Embed Size (px)
Citation preview

373Copyrights © 2014 The Korean Society of Radiology
INTRODUCTION
Gardner syndrome is a rare autosomal dominant disorder characterized by colonic polyposis and bone and soft tissue manifestations including osteomas, and mesenchymal tumors of the skin and soft tissues (1-3). To our knowledge, unilateral chest wall anomaly has not been reported in patients with Gard-ner syndrome. We describe here a case of unilateral hypertrophy of the ribs and intercostals muscles occurring in a patient with Gardner syndrome.
CASE REPORT
A 32-year-old man was admitted to the gastrointestinal de-partment of our institution complaining of diarrhea and bloody stools. The patient had past histories of excision of lipomas from
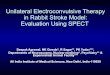
his left ear and back and hemorrhoidectomy. Familial history was not specific. A digital rectal examination revealed multiple polypoid masses. Insertion of a colonoscope as far as 40 cm above the anal verge showed extensive polypoid lesions along the entire colon (Fig. 1A). A 5 cm sized mass was observed 10 cm above the anal verge (Fig. 1B). Under the impression of fa-milial adenomatous polyposis (FAP), the patient also under-went duodenoscopy, which showed numerous small polypoid lesions in the gastric body and multiple erythematous polypoid lesions in the duodenal bulb (Fig. 1C). Endoscopic biopsy of some of these lesions showed that they were adenomas with low grade dysplasia.
An abdominal and pelvic CT scan revealed an intraluminal polypoid mass with perirectal infiltrations in the upper rectum (Fig. 2A). The mass was regarded as the same lesion on previous colonoscopy (Fig. 1B), which was confirmed as being a tubular
Case ReportpISSN 1738-2637 / eISSN 2288-2928J Korean Soc Radiol 2014;70(5):373-377http://dx.doi.org/10.3348/jksr.2014.70.5.373
Received October 29, 2013; Accepted March 27, 2014Corresponding author: So-Yeon Lee, MDDepartment of Radiology, Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine, 29 Saemunan-ro, Jongno-gu, Seoul 110-746, Korea.Tel. 82-2-2001-1030 Fax. 82-2-2001-1031E-mail: [email protected]
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distri-bution, and reproduction in any medium, provided the original work is properly cited.
Gardner syndrome is a familial disease consisting of colonic polyposis, osteomas, and soft tissue tumors. We describe unilateral chest wall anomaly in a 32-year-old man with Gardner syndrome. A chest radiograph showed asymmetric hypertrophy of the right seventh to tenth ribs. CT images showed increased size of the medullary portions of these lesions, but relatively normal thickness of the cortex. Intercostal muscles along the right seventh to tenth ribs were hypertrophied as compared with the contralateral ribs. Both lungs were clear but the volume of right lung showed slightly smaller than left one.
Index termsGardner SyndromeRibFamilial Adenomatous PolyposisCTChest Wall
Unilateral Chest Wall Anomaly in a Patient with Gardner’s Syndrome: Case Report1
가드너 증후군 환자에 동반된 일측성 흉벽 기형: 증례 보고1
Eun Hee Song, MD1, So-Yeon Lee, MD1, Hee Jin Park, MD1, Heon-Ju Kwon, MD1, Mi Sung Kim, MD1, Hae Won Park, MD1, Hyon Joo Kwag, MD1, Hye Jin Kim, MD2 1Department of Radiology, Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine, Seoul, Korea2Department of Radiology, Eulji General Hospital, Eulji University School of Medicine, Seoul, Korea

Unilateral Chest Wall Anomaly in a Patient with Gardner’s Syndrome
374 jksronline.orgJ Korean Soc Radiol 2014;70(5):373-377
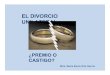
performed 19 months later showed no changes in these lesions. Precontrast CT showed two adrenal masses, of less than 10 Hounsfield units, which were diagnosed as adrenal adenomas (Fig. 2E).
Based on the clinical, colonoscopic, and radiologic findings, the patient was diagnosed with Gardner syndrome. A preopera-
adenoma with low grade dysplasia following surgical excision. Axial postcontrast CT images showed soft tissue tumors with heterogenous density around the left paraspinal and quadratus lumborum muscles (Fig. 2B), the subcutaneous fat layer of the left thorax (Fig. 2C) and along the right ninth intercostal muscle (Fig. 2D), suggesting desmoids tumors. A repeat examination
Fig. 1. Colonoscopy and endoscopy in a 32-year-old man with Gardner’s syndrome.A. Colonoscopy reveals extensive polypoid lesions along the entire colon. B. A 5 cm sized polypoid mass is noted 10 cm above the anal verge, which was confirmed as being a tubular adenoma with low grade dysplasia following surgical excision.C. Endoscopy shows numerous small polypoid lesions on the gastric wall, which are confirmed by endoscopic biopsy as being tubular adenomas with low grade dysplasia.
BA C
Fig. 2. Postcontrast CT of the abdomen in a 32-year-old man with Gardner’s syndrome. A. Axial postcontrast CT scan shows an intraluminal polypoid mass (arrows) with perirectal infiltration in the upper rectum, which was confirmed as being a tubular adenoma with low grade dysplasia following surgical excision (same lesion with Fig. 1B). B-D. Axial postcontrast CT images, showing soft tissue tumors of heterogenous density (arrows) around the left paraspinal and quadratus lum-borum muscles (B), the subcutaneous fat layer of left thorax (C), and along the right ninth intercostal muscle (D), suggesting desmoids tumors. E. Axial noncontrast CT scan, showing a left adrenal mass (arrow) of less than 10 Hounsfield units, suggesting an adrenal adenoma.
E
B
D
A C

