Embed Size (px)
Citation preview

Two Systemic Lupus Erythematosus Patients WithSevere Pleurisy: Similar Presentations, DifferentCausesCAROLINE M. GULATI,1 MICHAEL J. SATLIN,1 CYNTHIA M. MAGRO,1 AND KYRIAKOS A. KIROU2
CASE PRESENTATIONS
Case 1
History of the present illness. A 25-year-old womanwas diagnosed with systemic lupus erythematosus (SLE) 2years prior to admission, after she presented with fever,malaise, lymphadenopathy, arthritis, myalgias, malar rash,and positive serologies for antinuclear antibody (ANA)and anti–double-stranded DNA (anti-dsDNA). Additionalserology tests were negative for anti-Ro/SSA, anti-La/SSB,RNP, and Sm antibodies, as well as antiphospholipid an-tibodies (aPL). She was treated with intermittent coursesof glucocorticoids (GC) for disease flares. Eight monthsbefore admission, she had a severe flare that manifestedwith high fevers, weight loss, delirium, spastic bladder,and non-nephrotic proteinuria. She was ultimately diag-nosed with gray matter transverse myelitis of the conusmedullaris and lupus nephritis. She was treated aggres-sively with pulse GC and intravenous (IV) cyclophos-phamide (CYC), which led to resolution of all symptoms.After completion of a 6-month course of IV CYC, she wasmaintained on 20 mg of prednisone. One month prior toadmission, she was admitted to another hospital with left-sided pleurisy, dyspnea, and high fever. A chest computedtomography (CT) scan excluded pulmonary embolism, butshowed bilateral lung lower lobe consolidations withpleural effusions (left larger than right) and a small fluidcollection adjacent to her spleen. Her blood cultures grewSalmonella. Her symptoms improved with cefepime and
high-dose GC, and she was discharged home 2 weeks lateron 60 mg of daily prednisone and oral levofloxacin for atotal of 3 weeks of antibiotics. In addition, she was dis-charged on trimethoprim/sulfamethoxazole (TMP/SMX)160/800 mg 3 times weekly for Pneumocystis jirovecipneumonia (PCP) prophylaxis. One week before her cur-rent admission, she was started on 1,000 mg of mycophe-nolate mofetil (MMF) daily. She then presented to ourhospital with acute left-sided pleuritic chest pain, dys-pnea, and arthralgias. She did not have fever or cough.
Medical history. She had a history of mild asthma andhypothyroidism.
Family and social history. Her family history was un-remarkable except for a maternal aunt who also had SLE.There was no history of smoking, alcohol, or illicit druguse.
Medications. Her home medications included predni-sone 40 mg daily, MMF 500 mg twice daily, hydroxychlo-roquine (HCQ) 200 mg daily, TMP/SMX 160/800 mg 3times weekly, esomeprazole 40 mg, and levothyroxine 50�g daily. She was not taking any supplements.
Review of systems. She denied fevers, chills, cough,dyspnea, leg swelling, joint pain, skin rash, or oral ulcers.
Physical examination. She appeared to have Cushin-goid features, but was afebrile and not hypoxic. Her bloodpressure was 140/90 mm Hg and her heart rate was 90beats per minute. She had decreased breath sounds overher left lower lung field. She had a normal cardiac exam-ination and no hepatosplenomegaly, lymphadenopathy,rashes, or ulcers. She had a normal neurologic examina-tion and no joint swelling or tenderness.
Laboratory and radiologic evaluation with hospitalcourse. Her initial blood tests are shown in Table 1. Shehad non-nephrotic proteinuria and microscopic hematuriawithout a rise in her baseline creatinine level. A kidneybiopsy was not performed because her nephritis appeared
Supported by the Mary Kirkland Center for Lupus Re-search.
1Caroline M. Gulati, MD, Michael J. Satlin, MD, CynthiaM. Magro, MD: New York Presbyterian Hospital and WeillCornell Medical College, New York; 2Kyriakos A. Kirou,MD: Hospital for Special Surgery, New York, New York.
Dr. Kirou has received consultant fees (less than $10,000)from Exagen Diagnostics.
Address correspondence to Kyriakos A. Kirou, MD, MaryKirkland Center for Lupus Research, Hospital for SpecialSurgery, 535 East 70th Street, New York, NY 10021. E-mail:[email protected].
Submitted for publication November 28, 2012; accepted inrevised form February 12, 2013.
