Embed Size (px)
Citation preview

Emily Wasco, Tufts Medical Student 4th yearGillian Lieberman MD
Tuboovarian AbscessTuboovarian Abscess
Emily C. Wasco, Tufts Medical School 4th yearGillian Lieberman MD
Advanced Radiology ClerkshipBeth Israel Deaconess Medical Center
October 17, 2003

2
Emily Wasco, Tufts Medical Student 4th yearGillian Lieberman MD
PatientPatient
• 61 year-old female with vague lower abdominal pain, constipation, intermittent nausea and vomiting for 10 days.
• PMH: significant only for tubal ligation at age 35

3
Emily Wasco, Tufts Medical Student 4th yearGillian Lieberman MD
PatientPatient
• PE significant for palpable 5 cm right adnexal mass, soft, non-tender. No guarding or rebound.
• Labs significant only for WBC 16.7
• Diagnostic tests performed showed a right tuboovarian abscess

Emily Wasco, Tufts Medical Student 4th yearGillian Lieberman MD
Next, a differential diagnosis to keep in mind when choosing imaging….
Next, a differential diagnosis to keep in mind when choosing imaging….

5
Emily Wasco, Tufts Medical Student 4th yearGillian Lieberman MD
Differential DiagnosisDifferential Diagnosis
• Ectopic pregnancy• Pelvic neoplasm• Endometrioma• Ovarian torsion• Hemorrhagic cyst• Ovarian hematoma• Appendiceal and diverticular abscesses• Tuboovarian abscess

6
Emily Wasco, Tufts Medical Student 4th yearGillian Lieberman MD
Definition and EpidemiologyDefinition and Epidemiology
• Tuboovarian abscess (TOA): Abscess involving the ovary or fallopian tube
• Tuboovarian complex (TOC): Edematous, dilated infected pelvic structures without abscess formation, vague margins
• Pyosalpinx: infected fallopian tube
• Incidence 100,000/year• Women 20-40, peak 20-24

7
Emily Wasco, Tufts Medical Student 4th yearGillian Lieberman MD
Anatomy that may be involved in TOA
Anatomy that may be involved in TOA
http://www.infertilitypa.com/images/pelvic.jpgUterosacral ligament
Broadligament
Ampulla
Mesosalpinx
Ovarianligament

8
Emily Wasco, Tufts Medical Student 4th yearGillian Lieberman MD
Causes of TOACauses of TOA
• Pelvic inflammatory disease (PID)• IUD (older devices, Dalkon Shield)• Pelvic surgery• Intra-abdominal processes/infections• Infertility treatments
– Ovarian hyperstimulation– Oocyte retrieval

9
Emily Wasco, Tufts Medical Student 4th yearGillian Lieberman MD
PID and TOAPID and TOA
• Virtually all cases of primary TOA• TOA is most severe/late form of PID• 1/3 hospitalized with PID, 15% of PID• Reproductive tract flora migrates into pelvic
peritoneal cavity, endometritis salpingitis• Tissue damage, surfaces adhere and form a
closed space• Bowel, ovary, fallopian tube, peritoneum,
uterus and omentum can be involved• Perfusion is compromised, anaerobes flourish

10
Emily Wasco, Tufts Medical Student 4th yearGillian Lieberman MD
Intra-abdominal processIntra-abdominal process
• Any cause of bowel perforation adjacent to adnexa can lead to TOA– Appendicitis – Diverticulitis
• Intraperitoneal spread of infection with abscess formation as described with PID

11
Emily Wasco, Tufts Medical Student 4th yearGillian Lieberman MD
PathogensPathogens
• Polymicrobial– Strep species– E. Coli– Other gram negatives
enterics– Gonococci and
Chlamydia common in PID but rare in TOA
• Anaerobes– Bacteroides– Prevotella– Peptostreptococcus

12
Emily Wasco, Tufts Medical Student 4th yearGillian Lieberman MD
Signs and SymptomsSigns and Symptoms
• 90% abdominal/pelvic pain• 60-80% fever/leukocytosis• 80-90% Palpable mass • Findings of ileus are common, TOA can
lead to bowel obstruction (distension, decreased bowel sounds)

Emily Wasco, Tufts Medical Student 4th yearGillian Lieberman MD
Moving on to imaging: Case images and description of
when to use ultrasound, CT, and MRI for TOA
Moving on to imaging: Case images and description of
when to use ultrasound, CT, and MRI for TOA

14
Emily Wasco, Tufts Medical Student 4th yearGillian Lieberman MD
UltrasoundUltrasound
• Test of choice for suspected TOA• Transvaginal is best for visualizing
adnexa• Differentiates between TOA and TOC• Sensitivity 82%, specificity 91%• Increased availability, tolerability,
speed and decreased cost (compared with CT, MRI)
• Ultrasound guided drainage

15
Emily Wasco, Tufts Medical Student 4th yearGillian Lieberman MD
Ultrasound TOAUltrasound TOA
• Complex cystic, thick walled, well-defined mass/contiguous masses in adnexa or retrouterine
• Usually hypoechoic• Can be multiloculated
with septations or solid components leading to varied echotexture
• Air fluid levels• Free fluid• Indistinct uterine
marginsKaakaji et al, “Sonography of Obstetric and Gynecological Emergencies,” AJR 2000, 174:651

