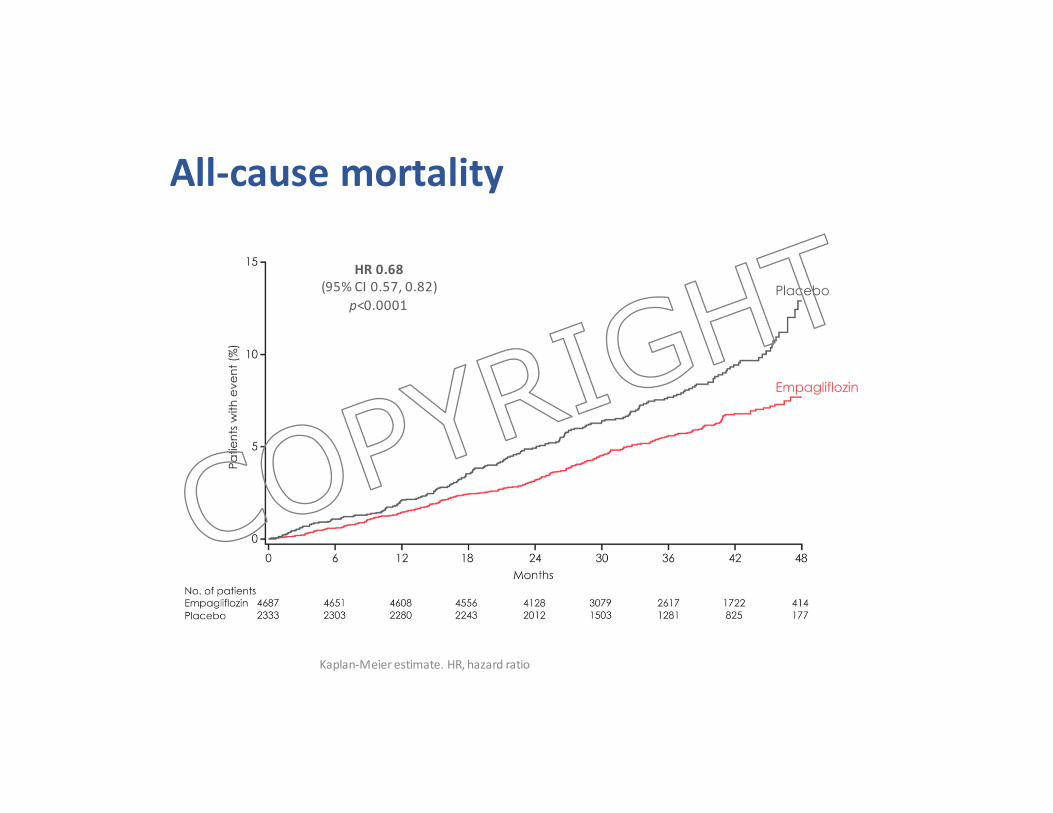
All-causemortality
HR0.68(95%CI0.57,0.82)
p<0.0001
Kaplan-Meierestimate.HR,hazardratio
COPYRIG
HT
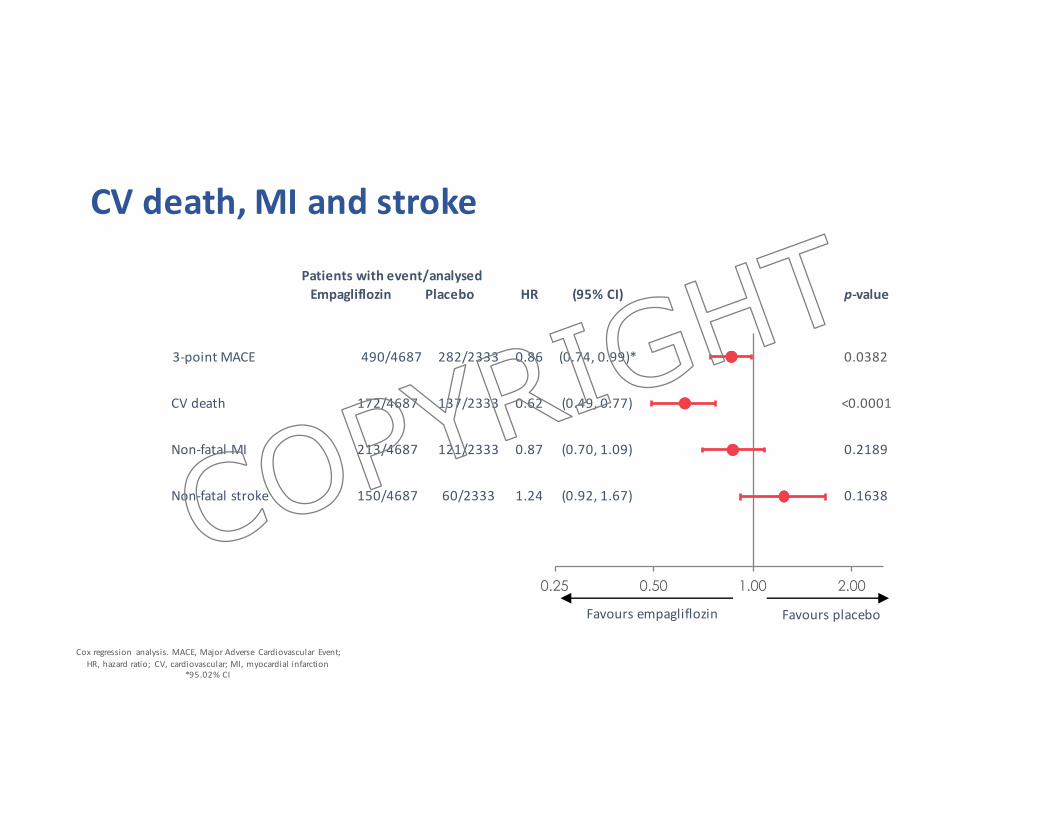
Patients with event/analysedEmpagliflozin Placebo HR (95%CI) p-value
3-pointMACE 490/4687 282/2333 0.86 (0.74,0.99)* 0.0382
CVdeath 172/4687 137/2333 0.62 (0.49,0.77) <0.0001
Non-fatalMI 213/4687 121/2333 0.87 (0.70,1.09) 0.2189
Non-fatalstroke 150/4687 60/2333 1.24 (0.92,1.67) 0.1638
0.25 0.50 1.00 2.00
CVdeath,MIandstroke
Favoursempagliflozin Favoursplacebo
Coxregression analysis.MACE,MajorAdverse Cardiovascular Event;HR,hazardratio; CV,cardiovascular;MI,myocardialinfarction
*95.02%CI
COPYRIG
HT
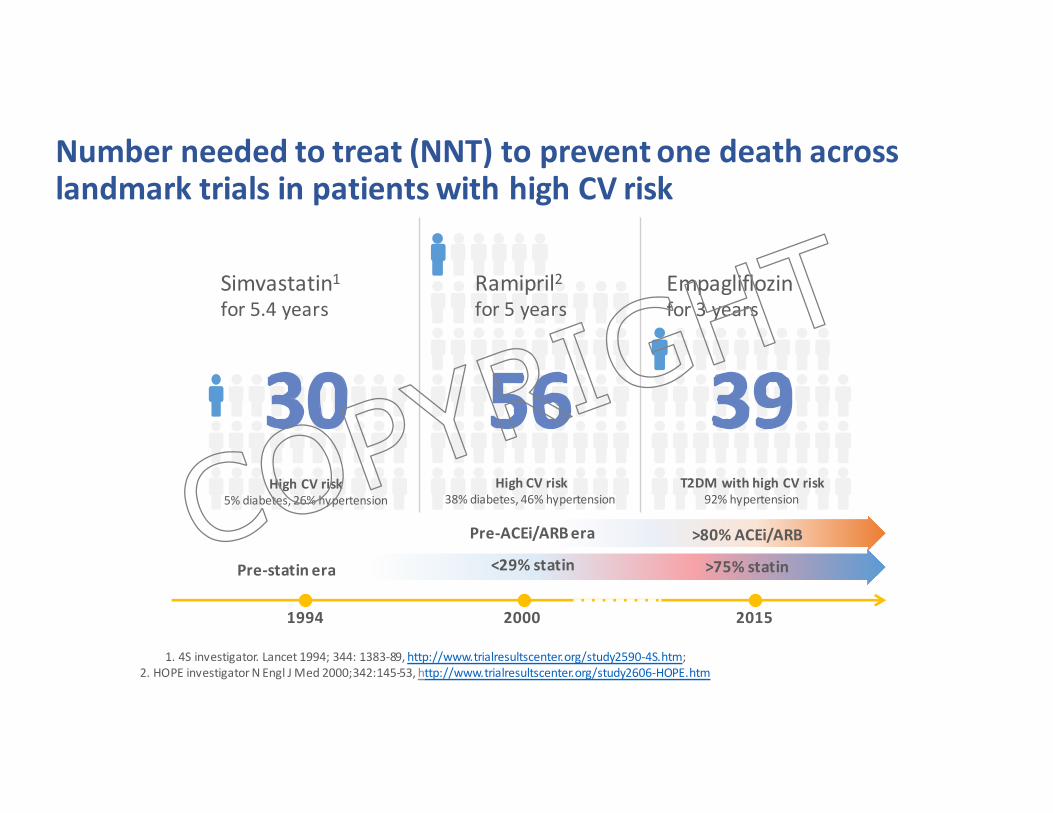
Numberneededtotreat(NNT)topreventonedeathacrosslandmarktrialsinpatientswithhighCVrisk
1.4Sinvestigator.Lancet1994;344:1383-89,http://www.trialresultscenter.org/study2590-4S.htm;2.HOPEinvestigatorNEnglJMed2000;342:145-53,http://www.trialresultscenter.org/study2606-HOPE.htm
Simvastatin1for5.4years
HighCVrisk5%diabetes,26%hypertension
1994 2000 2015
Pre-statinera
HighCVrisk38%diabetes,46%hypertension
Ramipril2for5years
Pre-ACEi/ARBera
<29%statin
Empagliflozinfor3years
T2DMwithhighCVrisk92%hypertension
