Embed Size (px)
Citation preview
1/25
UEMS PRM Section & Board
Clinical Affairs Committee
Template Version 2.1
Programme 12
PRM programme for patients with Spinal Cord Injury in the post-acute phase.
Issue
Version: 2.3
Date of the first version: 26/08/2013
Date of the last version: 23/08/2014
Accepted by 3 reviewers
Identification
Title MD
Family name NULLE
First name ANDA
Position CHAIR OF THE BOARD
HEAD OF THE SCI REHABILITATION PROGRAMME
Phone +371 67766124
Email [email protected]
Year of Board Certification 2013
Name of unit SCI REHABILITATION UNIT
Hospital (facility) NATIONAL REHABILITATION CENTRE “ VAIVARI”
Address ASARU PROSPEKTS 61
Post code LV2008
City JURMALA
Country LATVIA
2/25
Content
I. SUMMARY ....................................................................................................................................... 4
II. GENERAL FONDATIONS OF THE PROGRAMME ....................................................................... 5
A. PATHOLOGICAL AND IMPAIRMENT CONSIDERATIONS ...................................................................... 5 1. Aetiology ................................................................................................................................... 5 2. Natural history and relationship to impairment ......................................................................... 5 3. Diagnosis approach and prognosis ........................................................................................... 6 4. Impairment treatment principles ................................................................................................ 6
B. ACTIVITY LIMITATIONS AND PARTICIPATION RESTRICTIONS ............................................................. 6 C. SOCIAL AND ECONOMIC CONSEQUENCES ...................................................................................... 7
1. Epidemiological data ................................................................................................................. 7 2. Social data ................................................................................................................................ 7 3. Economic data .......................................................................................................................... 7
D. LEGAL FRAMEWORK ..................................................................................................................... 8
III. DESCRIPTION OF THE PROGRAMME...................................................................................... 9
A. ENVIRONMENT OF THE PROGRAMME ............................................................................................. 9 1. Clinical setting ........................................................................................................................... 9 2. Clinical programme ................................................................................................................... 9 3. Clinical approach ....................................................................................................................... 9 4. Facilities .................................................................................................................................... 9
B. TARGET POPULATION ................................................................................................................. 10 1. Inclusion criteria ...................................................................................................................... 10 2. Criteria for refusal .................................................................................................................... 10 3. Referrals of patients ................................................................................................................ 10 4. Stage of recovery before admission ....................................................................................... 10 5. Early management before admission ..................................................................................... 11
C. GOALS ...................................................................................................................................... 11 1. In terms of body structure and body function (impairment) .................................................... 11 2. Activities and participation ...................................................................................................... 12 3. In terms of participation ........................................................................................................... 12
D. CONTENT OF THE PROGRAMME .................................................................................................. 12 1. General scheme and time frame ............................................................................................. 12 2. Role of PRM specialist ............................................................................................................ 13 3. Specific role of each team member in SCI rehabilitation programme .................................... 13 4. Diagnostic and assessment tools ........................................................................................... 14 5. Specific therapeutic interventions ........................................................................................... 15 6. Assistive technology................................................................................................................ 15 7. Environment adaptation .......................................................................................................... 15
E. DISCHARGE PLANNING AND LONG TERM FOLLOW UP .................................................................... 16 1. Discharge criteria .................................................................................................................... 16 2. How patients are managed after the programme? ................................................................. 16
IV. ADDITIONAL INFORMATION ABOUT PRM ORGANISATION ............................................... 17
A. SAFETY AND PATIENT RIGHTS ..................................................................................................... 17 1. Safety ...................................................................................................................................... 17 2. Patient rights ........................................................................................................................... 17 3. Advocacy ................................................................................................................................. 17
B. PRM SPECIALISTS AND TEAM MANAGEMENT ............................................................................... 18 1. PRM Specialists in the Programme ........................................................................................ 18 2. Staff devoted to this programme ............................................................................................. 18 3. Team management ................................................................................................................. 19
C. INFORMATION MANAGEMENT ...................................................................................................... 19 1. Patient records ........................................................................................................................ 19 2. Data about general organization ............................................................................................. 19
3/25
3. Programme monitoring and outcomes .................................................................................... 20
V. QUALITY IMPROVEMENT ........................................................................................................ 22
A. WHAT ARE THE MOST POSITIVE POINTS OF YOUR PROGRAMME? .................................................. 22 B. WHAT ARE THE POINTS TO IMPROVE IN YOUR PROGRAMME? ........................................................ 22 C. WHAT ACTION PLAN DO YOU INTEND TO IMPLEMENT IN ORDER TO IMPROVE YOUR PROGRAMME? ... 22
