Embed Size (px)
Citation preview

lable at ScienceDirect
Parkinsonism and Related Disorders 20 (2014) 323e327
Contents lists avai
Parkinsonism and Related Disorders
journal homepage: www.elsevier .com/locate/parkreldis
Short communication
Tremor associated with Klinefelter syndrome e A case series andreview of the literature
Mariella Koegl-Wallner a, Petra Katschnig-Winter a, Tamara Pendl a, Barbara Melisch a,Martin Trummer b, Etienne Holl b, Ulrike Werner a, Reinhold Schmidt a,Petra Schwingenschuh a,*
aDepartment of Neurology, Medical University of Graz, Auenbruggerplatz 22, 8036 Graz, AustriabDepartment of Neurosurgery, Medical University of Graz, Graz, Austria
a r t i c l e i n f o
Article history:Received 4 May 2013Received in revised form25 October 2013Accepted 14 November 2013
Keywords:Klinefelter syndromeEssential tremorDeep brain stimulationDBSTremor analysis
* Corresponding author. Tel.: þ43 316 385 83379.E-mail address: petra.schwingenschuh@medunigr
1353-8020/$ e see front matter � 2013 Elsevier Ltd.http://dx.doi.org/10.1016/j.parkreldis.2013.11.010
a b s t r a c t
Background: Previous case series suggested a link between Klinefelter syndrome (KS) and essentialtremor (ET) or an ET-like syndrome.Methods: We investigated three KS-patients with tremor including tremor-analyzes and discuss our datain context to findings from a literature review. The clinical outcome after deep brain stimulation (DBS) isalso reviewed.Results: Tremor in KS is predominantly a postural and kinetic tremor that resembles ET. Our patientswere further characterized by absent family history for tremor in first degree relatives, lack of subjectivealcohol responsiveness inquired by history, and tremor onset in childhood. One of our patients and twocases from literature improved after DBS of the ventral intermediate nucleus (VIM) of the thalamus.Conclusions: Tremor in KS shares several features with ET. If other characteristics such as family history,alcohol responsiveness, and age at tremor onset may serve as discriminating factors from ET, needs to befurther investigated. First observations suggest that VIM-DBS may be efficacious.
� 2013 Elsevier Ltd. All rights reserved.
1. Introduction
Klinefelter Syndrome (KS) is the most frequent sex chromosomeabnormality among males (1:700) and the most common cause ofmale infertility. Before puberty physical anomalies are discrete.Thereafter the usually tall patients have small firm testes, gyneco-mastia in about 50%, varying symptoms of androgen deficiency, anda characteristic cognitive and behavioral syndrome. Testosteronereplacement therapy should be started as soon as possible [1].
Previous case series suggested a link between KS and essentialtremor (ET) or an ET-like syndrome [2]. A questionnaire-based studyshowed a significantly higher tremor frequency in KS compared tocontrols with onset at a younger age [3]. The pathophysiology of thetremor is unclear. Two cases with marked improvement from deepbrain stimulation (DBS) of the ventral intermediate nucleus (VIM) ofthe thalamus were reported [4,5].
2. Methods
We present three patients with KS (47XXY) and an ET-like tremorsyndrome and a review of the literature. Tremor-analysis was
az.at (P. Schwingenschuh).
All rights reserved.
performed in our patients. The study was approved by the localethics committee and was conducted in accordance with the Decla-ration of Helsinki. All procedures were carried out with the adequateunderstanding and written consent of the subjects involved.
2.1. Tremor-analysis
A triaxial accelerometer transducer was attached to the middlephalanx of the index finger bilaterally. Surface electromyography(EMG) was recorded from wrist flexors and wrist extensors. Tremorwas recorded during rest, posture (500 g loading), and action (fingerenose-testing). Data were analyzed as previously described [6].
3. Results
3.1. Case reports
3.1.1. Patient 1In 2011 this 51-years-old man presented with disabling arm
tremor. Tremor had started at age ten in his arms and head and hadincreased during the past five years resulting in early retirement.The patient reported a positive family history for tremor (maternalgrandfather), exacerbation of tremor by stress, and lack of alcohol

Table 1Tremor characteristics in our patients assessed by accelerometry and surface EMG.