>80%ACEi/ARB
>75%statinCOPYRIG
HT
COPYRIG
HT
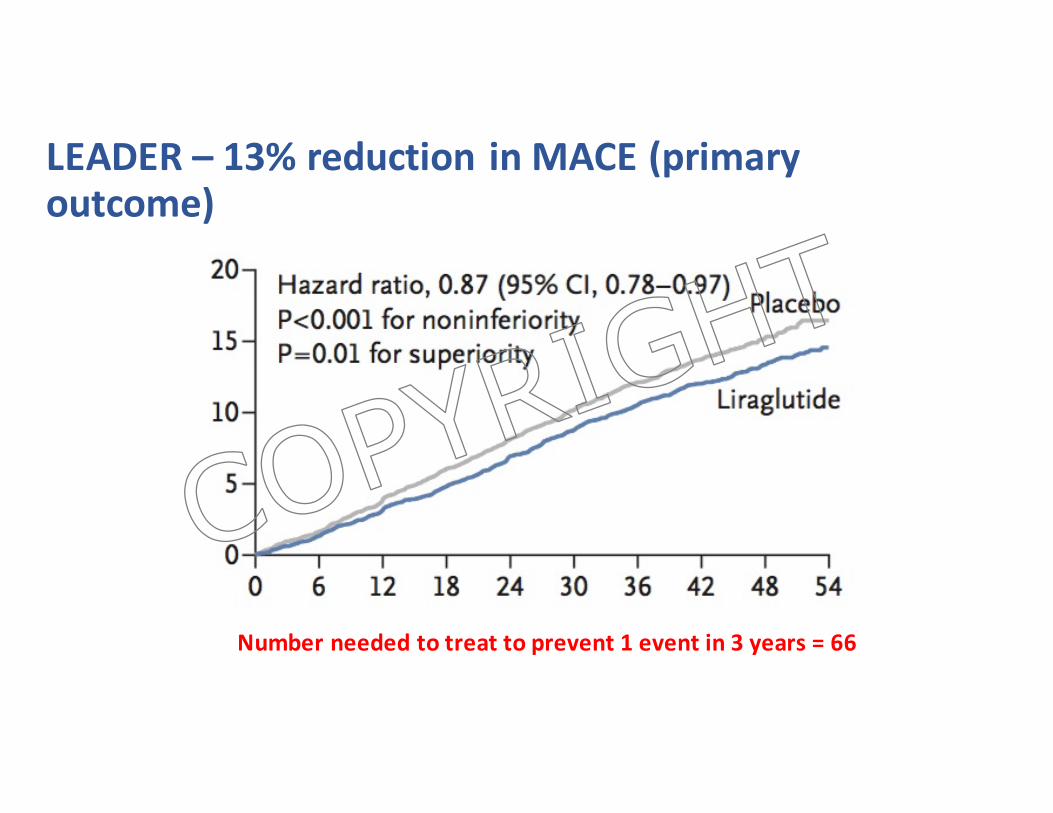
LEADER– 13%reductioninMACE(primaryoutcome)
Numberneededtotreattoprevent1eventin3years=66
COPYRIG
HT
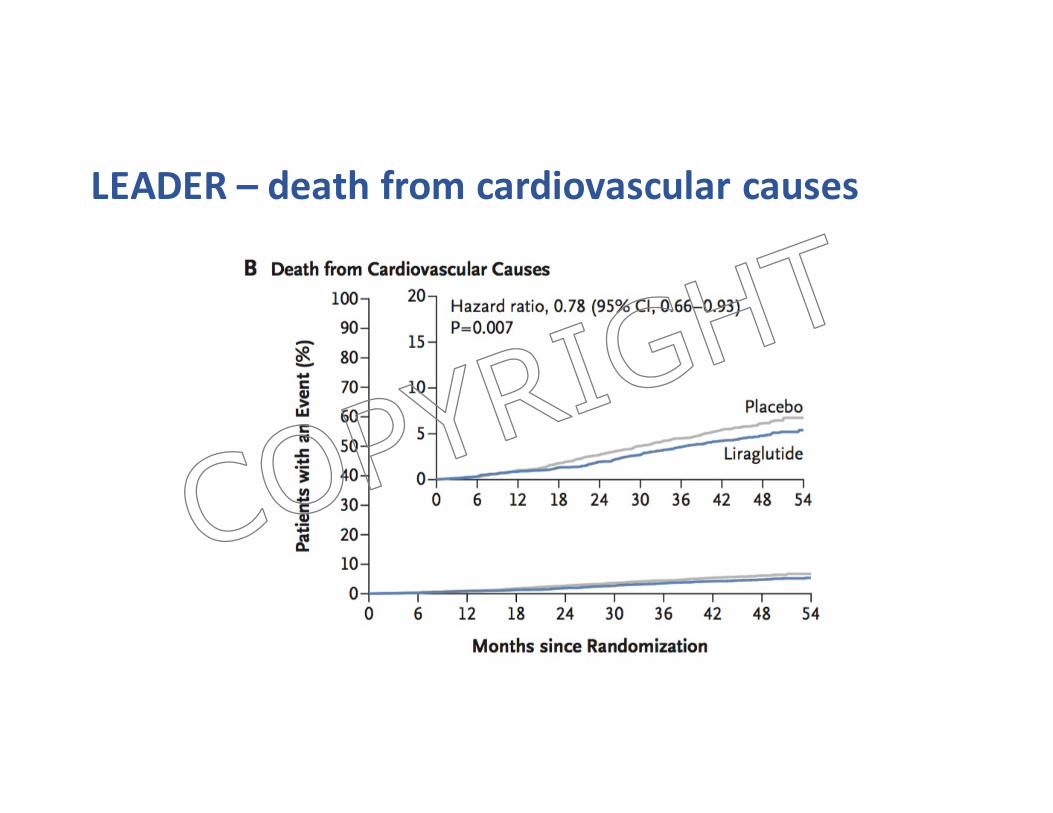
LEADER– deathfromcardiovascularcauses
COPYRIG
HT
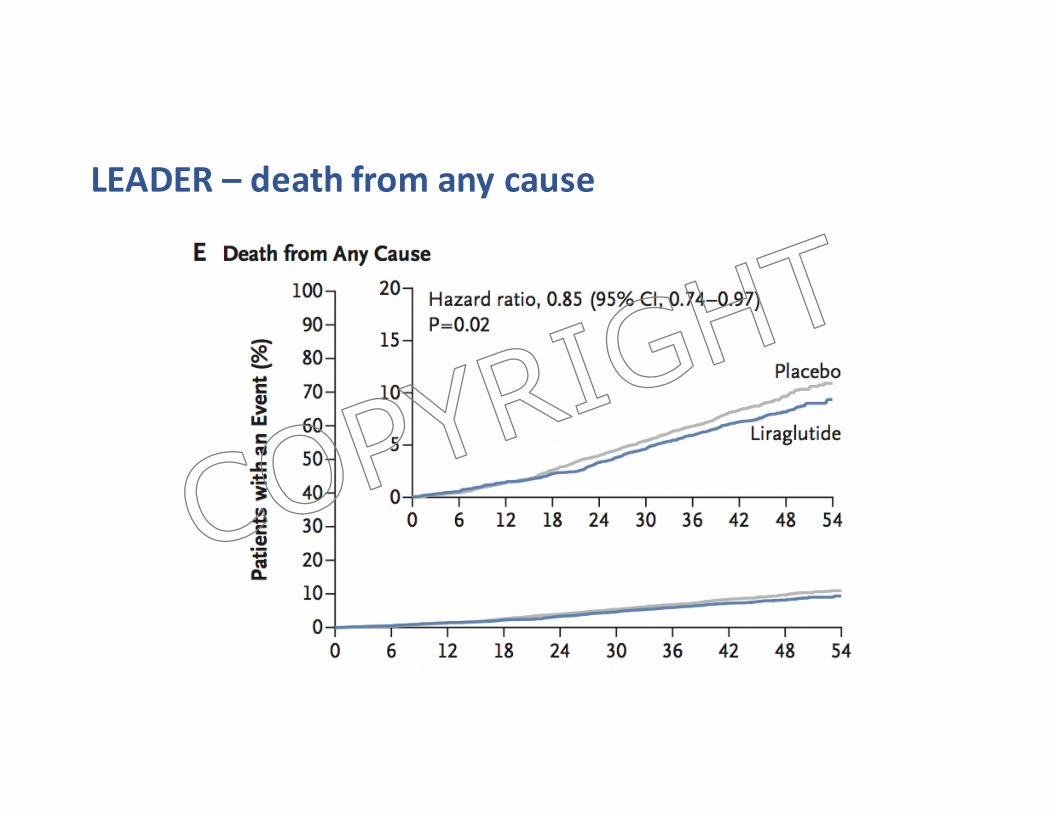
LEADER– deathfromanycause
COPYRIG
HT
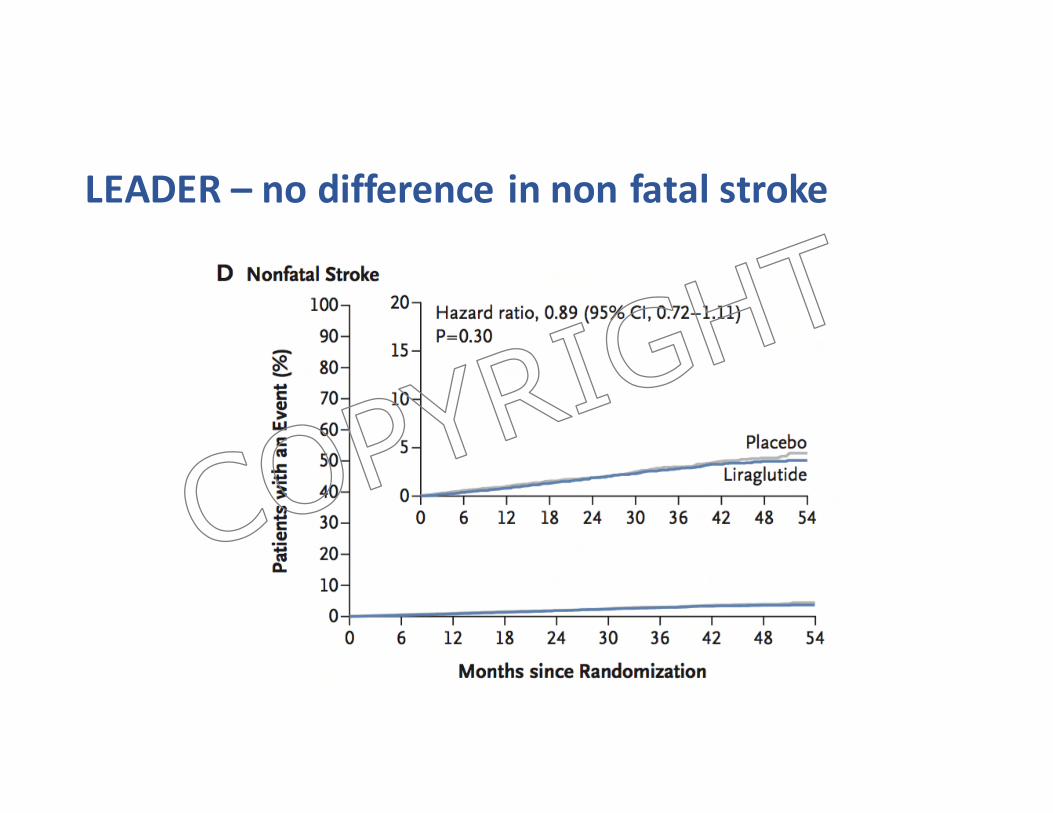
LEADER– nodifferenceinnonfatalstroke
COPYRIG
HT
NEngl JMed2016;375:323-334
COPYRIG
HT
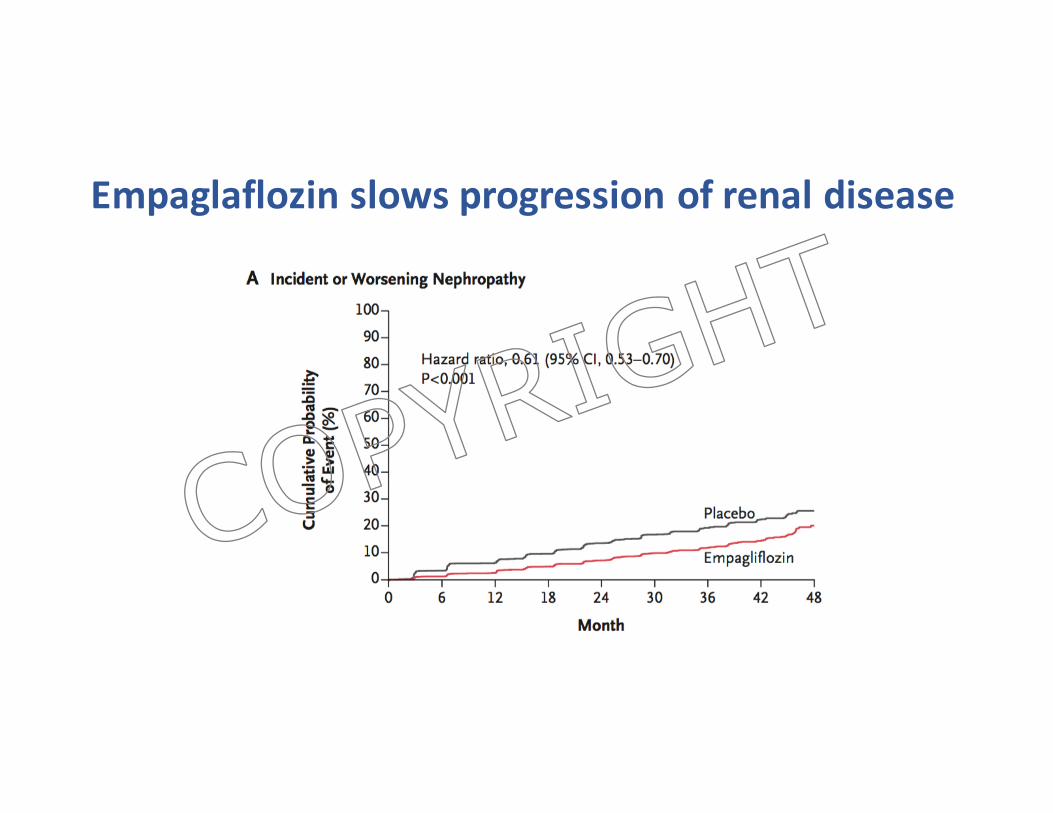
Empaglaflozin slowsprogressionofrenaldisease
COPYRIG
HT
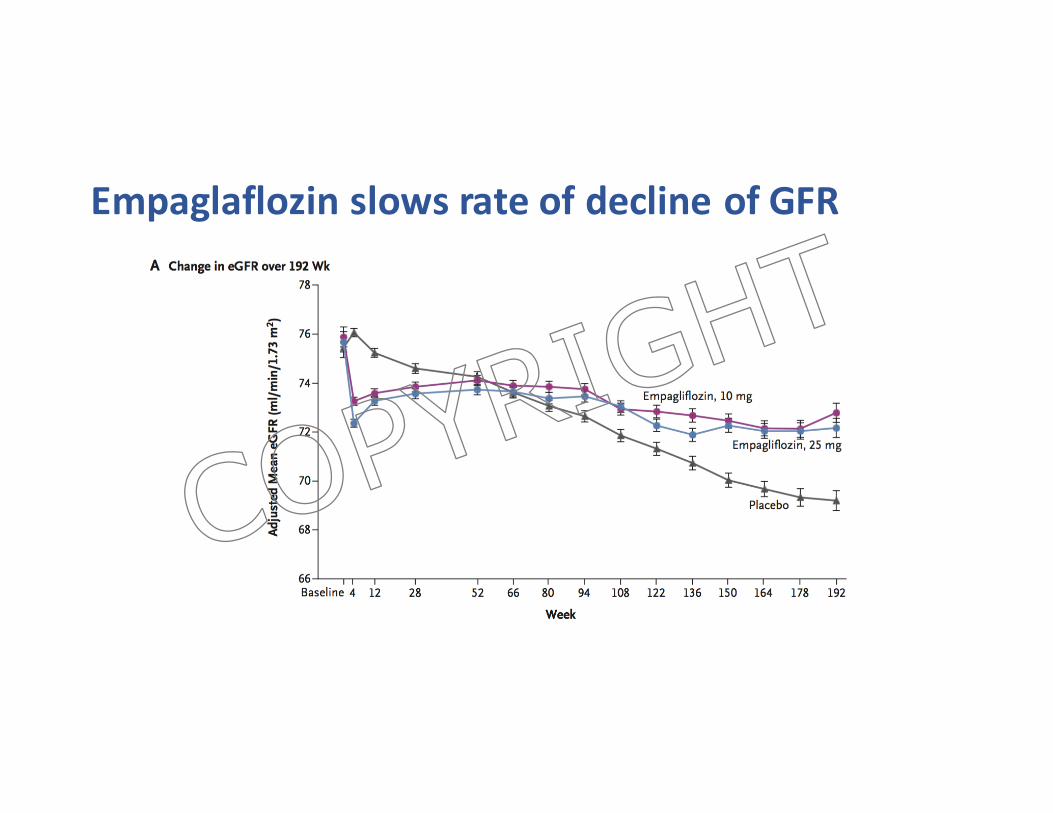
Empaglaflozin slowsrateofdeclineofGFR
COPYRIG
HT
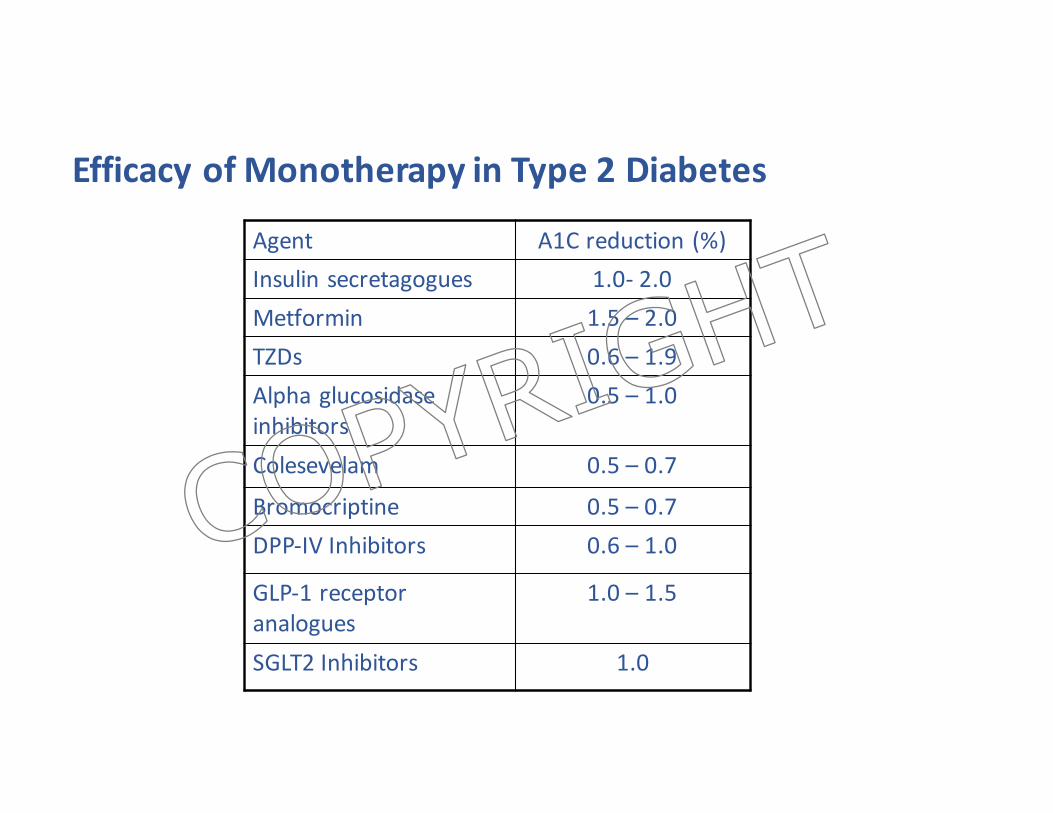
EfficacyofMonotherapy inType2Diabetes
Agent A1Creduction(%)Insulinsecretagogues 1.0- 2.0Metformin 1.5– 2.0TZDs 0.6– 1.9Alphaglucosidaseinhibitors
0.5– 1.0
Colesevelam 0.5– 0.7
Bromocriptine 0.5– 0.7DPP-IVInhibitors 0.6– 1.0
GLP-1receptoranalogues
1.0– 1.5
SGLT2Inhibitors 1.0
COPYRIG
HT
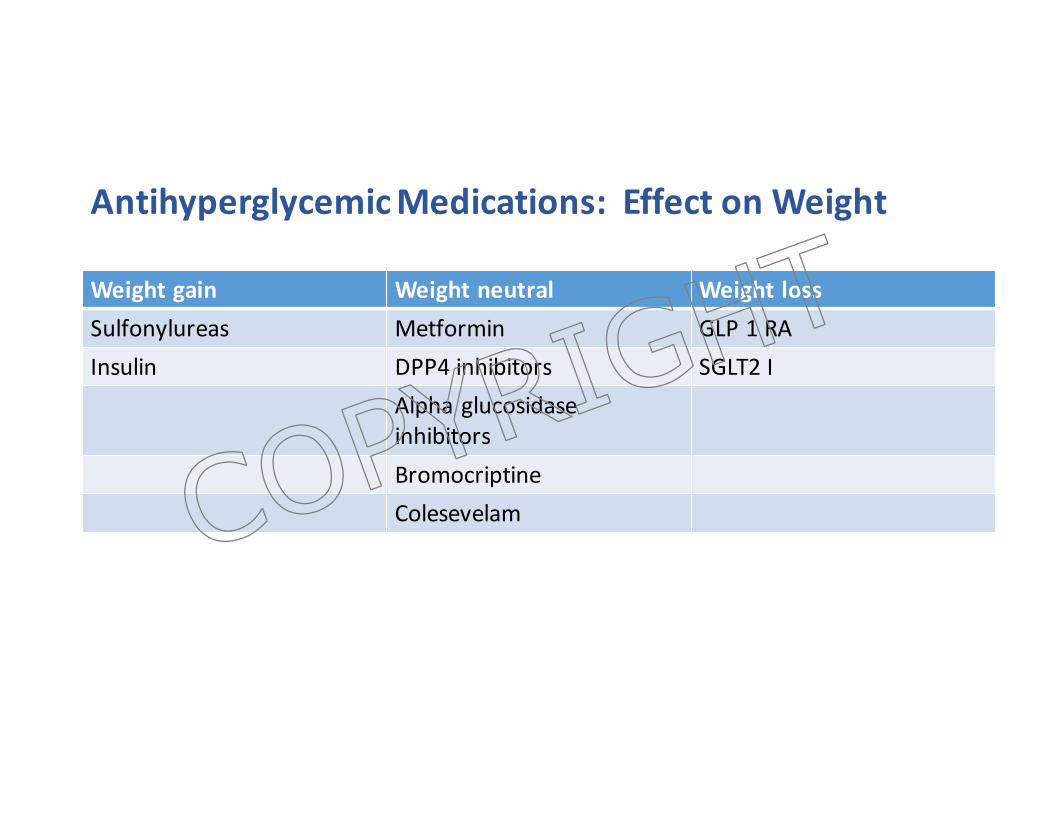
AntihyperglycemicMedications:EffectonWeight
Weightgain Weightneutral WeightlossSulfonylureas Metformin GLP1RAInsulin DPP4inhibitors SGLT2I
AlphaglucosidaseinhibitorsBromocriptineColesevelamCOPYRIG
HT

