Embed Size (px)
Citation preview

Romanian Journal of Morphology and Embryology 2005, 46(3):211–223
Tumoral stroma of salivary pleomorphic adenoma – histopathological, histochemical and
immunohistochemical study CL. MĂRGĂRITESCU1), M. RAICA2), CRISTIANA SIMIONESCU1), L. MOGOANTĂ3),
M. SURPĂŢEANU4), F. JAUBERT5), FL. BOGDAN6)
1)Department of Pathology, Emergency County Hospital, University of Medicine and Pharmacy of Craiova
2)Department of Cytology and Histology, “Victor Babeş” University of Medicine and Pharmacy, Timişoara
3)Department of Histology, University of Medicine and Pharmacy of Craiova 4)Department of Oral Maxilla Facial Surgery, Emergency County Hospital,
University of Medicine and Pharmacy of Craiova 5)Department of Pathology, “René Descartes” University Paris V, Faculty of Medicine, “Necker Enfants Malades” Hospital, France
6)Research Centre for Microscopic Morphology and Immunology, University of Medicine and Pharmacy of Craiova
Abstract The aims of our paper were to establish the main histopathological, histochemical and immunohistochemical aspects of tumoral stroma from salivary pleomorphic adenomas. For this purpose we investigated 103 cases by the classical histopathological technique with paraffin embedding and staining with Hematoxylin–Eosin (HE), Hematoxylin–Eosin–Safranin (HES), trichromic Masson, trichromic Goldner Szeckelly, orcein and Periodic Acid Schiff–Blue Alcian (PAS–AA). Immunohistochemically, they were investigated for AE1–AE3, MNF116, CK8, EMA, vimentin, α-actin calponin, S-100, GFAP, collagen IV, and PCNA. The results of our study suggest the key role of neoplastic myoepithelial cell in the achievement of diverse morphological aspects of stroma in such neoplasms. Keywords: pleomorphic adenoma, tumoral stroma, histochemistry, immunohistochemistry.
Introduction
The salivary gland pleomorphic adenoma is a benign epithelial neoplasm, histologically characterized by a great diversity of morphological aspects. It is the most common neoplasm of salivary gland origin; its incidence varies in different statistics from 45% to 74% of all the salivary gland tumors [1–4].
At the Armed Forces Institute of Pathology (AFIP) the pleomorphic adenomas represent 60 % of the benign tumors from all the salivary gland sites: 61% of the major gland tumors and 54% of the minor gland tumors [5].
Its structural pleomorphism is given both by the epithelial component, as a result of the cytological differentiations and the growing patterns, and by the stromal component because of its rich morphological and quantitative diversity [5, 6].
Pleomorphic adenoma is thinly encapsulated. Prominently myxoid tumors often have incomplete capsules, and tumor tissue is juxtaposed against normal gland. This is characteristic of pleomorphic adenoma in the minor glands, where a capsule is rarely well developed.
Extracellular stroma is one of the defining components of pleomorphic adenoma, ranging from scanty to abundant. According to the relative proportion of stroma and cellular components Seifert subclassified pleomorphic adenoma into four types: type I (stroma
comprises 30–50% of the tumor), type II (stroma comprises ~80% of the tumor), type III (stroma comprises ~20–50% of the tumor) and type IV (stroma attains similar proportion to that of type III, but there is focal monomorphic differentiation in the epithelial component) [3].
The stroma of these tumors may have diverse appearance: myxoid, chondroid, chondro-myxoid, hyaline, fibrous, sclero-hyaline and, very rarely, osseous and adipose. These aspects are usually associated with the predominance of one of them in variable proportion [5–10].
The pathognomonic stromal feature of pleomorphic adenoma is the presence of chondro-myxoid stroma. Most pleomorphic adenomas, particularly the long-standing lesions present variable amounts of elastic fibers, which are uncommon in other salivary gland tumors [11, 12].
Crystalloids composed of collagenous substance; tyrosine and oxalate are more often present in pleomorphic adenoma than in any other salivary gland neoplasm: their incidence varies from 1.5 to 21% [13–16].
Material and methods
Our study comprised 103 cases of pleomorphic adenomas selected during 10 years, from 1992 until 2001.
Cl. Mărgăritescu et al.
212
The surgical specimens were provided by the Oral Maxilla Facial Surgery Department of the Emergency County Hospital Craiova, mostly from 15–76 year-old females (65 cases), with prevalent parotid localization (77 cases).
The surgical specimens were routinely fixed with 10% buffered formalin and sent to the Laboratory of Cytology and Pathology of the same hospital. They were processed by the classical histopathological technique with paraffin embedding and stained with Hematoxylin–Eosin (HE), Hematoxylin–Eosin–Safranin (HES), trichromic Masson, trichromic Goldner Szeckelly, orcein and Periodic Acid Schiff–Blue Alcian (PAS–AA).
The immunohistochemical process was made in the Histological, Histopathological and Immuno-histochemical Techniques Laboratory from “Victor Babeş” University of Medicine and Pharmacy Timişoara, Department of Cytology and Pathology of the Hospital “Necker Enfants Malades” from Paris and in the Histological, Histopathological and Immuno-histochemical Techniques Laboratory from University of Medicine and Pharmacy of Craiova.
We use DAKO LSAB® 2 System, HRP technique for AE1–AE3, MNF116, CK8, EMA, vimentin, α-actin and S-100, and ABC/HRP technique for calponin, GFAP, collagen IV, and PCNA.
The tumors have been diagnosed according to WHO classification [17].
In most cases was made an internal control (a positive reaction of the fragments that were placed at a suitable distance away from the tumoral tissue).
As in immunohistochemistry there is no standard or universal accepted methods to select the histological fields in order to interpret the results (with the exception of PCNA) we used the criteria from literature data [18].
The intensity of the immunostaining reaction has been described as follows:
▪ (+++), when the immunostaining reaction is intense positive or ”all over” specific distributed, obvious at small magnification;
▪ (++), when the immunostaining reaction is focal or with moderate intensity, evident on average magnification;
▪ (+), when the immunostaining reaction is weak or very focal, visible only at strong magnification;
▪ (±), when the immunostaining reaction is very reduced, to limit;
▪ (−), when the immunostaining reaction is negative.
Results
Epidemiological aspect There were selected 103 pleomorphic adenomas
cases from 283 salivary gland lesions, diagnosed during 1992–2001.
In our study the mean age at presentation was 48 years, but the age ranges from the second to eight decades. The patients were mostly females (65 cases,
representing 63.1%), with a female to male ratio of 1.71 to 1.
The tumors developed especially in the major salivary glands (76 cases in the parotid, 16 cases in the submandibular glands and two cases in the sublingual gland, all representing about 92% of our casuistry).
The parotid was the most frequently involved gland (74%). The minor salivary glands were involved in eight cases at the level of the lower lip (three cases), oral mucosa (two cases) and palatine mucosa (three cases).
Histopathological, histochemical and immunohistochemical aspects of pleomorphic adenomas investigations
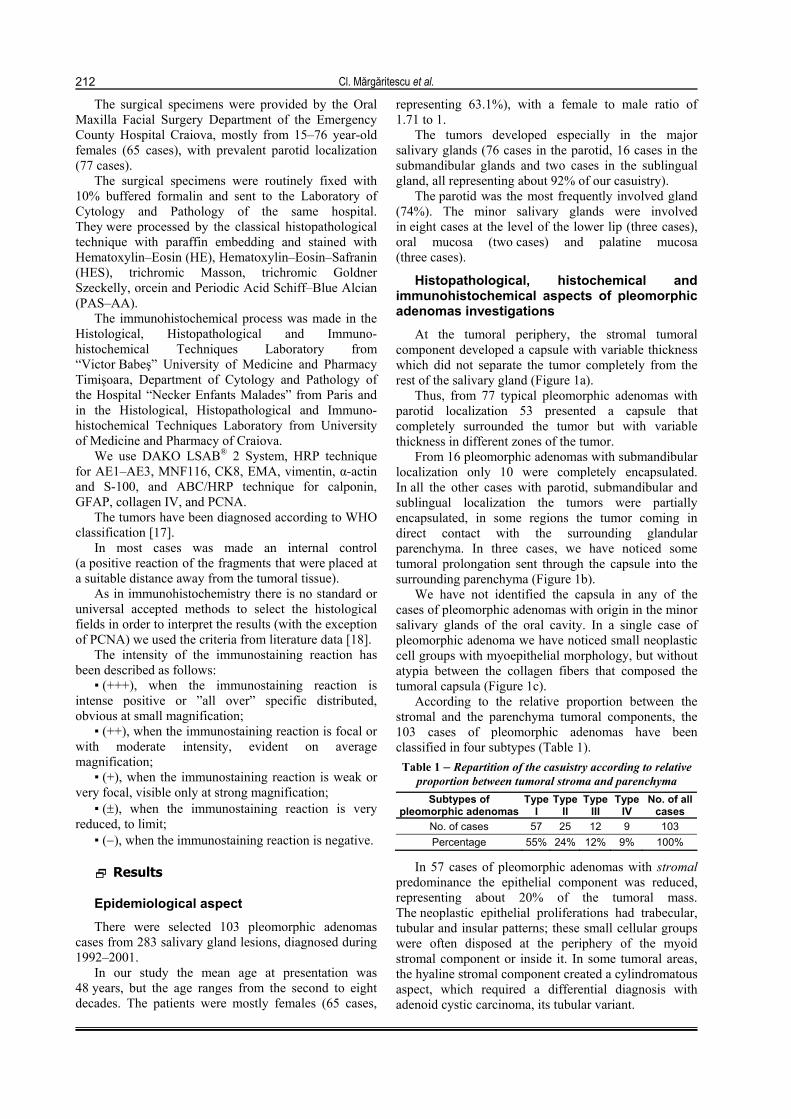
At the tumoral periphery, the stromal tumoral component developed a capsule with variable thickness which did not separate the tumor completely from the rest of the salivary gland (Figure 1a).