1. Extrinsic conditions that you wish to obtain. ........................................................................... 22 2. Intrinsic improvement of the programme ................................................................................ 22
VI. REFERENCES ........................................................................................................................... 23
A. LIST OF REFERENCES ................................................................................................................ 23
4/25
I. Summary 1
2
Spinal cord injury (SCI) instantly changes the person’s life and the further consequences 3 affect the person him/herself, his/her family, relatives and society. 4
During the last 20 years a modern, comprehensive rehabilitation system for SCI patients 5 has been established in Latvia. One single SCI centre is sufficient for 2, 2 million 6 inhabitants of Latvia. Rehabilitation is provided by certified physical and rehabilitation 7
medicine physicians and rehabilitation professionals in multidisciplinary team approach. 8
Reported global incidence of traumatic SCI lies between 10.4 and 83 per million inhabitants 9 per year. (1)The median calculated from these data for the Western Europe region is 16 10 per million inhabitants per year. 11
Limited amount of data are available from Eastern Europe. 2) Data for Latvia is 12 approximately 25 traumatic SCI per million. 13
All SCI patients with rehabilitation potential are the target population for SCI rehabilitation 14 programme in NRC “Vaivari”. Rehabilitation starts in acute setting and continues in the 15 dedicated SCI rehabilitation programme in the National Rehabilitation centre „Vaivari”. The 16 main goal is to reintegrate SCI person back into the community. Rehabilitation usually 17 starts on the 10-14th day post injury, when the patient is medically stable and able to 18 participate in an intensive rehabilitation process. In case of serious complications, 19 rehabilitation is temporary suspended. 20
All patients are included in a long term continuous follow up program. The follow up is 21 usually implemented once a year after first rehabilitation course. 22
Rehabilitation team consists of experienced experts – PRM doctor, physiotherapist, 23 occupational therapist, nursing staff, psychologist, social worker and nutritionist. Other 24 necessary consultants, such as a technical orthopaedist, urologist, and surgeon are 25 available. First treatment for newly injured paraplegic people lasts for 45-60 days and 60-26 90 days for tetraplegic patients. During the next 21-28 days, a rehabilitation course is 27 performed shortly after the first one. A follow up programme, with a yearly control, starts 28 after discharge. 29
A multiprofessional team managed by a PRM doctor, works together with the patient and 30 his/her family to set realistic rehabilitation goals and provide relevant care. They do their 31 best to maximise recovery, to prevent avoidable complications and to achieve maximum 32 independence of SCI patients within the limitations of his/her disability. 33
Patients are assessed with International Standards of Neurological Classification of SCI 34 (ISNCSCI) and Spinal Cord Independence Measure (SCIM). Data are collected in a 35 uniform manner with respect to International SCI Date set, International SCI Lower Urinary 36 Tract Function Basic Data Set and Autonomic Standards Assessment form. 37
Specialists of our rehabilitation team perform an efficient, respectful and cost effective 38 model of SCI rehabilitation. 39
Cooperation with nongovernmental organizations and local government social services is 40 used to achieve the goals. Family members and their relatives are involved in the 41 rehabilitation process. 42
NRC “Vaivari” has been certified as a Training Centre by the European Board of PRM. This 43
SCI rehabilitation programme has been introduced into the curriculum of the University 44 study process for medical residents and functional specialists. Training of specialists is 45 carried out in NRC “Vaivari” SCI rehabilitation department. 46
47
5/25
II. General fondations of the Programme 1
Specialized SCI rehabilitation program provides comprehensive and patient-focused 2 rehabilitation services for inpatient, outpatient and follow-up care with aim to empower 3 people with SCI and their families to achieve optimal quality of life continuing into the 4 community (focusing on increasing self-reliance and gaining independence).(5) 5
Rehabilitation is provided by certified physician and rehabilitation professionals in 6 multidisciplinary team approach. 7
Patients with traumatic spinal cord injuries and patients with non-traumatic spinal cord 8 injuries benefitted from the same rehabilitation program in a SCI rehabilitation program. It is 9 effective to admit and rehabilitate patients with injuries resulting from both traumatic and 10 non-traumatic aetiologies in the same specialized setting. (7) 11
A. PATHOLOGICAL AND IMPAIRMENT CONSIDERATIONS 12
1. Aetiology 13
SCI can result from different mechanisms leading to tissue damage: 1) destruction by 14 direct trauma; 2) compression by bone fragments, hematoma, or disk material; 3) ischemia 15 from damage or impingement on the spinal arteries. (4) 16
The spinal cord can be radically disrupted by injury. But there are also many 17 heterogeneous conditions in causes and outcomes, which can result from contusion, 18 compression, penetration or maceration of the spinal cord. SCI leads to the death of cells, 19 including neurons, oligodendrocytes, astrocytes and precursor cells and any resulting 20 cavities and cysts may interrupt descending and ascending axonal tracts, although 21 circumferential white matter is often spared. (6) 22
SCI is a dynamic process. Immediate lesions of the nervous tissue can be followed by 23 secondary damage due to vasogenic oedema and anoxia of the spinal cord. In all acute 24 cord syndromes, the full extent of injury may be not initially apparent. Incomplete cord 25 lesions may evolve into more complete lesions. (4) 26
2. Natural history and relationship to impairment 27
Patients with SCI usually have permanent and often devastating neurologic deficits and 28 disability. (8) 29
The degree of motor and/or sensory loss is determined by the location and seriousness of 30 cord damage. ASIA Impairment Scale (AIS) is used in grading the degree of impairment: 31
A = Complete. No sensory or motor function is preserved in the sacral segments S4-S5. 32
B = Sensory incomplete. Sensory but not motor function is preserved below the 33 neurological level and includes the sacral segments S4-S5, and no motor function is 34 preserved more than three levels below the motor level on either side of the body. 35
C = Motor incomplete. Motor function is preserved below the neurological level and more 36 than half of key muscle functions below the single neurological level of injury have a 37 muscle grade less than 3 (Grades 0–2). 38
D = Motor incomplete. Motor function is preserved below the neurological level, and at 39 least half (half or more) of key muscle functions below the neurological level have a muscle 40 grade >3. 41
E = Normal. If sensation and motor function as tested with the ISNCSCI are graded as 42 normal in all segments, and the patient had prior deficits, then the AIS grade is E. 43 Someone without a SCI does not receive an AIS grade (9-13). 44
6/25
Besides those levels, special anatomic types consist of, incomplete SCI produce anterior, 1 posterior, central spinal cord injury, Brown-Sequard syndrome or conus medullaris and 2 cauda equina (horse-tail) syndromes. (9-13) 3
3. Diagnosis approach and prognosis 4
