Embed Size (px)
Citation preview

PRENATAL DIAGNOSISPrenat Diagn 2010; 30: 438–442.Published online 5 April 2010 in Wiley InterScience(www.interscience.wiley.com) DOI: 10.1002/pd.2491
Twin anemia polycythemia sequence from a prenatalperspective†
Leonardo Gucciardo1, Liesbeth Lewi1, Pascal Vaast2, Marzena Debska3, Luc De Catte1, Tim Van Mieghem1,Elisa Done1, Roland Devlieger1 and Jan Deprest1*1Department of Obstetrics and Gynecology, University Hospitals, Leuven, Belgium2Department of Obstetrics and Gynecology, CHU Jeanne de Flandre, Lille, France3Klinika Połoznictwa i Ginekologii CMKP, Szpital Bielanski, Warszaw, Poland
Objectives To describe the prevalence, management and outcome of spontaneous twin anemia polycythemiasequence (TAPS) diagnosed in the prenatal period.
Method Retrospective analysis of 142 consecutive monochorionic twin pregnancies not diagnosed with twinto twin transfusion syndrome. TAPS cases were identified based on the presence of discordant middle cerebralartery peak systolic velocity (MCA-PSV) measurements and signs suggestive of a chronic intertwin transfusionimbalance: either an elevated reticulocyte count in the anemic twin or the presence of few small unidirectionalanastomoses during fetoscopy or at postnatal placental examination.
Results Three cases were identified, giving an estimated prevalence of 2%. Prenatal interventions weretailored to the characteristics of each case and consisted of intrauterine transfusion and interruption of theshared circulation by cord coagulation or laser separation.
Conclusion In monochorionic twin pregnancies, TAPS is an uncommon prenatal finding. Nonetheless, itsincidence seems high enough to recommend screening for this disease by MCA-PSV measurements. Copyright 2010 John Wiley & Sons, Ltd.
KEY WORDS: prenatal; monochorionic twin pregnancy; anemia; polycythemia; fetoscopic laser; cord coagulation;middle cerebral artery; intrauterine transfusion
INTRODUCTION
Monochorionic twin pregnancies nearly all have inter-twin anastomoses connecting the fetal circulations. Inmost cases, the intertwin transfusion is balanced. How-ever, imbalances may occur, leading to a number ofcomplications (Lewi et al., 2008b). Twin to twin transfu-sion syndrome (TTTS) is the best known clinical entity,with a well described ultrasound appearance of oligo-and polyhydramnios and its diagnosis is based on strictsonographic criteria defining the amniotic fluid discor-dance (Senat et al., 2004). TTTS is usually explained asa chronic net intertwin transfusion process. However, asthe majority of twins diagnosed with TTTS do not havesevere intertwin hemoglobin (Hb) differences (Denbowet al., 1998), hormonal factors are likely to be involvedas well (Mahieu-Caputo et al., 2000).
Severe intertwin Hb differences can neverthelessalso occur in monochorionic twin pregnancies in theabsence of severe amniotic fluid discordance typicalfor TTTS (Lopriore et al., 2005). Twin anemia poly-cythemia sequence (TAPS) was suggested as a separateclinical entity (Lopriore et al., 2007). TAPS can occur
*Correspondence to: Jan Deprest, Department of Obstetrics andGynecology, University Hospitals, Leuven, Herestraat 49, 3000Leuven, Belgium. E-mail: [email protected]† This work was presented at the ISUOG 2009 World Congress,Hamburg, Germany.
spontaneously in previously uncomplicated monochori-onic twin pregnancies. It is, however, better knownin its iatrogenic form as a complication of incompletelaser treatment for TTTS (Robyr et al., 2006). In bothinstances, the placentas typically show few, tiny andmostly unidirectional anastomoses (Lewi et al., 2008a;Lopriore et al., 2008). TAPS probably reflects a purenet intertwin transfusion, with a slow transfer of bloodover these tiny anastomoses. Whereas the prenatal diag-nosis, incidence and management of iatrogenic TAPShave been reported previously (Robyr et al., 2006), noinformation is yet available on the management of pre-natally diagnosed spontaneous TAPS (i.e. not occurringafter laser therapy). We therefore reviewed the preva-lence, management and outcome of TAPS in previouslyuncomplicated monochorionic twin pregnancies.