Thus, from 77 typical pleomorphic adenomas with parotid localization 53 presented a capsule that completely surrounded the tumor but with variable thickness in different zones of the tumor.
From 16 pleomorphic adenomas with submandibular localization only 10 were completely encapsulated. In all the other cases with parotid, submandibular and sublingual localization the tumors were partially encapsulated, in some regions the tumor coming in direct contact with the surrounding glandular parenchyma. In three cases, we have noticed some tumoral prolongation sent through the capsule into the surrounding parenchyma (Figure 1b).
We have not identified the capsula in any of the cases of pleomorphic adenomas with origin in the minor salivary glands of the oral cavity. In a single case of pleomorphic adenoma we have noticed small neoplastic cell groups with myoepithelial morphology, but without atypia between the collagen fibers that composed the tumoral capsula (Figure 1c).
According to the relative proportion between the stromal and the parenchyma tumoral components, the 103 cases of pleomorphic adenomas have been classified in four subtypes (Table 1). Table 1 – Repartition of the casuistry according to relative
proportion between tumoral stroma and parenchyma Subtypes of
pleomorphic adenomasType
I Type
II Type
III Type
IV No. of all
cases No. of cases 57 25 12 9 103 Percentage 55% 24% 12% 9% 100%
In 57 cases of pleomorphic adenomas with stromal predominance the epithelial component was reduced, representing about 20% of the tumoral mass. The neoplastic epithelial proliferations had trabecular, tubular and insular patterns; these small cellular groups were often disposed at the periphery of the myoid stromal component or inside it. In some tumoral areas, the hyaline stromal component created a cylindromatous aspect, which required a differential diagnosis with adenoid cystic carcinoma, its tubular variant.
Tumoral stroma of salivary pleomorphic adenoma – histopathological, histochemical and immunohistochemical study 213
Figure 1 – Typical pleomorphic adenoma: (a) type I – capsula (trichromic Masson staining, ×40); (b) type II – tumoralcapsula traversed by a tumoral prolongation (HE staining, ×40); (c) type I – presence of small groups of neoplastic cellinto the tumoral capsula (HE staining, ×40); (d) type I – scan image of the histopathological specimen (HES staining);
(e) type II – scan image of the histopathological specimen (HES staining); (f) type III – scan image of thehistopathological specimen (HES staining)
(e)
(a)
(f)
(d)(c)
(b)
214 Cl. Mãrgãritescu et al.
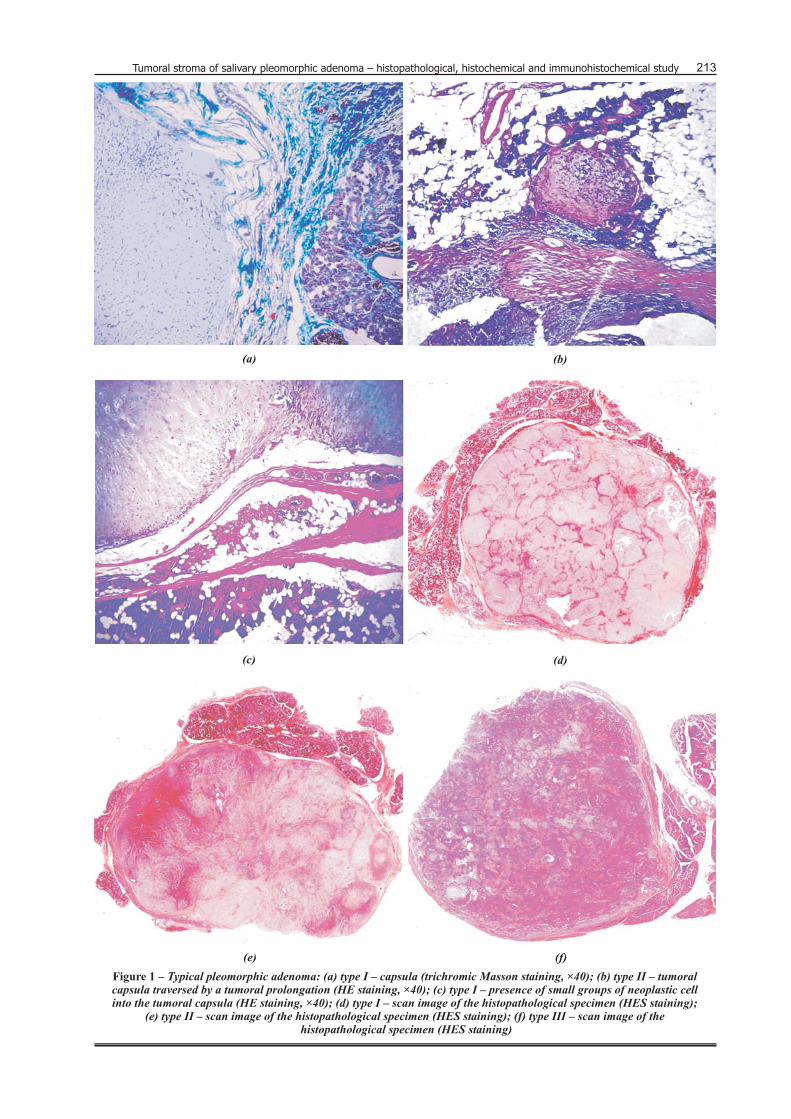
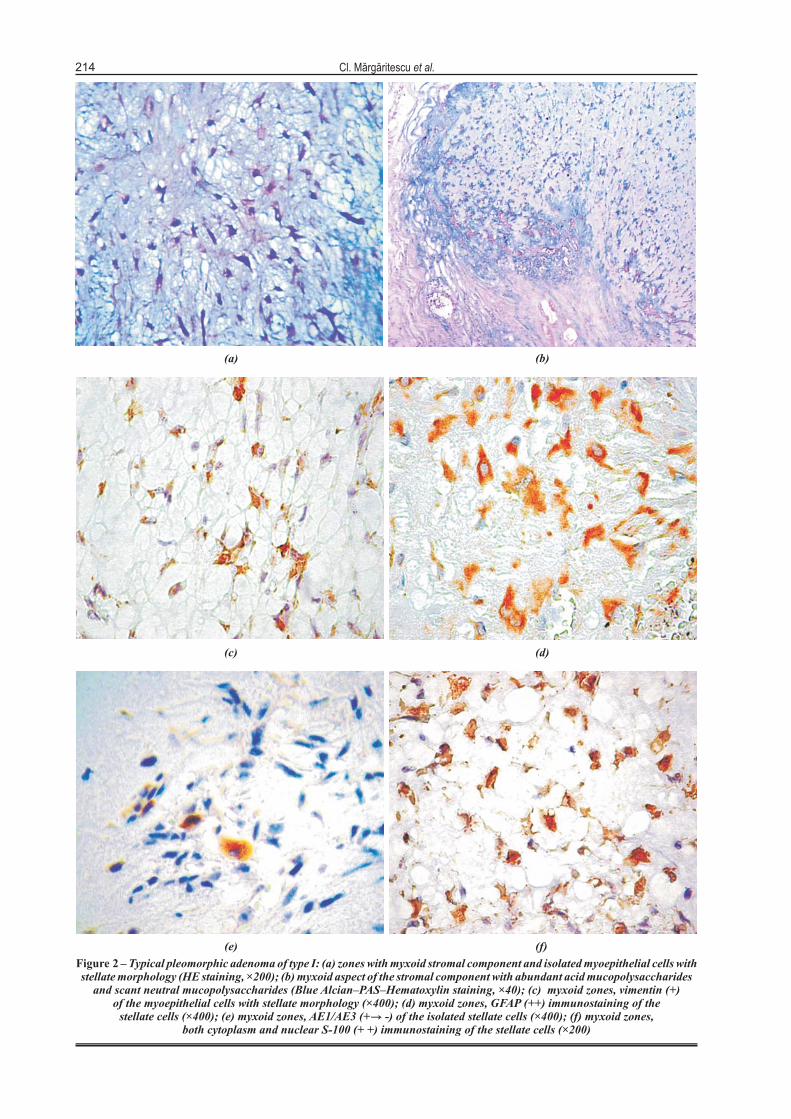
Figure 2 – Typical pleomorphic adenoma of type I: (a) zones with myxoid stromal component and isolated myoepithelial cells withstellate morphology (HE staining, ×200); (b) myxoid aspect of the stromal component with abundant acid mucopolysaccharides
and scant neutral mucopolysaccharides (Blue Alcian–PAS–Hematoxylin staining, ×40); (c) myxoid zones, vimentin (+)of the myoepithelial cells with stellate morphology (×400); (d) myxoid zones, GFAP (++) immunostaining of the
stellate cells (×400); (e) myxoid zones, AE1/AE3 (+ -) of the isolated stellate cells (×400); (f) myxoid zones,both cytoplasm and nuclear S-100 (+ +) immunostaining of the stellate cells (×200)
(f)(e)
(d)(c)
(a) (b)
Tumoral stroma of salivary pleomorphic adenoma – histopathological, histochemical and immunohistochemical study
215
Here and there, inside the myxoid component, there were present myoepithelial cells with stellate shape, isolated or grouped in small clusters. The stromal component realized about 80% of the tumoral mass and was mainly represented by the myxoid stroma (Figure 1d).
