Embed Size (px)
Citation preview

Treatment Options Treatment Options for End Stage for End Stage
Kidney DiseaseKidney Disease
Dr Vipula De SilvaDr Vipula De Silva

Chronic Kidney DiseaseChronic Kidney Disease
Very CommonVery Common Usually does not progressUsually does not progress Increases cardiovascular riskIncreases cardiovascular risk

K-DOQI Classification of K-DOQI Classification of CKDCKD
Stage GFR(ml/min)
Description Prevalence(%)
1 > 90 1 Kidney damage withnormal or GFR
3.3
2 60-89 1 Kidney damage withmild GFR
3.0
3 30-59 Moderate GFR 4.34 15-29 Severe GFR 0.25 < 15 Kidney failure 0.2

Most CKD patients are Most CKD patients are stablestable
Rate of GFR decline (ml/min/1.73m2/year) <2.0 2.0-2.9 3.0-3.9 4.0-4.9 >5.0 Age (years) <70 (%) 82 4 5 5 5 70-80 (%) 80 5 4 3 7 >80 (%) 77 6 3 4 10 All (%) 79 5 4 4 8

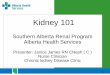
Go, A. S. et al. N Engl J Med 2004;351:1296-1305
Adjusted Hazard Ratio for Death from Any Cause, Cardiovascular Events, and Hospitalization among 1,120,295 Ambulatory Adults, According to the Estimated GFR

But a small proportion do But a small proportion do progressprogress
Renal function declines with timeRenal function declines with time Develop the complications of renal Develop the complications of renal
diseasedisease Renal AnaemiaRenal Anaemia Renal Bone DiseaseRenal Bone Disease
Approach End Stage Kidney DiseaseApproach End Stage Kidney Disease

Identifying ESKDIdentifying ESKD
SymptomsSymptoms Nausea / vomitingNausea / vomiting Poor appetite / weight lossPoor appetite / weight loss
SignsSigns Fluid overloadFluid overload
BiochemistryBiochemistry High potassium, acidosis, high phosphateHigh potassium, acidosis, high phosphate
Declining eGFRDeclining eGFR

Treatment Options for Treatment Options for ESKDESKD
Haemodialysis (HD)Haemodialysis (HD) Peritoneal Dialysis (CAPD or APD)Peritoneal Dialysis (CAPD or APD) Renal transplantationRenal transplantation Conservative PathwayConservative Pathway

How do we choose?How do we choose?
Careful patient educationCareful patient education Patient education programmesPatient education programmes Expert patientsExpert patients Visits to dialysis unitsVisits to dialysis units
Medical best adviseMedical best advise Some patients will tolerate dialysis Some patients will tolerate dialysis
poorly – e.g. cardiovascular problemspoorly – e.g. cardiovascular problems Some abdominal surgery can make Some abdominal surgery can make
CAPD impossibleCAPD impossible

Dialysis HistoryDialysis History
Thomas Graham coined Thomas Graham coined the term dialysis in the term dialysis in 18611861
Crystalloids diffuse Crystalloids diffuse through vegetable through vegetable parchment coated with parchment coated with albumin albumin

First Dialysis MachinesFirst Dialysis Machines
George Haas George Haas performed the first performed the first successful human successful human dialysis in 1924dialysis in 1924
The first practical The first practical human haemodialysis human haemodialysis machine was machine was developed by WJ Kolff developed by WJ Kolff and H Berk in 1943 and H Berk in 1943 (Rotating Drum)(Rotating Drum)

HaemodialysisHaemodialysis
Blood is removed from the Blood is removed from the patients and cleaned in an patients and cleaned in an extracorporeal circuitextracorporeal circuit
Requires high flow access Requires high flow access to circulation – AV fistula to circulation – AV fistula or large diameter dialysis or large diameter dialysis lineline
Usually centre or satellite Usually centre or satellite unit basedunit based
Usually 4 hours, 3 times a Usually 4 hours, 3 times a weekweek

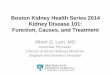
An AV fistula with dialysis An AV fistula with dialysis needlesneedles

A Dialysis CatheterA Dialysis Catheter

Disadvantages of HDDisadvantages of HD
Centre based – travel to unit 3 times Centre based – travel to unit 3 times a weeka week
Access complicationsAccess complications Line infectionsLine infections AV Fistula thrombosesAV Fistula thromboses
Cardiovascular traumaCardiovascular trauma Blood borne virus infection riskBlood borne virus infection risk AnticoagulationAnticoagulation