Arthritis Care & ResearchVol. 65, No. 6, June 2013, pp 1005–1013DOI 10.1002/acr.21988© 2013, American College of Rheumatology
CLINICOPATHOLOGIC CONFERENCE
1005

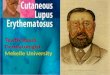
mild and the results were unlikely to change her manage-ment. CT imaging of the chest, abdomen, and pelvis againexcluded pulmonary embolism, but showed a left-sidedpleural effusion with adjacent lung consolidation and aparasplenic fluid collection. Her pleural fluid was sampledand showed an exudative process with a neutrophilic in-flammatory response (Table 1) without organisms on Gramstain or culture. A transthoracic echocardiogram was nor-mal. Her GC dose was increased to 16 mg of IV methyl-prednisolone (IVMP) every 8 hours and she received anadditional 500 mg dose of IVMP. MMF was continued atthe same dose. IV oxacillin was initiated after 1 of 2 sets ofblood cultures grew Staphylococcus warneri. Despitethese interventions, her symptoms did not improve. Bron-choscopy was performed 9 days after admission and bron-choalveolar lavage (BAL) yielded nonbloody, cellular,frothy fluid. The fluid was negative for bacterial, fungal,and mycobacterial pathogens, but was positive for influ-enza A by polymerase chain reaction (PCR). Oseltamivirwas prescribed for a 5-day course. Transbronchial biopsies(TBBX) were unable to be performed because of hypoxiaduring the procedure. Her abdominal fluid was sampledon day 14 by CT guidance to exclude an abscess andshowed serosanguinous fluid, consistent with serositis.She had a repeat chest CT scan 16 days after admissionthat showed loculations within a moderate left pleuraleffusion and an unchanged left lower lobe consolidationdespite high-dose GC, IV oxacillin, and oseltamivir (Figure1A). The patient underwent video-assisted thoracoscopicsurgery (VATS) 21 days after admission for a more defin-itive diagnosis.
Case 2
History of the present illness. A 23-year-old womanwas diagnosed with SLE 10 months before admission, aftershe presented with high fever, malaise, and alopecia. Shewas found to have pancytopenia, a pericardial effusion,and International Society of Nephrology/Renal PathologySociety class IV-G (A) lupus nephritis based on renal bi-opsy. Her serologic tests showed low complement levels,as well as antibodies to dsDNA, SSA, SSB, RNP, and Sm.aPL tests were negative. She improved after treatment withhigh-dose GC and one dose of IV CYC, and was started onMMF maintenance therapy. Four months before admis-sion, while receiving prednisone 15 mg daily, she devel-oped autoimmune hemolytic anemia. Her prednisone dos-age was increased to 50 mg/day and HCQ was added to herregimen. Eight weeks before admission, she developed anew severe left-sided pleuritic chest pain that promptedadmission at another hospital. She was noted to have aperipheral mass-like left lower lobe pulmonary infiltrateon a chest CT scan. She underwent a CT-guided needlebiopsy that revealed “organizing pneumonia with diffusealveolar damage.” She was treated with a short course ofIV antibiotics, her prednisone dosage was increased from35 mg to 50 mg/day, and MMF was continued. One weekafter discharge, her chest pain worsened and she wasreadmitted and treated with IV vancomycin and piperacil-lin tazobactam, followed by oral levofloxacin, for a total of10 days of antibiotics. After initial improvement, her pleu-ritic chest pain returned and she developed a new drycough, prompting her first admission to our hospital. Her
Table 1. Laboratory values at initial presentation*
Case 1 Case 2Normalvalues
WBC count, � 103/�l 11.5 9.8 3.5–10.7Absolute lymphocyte count, � 103/�l 0.3 0.2 0.9–5.2Hemoglobin, gm/dl 9.7 11.3 11.5–16Platelet count, � 103/�l 275 160 160–400Creatinine, mg/dl 1.3 1.62 0.44–1.03Albumin, mg/dl 2.7 3.3 3.5–4.8Globulin, mg/dl 2.9 1.8 1.8–3.3LDH, IU/liter 264 209 105–333ESR, mm/hour 86 46 4–20Complement C3, mg/dl 71 109 79–152Complement C4, mg/dl 30 29 16–38Anti-dsDNA Positive Negative NegativeUrine protein:creatinine ratio, gm 1.78 0.76 �0.2Urine RBC count, per hpf 17 22 0–4Urine WBC count, per hpf 8 5 0–5Pleural fluid
LDH, IU/liter 274 280Total protein, mg/dl 3.2 2.9Glucose, mg/dl 107 120pH 7.5 7.5RBC count, per �l 30,000 1,530WBC count, per �l 21,000 2,850Neutrophils, % 81 81Cytology Reactive mesothelial cells
* WBC � white blood cell; LDH � lactate dehydrogenase; ESR � erythrocyte sedimentation rate;anti-dsDNA � anti–double-stranded DNA; RBC � red blood cell; hpf � high-power field.
1006 Gulati et al

chest CT scan showed a left lower lobe and inferior lingu-lar lung consolidation with additional foci of more nodu-lar consolidations (increased since 5 weeks earlier). Inaddition, there were right upper lobe scattered ground-glass densities and a small loculated left-sided pleuraleffusion that was not large enough to be sampled (Figure1B). She was started empirically on IV vancomycin andpiperacillin tazobactam, TMP/SMX was initiated for PCPprophylaxis, and her prednisone (50 mg/day), MMF, andHCQ doses were unchanged. Bronchoscopy with BAL wasperformed and yielded nonbloody, frothy fluid. Lavagestudies revealed rhinovirus by PCR and 16,000 copies/mlof cytomegalovirus (CMV) DNA. Pathology from a fluoro-scopically guided TBBX showed lymphocytic infiltrationof the interstitium. There was also focal fibrin depositionwithin septal and alveolar spaces. On direct immunofluo-rescence (DIF), there was IgG, IgA, IgM, C3, C1q, fibrino-gen, and C5b–9 granular staining within the septa andseptal capillaries. There were no intracellular inclusionsto suggest CMV infection. The pathology findings wereinterpreted as interstitial pneumonitis with significantseptal capillary injury due to SLE. Blood and sputumcultures, as well as bacterial, fungal, Pneumocystis, andmycobacterial stains and cultures of the BAL fluid andbiopsy material, were negative. In addition, Histoplasma
and Legionella urinary antigens, galactomannan and cryp-tococcal serum antigens, and QuantiFeron-TB Gold testingwere negative. Because of persistent pleurisy, she wastreated with 1,000 mg of IVMP daily for 3 days, 750 mg ofIV CYC for 1 day, and 1,000 mg of IV rituximab for 1 day,and was discharged the next day. She was also placed onvalganciclovir for the CMV detected on BAL fluid. The dayafter discharge, she developed rapid deterioration of herleft chest pain and dyspnea and was readmitted to ourhospital.