METHODS
We conducted a retrospective analysis of our databaseincluding all monochorionic diamniotic twin pregnan-cies assessed in our unit during the year 2007. Weexcluded cases diagnosed with TTTS defined as apolyuric polyhydramnios in one twin [deepest verticalpocket (DVP) more than 8 cm before 20 weeks andmore than 10 cm after 20 weeks] in one twin and anoligouric oligohydramnios (DVP less than 2 cm) in theother. TAPS was diagnosed as the presence of dis-cordant middle cerebral artery peak systolic velocity
Copyright 2010 John Wiley & Sons, Ltd. Received: 15 October 2009Revised: 14 January 2010
Accepted: 24 January 2010Published online: 5 April 2010

TWIN ANEMIA POLYCYTHEMIA SEQUENCE 439
(MCA-PSV) measurements in combination with featuressuggestive of a chronic intertwin transfusion imbalance.In our center, we routinely measure MCA-PSV in allmonochorionic twin pregnancies from 15 weeks of ges-tation until birth. Discordant MCA-PSV measurementswere defined as a measurement over 1.5 MoM (multi-ples of the median) in one twin in combination with anMCA-PSV less than 0.8 MoM in its co-twin (Robyret al., 2006). An increased MCA-PSV suggests fetalanemia, whereas a decreased MCA-PSV is an indicativeof polycythemia. A chronic rather than an acute intertwintransfusion was diagnosed by an elevated reticulocytecount in the anemic twin or the presence of few smallunidirectional anastomoses typical for TAPS as identi-fied during fetoscopy or on placental injection studiesafter birth.
Information on the pregnancy and neonatal outcomewas obtained from the referring clinicians. The preg-nancy and perinatal outcomes of part of this series wereincluded in a larger prospective study reported elsewhere(Lewi et al., 2008b). Part of the MCA-PSV measure-ments from this cohort was included in a prospectivelongitudinal study performed in our unit (Klaritsch et al.,2009).
RESULTS
In 2007, 142 monochorionic twin pregnancies with-out TTTS were evaluated. Three cases fulfilled thecriteria of spontaneous TAPS (prevalence 2%, 95%confidence interval 0.44–6.3). The prenatal characteris-tics and neonatal outcomes are summarized in Tables 1and 2, respectively. Placental examination confirmedmonochorionicity and Kleihauer–Betke test, TORCH
screening and fetal karyotype were normal in all cases.Particularities of each individual case are describedbelow.
Case 1
A 35-year-old G2P1 was referred at 26 weeks becauseof suspected TTTS. The mother was diagnosed withpreeclampsia at the time of referral. On ultrasound,there was discordant growth, with a hydropic smallerfetus presenting with oligohydramnios (DVP of 1 cm).Doppler measurements were unremarkable, except foran elevated MCA-PSV (70 cm/s, 2.08 MoM). Also, itsplacental part was hydropic (Figure 1). The appropri-ately grown co-twin had a low MCA-PSV (22.6 cm/s,0.67 MoM) with normal amniotic fluid (DVP less than6 cm), umbilical artery and ductus venosus Dopplers.An intrauterine transfusion of the anemic donor (Hb:3.7 g/dL; reticulocyte count: 553 109/L—normal values20–100 109/L) was performed. The maternal situationdeteriorated quickly with progression to severe HELLPsyndrome. Intravenous antihypertensive drugs and mag-nesium sulfate were started, as well as a course ofsteroids. An emergency cesarean section was requireddue to pulmonary edema. The smaller twin weighed650 g and had an Hb of 4.6 g/dL. In contrast, the largertwin weighed 950 g and had an Hb of 20.2g/dL. Thesmaller twin was transfused immediately after birth. Thebaby was oxygen dependent at 28 days of life (bron-chopulmonary dysplasia) and later required a lobectomyfor a lung abscess. Neonatal course of the larger twinwas uneventful. Both had normal brain scans until dis-charge. The mother had an uneventful recovery with nor-mal blood pressures within 7 days. Placental fragmen-tation precluded injection of the chorionic plate vessels.