There were also present other stromal differentiations, generally in small quantities, but in variable proportion from case to case (chondro-myxoid, chondroid and fibro-hyaline differentiations).
In 25 cases of pleomorphic adenomas with well-balanced stromal / parenchyma proportion the epithelial component represented about 50% of the tumoral mass (Figure 1e).
The dominant tumoral pattern was tubular and solid- insular. Another pattern was trabecular and fascicular. The stromal component representing about 50% of the tumoral mass had mainly myxoid, chondro-myxoid and chondroid differentiations, more often associated. On the limited areas there have been noticed fibrous, fibro-hyaline stroma and in one case even an osteoid stromal differentiation.
In 12 cases of typical pleomorphic adenomas the epithelial component predominated, the neoplastic epithelial proliferation realized 70–80% of the tumoral mass (Figure 1f).
The most frequent encountered patterns were the tubular and the insular ones. Another tumoral pattern
present at the limited areas was micro-, macrocystic, cribriform and pseudoangiomatous. The stromal component was reduced, representing no more than 20–30% of the tumoral mass.
The most frequent encountered stromal differentiation was of myxoid type. In small proportion there were associated other stromal differentiations like those of fibrous, fibro-hyaline or fibro-myxoid type.
In 9 cases of typical pleomorphic adenomas the epithelial component predominated, but it presented focal monomorphic differentiations of squamous (three cases), oncocytic (one case), basaloid (one case), fusiform-myoepithelioma like (two cases) and plasmacytoid (one case).
These epithelial differentiations were described at the cytological differentiations of the epithelial tumoral component. The stromal component of these tumors was reduced and mainly represented by the myxoid and fibro-hyaline differentiation.
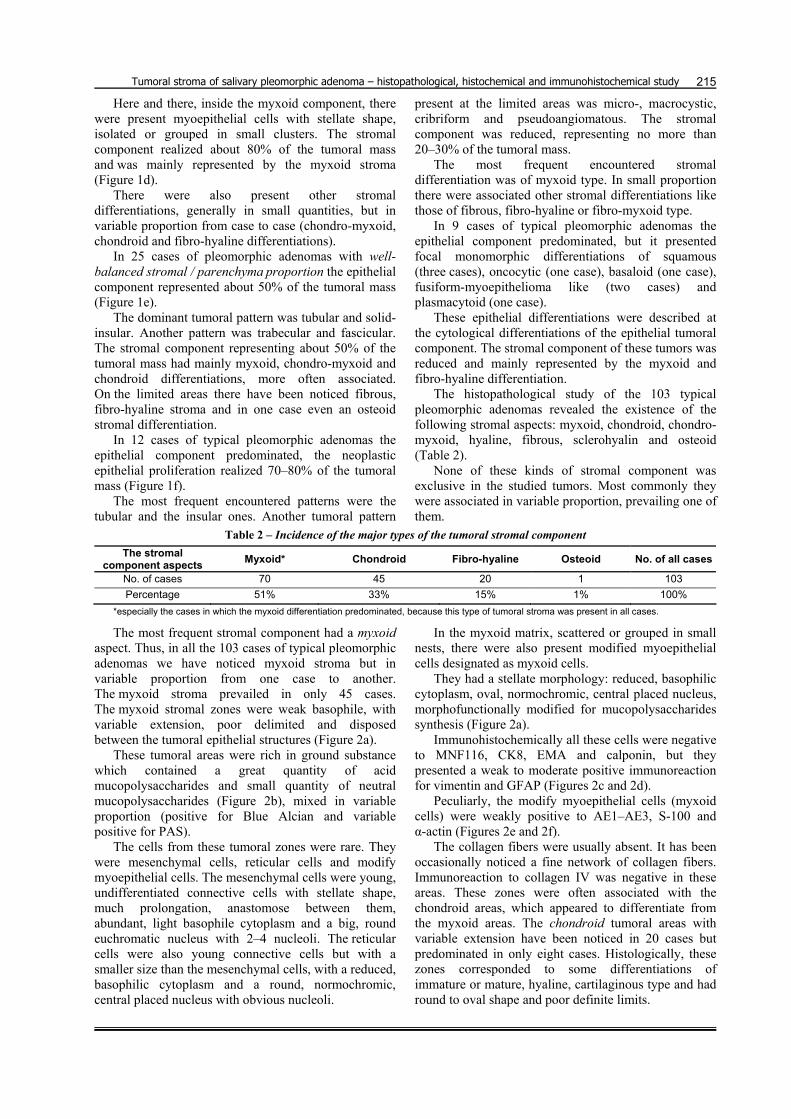
The histopathological study of the 103 typical pleomorphic adenomas revealed the existence of the following stromal aspects: myxoid, chondroid, chondro-myxoid, hyaline, fibrous, sclerohyalin and osteoid (Table 2).
None of these kinds of stromal component was exclusive in the studied tumors. Most commonly they were associated in variable proportion, prevailing one of them.
Table 2 – Incidence of the major types of the tumoral stromal component The stromal
component aspects Myxoid* Chondroid Fibro-hyaline Osteoid No. of all cases
No. of cases 70 45 20 1 103 Percentage 51% 33% 15% 1% 100%
*especially the cases in which the myxoid differentiation predominated, because this type of tumoral stroma was present in all cases.
The most frequent stromal component had a myxoid aspect. Thus, in all the 103 cases of typical pleomorphic adenomas we have noticed myxoid stroma but in variable proportion from one case to another. The myxoid stroma prevailed in only 45 cases. The myxoid stromal zones were weak basophile, with variable extension, poor delimited and disposed between the tumoral epithelial structures (Figure 2a).
These tumoral areas were rich in ground substance which contained a great quantity of acid mucopolysaccharides and small quantity of neutral mucopolysaccharides (Figure 2b), mixed in variable proportion (positive for Blue Alcian and variable positive for PAS).
The cells from these tumoral zones were rare. They were mesenchymal cells, reticular cells and modify myoepithelial cells. The mesenchymal cells were young, undifferentiated connective cells with stellate shape, much prolongation, anastomose between them, abundant, light basophile cytoplasm and a big, round euchromatic nucleus with 2–4 nucleoli. The reticular cells were also young connective cells but with a smaller size than the mesenchymal cells, with a reduced, basophilic cytoplasm and a round, normochromic, central placed nucleus with obvious nucleoli.