SOLET’SLOOKATSOMETREATMENTOPTIONSTRYINGTOMINIMIZEWEIGHTGAINANDHYPOGLYCEMIA
COPYRIG
HT
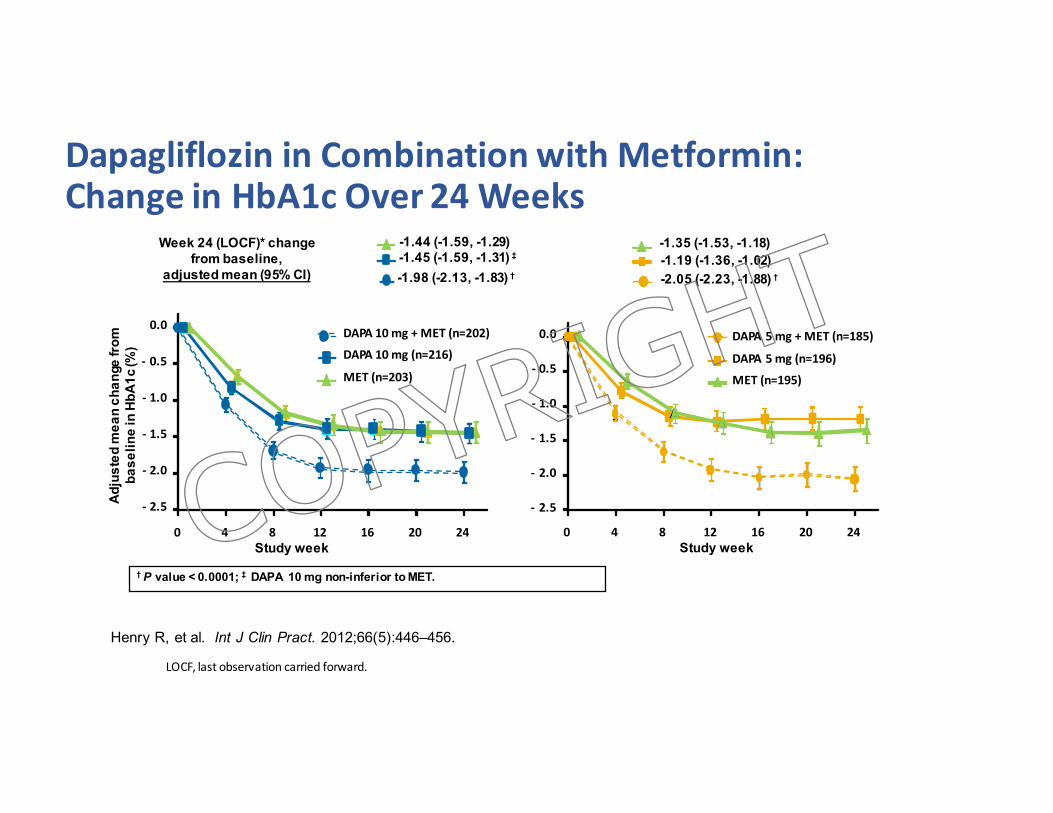
Week 24 (LOCF)* change from baseline,
adjusted mean (95% CI)
†P value < 0.0001; ‡ DAPA 10 mg non-inferior to MET.
- 2.5
- 2.0
- 1.5
- 1.0
- 0.5
0.0
0 4 8 12 16 20 24
DAPA5mg+MET(n=185)
DAPA5mg(n=196)
MET(n=195)
Study week
Adju
sted
mea
n ch
ange
from
ba
selin
e in
HbA
1c (%
)
- 2.5
- 2.0
- 1.5
- 1.0
- 0.5
0.0
0 4 8 12 16 20 24
DAPA10mg+MET(n=202)
DAPA10mg(n=216)
MET(n=203)
Study week
-1.19 (-1.36, -1.02)-1.35 (-1.53, -1.18)
-2.05 (-2.23, -1.88) † -1.98 (-2.13, -1.83) †
-1.44 (-1.59, -1.29)-1.45 (-1.59, -1.31) ‡
DapagliflozininCombinationwithMetformin:ChangeinHbA1cOver24Weeks
Henry R, et al. Int J Clin Pract. 2012;66(5):446–456.
LOCF,lastobservationcarriedforward.
COPYRIG
HT
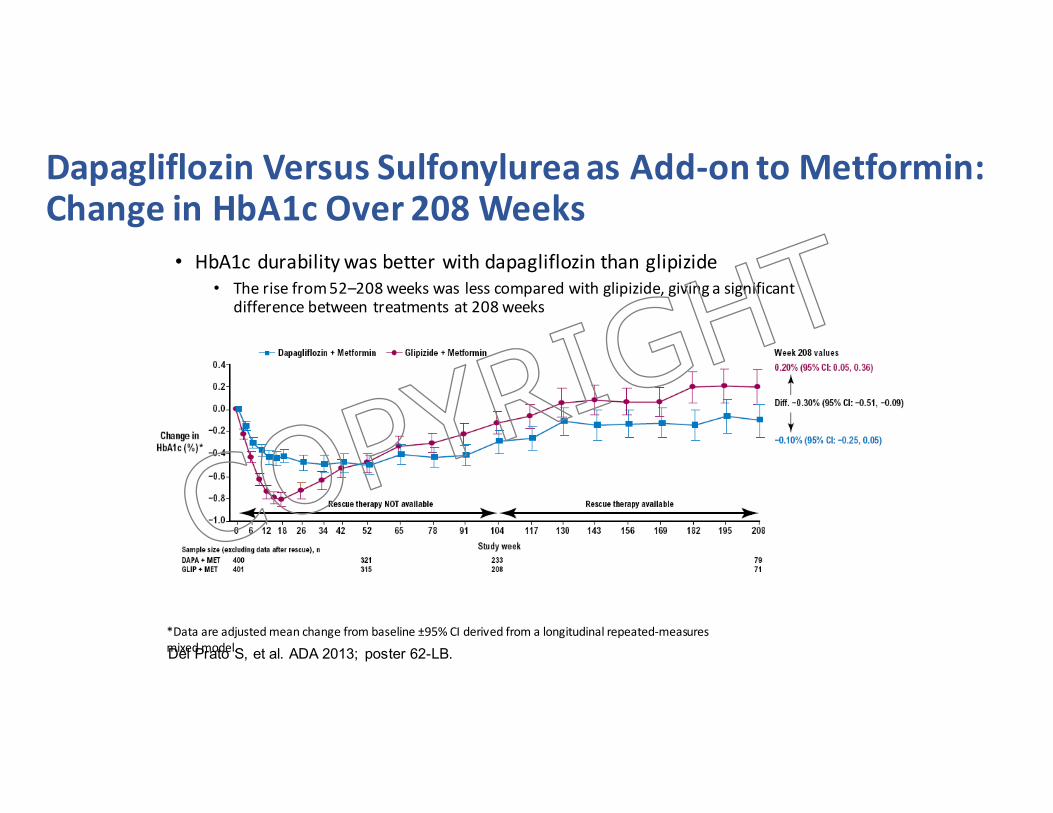
DapagliflozinVersusSulfonylureaasAdd-ontoMetformin:ChangeinHbA1cOver208Weeks
• HbA1cdurabilitywasbetterwithdapagliflozinthanglipizide• Therisefrom52–208weekswaslesscomparedwithglipizide,givingasignificant
differencebetweentreatmentsat208weeks
Del Prato S, et al. ADA 2013; poster 62-LB.*Dataareadjustedmeanchangefrombaseline±95%CIderivedfromalongitudinalrepeated-measuresmixedmodel.