Peritoneal DialysisPeritoneal Dialysis
Involves the use of the patients Involves the use of the patients peritoneal membrane as a dialysis peritoneal membrane as a dialysis membranemembrane
Dialysis fluid is put into peritoneal Dialysis fluid is put into peritoneal space via catheterspace via catheter
Left in for 6 hours and drained outLeft in for 6 hours and drained out Immediately replaced by more fluidImmediately replaced by more fluid Continuous Ambulatory Peritoneal Continuous Ambulatory Peritoneal
DialysisDialysis

Peritoneal DialysisPeritoneal Dialysis

Automated Peritoneal Automated Peritoneal DialysisDialysis
APD machine moves fluid in and out APD machine moves fluid in and out of peritoneal space while the patient of peritoneal space while the patient is asleepis asleep
More convenient for manyMore convenient for many Often avoids many day time Often avoids many day time
exchangedexchanged May provide more efficient dialysisMay provide more efficient dialysis

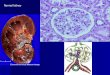
APD MachineAPD Machine

Disadvantages of PDDisadvantages of PD
Risk of peritonitisRisk of peritonitis Not as efficient a dialysis as HD – Not as efficient a dialysis as HD –
not suitable for very large patientsnot suitable for very large patients Glucose load to diabeticsGlucose load to diabetics Bloated feelingBloated feeling Dependent on regular bowel Dependent on regular bowel
movementsmovements

TransplantationTransplantation
First successful kidney transplant between First successful kidney transplant between identical twins was performed by Joseph E. identical twins was performed by Joseph E. Murray and J. Hartwell Harrison in 1954Murray and J. Hartwell Harrison in 1954
Very effective form of renal replacement Very effective form of renal replacement therapytherapy
About 50% of people in UK with ESRD kept About 50% of people in UK with ESRD kept alive by a working transplantalive by a working transplant
New immunosuppression means excellent 1 New immunosuppression means excellent 1 year and 5 year survivalyear and 5 year survival
Careful and very frequent follow up in the first Careful and very frequent follow up in the first yearyear

Renal TransplantationRenal Transplantation

TransplantationTransplantation
Number of patients needing kidneys Number of patients needing kidneys is increasing steadilyis increasing steadily
Cadaveric organ availability is falling Cadaveric organ availability is falling graduallygradually
Live related programme slowly Live related programme slowly expandingexpanding
Number of transplants per year – at Number of transplants per year – at best stablebest stable

Disadvantages of Disadvantages of TransplantsTransplants
Infection riskInfection risk BacterialBacterial ViralViral FungalFungal
New Onset Diabetes After New Onset Diabetes After Transplant (NODAT)Transplant (NODAT)
MalignancyMalignancy Skin tumours, lymphomaSkin tumours, lymphoma

Conservative PathwayConservative Pathway
Based on patient choiceBased on patient choice Aim to control symptoms of Aim to control symptoms of
progressive renal declineprogressive renal decline Close links with palliative care teamsClose links with palliative care teams Emphasis on trying to take care to Emphasis on trying to take care to
patients homespatients homes Increasing awareness that this Increasing awareness that this
provides better quality of life for many provides better quality of life for many patientspatients

Spectrum of treatment Spectrum of treatment availableavailable
Patient may start with CAPDPatient may start with CAPD Then may get a transplantThen may get a transplant 10 years later transplant fails – start 10 years later transplant fails – start
HDHD 5 years on HD, may decide on 5 years on HD, may decide on
withdrawing treatment and opting withdrawing treatment and opting for conservative carefor conservative care

The demand for RRTThe demand for RRT
Expanding at 7-8% each year in the Expanding at 7-8% each year in the UKUK
We are treating and increasingly We are treating and increasingly elderly populationelderly population
Co-morbidity burden is increasingCo-morbidity burden is increasing Expansion of dialysis capacity is Expansion of dialysis capacity is
constant challengeconstant challenge


Our AimOur Aim
To identify those needing RRT earlyTo identify those needing RRT early To prepare them physically, To prepare them physically,
psychologically and socially for end psychologically and socially for end stage kidney diseasestage kidney disease
To identify the best treatment option To identify the best treatment option for them as an individualfor them as an individual