Eun Hee Song, et al
375jksronline.org J Korean Soc Radiol 2014;70(5):373-377
gene), located at chromosomal band 5q21-q22. Approximately two thirds of all cases of Gardner syndrome are inherited, while one third are due to spontaneous mutation of the APC gene (4, 5). MYH (1p34.3-p32.1) is another gene associated with FAP (4). Symptoms are usually evident by the age 20 years, but they can present at any time between 2 months and 70 years. In gen-eral, the cutaneous and bone abnormalities develop approxi-mately 10 years prior to polyposis (4, 6).
The gastrointestinal manifestations of Gardner syndrome in-clude extensive adenomatous polyps in the colon, adenomatous polyps in the stomach and small intestine and periampullary carcinomas (1, 2, 4, 7). The colon is the most common site of in-volvement but other parts of the gastrointestinal tract may be involved (1). Most of the polyps are very small and difficult to visualize radiologically (4, 7). If left untreated, the potential for malignant transformation of colonic adenomatous polyps ap-proaches 100% by the fourth decade of life (1, 4, 5). Prophylactic resection (total colectomy with construction of an ileoanal pouch)
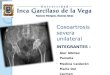
tive chest radiograph (Fig. 3A) showed asymmetric hypertrophy of the right seventh to tenth ribs. Both lungs were clear but the volume of right lung showed slightly smaller than left one. Pre-vious abdominal CT images showed increased size of the med-ullary portions of these lesions, but relatively normal thickness of the cortex (Fig. 3B, C). Intercostal muscles along the right seventh to tenth ribs were hypertrophied as compared with the contralateral ribs (Fig. 3D, E). The patient underwent prophy-lactic total colectomy with ileal pouch-anal anastomosis. The polypoid mass and numerous (more than 350) small polypoid lesions were histologically confirmed as tubular adenoma with low grade dysplasias.
DISCUSSION
Gardner syndrome is now recognized as a variant of FAP, since they share the same genetic alterations (4, 5). These disor-ders are linked to the adenomatous polyposis coli locus (APC
Fig. 3. CT and radiography of the chest in a 32-year-old man with Gardner’s syndrome. A. Posteroanterior plain radiograph of the chest, showing unilateral hypertrophy of the right seventh through tenth ribs (asterisks). B, C. Axial (B) and coronal (C) CT images with bone window shows increased size of the medullary portion of the involved ribs (arrows) with rel-atively normal thickness of the cortex. D, E. Axial (D) and coronal (E) CT images with soft tissue window shows increased size of the intercostals muscles (arrowheads) as compared with contralateral side. Left paraspinal muscle shows swelling with ill-defined mass-like lesion (arrows) due to desmoids tumor (same lesion with Fig. 2B).
E
B
D
A C