Patient 1 Patient 2(off stim)
Patient 3
Rest right arm Peak frequency (Hz) 5.9 5.9 NATotal power (milliG) 0.46 0.01 NA
Rest left arm Peak frequency (Hz) 6.2 4.9 NATotal power (milliG) 0.13 0.26 NA
Posture right arm Peak frequency (Hz) 6.2 6.2 7.8Total power (milliG) 10.22 1.25 0.04
Posture left arm Peak frequency (Hz) 5.9 5.2 9.8Total power (milliG) 28.50 8.98 0.11
Posture withloading right
Peak frequency (Hz) 6.8 6.5 9.1Total power (milliG) 30.30 3.26 0.07
Posture with loading left
Peak frequency (Hz) 6.2 5,9 9.1Total power (milliG) 55.58 5.20 0.22
Action right arm Peak frequency (Hz) 6.8 7.2 8.5Total power (milliG) 17.11 4.88 0.31
Action left arm Peak frequency (Hz) 6.8 6.2 8.5Total power (milliG) 34.92 15.20 1.58
EMG burst duration Mean � SD(milliseconds)
87 � 2 86 � 2 73�1
Phase-analysis degrees 44 30 133Test battery e
psychogenicversus organictremora
Range 0e10 points 0 1 0
Corresponding peaksin the frequencypower spectraof accelerometryand EMG e
“frequencyinvariantb”with loading
Yes Yes Yes
Hz, hertz; G, gravity; NA, not applicable (no tremor); off stim, deep brain stimulationturned off.
a Test battery (0e10 points): Cut-off score for a diagnosis of laboratory-supportedpsychogenic tremor was defined as �3 out of 10 points [6].
b Frequency invariant with loading: corresponding EMG peak with the accel-erometry power spectrum peak, which does not decrease in frequency bymore than1Hz after loading
M. Koegl-Wallner et al. / Parkinsonism and Related Disorders 20 (2014) 323e327324
responsiveness. At age 14 he had reached a height of 195 cm, therewere no learning difficulties in school, but mild mood instabilityand low self-esteem. Because of infertility, KS was diagnosed at age36, and testosterone replacement therapy was started withouttremor improvement. Propranolol (120 mg/day) had only a tran-sient effect on the tremor, all other drugs including topiramate(100 mg/day), clonazepam (1 mg/day), primidone (250 mg/day),gabapentin (1200 mg/day), and nimodipine had no benefit.
Neurological examination showed mild head and voice tremor,mild intermittent rest tremor of both hands, andmoderate bilateralasymmetric postural and action tremor of the upper limbs (left sidemore affected). He also hadmild postural tremor of both legs. Therewas slight slowness in repetitive finger tapping tasks without truebradykinesia and a pallhypaesthesia in both legs. The neurologicalexamination was otherwise unremarkable (see Video, segment 1).MRI of the brain and DAT-SPECT were normal. Neuropsychologicalassessment revealed an impairment of executive functions andlanguage skills.
Supplementary data related to this article can be found online athttp://dx.doi.org/10.1016/j.parkreldis.2013.11.010.
3.1.2. Patient 2This 29-years-old manwith KS (diagnosed at age 18) was referred
in 2009 because of disabling arm tremor. He was treated withtestosterone which had no effect on the tremor. Tremor had startedin his left arm at age three. During childhood he further developed atremor in the right arm, head, both legs and an intermittent voicetremor. In school he suffered from attention deficit disorder, moodinstability, and short-temperedness. He finished a traineeship aselectrician, but was unable to practice this job due to the tremor.
Family history for tremor was negative, he reported no alcoholresponse and propranolol (30 mg/day, side effects with hypoten-sion and bradycardia), clonazepam (2mg/day), primidone (250mg/day), and topiramate (200 mg/day) were tried without benefit.Clinical examination at age 26 showedmild head and rest tremor ofboth hands, severe asymmetric postural and action tremor of botharms, and mild postural leg tremor.