In the myxoid matrix, scattered or grouped in small nests, there were also present modified myoepithelial cells designated as myxoid cells.
They had a stellate morphology: reduced, basophilic cytoplasm, oval, normochromic, central placed nucleus, morphofunctionally modified for mucopolysaccharides synthesis (Figure 2a).
Immunohistochemically all these cells were negative to MNF116, CK8, EMA and calponin, but they presented a weak to moderate positive immunoreaction for vimentin and GFAP (Figures 2c and 2d).
Peculiarly, the modify myoepithelial cells (myxoid cells) were weakly positive to AE1–AE3, S-100 and α-actin (Figures 2e and 2f).
The collagen fibers were usually absent. It has been occasionally noticed a fine network of collagen fibers. Immunoreaction to collagen IV was negative in these areas. These zones were often associated with the chondroid areas, which appeared to differentiate from the myxoid areas. The chondroid tumoral areas with variable extension have been noticed in 20 cases but predominated in only eight cases. Histologically, these zones corresponded to some differentiations of immature or mature, hyaline, cartilaginous type and had round to oval shape and poor definite limits.
Cl. Mărgăritescu et al.
216
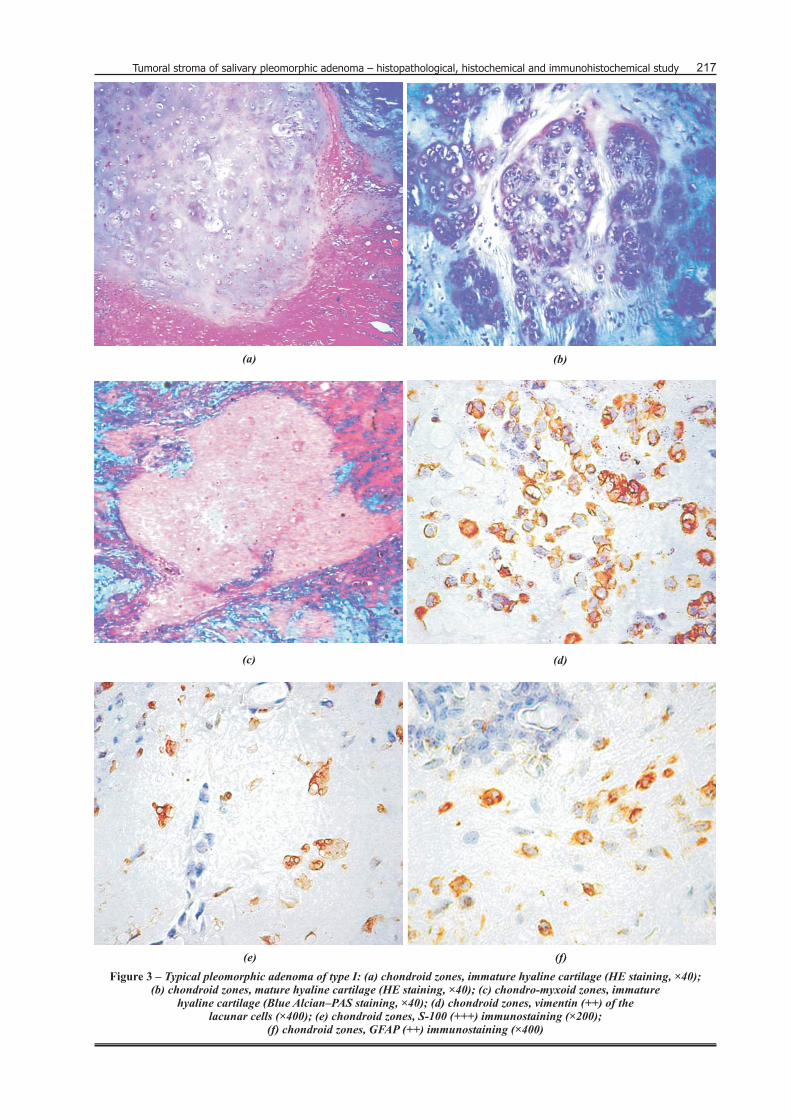
Most frequently the chondroid zones had the aspect of an immature, hyaline cartilage (Figure 3a), where the ground substance had an acidophilic aspect, rare chondroid lacunae with small, oval chondroblasts (with basophilic cytoplasm, round hypochromatic, central placed nucleus with obvious nucleoli).
The stromal zones with mature, hyaline, cartilaginous differentiation were rare (Figure 3b).
These areas had an abundant extracellular matrix rich in mucopolysaccharides (Figure 3c), with accentuate basophile around the chondroid lacunae but acidophilic in the rest, containing a small quantity of mucopolysaccharides but more collagen fibers.
Generally, the chondroid lacunae had one or no more than two chondrocytes (chondroid lacunae with diad). The chondrocytes were round when isolated and columnar when disposed in group of two cells; they had clear or weak acidophil cytoplasm, great, hypochromic, round to oval nucleus, nucleolated and placed central or little eccentric.
Immunohistochemically in these areas we noticed a positive reaction for vimentin (with variable intensity from moderate to strong) (Figure 3d), S-100 (an intense both cytoplasmic and nuclear reaction) (Figure 3e) and GFAP (a moderate cytoplasm immunoreaction) (Figure 3f), all other reaction were negative.
Most of the chondroid differentiations were surrounded by the myxoid stroma, fact that suggested the possibility of chondroid metaplasia of the myxoid stroma.
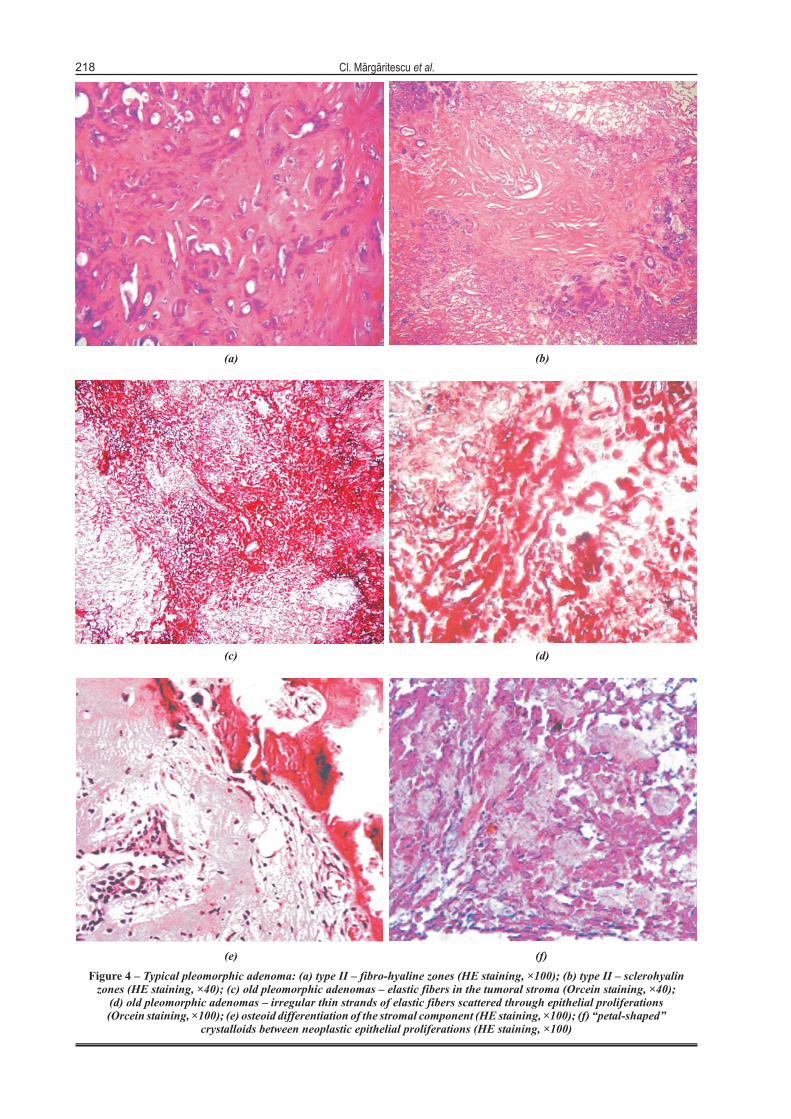
Another aspect of the stromal component encountered in 12 cases was fibrous, fibro-hyaline or sclerohyalin, represented by fascicles of collagen fibers with variable thickness (thicker in sclerohyalin variant), disposed in epithelial proliferations and often suffering hyaline dystrophy and even calcium precipitations (Figures 4a and 4b).