Medical history. She had no significant medical historyexcept for her SLE and complications of the disease, in-cluding chronic kidney disease with a baseline creatininelevel of 1.6 mg/dl, autoimmune hemolytic anemia, lym-phopenia, and arthralgias.
Family and social history. There was no family historyof SLE or other autoimmune diseases. She had no historyof smoking, alcohol, or illicit drug use.
Medications. Her home medications included predni-sone 40 mg daily, HCQ 200 mg daily, TMP/SMX 80/400mg daily, as well as carvedilol 12.5 mg twice daily, sim-vastatin 20 mg once daily, darbepoetin alfa, omeprazole 40mg once daily, risedronate, calcium, and vitamin D.
Review of systems. She denied fevers, chills, or nightsweats. Her weight was stable. She experienced throatpain and was found to have thrush. She had no rash,arthritis, or lymphadenopathy.
Physical examination. She appeared to have Cushin-goid features and seemed acutely ill. Her blood pressurewas 110/60 mm Hg and her heart rate was 115 beats perminute and regular. She was afebrile, but hypoxic to 85%on room air. She had decreased breath sounds and a rub atthe left lung base. She had a normal cardiac and abdominalexamination. She had no rashes except for some acne dueto GC. She was neurologically intact and had no signs ofsynovitis on joint examination.
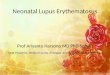
Laboratory and radiographic evaluation with hospitalcourse. Laboratory tests upon her initial admission areshown in Table 1. She had anemia with mild renal insuf-ficiency (at her baseline). She had mild proteinuria andmicroscopic hematuria. Her blood cultures were negative.A chest radiograph showed near complete opacification ofthe left hemithorax with a rightward mediastinal shift(Figure 2). A chest CT scan showed a large partially locu-lated left pleural effusion with near complete collapse ofher left lung, a small right pleural effusion, and small tomoderate pericardial effusion. She was started empiricallyon IV piperacillin tazobactam, her prednisone dosage wasdecreased to 20 mg/day, and TMP/SMX prophylaxis andHCQ were continued. A chest tube was placed to drain herenlarging pleural effusion. Fluid analysis showed an exu-dative process, normal complement levels, and a negativeANA. No lupus erythematosus cells were found. Pleuralfluid Gram, potassium hydroxide, and acid-fast stains
Figure 1. A, Consolidation with loculated effusion in case 1. B,Dense nodular consolidations within larger consolidation of theleft lower lobe in case 2. Smaller nodules were seen near thehilum and subpleurally. Associated pleural and pericardial effu-sions are shown.
Clinicopathologic Conference 1007

were negative and blood and urine cultures were negative.CMV from plasma showed 201 copies of DNA per ml.Given the size of the effusion, progressive hypoxia, andlack of a diagnosis, VATS was performed 6 days afteradmission for decortication and biopsies of the lung andpleura.
Case summariesBoth cases describe patients with severe SLE requiringheavy immunosuppression who developed severe pleu-risy while receiving high doses of GC and had concurrentloculated pleural effusions with lung consolidation. Pleu-ral fluid analyses revealed exudative and neutrophilic in-flammatory responses without evidence of empyema.Given their immunosuppression, there was concern forinfection in both cases. Case 1 had just recovered from asystemic infection with Salmonella, had evidence of in-fluenza infection in her BAL fluid, had one positive bloodculture for coagulase-negative staphylococci, and did notrespond to antiinfluenza and antistaphylococcal therapies.Case 2 had a more chronic course of pleurisy but an acuteexacerbation after pulse GC therapy. In addition, case 2had nodular consolidations on imaging that were of con-cern for infection and evidence of CMV reactivation inBAL fluid and plasma. Both cases had evidence for activeSLE with pleurisy, as well as active lupus nephritis withproteinuria and active urinary sediment. In addition, case2 had evidence for interstitial pneumonitis with septalcapillary injury and immune deposits that were consistentwith lupus pneumonitis.
DIFFERENTIAL DIAGNOSIS
InfectionsBoth patients had severe SLE and presented with painfulpleural effusions and lung consolidation while being se-verely immunosuppressed. The foremost differential diag-nosis in this clinical context is infection versus activelupus. Pulmonary infections are common in patients withSLE and should be a primary consideration in an SLEpatient presenting with respiratory symptoms. Patientswith SLE may be profoundly immunocompromised be-
cause of immunosuppressive medications and immuno-dysregulation associated with their underlying disease (1).Both patients had been receiving prolonged courses ofhigh-dose GC and also had received other immunosup-pressive agents such as IV CYC and MMF. They were alsoseverely lymphopenic (Table 1), likely related to GC andtheir underlying disease. Their immunocompromisedstates were highlighted by a recent history of salmonellosisin case 1 and CMV reactivation in case 2. Immunocompro-mised patients with SLE are at a high risk of pulmonaryinfections due to common bacteria, such as Staphylococ-cus aureus and Streptococcus pneumoniae, but also maybe at risk for opportunistic infections such as Mycobacte-rium tuberculosis, Nocardia, fungi (including Cryptococ-cus neoformans and Aspergillus), and P jiroveci (2–7). It isalso important to note that fever may be masked in patientsreceiving high doses of GC, and therefore the absence offever does not exclude infection.