COPYRIG
HT
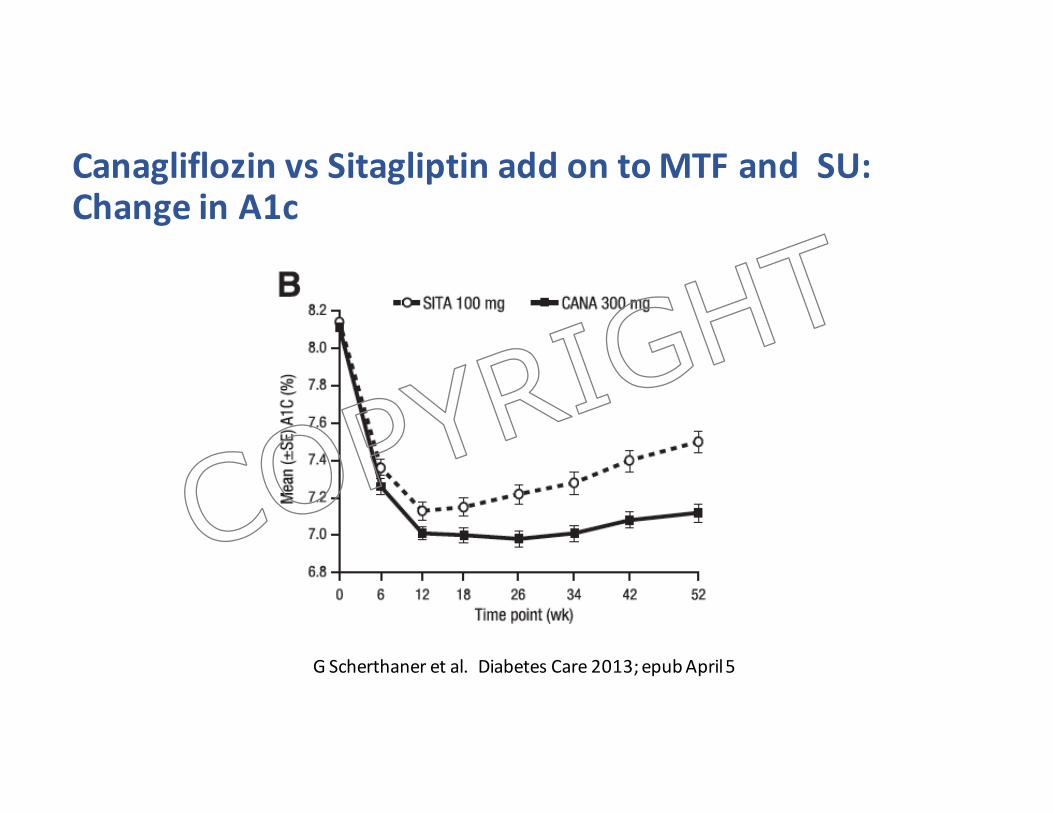
Canagliflozin vs Sitagliptin addontoMTFandSU:ChangeinA1c
GScherthaner etal.DiabetesCare2013;epubApril5
COPYRIG
HT
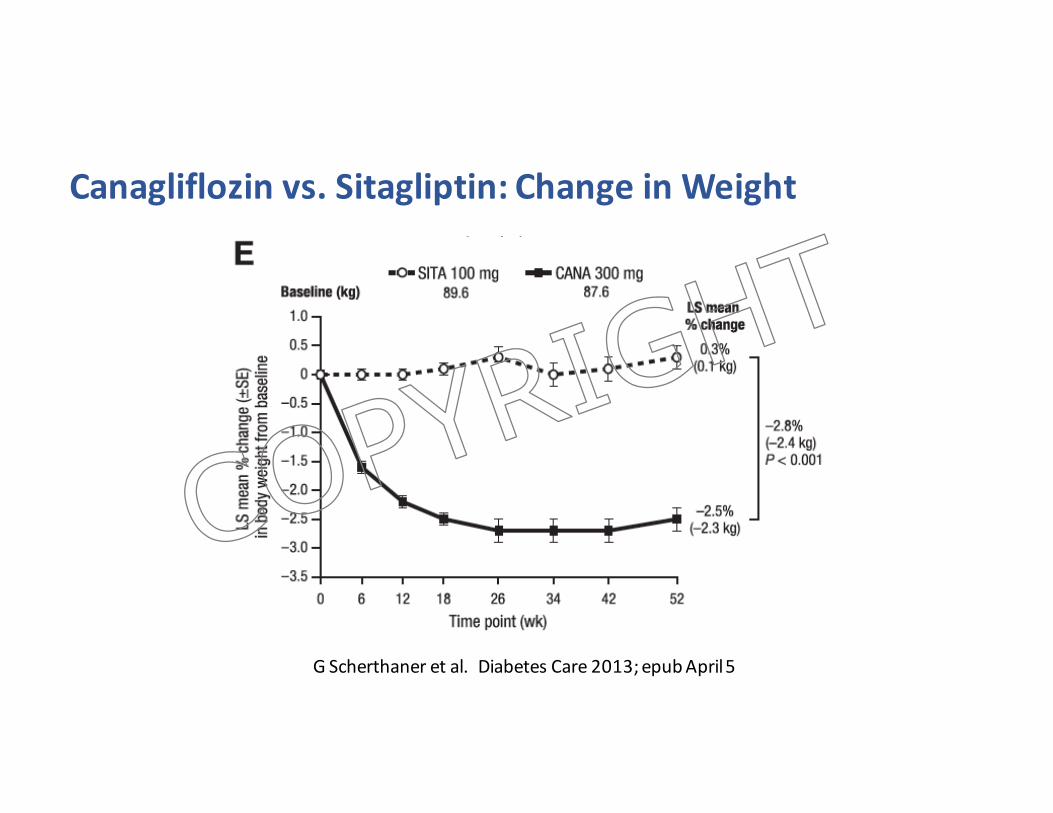
Canagliflozin vs.Sitagliptin:ChangeinWeight
GScherthaner etal.DiabetesCare2013;epubApril5
COPYRIG
HT
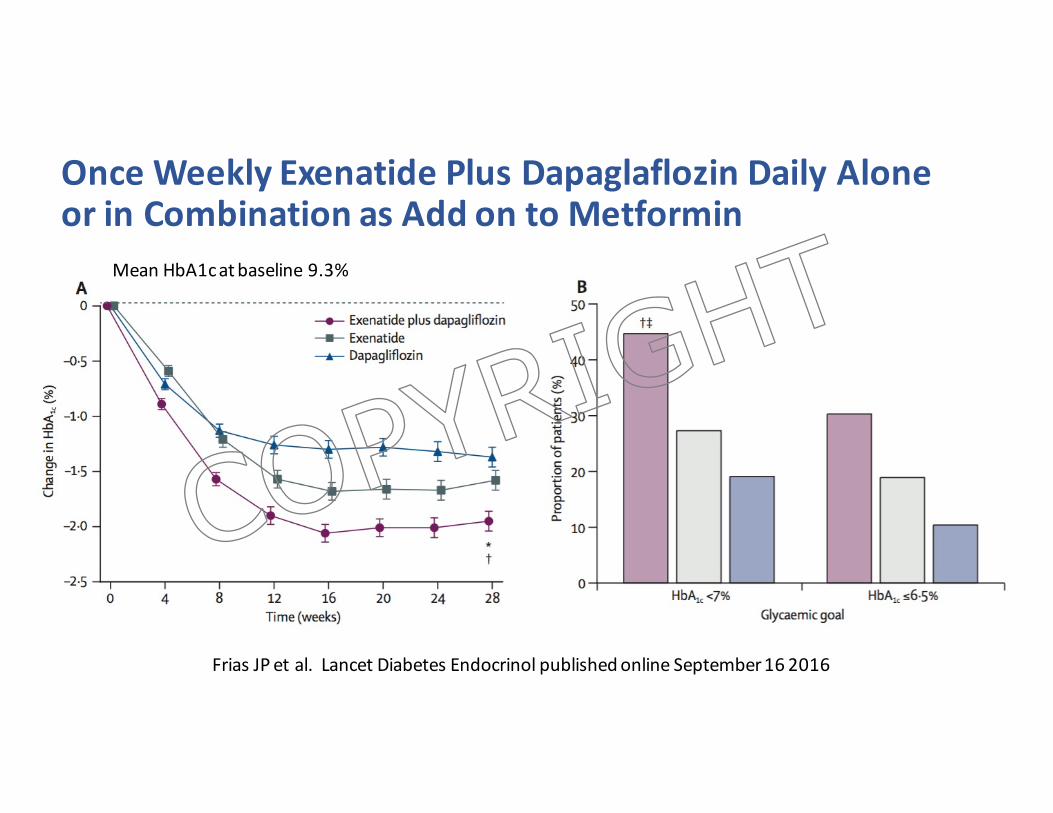
OnceWeeklyExenatide PlusDapaglaflozin DailyAloneorinCombinationasAddontoMetformin
FriasJPetal.LancetDiabetesEndocrinol publishedonlineSeptember162016
MeanHbA1catbaseline9.3%
COPYRIG
HT
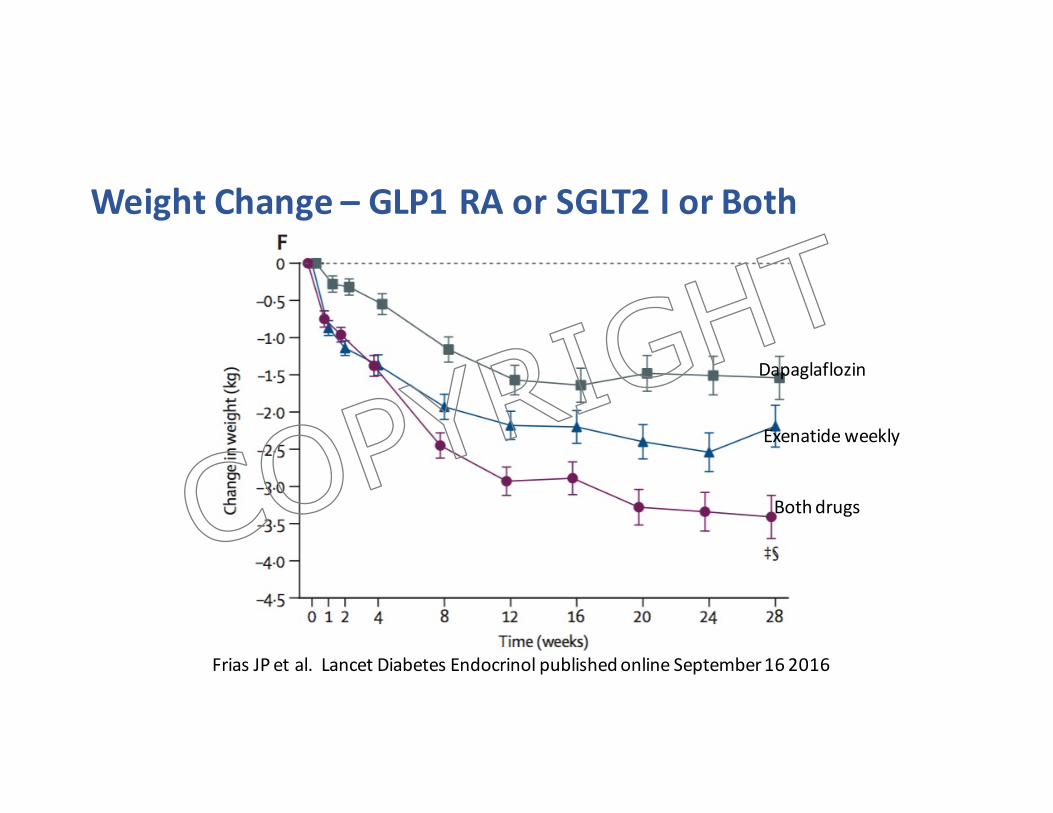
WeightChange– GLP1RAorSGLT2IorBoth
FriasJPetal.LancetDiabetesEndocrinol publishedonlineSeptember162016
Dapaglaflozin
Exenatideweekly
BothdrugsCOPYRIG
HT
BasalInsulinAnalogues– aretheyany“safer”?
• GlargineU-100• Biosimilarglargine• Levemir• GlargineU-300(Toujeo)• Degludec (Tresiba)
COPYRIG
HT
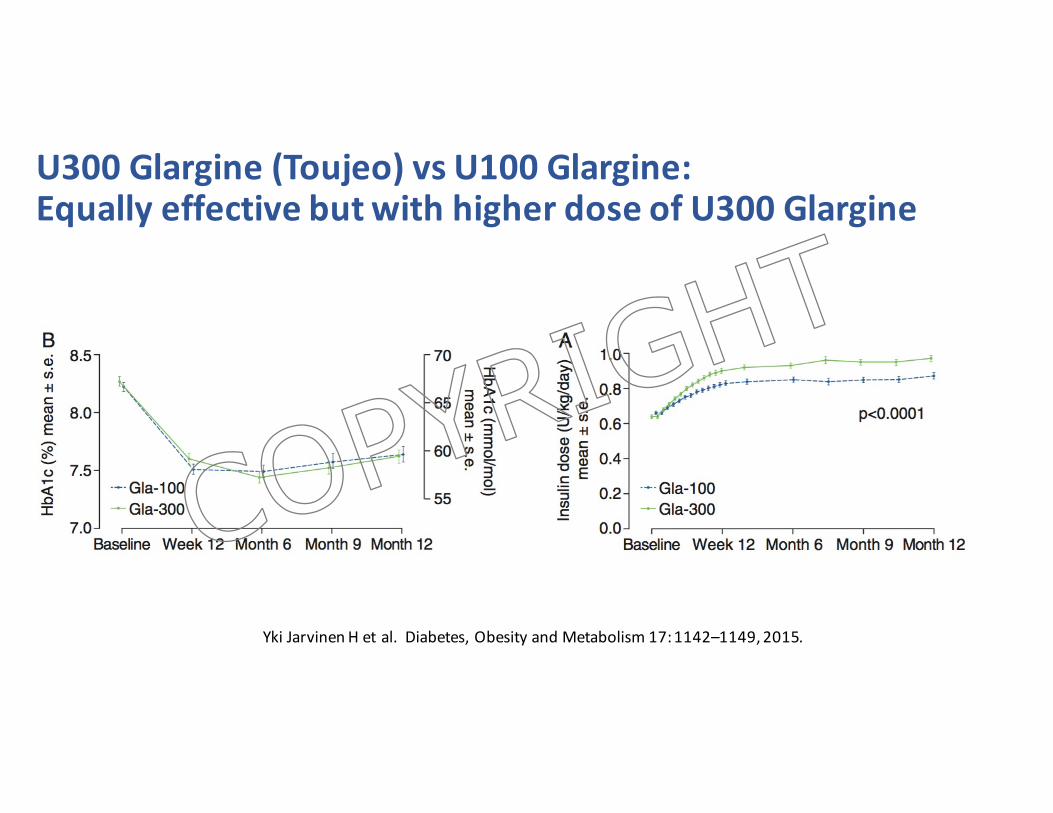
U300Glargine(Toujeo)vsU100Glargine:EquallyeffectivebutwithhigherdoseofU300Glargine
Yki JarvinenHetal.Diabetes,ObesityandMetabolism17:1142–1149,2015.