This kind of stroma predominated in only 5 cases, the age of these patients was advanced and these tumors had a longer evolution. The hyaline aspect was also present as eosinophil, acellular, homogenous, fine fibrilar bands scattered through the epithelial structure or surrounding the neoplastic ductal structures, which created a cylindromatous aspect for these tumoral regions.
This aspect was encountered in two cases of pleomorphic adenomas with stromal predominance. Few fibroblast cell from these areas were positive only to vimentin, all other immunostaining were negative.
In the old pleomorphic adenomas, we have also remarked the prevalence of elastic fibers in the tumoral stroma component, highlighted by orcein staining. These fibers were scattered through epithelial proliferations like the irregular compact masses or the irregular thin strands (Figures 4c and 4d).
In only one case, we have noticed an osteoid differentiation of the stromal component. In these tumoral areas, we have remarked the presence of osteoid trabeculae in tight connection with neoplastic epithelial proliferations (Figure 4e).
The osteoid areas were given by an eosinophil ground substance with vague lamellar disposition and rare osteoblasts-polyhedral cells that have small cytoplasmic processes, basophilic cytoplasm, PAS positive and round, normochromic, nucleolated and central placed nucleus.
In only one case we have found crystalloids, presented between neoplastic epithelial proliferations and in the stromal component. They were radially arranged, “petal-shaped”, blunt-ended clusters of eosinophilic tubular structures more probable being tyrosine crystalloids (Figure 4f).
Discussions
Our study reveals that only 68.31% of pleomorphic adenomas developed in the parotid glands were completely encapsulated and other 3% of had tumoral process extended in the normal salivary parenchyma. In the literature quantitative study showed that thickness of pleomorphic adenoma capsule ranged from 15–1750 mm [19].
When tumors were serially sectioned areas of capsular deficiency were seen in all cases [20]. In predominantly mucoid pleomorphic adenomas, the capsule may be virtual-absent and the tumor abuts onto the adjacent salivary gland. The extension of pleomorphic adenomas into the surrounding tissues through the capsule can be interpreted as separate satellite nodules, but they are invariably attached to the main tumor by an isthmus [20, 21].
The extension beyond the capsule of these tumors without nucleo-cytoplasmic atypia and atypical mitotic figures should not be interpreted as a sign of malignancy. The tumoral tissue in the capsule may be misunderstood as a sign of malignancy, but in these cases the atypia characteristic to malignant cells was absent.
According to the relative proportion between the stromal and the epithelial component of these tumors we found that 55% of them were of type I, 24% were of type II, 12% were of type III and 9% were of type IV.
Seifert G. et al. first submitted such histo-pathological classification of the pleomorphic adenomas in 1976. Considering the tumoral stroma / parenchyma proportion, these authors classified the pleomorphic adenomas in four subtypes: subtype I (30.5% of the cases, in which there were included pleomorphic adenomas with 30% to 50% of the tumoral stroma), subtype II (55% of the cases, with 80% of the stromal component), subtype III (9% of the cases, with 20% to 30% of the tumoral stroma) and subtype IV (5.5% of the cases, with poor represented tumoral stroma in a similar proportion to that from subtype III but with focal monomorphic epithelial differentiations) [22].
This distinction has no therapeutic significance but helps emphasize the broad morphologic spectrum possible within this neoplasm. Other observation of our study reveals the great diversity of morphological aspects of stroma in these tumors.
Tumoral stroma of salivary pleomorphic adenoma – histopathological, histochemical and immunohistochemical study 217
(e)
(a)
(f)
(d)(c)
(b)
Figure 3 – Typical pleomorphic adenoma of type I: (a) chondroid zones, immature hyaline cartilage (HE staining, ×40);(b) chondroid zones, mature hyaline cartilage (HE staining, ×40); (c) chondro-myxoid zones, immature
hyaline cartilage (Blue Alcian–PAS staining, ×40); (d) chondroid zones, vimentin (++) of thelacunar cells (×400); (e) chondroid zones, S-100 (+++) immunostaining (×200);
(f) chondroid zones, GFAP (++) immunostaining (×400)
218 Cl. Mãrgãritescu et al.
(f)(e)
(d)(c)
(a) (b)
Figure 4 – Typical pleomorphic adenoma: (a) type II – fibro-hyaline zones (HE staining, ×100); (b) type II – sclerohyalinzones (HE staining, ×40); (c) old pleomorphic adenomas – elastic fibers in the tumoral stroma (Orcein staining, ×40);
(d) old pleomorphic adenomas – irregular thin strands of elastic fibers scattered through epithelial proliferations(Orcein staining, ×100); (e) osteoid differentiation of the stromal component (HE staining, ×100); (f) “petal-shaped”
crystalloids between neoplastic epithelial proliferations (HE staining, ×100)

Tumoral stroma of salivary pleomorphic adenoma – histopathological, histochemical and immunohistochemical study
219
The most frequent stromal type was the myxoid one, encountered in all cases of pleomorphic adenomas but in variable proportion from case to case. This kind of stromal component appeared in 51% of the cases.
Other benign or malign salivary gland tumors may have on restricted areas tubular epithelial proliferations associated with myxoid or edematous stroma, as in the canalicular adenomas or the polymorphous low-grade adenocarcinomas. In such cases, making seriated sections and correlating the histopathological data with the clinical ones it may be avoided a wrong diagnosis.
We also have to bear in mind the tumors of soft tissue with an important myxoid component such as the myxoma, the myxofibroma, the myxoid lipoma and the myxoid neurofibroma. These tumors with mesenchymal origin were very rare in the salivary gland levels, representing about 1.9–5% of all the salivary tumors [23, 24].
Histochemically, we noticed the prevalence of acid mucopolysaccharides in the myxoid areas. When referring to the different mucin types present in the pleomorphic adenomas, the review data have specified the existence of two-mucin types: one of epithelial nature with a high content of neutral glycoprotein and another one of mesenchymal origin rich in sulphated and non-sulphated glycosaminoglycan [7–9].
The latter was produced by the modified myoepithelial cells depending on the tissue culture and the inoculation studies [25–27].
Zhao M et al. in a study concerning the glycosaminoglycans (GAGs) localization in pleomorphic adenoma reveals that both epithelial and mesenchymal-like tissues contain GAGs [28].
Myxoid region was consistently stained for both chondroitin 6-sulfate and hyaluronic acid but variably for chondroitin 4-sulfate, dermatan sulfate and keratan sulfate; heparan sulfate was not detected. The chondroid region showed increased staining for chondroitin 6-sulfate but reduced staining for hyaluronic acid when compared with the myxoid region. In addition, chondroitin 4-sulfate, dermatan sulfate and keratan sulfate were seen both in chondroid cells and the territorial matrix, whereas HS was present only in the cells. It is suggested that GAGs in PA are mainly produced by non-luminal cells and influence the proliferation, differentiation, secretory activity and shape of tumor cells, thus contributing to the morphological diversity of this tumor [28].
The greater hyaluronic acids composition of the pleomorphic adenomas comparative to those from the adenoid cystic carcinoma may be used in the differential diagnose of these salivary gland tumors [8].
Immunohistochemically we notice the presence of modify myoepithelial cells (positive to AE1–AE3, S-100 and α-actin) in the myxoid areas, involved in the genesis of these areas by epithelial-mesenchymal transdifferentiation process. Aigner T. et al. had proved that the cells from the tubular neoplastic areas had only epithelial characteristics, while the cells from the tubulo-myxoid zones had a mixed phenotype [29].
The detection in the ductal cells, by in situ hybridization, of the genes involved in the aggregan core protein mRNA synthesis and which was positive to cytokeratins, demonstrated the expression of the mesenchymal genes into cells with epithelial origin. This fact suggests that the neoplastic ductal cells were involved in the myxoid matrix production from the stromal areas of the pleomorphic adenomas.
This process was at the origin of the structural pleomorphism of such tumors and represented a furthermore argument for the single-cell theories, most probably a myoepithelial origin of all the neoplastic cells from these tumors. As well, Ogawa Y. et al., showed that in the myxoid zones of the pleomorphic adenomas, the CK14 immunoreaction had a sporadic character, limited to some tumoral cells with stellate morphology [30].
According to Brennan P. A. et al., α-smooth muscle actin in the pleomorphic adenoma is expressed only by the normal myoepithelial cells and by the so-called modify myoepithelial cells. The weak positive immunoreaction of some cells from the myxoid areas may be explained by the possible origin of the cells from the myofibroblasts [30].