Functional outcomes may vary with individuals, depending on such factors as the level and 5 completeness of the injury, neurological recovery (or loss), associated medical 6 complications (pain, spasticity, contractures, cardiac disease, musculoskeletal injury), the 7 amount of rehabilitation training that the patient receives, the rehabilitation team's level of 8 expertise, as well as the patient's motivation, age, and family and financial resources. 9
An important objective of acute SCI rehabilitation is to maximize patient functional 10 outcomes. Completeness of injury and neurologic level of injury are important factors in 11 predicting functional outcomes after SCI. (23-24, 27) Incomplete SCI tend to indicate a 12 more favourable prognosis. Tetraplegia is clearly more functionally impairing than 13 paraplegia, depending on the degree of motor-sensory sparing. 14
Functioning prognosis is better if the time lapse from the injury to the rehabilitation 15 department admission is shorter. (15) 16
The more incomplete the injury is, especially on initial examination at 72 hours to 1 week 17 after the injury has occurred, the more favourable the potential for neurological recovery. 18
Neurological recovery usually plateaus in the first 3-6 months (although changes have 19 been reported more than one year after injury). The use of orthotics and assistive devices 20 can sometimes facilitate patient's functional abilities. (11-13) 21
Comprehensive and detailed neurological examinations that are yearly repeated form an 22 important component of patient assessment and of neurological and functional outcome 23 prediction. Key elements of the examination include motor and sensory testing, which allow 24 the designation of a neurological level of injury and of the completeness of injury. In 25 addition, rectal examination is required to assess motor and sensory functions of the pelvic 26 floor. (14) 27
4. Impairment treatment principles 28
When acute SCI occurs, the patient is transported to the emergency room and undergoes 29 operation, if necessary. After the vital signs and the patient status are stabilized, the 30 rehabilitation process can begin. In traumatic SCI, adequate timing of medical treatment 31 and rehabilitation is essential for the recovery of functioning. The concept of "post-acute 32 rehabilitation" can be understood as the rehabilitation process being initiated as soon as 33 possible after acute medical management. (15) 34
In the rehabilitation of SCI patients, specific therapies and management, such as physical 35 and occupational therapy, bladder and bowel management should be carried out 36 simultaneously. Medical treatments for symptoms including orthostatic hypotension, pain, 37 and spasticity, are also required. 38
Therefore, a comprehensive evaluation on the patient's medical, functional, and social 39 status is necessary before planning the rehabilitation goals. (5) In the comprehensive 40 evaluation of SCI, the problem list oriented approach is known to be more useful than the 41 individual approach by each rehabilitation team member. 42
43
B. ACTIVITY LIMITATIONS AND PARTICIPATION RESTRICTIONS 44
See chapter E, ICF codes d4-d9 45
7/25
C. SOCIAL AND ECONOMIC CONSEQUENCES 1
1. Epidemiological data 2
Data for Latvia is approximately 25 traumatic SCI per million inhabitants per year (*) 3
Reported worldwide incidence of SCI lies between 10.4 and 83 per million inhabitants per 4 year. (1) One-third of patients with SCI are reported to be tetraplegia and 50% of patients 5 with SCI to have a complete lesion. The average age of patients sustaining their injury at is 6 reported as 33 years old, and the sex distribution (men/women) as 3.8/1.The causes of 7 these injuries ranging from motor vehicle accidents and community violence to recreational 8 activities and workplace-related injuries.(1-3) Limited amount of data are available from 9 Eastern Europe. New Estonian data are combined with regional data for Russia show the 10 main causes of TSCI in Estonia and Russia (Novosibirsk and Saint Petersburg) were falls 11 (median 40%) and land transport (median 25%). (2) 12
In Western Europe, reported rates are: Denmark (9.2 per million), Finland (13.8 per 13 million), France 19.4 per million, Germany 10.7 per million, Greece 33.6 per million, 14 Greenland 26 per million, Iceland 20 per million, Ireland 13.1 per million, Italy 19 per 15 million, Israel 15.9 per million, Netherlands 7.5 per million, Norway 26.3 per million, Spain 16 12.1 per million, Switzerland 15 per million. The median calculated from these data for the 17 Western Europe region is 16 per million. (2) 18
2. Social data 19
Life expectancies for persons with SCI are still significantly below life expectancies for 20 those with no SCI and have not improved since the 1980’s. Mortality rates are significantly 21 higher during the first year after injury than during subsequent years, particularly for 22 severely injured people. In the past, the leading cause of death among people with SCI is 23 OR used to be renal failure. Today, the more frequent causes of death for this population 24 are pneumonia and septicaemia. (26) 25
Whether a person returns to work after SCI is greatly influenced by his/her educational 26 level. Although this is true for the general public, it is especially important for the SCI 27 population. The more educated a person is at the moment of injury, the more he/she is 28 likely to return to work. The rates of employment also depend of functional status. People 29 with paraplegia are employed more frequently (32.8%) than those with tetraplegia (24.7%). 30 More specifically, the chance to return to work for people needing ADL assistance (18.2%) 31 is less than a half of the chance for those who do not require assistance (42%). (16) 32
3. Economic data 33
SCI has an impact on multiple systems. SCI has been classified among the five most 34 expensive hospital diagnoses. SCI onset is life-changing and a lengthy program of SCI 35 rehabilitation is needed to train patients to use their remaining abilities and to support 36 “adjustment” to a changed body and life situation. (16) 37
Significant costs are incurred throughout the life of a person with SCI, including initial 38 hospitalization and acute rehabilitation, home and vehicle modifications, and recurring 39 costs for durable medical equipment, medications, supplies, and personal assistance. 40
The level and extent of injury are important factors contributing to first-year costs. People 41 with high tetraplegia incurred over 3 times the charges that people with incomplete motor 42 paraplegia. (16) 43
Health care financing per one resident in Latvia in 2012 was 227, 89 LVL (324.26 EUR) or 44 3.21% from gross domestic product (GDP) No data are accessible for one SCI patient 45 costs in the country. (28) 46
8/25
D. LEGAL FRAMEWORK 1
After a spinal cord injury, patients are usually admitted to spine surgery or neurosurgical 2 departments in University hospitals or regional hospitals. 3
Rehabilitation starts in acute setting and continues in the dedicated SCI rehabilitation 4 programme in the National Rehabilitation centre „Vaivari”. This usually starts on the 10-5 14th day post injury, when the patient is medically stable and able to participate in an 6 intensive rehabilitation process. In case of serious complications, rehabilitation is 7 temporary suspended. 8
First treatment for newly injured paraplegic people lasts for 45-60 days and 60-90 days for 9 tetraplegia patients. During the next 21-28 days, a rehabilitation course is performed 10 shortly after the first one. A follow up programme, with a yearly control, starts after 11 discharge. 12
The follow up program can be implemented on an in-patient or day hospital basis, more 13 rarely – in out-patient clinics. The follow-up program for inpatients lasts for 10 - 14 days 14 (maximum 21 days for high tetraplegia or complicated patients). 15
Patients’ rights are guaranteed in Constitution of the Republic of Latvia: “The State will 16 protect human health and guarantee a basic level of medical assistance for everyone”. (28) 17
Rehabilitation programs in National Rehabilitation centre “Vaivari” are financed by state, 18 patient has to pay the “patient’s fee” according to Regulations of the Cabinet of Ministers of 19 Latvia. 20