COPYRIG
HT
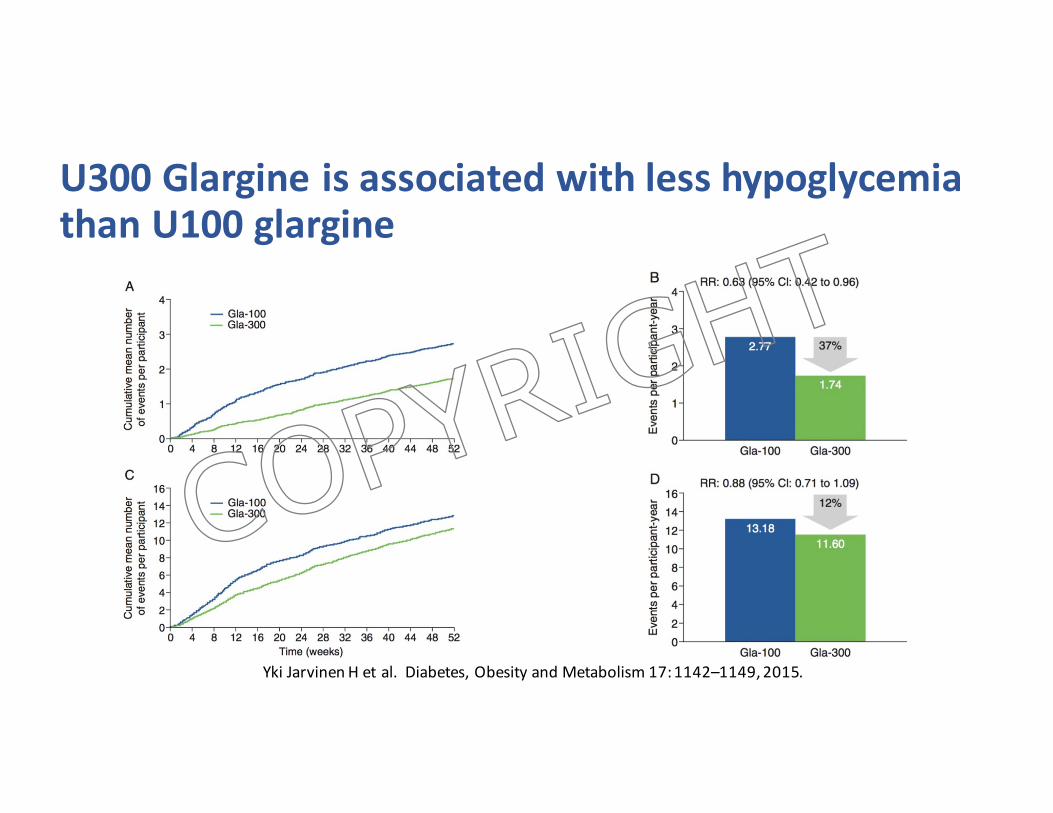
U300GlargineisassociatedwithlesshypoglycemiathanU100glargine
Yki JarvinenHetal.Diabetes,ObesityandMetabolism17:1142–1149,2015.
COPYRIG
HT
SWITCH 2Reduced risk of hypoglycaemia with insulin degludec vs. insulin
glargine U100 in a T2D population on basal insulin: A randomised
double-blind crossover trial
Clinical trial.gov identifier: NCT02030600Wysham et al. Presented at the American Diabetes Association, 76th Annual Scientific Sessions, 10–14 June 2016, New Orleans, LA, USA
COPYRIG
HT
Objective
Primary objective:
• To confirm superiority of IDeg OD compared with IGlar U100 OD in the rates of severe or BG-confirmed symptomatic hypoglycaemia during the maintenance period (after 16 weeks of treatment)
Secondary objectives:
• To confirm superiority of IDeg OD compared with IGlar U100 OD in the rates of severe or BG-confirmed symptomatic nocturnal hypoglycaemiaand the proportion of patients with severe hypoglycaemia during the maintenance period
BG, blood glucose; IDeg, insulin degludec; IGlar U100, insulin glargine U100; OD, once dailyWysham et al. Presented at the American Diabetes Association, 76th Annual Scientific Sessions, 10–14 June 2016, New Orleans, LA, USA
COPYRIG
HT
Hypoglycaemia risk: inclusion criteria
ADA, American Diabetes Association; eGFR, estimated glomerular filtration rateWysham et al. Presented at the American Diabetes Association, 76th Annual Scientific Sessions, 10–14 June 2016, New Orleans, LA, USA
Eligible patients had at least one of the following hypoglycaemia risk factors:
• ≥1 severe hypoglycaemic episodes within the last year
• Moderate chronic renal failure (eGFR 30–59 mL/min/1.73 m2)
• Hypoglycaemic symptoms unawareness
• Exposure to insulin >5 years
• Episode of hypoglycaemia episode within the last 12 weeks (according to ADA definition: ≤70 mg/dL [≤3.9 mmol/L])COP
YRIGHT
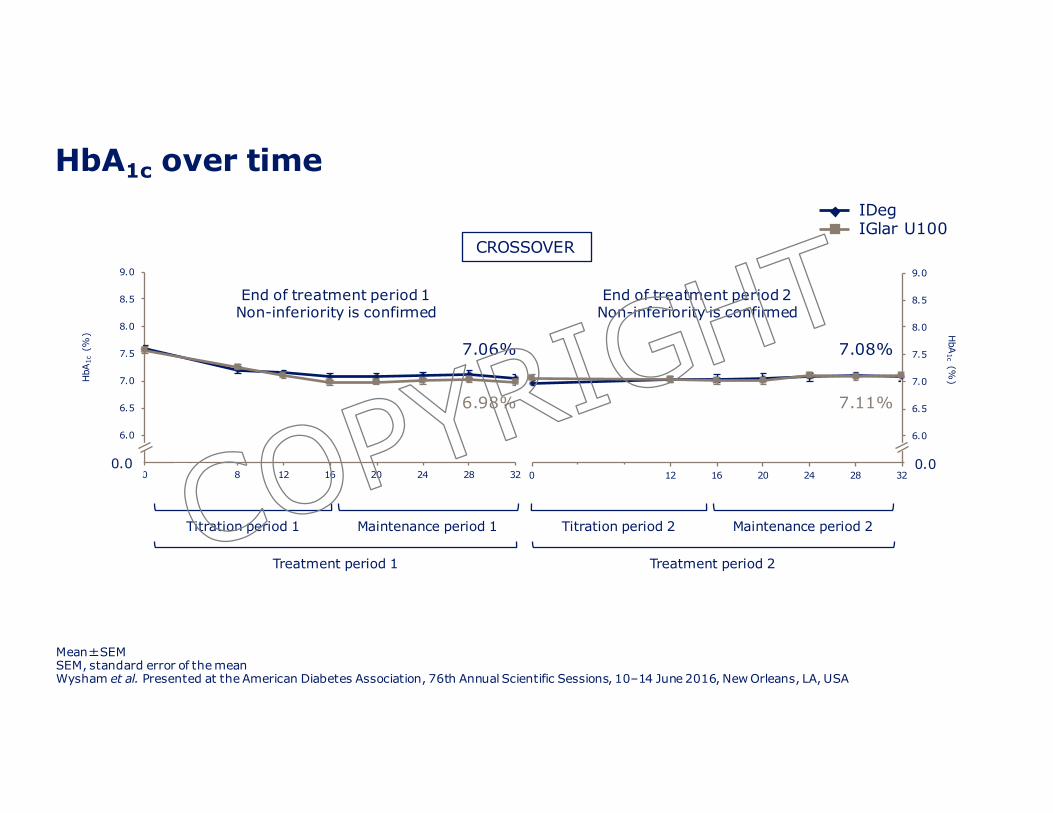
HbA1c over time
5.5
6.0
6.5
7.0
7.5
8.0
8.5
9.0
0 4 8 12 16 20 24 28 32
HbA
1c(%
)
5.5
6.0
6.5
7.0
7.5
8.0
8.5
9.0
0 4 8 12 16 20 24 28 32
HbA
1c(%
)
Titration period 1 Maintenance period 1 Titration period 2 Maintenance period 2
Treatment period 1 Treatment period 2
0.0 0.0
End of treatment period 1Non-inferiority is confirmed
End of treatment period 2Non-inferiority is confirmed
CROSSOVER
IDegIGlar U100
Mean�SEMSEM, standard error of the meanWysham et al. Presented at the American Diabetes Association, 76th Annual Scientific Sessions, 10–14 June 2016, New Orleans, LA, USA
6.98%
7.06% 7.08%
7.11%
COPYRIG
HT
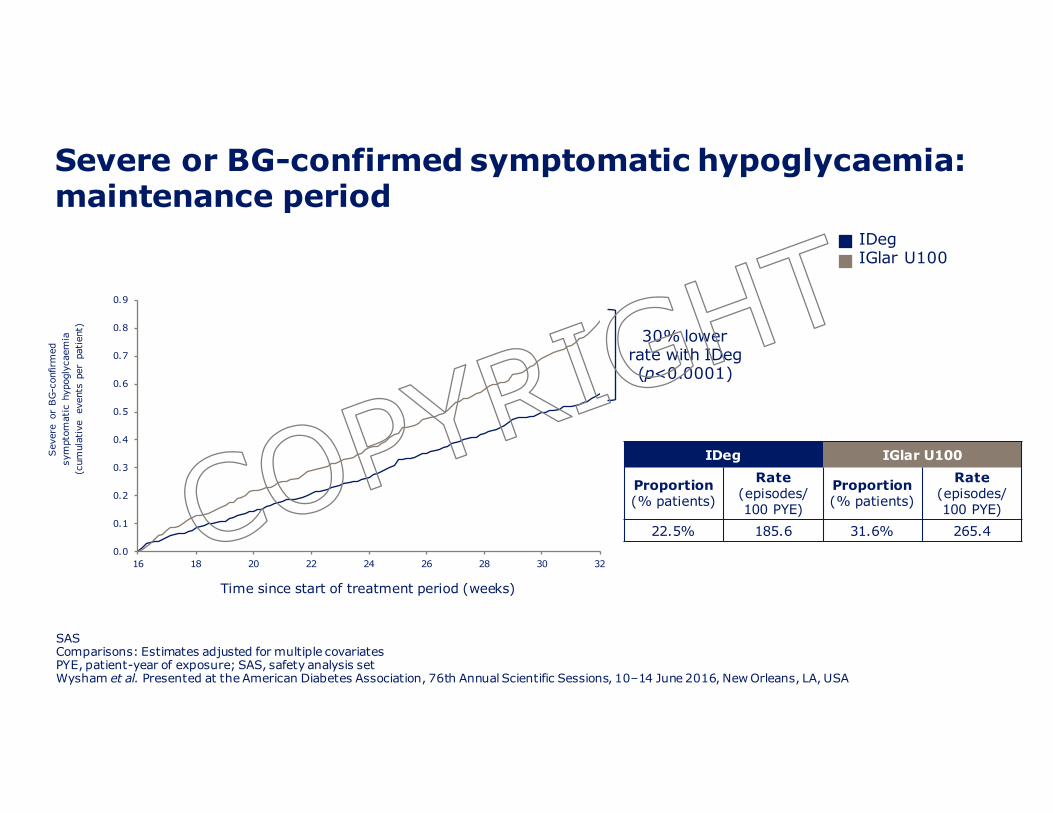
Severe or BG-confirmed symptomatic hypoglycaemia: maintenance period
SASComparisons: Estimates adjusted for multiple covariatesPYE, patient-year of exposure; SAS, safety analysis setWysham et al. Presented at the American Diabetes Association, 76th Annual Scientific Sessions, 10–14 June 2016, New Orleans, LA, USA
30% lower rate with IDeg(p<0.0001)