Brain MRI, F-Dopa-PET, and EEG were normal. Cognitive testingrevealed mild attention deficit and slight deficits in verbal fluency.Because of the disabling arm tremor, DBS of the VIMwas performedin 2009. This led to cessation of the tremor of the right arm andmarked improvement on the left side. Due to skin ulcerationsaround the pacemaker and cranial leads five reoperations werenecessarywithin two years postoperatively. Finally re-implantationand repair by a rotation flap were performed. Since then, stimula-tion significantly improved his tremor without any further com-plications. There was no more head or leg tremor, no tremor of theright upper limb and only a slight postural and action tremor on theleft side. The patient started a traineeship as design draftsman (alsosee Video, segments 2 and 3).
3.1.3. Patient 3This 24-years-old man presented in 2011 to our outpatient
clinic because of bilateral upper limb tremor that had started inchildhood and was aggravated by stress. Tremor was mild butbothersome, also during activities such as writing. KS was diag-nosed in adolescence and testosterone therapy was startedwithout improvement of the tremor. There was no family historyof tremor, no clear alcohol effect, and no anti-tremulous drugshad been tried so far. Neurological examination showed a mildpostural and action tremor of both arms, predominantly on theleft side. There was mild cogwheeling on the left arm, but norigidity and no bradykinesia. Brain MRI and DAT-SPECT werenormal. Propranolol (30 mg/day, side effects with sleepiness) ledto mild reduction of the tremor.
3.2. Tremor-analysis
Patients 1 and 2 had a 5e7 Hz asymmetric tremor during rest,posture, and action. Patient 3 had no rest tremor and a smalleramplitude but higher frequency (8e10 Hz) tremor during postureand action. For further details see Table 1.
3.3. Literature review
An overview of the literature regarding KS patients with tremoris provided in Table 2.
4. Discussion