Unilateral Chest Wall Anomaly in a Patient with Gardner’s Syndrome
376 jksronline.orgJ Korean Soc Radiol 2014;70(5):373-377
In conclusion, we have described a patient with unilateral hy-pertrophy of ribs and intercostal muscles in a patient with Gard-ner syndrome. Careful attention is necessary to recognize the variable and minute bone abnormalities in patients with Gard-ner syndrome.
REFERENCES
1.RaiAT,NguyenTP,HoggJP,GabrieleFJ.Aggressivefibro-
matosisoftheneckinapatientwithGardner’ssyndrome.
Neuroradiology2001;43:650-652
2.TraillZ,TusonJ,WoodhamC.Adrenalcarcinomainapa-
tientwithGardner’ssyndrome:imagingfindings.AJRAm
JRoentgenol1995;165:1460-1461
3.HatzimarkouA,FilippouD,PapadopoulosV,FilippouG,
RizosS,SkandalakisP.DesmoidtumorinGardner’sSyn-
dromepresentedasacuteabdomen.WorldJSurgOncol
2006;4:18
4.FotiadisC,TsekourasDK,AntonakisP,SfiniadakisJ,Genet-
zakisM,ZografosGC.Gardner’ssyndrome:acasereport
andreviewoftheliterature.WorldJGastroenterol 2005;
11:5408-5411
5.IshidaT,AbeS,MikiY,ImamuraT.Intraosseouspilomatri-
coma:apossiblerareskeletalmanifestationofGardner
syndrome.SkeletalRadiol2007;36:693-698
6.ChangCH,PiattED,ThomasKE,WatneAL.Boneabnor-
malitiesinGardner’ssyndrome.AmJRoentgenolRadium
TherNuclMed1968;103:645-652
7.HarnedRK,BuckJL,OlmstedWW,MoserRP,RosPR.Ex-
tracolonicmanifestationsofthefamilialadenomatous
polyposissyndromes.AJRAmJRoentgenol1991;156:481-
485
8.DolanKD,SeibertJ,SeibertRW.Gardner’ssyndrome.A
modelforcorrelativeradiology.AmJRoentgenolRadium
TherNuclMed1973;119:359-364
9.NandakumarG,MorganJA,SilverbergD,SteinhagenRM.
Familialpolyposiscoli:clinicalmanifestations,evaluation,
managementandtreatment.MtSinaiJMed2004;71:384-
391
should be performed before age 25 years, ideally between ages 16 and 20 years (4, 7). Since duodenal or jejunal adenomatous polyps and their malignant transformations may occur after col-ectomy, patients should be carefully monitored and larger ade-nomas endoscopically removed (7).
More than half of patients with FAP or Gardner syndrome have osseous involvement (7). The most common bone abnor-malities observed in patients with Gardner syndrome are osteo-mas consisting of dense osseous lesions originating on the bone surface (6). Almost all parts of the skeletal system may be in-volved. Rib abnormalities have been reported, including wavy and localized cortical thickening or osteomas of several ribs (2, 6, 8). Except for osteomas, few patients show other types of os-seous manifestations, including osteosarcoma and intraosseous pilomatricoma (5, 7). The recognition of osteomas is important because they frequently precede the appearance of intestinal polyposis and may be an early sign of this disorder (6).
The most common soft tissue lesions of Gardner syndrome are epidermoid cysts on the face, scalp, and extremities (4, 5, 7). Oth-er soft tissue tumors and tumor-like lesions include fibromas, neurofibromas, lipomas, leiomyomas, and pigmented skin le-sions (1, 9). Desmoid tumors appear in 3.5--5.7% of patients and they can appear at any time (4). Common locations are the inci-sion sites, the abdominal cavity and the retroperitoneum. These tumors are considered among the most troublesome manifesta-tions of Gardner syndrome, since they may cause life threatening complications and are usually resistant to treatment (3).
To our knowledge, unilateral chest wall anomaly has never been reported in patients with Gardner syndrome. There has been no report about a reduced long volume in patients with Gardner syndrome. This rare abnormality is possibly related to Gardner syndrome and also can be an incidental finding. The recognition of unilateral hypertrophy of the ribs can be an early sign of Gardner syndrome as well as osteomas. The possible hy-pothesis for unilateral chest wall anomaly is compensatory over-growth of chest wall due to a small lung volume. However the degree of reduced lung volume is minimal and the patient had no pulmonary symptoms. Inversely hypertrophied chest wall might restrict the growth of right lung.

Eun Hee Song, et al
377jksronline.org J Korean Soc Radiol 2014;70(5):373-377
가드너 증후군 환자에 동반된 일측성 흉벽 기형: 증례 보고1
송은희1 · 이소연1 · 박희진1 · 권헌주1 · 김미성1 · 박해원1 · 곽현주1 · 김혜진2
가드너 증후군은 대장용종과, 골종, 연부조직종양 등으로 이루어진 질환으로 골종 이외의 골격계 이상은 보고된 바가 거
의 없다. 저자들은 32세의 가드너 증후군 환자에서 일측성 흉벽 기형이 있어 보고하려 한다. 단순촬영에서 우측의 7~10번
째 갈비뼈가 비후되어 있었고, 단층촬영에서는 골 수질의 크기가 커져 있으나 피질은 정상두께였다. 우측의 7~10번째 늑
간근육은 건측에 비하여 비후되어 있었으며, 양측 폐야에 국소병변은 없었으나 우측 폐의 부피가 좌측 폐에 비하여 약간
작았다.
1성균관대학교 의과대학 강북삼성병원 영상의학과, 2을지대학교 을지병원 영상의학과