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
16 18 20 22 24 26 28 30 32
Sev
ere
or B
G-c
onfir
med
sym
ptom
atic
hyp
ogly
caem
ia(c
umul
ativ
e ev
ents
per
pat
ient
)
Time since start of treatment period (weeks)
IDegIGlar U100
IDeg IGlar U100
Proportion(% patients)
Rate(episodes/100 PYE)
Proportion(% patients)
Rate(episodes/100 PYE)
22.5% 185.6 31.6% 265.4COPYRIG
HT
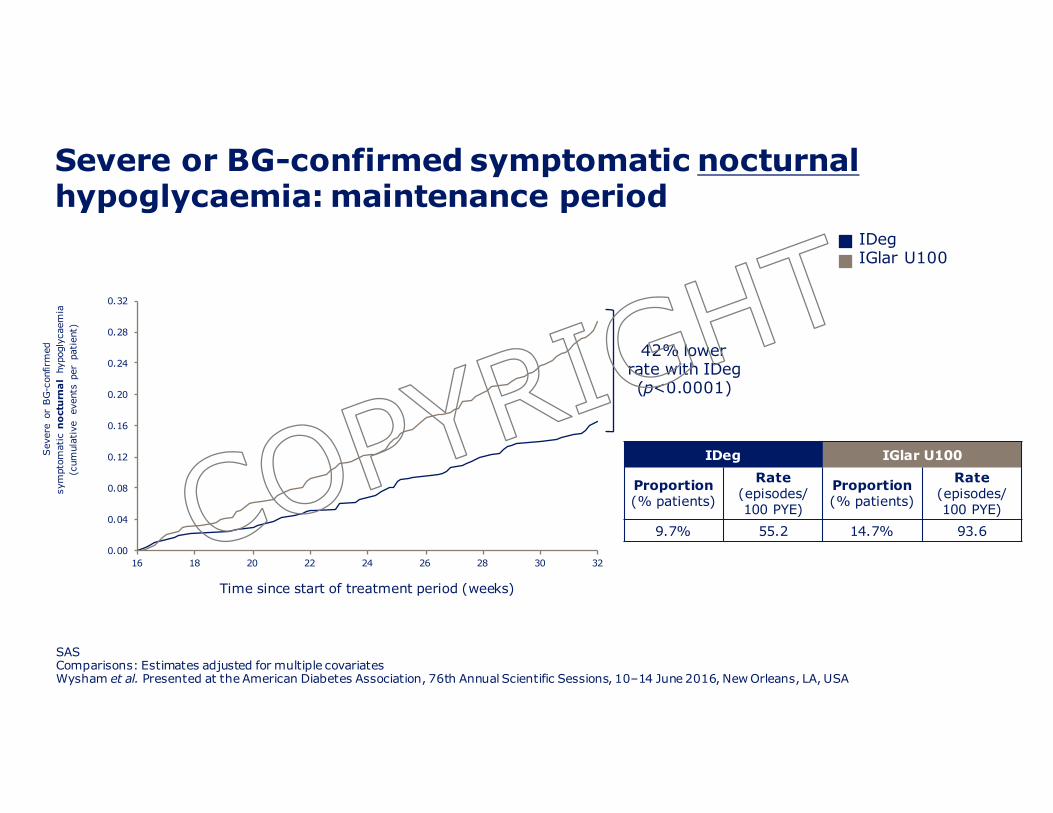
Severe or BG-confirmed symptomatic nocturnalhypoglycaemia: maintenance period
SASComparisons: Estimates adjusted for multiple covariatesWysham et al. Presented at the American Diabetes Association, 76th Annual Scientific Sessions, 10–14 June 2016, New Orleans, LA, USA
42% lower rate with IDeg(p<0.0001)
0.00
0.04
0.08
0.12
0.16
0.20
0.24
0.28
0.32
16 18 20 22 24 26 28 30 32
Sev
ere
or B
G-c
onfir
med
sym
ptom
atic
no
ctu
rna
lhy
pogl
ycae
mia
(cum
ulat
ive
even
ts p
er p
atie
nt)
Time since start of treatment period (weeks)
IDeg IGlar U100
Proportion(% patients)
Rate(episodes/100 PYE)
Proportion(% patients)
Rate(episodes/100 PYE)
9.7% 55.2 14.7% 93.6
IDegIGlar U100
COPYRIG
HT

Uptitrating basalinsulinvsbasalinsulinandGLP1RACOPYRIG
HT
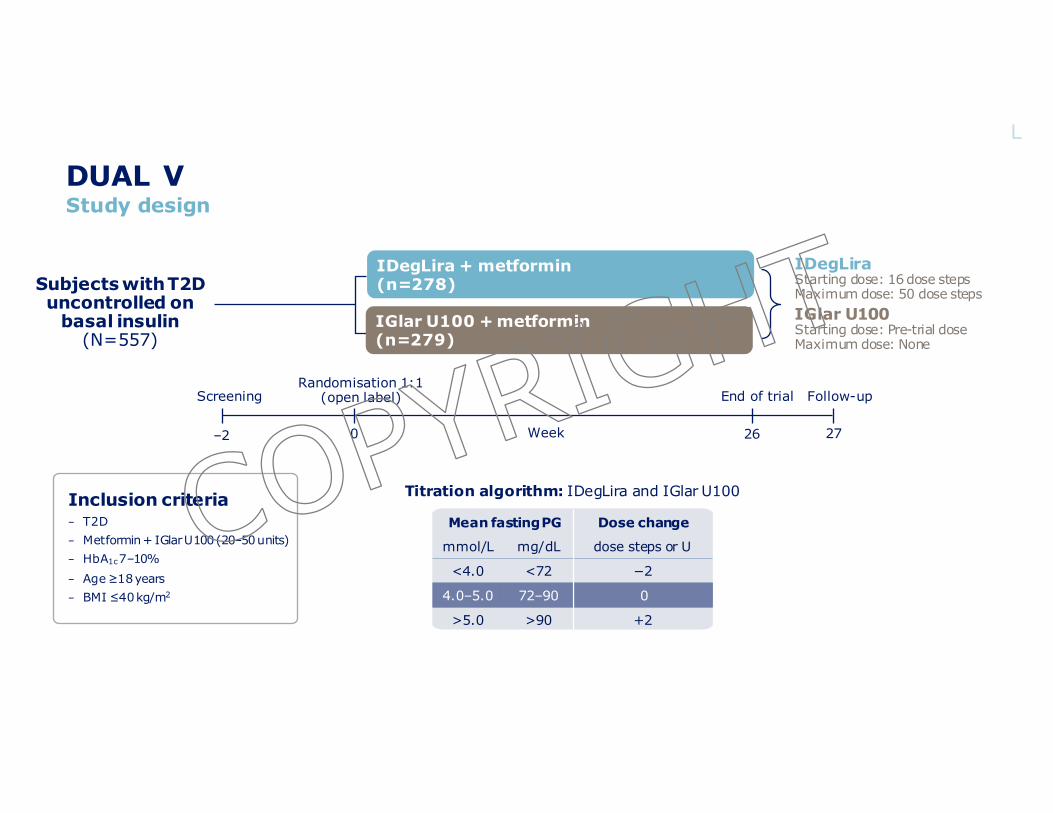
DUAL VStudy design
BMI, body mass index; HbA1c, glycated haemoglobin; IDegLira, insulin degludec/liraglutide; IGlar U100, insulin glargine U100; PG, plasma glucose; T2D, type 2 diabetes; U, unitsLingvay I et al. JAMA 2016;315:898–907
Inclusion criteria− T2D− Metformin + IGlarU100 (20–50 units)− HbA1c7–10%− Age ≥18 years− BMI ≤40 kg/m2
Subjects with T2D uncontrolled on
basal insulin(N=557)
IDegLiraStarting dose: 16 dose stepsMaximum dose: 50 dose stepsIGlar U100Starting dose: Pre-trial doseMaximum dose: None
ScreeningRandomisation 1:1
(open label) End of trial Follow-up
Titration algorithm: IDegLira and IGlar U100
mmol/L mg/dL
<4.0 <72
4.0–5.0 72–90
>5.0 >90
dose steps or U
−2
0
+2
Mean fasting PG Dose change
IGlar U100 + metformin(n=279)
IDegLira + metformin(n=278)
0 27–2 26Week
L
COPYRIG
HT
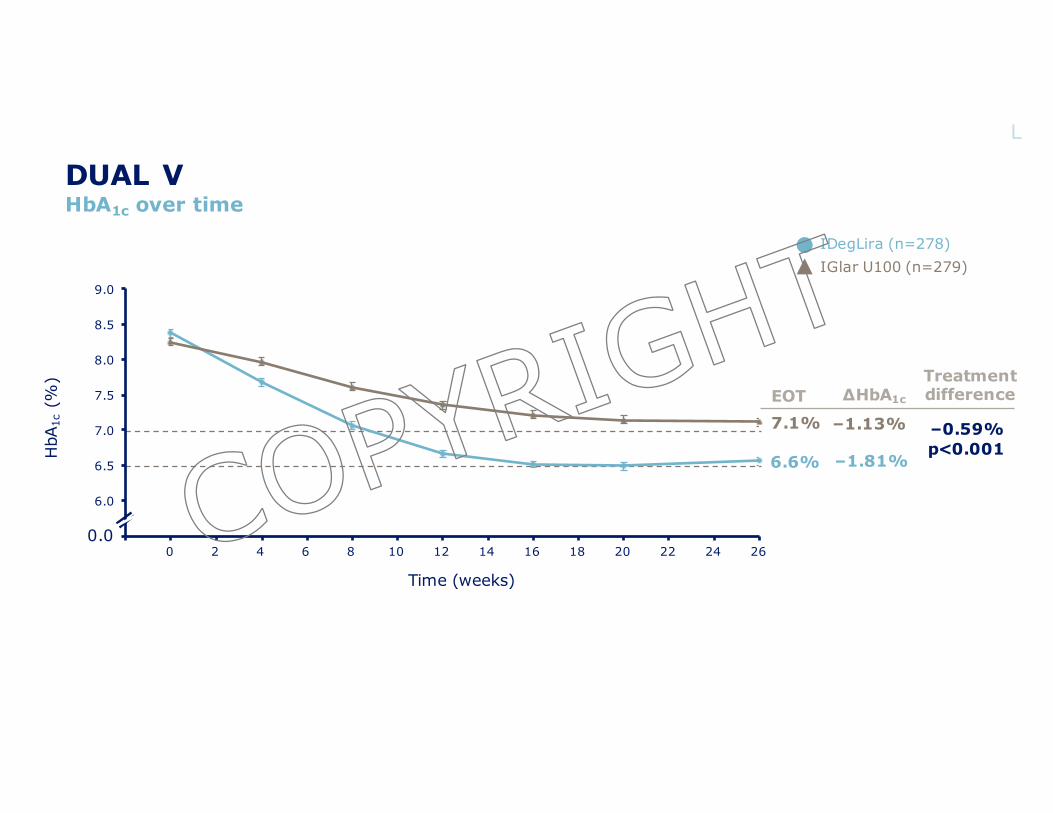
DUAL VHbA1c over time
Mean observed values with error bars (standard error mean) based on FAS and LOCF imputed data. Treatment difference is estimated from an ANCOVA analysis while ∆ values are observed LOCF. ADA/EASD HbA1c target <7.0%; AACE HbA1c target ≤6.5% AACE, American Association of Clinical Endocrinologists; ADA, American Diabetes Association; ANCOVA, analysis of covariance; EASD, European Association for the Study of Diabetes; EOT, end of trial; FAS, full analysis set; HbA1c, glycated haemoglobin; IDegLira, insulin degludec/liraglutide; IGlar U100, insulin glargine U100; LOCF, last observation carried forwardLingvay I et al. JAMA 2016;315:898-907
5.5
6.0
6.5
7.0
7.5
8.0
8.5
9.0
-2 0 2 4 6 8 10 12 14 16 18 20 22 24 26
7.1%
6.6%HbA
1c(%
)
Time (weeks)
IDegLira (n=278)IGlar U100 (n=279)
EOTTreatment difference ∆HbA1c
–1.81%
–1.13%
0.0