According to Anderson C. et al., the GFAP immunostaining is present only in the stromal cells from the myxoid and chondroid tumoral areas [31].
Achtstatter T. et al. consider that the reactivity of the myoepithelial cells to GFAP is the consequence of a cross-reaction to the intermediate filaments with the same structure and chemical composition as the glial fibrillary acidic protein [32].
Ostrzega N. et al. consider that the positive GFAP immunoreaction helps in the differential diagnose of the pleomorphic adenomas from the low-grade polymorphous adenocarcinoma, where this reaction is absent [33].
Study attempt by Aigner Th. and Neureiter D. had showed that small quantities of collagen I, III and V were present in the myxoid areas and more abundant in the fibrous zones and tumoral capsule [25, 29].
Luna M. G. had proved that type I and II collagens were co-distributed in the extracellular matrix of myxoid tissue in pleomorphic adenomas [34].
In the chondroid tissue, variable immunostaining patterns of type I and II collagens were also observed. Some proliferating myoepithelial cells in myxoid and chondroid tissue were immunostained with anti-alpha-smooth muscle actin antibody indicating their myoepithelial origin. These results suggested that proliferating myoepithelial cells may be the origin of the chondroid tissue and the expression of type IX collagen in cartilaginous tissue precedes the expression of type I and II collagens [34].
The second most encountered stroma was the chondroid (33% of the cases) and chondro-myxoid type, especially the immature, hyaline, cartilaginous one. The tumors rich in chondroid and chondromyxoid stroma imposed a differential diagnosis with cartilaginous type tumors, such as the chondroma or the
Cl. Mărgăritescu et al.
220
chondroblastoma, especially in the cases developed on the rest of the heterotopic salivary parenchyma. Also, we observed that the chondroid differentiations were surrounded by the myxoid stroma, fact that suggested the possibility of chondroid metaplasia of the myxoid stroma.
According to Aigner Th. et al. the chondroplastic cells derive from stellate cell of the myxoid areas of the tumor, which through mucopolysaccharides synthesis developed cartilaginous areas in the pleomorphic adenomas [29].
This fact was sustained by ultrastructural and immunohistochemical arguments [29, 35–38].
Kusafuka et al. have reported that the genesis of the chondroid stromal areas are associated with the overexpression of the bone morphogenetic proteins (BMPs) by the neoplastic myoepithelial cells [39].
This protein belongs to the transforming growing factor (TGF)-β superfamily which interferes with the regulation of the mesenchymal tissue formation. The TGF-β2 is expressed by the neoplastic ductal epithelial cells, while TGF-β3 is expressed by the neoplastic myoepithelial cells from the solid neoplastic epithelial proliferating areas, the metaplastic squamous cells and the luminal cells from the tubular neoplastic proliferating areas. TGF-β is involved in the control of the luminal and myoepithelial neoplastic cell differentiation [39].
Moreover, immunohistochemical investigation of bone morphogenetic protein-2 (BMP-2) and type II collagen, two cartilage-associated proteins, made by Zhao M. et al. demonstrated that in pleomorphic adenomas BMP-2 immunoreactivity was detected in the luminal and non-luminal cells of the tubulo-ductal structures, plasmacytoid cells, and other scattered tumor cells in solid areas [40].
In addition, tumor cells in chondroid areas in most cases, and stellate cells in myxoid areas in many cases, were also intensely labeled for BMP-2. Type II collagen was localized in the intercellular matrix of chondroid areas and in a few chondroid differentiating cells in myxoid areas, confirming its cartilage-specificity.
A proportional relationship was observed between BMP-2 expression and chondroid formation, although BMP-2 was also stained in occasional pleomorphic adenomas without chondroid formation. It is speculated that BMP-2 might be secreted by tumor cells and play a role in chondroid formation in pleomorphic adenomas by inducing some tumor cells to produce type II collagen and other chondroid matricial substances, like glycosaminoglycans.
The expression of BMP-2 is specific to pleomorphic adenoma and may possibly be used as a useful marker in differentiating pleomorphic adenomas from other salivary gland tumors [40].
Kusafuka et al. proved by immunohistochemical investigation that cartilage-derived morphogenic proteins (CDMP)-1 and -2 (proteins that belong to the bone morphogenetic protein (BMP) family, in the transforming growth factor (TGF)-β superfamily) play
essential roles in chondroid formation in salivary pleomorphic adenoma [41].
Thus, CDMP-1 was immunolocalized in the cuboidal neoplastic myoepithelial cells around the chondroid areas of the pleomorphic adenomas, whereas these molecules were not localized in the spindle-shaped neoplastic myoepithelial cells of the myxoid element or the lacuna cells of the chondroid element in these tumors.
CDMP-2 was expressed neither in normal salivary glands nor any of the elements of the pleomorphic adenomas. Type-II collagen and aggrecan were immunolocalized throughout the matrix around the lacuna cells of the chondroid element, whereas type-X collagen was not immunolocalized in any epithelial or stromal elements, including the chondroid elements.
Aggrecan was deposited not only on the chondroid matrix, but also on the myxoid stroma and intercellular spaces of the tubulo-glandular structures, whereas chondromodulin-I was deposited on the chondroid matrix. The phenotype of the lacuna cells was similar to that of mature to upper hypertrophic chondrocytes of the authentic cartilage. Also, Kusafuka et al. immunohistochemical investigated the expression in pleomorphic adenomas of two non-collageneous bone matrix proteins: osteonectin (OSN – glycoprotein involved in the early steps of the mineralization of skeletal tissue) and osteopontin (OPN – protein involved in normal and pathological calcifications) [42].
These authors showed a moderate positivity for OSN in the inner layer of tubulo-glandular structures and modified myoepithelial cells from myxoid areas. OSN was expressed in all of the lacuna cells in the chondroid areas. OPN was strongly expressed in the stroma of the myxoid and hyaline areas of the pleomorphic adenomas, but there was no expression of OPN in the chondroid area.
All cases of pleomorphic adenomas expressed type IV collagen. These findings suggested that OSN was related to the production of the type IV collagen by modified myoepithelial cells, whereas OPN was involved in the stromal formation of myxoid or hyaline tissues in pleomorphic adenomas [42].
Investigation of lumican (a keratan sulphate proteoglycan that belongs to the small leucine-rich repeat proteoglycans reported to be associated with cartilage formation) in pleomorphic adenomas demonstrated that this proteoglycan is associated with the formation of “mesenchyme”-like structures in this type of tumour [43].
Immunohistochemistry firstly performed with pepsin pretreatment, proved that lumican was predominantly deposited in the hyaline and fibrous areas and littler in the chondroid areas. Without pepsin pretreatment, lumican was identified in myoepithelial cells in myxoid areas, lacuna cells in chondroid areas, and in the cytoplasm of inner ductal cells. In situ hybridization revealed lumican mRNA expression mainly in the inner cells, the neoplastic myoepithelial cells, and the lacuna cells.
Tumoral stroma of salivary pleomorphic adenoma – histopathological, histochemical and immunohistochemical study
221
The fibrous and fibro-hyaline stromal component predominated in 15% of the cases. In about 2% of the cases, the hyaline was disposed like the homogenous, eosinophilic strand around the tubular epithelial proliferations realizing morphological aspects similar to the tubular variant of the adenoid cystic carcinomas; that is why it was necessary to make a differential diagnosis with this entity.
In literature, it has been specified that the existence of such modifications even in the limited tumoral areas imposes a multiple section performing and in the absence of atypia, we may conclude that it may be a benign tumor [44].
Some long-standing tumors show increasing hyalinisation and the epithelial component is progressively effaced. It is important, however, to scrutinize the residual epithelial elements of such old, scarred pleomorphic adenomas as there is a significant risk of malignant progression in such tumors [45].
Immunohistochemically studies proved that collagen IV and laminin were more intensively localized in hyaline, fibrous and chondroid types of stroma, whereas heparan sulfate proteoglycan was more prominent in myxoid areas [46].
The results suggest that the stroma contains these basement membrane components, which are possibly biosynthesized by epithelial tumor cells, and that histological variety of the stroma depends on proportion of local contents of each basement membrane molecule [46].
In such fibrous areas using orcein staining, we have noticed a great quantity of elastic fibers. Review data have specified that the presence of these fibers is relatively characteristic to the pleomorphic adenomas because these fibers may seldom be observed in other types of salivary gland tumors [12, 47, 48].