From a phenomenological point of view, tremor in our patientsand inmost cases from literature was predominantly a postural andkinetic tremor resembling ET. Previous reports had suggested apotential ET-KS association [2], although epidemiological studiesregarding the prevalence of tremor in KS are lacking. A recentquestionnaire-based screening study showed a significant increaseof tremor frequency in KS patients (63%) versus controls (14%) [3].However, if patients with KS and tremor truly suffer from ET or anET-like syndrome remains unknown. We have for the first timeperformed a detailed tremor analysis using accelerometry andsurface EMG, which showed a tremor in concordance, but notspecific for ET. For the first time, we report a normal DAT-SPECT or
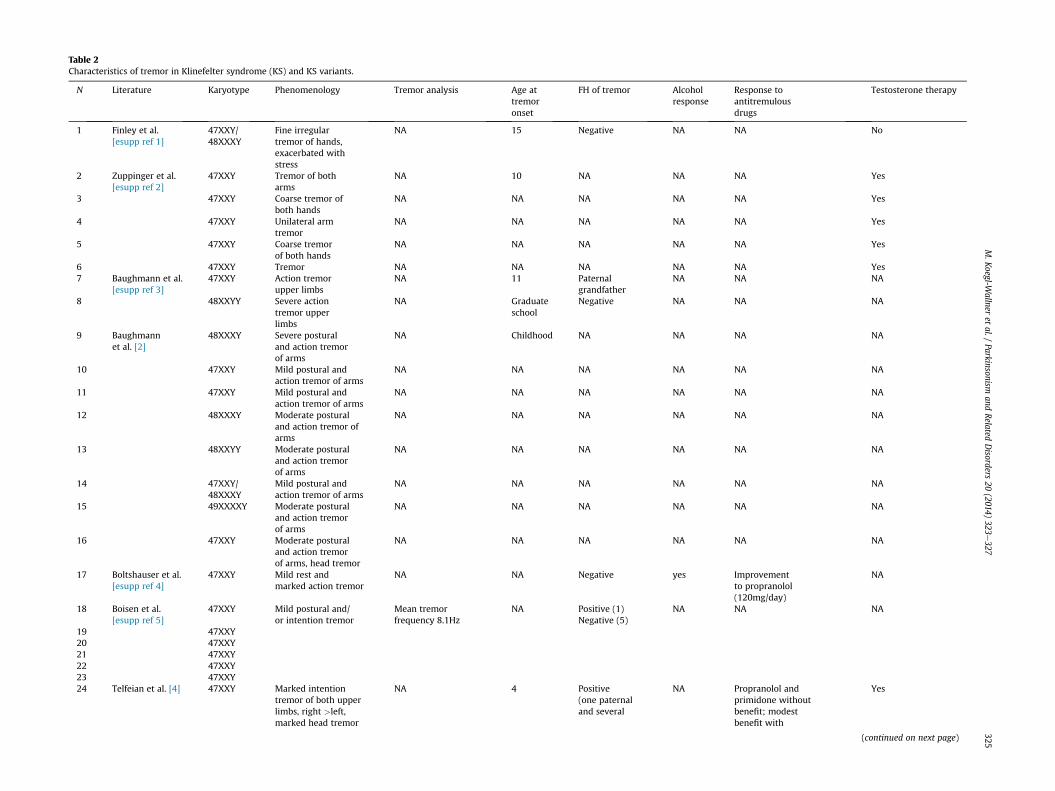
Table 2Characteristics of tremor in Klinefelter syndrome (KS) and KS variants.
N Literature Karyotype Phenomenology Tremor analysis Age attremoronset
FH of tremor Alcoholresponse
Response toantitremulousdrugs
Testosterone therapy
1 Finley et al.[esupp ref 1]
47XXY/48XXXY
Fine irregulartremor of hands,exacerbated withstress
NA 15 Negative NA NA No
2 Zuppinger et al.[esupp ref 2]
47XXY Tremor of botharms
NA 10 NA NA NA Yes
3 47XXY Coarse tremor ofboth hands
NA NA NA NA NA Yes
4 47XXY Unilateral armtremor
NA NA NA NA NA Yes
5 47XXY Coarse tremorof both hands
NA NA NA NA NA Yes
6 47XXY Tremor NA NA NA NA NA Yes7 Baughmann et al.
[esupp ref 3]47XXY Action tremor
upper limbsNA 11 Paternal
grandfatherNA NA NA
8 48XXYY Severe actiontremor upperlimbs
NA Graduateschool
Negative NA NA NA
9 Baughmannet al. [2]
48XXXY Severe posturaland action tremorof arms
NA Childhood NA NA NA NA
10 47XXY Mild postural andaction tremor of arms
NA NA NA NA NA NA
11 47XXY Mild postural andaction tremor of arms
NA NA NA NA NA NA
12 48XXXY Moderate posturaland action tremor ofarms
NA NA NA NA NA NA
13 48XXYY Moderate posturaland action tremorof arms
NA NA NA NA NA NA
14 47XXY/48XXXY
Mild postural andaction tremor of arms
NA NA NA NA NA NA
15 49XXXXY Moderate posturaland action tremorof arms
NA NA NA NA NA NA
16 47XXY Moderate posturaland action tremorof arms, head tremor
NA NA NA NA NA NA
17 Boltshauser et al.[esupp ref 4]
47XXY Mild rest andmarked action tremor
NA NA Negative yes Improvementto propranolol(120mg/day)
NA
18 Boisen et al.[esupp ref 5]
47XXY Mild postural and/or intention tremor
Mean tremorfrequency 8.1Hz
NA Positive (1)Negative (5)
NA NA NA
19 47XXY20 47XXY21 47XXY22 47XXY23 47XXY24 Telfeian et al. [4] 47XXY Marked intention
tremor of both upperlimbs, right >left,marked head tremor
NA 4 Positive(one paternaland several
