-
8/13/2019 Ulnar Neuropathy in the Distal Ulnar nerve lesions
1/5
Ulnar Neuropathy in the Distal UlnarTunnelDAVID W SHUPE, PT,
ATC
A brief anatomical review of the ulnar nerve and areas of ulnar
nerve entrapmentis discussed. The importance of the dorsal
cutaneous nerve is presented with regard tolocalizing a lesion to
the ulnar nerve in the forearm. A classification system isdescribed
for ulnar entrapment that occurs distal to the wrist. The case of a
nine-year-old girl with a fibrous entrapment of the ulnar nerve in
the distal ulnar tunnel ispresented . The clinical and diagnostic
procedures required for localizing the level ofthe ulnar nerve
entrapment are described along with the operative findings of
thiscase report.
When evaluating and treating patients withtrauma to the upper
extremity, a vital part of theassessment is the basic neurological
examination.One component of this examination is the evalu-ation of
peripheral nerve function. If ulnar nerveinvolvement is suspected,
then particular assess-ment of this nerve is warranted. Conclusions
de-rived from this assessment will allow the physicaltherapist to
develop more realistic treatment goalsand to enhance communication
with patients andothers in the medical community.The purpose of
this article is to give a briefanatomical review of the ulnar nerve
and potentialareas of ulnar nerve entrapment, with emphasison the
distal ulnar tunnel. A case report of apatient with a fibrous
entrapment of the ulnarnerve in the distal ulnar tunnel is
presented.ANATOMY OF THE ULNAR NERVEAn anatomical review of the
ulnar nerve showsthat after originating from the medial cord of
thebrachial plexus, it descends along the medial as-pect of the arm
with the median nerve. In thedistal aspect of the arm, it becomes
more super-ficial after passing through the intermuscular septum of
the triceps brachii Arcade of Struthers).At the elbow, the nerve
passes through a fibro-osseous tunnel, known as the cubital tunnel.
Lat-erally, this tunnel is bordered by the elbow joint,
Director. wrtsmedCenter.325 N.25th Street. Lafavette. IN
47904.0190-601 PI11 01 OOO6 03.OO/OTHEJOURNALF ORTHOPAEDICND
SPORTSPHYSICALHERAWCopyight 991 by The OrWqwdc and Sports
PhysicalTherapyS e c t i s of th Americen Physical Therapy ssociat
i
medially by the heads of the flexor carpi ulnaris,and anteriorly
by the medial epicondyle 1).After passing through the cubital
tunnel. thenerve enters the forearm, taking a less
superficialcourse when it descends between the two headsof the
flexor carpi ulnaris muscle 7).The ulnarnerve then takes a straight
course along the me-dial aspect of the forearm after giving
muscularbranches to the flexor carpi ulnaris and the
flexordigitorum profundus to the ring and little fingersbarring any
anomalies). It is important to notethat entrapments may occur at
the Arcade ofStruthers, in the cubital tunnel, and within
thefibrous tunnel formed by the two heads of theflexor carpi
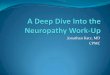
ulnaris.Approximately eight to ten centimeters prox-imal to the
ulnar styloid process, the dorsal cuta-neous nerve branches from
the ulnar nerve Figure1).Four to five centimeters proximal to the
styloidprocess, the dorsal cutaneous nerve crosses themedial aspect
of the ulna to take a position dorsalto the ulna 4, 7). This branch
provides sensoryinnervation to the ulnar portion of the dorsum
ofthe hand and parts of the dorsal aspect of thelittle and ring
fingers Figure 2).The ulnar nerve enters the hand through thedistal
ulnar tunnel 2, 5). This tunnel is four to fourand one-half
centimeter long, beginning at theproximal edge of the palmar carpal
ligament andextending to the fibrous arch of the hypothenarmuscles
Figure 3). As described by Gross andGelberman 2), the roof of the
tunnel from proximalto distal is composed of the palmar carpal
liga-ment, palmaris brevis muscle, and hypothenar fatand fibrous
tissue. Kleinert and Hayes 5) reportedthat this roof is
multilayered, with the palmar
SHUPE JOSPT 13:1 January 1991
Copyright1991JournalofOrthopaedic&S
portsPhysicalTherapy.Allrightsreserved.