Table 1—Prenatal characteristics. When two values are displayed, the first is from the recipient (polycythemic fetus) and thesecond is from the donor (anemic fetus)
Case 1 Case 2 Case 3
Prenatal findingsGA at diagnosis (weeks) 25 + 6 23 + 5 28 + 6
MCA-PSV (MoM) (R/D) 0.7/2.1 0.3/2.0 0.7/1.5
DVP (cm) (R/D) 4.4/1 8/1 12/3.5Growth discordance (%) 23.8 28 23.6
Prenatal findings (R) No abnormalities Umbilical vein pulsations Hypocontractility of the heartStructural heart defect MPI of 0.44 (normal ≤0.43)
Ascites
Prenatal findings fetus (D) Cardiothoracic index 0.4 Pericardial effusion. No abnormalitiesHypocontractility
Pericardial effusion, Placental hydrops (7 cm)Subcutaneous edema
Placental hydrops (7 cm)
Prenatal Hb (g/dL) andreticulocyte count (×10 exp9/L) (D)
3.7/553 3.1/442 4.4/NA
Prenatal interventions IUT of the anemic fetus Cord coagulation (R) Laser coagulationIUT (D) Hemodilution (R)
IUT (D)
D, donor; DVP, deepest vertical pocket; Hb, hemoglobin; IUT, intrauterine transfusion; MCA-PSV, middle cerebral artery peak systolic velocity;MPI, myocardial performance index; MoM, multiples of the median; NA, not available; R, recipient.
Copyright 2010 John Wiley & Sons, Ltd. Prenat Diagn 2010; 30: 438–442.DOI: 10.1002/pd
440 L. GUCCIARDO et al.
Table 2—Neonatal outcome. When two values are displayed, the first one is from the recipient (polycythemic) and the second isfrom the donor (anemic) neonate
Neonatal findings Case 1 Case 2 Case 3
Gestational age at birth 26 weeks 27 weeks and 3 days 34 weeks 2 daysNeonatal weight R/D (g) 950/660 995 1805/1525Neonatal Hb R/D (g/dL) 20.2/4.6 12 21.5/14.2Absolute reticulocyte count (D) (10exp9/L) 521 N/A 116
D, donor; Hb, hemoglobin; N/A, not available; R, recipient.
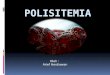
Figure 1—Case 1: hydropic placental territory of the donor (anemicfetus)
However, pathological examination confirmed placentaledema without features of placental abruption.
Case 2
A 30-year-old G3P2 was referred at 24 weeks of gesta-tion for suspected TTTS. Both twins had normal growthbut there was a marked amniotic fluid discordance. Onetwin had an elevated MCA-PSV (60 cm/s, 1.95 MoM)with oligohydramnios (DVP of 1 cm). Umbilical arteryand ductus venosus Dopplers were normal. Its placen-tal part was hydropic. The co-twin had a low MCA-PSV(8 cm/s, 0.26 MoM) as well as polyhydramnios (DVP of8 cm). The a-wave in the ductus venosus was positiveand there was monophasic pulsatility in the umbilicalvein. Ascites was associated with severe cardiomegaly,significant tricuspid regurgitation and a morphologicallyabnormal ascending aorta. The parents opted for selec-tive fetocide of the recipient. We performed a cordocclusion and concomitant transfusion of the co-twin(Hb: 3.1 g/dL; reticulocyte count: 442 109/L). Follow-ing that, its MCA-PSV returned to 40 cm/s. The patientdelivered at 27 weeks because of preterm rupture of themembranes followed by spontaneous labor. The new-born weighed 995 g and was extubated after 3 days withnasal oxygen support for 10 weeks. Hb at the time ofbirth was 15.5 g/dL. The immediate neonatal period wasmarked by symptomatic cardiogenic shock and gradeII intraventricular hemorrhage with spontaneous resolu-tion on day 12. One red blood cell transfusion and twoplatelet transfusions were required before discharge.