–0.59%p<0.001
L
COPYRIG
HT
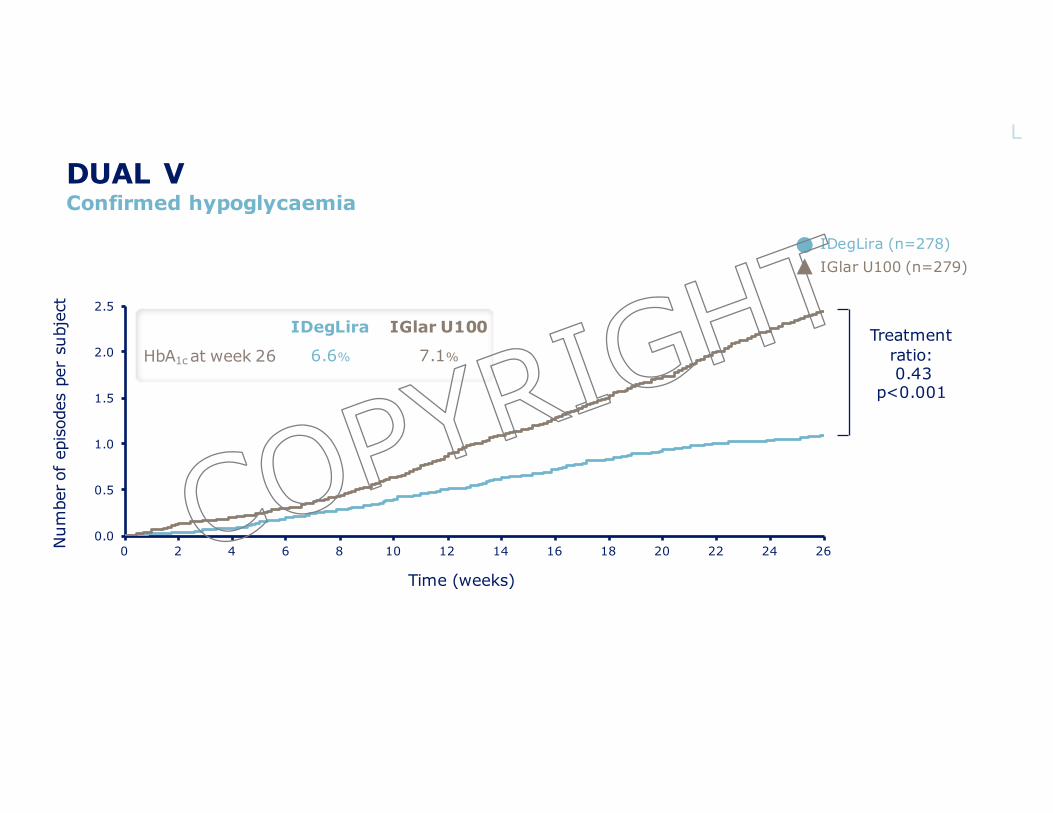
DUAL VConfirmed hypoglycaemia
Mean cumulative function based on SASTreatment ratio is estimated from a negative binomial model based on FASFAS, full analysis set; HbA1c, glycated haemoglobin; IDegLira, insulin degludec/liraglutide; IGlar U100, insulin glargine U100; SAS, safety analysis setLingvay I et al. JAMA 2016;315:898–907
0.0
0.5
1.0
1.5
2.0
2.5
0 2 4 6 8 10 12 14 16 18 20 22 24 26Num
ber o
f ep
isod
es p
er s
ubje
ct
Treatment ratio:0.43
p<0.001
IDegLira IGlar U100
HbA1c at week 26 6.6% 7.1%
Time (weeks)
IDegLira (n=278)IGlar U100 (n=279)
L
COPYRIG
HT
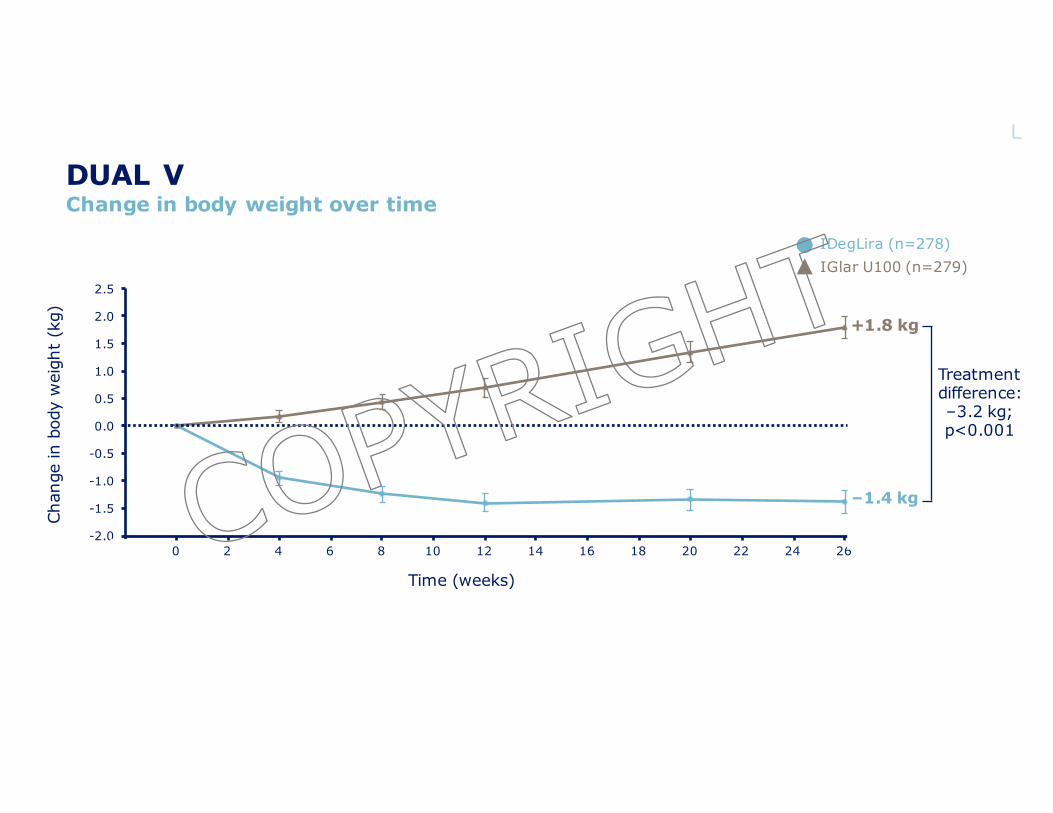
DUAL VChange in body weight over time
Mean observed values with error bars (standard error mean) based on FAS and LOCF imputed dataTreatment difference is estimated from an ANCOVA analysis while ∆ values are observed LOCFANCOVA, analysis of covariance; FAS, full analysis set; IDegLira, insulin degludec/liraglutide; IGlar U100, insulin glargine U100; LOCF, last observation carried forwardLingvay I et al. JAMA 2016;315:898–907
-2.0
-1.5
-1.0
-0.5
0.0
0.5
1.0
1.5
2.0
2.5
-2 0 2 4 6 8 10 12 14 16 18 20 22 24 26
Treatmentdifference:–3.2 kg;p<0.001
Chan
ge in
bod
y w
eigh
t (k
g) +1.8 kg
–1.4 kg
Time (weeks)
IDegLira (n=278)IGlar U100 (n=279)
L
COPYRIG
HT
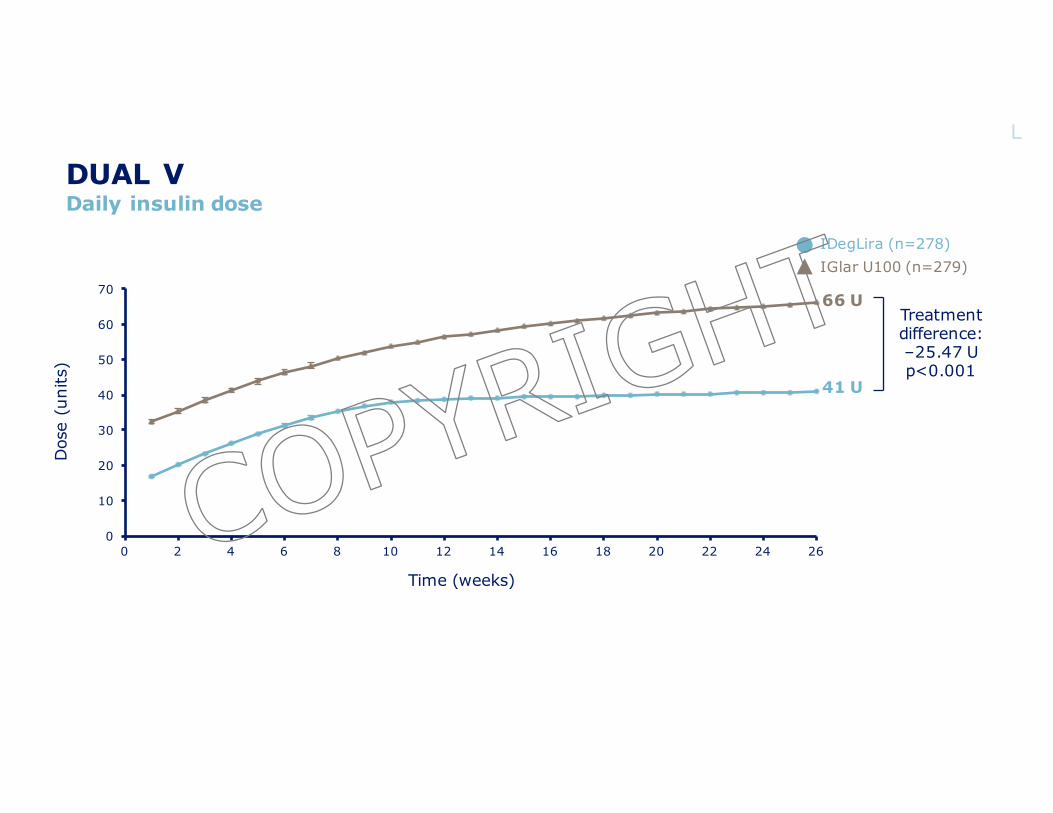
DUAL VDaily insulin dose
There was no maximum dose for IGlar U100Mean observed values with error bars (standard error mean) based on SAS and LOCF imputed dataTreatment difference is estimated from an ANCOVA analysisANCOVA, analysis of covariance; IDegLira, insulin degludec/liraglutide; IGlar U100, insulin glargine U100; LOCF, last observation carried forward; SAS, safety analysis set; U, unitsLingvay I et al. JAMA 2016;315:898–907
0
10
20
30
40
50
60
70
0 2 4 6 8 10 12 14 16 18 20 22 24 26
Dos
e (u
nits
)
41 U
66 UTreatment difference:–25.47 Up<0.001
Time (weeks)
IDegLira (n=278)IGlar U100 (n=279)
L
COPYRIG
HT
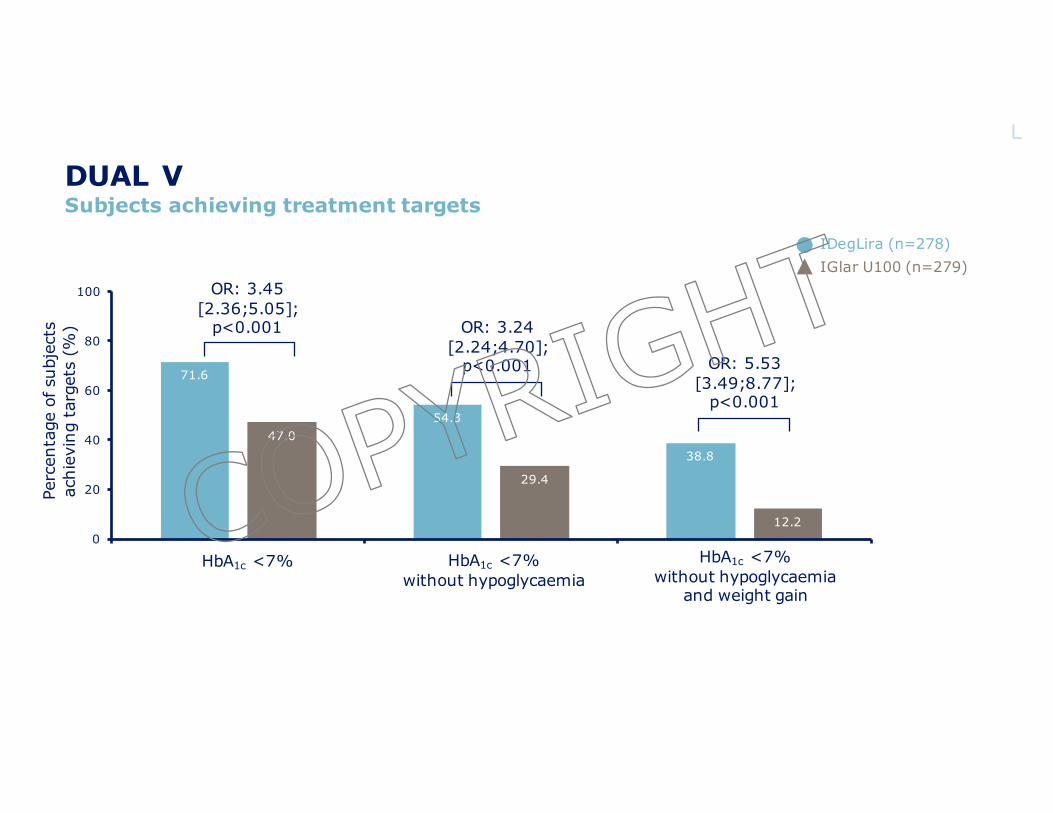
DUAL VSubjects achieving treatment targets
Values are based on FAS and LOCF imputed dataOdds ratios (IDegLira/IGlar U100) are from a logistic regression modelFAS, full analysis set; HbA1c, glycated haemoglobin; IDegLira, insulin degludec/liraglutide; IGlar U100, insulin glargine U100; LOCF, last observation carried forward; OR, odds ratioLingvay I et al. JAMA 2016;315:898–907
71.6
54.3
38.8
47.0
29.4
12.20
20
40
60
80
100 OR: 3.45[2.36;5.05];
p<0.001 OR: 3.24[2.24;4.70];
p<0.001 OR: 5.53[3.49;8.77];
p<0.001
Perc
enta
ge o
f sub
ject
sac
hiev
ing
targ
ets
(%)
HbA1c <7% HbA1c <7%without hypoglycaemia
HbA1c <7%without hypoglycaemia
and weight gain
IDegLira (n=278)IGlar U100 (n=279)
L
COPYRIG
HT
AddingGLP1RAtobasalinsulin:impactonglucosecontrol,weightandhypoglycemiaCOPYRIG
HT
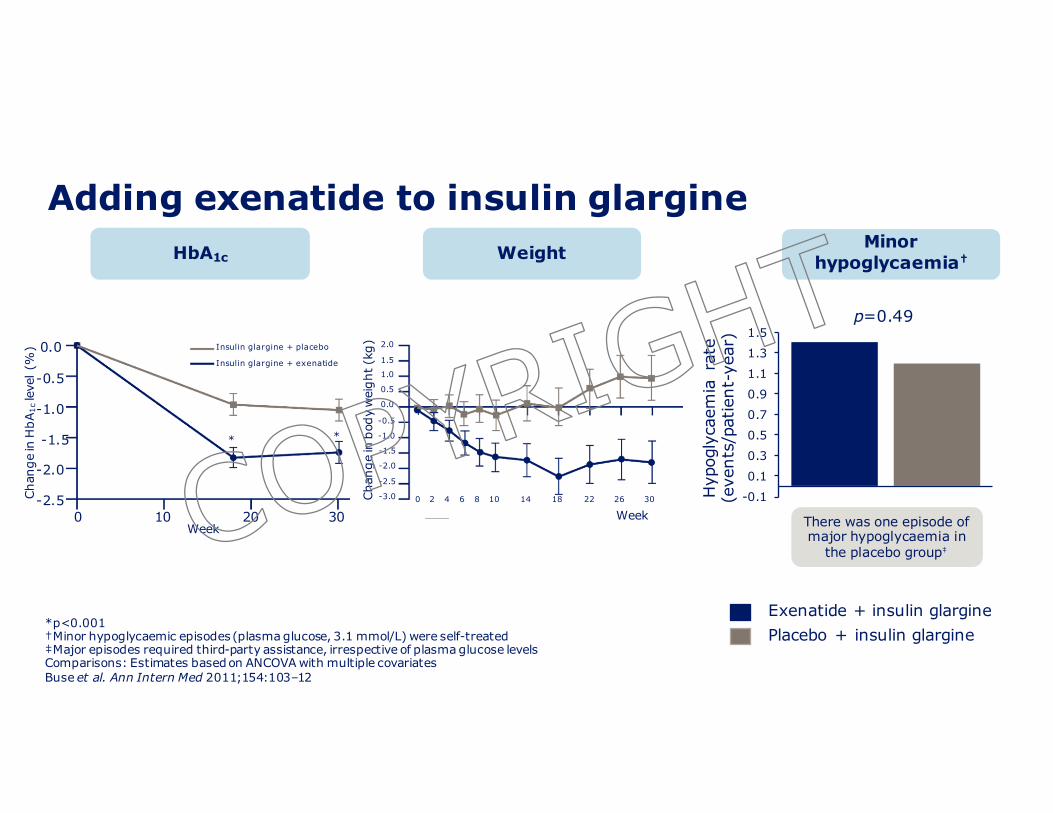
Adding exenatide to insulin glargine
-0.1
0.1
0.3
0.5
0.7
0.9