-
8/13/2019 Ulnar Neuropathy in the Distal Ulnar nerve lesions
2/5
carpal ligament blending distally with the hypoth-enar fascia,
radially with the palmar aponeurosis,and proximally with the volar
forearm fascia.The floor of the tunnel is formed by thetendons of
the flexor digitorum prcifundus, thetransverse carpal ligament, the
pisohamate andpisometacarpal ligaments, and the opponens
digitiminimi 2). The flexor carpi ulnaris, the pisiform,
DorsalCutaneous Branch
Ulnaris
Figure 1. Course of the dorsal cutaneous nerve.
and the abductor digiti minimi comprise the ulnarwall. The
radial wall is formed by the tendons ofthe extrinsic flexors, the
transverse carpal liga-ment, and the hook of the hamate. Along with
theulnar nerve, the ulnar artery lies within the distalulnar
tunnel.Within the distal ulnar tunnel, the ulnar nervedivides into
a superficial branch and a deep branch5). The superficial branch
supplies the skin onthe palmar aspect of the little finger and the
medialhalf of the ring finger. Motor fibers to the palmarisbrevis
also take their origin from the superficialbranch. After
innervating the abductor digiti min-imi, flexor digiti minimi, and
opponens digiti minimimuscles, the deep palmar branch turns
laterallyto supply the dorsal and palmar interossei, thethird and
fourth lumbricals, the adductor pollicis,and the deep head of the
flexor pollicis brevismuscles.In their anatomical study of the
distal ulnartunnel, Gross and Gelberman 2)used an anatom-ical basis
for dividing the tunnel into three zones.
Zone one is the portion of the tunnel proximal tothe bifurcation
of the nerve. Any lesion of the ulnarnerve in this zone would lead
to both motor andsensory deficits. Zone two encompasses thedeep
motor branch of the nerve. Any involvementof the nerve in this zone
would lead to motordeficits only. The superficial branch is located
inzone three. Any lesion at this level would lead tosensory
involvement and a motor deficit of thepalmaris brevis.
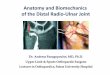
Figure 2. Sensory distribution of the dorsal cutaneous branch of
the ulnar nerve.
SENSORY ND MOTOR EV LU TIONUnderstanding the distribution of the
dorsal cuta-neous branch of the ulnar nerve is extremelyimportant
in helping to differentiate the approxi-mate level of any lesion of
the ulnar nerve in thedistal one-half of the forearm. Any problem
prox-imal to the dorsal cutaneous branch would resultin a sensory
disturbance to the dorsal and ulnaraspect of the hand, parts of the
dorsal aspect ofthe ring and little fingers, and a sensory deficit
onthe palmar surface of the little finger and medialaspect of the
ring finger. A lesion distal to theorigin of this small cutaneous
branch would onlyproduce a sensory deficit in the little finger
andmedial aspect of the ring finger 7). Regardless ofwhere an ulnar
nerve lesion in the distal forearmwould be located, the same motor
deficit wouldexist.A thorough assessment of the motor functionof
the hand, fingers, and thumb is an essentialcomponent of the
evaluation process. Along withany functional tests, a detailed
manual muscletest should always be performed. Strength defi-cits in
the hand muscles innervated by the ulnarnerve can result directly
from an ulnar motorbranch dysfunction as discussed. However,
these
OSPT 3: anuary 99 ENTRAPMENT AT DISTAL ULNAR TUNNEL 7
Copyright1991JournalofOrthopaedic&S
portsPhysicalTherapy.Allrightsreserved.