SLE pleurisyPleurisy is the most common pulmonary manifestation ofSLE and occurs in 30–50% of patients (7). The presenta-tion varies and may consist of pleuritic chest pain alonewithout an effusion. Not infrequently, pleurisy is associ-ated with pericarditis (pleuropericarditis), which can alsopresent isolated. SLE pleurisy is thought to be caused byimmune complex deposition in vessels with subsequentcomplement activation and direct binding of anti-dsDNAantibodies to the mesothelium (8–10). Although rare, ef-fusions can be unilateral (10,11). Pleural fluid can be lym-phocytic or neutrophilic and typically has a pH �7.35, asin both of our cases (12). Complement, ANA, and anti-dsDNA levels can be measured in pleural fluid and arehelpful in assessing the role of SLE as a cause of pleuraleffusion (13,14). Pleural fluid ANA levels are nonspecific,since they may also be elevated in malignancy, but theyare sensitive. Therefore, the absence of pleural fluid ANAmakes it unlikely that SLE is the cause of a pleural effusion(15,16). On the other hand, the presence of either anti-dsDNA antibodies or lupus erythematosus cells (neutro-phils with ingested nuclear debris appearing as a homog-enous round inclusion) are diagnostic of SLE, but are not
Figure 2. Two days before (A) and 3 days after (B) pulse glucocorticoid therapy incase 2.
1008 Gulati et al

sensitive (17,18). In case 2, the pleural fluid was negativefor ANA and lupus erythematosus cells, providing evi-dence against SLE as the primary etiology of the effusion.These tests were not performed in case 1. The differentialdiagnosis of pleurisy in SLE is shown in Table 2.
Acute lupus pneumonitis (ALP)Other acute pulmonary manifestations of SLE include ALPand diffuse alveolar hemorrhage (DAH). ALP is relativelyuncommon, occurring in 1–12% of patients with SLE (19–23). The clinical presentation includes cough, pleurisy,dyspnea, hypoxia, and patchy infiltrates, often with bilat-eral consolidations that resemble “bronchopneumonia”(20,21,23). Given the indistinguishable clinical and radio-graphic presentation from infectious etiologies of pneumo-nia, establishing the diagnosis requires ruling out infec-tious processes, often necessitating bronchoscopy. Thehistopathology of ALP often shows nonspecific findings,such as diffuse alveolar damage with hyaline membranesand interstitial edema (4,19). The presence of vasculitisand hematoxylin bodies with pleuritis is thought to bemore specific for SLE-induced disease (4,19). DAH is themost severe acute pulmonary manifestation of SLE. Thesepatients typically present acutely, as in ALP, and oftenpresent with hemoptysis and a precipitous drop in hemo-globin. Imaging shows bilateral alveolar infiltrates andsequential BAL fluid reveals progressively more hemor-rhagic lavage aliquots. Cytology is notable for hemosider-in-laden macrophages. Our patients’ presentations and
BAL fluid did not suggest DAH, but they could have beenconsistent with ALP. Nevertheless, the largely unilaterallung involvement and lack of significant hypoxia providedevidence against ALP.
Chronic interstitial diseaseIn addition to these acute pulmonary manifestations, SLEis also associated with chronic interstitial lung disease,which is seen in 3–13% of patients and typically presentswith dry cough and dyspnea on exertion (7). Radiologicfindings include ground-glass and reticular infiltrates aswell as honeycombing. Associated histologic patterns in-clude nonspecific interstitial pneumonia, usual interstitialpneumonia and, less often, lymphocytic interstitial pneu-monia. In SLE, this entity is associated with anti-Ro anti-bodies (24–26). Magro et al have found evidence for mi-crovascular injury and IgG, IgA, and/or complementdeposition in septal capillaries in patients with chronicinterstitial lung disease in the setting of various collagenvascular diseases, including anti-Ro–positive SLE (25,26).The same authors also found reactivity in sera from thesepatients against endothelial cells and suggested a possiblepathogenic link between this antibody-mediated (Gell andCoombs type II immune reaction) microvasculopathy andpulmonary fibrosis (26). In addition to anti-Ro, other anti-bodies such as aPL have also been implicated. Similarmicrovascular injury and DIF findings were noted on theTBBX of case 2.
Other potential causesAnother important consideration when dealing with acutepleurisy in SLE is pulmonary embolism, especially whenpatients are positive for aPL or have other risk factors forthromboembolic disease. Both cases were negative for aPLand did not have other pulmonary embolism risk factors,such as intake of oral contraceptives or prolonged immo-bilization. In addition, pulmonary embolism was excludedby CT angiography in case 1, and the chronic presentationof case 2 with marked lung consolidation was not consis-tent with pulmonary embolism. Another consideration inthe differential diagnosis is malignancy, including bron-chial carcinoma or lymphoma. However, both of our pa-tients had disease courses that were marked by acute andsubacute flares of their pleurisy, providing evidenceagainst this diagnosis and in favor of either active SLE orinfection. The absence of lymphadenopathy on chest CTscan and a negative history for smoking also providedevidence against malignancy.