9/25
III. Description of the Programme 1
A. ENVIRONMENT OF THE PROGRAMME 2
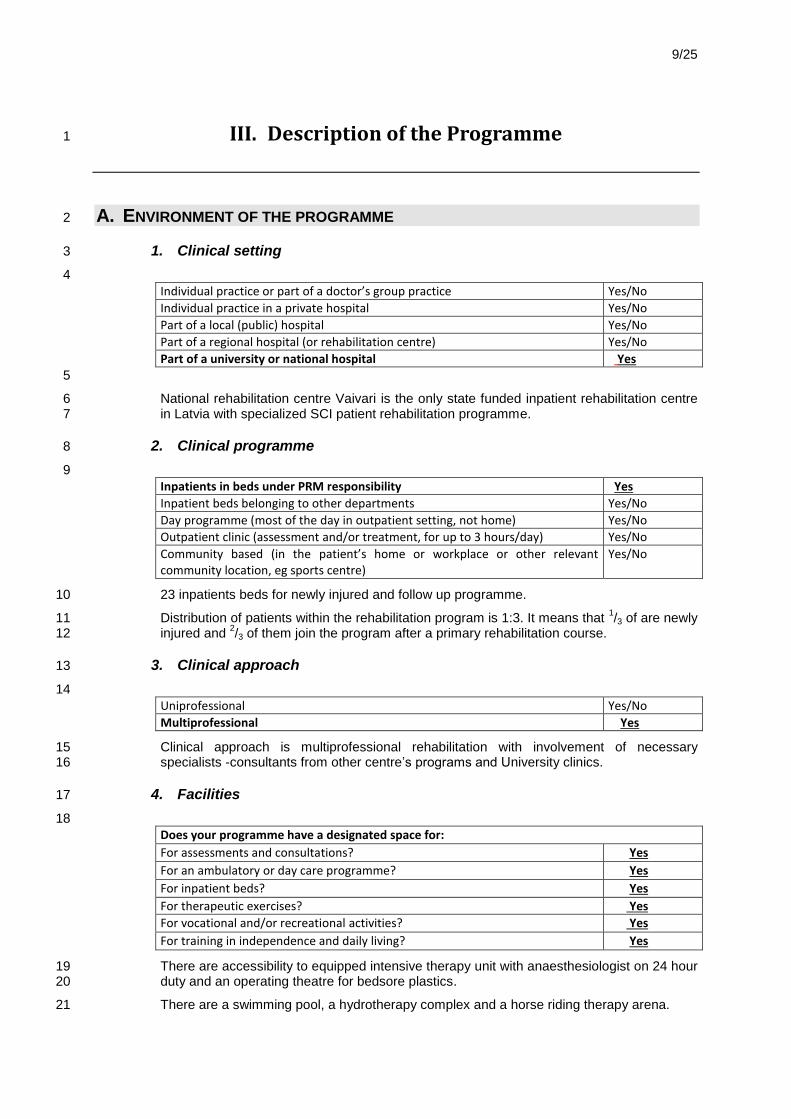
1. Clinical setting 3
4
Individual practice or part of a doctor’s group practice Yes/No
Individual practice in a private hospital Yes/No
Part of a local (public) hospital Yes/No
Part of a regional hospital (or rehabilitation centre) Yes/No
Part of a university or national hospital Yes
5
National rehabilitation centre Vaivari is the only state funded inpatient rehabilitation centre 6 in Latvia with specialized SCI patient rehabilitation programme. 7
2. Clinical programme 8
9
Inpatients in beds under PRM responsibility Yes
Inpatient beds belonging to other departments Yes/No
Day programme (most of the day in outpatient setting, not home) Yes/No
Outpatient clinic (assessment and/or treatment, for up to 3 hours/day) Yes/No
Community based (in the patient’s home or workplace or other relevant community location, eg sports centre)
Yes/No
23 inpatients beds for newly injured and follow up programme. 10
Distribution of patients within the rehabilitation program is 1:3. It means that 1/3 of are newly 11
injured and 2/3 of them join the program after a primary rehabilitation course. 12
3. Clinical approach 13
14
Uniprofessional Yes/No
Multiprofessional Yes
Clinical approach is multiprofessional rehabilitation with involvement of necessary 15 specialists -consultants from other centre’s programs and University clinics. 16
4. Facilities 17
18
Does your programme have a designated space for:
For assessments and consultations? Yes
For an ambulatory or day care programme? Yes
For inpatient beds? Yes
For therapeutic exercises? Yes
For vocational and/or recreational activities? Yes
For training in independence and daily living? Yes
There are accessibility to equipped intensive therapy unit with anaesthesiologist on 24 hour 19 duty and an operating theatre for bedsore plastics. 20
There are a swimming pool, a hydrotherapy complex and a horse riding therapy arena. 21
10/25
B. TARGET POPULATION 1
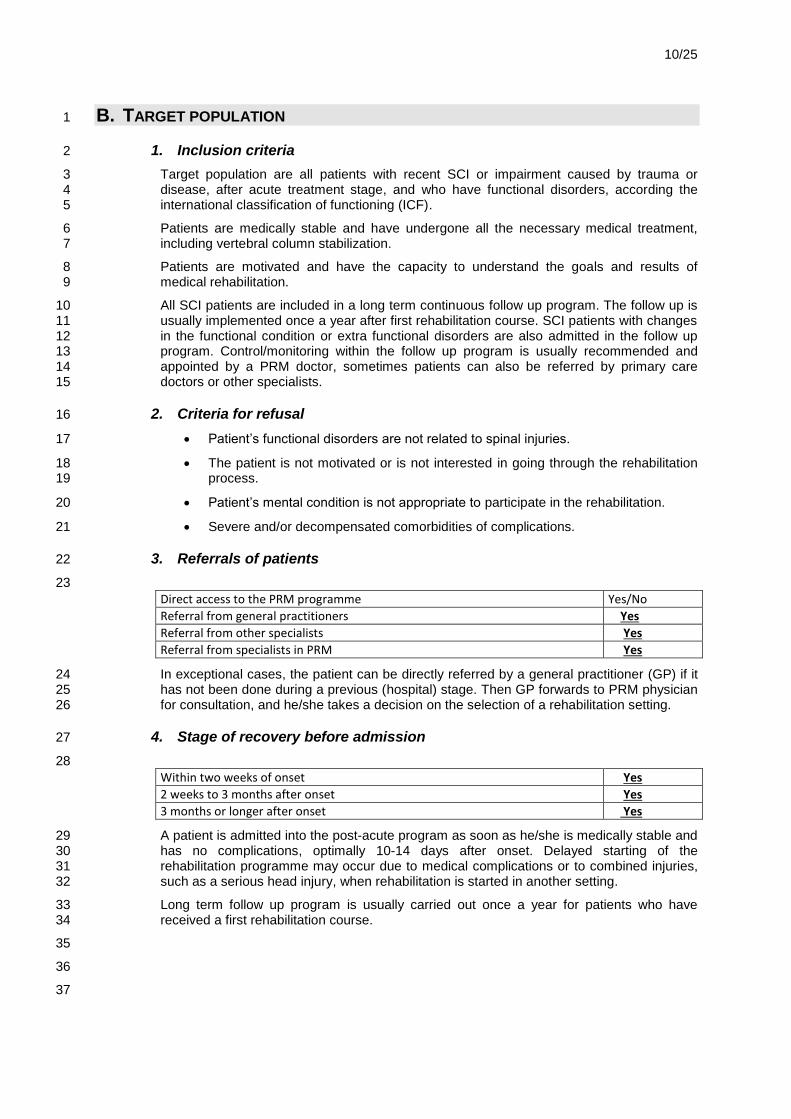
1. Inclusion criteria 2
Target population are all patients with recent SCI or impairment caused by trauma or 3 disease, after acute treatment stage, and who have functional disorders, according the 4 international classification of functioning (ICF). 5
Patients are medically stable and have undergone all the necessary medical treatment, 6 including vertebral column stabilization. 7
Patients are motivated and have the capacity to understand the goals and results of 8 medical rehabilitation. 9
All SCI patients are included in a long term continuous follow up program. The follow up is 10 usually implemented once a year after first rehabilitation course. SCI patients with changes 11 in the functional condition or extra functional disorders are also admitted in the follow up 12 program. Control/monitoring within the follow up program is usually recommended and 13 appointed by a PRM doctor, sometimes patients can also be referred by primary care 14 doctors or other specialists. 15
2. Criteria for refusal 16
Patient’s functional disorders are not related to spinal injuries. 17
The patient is not motivated or is not interested in going through the rehabilitation 18 process. 19
Patient’s mental condition is not appropriate to participate in the rehabilitation. 20
Severe and/or decompensated comorbidities of complications. 21
3. Referrals of patients 22
23
Direct access to the PRM programme Yes/No
Referral from general practitioners Yes
Referral from other specialists Yes
Referral from specialists in PRM Yes
In exceptional cases, the patient can be directly referred by a general practitioner (GP) if it 24 has not been done during a previous (hospital) stage. Then GP forwards to PRM physician 25 for consultation, and he/she takes a decision on the selection of a rehabilitation setting. 26
4. Stage of recovery before admission 27
28
Within two weeks of onset Yes
2 weeks to 3 months after onset Yes
3 months or longer after onset Yes
A patient is admitted into the post-acute program as soon as he/she is medically stable and 29 has no complications, optimally 10-14 days after onset. Delayed starting of the 30 rehabilitation programme may occur due to medical complications or to combined injuries, 31 such as a serious head injury, when rehabilitation is started in another setting. 32
Long term follow up program is usually carried out once a year for patients who have 33 received a first rehabilitation course. 34
35
36
37
11/25
5. Early management before admission 1
a) How are patients selected? 2
The patients are selected in the hospital by the attending surgeon or neurologist together 3 with the PRM doctor who performs the assessment of patient’s functioning disorders, 4 rehabilitation potential and indications, who designs the rehabilitation plans in the hospital 5 and for further rehabilitation, and who manages the transfer of the patient to the 6 rehabilitation centre. Occasionally, a general practitioner can send a patient to the PRM 7 doctor who then completes the assessment of the functioning disorders, potential, 8 indications and admits the patient to the rehabilitation programme. 9
b) Do patients benefit from PRM advice in acute settings? 10
At the University Clinics, specialized and regional hospitals the PRM services are 11 accessible where patients are consulted and the rehabilitation course has been started in 12 the acute stage and then the patient is sent for further rehabilitation within a specialized 13 programme. 14
c) What alternate solutions are proposed to refused patients? 15
The refused patients continue the medical treatment and the stabilization of health 16 conditions in the hospital. They take treatment of comorbidities and complications in the 17 hospital setting. Then, they are oriented to Long term Care hospitals or Social Care Centre 18 without intensive rehabilitation or they return back home where they are under the care of 19 their general practitioner and their family. 20
C. GOALS 21
22
Main goals of the programme are: 23
to reduce impairment 24
to provide improvement of functional abilities in activity and participation domains 25
to help the patient to return to productive life, 26
to prevent secondary complications and avoid rehospitalisation 27
to realize educational program for persons with SCI and caregivers 28
There is a large variety of functional problems reflecting the complexity of SCI. The ICF can 29 provide a comprehensive framework for the description of functional health in individuals 30 with SCI worldwide. (21-22) 31
32
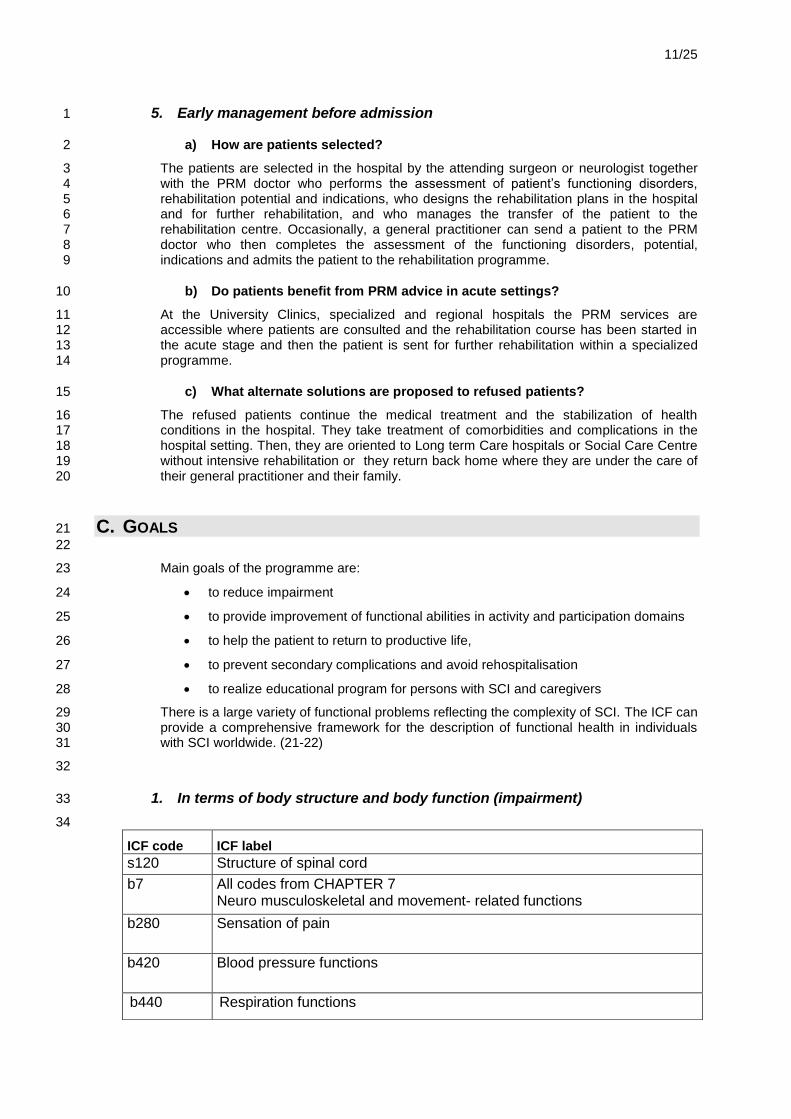
1. In terms of body structure and body function (impairment) 33
34
ICF code ICF label
s120 Structure of spinal cord
b7 All codes from CHAPTER 7 Neuro musculoskeletal and movement- related functions
b280 Sensation of pain
b420 Blood pressure functions
b440 Respiration functions
12/25
In the body structures domain, the relevant item was the spinal cord and related structures 1 (s120). In the body function domain, muscle power functions, urination functions, 2 defecation functions, and sensation of pain were frequently mentioned. These items 3 involve problems which most of the SCI patients suffer from. This is directly influenced by 4 the spinal cord injury itself. (21-22) 5
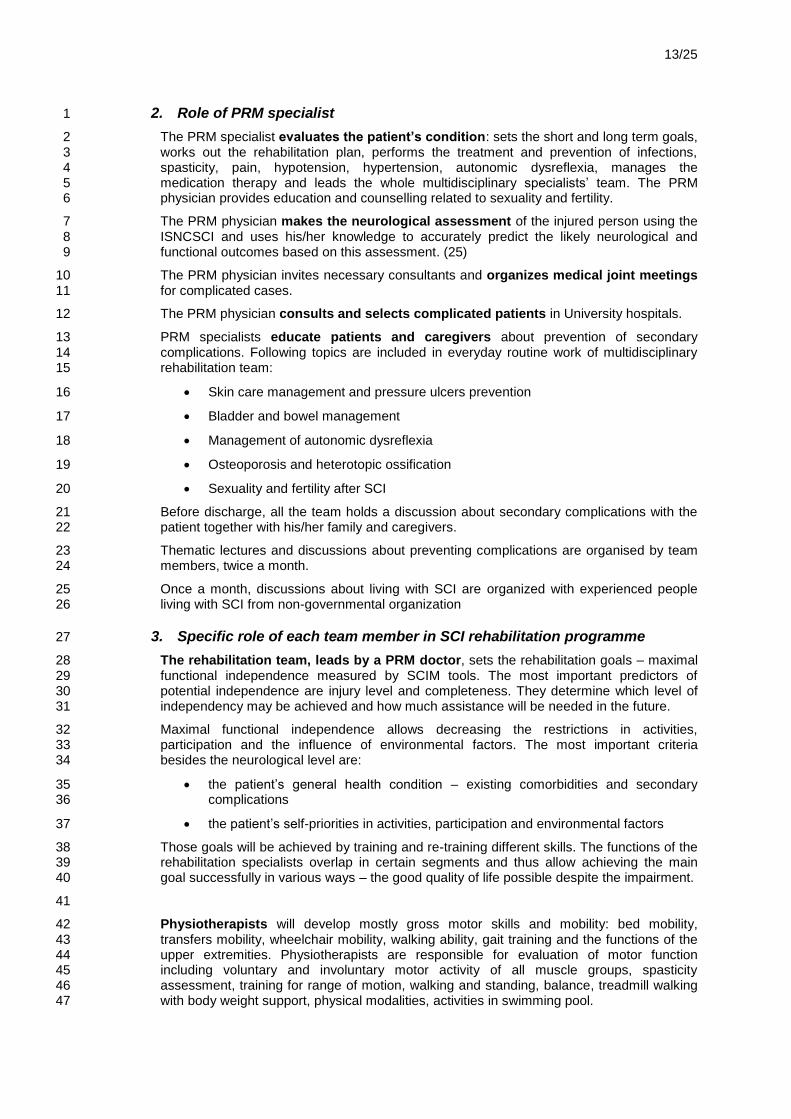
2. Activities and participation 6
7
ICF code ICF label
d4 all codes from Chapter 4 Mobility
d5 All codes from Chapter 5 Self-care
d620 Acquisition of goods and services
d630 Preparing meals
d640 Doing housework
d650 Caring for household objects
3. In terms of participation 8
9
ICF code ICF label
D770 Intimate relationships
D845 Acquiring, keeping, terminating a job
D920 Recreation and leisure
D. CONTENT OF THE PROGRAMME 10
1. General scheme and time frame 11
SCI patients in acute phase have usually been admitted to spine surgery or neurosurgical 12 department of University or regional hospitals. Rehabilitation has usually been started in an 13 acute setting. Then the process continues in the specialized SCI rehabilitation programme 14 of NRC ‘’Vaivari”. 15