-
8/13/2019 Ulnar Neuropathy in the Distal Ulnar nerve lesions
3/5
Opponens Digiti MinimiFlexor Digiti Minimi
Superficial BranchDeep Branch Ulnar Nerve
Abductor Digiti MinimiHamate
Pisohamate LigamentTransverse CarpalLigamentPalmar
CarpalLigament Flexor Carpi U lnaris
strength deficits may also arise from othersources that should
not be ignored, even in thepresence of known trauma to the ulnar
nerve.Other sources of dysfunction may include motorneuron
diseases, nerve root compression, bra-chial plexopathy from various
etiologies, diseasesof peripheral nerves, mechanical abnormalities
asa result of a disease process, and nerve entrap-ments (3).C SE
REPORTA nine-year-old girl fell from a balance beam
duringgymnastics practice. She landed on her right handwith the
wrist extended and the elbow in a fullyextended position (Figure
4). Immediate pain anddisability were reported in the right elbow.
Afterx-ray examination revealed a displaced fractureof the medial
epicondyle of the right humerus, anopen reduction and internal
fixation of the dis-placed fragment were performed (Figure 5).
Sta-bilization was maintained with percutaneous pin-ning, and a
posterior plaster splint was appliedwith the elbow at 60' of
flexion.After five weeks, the Steinman pins wereremoved and the
patient was referred to physicaltherapy for rehabilitation. Active
range of motion(AROM) of the right elbow was 50-1 05'; supina-tion
was 0-45'; and pronation was 0-73'. AnAROM and gravity-assisted,
static-stretching pro-gram was begun.At the seventh postoperative
week, elbowAROM was 48-1 13O, with supination and prona-tion
showing normal ROM measurements. Thepatient, now less focused on
the elbow, reported
that her ring and little fingers 'felt cold at times.Examination
of the right hand revealed an abnor-mal resting finger position
that consisted of claw-ing of the fourth and fifth fingers 6).
Atrophy ofthe intrinsic hand muscles innervated by the ulnarnerve
was noted. Trophic changes were presentin the ring and little
fingers, consisting of a white,leathery appearance to the skin and
a brittie,ridged look to the nails.A sensory evaluation was normal
to lighttouch and pinprick. Two-point discrimination wasalso normal
at five millimeters. Manual muscletesting revealed normal function
of all musclesinnervated by the median nerve. Normal functionof the
flexor carpi ulnaris and flexor digitorumprofundus to all fingers
was present. No functionof the intrinsic hand muscles innervated by
theulnar nerve was noted, although a minimal degreeof abduction of
the little finger was present. Thiswas in the presence of no
palpable contractionof the abductor digiti minimi and was thoughtto
have resulted from aponeurotic attachmentsfrom the flexor carpi
ulnaris to the abductor digitiminimi.Finger tip prehension (thumb
to index) waspossible, but lateral prehension was not. A nega-tive
Tinel's sign was present at the elbow andwrist over the ulnar and
median nerves. Markedtenderness was found with palpation in the
areaof the hook of the hamate. A positive Tinel's signwas also
present at this location. These findingswere documented and
reported to the referringphysician.After carpal tunnel views of the
right wristruled out a fracture of the hook of the hamate (6),
Figure3 Diagramo the distal ulnar tunnel
SHUPE JOSPT 3: January
Copyright1991JournalofOrthopaedic&S
portsPhysicalTherapy.Allrightsreserved.
-
8/13/2019 Ulnar Neuropathy in the Distal Ulnar nerve lesions
4/5
Figure 4. Mechanism of injury for nine-yearsld pa-tient in case
study.
the decision was made in favor of nonsurgicalmanagement to see
if spontaneous recovery offunction would occur.At five months
postinjury, ROM measure-ments of the right, elbow, along with
supinationand pronation of the forearm, were normal.
Theneurological status, however, remained un-changed. At this time,
further evaluation was re-quested by her physician.Motor and
sensory nerve conduction studiesof the right median nerve were
normal. Ulnar nerve
studies using a needle electrode showed noresponse from the
abductor digiti minimi or thefirst dorsal interosseous muscles. No
evoked sen-sory action potential was elicited when recordingfrom
the little finger using an antidromic testingtechnique.Ulnar
sensory testing for the dorsal cuta-neous nerve showed significant
slowing, with theamplitude of evoked sensory action
potentialsomewhat decreased compared to the contralat-era1 side.