Case 3
This 32-year-old G3P2 was referred for mild discor-dant growth at 16 weeks with normal amniotic fluid.At 22 weeks, the larger fetus developed polyhydram-nios (DVP of 9 cm) and MCA-PSV was 20 cm/s (0.71MoM). The smaller twin had an MCA-PSV of 32 cm/s(1.14 MoM) with low normal amniotic fluid (DVP of3 cm). A progressive increase of the growth discor-dance was noticed. At 29 weeks, the criteria for pre-natal TAPS were met. The larger twin [estimated fetalweight (EFW): 1241 g] had an MCA-PSV of 28 cm/s(0.7 MoM) whereas its co-twin (EFW: 948 g) had anMCA-PSV of 58 cm/s (1.5 MoM). The polyhydram-nios of the larger twin had increased to a DVP of12 cm. There were also signs of heart failure as evi-denced by an increased myocardial performance index(Van Mieghem et al., 2009). The anemic twin still hadnormal fluid. Steroids for lung maturation were initi-ated and in- as well as ex-utero therapeutic optionswere discussed. The parents opted for an attempt oflaser coagulation of vascular anastomoses, as well asintrauterine transfusion of the anemic twin combinedwith hemodilution of the polycythemic co-twin. All thiswas foreseen with back up cesarean section. Three tinyarteriovenous anastomoses were identified and coagu-lated and 3 L of amniotic fluid was drained. The ane-mic twin (Hb: 4.4g/dL) was transfused and hemodilu-tion was performed in the polycythemic co-twin (Hb:22.2 g/dL; hematocrit of 67%) by replacing 11 mL offetal blood with 8 mL of 20% albumin solution (Baxter).During follow-up, MCA-PSV normalized in both twins,and there was catch-up growth of the formerly anemictwin. The patient was electively delivered at 34 weeks.The former donor weighed 1525 g, its neonatal Hb was14.2 g/dL. The former recipient weighed 1805 g with anHb of 21.5 g/dL. Both babies had an uneventful neona-tal course with normal brain scans until discharge. Onplacental injection (Figure 2), there were no residualanastomoses.
CONCLUSION
This is the first case series describing the prevalence,clinical presentation and management of spontaneouslyoccurring TAPS diagnosed during pregnancy. We tai-lored therapy according to the clinical characteristicsof each case. Symptomatic treatment always consistedof intrauterine transfusion of the anemic twin. In onecase, laser therapy was used as a causative treatment. In
Copyright 2010 John Wiley & Sons, Ltd. Prenat Diagn 2010; 30: 438–442.DOI: 10.1002/pd

TWIN ANEMIA POLYCYTHEMIA SEQUENCE 441
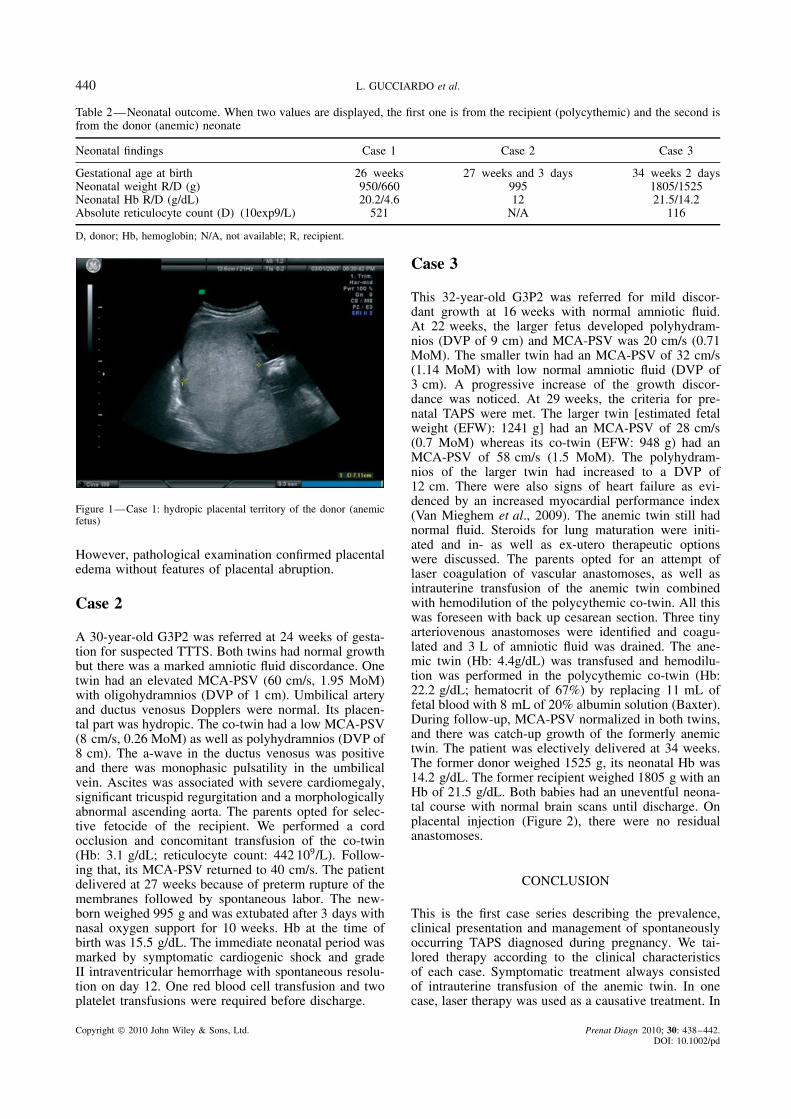
Figure 2—Placenta injection with color dye (case 4). Left image: the donor (anemic fetus, twin 2, 2 clamps) has blue arteries and red veins.The recipient (polycythemic fetus, twin 1, 1 clamp) has purple colored arteries and white veins. Right image: the white arrow shows one of thethree coagulated arteriovenous anastomoses
another, selective feticide was offered because of asso-ciated anomalies, arresting the intertwin transfusion atthe same time.