Comparison of casesIn case 1, influenza infection was identified. However,there was concern for an alternate disease process, partic-ularly given the dense consolidation and pleural effusion(both unusual in influenza), the lack of improvement withoseltamivir, and the broad infectious differential diagno-sis. The positive blood culture for S warneri was thought torepresent skin contamination because it grew in only oneset of blood cultures and coagulase-negative staphylococcido not typically cause pneumonia. The 2 most likely eti-
Table 2. Differential diagnosis of pleuritic chest painwith or without pleural effusion in patients with SLE*
1. SLE relatedLupus serositis (pleurisy or pericarditis)Acute lupus pneumonitisShrinking lung syndrome
2. Musculoskeletal pain in the rib cage, i.e.,costochondritis
3. Pulmonary embolism/infarction4. Infection related
Bacterial pneumonia (empyema or uncomplicatedparapneumonic effusion)
Atypical pneumonia (viral, Mycoplasma pneumoniae,Legionella species, Chlamydophila pneumoniae)
Pleural tuberculosisFungal disease (aspergillosis, histoplasmosis,
cryptococcosis, pneumocystis)Nocardia/ActinomycesSubphrenic abscess
5. Drug induced, including drug-induced lupus, i.e.,due to hydralazine, procainamide, etc.
6. Malignant or paramalignant effusions (non-Hodgkin’s lymphoma, primary lung cancer, etc.)
7. Selected miscellaneous causesUremic pleurisyPost–cardiac injury syndromeAscites (it may represent serositis due to SLE)Pancreatitis (acute or chronic)
* Effusions without pain may be due to nephrotic syndrome, hy-poalbuminemia, heart failure, atelectasis, trapped lung (due to pre-vious severe SLE pleurisy), etc. SLE � systemic lupuserythematosus.
Clinicopathologic Conference 1009

ologies of the presentation of case 1 were thought to besevere lupus pleurisy with compression atelectasis orpneumonia due to an unidentified pathogen with associ-ated parapneumonic effusion/empyema. VATS was there-fore undertaken to differentiate between these 2 possibil-ities.
In contrast to case 1, the infiltrates in case 2 appeared tobe true consolidations with distinct nodules. This radio-graphic appearance, as well as their chronicity and pro-gression over time, provided evidence for an infectioninstead of ALP. The acute clinical deterioration and wors-ening of the effusion after receiving pulse GC also sup-ported an infectious etiology. The chronic course of dis-ease was not typical of bacterial pneumonia, and nodularinfiltrates were more suggestive of fungal, mycobacterial,and Nocardia infection than PCP or viral processes. TheTBBX in case 2 revealed histologic and DIF features ofchronic interstitial lung disease (26). Her clinical and ra-diologic presentation, however, was not consistent withthis diagnosis. Therefore, it was unclear if the pathologicfindings represented a concomitant chronic interstitiallung disease in a preclinical stage or were false-positive inthe setting of inflammation/immune response due to con-comitant infection.
DISEASE COURSE
Case 1The patient underwent VATS with decortication and bi-opsies were taken of the lung and pleura. Grossly, a mod-erate amount of serous fluid was identified in the pleuralspace and a thick pleural rind and pleural adhesions werealso found. The histology of the lung and pleura showedmild chronic interstitial lung disease and marked reactivefibrinous pleuritis, respectively (Figure 3). DIF showed IgGand IgM deposition and complement activation with cap-illary injury in interalveolar septa. The patient markedlyimproved after surgery. She was treated with 1 gm of pulseIVMP and rituximab (1,000 mg every 2 weeks for 2 doses)and was discharged on 2,000 mg per day of MMF and 40
mg of daily prednisone. Her infiltrate and effusion re-solved completely within a few months and she was ableto taper her prednisone to 10 mg daily at the last followup,7 months later.
Case 2The patient also underwent a VATS with decorticationand biopsies were taken of the lung and pleura. The lungwas strongly adherent to the diaphragm and chest well,requiring a lengthy blunt dissection. On gross inspection,the pleural surfaces, pericardium, and diaphragm werestudded with fibrous nodules (Figure 4). Biopsy samples ofboth the pleura and lung revealed a neutrophilic, suppu-rative, organizing granulomatous inflammatory responsewith necrotizing abscesses in the setting of a backgroundof capillary injury and fibrin deposition, as seen previ-ously on TBBX (Figures 5A and B). Gram stain of thepleura and pleural fluid revealed branching, beaded gram-positive rods (Figure 5C), and modified acid-fast Kinyounstain revealed partially acid-fast bacilli. Bacterial culturessubsequently grew Nocardia nova that eventually testedsusceptible to TMP/SMX and carbapenems. At the time ofher second admission to our hospital, it was noted that asputum culture that had been sent during her first admis-sion to our laboratory to detect Legionella had grownbeaded gram-positive rods. Unfortunately, the culture hadbeen discarded and was not available for further analysis.After the diagnosis of nocardiosis was made, she wasstarted on 15 mg/kg of daily TMP/SMX, divided into 3doses, and 500 mg of IV meropenem every 8 hours. Shecontinued to receive dual therapy for 6 weeks and thenwas transitioned to TMP/SMX oral monotherapy for 1year. A magnetic resonance image of her brain was normal.The patient improved rapidly with complete resolution ofinfiltrate and effusion within a few months.