NA Propranolol andprimidone withoutbenefit; modestbenefit with
Yes
(continued on next page)
M.Koegl-W
allneret
al./Parkinsonism
andRelated
Disorders
20(2014)
323e327
325
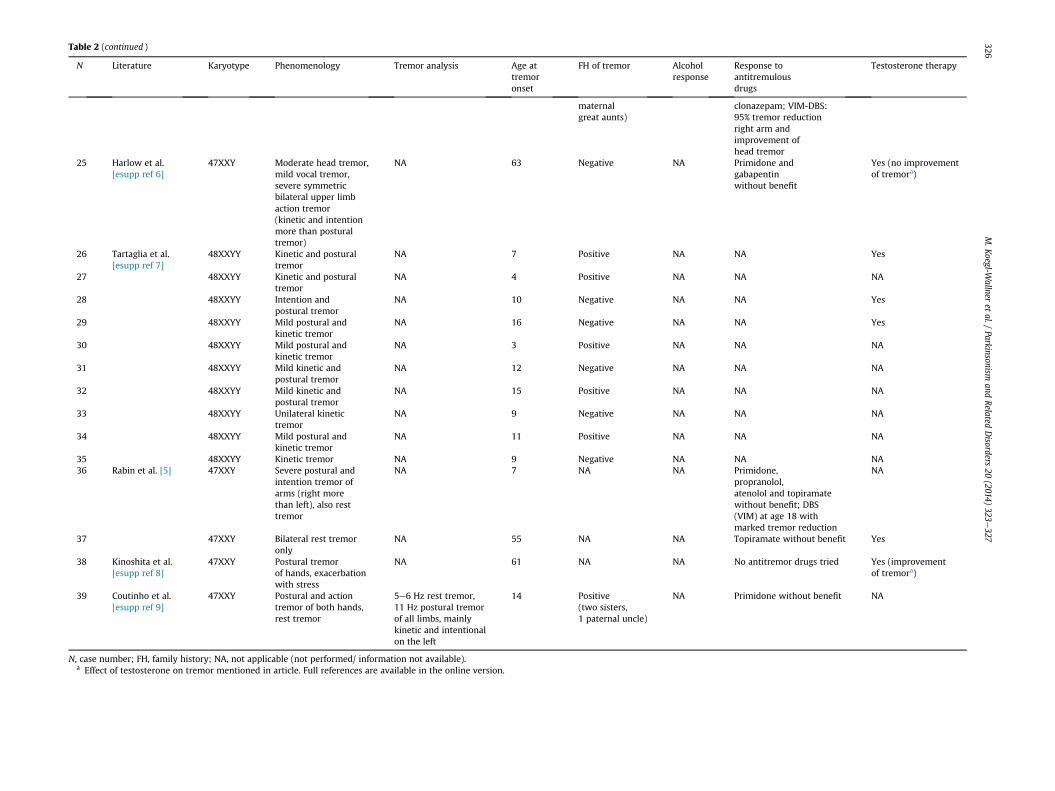
Table 2 (continued )
N Literature Karyotype Phenomenology Tremor analysis Age attremoronset
FH of tremor Alcoholresponse
Response toantitremulousdrugs
Testosterone therapy
maternalgreat aunts)
clonazepam; VIM-DBS:95% tremor reductionright arm andimprovement ofhead tremor
25 Harlow et al.[esupp ref 6]
47XXY Moderate head tremor,mild vocal tremor,severe symmetricbilateral upper limbaction tremor(kinetic and intentionmore than posturaltremor)
NA 63 Negative NA Primidone andgabapentinwithout benefit
Yes (no improvementof tremora)
26 Tartaglia et al.[esupp ref 7]
48XXYY Kinetic and posturaltremor
NA 7 Positive NA NA Yes
27 48XXYY Kinetic and posturaltremor
NA 4 Positive NA NA NA
28 48XXYY Intention andpostural tremor
NA 10 Negative NA NA Yes
29 48XXYY Mild postural andkinetic tremor
NA 16 Negative NA NA Yes
30 48XXYY Mild postural andkinetic tremor
NA 3 Positive NA NA NA
31 48XXYY Mild kinetic andpostural tremor
NA 12 Negative NA NA NA
32 48XXYY Mild kinetic andpostural tremor
NA 15 Positive NA NA NA
33 48XXYY Unilateral kinetictremor
NA 9 Negative NA NA NA
34 48XXYY Mild postural andkinetic tremor
NA 11 Positive NA NA NA
35 48XXYY Kinetic tremor NA 9 Negative NA NA NA36 Rabin et al. [5] 47XXY Severe postural and
intention tremor ofarms (right morethan left), also resttremor
NA 7 NA NA Primidone,propranolol,atenolol and topiramatewithout benefit; DBS(VIM) at age 18 withmarked tremor reduction
NA
37 47XXY Bilateral rest tremoronly
NA 55 NA NA Topiramate without benefit Yes
38 Kinoshita et al.[esupp ref 8]
47XXY Postural tremorof hands, exacerbationwith stress
NA 61 NA NA No antitremor drugs tried Yes (improvementof tremora)
39 Coutinho et al.[esupp ref 9]
47XXY Postural and actiontremor of both hands,rest tremor
5e6 Hz rest tremor,11 Hz postural tremorof all limbs, mainlykinetic and intentionalon the left
14 Positive(two sisters,1 paternal uncle)
NA Primidone without benefit NA
N, case number; FH, family history; NA, not applicable (not performed/ information not available).a Effect of testosterone on tremor mentioned in article. Full references are available in the online version.