1.1
1.3
1.5
Hyp
ogly
caem
ia r
ate
(eve
nts/
patie
nt-y
ear)
Exenatide + insulin glarginePlacebo + insulin glargine
Minorhypoglycaemia†
p=0.49
There was one episode of major hypoglycaemia in
the placebo group‡
*p<0.001†Minor hypoglycaemic episodes (plasma glucose, 3.1 mmol/L) were self-treated ‡Major episodes required third-party assistance, irrespective of plasma glucose levelsComparisons: Estimates based on ANCOVA with multiple covariates Buse et al. Ann Intern Med 2011;154:103–12
Insulin glargine + placebo
Insulin glargine + exenatide
Week0 10 20 30
-2.5
-2.0
-1.5
-1.0
-0.5
0.0
Chan
ge in
HbA
1cle
vel (
%)
* *
HbA1c Weight
Chan
ge in
bod
y w
eigh
t (kg
) 2.0
1.5
1.0
0.5
0.0
-0.5
-1.0
-1.5
-2.0
-2.5
-3.0 0 2 4 6 8 10 14 18 22 26 30
WeekCOPYRIG
HT
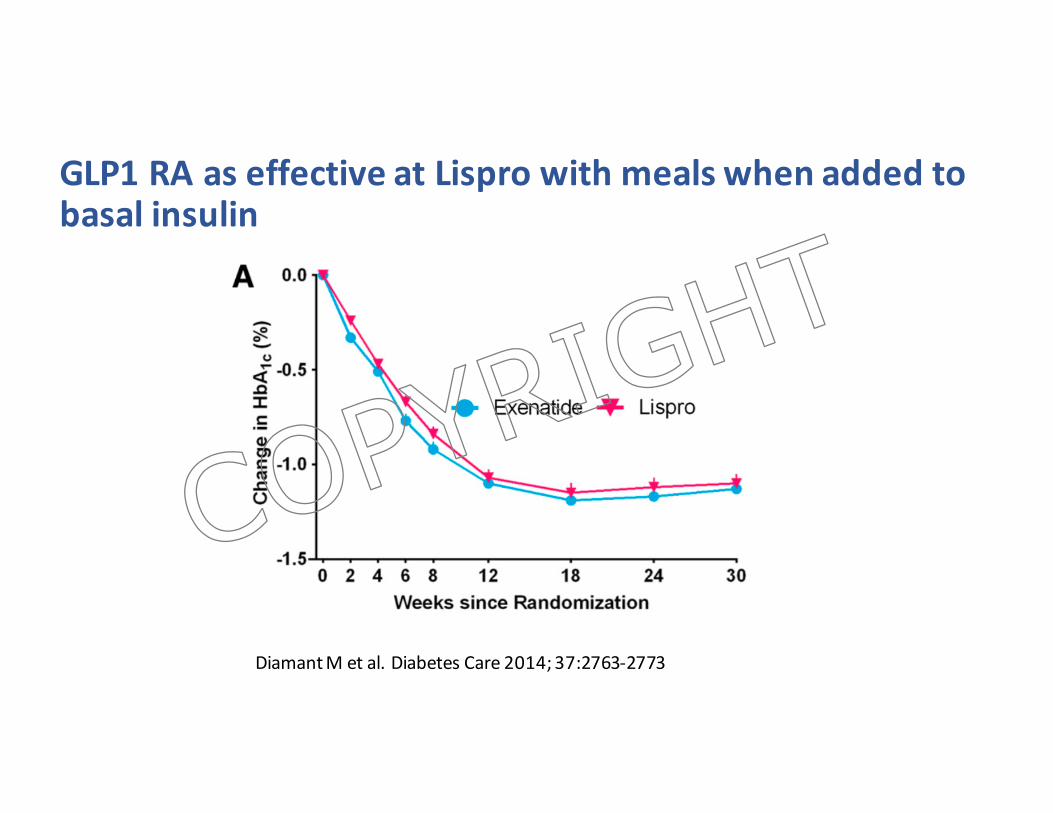
GLP1RAaseffectiveatLispro withmealswhenaddedtobasalinsulin
DiamantMetal.DiabetesCare2014;37:2763-2773
COPYRIG
HT
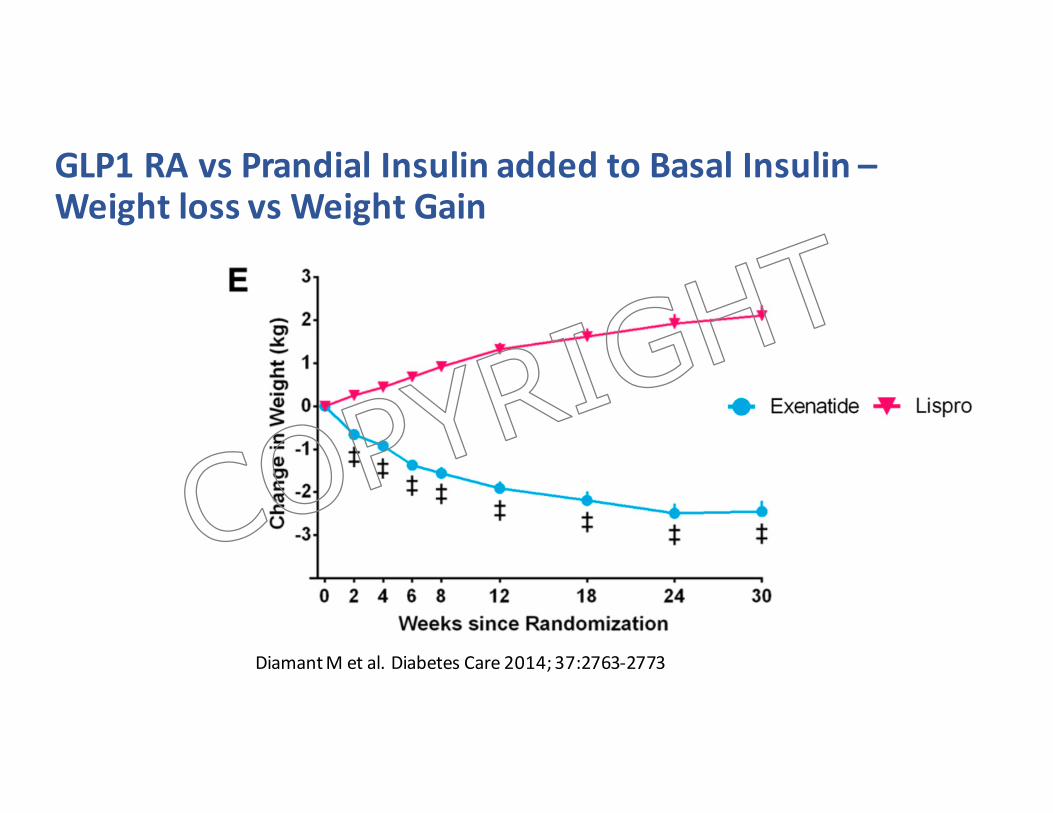
GLP1RAvsPrandialInsulinaddedtoBasalInsulin–WeightlossvsWeightGain
DiamantMetal.DiabetesCare2014;37:2763-2773
COPYRIG
HT
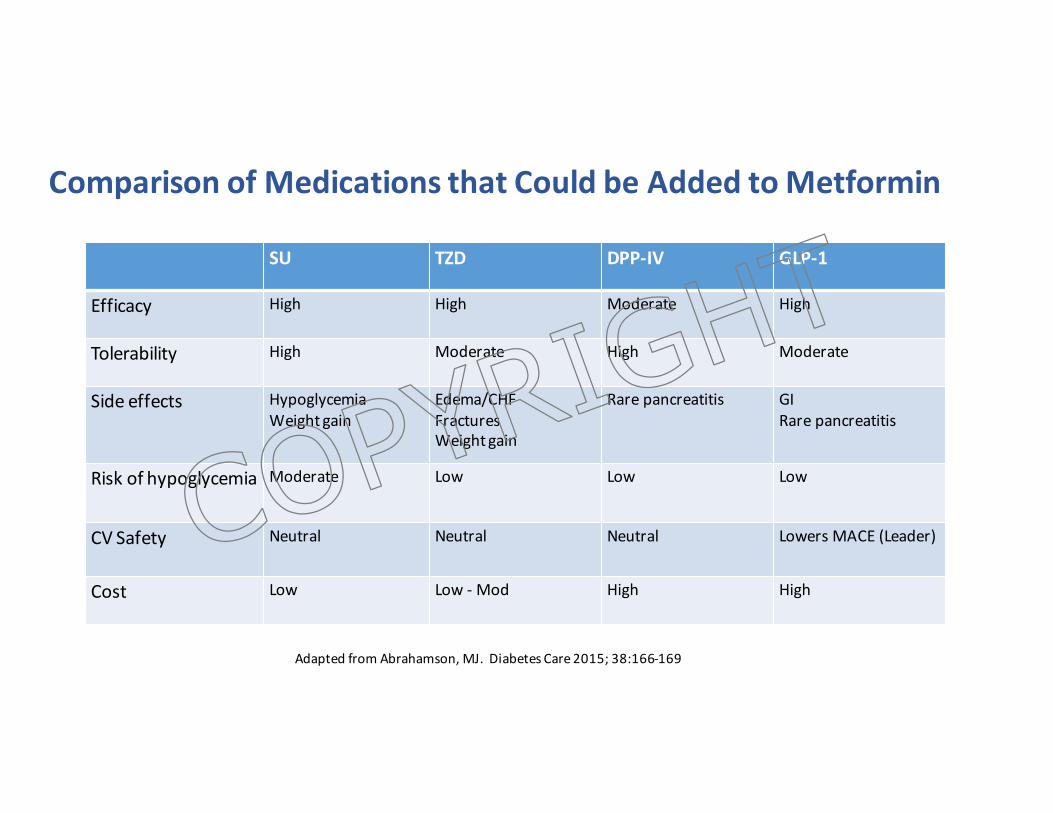
ComparisonofMedicationsthatCouldbeAddedtoMetformin
SU TZD DPP-IV GLP-1
Efficacy High High Moderate High
Tolerability High Moderate High Moderate
Sideeffects HypoglycemiaWeightgain
Edema/CHFFracturesWeightgain
Rarepancreatitis GIRarepancreatitis
Riskofhypoglycemia Moderate Low Low Low
CVSafety Neutral Neutral Neutral LowersMACE(Leader)
Cost Low Low - Mod High High
AdaptedfromAbrahamson,MJ.DiabetesCare2015;38:166-169
COPYRIG
HT
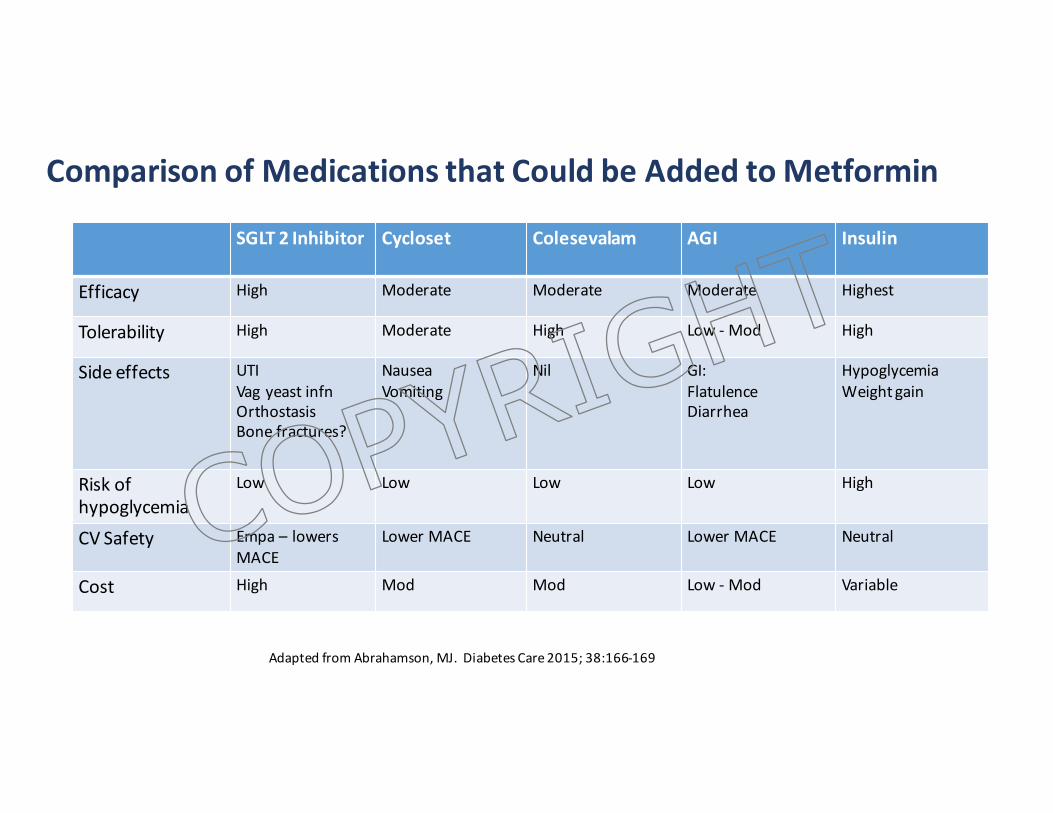
ComparisonofMedicationsthatCouldbeAddedtoMetformin
SGLT 2Inhibitor Cycloset Colesevalam AGI Insulin
Efficacy High Moderate Moderate Moderate Highest
Tolerability High Moderate High Low- Mod High
Sideeffects UTIVag yeastinfnOrthostasisBonefractures?
NauseaVomiting
Nil GI:FlatulenceDiarrhea
HypoglycemiaWeightgain
Riskofhypoglycemia
Low Low Low Low High
CVSafety Empa – lowersMACE
LowerMACE Neutral LowerMACE Neutral
Cost High Mod Mod Low - Mod Variable
AdaptedfromAbrahamson,MJ.DiabetesCare2015;38:166-169
COPYRIG
HT
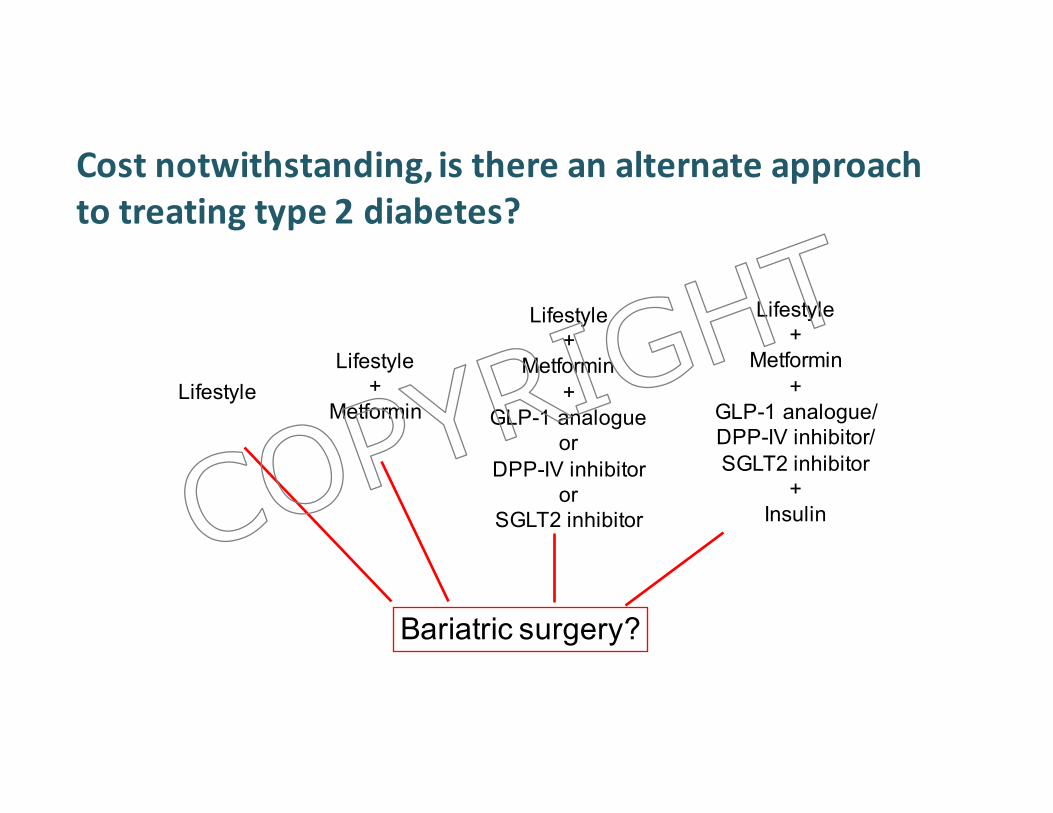
Costnotwithstanding,isthereanalternateapproachtotreatingtype2diabetes?
Lifestyle+
Metformin+
GLP-1 analogue/DPP-IV inhibitor/SGLT2 inhibitor
+Insulin
LifestyleLifestyle
+Metformin
Lifestyle+
Metformin+
GLP-1 analogueor
DPP-IV inhibitoror
SGLT2 inhibitor
Bariatric surgery?
COPYRIG
HT
Summary• Multiplepathophysiologicalabnormalitiesexistinthepersonwithtype2DM
• Therearemedicationsthatcanaddressmostofthesepathophysiologicderangements
• NewerdataisemergingontheCVsafetyofdrugsusedtotreattype2DM• Moredrugsarenowavailablethathaveweight“benefit”andarenotassociatedwithhypoglycemia
• Useofnewerbasalinsulinanalogues,andcombinationsofbasalanalogueswithGLP1receptoragonistsreducesratesofhypoglycemia
• GLP1RAcanbeusedaseffectivelyasprandialinsulinwithfeweradverseevents
COPYRIG
HT