We have found the osteoid stromal differentiation in only 1% of the cases. The review data have quoted few cases of pleomorphic adenomas with osteoid stromal differentiations [5, 10, 49].
In such cases there was observe a tendency of osteoid calcification that realized lacy bony trabeculae with basophile tint, rare bony lacunae with osteocyte (oval cells with reduce pale basophile or even acidophil cytoplasm, oval, normochromic, nucleus, central placed). Still some authors have indicated the presence of morphogenetic bony protein in high percentage in the pleomorphic adenomas [40–42, 50, 51].
In about 1% of the cases, we have noticed tyrosine crystals both in the stromal component and among the epithelial proliferations. According to review data, the incidence of such crystalloid structures in pleomorphic adenomas is about 1.5–21% [13–16].
Besides these tyrosine crystalloids, the review data have specified the existence of other two types of collagen crystalloids (eosinophil, fibrilar structures with radial disposal around some annular spaces made up of by connective tissue and sanguine vessels) and crystalloids structures similar to the calcium oxalate [13, 52, 53].
Skalova A. had showed that extracellular collagenous crystalloids from pleomorphic adenomas contain types I and III collagen but not type II, IV, or VI collagen [54]. Moreover, cells surrounding collagenous crystalloids expressed the basement membrane molecules laminin and type IV collagen.
As far as the tyrosine crystalloids are concerned, the review data have specified that they are structures stained with Millon reagent and not with specific collagen staining. It has also been specified that some of these structures would contain much more arginine than tyrosine [14, 55] and that they are the result of the collagen products precipitation secreted by the modified myoepithelial tumoral cells [56].
Tumors that have a lipomatous stromal component of 90% or more have been called lipomatous pleomorphic adenomas [57–60].
In such case we must bear in mind the existence of other fat-containing tumors (such as lipoadenoma, spindle cell lipoma, interstitial lipomatosis, and benign mesenchymoma). Occasional, following spontaneous infarction or fine needle aspiration can be observed extensive inflammation and necrosis. In such tumors may be an increase in mitotic figures and some cellular atypia [61].
Conclusions
Our study demonstrated a great diversity of morphological aspects of stroma in these tumors; the most frequent stromal type being the myxoid one.
The histochemically and immunohistochemically investigations confirm the key role of myoepithelial cells in stromal histogenesis.
Thus, neoplastic myoepithelial cell differentiate to stellate cells, which produce myxoid matrix, generating stromal myxoid areas and farther these one differentiate to chondroplastic cells, which through muco-polysaccharides synthesis develop cartilaginous areas in the pleomorphic adenomas.
References [1] ENEROTH C. M., Salivary gland tumors in the parotid gland,
submandibular gland, and the palate region, Cancer, 1971, 27:1415–1418.
[2] EVESON J. W., CAWSON R. A., Salivary gland tumours. A review of 2410 cases with particular reference to histological types, site, age and sex distribution, J Pathol, 1985, 146:51–58.
[3] SEIFERT G., MIEHLKE A., HAUBRICH J., CHILLA R., Diseases of the salivary glands: diagnosis, pathology, treatment, facial nerve surgery, Georg Thieme Verlag, Stuttgart, 1986, 65–130.
[4] SPIRO R. H., Salivary neoplasms: overview of a 35-year experience with 2807 patients, Head Neck Surg, 1986, 8:177–184.
[5] ELLIS G. L., AUCLAIR P. L., Mixed tumor (pleomorphic adenoma). In: Tumors of the salivary glands. Atlas of Tumor Pathology, chapter 4, section 4.1, 3rd series, fascicle 17, Armed Forces Institute of Pathology, Washington, 1996, 39–57.
[6] CHEUK W., CHAN J. K. C., Salivary gland tumors. In: FLETCHER D. M. (ed), Diagnostic histopathology of tumors, chapter 7, volume I, 2nd edition, Churchill Livingstone, London, 2000, 231–312.
Cl. Mărgăritescu et al.
222
[7] HARRISON J. D., AUGER D. W., Mucosubstance histochemistry of pleomorphic adenoma of parotid and submandibular salivary glands of man. Light and electron microscopy, Histochem J, 1991, 23:293–302.
[8] NAKANISHI K., KAWAI T., SUZUKI M., SHINMEI M., Glycosaminoglycans in pleomorphic adenoma and adenoid cytic carcinoma of the salivary gland, Arch Pathol Lab Med, 1990, 114:1227–1231.
[9] NARA Y., TAKEUCHI J., YOSHIDA K. et al., Immuno-histochemical characterization of extracellular matrix components of salivary gland tumors, Br J Cancer, 1991, 64:307–314.
[10] NEVILLE B. W., DAMM D. D., ALLEN C. M., BOUQUOT J. E., Salivary glands tumors. In: REGEZI J., SCIUBBA J., JORDAN R. (eds), Oral & Maxillofacial Pathology. Chapter 11. Salivary gland pathology, WB Saunders, Philadelphia, 2002, 410–432.
[11] DAVID R., BUCHNER A., Elastosis in benign and malignant salivary gland tumors. A histochemical and ultrastructural study, Cancer, 1980, 45:2301–2310.
[12] NIKAI H., OGAWA I., IJUHIN N. et al., Ultrastructural cytochemical demonstration of elastin in the matrix of salivary gland tumors, Acta Pathol Jpn, 1983, 33:1171–1181.
[13] CAMPBELL W. G. JR., PRIEST R. E., WEATHERS D. R., Characterization of two types of crystalloids in pleomorphic adenomas of minor salivary glands. A light-microscopic, electron-microscopic, and histochemical study, Am J Pathol, 1985, 118:194–202.
[14] CHAPLIN A. J., DARKE P., PATEL S., Tyrosine- rich crystals in pleomorphic adenomas of parotid glands, J Oral Pathol, 1983, 12:342–346.
[15] NOCHOMOVITZ L. E., KAHN L. B., Tyrosine crystals in pleomorphic adenomas of the salivary gland, Arch Pathol, 1974, 97:141–142.
[16] THOMAS K., HUTT M. S., Tyrosine crystals in salivary gland tumours, J Clin Pathol, 1981, 34:1003–1005.
[17] SEIFERT G., SOBIN L. H., Histological typing of salivary gland tumours. World Health Organization international histological classification of tumours, 2nd edition, Springer Verlag, New York, 1991, 123–148.
[18] JASANI B., SCHMID K. W., Immunocytochemistry in diagnostic histopathology, Churchill Livingstone, Edinburgh, 1993, 32–135.
[19] WEBB A. J., EVESON J. W., Pleomorphic adenomas of the major salivary glands: a study f the capsular form in relation to surgical management, Clin Otolaryngol, 2001, 26:134–142.
[20] LAM K. H., WEI W. I., HO H. C., HO C. M., Whole organ sectioning of mixed parotid tumors, Am J Surg, 1990, 160:377–381.
[21] PATEY D. H., THACKRAY A. C., The treatment of parotid tumours in the light of a pathological study of parotidectomy material, Br J Surg, 1958, 45:477–487.
[22] SEIFERT G., LANGROCK I., DONATH K., A pathological classification of pleomorphic adenoma of the salivary glands, HNO, 1976, 24(12):415–426.
[23] AUCLAIR P. L., ELLIS G. L., GNEPP D. R. et al., Salivary gland neoplasms: general considerations. In: ELLIS G. L., AUCLAIR P. L., GNEPP D. R. (eds), Surgical pathology of the salivary glands, WB Saunders, Philadelphia, 1991, 135–164.
[24] SEIFERT G., OEHNE H., Die mesenchymalen (nicht- epithelialen) speicheldrusentumorens. Analyse von 167 tumorfallen des speicheldrusen-registers, Laryngol Rhinol Otol (Stuttg), 1986, 65:485–491.
[25] NEUREITER D., BOHMER J., KIRCHNER T., AIGNER T., Pleomorphic adenomas of the parotid express different mesenchymal phenotypes: demonstration of matrix gene expression products characteristic of the fibroblastic and chondrocytic cell lineages, Histopathol, 1999, 35(4):373–379.
[26] TAKEUCHI J., SOBUE M., YOSHIDA M. et al., Pleomorphic adenoma of the salivary gland. With special reference to histochemical and electron microscopic studies and biochemical analysis of glycosaminoglycans in vivo and in vitro, Cancer, 1975, 36:1771–1789.
[27] FUJITA Y., YOSHIDA T., SAKAKURA Y., SAKAKURA T., Reconstruction of pleomorphic adenoma of the salivary glands in the three-dimensional collagen gel matrix culture, Virchows Arch, 1999, 434:137–143.