16
Emily Wasco, Tufts Medical Student 4th yearGillian Lieberman MD
Ultrasound TOAUltrasound TOA
Kaakaji et al, “Sonography of Obstetric and Gynecological Emergencies,” AJR 2000, 174:651
Right Adnexa
Left Adnexa
Uterus

17
Emily Wasco, Tufts Medical Student 4th yearGillian Lieberman MD
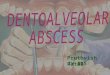
Ultrasound TOCUltrasound TOC
• Dilated fallopian tubes
• Echogenic Fluid (pyosalpinx)
• Enlarged, hyperemic ovary (oophoritis) can be seen with ultrasound but not shown here
Kaakaji et al, “Sonography of Obstetric and Gynecological Emergencies,” AJR 2000, 174:651

18
Emily Wasco, Tufts Medical Student 4th yearGillian Lieberman MD
Ultrasound of PatientUltrasound of Patient
• Complex, hypoechoic cystic mass predominately containing fluid and debris
• 5.0 x 5.4 x 6.7 cm• Slight peripheral
Doppler color flow onlyBIDMC PACS

19
Emily Wasco, Tufts Medical Student 4th yearGillian Lieberman MD
Computed TomographyComputed Tomography
• Adjunct to ultrasound if atypical, unresponsive to therapy or differential is large
• CT recommended to evaluate for full range of collections if free fluid/peritonitis
• Look for abscess in adnexa– Thick walled, fluid density (low attenuation mass)– Internal septations common– Internal gas bubbles– Loss of definition of uterine wall– Thickened uterosacral ligaments/increased density of
presacral and perirectal fat– Hydronephrosis if ureters involved– Para-aortic LAD

20
Emily Wasco, Tufts Medical Student 4th yearGillian Lieberman MD
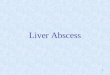
CT of PatientCT of Patient• Contrast enhanced
CT Abd/Pelvis• 5.0 x 5.2 cm right
adnexal fluid collection, closely associated with uterus and broad ligament
• Heterogeneously enhancing rim
• Indistinct uterine margins
BIDMC PACS
Fluid Collection (TOA)
Surrounding inflammation,Indistinct uterine borders

21
Emily Wasco, Tufts Medical Student 4th yearGillian Lieberman MD
CT of PatientCT of Patient
• Non-dependent gas• Compressed loop of
small bowel• Appendix visualized
with no evidence of inflammation
• No diverticulitis• Consistent with TOA
BIDMC PACS

22
Emily Wasco, Tufts Medical Student 4th yearGillian Lieberman MD
CT of Patient: Reconstructions CT of Patient:
Reconstructions
BIDMC PACS
TOA
BIDMC PACS

23
Emily Wasco, Tufts Medical Student 4th yearGillian Lieberman MD
Magnetic Resonance ImagingMagnetic Resonance Imaging
• MRI also accurate at diagnosing PID, however not well studied
• Good soft tissue contrast between pelvic organs
• Visualize fluid filled tubes, abscesses, and smaller amounts of free fluid than ultrasound
• Abscess with low intensity on T1 and high on T2 and thick, irregular walls
• Not first line for evaluation of pelvic masses• Cost, time

24
Emily Wasco, Tufts Medical Student 4th yearGillian Lieberman MD
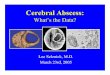
Magnetic Resonance ImagingMagnetic Resonance Imaging
T1 T2
Tukeva et al, “MR Imaging in Pelvic Inflammatory Disease: Comparison with laparoscopy and ultrasound,” Radiology 1999, 210:209

Emily Wasco, Tufts Medical Student 4th yearGillian Lieberman MD
Now that we have seen how to diagnose TOA, what are
the treatment options?
Now that we have seen how to diagnose TOA, what are
the treatment options?

26
Emily Wasco, Tufts Medical Student 4th yearGillian Lieberman MD
TreatmentTreatment
• No standard of care
• Medical: Inpatient 10 day trial of IV broad spectrum antibiotics with anaerobic coverage, especially if young, stable. – Watch for sepsis– If condition does not improve in 2-3 days,
further intervention warranted– Mass may take up to 6 months to resolve

27
Emily Wasco, Tufts Medical Student 4th yearGillian Lieberman MD
Radiologic DrainageRadiologic Drainage
• Ultrasound guided drainage: 80-85% effective– Transcutaneous is standard– Transvaginal with endovaginal sonographic can be
more direct if abscess better visualized, but can be painful if PID or prepubescent
– Transgluteal, transrectal can be chosen depending on location of abscess
– Drainage catheter placement or needle aspiration– Avoids risks associated with general anesthesia and
surgery– Minimally invasive

28
Emily Wasco, Tufts Medical Student 4th yearGillian Lieberman MD
Radiologic DrainageRadiologic Drainage
• Drainage catheter placed in adnexal mass in woman with PID
Lee et al, “Single-step transvaginal aspiration and drainage for suspected pelvic abscesses refractory to antibiotic therapy,” J Ultrasound Med 2002, 21:731