The simultaneous occurrence of anemia and poly-cythemia in monochorionic twins has been describedboth in the prenatal and postnatal periods, however,with diverging definitions. As mentioned above, TAPS isthought to result from a chronic net intertwin transfusionacross tiny unidirectional anastomoses. Although a con-sensual definition is still lacking, we defined TAPS as theoccurrence of discordant MCA-PSV measurements. Todifferentiate TAPS from an acute fetofetal transfusion, anelevated reticulocyte count suggesting chronic anemia orthe presence of the typical few small anastomoses as evi-denced by fetoscopy or on postnatal placental injectionstudies were added to the inclusion criteria.
The association between severe anemia and MCA-PSV above 1.5 MoM has been well established insingletons. However, prior to 18 weeks, MCA-PSVvalues are somewhat higher in monochorionic twins thanin singletons. Therefore, in order to avoid false-positivediagnoses of suspected anemia, it seems better to usereference ranges specific for monochorionic twins inearly gestation (Klaritsch et al., 2009). Another caveatis that an elevated MCA-PSV in the presence of growthrestriction does not necessarily imply that the fetus isanemic (Mari et al., 2007). Also, the association ofMCA-PSV below 0.8 MoM with polycythemia stillrequires validation. It would seem important to excludeother causes of fetal anemia, such as alloimmunization,congenital infection or fetomaternal hemorrhage. Also,in the absence of a validated correlation, it seemsmandatory to confirm the presence of severe anemia inthe donor twin by cordocentesis before embarking onany causative invasive intervention.
Our cases were all diagnosed between 24 and29 weeks. In the prenatal period, TAPS seems to be lessfar common than TTTS (2 vs 10%, respectively)(Lewiet al., 2008b). However, postnatal data suggest a morecommon condition, affecting up to 4% of pregnancies,all diagnosed beyond 30 weeks. In one of the pregnan-cies complicated by TAPS, fetal demise of the ane-mic twin occurred at 33 weeks (Lewi et al., 2008a,b).Because TAPS seems to occur primarily in the third
trimester, large prospective follow-up studies with doc-umentation of the MCA-PSV until birth are required todocument its exact incidence and natural history. In thelongitudinal study of 50 monochorionic twins that werebooked for delivery in our hospital, we were able to doc-ument MCA-PSV measurements until birth (Klaritschet al., 2009). However, none of these patients devel-oped TAPS, which supports the observation that TAPS isindeed rather uncommon. Nevertheless, because undiag-nosed TAPS may lead to intrauterine demise, MCA-PSVmeasurements appear as a simple and useful tool toidentify TAPS in the prenatal period. All our cases hadcomplicating features other than discordant MCA-PSVmeasurements, which may be due to a referral bias andagain larger prospective series are needed to documentthe exact incidence and natural history of TAPS in pre-viously uncomplicated monochorionic twin pregnancies.