The earliest time when the patients can start the rehabilitation in our programme is on the 16 10
th day after injury. The average time the patient joins our programme is 2-3 weeks after 17
impairment. Lengths of stay for newly injured patients are 45-60 days for paraplegics and 18 60-90 days for tetraplegics. A recurrent 21-28 day rehabilitation course is usually 19 performed after a short gap following the primary course. 20
The follow up is usually implemented once a year after the first post-acute rehabilitation 21 course. 22
23
b445 Respiratory muscle functions
b525 Defecation functions
b550 Thermoregulatory functions
b620 Urination functions
b640 Sexual functions
13/25
2. Role of PRM specialist 1
The PRM specialist evaluates the patient’s condition: sets the short and long term goals, 2 works out the rehabilitation plan, performs the treatment and prevention of infections, 3 spasticity, pain, hypotension, hypertension, autonomic dysreflexia, manages the 4 medication therapy and leads the whole multidisciplinary specialists’ team. The PRM 5 physician provides education and counselling related to sexuality and fertility. 6
The PRM physician makes the neurological assessment of the injured person using the 7 ISNCSCI and uses his/her knowledge to accurately predict the likely neurological and 8 functional outcomes based on this assessment. (25) 9
The PRM physician invites necessary consultants and organizes medical joint meetings 10 for complicated cases. 11
The PRM physician consults and selects complicated patients in University hospitals. 12
PRM specialists educate patients and caregivers about prevention of secondary 13 complications. Following topics are included in everyday routine work of multidisciplinary 14 rehabilitation team: 15
Skin care management and pressure ulcers prevention 16
Bladder and bowel management 17
Management of autonomic dysreflexia 18
Osteoporosis and heterotopic ossification 19
Sexuality and fertility after SCI 20
Before discharge, all the team holds a discussion about secondary complications with the 21 patient together with his/her family and caregivers. 22
Thematic lectures and discussions about preventing complications are organised by team 23 members, twice a month. 24
Once a month, discussions about living with SCI are organized with experienced people 25 living with SCI from non-governmental organization 26
3. Specific role of each team member in SCI rehabilitation programme 27
The rehabilitation team, leads by a PRM doctor, sets the rehabilitation goals – maximal 28 functional independence measured by SCIM tools. The most important predictors of 29 potential independence are injury level and completeness. They determine which level of 30 independency may be achieved and how much assistance will be needed in the future. 31
Maximal functional independence allows decreasing the restrictions in activities, 32 participation and the influence of environmental factors. The most important criteria 33 besides the neurological level are: 34
the patient’s general health condition – existing comorbidities and secondary 35 complications 36
the patient’s self-priorities in activities, participation and environmental factors 37
Those goals will be achieved by training and re-training different skills. The functions of the 38 rehabilitation specialists overlap in certain segments and thus allow achieving the main 39 goal successfully in various ways – the good quality of life possible despite the impairment. 40
41
Physiotherapists will develop mostly gross motor skills and mobility: bed mobility, 42 transfers mobility, wheelchair mobility, walking ability, gait training and the functions of the 43 upper extremities. Physiotherapists are responsible for evaluation of motor function 44 including voluntary and involuntary motor activity of all muscle groups, spasticity 45 assessment, training for range of motion, walking and standing, balance, treadmill walking 46 with body weight support, physical modalities, activities in swimming pool. 47
14/25
Occupational therapists provide training of participation in activities of daily living and 1 upper limb function and hand fine motor skills retraining, special equipment prescribing and 2 environmental modification, new technique and use special equipment for achieving these 3 goals. Occupational therapists determine the necessity of different types of assistive 4 technology. They also organize recreational activities. 5
Psychologists: assessment of personal factors, support, adaptation to new abilities 6 (disability), rebuilding self- esteem. 7
Social workers: advice and help in social security fields, cooperation with the family and 8 local municipalities about financial support, house adaptation, returning to school or to work 9 and founding solutions about the discharge place. 10
Nutritionists consult about energy needs, protein needs, ideal body weight, fluid needs, 11 and fibre needs, especially for those who have pressure ulcers. 12
The urologist consults for complicated cases and select patients for more specific 13 urological investigations and treatment. They perform urodynamic tests, intravesical botulin 14 toxin injections and surgical procedures in other hospital settings. 15
The nursing staffs provide bowel management, intermittent catheterisation. Nurses teach 16 self-catheterisation, maintenance of skin integrity and ulcer prevention. They monitor 17 autonomic dysreflexia and autonomic instability. Nurses are responsible for positioning in 18 bed. They teach patients to perform everyday life skills. Nursing staff often has close 19 interactions with family members. (23-25) 20
21
4. Diagnostic and assessment tools 22
Diagnostic equipment: X-ray, clinical and biochemical laboratory, abdominal ultrasound, 23 electrocardiography, portable ultrasound for residual urine. 24
Tools for clinical assessment (9-14, 18-19): 25
International Standards of Neurological Classification of SCI (ISNCSCI), which 26 describe the motor level and completeness of injury, 27
The Spinal Cord Independence Measure (SCIM) - independence scale specifically 28 developed for subjects with SCI. 29
Modified Asworth Scale 30
The Barthel Index 31
International SCI Date set 32
International SCI Lower Urinary Tract Function Basic Data Set 33
Autonomic Standards Assessment form 34
Braden’s scale is used for assessment of pressure ulcer risk. 35
Nurses and nurse assistants provide regular skin check and repositioning every 1,5-2 36 hours patients with high pressure ulcer risk. Every day visual checking is done for skin 37 pressure control. A specialized Seating Clinic with specific equipment for pressure 38 measurement will be developed in future. 39
40
41
Instrumental assessment: 42
Video Gait analysis laboratory for gait assessment. 43
Electroencephalography 44
Spirometer (Care Fusion Micro lab) and Peak flow meter for respiratory function 45 control. 46
15/25
5. Specific therapeutic interventions 1
Botox injection for spasticity management. 2
Endotracheal suctioning for secretion management. 3
Cough Assist machine - a noninvasive therapy for safely remove secretions in 4 patients with an ineffective ability to cough. High-level SCI often lack the muscle 5 strength and muscle control to create the full inhalation/explosive exhalation 6 required to cough and thereby remove bronchial secretions from the lungs. 7
Management of ventilation depended patients, in cooperation with 8 anesthesiologists. 9
Vacuum assisted closure for wound care management. 10
11
6. Assistive technology 12
Technical assistive aids are provided in the rehabilitation centre during the rehabilitation 13 course. 14
Different types of wheelchairs (passive, active, electrical, stand up) and walkers, crutches 15 as well as aids for carrying out everyday activities are accessible during rehabilitation and 16 after discharge. The patient’s functional condition is evaluated and the decision about the 17 most suitable aids is made during the rehabilitation course. 18