Over a six centimeter segment, thelatency on the left was 1.8 msec
with an amplitude
Figure 5. Postoperative radiographs of right elbow:A lateral
view; B anterior-posterior view.of 21.0 pV. The values on the right
were 4.2 msecand 11.3 pV, respectively.This was a somewhat
surprising finding sincesensory testing of the dorsal cutaneous
nervewas normal. The slowing, thought to result froma retrograde
demyelination rather than from amore proximal process, seemed to be
supportedby the electromyographic EMG) findings.Electromyographic
sampling of the right a bductor pollicus brevis and the flexor
carpi ulnarismuscles showed normal, insertional activity
withelectrical silence at rest. Motor units were normalfor shape,
amplitude, and duration, and there wasa normal interference pattern
in the abductor pol-licus brevis with a slightly reduced
interferencepattern in the flexor carpi ulnaris. The
decreasedinterference pattern in the flexor carpi ulnaris
wasassociated with subjective complaints of pain atthe sampling
site.When the abductor digiti minimi and the firstdorsal
interosseous muscles were sampled, min-imal insertional activity
with 2+ denervation po-tentials at rest was noted in both muscles.
No
JOSPT 3: January 99 ENTRAPMENT AT DISTAL ULNAR TUNNEL 9
Copyright1991JournalofOrthopaedic&S
portsPhysicalTherapy.Allrightsreserved.
-
8/13/2019 Ulnar Neuropathy in the Distal Ulnar nerve lesions
5/5
motor units were located at multiple samplingsites in either of
the latter muscles.
A surgeon localized the ulnar nerve lesionand performed surgery
at a level distal to thewrist. The hook of the hamate was found to
bestable, but a significant fibrosis of the motorbranch of the
ulnar nerve and a lesser degree offibrosis of its sensory branch
was observed.Dissection, release of the entrapment, and anexternal
neurolysis were performed in all threezones (2).
At two weeks postsurgery, the patient re-ported that the fourth
and fifth fingers feltwarmer. According to the surgeon, some
inter-ossei muscle function was noted at four weeksfollowing
surgery. After this time, objective infor-mation and the
opportunity for further evaluationof the patient were no longer
available to theauthor. However, at four months postsurgery,an
uncomplicated recovery was reported by thesurgeon.
SUMM RYPeripheral nerve njury can bea common sequelaein trauma
involving the upper extremity. Recog-nizing an orthopaedic injury
and its soft tissueand/or neurological components is critical.
Neu-rological assessment should be a routine part ofa thorough
physical therapy examination in anyorthopaedic and sports
rehabilitation practice.
Appreciation s extended to Hospital Services. Inc. for all o th
irassistance.
REFERENCES1. Green DP: Operative Hand Surgery. d 2.
Churchill/Livingstm:New York 19822. Gross MS. Gelbennan RH:The
Anatomyofth Distal Unar Tunnel.Clin Orthop 196:238-247. 19853.
Hogue RE: Compression of the deep palmar branchof th ulnarnerve:
case report. Phys Ther 65203-205.19854. Jabre JF: Unar nerve
lesions at the wrist: new technique forrecording rom the sensory
dorsal branch of the ulnar nerve.Neurology 30373-876. 19805.
Klemert HE. Hayes JE: The Unar TunnelSyndrwne.Plast ReconstrSurg
47:21-24. 19716. Parker RD. Berkowitz MS. Brahrns MA. Bohl WR Hook
o thharnate fractures in athletes. Am J Sports Med 14517-523.
19867. Spmner M: Injuries to the Major Branches of PeripheralNw es
ofthe Forearm, pp 114-127. Philadelphia: WE Saunders
SHUP JOSPT 3: January 99
Copyright1991JournalofOrthopaedic&S
portsPhysicalTherapy.Allrightsreserved.








![Electrophysiological Features of Ulnar Tunnel Syndrome ... · Ulnar tunnel syndrome (UTS) is an uncommon ulnar entrapment neuropathy. Guyon [1] described the anatomy of the area in](https://img.pdfslide.net/doc/110x75/601bca5f935324075a08994b/electrophysiological-features-of-ulnar-tunnel-syndrome-ulnar-tunnel-syndrome.jpg)

