DISCUSSION
These cases describe young women with SLE who pre-sented with pleuritic chest pain, pleural effusion, andpulmonary infiltrate. This is a relatively common clinicalscenario encountered by physicians who care for patients
Figure 3. Fibrinoid pleuritis with pleural edema and extensivedeposition of fibrin on the pleural surface in case 1.
Figure 4. Intraoperative granulomas (arrows) noted on the peri-cardium and diaphragm in case 2.
1010 Gulati et al

with SLE, and our cases offer several instructive points fortheir management. Differentiating active lupus from infec-tion is the main challenge in such cases. This can be verydifficult, since typically many of these patients have activelupus and at the same time are markedly immunosup-pressed. A meticulous microbiologic evaluation for infec-tion, including opportunistic infection, should be per-formed in all cases. This often requires thoracentesis toobtain pleural fluid and bronchoscopy to obtain BAL fluidand TBBX samples. If these tests are negative but there isstill a strong suspicion for infection as in our cases, VATSmay provide a more definitive diagnosis (SLE-associatedfibrinous pleuritis in case 1 and Nocardia infection in case2).
Adding to the diagnostic challenge, GC, especially atrelatively high doses as in our cases, both alter the presen-tation of infections and increase the spectra of possibleinfectious etiologies. GC impair both innate and acquiredimmunity and impair the generation of inflammatory ex-udates by decreasing the production of various proinflam-matory mediators (27). Clinically, these effects are mani-fested by a decreased febrile response and decreased lunginfiltrates and effusions. The fact that the pleural fluid incase 2 did not have clear features of empyema was possi-bly related to an antiinflammatory GC effect. Nevertheless,despite high doses of GC, there was still substantial in-flammation with development of adhesions and locula-tions of pleural fluid not only in case 2, but also in case 1,
in which the effusion was not due to infection, but ratherto SLE itself.
The risk of Nocardia infection is significantly increasedin immunocompromised patients, and GC are an indepen-dent risk factor for nocardiosis (28,29). Lung infectionscaused by Nocardia can manifest as single or multiplelung nodules, reticulonodular infiltrates, lobar consolida-tions with or without cavitation, and pleural effusions(30,31). Therefore, nocardiosis should be considered inimmunosuppressed patients with SLE, particularly thosereceiving high doses of GC who have unexplained pulmo-nary infiltrates. The lack of growth of Nocardia on BALfluid and TBBX cultures in case 2 demonstrates the fastid-ious nature of Nocardia and the difficulty in cultivatingthese organisms by conventional cultures. These proper-ties explain why the time from onset of symptoms untildiagnosis of pulmonary nocardiosis is typically more than1 month (32). In case 2, the initiation of prophylacticTMP/SMX 2 days prior to the bronchoscopy may also havedecreased the culture yield. If infection with Nocardia issuspected, clinicians should ask the microbiology labora-tory to perform a modified acid-fast stain on respiratoryspecimens that uses a weaker acid as a decolorizer ratherthan a full acid-fast stain. This modification to the conven-tional acid-fast stain allows the moderately acid-fast No-cardia to retain the initial stain and to be visualized (33).Although routine aerobic culture media can support No-cardia, clinicians can also ask for selective media, such as
Figure 5. A, Areas of neutrophilic and granulomatous inflammation consistent withan infectious-based etiology in case 2. Adjacent areas of morphologic pattern thatcould be interpreted as changes of lupus pneumonitis based on the pattern of pauci-cellular septal and intraalveolar fibrin deposition are shown. B, Septal and intraal-veolar fibrin deposition accompanied by red cell extravasation. The process is pauci-inflammatory. Overall, the pattern of parenchymal injury is characteristic for a Gelland Coombs type II immune reaction targeting the endothelium. Immunohistochem-istry showed prominent granular deposition of IgG within the septa of the lungs,largely localized to the septal capillaries compatible with an anti–endothelial cellantibody reaction pattern. There was also prominent granular deposition of C5b–9within the septa. C, Gram-positive branching rods are seen in pleural fluid, consistentwith Nocardia.
Clinicopathologic Conference 1011

buffered charcoal yeast extract that is used to isolate Le-gionella. These media are beneficial to support Nocardiabecause they decrease the overgrowth of other organismsin specimens obtained from nonsterile sites (33). In case 2,a sputum specimen obtained before initiation of TMP/SMX prophylaxis during her initial hospitalization in ourinstitution that was sent for Legionella culture grew gram-positive rods, which was the first clue that suggested no-cardiosis. This case also highlights that Nocardia are not acomponent of the normal respiratory flora and should beconsidered a pathogen when grown from any respiratoryspecimen (33). Finally, if Nocardia are suspected, the mi-crobiology laboratory should be instructed to hold respi-ratory specimens for an extended period of time. Respira-tory cultures are often discarded at 48–72 hours, andNocardia often require a longer incubation period to grow(33).