The patient himself completes a submission form for technical aids. 19
PRM doctor, considering the team decision – physiotherapist, occupational therapist, social 20 worker, psychologist and patient’s opinion - writes the application addressed to the 21 Technical Assistance Centre, which is one of the structural units of National Rehabilitation 22 centre. 23
Newly injured people receive assistive aids out of turn. Generally the wheelchair and 24 pressure relief cushion are provided while the patient is in the rehabilitation centre. The 25 wheelchair is tried and adapted to the individual under the guidance of an occupational 26 therapist. Necessary assistive aids are provided from the State Budget. 27
People with SCI have an access to wheelchairs – electrical, passive, active, and scooters. 28 If the patient works or studies, two wheelchairs are insured by the State Budget. If the state 29 provided wheelchair does not suit the patient, he/she can choose another option and 30 receive the basic funding from the State Budget and add on the co-payment to cover the 31 necessary expenses. Participants in Paralympic sports activities are provided with special 32 wheelchairs. 33
7. Environment adaptation 34
The social worker of SCI rehabilitation program provides the information about the 35 possibilities to renovate or adapt the apartment or a house when the patient has entered 36 the SCI program. The social worker communicates with the municipality. Whether the 37 changes and adaptation of the accommodation are implemented before the patient returns 38 from the rehabilitation centre very much depends on the municipality. In case the 39 accommodation is not suitable for the patient, the rehabilitation course could be shortly 40 prolonged till the problem is solved. 41
There are some cases when the patient has to be sent to a social care institution. 42
43
44
16/25
E. DISCHARGE PLANNING AND LONG TERM FOLLOW UP 1
1. Discharge criteria 2
The patient is discharged after post-acute rehabilitation program on day 60-90 in the case 3 of tetraplegia, on day 45- 60 in the case of paraplegia after admittance in the rehabilitation 4 hospital as soon as the short term goals have been reached: assistive aids have been 5 adapted for the needs of the patient, the patient has been taught how to use them, the 6 patient is ready to perform everyday activities, if necessary, the relatives and/or assistants 7 have been trained to help him/her. 8
2. How patients are managed after the programme? 9
Before discharge, a social worker informs the patient about the possibilities of vocational 10 reintegration after the rehabilitation program. 11
The social worker helps clear formalities for applying to the State Social Integration Agency 12 for requalification courses and training, which are financed by the State Budget. Before 13 discharge, the patient's evaluation is performed for the necessity to participate in the follow-14 up programme. 15
16
The follow up program focuses on prevention of secondary complications, functional 17 testing and training. Rehabilitation specialists give attention to psychosocial and sexual 18 problems, as well as involvement in sports and recreation activities. Simultaneous 19 rehabilitation programme for newly injured and experienced SCI patients is very helpful. 20
Conformity assessment of technical aids is executed for patients and new technical aids 21 are prescribed where appropriate. 22
Management of urinary disorders is reassessed for all SCI patients, once a year as a 23 routine USG is executed as to kidneys and urinary bladder, clinical and biochemical tests 24 are performed, urodynamic testing is performed where appropriate, advisory services by 25 urologists and advisors of other specialities are available. 26
Functional changes were assessed and expierenced PRM doctor evaluete neurological 27 symptoms. If necessary, suppose syringomyelia, patient will be sent for magnetic 28 resonance imaging. 29
A training program concerning prevention of secondary complications is simultaneously 30 implemented both for newly injured and experienced SCI patients. Thematic lectures about 31 prevention of secondary complications and discussions are organised by team members 32 twice a month. Support group activities are carried out jointly for newly injured and 33 experienced SCI patients. 34
Most of SCI patients are discharged to return home where they can live with their relatives. 35 Home assistance is offered by social institutions and visiting nurse services. Those patients 36 who cannot take care of themselves after concluded rehabilitation are accommodated in 37 social institutions. (16) 38
The future rehabilitation plan has been designed in accordance with the level and severity 39 of the lesion. Before discharge from first rehabilitation course, the rehabilitation team make 40 further plan and follow up program together with the patient. 41
If the first course, due to various conditions, has not been sufficient, a recurrent 42 rehabilitation course can be planned after a temporary stay at home. Subsequent control of 43 patients in the rehabilitation centre is carried out once a year. In case of changes in the 44 patient’s functional condition, a recurrent rehabilitation course is prescribed as necessary. 45 Patient’s medical record contains detailed recommendations for the patient and the general 46 practitioner, and also roughly states the time of the next rehabilitation review. 47
For patients with a low level and C; D/ AIS of the lesion, further rehabilitation is planned as 48 an out-patient course or as a course of rehabilitation in the day care centre. 49
17/25
IV. Additional information about PRM organisation 1
A. SAFETY AND PATIENT RIGHTS 2
1. Safety 3
4
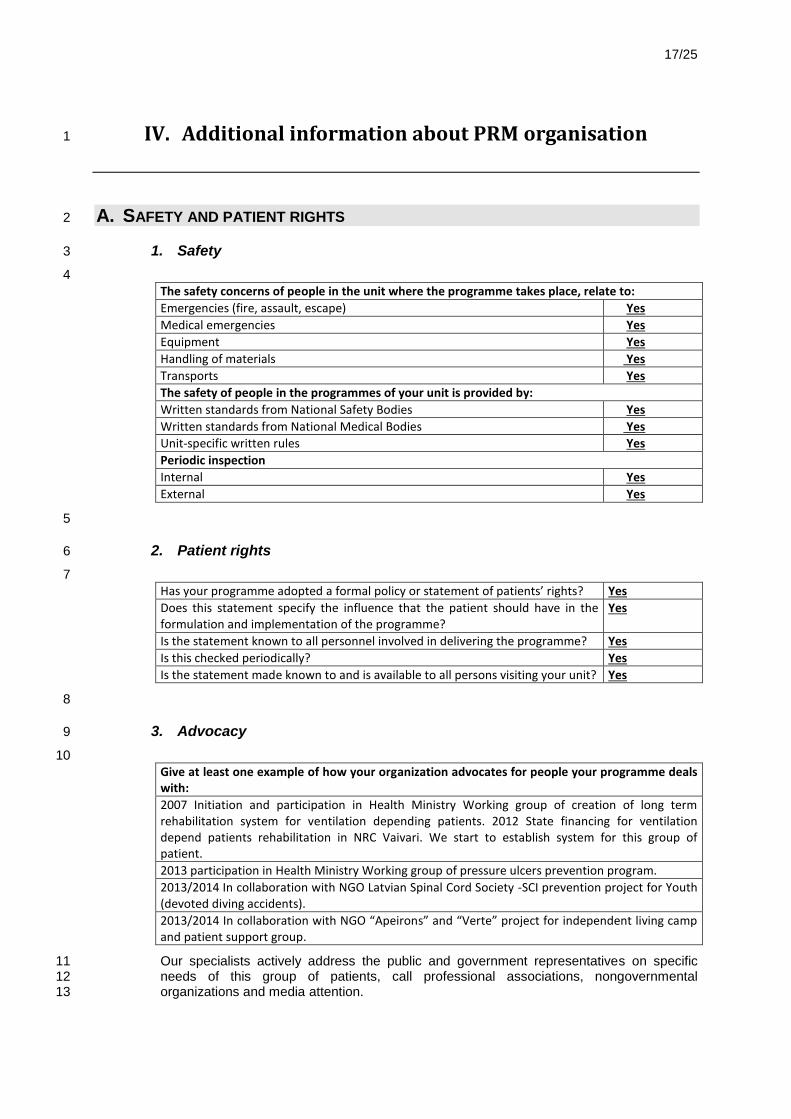
The safety concerns of people in the unit where the programme takes place, relate to:
Emergencies (fire, assault, escape) Yes
Medical emergencies Yes
Equipment Yes
Handling of materials Yes
Transports Yes
The safety of people in the programmes of your unit is provided by:
Written standards from National Safety Bodies Yes
Written standards from National Medical Bodies Yes
Unit-specific written rules Yes
Periodic inspection
Internal Yes
External Yes
5
2. Patient rights 6
7
Has your programme adopted a formal policy or statement of patients’ rights? Yes
Does this statement specify the influence that the patient should have in the formulation and implementation of the programme?
Yes
Is the statement known to all personnel involved in delivering the programme? Yes
Is this checked periodically? Yes
Is the statement made known to and is available to all persons visiting your unit? Yes
8
3. Advocacy 9
10
Give at least one example of how your organization advocates for people your programme deals with:
2007 Initiation and participation in Health Ministry Working group of creation of long term rehabilitation system for ventilation depending patients. 2012 State financing for ventilation depend patients rehabilitation in NRC Vaivari. We start to establish system for this group of patient.
2013 participation in Health Ministry Working group of pressure ulcers prevention program.
2013/2014 In collaboration with NGO Latvian Spinal Cord Society -SCI prevention project for Youth (devoted diving accidents).
2013/2014 In collaboration with NGO “Apeirons” and “Verte” project for independent living camp and patient support group.
Our specialists actively address the public and government representatives on specific 11 needs of this group of patients, call professional associations, nongovernmental 12 organizations and media attention. 13
18/25
B. PRM SPECIALISTS AND TEAM MANAGEMENT 1
1. PRM Specialists in the Programme 2
3
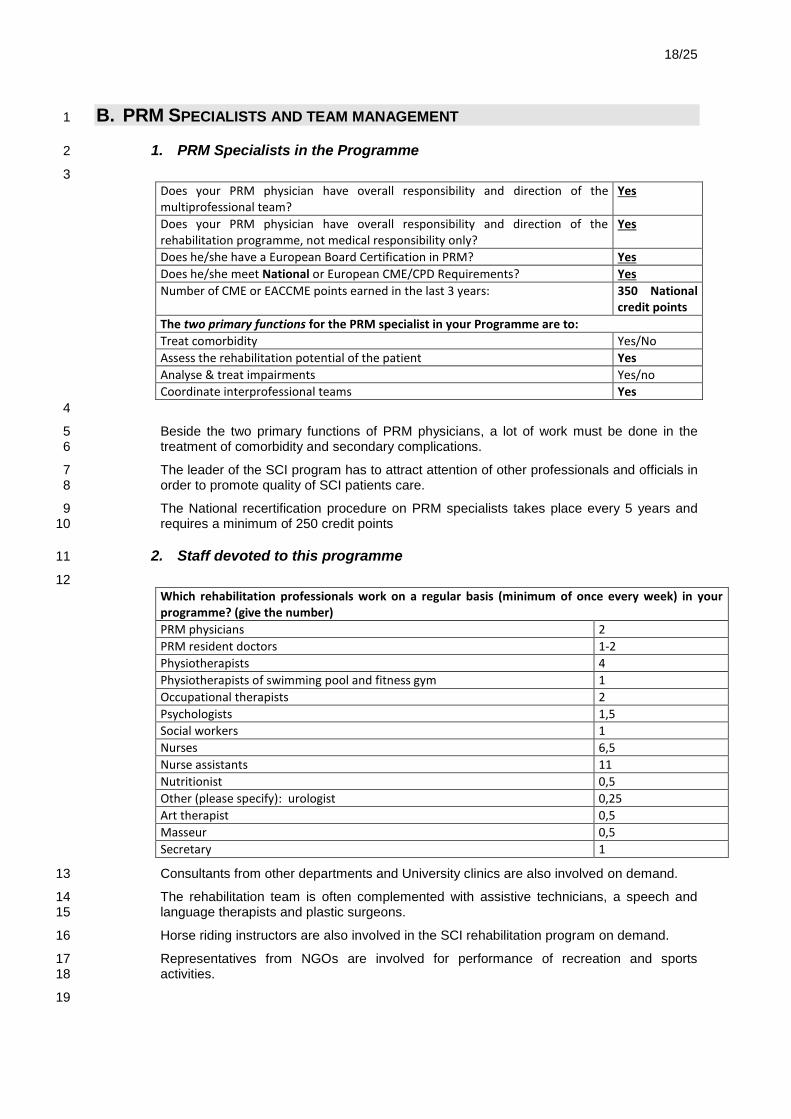
Does your PRM physician have overall responsibility and direction of the multiprofessional team?
Yes
Does your PRM physician have overall responsibility and direction of the rehabilitation programme, not medical responsibility only?