29
Emily Wasco, Tufts Medical Student 4th yearGillian Lieberman MD
Surgical DrainageSurgical Drainage
• Laparoscopic drainage: 90-95% effective• Laparotomy:
– Often used if diagnosis of TOA versus perforated viscus unclear
– increased in women over childbearing age – unstable/septic – rupture of TOA– Resection of all infected organs (hysterectomy,
salpingo-oophorectomy), assess for metastatic abscesses
– Drawbacks include loss of future fertility and endogenous estrogen if premenopausal

30
Emily Wasco, Tufts Medical Student 4th yearGillian Lieberman MD
TOA RisksTOA Risks
• If left untreated, TOA associated with: – increased morbidity from rupture and
peritonitis– chronic pelvic pain– adhesion formation– ectopic pregnancy– impaired future fertility

31
Emily Wasco, Tufts Medical Student 4th yearGillian Lieberman MD
PatientPatient
• Patient did not improve on antibiotics so exploratory laparotomy with abscess drainage was performed.
• Tip of appendix adherent to superior aspect of mass, question of small appendiceal tear but no frank appendicitis
• Diagnosis: TOA from prior episode of undiagnosed appendicitis

32
Emily Wasco, Tufts Medical Student 4th yearGillian Lieberman MD
ConclusionsConclusions
• TOA is an abscess of the adnexa, caused most often by PID, but also from instrumentation and GI tract infections
• Diagnostic imaging first line is transvaginal sonography, with CT and MRI offering additional detail in complicated or unclear cases
• Serious condition which must be treated due to avoid known sequelae
• Treatment includes medical, radiologic and surgical options

33
Emily Wasco, Tufts Medical Student 4th yearGillian Lieberman MD
• Ginsburg et al, “Tuboovarian abscess: A retrospective review,” Am J Obstet Gynecol 1980, 138: 1055.
• Sweet et al, “Pelvic infection and abscess, in Infectious Diseases of the Female Genital Tract,” Williams and Wilkins, Baltimore, 1990: 90.
• Wiesenfeld et al, “Progress in the management of tuboovarian abscesses,” Clin Obstet Gynecol 1993, 36: 433.
• Burkman et al, “Intrauterine devices and pelvic inflammatory disease: evolving perspectives on the data,” Obstet Gynecol Survey 1996, 51: s35
• Moir et al, “Role of ultrasound, gallium scannin and CT in the diagnosis of intra- abdominal abscess,” Am J Surg 1982, 143:582.
• Reed et al, “Antibiotic treatment of tuboovarian abscess,” Am J Obstet Gynecol, 1991, 164:1556.
• Nelson et al, “Endovaginal ultrasonographically guided transvaginal drainage of pelvic abscess,” Am J Obstet 1995, 172:1926.
• Casola et al, “Percutaneous drainage of tuboovarian abscesses,” Radiology 1992, 182: 399.
• Caspi et al, “Sonographically guided aspiration: an alternative therapy for tuboovarian abscess,” Ultrasound Obstet Gynecol 1996, 7:439.
• Van Sonnenberg et al, “US-guided transvaginal aspiration of pelvic abscesses and fluid collections,” Radiology 1991, 181:53.
ReferencesReferences

34
Emily Wasco, Tufts Medical Student 4th yearGillian Lieberman MD
ReferencesReferences• Shulman et al, “Percutaneous catheter drainage of tuboovarian abscess,” Obstet
Gynecol, 1992, 80:55.• Teisala et al, “Transvaginal ultrasound in the diagnosis and treatment of
tuboovarian abscess.” Br J Obstet Gynaecol 1990, 97:178.• Reich et al, “Laparoscopic treatment of tuboovarian and pelvic abscess,” J
Reprod Med 1987, 32_747. • Kaakaji et al, “Sonography of Obstetric and Gynecological Emergencies,” AJR
2000, 174:651.• Varghese et al, “Transvaginal Catheter drainage of tuboovarian abscess using
the trocar method,” AJR 2001, 177:139.• Lee et al, “Single-step transvaginal aspiration and drainage for suspected pelvic
abscesses refractory to antibiotic therapy,” J Ultrasound Med 2002, 21:731.• Wilbur et al, “CT findings in Tuboovarian Abscess,” AJR 1992, 158:575.• www.eMedicine.com, “Pelvic Inflammatory Disease/Tubo-ovarian Abscess,”
November 2002.• Tukeva et al, “MR Imaging in Pelvic Inflammatory Disease: Comparison with
laparoscopy and ultrasound,” Radiology 1999, 210:209.• Bennet et al, “Gynecologic Causes of Acute Pelvic Pain: Spectrum of CT
Findings,” Radiographics 2002, 22:785.• http://www.infertilitypa.com/images/pelvic.jpg

35
Emily Wasco, Tufts Medical Student 4th yearGillian Lieberman MD
AcknowledgementsAcknowledgements
• Staff, Residents and Fellows, BIDMC• Gillian Lieberman, MD• Larry Barbaras, webmaster• Pamela Lepkowski