M.Koegl-W
allneret
al./Parkinsonism
andRelated
Disorders
20(2014)
323e327
326

M. Koegl-Wallner et al. / Parkinsonism and Related Disorders 20 (2014) 323e327 327
F-DOPA-PET in all three patients, supporting the integrity of thenigrostriatal system in this disorder.
Furthermore we have reported other characteristics relevant inpatients with tremor such as alcohol responsiveness, family history,age at tremor onset, and treatment response. Unfortunately thesedata are lacking in most previous reports. ET shows a positiveresponse to alcohol in two thirds of patients [7]. None of our pa-tients reported a positive alcohol effect. No conclusions regardingalcohol responsiveness can be drawn from the literature review,since this was documented on for one case only (as positive). Only1/3 patients reported here (maternal grandfather) and 9/39 pa-tients from literature had a positive family history for tremor, whilethis is reported in up to 80% of young onset cases with ET [8]. Whilea bimodal age at onset (2nd and 6th decade) has been reported forET by some authors [7], others have suggested a mean age of onsetof 15 years or 40 years in familial, and 50 years in sporadic cases [9].In contrast, 18/21 cases from the literature, in which the relevantinformation was available, had a tremor onset in childhood oradolescence, and only three cases had tremor onset after the age of50 years. All our patients reported tremor onset in childhood.
Two of our three patients had a rest tremor in addition to apostural and kinetic tremor, with the rest tremor component hav-ing the smallest amplitude (see Table 2). Although rest tremor in ETis a controversial issue and some authors have raised the question ifET patients with rest tremor rather have a dystonic tremor even inthe absence of overt dystonia [10], most authors accept ET with resttremor as an ET subtype occurring in 14e18% of patients [11].Therefore the presence of a rest tremor in patients with KS doesneither support nor refute its link to ET.
Propranolol and Primidone are estimated to be effective in 30e70% of ET patients [12]. Regarding treatment response in KS-associated tremor, patient 1 reported only a transient benefitfrom propranolol (120 mg/day) and patient 3 (30 mg/day) showedonly mild benefit. According to medical records, all other drugstried in our patients had no effect e at least at the maximumprescribed and tolerated dosage. Drugs tried for tremor are onlydocumented in 6/39 cases from literature, with one patientshowing a benefit to propranolol and one to clonazepam. None ofour patients noted a tremor reduction with testosterone. Responseto oral drug treatment remains inconclusive, since the dosage triedwas not appropriate in some cases and length of treatment andobjective evaluation of the improvement is not available.
Patient 2 underwent VIM-DBS with marked objective tremorreduction. However, recurrent device-related skin ulcerationsmade reoperation necessary five times. Two KS patients reported inthe literature underwent VIM-DBS and showed marked tremorreduction [4,5]. Postoperative complications are not reported.
Further studies in a larger patient cohort are warranted toinvestigate if alcohol responsiveness, family history, and age attremor onset differ between ET and KS-associated tremor.