Yes
Does he/she have a European Board Certification in PRM? Yes
Does he/she meet National or European CME/CPD Requirements? Yes
Number of CME or EACCME points earned in the last 3 years: 350 National credit points
The two primary functions for the PRM specialist in your Programme are to:
Treat comorbidity Yes/No
Assess the rehabilitation potential of the patient Yes
Analyse & treat impairments Yes/no
Coordinate interprofessional teams Yes
4
Beside the two primary functions of PRM physicians, a lot of work must be done in the 5 treatment of comorbidity and secondary complications. 6
The leader of the SCI program has to attract attention of other professionals and officials in 7 order to promote quality of SCI patients care. 8
The National recertification procedure on PRM specialists takes place every 5 years and 9 requires a minimum of 250 credit points 10
2. Staff devoted to this programme 11
12
Which rehabilitation professionals work on a regular basis (minimum of once every week) in your programme? (give the number)
PRM physicians 2
PRM resident doctors 1-2
Physiotherapists 4
Physiotherapists of swimming pool and fitness gym 1
Occupational therapists 2
Psychologists 1,5
Social workers 1
Nurses 6,5
Nurse assistants 11
Nutritionist 0,5
Other (please specify): urologist 0,25
Art therapist 0,5
Masseur 0,5
Secretary 1
Consultants from other departments and University clinics are also involved on demand. 13
The rehabilitation team is often complemented with assistive technicians, a speech and 14 language therapists and plastic surgeons. 15
Horse riding instructors are also involved in the SCI rehabilitation program on demand. 16
Representatives from NGOs are involved for performance of recreation and sports 17 activities. 18
19
19/25
3. Team management 1
2
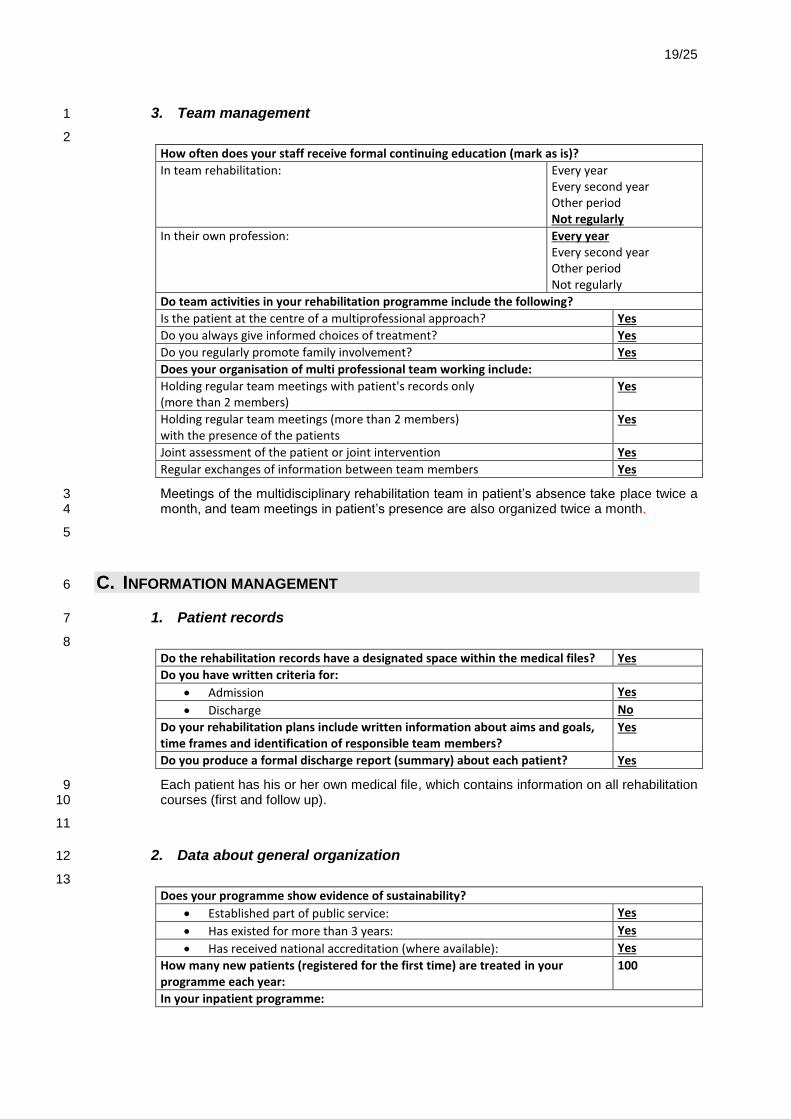
How often does your staff receive formal continuing education (mark as is)?
In team rehabilitation: Every year Every second year Other period Not regularly
In their own profession: Every year Every second year Other period Not regularly
Do team activities in your rehabilitation programme include the following?
Is the patient at the centre of a multiprofessional approach? Yes
Do you always give informed choices of treatment? Yes
Do you regularly promote family involvement? Yes
Does your organisation of multi professional team working include:
Holding regular team meetings with patient's records only (more than 2 members)
Yes
Holding regular team meetings (more than 2 members) with the presence of the patients
Yes
Joint assessment of the patient or joint intervention Yes
Regular exchanges of information between team members Yes
Meetings of the multidisciplinary rehabilitation team in patient’s absence take place twice a 3 month, and team meetings in patient’s presence are also organized twice a month. 4
5
C. INFORMATION MANAGEMENT 6
1. Patient records 7
8
Do the rehabilitation records have a designated space within the medical files? Yes
Do you have written criteria for:
Admission Yes
Discharge No
Do your rehabilitation plans include written information about aims and goals, time frames and identification of responsible team members?
Yes
Do you produce a formal discharge report (summary) about each patient? Yes
Each patient has his or her own medical file, which contains information on all rehabilitation 9 courses (first and follow up). 10
11
2. Data about general organization 12
13
Does your programme show evidence of sustainability?
Established part of public service: Yes
Has existed for more than 3 years: Yes
Has received national accreditation (where available): Yes
How many new patients (registered for the first time) are treated in your programme each year:
100
In your inpatient programme:
20/25
What is the mean duration spent in therapy by patients on this programme
24 Days
How many hours a day do the patients spend in therapy. 4 Hours
Give the mean duration of stay spent in the programme: 31 Days
Primary rehabilitation course for newly injured patients has longer length of stay and follow- 1 up programme has shorter lengths of stay. 2
3
3. Programme monitoring and outcomes 4
5
Does your programme have an overall monitoring system in addition to patient's records?
No
Are the long term outcomes of patients who have completed your programme regularly monitored?
Impairment (medical) outcomes: Yes
Activity/Participation (ICF) outcomes: Yes
Duration of follow up of the outcomes: 3-6 months 12 months longer
Do you use your outcome data to bring about regular improvements in the quality of your programme’s performance?
Yes
Do you make the long term overall outcomes of your programme available to your patients or to the public?
No
6
Patients are followed-up after discharge every year. They undergo a control examination 7 by a PRM physician. A routine urological testing is performed (urine delay measurements, 8 US scanner test, clinical and biochemical blood analysis). 9
Adequacy of the prescribed medical technical aids is checked. Secondary complications 10 resulting from spinal cord injury are controlled and treated. Counselling related to sexual 11 dysfunction is provided. 12
Some outcome data of our SCI program have been presented to international and local 13 professional meetings: 14
„The impact of traumatic spinal cord injury on person s health related quality of life” 15 A.Nulle, A.Vētra 52
nd Annual Scientific meeting of International Spinal Cord Society , 16
Istanbul,Turkey, 2013 17
“Influence of organized and purposeful physical and recreation activities of persons after SCI” 18 F.Bernadskis, U.Purena, A.Nulle 7th Baltic Rehabilitation Association Conference on 19 PRMVilnius, Lithuania, 2012 20
Poster presentation ,,Impact of SCI on the functions of respiratory system ” S. Zommere, 21 D.Stirane, A.Vētra, A.Nulle 18th PRM European congress Thessaloniki, Greece,2012 22
Case report „Osteoporosis and SCI” A.Nulle American Austrian Foundation Sazburg 23 Medical seminars in Rehabilitation Medicine, Salzburg, Austria, 2012 24
*„Epidemiology and Rehabilitation of SCI patients in Latvia” A.Nulle, A.Vētra 25
„Changes of testosterone level after traumatic SCI” A.Nulle, A.Vētra 6th Congress of 26 BalticSpinal Cord Society (BaSCoS), Riga, Latvia, 2011 27
"Pilot study of International SCI Data Sets and SCIM-III for assessment and 28 documentation” G.Bērziņa, A.Nulle, A.Vetra 29
” Development of recreation program for person with SCI” R.Mieze, A.Nulle 2nd Baltic & 30 North Sea Conference on PRM, Vilnius, Lithuania, 2011 31
Presentation of Case report ” Complicated SCI patient.” 32
21/25
American Austrian Foundation Salzburg Medical seminars in Rehabilitation Medicine, 1 Salzburg, Austria,2010 2
„Organization of SCI care in Latvia” 2008 5th Congress of BalticSpinal Cord Society 3 (BaSCoS), Tartu, Estonia 4
Research project “Spinal Cord injury Care in Primary Medicine” A.Nulle Baltic Forum- 5 research in Primary Care, Jurmala, Latvia, 2008 6
„The Perspectives of SCI Patient Care in the Baltic Countries Joining the EU” A.Nulle 3rd 7 Congress of BaSCoS, Riga, Latvia, 2004 8
Poster presentation “Analysis of rehabilitation experience of child with SCI”A.Nulle ISCoS 9 joint meeting with ASIA, Vancouver, Canada, 2002 10
“Analysis of epidemiological indicators and application of the rehabilitation technologies in 11 the rehabilitation of the SCI patients” A.Nulle, D.Namniece, A.Vetra BaSCoS 2
nd Congress 12
Tallinn, Estonia,2002 13
22/25
V. Quality improvement 1
A. WHAT ARE THE MOST POSITIVE POINTS OF YOUR PROGRAMME? 2
There are effective planning and selection of SCI patients in cooperation with University 3 Clinics. 4
Close professional contacts with neurosurgeons, orthopaedic surgeons, plastic surgeons. 5
Experienced multidisciplinary, professional staff with few staff turnover and well educated 6 young colleagues. 7
There is availability of intensive therapy unit with anaesthesiologist on 24 hour duty. 8
Close cooperation with NGO’s for re-socialisation and sports activities. 9
B. WHAT ARE THE POINTS TO IMPROVE IN YOUR PROGRAMME? 10
Regular accessibility of urodynamic testing. 11
Reduction of spasticity with baclofen pump. 12
Cooperation with the GPs after discharge. 13
Robotic technology systems and fitness equipment. 14
Prevention of pressure sores for wheelchair users. 15
Prevention of the staff Burn-out syndrome 16