[28] ZHAO M., TAKATA T., OGAWA I. et al., Localization of glycosaminoglycans (GAGs) in pleomorphic adenoma (PA) of salivary glands: an immunohistochemical and histochemical evaluation, J Oral Pathol Med, 1998, 27(6):272–277.
[29] AIGNER T., NEUREITER D., VOLKER U. et al., Epithelial-mesenchymal transdifferentiation and extracellular matrix gene expression in pleomorphic adenomas of the parotid salivary gland, J Pathol, 1998, 186:178–185.
[30] OGAWA Y., TOYOSAWA S., ISHIDA T., IJUHIN N., Keratin 14 immunoreactive cells in pleomorphic adenomas and adenoid cystic carcinomas of salivary glands, Virchows Arch, 2000, 437:58–68.
[31] ANDERSON C., KNIBBS D. R., ABBOTT S. J. et al., Glial fibrillary acidic protein expression in pleomorphic adenoma of salivary gland: an immunoelectron microscopic study, Ultrastruct Pathol, 1990, 14:263–271.
[32] ACHTSTATTER T., MOLL R., ANDERSON A. et al., Expression of glial filament protein (GFP) in nerve sheaths and non-neural cells re-examined using monoclonal antibodies, with special emphasis on the co-expression of GFP and cytokeratins in epithelial cells of human salivary gland and pleomorphic adenomas, Differentiation, 1986, 31:206–227.
[33] OSTRZEGA N., CHENG L., LAYFIELD L., Glial fibrillary acid protein immunoreactivity in fine-needle aspiration of salivary gland lesions: a useful adjunct for the differential diagnosis of salivary gland neoplasms, Diagn Cytopathol, 1989, 5(2):145–149.
[34] LUNA M. G., Immunohistochemical localization of Type I, II and IX collagens in pleomorphic adenoma of human salivary glands, Kokubyo Gakkai Zasshi, 1996, 63(1):122–130.
[35] AIGNER T., NEUREITER D., MULLER S. et al., Phenotypic diversity of neoplastic chondrocytes and extracellular matrix gene expression in cartilaginous neoplasm, Am J Pathol, 1997, 150:2133–2141.
[36] ERLANDSON R. A., CARDON-CARDO C., HIGGINS P. J., Histogenesis of benign pleomorphic adenoma (mixed tumor) of the major salivary glands. An ultrastructural and immunohistochemical study, Am J Surg Pathol, 1984, 8:803–820.
[37] DARDICK I., VAN NOSTRAND A. W. P., JEANS M. T. et al., Pleomorphic adenoma. I. Ultrastructural organization of epithelial regions, Hum Pathol, 1983, 14:780–797.
[38] MILLS S. E., COOPER P. H., An ultrastructural study of cartilaginous zones and surrounding epithelium in mixed tumors of salivary glands and skin, Lab Invest, 1981, 44(1):6–12.
[39] KUSAFUKA K., YAMAGUCHI A., KAYANO T., TAKEMURA T., Immunohistochemical localization of members of the transforming growth factor (TGF)-β superfamily in normal human salivary glands and pleomorphic adenomas, J Oral Pathol Med, 2001, 30:413–420.
[40] ZHAO M., TAKATA T., OGAWA I. et al., Immunohistochemical demonstration of bone morphogenetic protein-2 and type II collagen in pleomorphic adenoma of salivary glands, J Oral Pathol Med, 1998, 27(7):293–296.
[41] KUSAFUKA K., LUYTEN F. P., DE BONDT R. et al., Immunohistochemical evaluation of cartilage-derived morphogenic protein-1 and -2 in normal human salivary glands and pleomorphic adenomas, Virchows Arch, 2003, 442(5):482–490.
[42] KUSAFUKA K., YAMAGUCHI A., KAYANO T., TAKEMURA T., Expression of bone matrix proteins, osteonectin and osteopontin, in salivary pleomorphic adenomas, Pathol Res Pract, 1999, 195(11):733–739.
Tumoral stroma of salivary pleomorphic adenoma – histopathological, histochemical and immunohistochemical study
223[43] KUSAFUKA K., ISHIWATA T., SUGISAKI Y. et al., Lumican
expression is associated with the formation of mesenchyme-like elements in salivary pleomorphic adenomas, J Pathol, 2004, 203(4):953–960.
[44] PARHAM D. M., BUGG M. F., PRATT C. B., Carcinomas, adenomas precursor lesions and second malignancies. In: PARHAM D. (ed), Paediatric neoplasia morphology and biology, Lippincott–Raven, Philadelphia, 1996, 363–404.
[45] AUCLAIR P. L., ELLIS G. L., Atypical features in salivary gland mixed tumors: their relationship to malignant transformation, Mod Pathol, 1996, 9:652–667.
[46] SAKU T., CHENG J., OKABE H., KOYAMA Z., Immuno-localization of basement membrane molecules in the stroma of salivary gland pleomorphic adenoma, J Oral Pathol Med, 1990, 19(5):208–214.
[47] DAVID R., BUCHNER A., Elastosis in benign and malignant salivary gland tumors. A histochemical and ultrastructural study, Cancer, 1980, 45:2301–2310.
[48] DAVID R., BUCHNER A., Tannic acid–glutaraldehyde fixative and pleomorphic adenomas of the salivary gland: an ultrastructural study, J Oral Pathol, 1982, 11:26–38.
[49] CHEUK W., CHAN J. K. C., Salivary gland tumors. In: FLETCHER D. M. (ed), Diagnostic histopathology of tumors, chapter 7, volume I, 2000, 231–312.
[50] LIANJIA Y., YAN J., HITOSHI N. et al., An immunohisto-chemical study of bone morphogenetic protein in pleomorphic adenoma of the salivary gland, Virchows Arch [A], 1993, 422:439–443.
[51] HATAKEYAMA S., SATOH M., YOSHIMURA N., OTSU T., Immunocytochemical localization of bone morphogenetic proteins (BMPs) in salivary gland pleomorphic adenoma, J Oral Pathol Med, 1994, 23(5):232–236.
[52] HUMPHREY P. A., INGRAM P., TUCKER A., SHELBURNE J. D., Crystalloids in salivary gland pleomorphic adenomas, Arch Pathol Lab Med, 1989, 113:390–393.
[53] DYKE P. C., HAJDU S. I., STRONG E. W. et al., Mixed tumor of parotid containing calcium oxalate crystals, Arch Pathol, 1971, 91:89–92.
[54] SKALOVA A., LEIVO I., MICHAL M., SAKSELA E., Analysis of collagen isotypes in crystalloid structures of salivary gland tumors, Hum Pathol, 1992, 23(7):748–754.
[55] VALENTE P. T., HOOBER J. K., PHILLIPS S. J., Tyrosine-rich crystalloids in pleomorphic adenoma: SEM findings and partial biochemical characterization, Ultrastruct Pathol, 1988, 12:613–620.
[56] HARRIS B. R., SHIPKEY F., Tyrosine-rich crystalloids in neoplasms and tissues of the head and neck, Arch Pathol Lab Med, 1986, 110:709–712.
[57] HASKELL H. D., BUTT K. M., WOO S. B., Pleomorphic adenoma with extensive lipometaplasia: report of three cases, Am J Surg Pathol, 2005, 29(10):1389–1393.
[58] IDE F., KUSAMA K., Myxolipomatous pleomorphic adenoma: an unusual oral presentation, J Oral Pathol Med, 2004, 33(1):53–55.
[59] NG W. K., MA L., Pleomorphic adenoma with extensive lipometaplasia, Histopathol, 1995, 27:285–288.
[60] SEIFERT G., DONATH K., SCHAFFER R., Lipomatous pleomorphic adenomas of the parotid gland. Classification of lipomatous tissue in salivary glands, Pathol Res Pract, 1999, 195:247–252.
[61] LI S., BALOCH Z. W., TOMASZEWSKI J. E., LIVOLSI V. A., Worrisome histologic alterations following fine-needle aspiration of benign parotid lesions, Arch Pathol Lab Med, 2000, 124:87–91.
Mailing address Claudiu Mărgăritescu, Assistant Professor, M. D., Ph. D., Department of Pathology, Faculty of Dentistry, University of Medicine and Pharmacy of Craiova, Street Petru Rareş no. 2–4, 200 349 Craiova, Romania; Phone +40251–523 654, E-mail: [email protected], [email protected] Received: 25 November, 2005
Accepted: 10 December, 2005





