In conclusion, this case series provides an opportunityto inform fetal medicine specialists about TAPS as apotential complication of monochorionic pregnanciesand the tools available for its diagnosis and management.The prevalence and possible implications of TAPS seemto justify routine MCA-PSV measurements in everymonochorionic twin pregnancy.
ACKNOWLEDGEMENTS
E. Done (MEST CT2005 019707), L. Gucciardo(EuroSTEC; LSHC-CT-2006-037409) as well as L.Lewi (QLG1-CT-2002-01632 EuroTwin2Twin) receivegrants from the European Commission. J. Deprest is a‘Fundamental Clinical Researcher’ and receives a grantof the Fonds Wetenschappelijk Onderzoek-Vlaanderen(1.8.012.07.N.02). T. Van Mieghem is beneficiary of agrant of the Flemish Government (Instituut voor Weten-schap en Technologie; IWT 070715).
REFERENCES
Denbow M, Fogliani R, Kyle P, Letsky E, Nicolini U, Fisk N. 1998.Haematological indices at fetal blood sampling in monochorionicpregnancies complicated by feto-fetal transfusion syndrome. PrenatDiagn 18: 941–946.
Klaritsch P, Deprest J, Van Mieghem T, et al. 2009. Reference rangesfor middle cerebral artery peak systolic velocity in monochorionic
Copyright 2010 John Wiley & Sons, Ltd. Prenat Diagn 2010; 30: 438–442.DOI: 10.1002/pd

442 L. GUCCIARDO et al.
diamniotic twins: a longitudinal study. Ultrasound Obstet Gynecol34: 149–154.
Lewi L, Gucciardo L, Huber A, et al. 2008a. Clinical outcome andplacental characteristics of monochorionic diamniotic twin pairswith early- and late-onset discordant growth. Am J Obstet Gynecol199: 511. e1-7.
Lewi L, Jani J, Blickstein I, et al. 2008b. The outcome ofmonochorionic diamniotic twin gestations in the era of invasivefetal therapy: a prospective cohort study. Am J Obstet Gynecol 199:514. e1-8.
Lopriore E, Deprest J, Slaghekke F, et al. 2008. Placental Character-istics in Monochorionic Twins With and Without Twin Anemia-Polycythemia Sequence. Obstet Gynecol 112: 753–758.
Lopriore E, Middeldorp JM, Oepkes D, Kanhai HH, Walther FJ,Vandenbussche FP. 2007. Twin anemia-polycythemia sequencein two monochorionic twin pairs without oligo-polyhydramniossequence. Placenta 28: 47–51.
Lopriore E, Sueters M, Middeldorp JM, Vandenbussche FP, WaltherFJ. 2005. Haemoglobin differences at birth in monochorionic twins
without chronic twin-to-twin transfusion syndrome. Prenat Diagn25: 844–850.
Mahieu-Caputo D, Dommergues M, Delezoide AL, et al. 2000. Twin-to-twin transfusion syndrome. Role of the fetal renin-angiotensinsystem. Am J Pathol 156: 629–636.
Mari G, Hanif F, Kruger M, Cosmi E, Santolaya-Forgas J, Tread-well MC. 2007. Middle cerebral artery peak systolic velocity: a newDoppler parameter in the assessment of growth-restricted fetuses.Ultrasound Obstet Gynecol 29: 310–316.
Robyr R, Lewi L, Salomon LJ, et al. 2006. Prevalence andmanagement of late fetal complications following successfulselective laser coagulation of chorionic plate anastomoses in twin-to-twin transfusion syndrome. Am J Obstet Gynecol 194: 796–803.
Senat MV, Deprest J, Boulvain M, Paupe A, Winer N, Ville Y. 2004.Endoscopic laser surgery versus serial amnioreduction for severetwin-to-twin transfusion syndrome. N Engl J Med 351: 136–144.
Van Mieghem T, Gucciardo L, Lewi P, et al. 2009. Validation ofthe fetal myocardial performance index in the second and thirdtrimesters of gestation. Ultrasound Obstet Gynecol 33: 58–63.
Copyright 2010 John Wiley & Sons, Ltd. Prenat Diagn 2010; 30: 438–442.DOI: 10.1002/pd