C. WHAT ACTION PLAN DO YOU INTEND TO IMPLEMENT IN ORDER TO IMPROVE 17
YOUR PROGRAMME? 18
1. Extrinsic conditions that you wish to obtain. 19
Urodynamic testing accessibility on regular basis. 20
Extensions of the spasticity programme with baclofen pump implantation. 21
Implementation of robotic technologies and extension of fitness equipment. 22
Specialized Seating Clinic with specific equipment for cutaneous pressure measurement. 23
Extensions of the rehabilitation team by a recreational therapist and a respiratory therapist. 24
Couch for sport activities (wheelchair basketball) and canoe for balance training in 25 swimming pool and/or at sea. 26
2. Intrinsic improvement of the programme 27
Implementation of International SCI date core set and assessment tools. 28
Learning workshop about using specific assessment tools for all team members. 29
Digital medical records. 30
Regular training and education program of the staff. Prevention of Burn-out syndrome. 31
International cooperation and research work. 32
Regular update of the program. 33
23/25
VI. References 1
A. LIST OF REFERENCES 2
3
1. R A Cripps, B Lee, P Wing, E Weerts, J Mackay and D Brown A global map for traumatic 4 spinal cord injury epidemiology: towards a living data repository for injury prevention Spinal 5 Cord 49, 493-501 (April 2011) 6
2. B B Lee, R A Cripps, M Fitzharris and P C Wing
The global map for traumatic spinal cord 7
injury epidemiology: update 2011, global incidence rate Spinal Cord advance online 8 publication 26 February 2013 9
3. P W New, R A Cripps and B Bonne Lee Global maps of non-traumatic spinal cord injury 10 epidemiology: towards a living data repository Spinal Cord , (15 January 2013) 11
4. Lawrence S Chin, Fassil B Mesfin, Segun T Dawodu Spinal cord injyry 12 /Pathophysiology/ Chief Editor: Allen R Wyler, Wyler, Northstar Neuroscience, Inc 13 http://emedicine.medscape.com/article/ 14
5. B.Wolfe DL, Hsieh JTC, Mehta S (2012). Rehabilitation Practices and Associated 15 Outcomes Following Spinal Cord Injury. In Eng JJ, Teasell RW, Miller WC, Wolfe DL, 16 Townson AF, Hsieh JTC, Connolly SJ, Noonan V, Mehta S, Sakakibara BM, Boily K, 17 editors Spinal Cord Injury Rehabilitation Evidence. Version 4.0 18
6.Sandrine Thuret, Lawrence D. F. Moon and Fred H. Gage Therapeutic interventions after 19 spinal cord injury Neuroscience volume7 August 2006 ; 643-628 20
7. P Kennedy and Z J Chessell Traumatic versus non-traumatic spinal cord injuries: are 21 there differential rehabilitation outcomes? Spinal Cord 51, 579-583 (July 2013) 22
8.Anthony S. Burns Colleen O'Connell The challenge of spinal cord injury care in the 23 developing world Spinal Cord Med. 2012 January; 35(1): 3–8. 24
9. Consortium for Spinal Cord Medicine Clinical Practice Guidelines Access evidenced 25 based clinical practice guidelines on topics related to SCI. 26 http://www.pva.org/site/c.ajIRK9NJLcJ2E/b.7516843/k.6FC/Paralyzed_Veterans_of_Ameri27 ca_Publ 28
10.Consortium for Spinal Cord Medicine Outcomes following traumatic spinal cord injury: 29 clinical practice guidelines for health-care professionals. J Spinal Cord Med. 30 2000,23(4):289-316. 31
11.William P Waring, III, Fin Biering-Sorensen, Stephen Burns, William Donovan, Daniel 32 Graves, Amitabh Jha, Linda Jones, Steven Kirshblum, Ralph Marino, M.J Mulcahey 2009 33 Review and Revisions of the International Standards for the Neurological Classification of 34 Spinal Cord Injury J Spinal Cord Med. 2010 October; 33(4): 346–352. 35
12.Kirshblum SC, Burns SP, Biering-Sorensen F, Donovan W, Graves DE, Jha A, 36 Johansen M, Jones L, Krassioukov A, Mulcahey MJ, Schmidt-Read M, Waring W. 37 International standards for neurological classification of spinal cord injury (revised 2011). J 38 Spinal Cord Med. 2011 Nov;34(6):535-46 39
13.International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI): 40 http://www.asia-spinalinjury. 41
14.Ditunno JF Jr, Burns AS, Marino RJ. Neurological and functional capacity outcome 42 measures: essential to spinal cord injury clinical trials.J Rehabil Res Dev. 2005 May-43 Jun;42(3 Suppl 1):35-41. 44
24/25
15.Högel F, Mach O, Maier D. Functional outcome of patients 12 and 48 weeks after acute 1 traumatic tetraplegia and paraplegia: data analysis from 2004-2009. Spinal Cord. 2012 Jul; 2 50(7):517-20. 3
16. Priebe MM, Chiodo AE, Scelza WM, Kirshblum SC, Wuermser LA, Ho CH. Spinal cord 4 injury medicine. 6. Economic and societal issues in spinal cord injury. Arch Phys Med 5 Rehabil 2007; 88(3 Suppl 1):S84-8. 6
17.Taylor-Schroeder S, LaBarbera J, McDowell S, Zanca JM, Natale A, Mumma S, 7 Gassaway J, Backus D. The SCI Rehab project: treatment time spent in SCI rehabilitation. 8 Physical therapy treatment time during inpatient spinal cord injury rehabilitation. J Spinal 9 Cord Med. 2011;34 (2):149-61. 10
18.DeVivo M, Biering-Sørensen F, Charlifue S, Noonan V, Post M, Stripling T, Wing P; 11 Executive Committee for the International SCI Data Sets Committees. International Spinal 12 Cord Injury Core Data Set. Spinal Cord. 2006 Sep;44(9):535-40. 13
19.Biering-Sørensen F, Craggs M, Kennelly M, Schick E, Wyndaele JJ International lower 14 urinary tract function basic spinal cord injury data set. Spinal Cord. 2008 May; 46(5):325-15 30. 16
20. SCIM (Spinal Cord Independence Measure):http://scimscore.com 17
21.Hyung Seok Nam, Kwang Dong Kim, Hyung Ik Shin, ICF Based Comprehensive 18 Evaluation for Post-Acute Spinal cord Injury Ann Rehabil Med. 2012 December; 36(6): 19 804–814. 20
22.Biering-Sørensen F, Charlifue S, Baumberger M, Campbell R, Kovindha A, Ring H, 21 Sinnott A, Scheuringer M, Stucki G Identification of the most common problems in 22 functioning of individuals with spinal cord injury using the International Classification of 23 Functioning, Disability and Health. Spinal Cord. 2010 Mar; 48(3):221-9 24
23. Consortium for Spinal Cord Medicine Outcomes following traumatic spinal cord injury: 25 clinical practice guidelines for health-care professionals. J Spinal Cord Med. 2000, 26 23(4):289-316. 27
24.Gale Whiteneck, , Julie Gassaway, Marcel Dijkers, Amitabh Jha, New Approach to 28 Study the Contents and Outcomes of Spinal Cord Injury Rehabilitation: The SCI Rehab 29 Project J Spinal Cord Med. 2009 June; 32(3): 251–259. 30
25. Lyn Emerich, Kenneth Parsons, Adam Stein White Paper on competent care and SCI 31 rehab standards.Competent Care for Persons with Spinal Cord Injury and Dysfunction in 32 Acute Inpatient Rehabilitation. www.asia-spinalinjury.org/ 33
26. Annual Report on the NSCISC website: https://www.nscisc.uab.edu/reports.aspx 34
27.William McKinley, Katia Santos, Michelle Meade, Karen Brooke, Functional Outcomes 35 per Level of Spinal Cord Injury J Spinal Cord Med. 2007; 30(3): 215–224. 36
28 https://www.vestnesis.lv 37
38
DETAILS ABOUT NATIONAL DOCUMENTS 39
*„Epidemiology and Rehabilitation of SCI patients in Latvia” A. Nulle, A. Vētra 6th Congress 40 of Baltic Spinal Cord Society (BaSCoS), Riga, Latvia, 2011 41
Laws and Regulations of the Cabinet of Ministers of Latvia. (28) 42
Constitution of the Republic of Latvia15.02.1922 43
Tehnisko palīglīdzekļu noteikumi (Regulations of Technical Aids) 15.12.209.Nr1474 44 Ārstniecības likums (Medical Treatment Law) 22.06.1997. 45
Fizisko personu datu aizsardzības likums (Law on Personal Data Protection) 23.03. 2000 46
Pacientu tiesību likums (Law on the Rights of Patients) 17.12.2009 47
25/25
Invaliditātes likums (Disability Law) 20.05.2010 1
Veselības aprūpes organizēšanas un finansēšanas kārtība (Health Care Organization and 2 Financing.) 19. 12.2006. Nr1046. 3
Noteikumi par obligātajām prasībām ārstniecības iestādēm un to struktūrvienībām (Rules 4 on minimum requirements for medical institutions and their departments.) 20.01.2009. Nr. 5 60. 6
Zāļu iegādes, uzglabāšanas, izlietošanas, uzskaites un iznīcināšanas kārtība ārstniecības 7 iestādēs un sociālās aprūpes institūcijās (Medicine purchase, storage, use, inventory and 8 disposal procedures in medical institutions and social care institutions.) 27. 03. 2007. 9
Medicīnisko dokumentu lietvedības kārtība (Medical institution and medical record clerical 10 procedures) 04.04.2006. Nr.265. 11
Noteikumi par higiēniskā un pretepidēmiskā režīma pamatprasībām ārstniecības iestādē 12 (Regulations on hygiene and counter-epidemic safety standards in the medical institutions) 13 11.07.2006.Nr.574. 14
15
16