Although there are no randomized trials to determinethe optimal treatment of nocardiosis, sulfonamides, suchas TMP/SMX, are considered the standard of therapy.However, most authorities recommend initial combinationtherapy, particularly given recent reports of emerging re-sistance to TMP/SMX (34,35). Although clinical improve-ment is typically noted within 2 weeks of initiating ther-apy, prolonged antibiotic courses of up to 12 months arerecommended because of high rates of relapse. Nocardiaoften invade blood vessels and have a propensity to causebrain infections. In fact, the central nervous system (CNS)is the most common extrapulmonary location for nocardi-osis (28). Therefore, any symptoms of CNS disease warrantbrain imaging to exclude brain abscess, and many author-ities recommend brain imaging in all immunocompro-mised hosts with Nocardia (34). Fortunately, case 2 didnot have CNS lesions on imaging. Case 2 had a dramaticresponse to antibiotics and is expected to complete a fullyear of therapy with TMP/SMX.
Mild pleurisy due to active SLE is treated first withnonsteroidal antiinflammatory drugs (NSAIDs) (7). How-ever, if the presentation is severe (as in our cases), or if thepatient does not respond to NSAIDs in a few days, mod-erate to high doses of GC may be used (7). The most severecases may also be treated with IV pulse GC. In rare caseswhere GC cannot be tapered because of severe (such as inour case 1) or recurrent inflammation, other immunosup-pressive agents, such as azathioprine and MMF, may beneeded. Tetracycline or talc pleurodesis have been usedfor recurrent large effusions (7). Of note, uncontrolledpleural inflammation may lead to fibrothorax and trappedlung (7,36). Our case 1 responded dramatically to decorti-cation, supporting its therapeutic role in severe forms ofthis disease.
The discrepant diagnoses from these 2 similar case pre-sentations provide evidence for early consideration ofVATS to distinguish between infection and SLE-associ-ated pleurisy. Despite extensive evaluations with imaging,bronchoscopy, and pathology (using 2 different samplingtechniques in case 2, specifically, percutaneous CT-guidedneedle biopsy and TBBX), the correct diagnoses were notidentified and therefore, appropriate care was delayed. Notonly does VATS offer diagnostic value, it may have atherapeutic benefit (7,36). Case 1 improved rapidly after
VATS, before one would expect a benefit from rituximabor an increased dose of MMF. In case 2, the diagnosis wasnot made until VATS was performed. These cases high-light the important role of VATS in patients with SLE andpulmonary pathology of unclear etiology despite less in-vasive diagnostic procedures.
FINAL DIAGNOSIS
Case 1Marked reactive fibrinous pleuritis due to active SLE withcompression atelectasis of the adjacent lung. Mild chronicinterstitial lung disease due to SLE.
Case 2Pneumonia and empyema due to Nocardia nova infection.Possible interstitial lung disease due to SLE.
AUTHOR CONTRIBUTIONS
All authors were involved in drafting the article or revising itcritically for important intellectual content, and all authors ap-proved the final version to be published. Dr. Kirou had full accessto all of the data in the study and takes responsibility for theintegrity of the data and the accuracy of the data analysis.Study conception and design. Gulati, Magro, Kirou.Acquisition of data. Gulati, Satlin, Magro, Kirou.Analysis and interpretation of data. Gulati, Magro, Kirou.
REFERENCES
1. Zandman-Goddard G, Shoenfeld Y. Infections and SLE. Au-toimmunity 2005;38:473–85.
2. Ruiz-Irastorza G, Olivares N, Ruiz-Arruza I, Martinez-Ber-riotxoa A, Egurbide MV, Aguirre C. Predictors of major infec-tions in systemic lupus erythematosus. Arthritis Res Ther2009;11:R109.
3. Chen HS, Tsai WP, Leu HS, Ho HH, Liou LB. Invasive fungalinfection in systemic lupus erythematosus: an analysis of 15cases and a literature review. Rheumatology (Oxford) 2007;46:539–44.
4. Quadrelli SA, Alvarez C, Arce SC, Paz L, Sarano J, SobrinoEM, et al. Pulmonary involvement of systemic lupuserythematosus: analysis of 90 necropsies. Lupus 2009;18:1053–60.
5. Jick SS, Lieberman ES, Rahman MU, Choi HK. Glucocorticoiduse, other associated factors, and the risk of tuberculosis.Arthritis Rheum 2006;55:19–26.
6. Lionakis MS, Kontoyiannis DP. Glucocorticoids and invasivefungal infections. Lancet 2003;362:1828–38.
7. Kamen DL, Strange C. Pulmonary manifestations of systemiclupus erythematosus. Clin Chest Med 2010;31:479–88.
8. Balbir-Gurman A, Yigla M, Nahir AM, Braun-Moscovici Y.Rheumatoid pleural effusion. Semin Arthritis Rheum 2006;35:368–78.
9. Guo H, Leung JC, Chan LY, Chan TM, Lai KN. The pathoge-netic role of immunoglobulin G from patients with systemiclupus erythematosus in the development of lupus pleuritis.Rheumatology (Oxford) 2004;43:286–93.
10. Man BL, Mok CC. Serositis related to systemic lupuserythematosus: prevalence and outcome. Lupus 2005;14:822–6.
11. Swigris JJ, Fischer A, Gillis J, Meehan RT, Brown KK. Pulmo-nary and thrombotic manifestations of systemic lupus ery-thematosus. Chest 2008;133:271–80.