Among patients with other diagnoses, skin erosions/ulcerationsaround the DBS-impulse generator, burr hole cap, and along thecourse of the cables occur in up to 24.7% [13] typically caused byunderlying pressure from the leads against the skin or leadmigration. Up to 13% of KS patients suffer from wound healingdisorders and leg ulcers, often without a history of chronic venousinsufficiency or deep venous thrombosis, possibly related to ahigher plasma level of plasminogen activator inhibitor-1 (PAI-1)
(PAI-1 was not assessed in patient 2) [14]. If KS itself represents arisk factor for DBS-related skin complications needs to be evaluatedin future studies.
In conclusion, we confirm that tremor in KS clinically andelectrophysiologically resembles ET. If other characteristics such asfamily history, alcohol responsiveness, and age at tremor onset mayserve as discriminating factors from ET, needs to be further inves-tigated. VIM-DBS was effective in one patient reported here and intwo patients reported in literature andmay therefore be consideredas a treatment option in KS patients with severe disabling armtremor.
Conflicts of interest
The authors declare that they have no conflict of interest relatedto this study.
Acknowledgments
The authors thank Dr. Barbara Pendl for referral of patients andthank all patients for their contribution to this research.
Appendix A. Supplementary data
Supplementary data related to this article can be found at http://dx.doi.org/10.1016/j.parkreldis.2013.11.010.
References
[1] Lanfranco F, Kamischke A, Zitzmann M, Nieschlag E. Klinefelter’s syndrome.Lancet 2004;364:273e83.
[2] Baughman Jr FA, Higgins JV, Mann JD. Sex chromosome anomalies andessential tremor. Neurology 1973;23:623e5.
[3] Harlow TL, Gonzalez-Alegre P. High prevalence of reported tremor in Kline-felter syndrome. Parkinsonism Relat Disord 2009;15:393e5.
[4] Telfeian AE, Boockvar JA, Simuni T, Jaggi J, Skolnick B, Baltuch GH. Efficacy ofunilateral deep brain stimulation of the thalamic ventralis intermedius nu-cleus in a patient with bipolar disorder associated with Klinefelter syndromeand essential tremor. Case report. J Neurosurg 2000;93:127e8.
[5] Rabin ML, Moghimi N, Jabbari B. Tremor and Klinefelter’s syndrome. MovDisord 2011;26:S381.
[6] Schwingenschuh P, Katschnig P, Seiler S, Saifee TA, Aguirregomozcorta M,Cordivari C, et al. Moving toward “laboratory-supported” criteria for psy-chogenic tremor. Mov Disord 2011;26:2509e15.
[7] Lou JS, Jankovic J. Essential tremor: clinical correlates in 350 patients.Neurology 1991;41:234e8.
[8] Deng H, Le W, Jankovic J. Genetics of essential tremor. Brain 2007;130:1456e64.
[9] Koller WC, Busenbark K, Miner K. The relationship of essential tremor to othermovement disorders: report on 678 patients. Essential Tremor Study Group.Ann Neurol 1994;35:717e23.
[10] Nistico R, Pirritano D, Novellino F, Salsone M, Morelli M, Valentino P, et al.Blink reflex recovery cycle in patients with essential tremor associated withrest tremor. Neurology 2012;79(14):1490e5.
[11] Whaley NR, Jd Putzke, Baba Y, Wszolek ZK, Uitti RJ. Essential tremor:phenotypic expression in a clinical cohort. Parkinsoism Relat Disord 2007;13:333e9.
[12] Benito-Leon j, Louis ED. Update on essential tremor. Minerva Med 2011;102:417e40.
[13] Sixel-Doring F, Trenkwalder C, Kappus C, Hellwig D. Skin complications indeep brain stimulation for Parkinson’s disease: frequency, time course, andrisk factors. Acta Neurochir (Wien) 2010;152:195e200.
[14] Zollner TM, Veraart JC, Wolter M, Hesse S, Villemur B, Wenke A, et al. Legulcers in Klinefelter’s syndromeefurther evidence for an involvement ofplasminogen activator inhibitor-1. Br J Dermatol 1997;136:341e4.