12. Segal AM, Calabrese LH, Ahmad M, Tubbs RR, White CS. Thepulmonary manifestations of systemic lupus erythematosus.Semin Arthritis Rheum 1985;14:202–24.
1012 Gulati et al

13. Toworakul C, Kasitanon N, Sukitawut W, Wichinun R, Lou-threnoo W. Usefulness of pleural effusion antinuclear anti-bodies in the diagnosis of lupus pleuritis. Lupus 2011;20:1042–6.
14. Good JT Jr, King TE, Antony VB, Sahn SA. Lupus pleuritis:clinical features and pleural fluid characteristics with specialreference to pleural fluid antinuclear antibodies. Chest 1983;84:714–8.
15. Wang DY, Yang PC, Yu WL, Kuo SH, Hsu NY. Serial antinu-clear antibodies titre in pleural and pericardial fluid. EurRespir J 2000;15:1106–10.
16. Swissa M, Amital-Teplizki H, Haim N, Cohen Y, Shoenfeld Y.Autoantibodies in neoplasia: an unresolved enigma. Cancer1990;65:2554–8.
17. Halla JT, Schrohenloher RE, Volanakis JE. Immune complexesand other laboratory features of pleural effusions: a compar-ison of rheumatoid arthritis, systemic lupus erythematosus,and other diseases. Ann Intern Med 1980;92:748–52.
18. Riska H, Fyhrquist F, Selander RK, Hellstrom PE. Systemiclupus erythematosus and DNA antibodies in pleural effu-sions. Scand J Rheumatol 1978;7:159–60.
19. Haupt HM, Moore GW, Hutchins GM. The lung in systemiclupus erythematosus: analysis of the pathologic changes in120 patients. Am J Med 1981;71:791–8.
20. Mayberry JP, Primack SL, Muller NL. Thoracic manifestationsof systemic autoimmune diseases: radiographic and high-res-olution CT findings. Radiographics 2000;20:1623–35.
21. Matthay RA, Schwarz MI, Petty TL, Stanford RE, Gupta RC,Sahn SA, et al. Pulmonary manifestations of systemic lupuserythematosus: review of twelve cases of acute lupus pneu-monitis. Medicine (Baltimore) 1975;54:397–409.
22. Levin DC. Proper interpretation of pulmonary roentgenchanges in systemic lupus erythematosus. Am J RoentgenolRadium Ther Nucl Med 1971;111:510–7.
23. Murin S, Wiedemann HP, Matthay RA. Pulmonary manifes-tations of systemic lupus erythematosus. Clin Chest Med1998;19:641–65.
24. Hedgpeth MT, Boulware DW. Interstitial pneumonitis in an-tinuclear antibody–negative systemic lupus erythematosus: a
new clinical manifestation and possible association withanti–Ro (SS-A) antibodies. Arthritis Rheum 1988;31:545–8.
25. Magro CM, Crowson AN. The cutaneous pathology associatedwith seropositivity for antibodies to SSA (Ro): a clinicopath-ologic study of 23 adult patients without subacute cutaneouslupus erythematosus. Am J Dermatopathol 1999;21:129–37.
26. Magro CM, Ross P, Marsh CB, Allen JN, Liff D, Knight DA, etal. The role of anti-endothelial cell antibody-mediated micro-vascular injury in the evolution of pulmonary fibrosis in thesetting of collagen vascular disease. Am J Clin Pathol 2007;127:237–47.
27. Chatham WW, Kimberly RP. Treatment of lupus with corti-costeroids. Lupus 2001;10:140–7.
28. Beaman BL, Beaman L. Nocardia species: host-parasite rela-tionships. Clin Microbiol Rev 1994;7:213–64.
29. Peleg AY, Husain S, Qureshi ZA, Silveira FP, Sarumi M, ShuttKA, et al. Risk factors, clinical characteristics, and outcome ofNocardia infection in organ transplant recipients: a matchedcase-control study. Clin Infect Dis 2007;44:1307–14.
30. Mok CC, Yuen KY, Lau CS. Nocardiosis in systemic lupuserythematosus. Semin Arthritis Rheum 1997;26:675–83.
31. Palmer DL, Harvey RL, Wheeler JK. Diagnostic and therapeu-tic considerations in Nocardia asteroides infection. Medicine(Baltimore) 1974;53:391–401.
32. Martinez Tomas R, Menendez Villanueva R, Reyes Calzada S,Santos Durantez M, Valles Tarazona JM, Modesto Alapont M,et al. Pulmonary nocardiosis: risk factors and outcomes. Re-spirology 2007;12:394–400.
33. McNeil MM, Brown JM. The medically important aerobicactinomycetes: epidemiology and microbiology. Clin Micro-biol Rev 1994;7:357–417.
34. Wilson JW. Nocardiosis: updates and clinical overview. MayoClin Proc 2012;87:403–7.
35. Uhde KB, Pathak S, McCullum I Jr, Jannat-Khah DP, ShadomySV, Dykewicz CA, et al. Antimicrobial-resistant nocardia iso-lates, United States, 1995-2004. Clin Infect Dis 2010;51:1445–8.
36. Sharma S, Smith R, Al-Hameed F. Fibrothorax and severelung restriction secondary to lupus pleuritis and its success-ful treatment by pleurectomy. Can Respir J 2002;9:335–7.
Clinicopathologic Conference 1013